
Abstract
We propose an analysis of sports injury policies founded on the assertion that injuries are due to both uncontrollable risks (accidents from participating in sports) and controllable risks (athlete's deliberate choices in risk-taking). We compare the adoption decision of an injury policy made by: (a) a sport's organizer who maximizes welfare, (b) a sport's organizer who fails to account for athletes’ behavioral risk responses, and (c) the athletes themselves. We argue that policies that escalate risk, such as mandatory protective equipment, are over-adopted by the naïve sport organizer and the athletes, while policies that de-escalate risk, such as return-to-play rules, are under-adopted.
Keywords
Introduction
Injuries impose massive costs in amateur and professional sports. Fair and Champa (2019) estimate that up to $18.4 billion could be saved per year if contact was eliminated from college sports. According to Eliakim et al. (2020), the English Premier League of professional association football loses a combined £900 million GBP per season from “injury-related decrement in performance.” Verhagen (2010) estimates that the annual costs of sports injuries in the Netherlands alone was over €3 billion. These figures do not capture many of all long-term health consequences of injuries (e.g., decreased cognitive acuity and depression associated with concussions, Montenigro et al., 2017). It is no surprise that sport injuries are a major concern.
The medical and sports management literatures largely view injuries as misfortunate events that are an unwanted yet inevitable byproduct of participating in sports. A wide variety of interventions attempt to minimize injury costs, including prevention, treatment, protective equipment, or changes in a sport's rules (Finch, 2006). A good intervention is said to be one that reduces the chance of an injury occurring or that attenuates its severity (Chalmers et al., 2004). However, the underlying assumption of this approach is that athletes are but passive victims of injuries.
This article offers a complementary perspective to analyze injury policies that incorporates athlete risk-taking decisions in competitive sports. We start from the recognition that some injuries occur because athletes take risk in pursuit of exceptional performance. We consider a standard Tullock contest between two athletes who choose a risk level to undertake. Athletes balance the benefits from increased performance with the cost from increased chance of injury, including failing health, time lost from play, decrease in future performance, lower salaries, and so on and so forth. We then model the adoption of an injury policy as a change in the injury cost born by athletes. This approach covers a wide range of responses to injuries studied in the literature, and some discussed in this work, such as protection equipment, return-to-play rules, safe-play rules, and medical treatment. Combining the medical and economic perspectives, we assume that an injury policy changes the cost of injury through two channels: first, it lowers the “baseline injury cost,” a cost that does not depend on athletes’ behaviors. Second, an injury policy can change athletes’ incentives to take risk.
The incentive channel determines whether the injury policy de-escalates—or possibly escalates—the athlete's choice of risk. To illustrate this distinction, it helps to contrast two injury policies used in practice. First, consider a return-to-play rule that attempts to attenuate the consequences of a concussion (Putukian et al., 2019). Such a rule requires players to wait for the outcome of medical examinations before they can again participate in their sport after a suspected concussion. Stricter rules, such as those that impose longer delays, increase the cost borne by the athlete and should thereby reduce risk-taking. In summation, return-to-play rules have two impacts on injury costs: a direct impact of reducing the possibility of re-aggravation and an indirect impact due to decreased risk-taking. Conversely, protective equipment that helps mitigate the gravity of an injury sometimes encourage athletes to take more risks: while the baseline cost of the injury decreases, so too does the cost of taking risk. These two examples illustrate diverging outcomes: return-to-play rules increase, while protective equipment decrease, the athlete's cost of taking risk.
We apply this insight to analyze two decisions that sports’ organizer(s) often struggle with. First, we assume that a sport's organizer must choose between mandating and prohibiting the use of a new injury policy. To do so, we compare the per-athlete welfare under adoption (i.e., when athletes play the Nash equilibrium using the new cost function imposed after adoption), and nonadoption (i.e., when athletes play the Nash equilibrium using the prevailing cost function). We show that a naïve decision-maker—one who does not consider athletes’ risk responses—will tend to over-adopt risk-increasing policies and under-adopt risk-decreasing ones. Over-adoption is consistent with the weak, or even negative, impact of some injury policies studied in the literature (Parkkari et al., 2001). Counter-intuitively, an injury policy that increase welfare in the absence of athlete response can increase total injury costs once the athletes’ risk response is considered. This mechanism explains the increase in fatal crashes after the introduction of safer racing cars (Potter, 2011).
In our second scenario, a sport's organizer chooses to permit adoption. This extension is relevant, for example, for some types of protective equipment for which there is not enough support to mandate adoption. The sport's organizer can, however, permit and recommend adoption. To inform this decision, the sport's organizer compares athletes’ welfare when adoption is permitted and when it is not. When adoption is permitted, athletes play a two-stage game: In stage 1, each athlete decides whether to adopt or not. In stage 2, the two athletes choose a risk level conditional on the adoption decisions made in stage 1. We show that athletes tend to over-adopt policies that reduce the cost of risk-taking and under-adopt those that increase the cost of risk-taking.
