
Abstract
The COVID-19 pandemic in the US prompted a sudden shift to telehealth in nurse-led care sites which provide services to diverse geolocations. Using a lens of intersectionality, this study characterizes provider and patient-perceived best and promising practices emerging from geographical variation. The aim of this study was to identify best practices of implementing telehealth in nurse-led care models in Colorado through patient and provider experiences of the sudden implementation of telehealth that can enhance health equity. In this exploratory/descriptive qualitative study, a purposive sample of 18 providers and 30 patients were interviewed using a guide informed by the RE-AIM implementation and evaluation framework to capture the contextual experiences related to the sudden shift to telehealth. Textual theme analysis and reflexive team strategies guided the interpretation. Four primary themes of perceived best practices were identified: using multiple modalities, tailoring triage and scheduling, cultivating safety through boundaries and expectations, and differentiating established versus new patient relationships. The findings suggest that telehealth is a flexible and powerful tool to enhance the delivery of equitable care through nurse-led care models within diverse communities such as the one represented in this study. Nurse leaders are positioned to participate in innovative research and create policies and protocols to ensure telehealth is a viable resource to deliver equitable, safe, and accessible high-quality healthcare.
Keywords
Introduction
The COVID-19 pandemic created disruption across the globe in social, economic, and healthcare domains. To decrease exposure of SARS-CoV-2 among patients and the healthcare workforce, a sudden transition to care delivery via telehealth occurred in mid-March 2020 (Monaghesh & Hajizadeh, 2020). Prior to the COVID-19 pandemic, widespread adoption of telehealth in the United States had been constrained due to technological, financial, legal, and human resource issues (LeRouge & Garfield, 2013). However, policy changes from the federally funded Centers for Medicare and Medicaid Services supporting provider reimbursement for telehealth visits similar to office visits (Hong et al., 2020) facilitated a rapid shift to virtual care (Hollander & Carr, 2020). The rapid expansion of telehealth in response to COVID-19 created an opportunity to study the innovations and challenges encountered by patient and provider experiences that help characterize perceived best and promising practices to identify the ways in which telehealth may be best utilized to enhance health equity moving forward.
Background
A review of telehealth implementations before COVID-19 revealed telehealth to be equivalent to in-person care for a wide variety of chronic and behavioral health conditions, with the potential to improve access for rural residents or those with transportation issues (Shigekawa et al., 2018). However, in a national consumer survey, Park et al. (2018) noted that low-income respondents used live video communication less than other groups. While telehealth and remote monitoring have been highly effective in managing chronic disease conditions, a randomized controlled trial demonstrated that this modality had a lower impact and utilization among low-income, Black, and Hispanic patients (Pekmezaris et al., 2019). This variance creates concerns about the possibility of telehealth paradoxically widening the inequities among historically underserved populations. These include rural communities, older adults, racial and ethnic minorities, and those with low socioeconomic status, who have lower rates of smartphone ownership, home broadband access, internet use, and basic digital literacy (Lau et al., 2022; Nouri et al., 2020).
In the state of Colorado, innovative nurse-led models of care at the registered nurse and advanced practice registered nurse levels are a vital component of healthcare delivery for the most ethnically, geographically, and economically diverse populations. Three successful nurse-led healthcare delivery models have been established through federally qualified health centers (FQHC) (Weber et al., 2021), certified nurse-midwifery practices (CNM) (Nodine et al., 2020), and the Nurse-Family Partnership home visitation program (NFP) (Neal & Fixsen, 2020). These models in Colorado experienced a rapid shift to telehealth in response to legislative state actions addressed in bipartisan Senate bill 20-212, signed by Governor Polis on July 6, 2020 (State of Colorado, 2020). The American Academy of Nursing clearly articulated nurses’ expanded roles in pandemic response, recognizing their crucial role in care coordination, primary care, and strengthening the public health infrastructure (Corless et al., 2018).
