
Abstract
Multimorbidity affects 75% of older adults (aged 65 years and older) in the United States and increases risk of poor medical outcomes, especially among the poor and underserved. The creation of a Medicaid option allowing states to establish health homes under the Affordable Care Act was intended to enhance coordinated care for Medicaid beneficiaries with multimorbidity. The Community-Based Health Home (CBHH) model uses the infrastructure of the Adult Day Health Center (ADHC) to serve as a health home to improve outcomes for medically complex vulnerable adults. Between 2017 and 2018, we used a sequential explanatory mixed-methods approach to (a) quantitatively examine changes in depression, fall risk, loneliness, cognitive function, nutritional risk, pain classification, and health care utilization over the course of 12 months in the program and (b) qualitatively explore the perspectives of key stakeholders (registered nurse navigators, participants, ADHC administrators, and caregivers) to identify the most effective components of CBHH. Using data integration techniques, we identified components of CBHH that were most likely driving outcomes. After 12 months in CBHH, our racially diverse sample (N = 126), experienced statistically significant (p < .05) reductions in loneliness, depression, nutritional risk, poorly controlled pain, and emergency department utilization. Stakeholders who were interviewed (n = 40) attributed positive changes to early clinical intervention by the registered nurse navigators, communication with providers across settings, and a focus on social determinants of health, in conjunction with social stimulation and engagement provided by the ADHC. CBHH positions the ADHC as the locus of an effective health home site and is associated with favorable results. CBHH also demonstrates the unique capacity and skill of registered nurses in integrating health and social services across community settings. Continued exploration of CBHH among diverse populations with multimorbidity is warranted.
The 20th century saw a dramatic increase in life expectancy. However, longer lives are not necessarily synonymous with high quality of life or high levels of functioning (Angel, Angel, & Hill, 2014). In 2018, nearly 85% of adults in the United States over 65 years of age had at least one chronic condition and 75% experienced multimorbidity (Centers for Disease Control and Prevention [CDC], 2018), which is defined as having at least two chronic conditions (Wallace et al., 2015). Multimorbidity is a common and burdensome condition that can affect quality of life, increase medical needs, and increase the likelihood of living more years of life with disability (Vetrano et al., 2017). In older persons with multimorbidity, aging and chronic disease fuel one another in a vicious circle, each accelerating the progression of the other (Fabbri et al., 2015; Yokota et al., 2016). Among adults in the United States aged 18 and older, 71% of total health care spending is associated with care of those with more than one chronic condition (CDC, 2018).
Multimorbidity specifically increases the complexity of care management (Casado, van Vulpen, & Davis, 2011) and failure to coordinate care across primary, secondary, and tertiary health care settings increases individuals’ risk of poor medical outcomes (Parekh, 2011). This risk is especially pronounced among vulnerable groups with low levels of education and income, for whom longer lives may bring prolonged periods of poor functioning, dependence on caregivers, and poverty (Angel et al., 2014). Due to its complexity and the lack of clear evidence steering its management, effectively addressing multimorbidity represents a major challenge for clinicians, researchers, and policymakers (Barnett et al., 2012: Prince et al., 2015).
Efforts to redesign the U.S. health care delivery system to meet the needs of patients with multimorbidity by integrating health and social services have been slowly emerging since the passage of the Affordable Care Act in 2010 (Donelan et al., 2019). Successful interventions to address multimorbidity require a patient and family-centered approach to care throughout the health system, but understanding how to deliver this care effectively and efficiently remains a challenge (Boyd & Fortin, 2010).
Federal policies to address this challenge have included the creation of an optional Medicaid State Plan benefit for states to establish Health Homes under the authority of the Affordable Care Act of 2010, Section 2703 (1945 of the Social Security Act). The Health Home model is intended to coordinate care for people with Medicaid who have complex chronic conditions. It is in some ways similar to the more commonly discussed patient-centered medical home, but it is distinct in its focus on “high-cost, high-need populations” and facilitating access to community services and support (Ormond, Richardson, Spillman, & Feder, 2014). Moreover, a variety of providers can serve as health homes, including home health agencies and community mental health centers (Ormond et al., 2014). The Community-Based Health Home (CBHH) model, described later on, was designed to incorporate Health Home required services (comprehensive care management, care coordination, health promotion, comprehensive transitional care/follow-up, patient and family support, and referral to community and social support services) using the existing infrastructure of the strength-based Adult Day Health Care model, which has existed in the United States since the early 1980s.
Adult Day Health Centers (ADHCs) are increasing in number across the United States. As of 2017, they served more than 260,000 community-dwelling chronically ill and functionally impaired individuals annually, the majority of whom lived below federal poverty thresholds (National Adult Day Services Association [NADSA], 2017). Given the prevalence of chronic conditions such as hypertension (46%), diabetes (31%), and dementia (46%) among participants, ADHCs are becoming a preferred platform for chronic disease management and long-term care services among older adults with multimorbidity (NADSA, 2017). These community-based centers are designed to provide both a socially supportive environment and health services to adults who require supervised care and health services during the day.