An implication is that athletes will resist adoption of welfare increasing interventions when these interventions increase the cost of risk-taking. This is consistent with the observation that athletes under-report their own injuries to avoid the consequences of return-to-play rules (Torres et al., 2013). The analysis also suggests that return-to-play rules are less effective when game stakes are elevated or at the end of the season when the consequence on lost play is reduced.
Our work offers an alternative approach to the risk compensation theory (also referred to as risk homeostasis theory; Wilde, 1982) which stipulates that individual agents adjust risk in light of policy interventions to remain at their preferred level of risk (Hagel & Meeuwisse, 2004). According to this view, little can be done to influence risk-taking. In contrast, our analysis says that athletes re-optimise their behavior in response to the change in incentives they face. The analysis is also related to two other literatures: consumer protection and doping. The notion of risk escalation is reminiscent of Peltzman's “offsetting effect” (1975) and his controversial conclusion that a safety regulation may have the opposite impact than intended. Earlier work on doping in sports has pointed out the possibility of unintended response to policy interventions (e.g., Mohan & Hazari, 2016). Finally, economists have dedicated some attention to risk-taking in sports (e.g., DeAngelis & Viscusi, 2020; Lybbert et al., 2012; Potter, 2011) and to the overall cost of injuries in youth sports (Fair & Champa, 2019), however, we are not aware of any analysis of the design of sports injury policies and their effectiveness at reducing injury costs as done here.
The remainder of this study is organized as follows: the next section reviews the literature and motivates our approach; the third section presents the model, derives the main results, and discusses applications to various sport injury interventions; and the final section offers concluding remarks and a discussion of remaining issues for future research.
Literature Background: Sports Injuries and Injury Interventions
Most sports professionals agree that participation in sport should be made as safe as possible (Parkkari et al., 2001). 1 They typically view injuries as unfortunate yet largely unavoidable accidents that result from a complex interaction of risk factors, preconditions, and external circumstances. Scholars have studied the prevalence and cause of injuries from participating in sports, estimated the health consequences, and, ultimately, proposed changes in hopes of making professional, amateur, and youth sports safer.
The literature has looked at many sports (including contact and noncontact varieties) and studied different types of injuries (e.g., concussions or soft-tissue knee injuries among others) and their immediate and differed impacts (Montenigro et al., 2017) on the performance, health, and earnings of athletes (Secrist et al., 2016). Findings can vary by sport. For example, evidence from the National Football League (NFL) shows that a concussion decreases future performance (Heintz et al., 2020b), play time (Heintz et al., 2020a; Wennberg & Tator, 2008), and player salary (Navarro et al., 2017). Conversely, no evidence of decreased performance postconcussion has been found in basketball (Yengo-Kahn et al., 2016) while results are mixed in baseball (Turbyfill et al., 2021).
Policy research tends to focus on injury information, awareness, prevention, training, detection, safe-play, and treatment (Soomro et al., 2016; Van Mechelen et al., 1992). Prevention includes recording and monitoring (Deubert et al., 2017), guidelines for warm-up, training, practice, and competition, screening, and compliance enforcement (Van Tiggelen et al., 2008). The medical field has also debated when professional athletes should return-to-play after an injury (Reams et al., 2017) and the process followed to make this decision (Brayton et al., 2019; Deubert et al., 2017).
Professional sports bodies have independently implemented sports injury prevention programs (Kim et al., 2017; Quarrie et al., 2020), although there is much debate that such programs are sufficient (Parkkari et al., 2001). 2 This has occasionally led to legislative injunctions: following a rise in awareness of the dangers of concussions in youth sports in the mid-2000s (Rotolo & Lengefeld, 2020), all 50 U.S. states passed regulations stipulating rules detailing when youth athletes can return-to-play after an injury diagnosis (Kim et al., 2017).
Motivation: Risk-Taking, Injuries, and Incentives
We first recognize that athletes face different types of risks, some within and some beyond their control. Injuries can happen for many reasons such as chance (i.e., bad luck), external circumstances (e.g., weather or playing surface; Cisyk & Courty, 2023), rules of engagement (Fair & Champa, 2019), or because an athlete takes excessive risk. This latter case, which we label controllable risk, can manifest itself as, among other mechanisms, an athlete expending maximal exertion, switching to strategies that put strain on the body or that involve more body-contact, or investing less in injury prevention and recovery. There is much evidence for the association between controllable risk, exceptional performance, and injuries (e.g., Bolling et al., 2020; Chen et al., 2019; Turner et al., 2004; Verhagen et al., 2010).