According to Lewis and Latney (2002), best practices are used to continuously, collaboratively, and systematically examine the strengths and weaknesses of different internal procedures. Best practices for telehealth have been recommended by the Department of Health and Human Services to support its use in the management of chronic conditions, maternal health services, behavioral health services, and with patients in rural areas among others (Health Resources and Services Administration, n.d). While these guidelines outline equipment needed and suggest the types of visits that are best suited for telehealth, they fail to include patient and provider experience in the recommendations. Several studies have evaluated patient and provider experiences with telehealth both prior to and after the onset of the COVID-19 pandemic (Barney et al., 2020; Gomez et al., 2021; Khairat et al., 2023; Powell et al., 2017). Findings from these studies suggest that there are changes within the patient-provider interaction that yield satisfaction and improved access for some, and infrastructure challenges and increased barriers exist for others (Gomez et al., 2021; Khairat et al., 2023; Powell et al., 2017), while also raising concerns for health equity (Barney et al., 2020). Previous recommendations from the literature have included the need to clarify expectations for the type of care that may be provided via telehealth, to improve usability of this modality, to ensure confidentiality, and to limit provider burden of facilitating the visit. No studies included patient and provider perspectives from nurse-led facilities. The current study aimed to identify themes of best and promising practices as grounded in patient and provider experiences within geographically diverse nurse-led care settings to inform the delivery of high-quality, safe, accessible, and equitable care to ethnically and geographically diverse communities.
Conceptual Research Framework
A theoretical lens of intersectionality was adopted to conduct and analyze qualitative data from interviews situated within the complex interconnected health system during the COVID-19 pandemic. Intersectionality is “a way of understanding and analyzing complexity in the world, in people, and in human experiences” (Collins & Bilge, 2016, p. 2) by considering the diverse interconnected social, political, and organizational factors that influence power imbalances and inform health inequalities. By employing intersectionality to guide this qualitative research process (Abrams et al., 2020), the research team captured the lived and multifaceted experiences of people's use of telehealth within diverse ethnicities, social and economic positions, and geographical locations.
Methods
In this descriptive exploratory qualitative study conducted between March 2020 and May 2021, semi-structured interviews were completed with patients and providers in English and Spanish and analyzed using a general inductive approach with an emergent design. The study protocol was approved by the Colorado Multiple Institutional Review Board (COMIRB-20-1513).
Setting
Study participants were recruited from a larger study evaluating the impacts of the implementation of telehealth in five nurse-led care sites across rural and urban communities in Colorado during the COVID-19 pandemic (Barton et al., 2023). These sites provide care to close to 50,000 low-income, ethnically diverse Coloradans living in urban, rural, and frontier regions of the state within three innovative nurse-led models of care: (1) community-based primary care/behavioral health in three FQHC located in frontier, rural, and urban settings; (2) the NFP implemented statewide; (3) and two CNM practices serving urban and suburban communities. Each of these sites were provided a stipend to promote participation in the study through advertisements disseminated in patient and provider portals with an invitation to participate using a linked survey.