ADHCs are typically state licensed, certified, or both (Dabelko & DeCoster, 2007). Licensure requirements for ADHCs vary by state. Certification implies that an ADHC has been evaluated and approved by the state according to standards set by the U.S. Department of Health and Human Services (U.S. HHS; NADSA, 2017). ADHC staff members, who supervise and interact with their participants for at least 4 hours a day, often possess a great deal of clinical data which are underutilized by clinicians in other settings. Staff within ADHC centers are well positioned to recognize, optimize, and holistically address the biopsychosocial factors affecting health, such as access to health services, medication management and compliance, food insecurity, health literacy, and social isolation. They also support wellness and prevention (Sadarangani & Murali, 2018).
There is evidence within the extant literature to support an association between ADHC use and improved quality of life, reductions in institutional placements, and other favorable outcomes, such as improvement of mental health and prevention of isolation (Fields, Anderson, & Dabelko-Schoeny, 2012; Kelly, Purveen, & Gill, 2014; Sadarangani & Murali, 2018). However, traditional free-standing ADHCs, of which there are more than 4,600 across the United States, typically lack resources or mandates to integrate care across settings (e.g., primary and acute care). Despite being viewed as an important setting for disease management, little, if anything, is known about the capacity of ADHCs to serve as health homes that coordinate care for individuals with multimorbidity across health settings (Centers for Medicare and Medicaid Services [CMS], n.d.).
The purpose of this article is to describe a study that evaluated outcomes associated with the CBHH model. Specifically, we used a mixed-methods approach to (a) examine changes in social and emotional aspects of health (depression, fall risk, loneliness, cognitive function, nutritional risk, pain classification, and health care utilization) after 12 months in the program and (b) qualitatively explore the perspectives of key stakeholders (registered nurse navigators [RN-Ns], participants, administrators, and caregivers) to identify the most effective components of CBHH.
Background
The CBHH model is the first in the nation to use the ADHC as a health home for medically complex vulnerable adults. The CBHH design builds on the strength-based nature of the ADHC model, which utilizes interdisciplinary team (IDT) services that are individualized and person-centered. These services include daily nursing surveillance and treatments combined with skilled therapies. Beginning in 2012, the California-based Alliance for Leadership and Education (ALE), which serves as the nonprofit research and development arm of the California Association for Adult Day Services, designed, implemented, and tested the CBHH model. Using the ADHC as a health home to advance the nation’s Triple Aim of health care, which refers to (a) improving the experience of care, (b) improving the health of populations, and (c) reducing per capita costs of health care (Berwick, Nolan, & Whittington, 2008), is a novel and promising approach.
In partnership with primary care providers, the CBHH model sets out to comprehensively strengthen effective care and support for vulnerable, chronically ill adults (ALE, 2016). The CBHH model is rooted in intensification of the ADHC’s nursing care coordination and in-depth needs assessment. In addition, CBHH delivers transitional care support, patient activation, and education to advance health literacy (ALE, 2016). These services are provided through the inclusion of a “registered nurse navigator (RN-N)” within the ADHC IDT (ALE, 2016). The RN-N deepens understanding of the highest risk individuals’ unique challenges and social environments by conducting health and psychosocial assessments, making home visits whenever needed, and facilitating care transitions (ALE, 2016). A full-time RN-N manages an average case load of 19 patients, providing an average 2 hours of high-intensity care to each participant on a weekly basis (ALE, 2016). As a result, specialized nursing and care management expertise are extended beyond the walls of the ADHC center and into the participants’ homes along with their medical and community care settings. This creates an individualized system of care and unifies care across the biopsychosocial continuum (ALE, 2016).
RN-Ns work with the ADHC’s IDTs (registered nurse, physical therapist, occupational therapist, speech pathologist, social worker, and dietician) in coordination with the participant’s physician. The RN-N’s priority is to promptly address emerging crises within a high-risk caseload of patients. The RN-N also supports the physician’s care plan, coordinates with caregivers and other providers, and formulates patient-centered action plans to stabilize and improve participants’ health. The overall goals of CBHH are to stabilize individuals’ social, medical, and psychological conditions and reduce unnecessary utilization of health services while improving quality of life and self-care capacity.
The CBHH RN-Ns are trained in motivational interviewing techniques, which help participants identify and change behaviors that heighten their risk of health problems (Bundy, 2004). In addition, they receive training in using the battery of CBHH standardized screening and assessment tools and when and how to enter data into a cloud-based database. They also provide monthly data on emergency department use, hospital admissions, hospital readmissions, and the level of effort (e.g., hours RN-Ns spent) to support their CBHH participant caseload. Regular project team meetings and trainings related to the acquisition of key knowledge and skills required for the project are a key component of the CBHH.
Methods
The evaluation of CBHH warranted an exploratory sequential mixed-methods approach. We received approval for this evaluative study from the institutional review board at the first author’s institution. The original quantitative data, consisting of utilization data and participant assessments, were collected by CBHH RN-Ns every 6 months from September 2013 to March 2017 with oversight by ALE. Assessment and utilization data were deidentified by ALE staff members in March 2017 and analyzed by the first author using SPSS version 24.0.
General Community-Based Health Home Eligibility Criteria.
