
Abstract
Introduction
In recent years, medical advances have led to a steady increase in the frequency of organ donation following death by circulatory criteria (DCC). In Canada, annual statistics reported a record of 262 DCC donors in 2022, contributing to 32% of the deceased donations in the country that year. 1 It was reported that this was a 50% increase from 2013 to 2022, illustrating the growing role of DCC in donation and transplantation practices, and the prospects this specific strategy can add to saving lives. 1 Therefore, it is worthwhile to further explore this innovative method, to identify opportunities for additional advancements that may continue to expand the donor pool.
While the literature on the use of DCC organ donation in Canada exists, with protocols published outlining best practices, the literature on this practice is fragmented. This suggests a need to summarize this information to gain a clearer picture of how DCC organ donation in Canada functions, with particular emphasis on the development and implementation of guidelines, as well as complexities, challenges, strategies, and potential opportunities. Synthesis of these aspects identified gaps for future research, practices, and policy to advance in this field.
Objective
The purpose of this integrative review was to provide a comprehensive overview of Canadian practices with organ donation after DCC. The overarching research question aimed to determine how organ donation after DCC evolved. Sub-questions relevant to the review were developed to identify existing protocols and guidelines, challenges and strategies related to implementation, as well as the perspectives regarding the practice.
Methods
Design
An integrative methodological approach was used for this review. The guidelines for conducting an integrative review provided by Whittemore and Knafl were used in the development, which included problem identification, literature review, data evaluation, and data analysis. 2
Search Strategy
An electronic search strategy was developed by the primary researcher, with the support of a librarian specialist in health sciences, and was performed using the following databases: CINAHL Complete, MEDLINE-OVID, Embase, ProQuest—Nursing & Allied Health Premium, PsychINFO, and Web of Science Complete. These databases were searched using variations of several key terms and phrases, as well as Medical and Subjective Headings (MeSH) (available upon request). A gray literature search of Google Scholar was also performed, considering the first 100 resources. Additional literature was obtained and reviewed using the snowballing technique, by screening the title of articles referenced within articles that met the inclusion criteria. 3
Article Selection
Articles located through these search methods were imported into Covidence®, a review management software, to undergo a multi-phase and systematic screening process. Screening was completed first by title and abstract, then by full text. Articles were considered for any date up until the search was performed on June 1, 2024. There was no date limitation set due to the unknown initiation period of DCC prior to the first published guidelines in 2006. Articles were considered if written in English, French, Portuguese, or Spanish, languages spoken by the authors. Exclusion criteria included any articles focused on donation after neurological death, tissue donation, or feasibility studies for procedures.
Data Extraction and Analysis
Outcome Measures
Data were extracted from the included articles using an extraction table developed by the first author. Quantitative data was collected to identify the title, author(s), date of publication, type of article, and journal location of the included articles. Additional information pertaining to study design, participants and setting were collected for applicable articles. These elements provided an overview of the publication trends and were subsequently used to conduct a bias assessment. Qualitative outcomes collected aligned with the research questions and included key statements pertaining to the evolution of DCC, policy and program description, stakeholder experiences, challenges and strategies. Additional qualitative outcomes extracted included pertinent article recommendations and limitations.
Descriptive statistics were used to analyze the collected data quantitatively and to provide an overall description of the included articles characteristics. An inductive content analysis approach was used to analyze collected data qualitatively, and to synthesize the main findings that could be used to answer the research questions. The initial areas of interest based on the research questions informed the analysis, while themes and categories were developed inductively by performing multiple reviews of the extracted data to identify common concepts and develop initial codes. 3 These ideas and codes were then grouped together with others based on their relationship to one another and used to develop the main categories. 3
Bias Assessment
The data evaluation stage of an integrative review can be quite complex due to the inclusion of various methodological designs; therefore, the Mixed-Method Appraisal Tool (MMAT)® was used to address potential bias and assess the quality of the included articles. 4 Evaluation of the data was performed by the primary researcher and peer-reviewed by another member of the research team. First, all included articles were evaluated based on whether they had clear research questions or research purpose and if and how well data were collected to provide a response to those. Articles that met these initial screening questions underwent subsequent evaluation applicable to the study design. Qualitative studies were assessed using 5 criteria considering their appropriateness of the approaches, adequacy of the data collection methods, and the overall quality and coherence of the interpreted data. Quantitative designs were assessed using 5 criteria related to sampling, measurement, and data analysis strategies.