Sample
Eligible participants were those who either provided or received care at one of the sites during the study time frame, 12 years and older, and English or Spanish-speaking. Survey respondents who volunteered for an interview were recruited through phone and email. Although the initial response was high with approximately 70% of survey respondents volunteering, recruitment became difficult over time with rejections related to time limits, inability of researchers to reach the population after three attempts, and personal or professional challenges in an ongoing pandemic. While convenience sampling was initially used, maximum sample variation was also sought to ensure heterogeneity in terms of nurse-led model, age, gender, ethnicity, and geographic location. Concurrent data collection and analysis informed the final sample size through cross-site informational saturation.
Data Collection
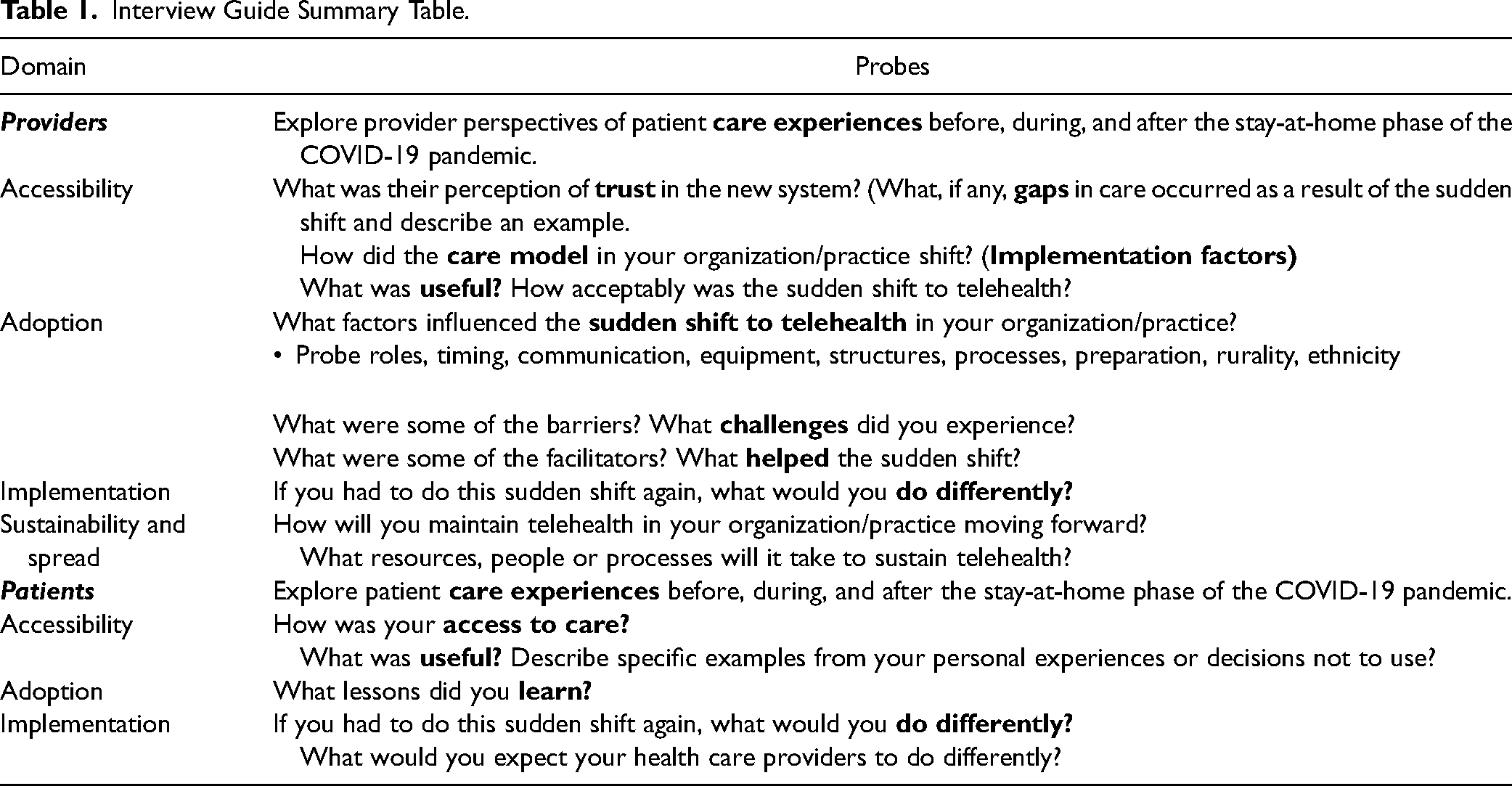
Individual interviews were conducted via Zoom or telephone by study-trained nurse research assistants and qualitative research experts, each lasting 20–60 min. The researchers used a semi-structured interview guide (Table 1) informed by Reach, Efficacy, Adoption, Implementation and Maintenance (RE-AIM) framework domains (Holtrop et al., 2018) to identify experiential nuances of the implementation of telehealth. Key areas of prompted discussion with patients included access to services, perceptions about telehealth, barriers, and needs, while paying special consideration to context and social determinants of health (e.g., rurality, gender, income, and ethnicity). Healthcare providers were asked to describe their experiences which addressed key topics of acceptability, adoption, implementation, and sustainability of the telehealth environment. The interview guide was translated into Spanish and culturally tailored by a native-speaking researcher and iteratively revised across the interviews to probe emerging themes. Interviews were conducted in the participants’ preferred language with native English or Spanish speakers. Verbal consent was obtained from interview participants.
Interview Guide Summary Table.
Analysis
Theme analysis commenced with the first participant interview and preceded alongside subsequent data collection until informational saturation was met (Creswell & Poth, 2018). Zoom and telephone interviews were digitally recorded, and English transcripts were created using Zoom transcripts when available. These transcripts were reviewed and cleaned by the research team. Spanish interviews were professionally translated from recordings and curated by native-speaking team members. ATLAS.ti V9 qualitative data analysis software was used by the research team to assist with data storage, coding, and memoing (Paulus & Lester, 2021). All team members were involved in the process of coding, with one lead methodologist acting as project manager. First cycle descriptive and in-vivo codes were revisited on a regular basis to define, rename, combine, and create coding groups to avoid replication (Saldana, 2016). Themes were identified over time as the patterns of codes were explored in reference to the study aim and later deductively with an intersectionality lens.