Contest theory offers a theoretical framework to understand risk-taking in competitive sports. In this paradigm, athletes participate in a contest to win some payoff. Contestants make investments to increase their chance of success, which may include training, concentration, or exertion (Frick, 2003). These investments are all captured in the literature under the label of “effort” (Kahn, 2000). We add to this the stipulation that effort also includes the athlete's willingness to take risks. The next section adopts the standard Tullock contest model to analyze the impact of an injury intervention on athletes’ risk-taking (see also Szymanski, 2003 and Dietl et al., 2009 for sports applications of Tullock models, and Ryvkin (2013) and Mohan and Hazari (2016) for a recent application of a Tullock model with doping).
Model and Analysis
We analyze three variants of an adoption game with three players, which we respectively label the sport's organizer and its athletes. Although the model has two individual athletes, few refinements are required to generalize the analysis to team sports. 3 We assume the athletes to be risk neutral: this greatly simplifies the analysis as the sport's organizer needs only to consider expected injury costs, yet we note that the main insights generalize to risk aversion.
Risk-taking increases the chance of winning a fixed payoff that includes all returns from winning, such as cash prizes, increases in future career opportunities, and the intrinsic “thrill of victory.” For simplification, we assume that both athletes earn the same payoff from winning, k, and nothing otherwise, and both athletes have the same utility function. Athlete
Figure 1 summarizes the timeline and player decisions in the first variant. In the adoption stage, the sport's organizer can mandate adoption of injury policy


Adoption game (first variant analyzed in the Sophisticated and Naïve Adoption section).
The sport's organizer maximizes the per-athlete welfare defined as average utility net of implementation cost. The Sophisticated and Naïve Adoption section distinguishes two types of sport organizers. The sophisticated type anticipates that athletes change their risk choices in the contest stage in response to the adoption decision A. The (
The Athlete Adoption section analyzes the other two variants of the game. It starts by analyzing a variant where the sport's organizer permits adoption but leaves the decision to athletes. An example is a protective equipment that is recommended but not required. The sport's organizer becomes a passive agent and we obtain a two-stage game between athletes. In the first stage, the adoption stage, each athlete decides whether to pay fixed cost F to adopt. The Tullock contest stage is the same as before but now incorporates the adoption decisions made by each athlete in the first stage. 4 The last variant integrates the first two variants: the sport's organizer can mandate, prohibit, or permit adoption and the athletes respond accordingly. We discuss more general policy options in the discussion section.
Before tackling the adoption game, we derive in the next section the athletes’ risk choice in the Tullock contest stage and analyze how this choice responds to a marginal change in
Tullock Contest Stage: Analysis of Risk Responses
We solve for the athletes’ choice of risk for injury policy
The remainder of this section computes comparative statics with respect to
In the pure strategy Nash equilibrium, athletes do not respond to a change in
Proposition 1 says that an increase in cost reduction triggers a positive risk response when risk-taking and cost reduction are substitute inputs in the cost function, and a negative one when the two inputs are complementary. There is no risk response when the two inputs are independent. Behavioral responses to injury intervention have been largely overlooked in the analysis and design of injury intervention, despite the existence of a large body of anecdotal evidence documenting unintended responses to injury policies. We present a few examples of risk-taking response to injury interventions:
Sobel and Nesbit (2007) and Potter (2011) show that Formula One drivers increase risk-taking (measured by the number of accidents) as cars become safer (measured by the probability of being injured in a collision). Torg et al. (1979) argues that the introduction of helmets and facemasks in American football triggered a change in injury patterns: the number of serious head injuries decreased (due to the enhanced protective capabilities of the new helmet) yet the number of serious spinal injuries increased (due to increased use of the head as the primary point of contact in blocking, tackling, and head-butting, i.e., “spearing”).
5
In response, the NFL initiated the “crown of the helmet rule” in 2012 to penalize any player using the helmet in collisions. Hanson et al. (2017) shows that doing so reduced the number of concussions but increased lower injury extremity, thus demonstrating a substitution response in risk-taking. Ulnar collateral ligament (UCL) reconstruction surgery, colloquial known as “Tommy John surgery,” to repair elbow injuries of baseball players has been facetiously referred to as “a pitcher's best friend” as it has remedied what was previously a career-ending injury (Dodd, 2003). The procedure has been so successful that it has altered the perception of elbow injuries and the risk factors thereof: many parents, high-school and collegiate athletes, as well as coaches falsely believe that young players should no longer avoid an undue volume of pitches or throwing motions that put great amounts of strain on the elbow (Ahmad et al., 2012).
6
Proposition 1 offers an alternative view of behavioral response to the one offered under risk compensation theory wherein athletes have “a target level of risk they are willing to accept” (Hagel & Meeuwisse, 2004). According to this view, injury interventions that reduce the perceived level of risk lead athletes to adjust their behavior to take on additional risks (Thomson & Carlson, 2015). Using the language of our model, the risk compensation theory says that athletes respond to an intervention that decreases the cost of participating in sports (
Next, we analyze the impact of a marginal change in
In the pure strategy Nash equilibrium, an increase in
The inequality stated in Proposition 2 always holds when the two inputs are complements or independent in the cost function (
We illustrate Proposition 2 with the two injury policies discussed in the introduction: return-to-play rules and mandatory protective equipment. Return-to-play rules require that a player be removed from a game and put under observation in the event of a suspected concussion, only returning to play after medical clearance. Recovery periods can last several weeks or even longer: NFL players miss on average one game following a concussion event (Heintz et al., 2020a) while National Hockey League (NHL) players miss between 8 to 13 games (Wennberg & Tator, 2008).