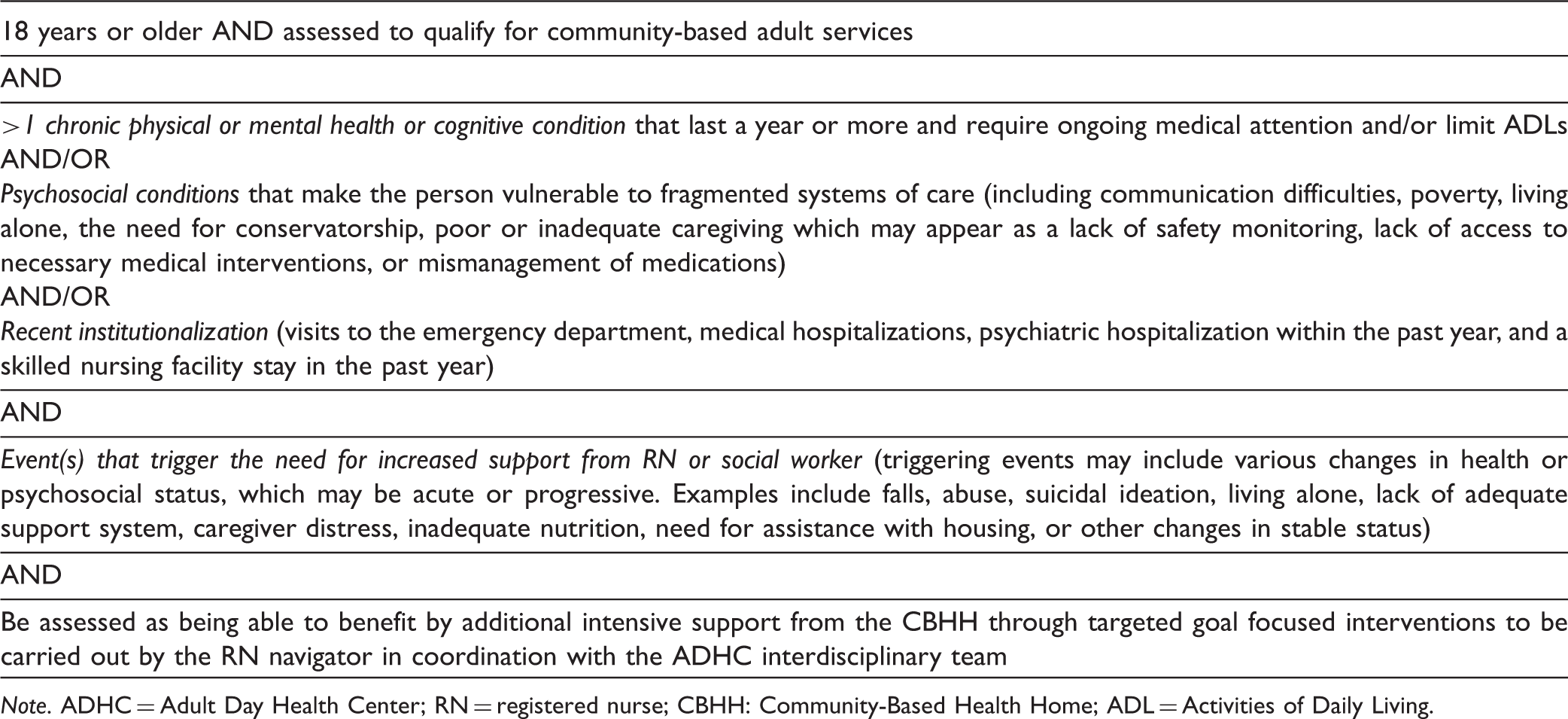
Note. ADHC = Adult Day Health Center; RN = registered nurse; CBHH: Community-Based Health Home; ADL = Activities of Daily Living.
Quantitative Data
Community-Based Health Home Participant Demographics, 2013–2017 (n = 126).
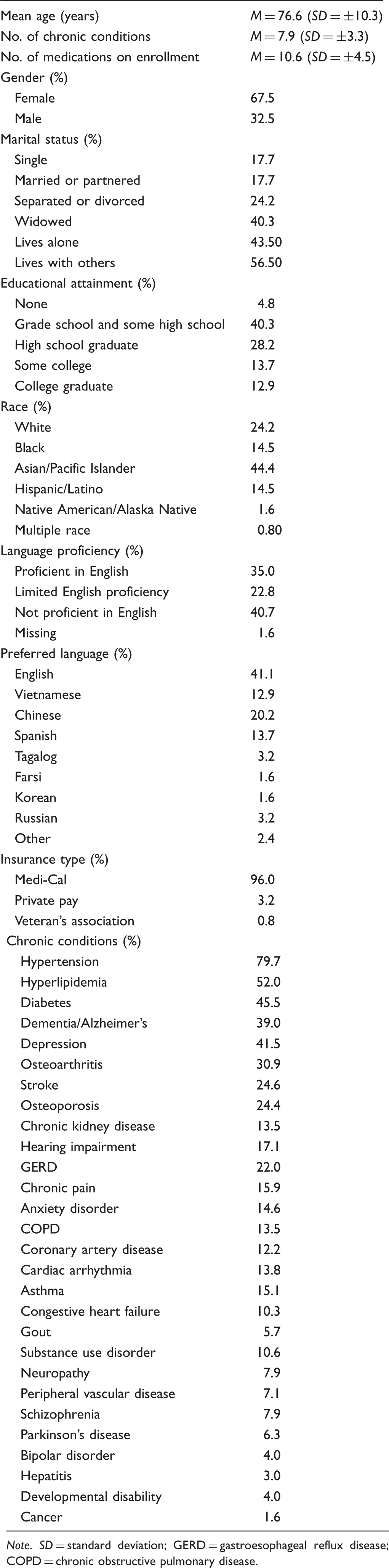
Note. SD = standard deviation; GERD = gastroesophageal reflux disease; COPD = chronic obstructive pulmonary disease.