The research team was intentional in using rigorous procedures and strategies to establish confidence in the findings of this study. A team-based iterative, inductive, and deductive toolkit of analytic strategies was used to address credibility, dependability, confirmability, transferability, and authenticity (Cope, 2014). These strategies included field notes, memoing, general theme analysis, consultative and reflexive analysis, participant validation, and participant and triangulation. To reduce the risk of bias, analytical diaries and weekly team meetings aided in reflexive engagement, reflecting upon emergent categories, and confirming that the emergent codes and identified themes were grounded in the data. Validity and transparency were addressed by staying close to the data as text through the use of participant quotations and ensuring the participants’ own meaning and perspectives were represented. The study was reported in line with the Consolidated Criteria for Reporting Qualitative Research checklist (Tong et al., 2007).
Results
Eighteen healthcare providers and 30 patients were included in the study from four geographically varied locations representing three nurse-led models of care (Table 2). The providers were represented by white Caucasian non-Hispanic English-speaking women who worked in urban (n = 13) and rural locations (n = 5). While the patient demographics were more diversified, they were 20 years or older, predominately represented female, white, non-Hispanics (n = 21). Ten percent of the patient participants were male, 17% were primary Spanish-speaking, and 28% identified as Hispanics. All participants either provided or received care in the telehealth environment during the sudden implementation of telehealth.
Participant Demographic Table.
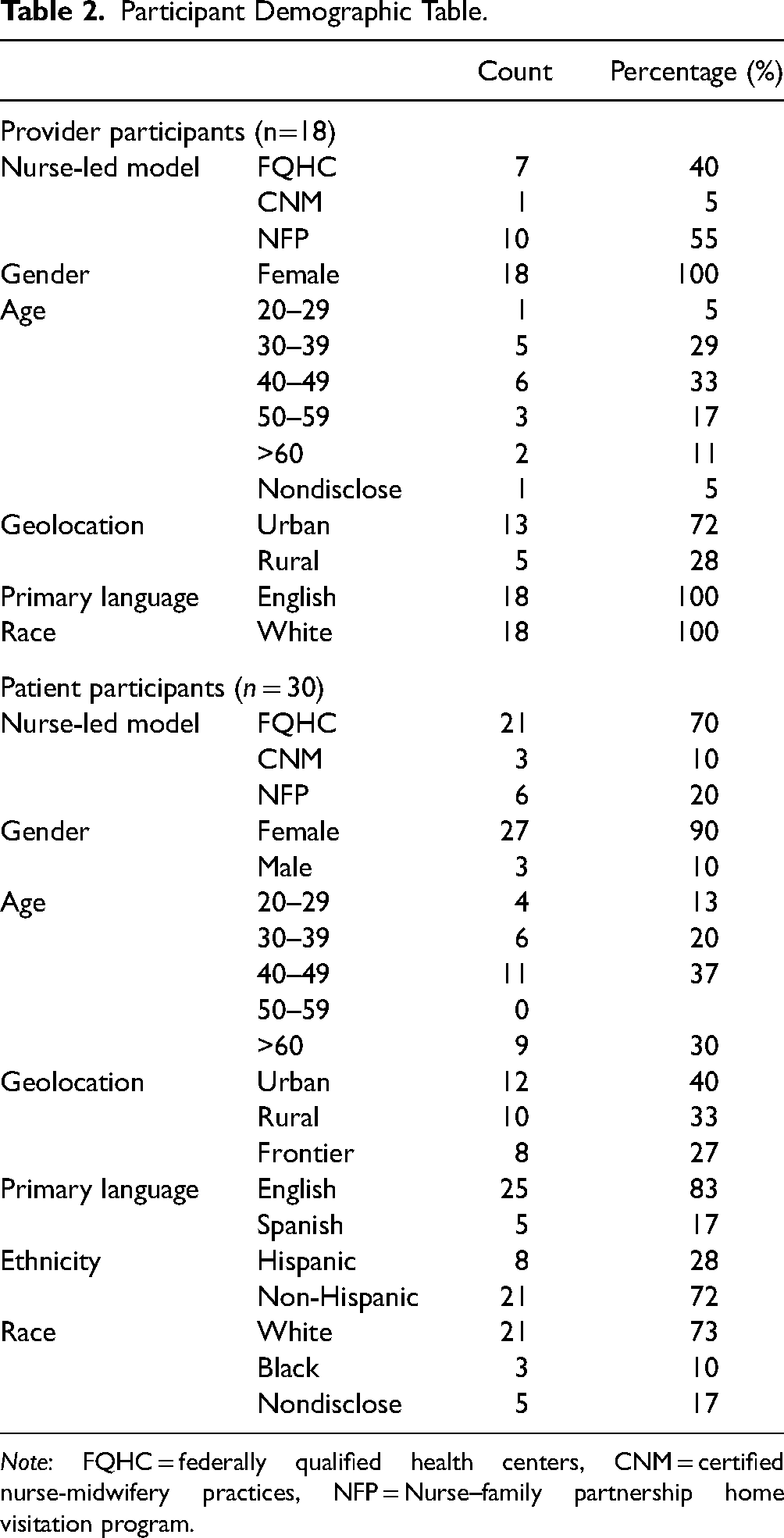
Note: FQHC = federally qualified health centers, CNM = certified nurse-midwifery practices, NFP = Nurse–family partnership home visitation program.