7
Return-to-play rules are meant to reduce the chance of injury aggravation, corresponding to a reduction in the baseline cost of injury (
Conversely, recall that a mandatory protective equipment is designed to reduce the gravity of an injury and to protect athletes. This includes a wide variety of applications such as vehicle safety in auto racing and protective helmets. Such equipment is designed to provide baseline cost-savings (
Sophisticated and Naïve Adoption
This section analyzes the choice to mandate or prohibit injury policy


A naïve sport organizer may over- or under-adopt an injury policy.
To demonstrate that over-adoption can happen, we compute the sophisticated and naïve adoption decisions for the injury cost function:

Figure 2 plots the adoption decision by the naïve and sophisticated sport organizers for parameter values
Naïve and sophisticated adoption.
This conclusion, however, does not follow when there are cost savings from taking additional risk (
The two lines meet for parameter values such that both naïve and sophisticated sport organizers are indifferent with adoption and nonadoption. As discussed above, this occurs for
As Proposition 2 states, this absurdity can happen only when the athlete's risk choice and the cost reduction parameter are substitute. In fact, when the interaction of risk and cost savings (
The key message of this section is that an ill-designed injury intervention (i.e., one that ignores behavioral responses) may not deliver its intended effect of reducing injury costs. This possibility is supported by the research that argues that some interventions have little to no effect on health outcomes (Parkkari et al., 2001). Explanations for this null finding include implementation flaws or over-estimating the reduction in injury cost (e.g., the realized
An application is observed in the modification of game rules that attempt to reduce injury costs by changing athletes’ behavior. Arias et al. (2011) states that the main rationale for rule modification is to prevent injuries, yet surprisingly finds that this intended goal is achieved less than half the time. The main challenge with altering game rules is unintended responses. Such responses can explain why well-intended policies sometimes lower welfare and can even increase total injury costs. A case at hand is the crashes that happen at the end of cycling races. The governing body of professional cycling “has instituted various rules to moderate the chaos of sprint finishes during stage races” (Lybbert et al., 2012). These authors study a specific modification to an existing rule, akin to a change in