Screening Tools Used for Participant Risk Assessments.
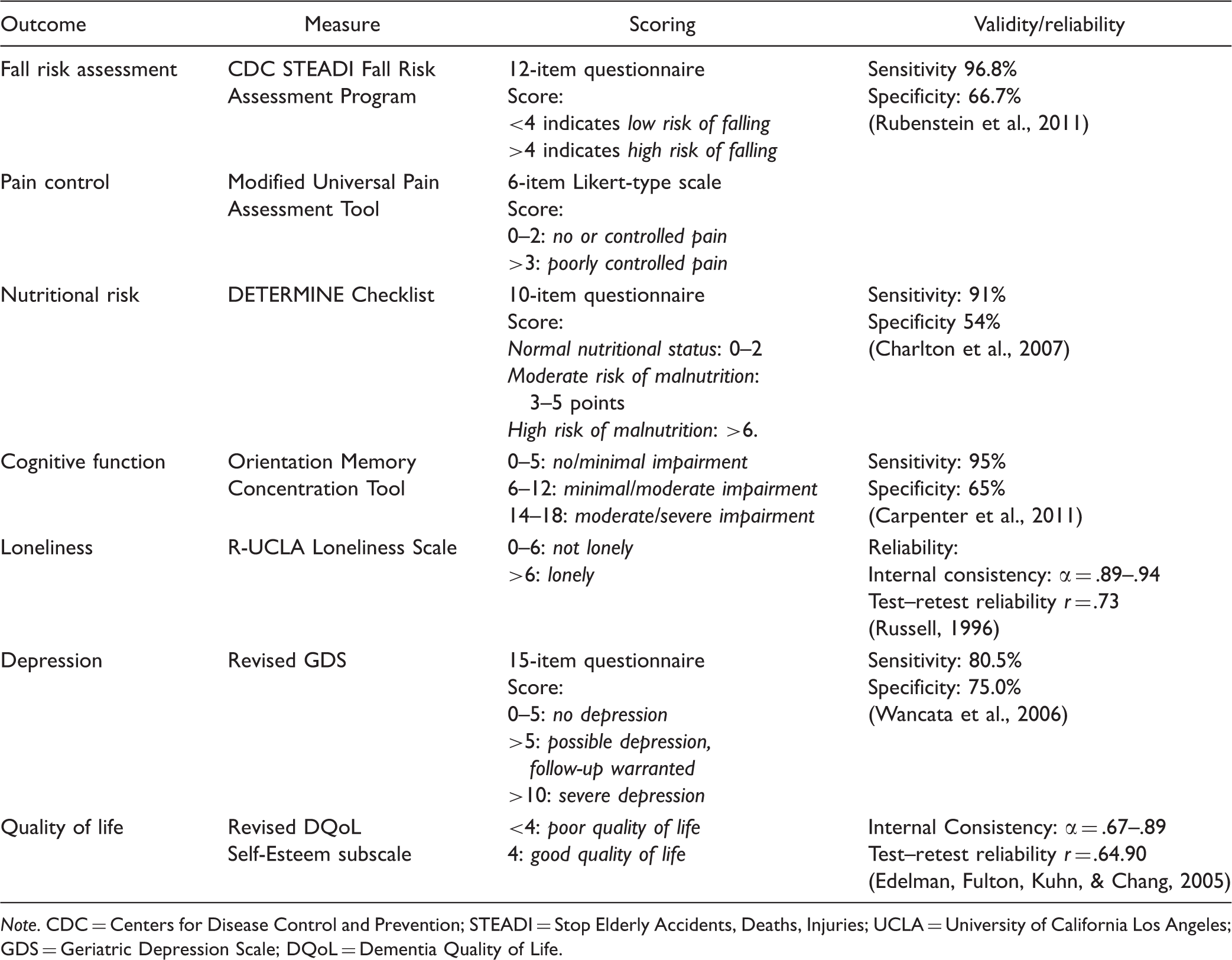
Note. CDC = Centers for Disease Control and Prevention; STEADI = Stop Elderly Accidents, Deaths, Injuries; UCLA = University of California Los Angeles; GDS = Geriatric Depression Scale; DQoL = Dementia Quality of Life.
Data pertaining to demographics and health care utilization were entered into Excel, while the results of clinical assessments were entered into TOPS® (Tracking Outcomes for Program Success), a cloud-based database that complies with Health Insurance Portability and Accountability Act regulations related to protecting patient privacy (U.S. HHS, 2013). All data were ultimately merged into SPSS version 24.0 for cleaning and analysis. Primary analyses consisted of univariate descriptive statistics and bivariate χ2 analysis to assess statistically significant relationships between groups at enrollment and 12 months. Statistical significance was set at p < .05.