To assist in the interpretation and synthesis of data based on the quality of the included articles, a percentage score was calculated for each study that underwent secondary evaluation using the MMAT®. Articles meeting all 5 MMAT® criteria for the respective study design obtained a 100% (5/5) score, 4 criteria obtained an 80% score (4/5), and so forth. Articles described as summaries of consensus or guideline development meetings were scored using qualitative criteria. Rationale for this decision is because the corresponding articles incorporated qualitative-like approaches by use of expert panel evidence synthesis and discussions to provide a summary of key themes.
Results
A total of 792 articles were located through the search for published literature. After the removal of 202 duplications, there were 591 articles that underwent screening, with 50 ultimately included ( Figure 1 ). Results were separated into quantitative and qualitative components.
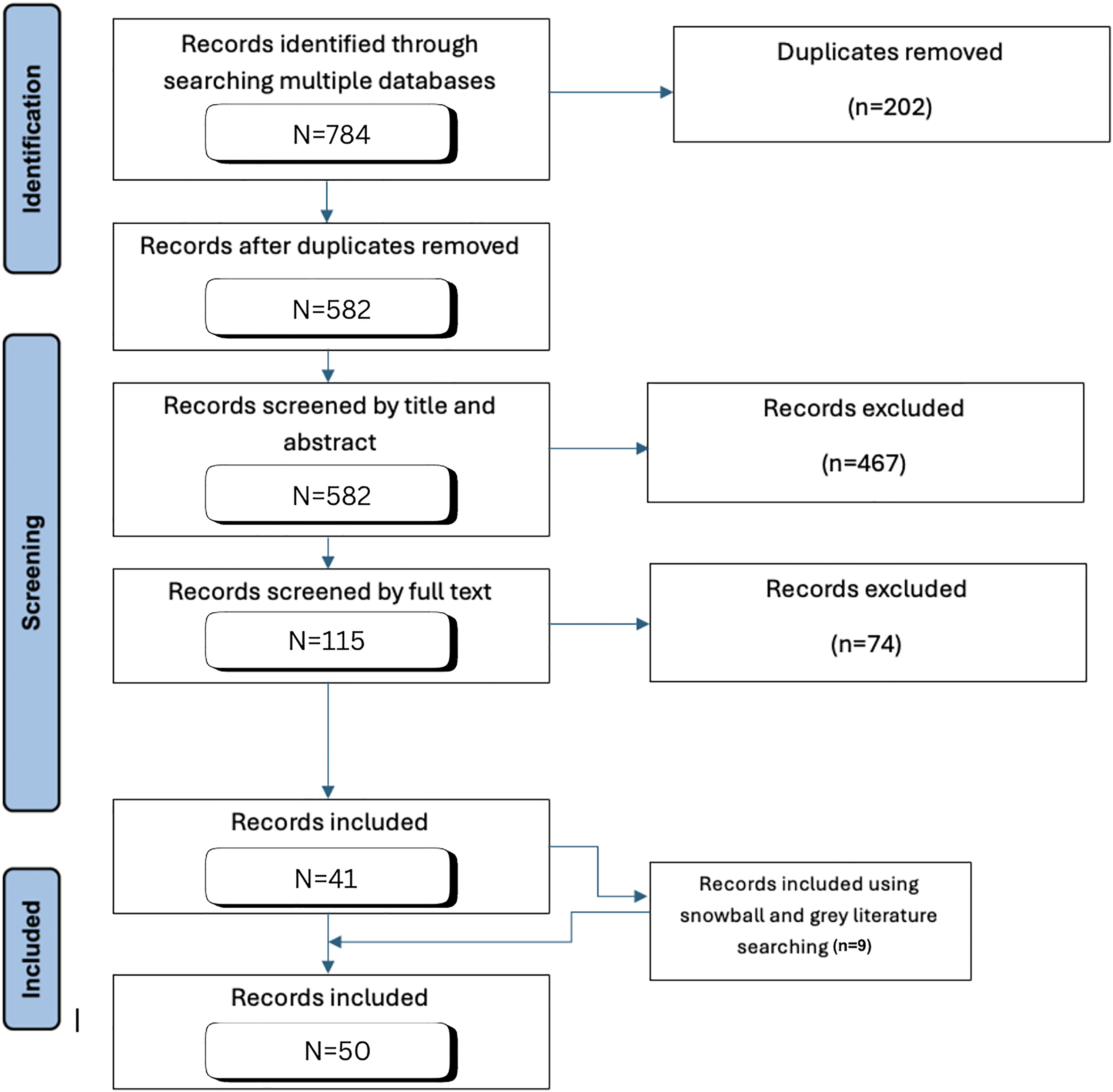
Literature identified for organ donation after death by circulatory criteria.