Athlete Adoption
This section assumes that the sport's organizer permits athletes to adopt injury policy
We have already solved for the Nash equilibria that take places in the subgames where both athletes adopt or both do not adopt (i.e., where
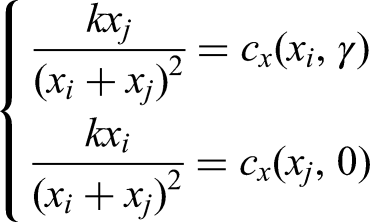
There are three types of equilibria: adoption by both athletes is an equilibrium when an adopter does not want to unilaterally deviate and become a nonadopter in the asymmetric equilibrium:


When C1 holds and C2 fails, both athletes adopt. When C2 holds and C1 fails, neither athlete adopt. When C1 and C2 fail, one athlete adopts and the other doesn’t (asymmetric adoption). When C1 and C2 hold, either both athletes do or both athletes do not adopt.
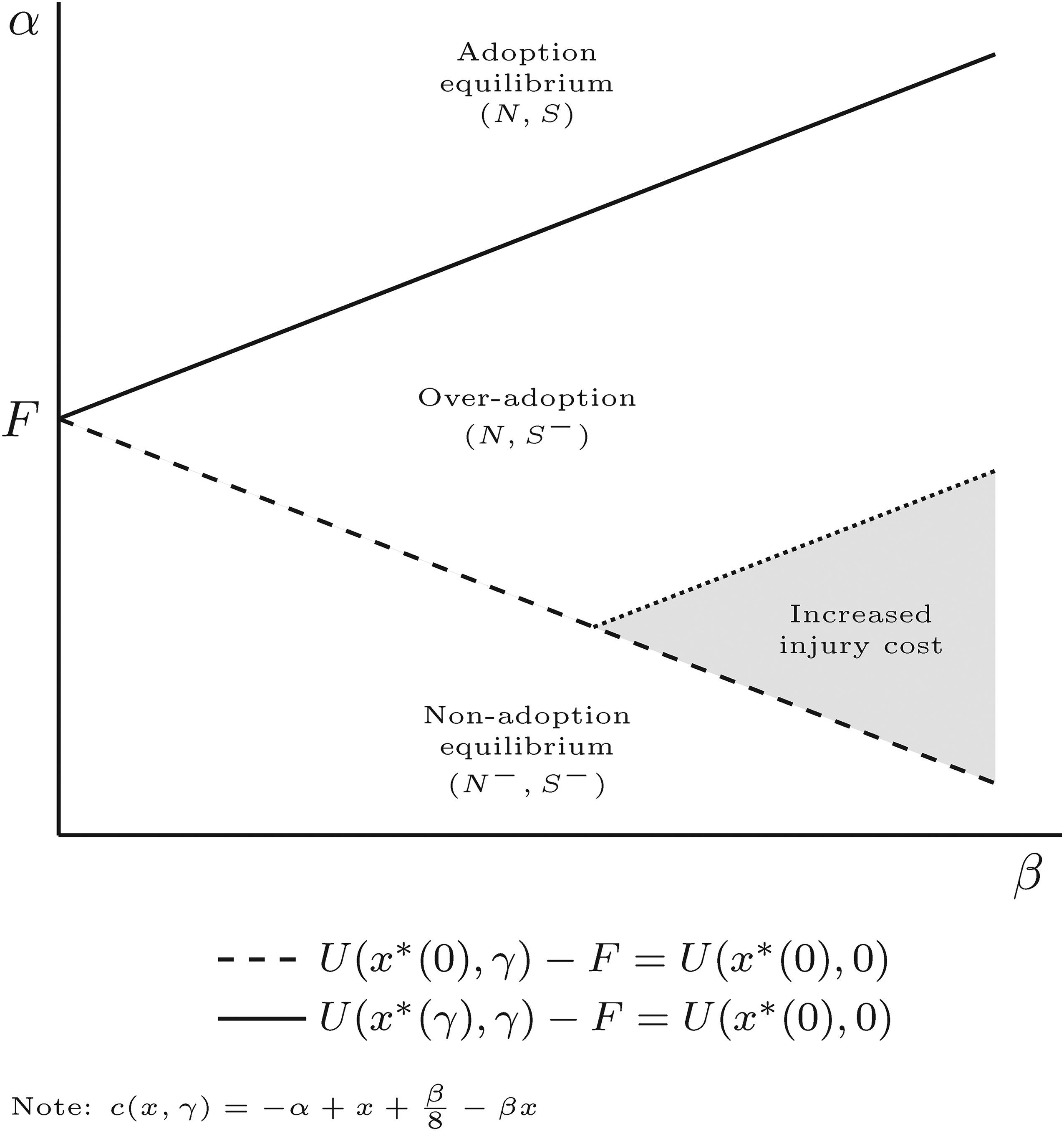
Figure 3 illustrates three (out of the four) types of equilibria in the parametric example. The figure plots the curves that results once inequalities C1 and C2 are set to equalities. The curve with long dashes plots the set of policies
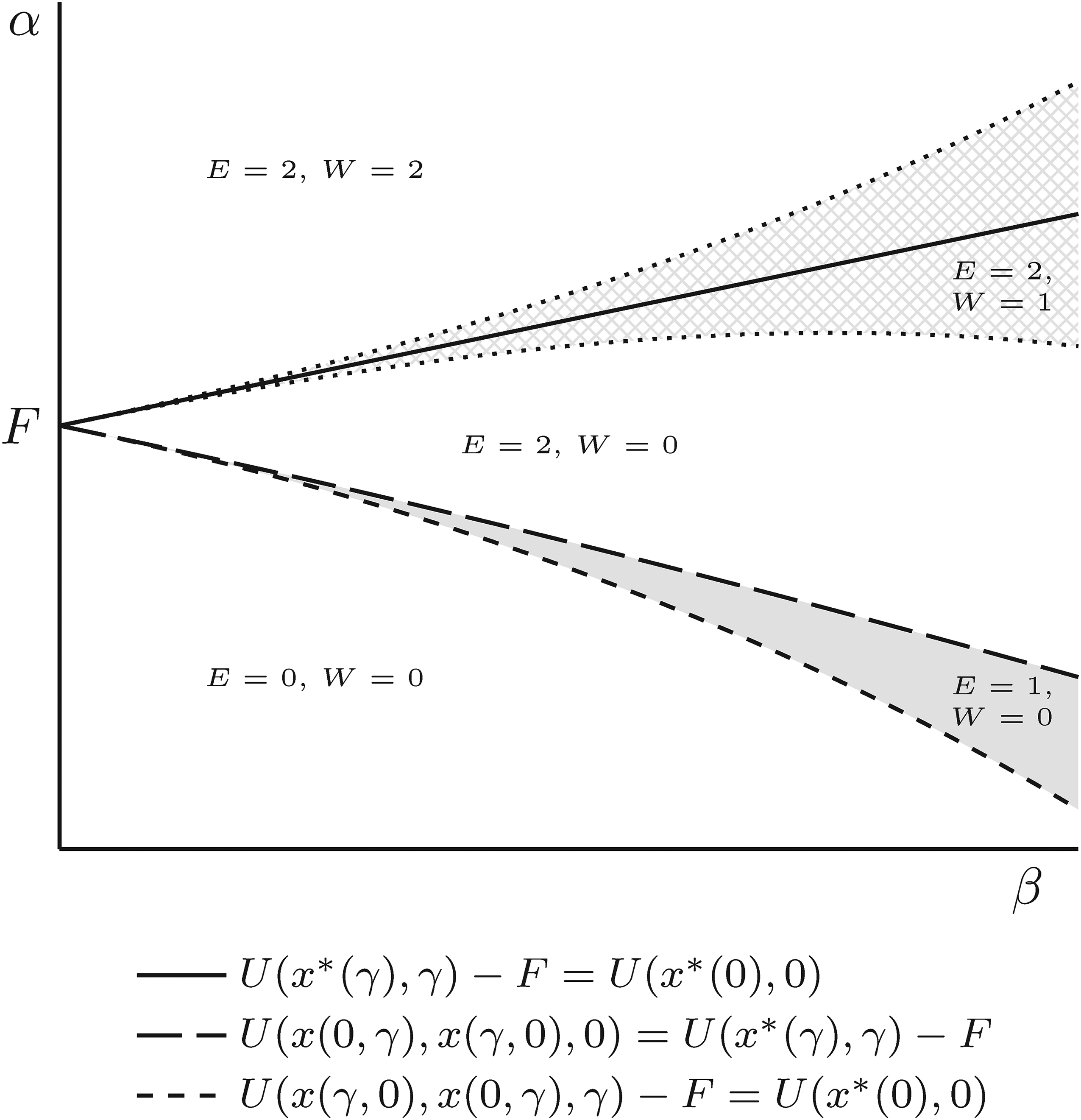
Athlete over-adoption.
To conclude the analysis, we integrate the two variants of the model, sport's organizer adoption and athlete adoption, into a single model where the sport's organizer can choose to mandate, prohibit, or permit adoption. The interesting question is when the sport's organizer can delegate the adoption decision to athletes. This will be the case when there is a unique equilibrium which implements the efficient adoption choice. The Appendix solves for all parameter values such that this happens. We report here two sufficient conditions such that sport's organizer does not want to leave the adoption decision to athletes.
Prohibiting adoption is strictly optimal when S and C2 do not hold and C1 does; Mandating adoption is strictly optimal when S and C2 hold and C1 does not.
Proposition 5 states sufficient conditions such that permitting adoption can be dominated by mandating or by prohibiting adoption. When the first set of conditions stated in Proposition 5 holds, adoption is the only equilibrium but nonadoption maximizes welfare. For the second set of conditions, nonadoption is the only equilibrium but adoption maximizes welfare. We illustrate the possibility that prohibiting adoption can be strictly optimal by returning to Figure 3. The three upper curves (one with solid and two with dotted lines) separate the parameter space considering athlete welfare. The welfare analysis differs from Figure 2 because the sport's organizer must consider the athletes’ welfare under asymmetric adoption, in addition to adoption and nonadoption.