Qualitative Data
One-on-one semistructured interviews were conducted by the first author in a private interview room in May 2018 at each of six sites, all of which were in northern California. Returning to all 12 sites in 2018 was not feasible because some had closed. Hence, these six sites were selected because they remained open, had diverse clientele, and spanned both rural and urban locales. ADHC staff posted flyers created by the first author at each ADHC and assisted with disseminating information about the study to participants during their daily interactions at the ADHC. Six types of CBHH stakeholders were interviewed: participants, family caregivers, RN-Ns, ADHC RNs who were not nurse navigators, ADHC administrators, and ADHC social workers. Such diverse perspectives were used to provide a holistic view of the program’s impact.
Interview questions were informed by results of the quantitative data analysis and were specific to each category of stakeholder. For example, participants were asked, “Can you tell me how your health has changed since you have enrolled in CBHH?” RN-Ns were asked, “How does the design of the program affect your ability to deliver care to participants?” Questions were designed to focus the interview while still allowing participants to speak freely about their experiences. Interviews lasted between 30 and 45 minutes. Interviews garnered data on participants’ involvement in the CBHH program and their overall experiences at their ADHCs.
Fifteen interviewees were not native English speakers and had limited English proficiency. Their preferred languages were Cantonese (5), Mandarin (4,) Russian (3), and Farsi (3). Non-CBHH bilingual staff provided interpretation when needed. They received the interview guide and were familiarized with the questions and processes around interview in advance. Participant identifiers were removed from the recording and sent to a professional transcription company. The interviews were transcribed in the participants’ native languages, and original recordings were translated into English by the transcription company to verify the initial interpretation was accurate and comprehensive. The interviews, as transcribed and interpreted by the company, were used for analysis.
Data Analysis
Analysis of deidentified interview transcripts was conducted by the first author and two research team members, a registered nurse and a medical student, both with backgrounds in geriatrics. Initially, the coders analyzed the same three transcripts using a codebook developed by the first author as a basis for comparison. To maintain methodological rigor, the team met for regular debriefings to discuss any deviations from the coding scheme. The qualitative coders were initially blinded to the quantitative data. The coders met weekly with the first author to go over coding and resolve discrepancies. Coding disagreements were discussed in-depth until consensus could be reached. The coding categories were summarized across cases (i.e., study participants), and within-case analysis was used to identify the key elements of each participant’s responses.