Four themes were identified as related to evolving perceived best practices in telehealth: (1) using multiple modalities, (2) tailoring triage and scheduling, (3) cultivating safety through boundaries and expectations, and (4) differentiating established versus new patient relationships. While these themes converge and interconnect in aspects (Figure 1), they are unique in informing meaning within the data and shaping our emerging understanding of best and promising practices to deliver high-quality care within the boundaries of the technological environment to support ethnically, geographically, and economically diverse communities.
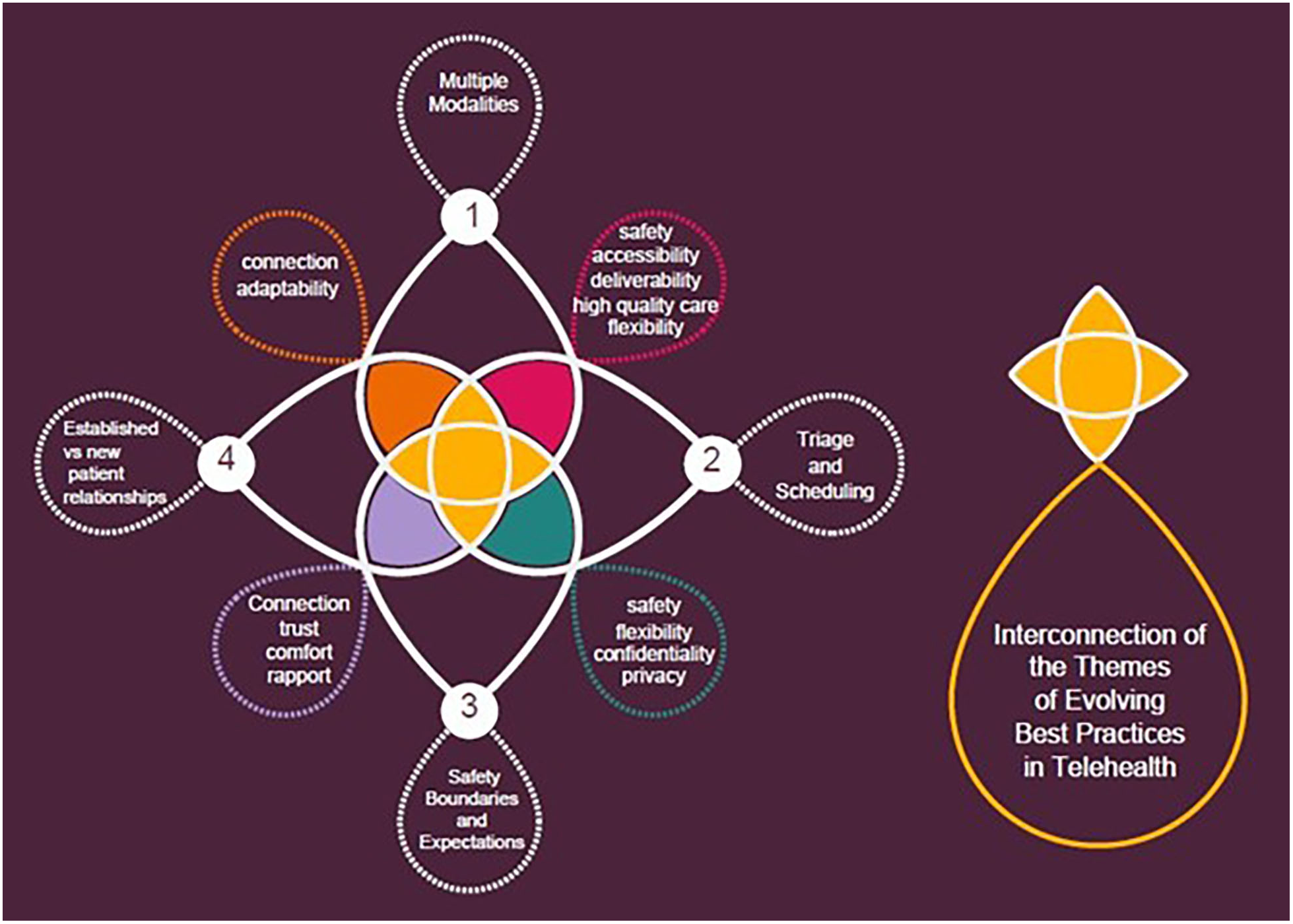
Interconnection of Themes.