10
Asymmetric adoption is optimal for parameter values between the two dotted curves (shaded with a cross-hatched pattern).
11
Adoption dominates both nonadoption and asymmetric adoption for values of
The figure distinguishes five areas, and labels each with its corresponding equilibrium and the welfare-maximizing adoption outcome. For example, the area in between the two dotted lines, labeled
It is useful to distinguish injury policies that are efficiently adopted (E = W), over-adopted (E > W), and under-adopted (W > E). We first note that athletes often voluntarily attempt to reduce their own expected injury costs by engaging in activities that are not mandated, or necessarily even recommended, by sport's organizers. For example, athletes dedicate much time to warm-up, training, and physiotherapy with little external incentive to do so. As another example, many athletes choose to follow unwritten rules regarding safe play even if they face no punishment for violations.
Over-adoption is relevant to many drug treatments and medical interventions. Athletes who take risks can use legal substances (such as Cortisone, Toradol, or even opioids among other drugs) to relieve the pain of an injury. Although these drugs allow players to ignore their injuries in the short term, their use can lead to long-term consequences including dependency and/or substance-use disorder. Over-adoption of drug treatments explain why many sports organizations have adopted the standards promoted by the World Anti-Doping Agency, to restrict the use of performance-enhancing drugs. For example, the NFL recently circulated a memo asking teams to voluntarily limit the use of some pain relievers (Goldberg, 2021). Regarding medical treatment interventions, our model suggests that requiring athletes to bear the cost of medical interventions may reduce over-adoption (e.g., “Tommy John” surgery discussed above).
Under-adoption can be easily illustrated with protective equipment (when risk and cost reduction are complements,
Correcting for under-adoption with a mandated policy can be difficult to enforce and monitor compliance. There is much evidence, for example, showing that many athletes prefer to continue playing after being the victim of an injury, even if doing so means concealing the injury. The NFL uses concussion spotters to remove players from a game and enforce, arguably imperfectly, return-to-play rules. Athletes have also been found to avoid self-reporting injuries because they do not want to lose playing time or to miss future games (Torres et al., 2013).