After both the quantitative and qualitative data were analyzed, the authors used data integration techniques to identify the components of CBHH that were most likely driving outcomes evidenced in the quantitative data. Within our explanatory sequential evaluation design, data integration involved connecting the results from the initial quantitative phase to help plan the qualitative data collection phase (O’Cathain, Murphy, & Nicholl, 2010). To help explain the quantitative results, we compared changes in biopsychosocial outcomes (reflected within the screening and assessment tools used) to stakeholders’ perceptions of the CBHH program and their identifications of its most effective components. Integrating these data sets helped illustrate what components of CBHH were most essential. Data integration was also important for understanding the social circumstances of participants and the role of the RN-N in meeting their health care needs.
Results
The mean age of participants was 76.6 years (±10.3). Each had, on average, 7.9 (±3.3) chronic conditions and required 10.6 (±4.5) medications. The sample was predominately female (67.5%), and only a small proportion were married or partnered (17.7%). The majority (56.5%) lived with others and 45.1% had less than a high school education. The sample was disproportionately Asian (44.4%). When questioned by the RN-N on proficiency in English, 60% reported that they could speak only a few words or were unable to speak English at all. The sample was almost entirely (96.1%) insured by Medi-Cal (California’s state-based Medicaid coverage for low-income individuals). The top five most frequent chronic conditions affecting this population were hypertension (79.7%), hyperlipidemia (52.0%), diabetes (45.5%), dementia/Alzheimer’s (39.0%), and depression (41.5%).
Changes in Socioemotional Health During CBHH
Result of Participant Screenings at Enrollment and 12 Months.
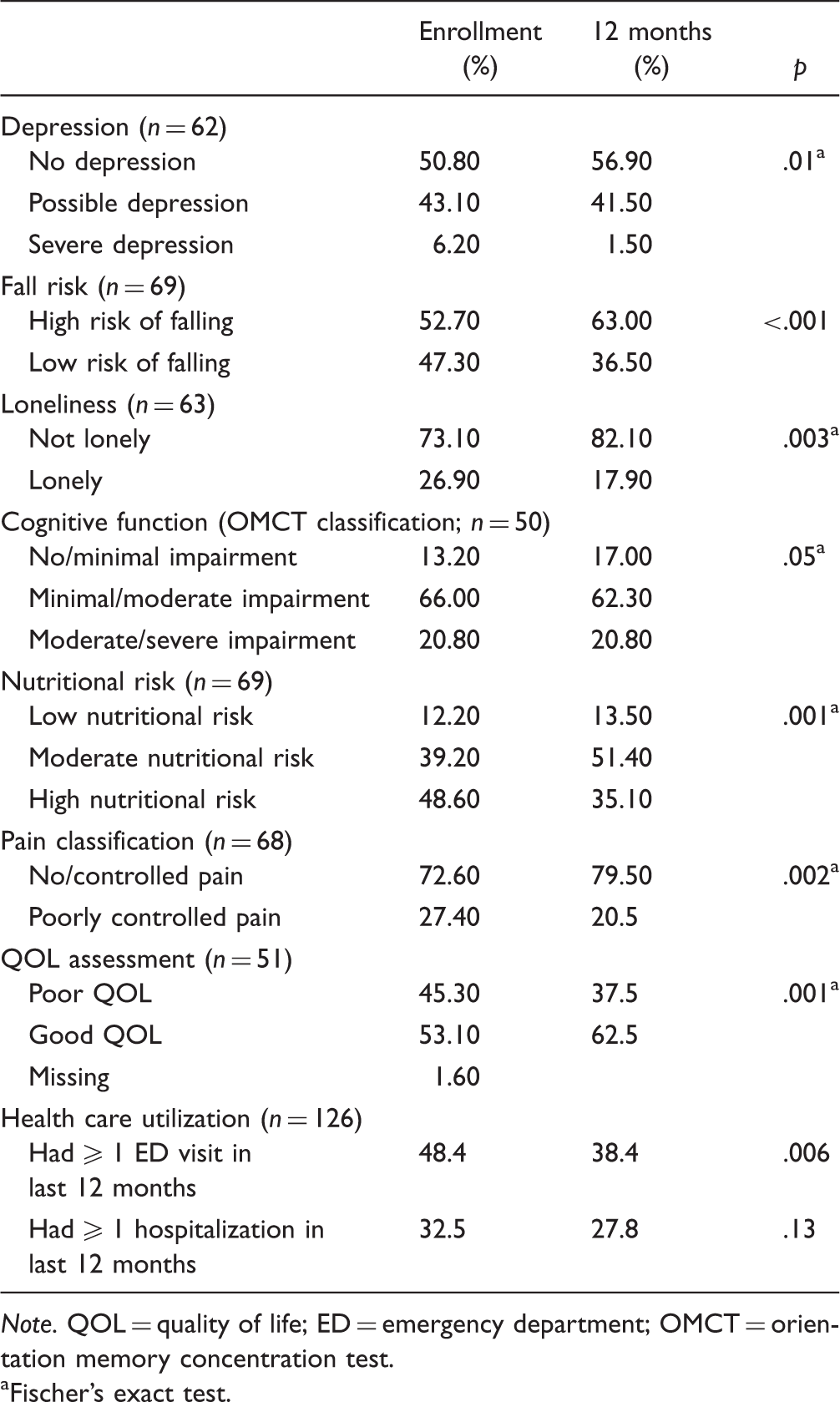
Note. QOL = quality of life; ED = emergency department; OMCT = orientation memory concentration test.
Fischer’s exact test.
Participant and Stakeholder Experiences in CBHH
Identification of Factors Associated With Health Improvements Among CBHH Participants Based on Interviews.
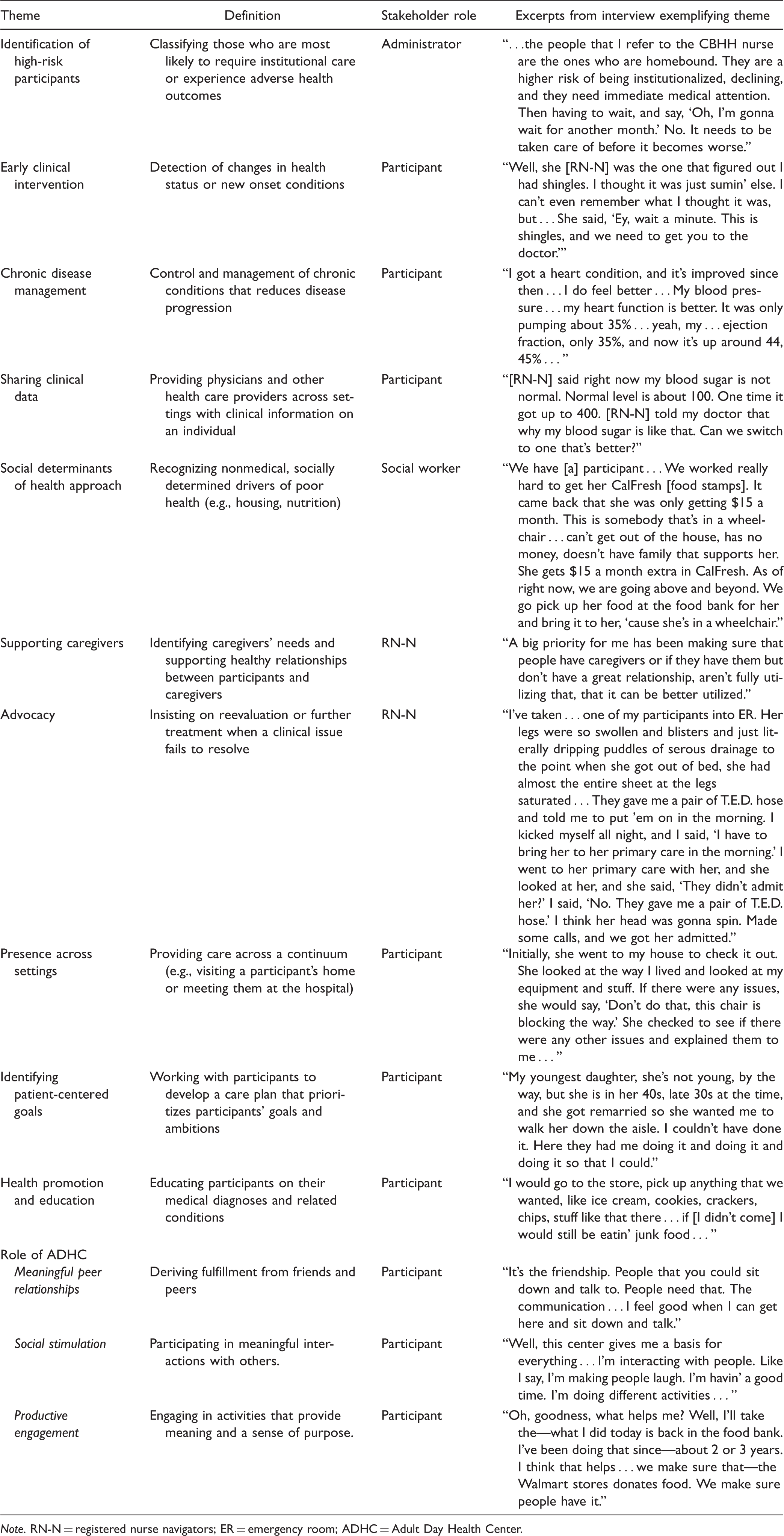
Note. RN-N = registered nurse navigators; ER = emergency room; ADHC = Adult Day Health Center.