Using Multiple Modalities
The first theme describes the opportunities that telehealth introduced for healthcare providers to provide and maintain access to high-quality, safe, and accessible healthcare within diverse communities and the need for these providers to remain flexible when implementing modalities of telehealth. The modalities of delivering care mentioned in this study included live video, audio-only, chat and text, or traditional in-person. Several healthcare provider participants discussed how telehealth introduced new opportunities for healthcare delivery that were not present before the COVID-19 pandemic. Equitable access to mental health care was challenging before and during the pandemic. However, some of the mental healthcare provider participants shared stories of the opportunity to provide high-quality access to their patients through the telehealth modalities of videoconferencing and phone calls. So, she (patient) was 16 then and I thought about telehealth is going to be a nightmare because I was having trouble connecting with her in real life. She's had severe mental health issues, you know, really depressed, it's just like this is gonna be really difficult. And she did better on telehealth. I mean she sat in her bedroom on her bed, and the baby is crawling around, and she like opened up. (Provider 1, Rural)
I have to figure out how we’re going to do this … remotely, what are we going to do, and so I would kind of formulate a procedure and then we try it in real life with a patient, and then we like, okay, so that didn't work as well, how can we adapt? There was also some learning as you go. (Provider 10-Urban)
Tailoring Clinical Triage and Scheduling
The second theme describes the complexities with providing safe clinical triage and scheduling nuances that the sudden shift to telehealth introduced to healthcare providers, healthcare team members, and patients. Often provider participants reported the need for established protocols to assist healthcare team members in matching the best patient to the best encounter modality. Provider and patient participants identified the need for patients to be informed and educated about telehealth before the encounter. Because telehealth has both video and audio call, it gets confusing when telehealth is scheduled because you aren't sure which is being scheduled, from a provider's end. It's supposed to be a phone call, and not a Zoom, ya know, and we have to use up appointment time. I think using the word telehealth for two different things is confusing for the patient. (Patient 12-Frontier) I think one other thing is this possibility of we're missing something when we're not examining the patient. I’ve been a midwife for (many) years … and you know that one minute of listening, hearing something that wasn’t quite right that needed emergent care. (Provider 15-Urban) I think with any telehealth it is much better than the phone to see people physically, and even when there are obvious limitations, you get a better sense of like a postpartum mom, is she swollen, is (she) you know looking yuck? (Provider 15-Urban) The format of telehealth helps you in a follow up visit because you had the physical appointment in person, where you were able to be assessed, start working on some solutions, but then you are able to follow up on the phone to think about what's the next step. (Patient 8-Frontier)
Cultivating Safety Through Boundaries and Expectations
The third theme describes the need for healthcare providers and teams to create procedures and protocols addressing the variables of environmental safety in the telehealth visit. Several nurse participants who provide in-home perinatal care spoke to the challenges of obtaining intimate partner violence assessments within the telehealth patient encounter. What ways can we make sure that she's safe and that there's nobody else there to hear her answer these questions, or you know, is there someone in the room? (Provider 2-Rural)
Their identified challenges speak to the need for cultivating safety assessment protocols and communicating these protocols to all patients. Some provider participants shared their experiences with personal knowing, described as intuition. These participants told stories of knowing when a patient was not feeling comfortable or when someone else was in the room but not on camera. Yet these nurses were unsure how to proceed in the telehealth visit, ensuring the patient's safety and privacy. You're doing an intimate partner violence assessment and you think no one is there and then you don't know who's walking into the home five minutes later, after you've made sure no one is there and you're still asking those questions. Something is going on; you know there's another conversation going on off screen. (Provider 3-Rural) I'll just say hey let's reschedule, this isn't a good time because you know, that's not really safe for you to be video chatting and driving. I'll just tell it like you know, I wanted to talk today, I don't know if you really want to talk about it when you're at the grocery store, so why don't we reschedule. (Provider 11-Rural)
Differentiating Established Versus New Patient Relationships