We conclude by noting the effect of game stakes on athletes’ adoption. As k increases, the slopes of the dashed curves of Figure 3 steepen and rotate around the point F. This increases the size of the area with over-adoption: therefore, the same injury policy can have different equilibrium outcomes depending on the context in which it is applied.
An example of a policy intervention designed to address the perverse effect of an increase in game stakes is the safe-play rule introduced by the NFL to reduce concussions in preseason practices. Prior to the beginning of each playing season, teams hold formal training camps to evaluate athletes and assess individual athletic skills. Due to the high-stakes nature of these effective auditions for employment, severe injuries, such as concussions or soft-tissue knee injuries, are not uncommon. These injuries typically happen during specific high-risk drills. According to the model, the value of k is higher during preseason than regular-season practice (personnel decisions have largely been made by the end of the preseason, ending the try-outs of marginal athletes). Prior to the introduction of the safe-play rule, teams self-restrain using these drills outside preseason practices. To address the growing concern of concussions, the NFL collectively banned the practice of three contact-intensive drills prior to the beginning of the 2019 preseason with one additional drill banned the following year. Figure 4 shows that a significant decrease in the number of concussions sustained during preseason practice took place after the introduction of safe play rules.
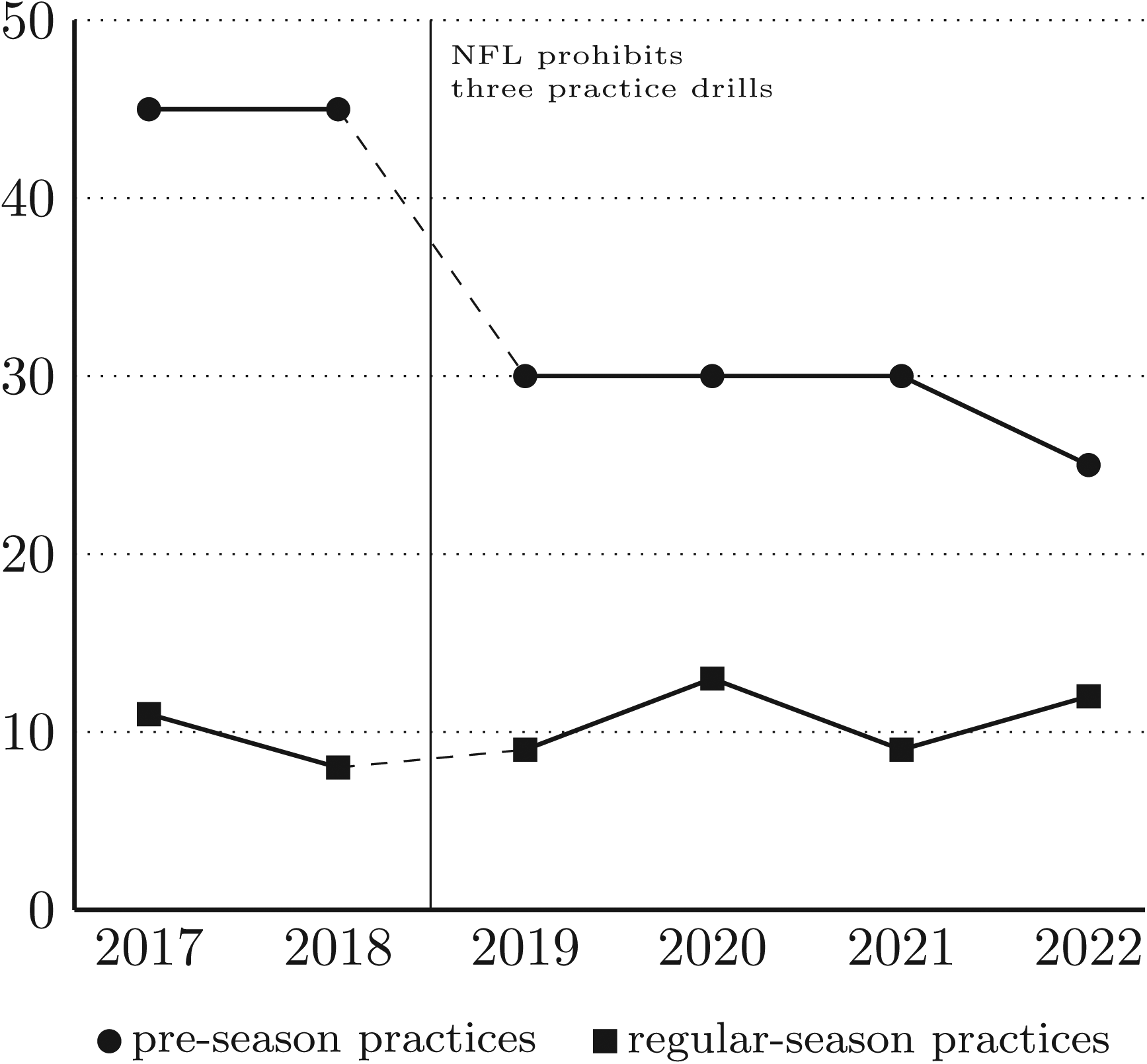
Concussions in NFL preseason practices (2017–2022).