Discussion
CBHH participants saw improvements that were both clinically and statistically significant in several aspects of their well-being. Participant demographic data paint a picture of chronically ILL older adults who, in addition to being medically complex (participants were on an average of more than 10 medications and had an average of seven chronic conditions), faced barriers to health care access. These included language barriers (35% were proficient in English), low socioeconomic status (96% were Medi-Cal recipients), and low levels of educational attainment (46.1% lacked a high school diploma). Notably, although participants who were selected to participate in CBHH were identified by the IDT as being at high risk for adverse health outcomes, their clinical profiles did not differ from the average ADHC participant.
Although our sample, which was 24% White, was more racially diverse than ADHC users nationally, where 40% are White (Harris-Koteijen et al., 2016), the most common chronic conditions in our sample (hypertension, diabetes, hyperlipidemia, dementia, and depression) are consistent with those seen among ADHC users nationally (NADSA, 2017). The racial diversity of our sample, particularly the proportion of Asians, could reflect the diversity of California where the study took place. Nearly one-third (31%) of the Asian Americans in the United States live in California (Lopez, Ruiz, & Patten, 2017).
Similarities between the demographic and clinical profiles of CBHH users and the broader ADHC population suggest that there may be more individuals with complex biopsychosocial needs in the ADHC who would be well served by the coordination provided by CBHH. Moreover, because ADHC users are functionally impaired and chronically ill, ADHCs could benefit from routinely screening all of their participants for issues such as malnutrition (Sheean et al., 2018) and loneliness (Krieg, Hudon, Chouinard, & Dufour, 2016), which are associated with adverse health outcomes.
Factors Underpinning Improved Health and Reductions in Health Care Utilization
Participants who benefited from additional care coordination and attention from the RN-N, as part of the CBHH model, also saw statistically significant reductions in emergency department utilization (p = .006). These changes may be attributable to improved interdisciplinary care coordination by the RN-N that integrated the care being provided in the ADHC with acute and primary care providers. RN-Ns shared clinical data with providers, participated in clinical encounters across health care settings, recognized and intervened with respect to emerging clinical issues, and advocated on patients’ behalf.
These actions integrated care, such that care from disparate providers was no longer delivered within silos. The actions also effectively allowed the ADHC to become part of the continuum of care (Capp et al., 2017). Moreover, RN-Ns facilitated commonly overlooked care transitions, such as from the provider’s office to the pharmacy, ensuring prescribed medications were ordered. Or, as another example, RN-Ns ensured that meals being provided by government programs were actually making their way into the homes of participants. The CBHH, therefore, expands the traditional focus of transitional care models and their emphasis on the passage of patients from hospital to home (Naylor & Keating, 2008), to include transitions within the community. Improved medication management, greater advocacy on behalf of the participant, visits to participants’ homes, and ensuring their basic needs (e.g., food, safety) are met likely contributed to improvements in pain control and nutritional risk seen over 12 months.
Comments from the interviewed stakeholders and participants emphasize that the strength of CBHH lies in the nurses’ clinical skills and their ability to intervene with respect to social determinants of health. The National Academy of Medicine has recommended measurement domains of social determinants that can potentially lead to improved patient care. These include social factors (social isolation, stress, depression), and sociodemographics (education, race, ethnicity, and income; Matthews, Adler, Forrest, & Stead, 2016). CBHH nurses are identifying and addressing many of these components. For example, there were significant reductions in the proportion of the sample who screened positively for severe depression, improvements in self-reported quality of life, and reductions in loneliness.
Additional Outcomes and Considerations
Not all health outcomes improved over the course of the study. For instance, the proportion of those at high risk for falls increased after 12 months. This may because CBHH nurses were more accurately able to identify those at risk as the program went on. Another reason may be the natural progression of disease and difficulty in altering that progressive decline within 12 months.