The fourth theme communicates the patient's experience of developing and maintaining trust and connection in established versus new relationships with their healthcare providers and healthcare team members through and within the telehealth virtual environment. Multiple patient participants expressed feelings of comfort, trust, and connection with their healthcare provider when the healthcare relationship was previously established in-person before the implementation of a telehealth encounter. Some patient participants shared their feelings of not being known, a lack of rapport, a lack of connection, and a lack of trust when they established care with a new provider in the telehealth virtual environment. Other patients expressed being open to and comfortable with establishing new healthcare relationships via telehealth when they had experienced prior positive telehealth encounters. I think the relationship that I had with my doctor and my counselor before I started telehealth helped me to be even more comfortable with the telehealth with my psychiatrist that I have not met in person. (Patient 22-Rural)
It was cold, whether I was in-person with him or on telehealth with him, just very cold. And I just got the overwhelming feeling that he just wanted to get on to the next appointment. (Patient 14-Frontier)
Discussion
The COVID-19 pandemic revealed systemic health inequities, including barriers to accessing care and quality of care that disproportionately impacted diverse communities across the United States (Lau et al., 2022; Poulson et al., 2021). The themes identified help to define the facilitators and barriers around best practices that should be addressed by providers wishing to implement or increase the use of telehealth. The need for flexibility to address these barriers and planning for when and how to utilize telehealth is clearly represented in the data. Providers in this study voiced frustration about disparities in technological infrastructures and multiple, changing telehealth modalities that made initiating telehealth care challenging. Cohen (2021) describes the intersectional challenges that complicate rural health care, including access to transportation, financial resources, and limited income. Telehealth can provide an alternative to in-person care that limits the need for travel, however, many rural areas lack broadband access (Dornauer & Bryce, 2020; Graves et al., 2021) compared to their urban counterparts. Telehealth also presents challenges in urban areas, with non-English-speaking and low-income patients having less access to technology (Park et al., 2018; Pekmezaris et al., 2019).
Despite challenges accessing safe and equitable care through telehealth, telehealth is shown to be an effective tool for reaching hard-to-reach patients. Current literature provides examples of shared positive experiences between mental health providers and patients with telehealth reducing or eliminating barriers to care such as excessive travel. Nicholas et al. (2021) found that telehealth facilitated engagement between patients and providers by eliminating barriers and that patients using telehealth to access care felt supported and respected. Provider participants in this study indicated that appropriate triage and scheduling were essential for effective care delivery via telehealth. This study's finding is consistent with results by Gentry et al. (2021), which emphasized the importance of institutional support to design a process for triage and scheduling along with the proactive investment of time and capital to assess technologic infrastructure and clinician readiness to deliver care using telehealth.
The implications of telehealth on cultivating safety screening, privacy, and confidentiality are important themes consistent with emerging international literature. The ability to accurately assess risk for violence is commonly named a concern among telehealth providers in Lebanon and Australia (Ayres et al., 2021; Helou et al., 2020). The need to ensure that the patient is in a space that allows for privacy and safety was a concern, particularly among providers of social services or mental health services (Ayres et al., 2021; Nicholas et al., 2021). While a survey by Nicholas et al. (2021) noted that only 36% of providers felt telehealth had a negative impact on their ability to provide safe care, follow-up analysis of open-ended responses from this sample indicated clinicians had concerns about telehealth impacting the ability to perform adequate risk assessments or to ensure that clients have a private and safe space for telehealth visits. Established protocols for ensuring appropriate risk and safety assessments and patient privacy should be an integral component of telehealth practice.
While some providers have indicated that they found telehealth equally appropriate for new and established patients (Gentry et al., 2021), most emerging studies support this study's findings that telehealth may be a barrier to establishing rapport in a new patient-provider relationship. While some providers have gone so far as to say that an initial visit cannot be done remotely (Helou et al., 2020), many state that it is difficult to establish a therapeutic relationship over telehealth (Altman et al., 2023; Nicholas et al., 2021). Specific to developing relationships in community partnerships, there has been an emphasis on the importance of establishing a relationship with clients in-person that creates a foundation for enhancing future telehealth encounters (Ayres et al., 2021). Providers incorporating telehealth into practice should consider the nature of the patient-provider relationship and the ability to establish rapport in the relationship over telehealth versus in-person initial interactions.