Game stakes also has implications for enforcement of mandated policies. For example, return-to-play rules are less effective at preventing injuries at the end of a season or at the end of an athlete's career as the cost of missing a game is lower. 15 These rules should be stringently enforced in high-stakes games due to the increased incentive to take risk.
Discussion
Two properties of the athletes’ payoff functions are worth revisiting. Athletes face a prisoner's dilemma in competitive sports because the payoff functions depend on both athletes’ choice of risk. An injury policy is never required when game stakes are low. This is the case in recreational sports to the extent that an athlete's payoff is intrinsic and does not largely depend on winning. Examples include many activities such as fitness, yoga, hiking, and to a large extent to competitive sports with low stakes such as an exhibition game, a fundraising event, or a friendly match. The sport's athletes and organizer have the same objective function. This is consistent with the observation that many injury regulations apply to competitive activities where risk escalation is a concern.
Injury concerns do exist in noncompetitive sports but these fall under the standard analysis of consumer protection regulations to reduce accidents (e.g., cyclist wearing helmets or restriction on ski slopes). 16 The model argues that many injury interventions are specific to competitive sports where risk escalation is an important consideration. This point also talks to the observation that injuries are about equally likely to occur in training and competition and this is despite the fact that athletes spend a relatively small time competing (Parkkari et al., 2001): the return to risk is higher in competition than training.
Another feature of the model is the zero-sum, winner-takes-all, assumption in the payoff function. This is a strong assumption that rules out the possibility that risk has an entertainment benefit when the public values the excitement associated with risk. This could be included in the analysis and the operating principle that athletes do not internalize the impact of risk-taking on competitor welfare would remain. The difference is that sports organizations must also appraise fan excitement when they assess risk-taking in sports but doing so does not change the approach for policy analysis proposed in this work.
The model has considered the options to mandate, prohibit, or permit adoption. In general, however, the sport's organizer has more options to improve welfare. For example, the sport's organizer may encourage adoption through a subsidy or discourage it by setting a tax or a high standard. The model can accommodate these options, for example, as a change in the fixed cost F borne by athletes, keeping the fixed cost in the welfare calculations the same. Adoption can be implemented by setting the athlete's fixed cost low enough (possibly negative) such that C1 holds and C2 does not. In Figure 3, a lower athlete fixed cost shifts down the two dashed lines while keeping the other three curves unchanged. Alternatively, a sufficiently high value of the athlete's fixed cost, such that C2 holds while C1 does not, can switch an adoption equilibrium to a nonadoption one (the two dashed lines in Figure 3 shift upwards).
Conclusions
We incorporate athlete's incentives to take risk in evaluating the impact of injury policies in competitive sports. We model an injury policy as a change in the injury cost of risk-taking. The injury policy may be adopted by athletes or by a sport's organizer. In the equilibrium that results after adoption, athletes may de-escalate risk-taking (as in the case of a return-to-play rule) or escalate risk-taking (as in the case with the introduction of protective equipment). A paradoxical implication of the model is that an adoption decision that ignores athletes’ risk responses may wrongly lead to adopting an injury policy that ends up increasing injury costs. This will happen when the risk-escalating response dominates the baseline impact of the intervention. We also show that athletes under-adopt injury interventions that increase the cost of taking risk and over-adopt those that decrease this cost. Such adoption distortions are more likely to occur in high-stakes competitions. We apply this insight to several interventions used in practice and studied in the sports medicine literature.
Our approach offers an alternative view to the one found in the sports medicine literature that ignores the contribution of risk-taking in total injury costs. Although there are significant personal costs associated with injuries, these costs alone do not deter athletes from engaging in risky play. When risk-taking contributes to severe injuries (e.g., concussions), an effective way to contain injuries is to design injury interventions that increase the cost of taking risk. We argue that the adoption of strict return-to-play rules by many sports organizations act as a deterrence to risk-taking.
We end this article by touching on points being beyond the scope of this research but worthy of future attention. The results in this study complement other economic rationales for injury interventions not considered here such as the need to protect athletes against cognitive bias and the difficulty to assess the life-time costs of injuries. 17 Finally, our model does not capture the nonpecuniary prizes athletes compete for (the “thrill of victory”). Reminiscent of other sports controversies, such as cheating and doping, injuries will forever be a consequence of the eagerness to take risk in the pursuit of extraordinary performance.
Footnotes
Acknowledgements
The authors thank Zeeshan Hassan, Kristopher Hult, Daniel Rondeau, and Veska Suleva in addition to the two anonymous referees for their invaluable comments and assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.