In addition, there are practical limitations to implementing CBHH. This includes the high cost of using a registered nurse compared with costs incurred by insurers when paying other health care personnel such as community health workers. In 2018, the median annual salary of a registered nurse in the United States was US$70,000 (Bureau of Labor Statistics, 2018). The model designers intentionally chose a nurse to serve as a care navigator, in contrast to other models that utilize social workers and community health workers, because the target population experienced highly complex medical conditions and the expertise of a licensed registered nurse facilitated credible access to and clear communication with the medical community. Moreover, the potential cost savings of reduced health care utilization (e.g., reductions in emergency department use) and the costs of the ADHC relative to a nursing home should be attractive to insurers who would finance this model of care, particularly government insurers like Medicaid. The daily Medicaid reimbursement rate for adult day services (US$76.27 in California in 2019; State of California, n.d.) is far less than what is spent on the 1.4 million adults in nursing homes, where the average cost of care is between US$225 and US$253 per day (U.S. HHS, 2017).
Even without the formal CBHH structure, our findings illustrate that health care providers in the community can benefit from greater collaboration and exchange of clinical information with the ADHC to identify emerging clinical issues. Primary care providers and RNs at ADHCs can work together to develop dynamic patient-centered care plans that reflect participants’ changing needs.
Discussion
Limitations
This study had several limitations. First, we were unable to parse out the effects of CBHH from the impact of the ADHC itself, though the mixed-methods approach offered some insight into this. Participants’ responses suggested that although the ADHC is a medically effective provider of health services, it is also a source of meaningful relationships and positive interactions. Second, the study lacked a control group making it challenging to determine whether improvements in health were the result of CBHH or the ADHC itself. Third, we were also limited by the small subsample for whom there was 1 year of data available. We may have inadvertently introduced selection bias by limiting our analysis to those who spent a full year within the program because these individuals may have been healthier overall. However, as we previously noted, differences in demographic characteristics between those in the program for greater than or equal to 12 months and those in enrolled for less than 12 months were not significant. Fourth, the data are not nationally representative and reflect the unique state context of California. Fifth, due to the nature of the secondary quantitative analysis, we were limited by the data available to us.
To more thoroughly assess the program’s impact, we recommend working with program designers to (a) evaluate changes in overall continuous scores using paired or group-wise t tests, (b) examine changes in the component parts of each score in future analyses, and (c) perform a robust missing data analysis.
Implications for Policy
As of 2017, the U.S. HHS (2017) spends over US$1 trillion a year on health care for elderly and vulnerable adults. One of the Department’s goals is to enhance integration of health and social programs, such as housing and nutrition (Azar, 2018). For example, Medicaid operates independent of the Supplemental Nutrition Assistance Program. Yet, both of these programs impact health and serve low-income individuals. Models such as CBHH in which RN-Ns ensure Medicaid recipients at the ADHC have sufficient access to food at home are successful in bridging the gap between health and social services. RN-Ns identify each adult’s biopsychosocial needs, organize IDTs around these needs, connect adults to appropriate services, and advocate on their behalf.
CBHH demonstrates that the ADHC, specifically, has the infrastructure and capacity around which to build the health home, particularly an existing IDT and the ability to surveil participants in a controlled setting. The proportion of ADHCs in our study that were forced to close or leave CBHH for financial reasons (22.7%), however, illustrates the challenges of implementing CBHH in these centers. Despite facilitating health management and promotion for medically complex adults, these centers may not be adequately reimbursed for the services they are providing, which include preventive health services, cognitive and behavioral health services, and nutrition. Adult day services providers spend a significant time with their clients and possess a wealth of clinical data that can be useful to clinicians. But ADHCs are primarily viewed and reimbursed as social service providers.
The results of our evaluation suggest that, with the addition of an RN-N, the ADHC may be able to improve health outcomes for vulnerable seniors by leveraging its ability to suveil participants and intervene on their behalf to prevent adverse outcomes before they arise. We recommend that Medicaid reimburse CBHH in order to allow for widespread implementation.
We also recommend Medicare Advantage consider reimbursing CBHH as part of its expanded benefits programs. Beginning in 2019, CMS expanded the definition of health services that may be offered as supplemental benefits in Medicare Advantage plans. Services that are “primarily health related, including those that reduce avoidable emergency and health care utilization, like CBHH and care provided in ADHCs (Coleman, 2018). Adult day care services, which were previously only reimbursable by Medicaid, Veteran’s Administration, or private long-term care insurance, are included in this supplemental benefit. Thus, the onus is on ADHCs, alongside clinicians, researchers, and IDT members, to demonstrate their effectiveness in improving health outcomes to justify and support Medicare health plan reimbursements at a level commensurate with the effort and the outcomes. Both federal (e.g., National Institute of Nursing Research) and local (Area Agencies on Aging) funders must sponsor additional research that supports evaluation and implementation of nurse-led programs like CBHH.
Conclusion
CBHH uses a person-centered, biopsychosocial health-focused approach that incorporates and addresses social determinants of health. CBHH is a promising solution to improving care for vulnerable older adults with multimorbidity, particularly with respect to reducing emergency department utilization and improving socioemotional health (e.g., quality of life, loneliness, depression). Embedding the RN-N into the ADHC facilitates integration of services and allows the ADHC, which is commonly overlooked as an effective and desirable care site, to be part of the care continuum. In the absence of an RN-N, similar success may be achievable through enhanced communication between health care providers and greater recognition of the value of clinical information ADHCs can provide.
Footnotes
Acknowledgment
The authors would like to acknowledge Dr. Christine Kovner for her support of this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute on Aging/National Institute on Minority Health and Health Disparities.