Implications for Nurse Leaders in Healthcare Policy and Practice
As the nursing discipline continues to evolve and adapt to technology, nursing practice is called to find innovative ways to deliver care and to adapt to urgent health challenges during a pandemic and beyond. Nurses, nurse leaders, and healthcare policy advocates should design telehealth services that incorporate lessons learned and best practices from the evidence (Kissler et al., 2023). Implications for policy and practice include: addressing access disparities by supporting legislative actions that promote a robust and equitable technological infrastructure which remains reimbursable; policies and protocols to ensure safe, appropriate engagement with telehealth care; policies, protocols, and education around the types of visits most suited to telehealth; and inclusion of nurse-led practices as reimbursable telehealth models of care.
There is a clear need to prioritize policies that address technological inequalities to ensure widespread access to telehealth services (Lau et al., 2022; Shahid et al., 2023). Access to technology should be considered an essential determinant of health. As such, policy leaders should work to build technology and internet infrastructure that supports the broad range of modalities available as telehealth services, to include audio-only, live chat, and Apple Facetime video. It is imperative to support and introduce legislative actions that improve healthcare delivery for ethnically, geographically, and economically diverse communities while ensuring the systems implemented do not disadvantage those who have been historically marginalized or oppressed.
This study provides valuable perspectives which indicate the ongoing need for nurses to be proactive in addressing safety standards and privacy practices in the telehealth environment. The providers in this study emphasized the need for creating and implementing policies and protocols that address ethical questions around interpersonal violence and determine the patient's safety in their home environment. Nursing practice will need to also include training for patients about how to maximize benefit from a telehealth visit by ensuring they are in a private, appropriate environment where they can engage with providers without distractions or breaches in security standards.
Policies should be established that promote proper screening of visit requests to determine the best fit for telehealth services. Consideration for telehealth should include visit type, presence or absence of existing patient–provider relationship, and accessibility of appropriate telehealth modality by provider and patient. Nurses should include education for patients on the types of needs that are best met via telehealth. Additionally, protocols that appropriately triage visits to the most suited modality should be established.
Finally, the context of telehealth services and insurance reimbursement remains uncertain and is situated upon shifting legislative grounds. Nurses need to lead the way by developing and advocating for federal and state policies that improve quality healthcare access that is nurse-led. Nurses must have an infrastructure to document the quality and value-driven care that they provide while working in systems that allow for billing without restrictions. Nursing leaders must advocate for and continue to support bills which aim to protect local and universal access to telehealth services by partnering with their legislative representatives.
Strengths and Limitations
This study's strengths include the geographically representative nature of the participants served by both urban and rural clinical sites, the availability to conduct interviews in the preferred language, and the collection of rich qualitative data over the course of rapid telehealth implementation during the COVID-19 pandemic. There are also several limitations to this study. While this study has a large sample size, the learnings are contextually situated and nuanced and are not expected to be transferrable to all clinical settings. Second, our qualitative process continued data collection up to the point of saturation of themes for analysis, although it is possible that some factors were not discussed or missed during the semi-structured interviews. Third, our study focused on the experiences of individuals who engaged in telehealth and were comfortable participating in interviews virtually, but perspectives of individuals who did not engage in telehealth were not represented. We were unable to recruit enough Hispanic or Spanish-speaking rural patients to match the region's demographic. Additional research is needed to understand experiences among those for whom a digital divide, a language barrier, or hesitancy in engaging in conversations remotely might have occurred.
Conclusion
Telehealth can be a powerful tool to increase access to safe and equitable nursing-led models of care within frontier, rural, and urban communities. Grounded in experiential evidence, this study emphasizes important considerations for implementing or modifying a telehealth program, including using multiple modalities, tailoring triage and scheduling, cultivating safety boundaries, and differentiating the needs between established versus new patients. As patients and their support systems demand more flexibility for reimbursable technologically driven and high-quality healthcare service delivery, the nursing profession will need to evolve practices to meet these demands. It is essential that nursing leaders within complex healthcare systems collaborate to establish and implement best practices within telehealth environments to ensure the protection, promotion, and optimization of equitable health outcomes for patients now and for future generations.
Footnotes
Acknowledgments
Amy Joachim, Lorraine Garcia, Cheryl Taccogno, Rosario Medina, Jennifer Villalobos.
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded under grant number 5 R01 HS028085 from the 10.13039/100000133Agency for Healthcare Research and Quality (AHRQ), 10.13039/100000016U.S. Department of Health and Human Services (HHS). The authors are solely responsible for this document's contents, findings, and conclusions, which do not necessarily represent the views of AHRQ. Readers should not interpret any statement in this report as an official position of AHRQ or of HHS. None of the authors has any affiliation or financial involvement that conflicts with the material presented in this report.