Quantitative Results
Study Characteristics
The year of publication ranged from 2002, a time before DCC was officially introduced to 2024. Most of the articles included were published between 2016 to 2024 (N = 37, 74%), and 19 (38%) were published in the Canadian Journal of Anesthesia. Others were published primarily in journals dedicated to transplantation (N = 8, 16%), critical and emergency care (N = 11, 22%), and medical ethics (N = 1, 2%). Methodological approaches of the included articles involved quantitative descriptive designs including prospective studies (N = 3, 6%), cross-sectional surveys (N = 8, 16%), retrospective studies (N = 2, 4%), and secondary analyses (N = 2, 4%), as well as qualitative designs using descriptive (N = 3, 6%) and exploratory (N = 1, 2%) methods. Other document types included consensus/guideline development meetings (N = 12, 24%), qualitative content analysis/discussion papers (N = 16, 32%), and scoping reviews (N = 3, 6%).
Quality Appraisal
Among the 35 articles that met the MMAT® initial screening questions, 28 met all 5 MMAT® criteria, scoring 100%, 6 met 4/5 MMAT® criteria, scoring 80% and 1 met 3/5 MMAT® criteria, scoring 60%. There were 15 articles that could not be evaluated using secondary MMAT® questions due to their underlying document type of discussion paper. All articles that met the inclusion criteria were subsequently included despite some of the inconsistencies identified, because of their overall quality and relevance to the research questions. Data from those given percentage scores were incorporated more thoroughly throughout the results. A summary of the quality assessment is available upon request.
Qualitative Results
The inductive content analysis approach revealed 3 main categories that were used for reporting on how DCC has evolved. These include a) Evolution of DCC organ donation guidelines, b) Experiences with DCC program development and delivery and c) Perspectives and understanding of DCC. Several sub-categories also emerged from the analysis, providing further context for how Canada has evolved in DCC.
Evolution of Death by Circulatory Criteria Organ Donation Guidelines
The landscape of organ donation has expanded over the years, demonstrating the strides made to transform healthcare and save the lives of Canadians, and 24 papers included this discussion. Knoll and Mahoney suggested that there were 3 main issues that initially restricted usage of DCC organ donors. 5 These included education, ethics, and the availability of resources such as physicians, nurses, critical care beds, and operating rooms. 5 Similarly, Knoll and Tinckam suggested that coordination of deceased organ donation was complex because of the expansive size of the country and specific mandates for healthcare that vary according to the province. 6 While others alluded to the fragmented nature of organ donation programs, as each province has their own Organ Donation Organization, despite organ retrieval and allocation being made in a collective manner in most situations.7-9
The first effort to establish DCC practices occurred in 2005 during a national forum aimed to developing recommendations for the practice and procedures, as well as ethical and legal components. 8 The forum began with a deep dive into the national and international literature on the use of DCC donors, to summarize current practices and outcomes. Following this, a large portion of the designated time was for presentations on family, patient and medical perspectives, as well as presentations from medical experts from countries where DCC was used such as the United Kingdom and the United States of America. Small and large group discussions were conducted to explore the various processes of care identified, including death determination and criteria for organ donation, procedures for withdrawing life-sustaining measures, organ donation options and consent, phases of care, post-mortem care, organ viability limitations, and preservation techniques. These discussions were used to develop the recommendations specific to each process. In addition to this, core values for guiding program developments were outlined by this forum, including the respect of life and dignity of all individuals, holistic end-of life care, respect for autonomy, support for family and loved ones, public trust, and respect for professional integrity. 8 A pilot program for DCC was launched in 2007 in Quebec, which resulted in 33 successful transplants between 2007 and 2009. 9
At the time these national recommendations on DCC organ donation were provided, deceased donation definitions and guidelines were based primarily on the cessation of cardiac functioning or neurological functioning. Downie et al suggested that this definition was unclear and left healthcare providers at risk for liability. 10 Therefore, a new practice guideline was developed in 2023, recommending that both pathways of deceased donation be defined and determined using a brain-based definition of death. 11 As a result, a focus on the absence of extra-cranial circulation to declare circulatory death was introduced. Rationale for this guideline change was provided by Murphy et al (2023), suggesting that part of the shift was to adhere to more contemporary biomedical and legal understandings of death, to have universal definitions of death among the provinces, providing clarification for public and professional confusion, to accommodate emergence in technology, minimize risk of diagnostic errors, and to align terminology with current practices. 12 There were a number of other changes recommended for deceased organ donation within this new national guideline for DCC organ donation, particularly related to diagnostic testing for confirming cessation of circulation. 11 Consequently, Murphy et al (2023) suggested that some of the updated guidelines enabled interventions aimed at restoring circulation in DCC donors to be introduced, such as normothermic regional perfusion (NRP), tidal ventilation in lung donation, and the use of uncontrolled DCC donors in some capacity. 13
Since the time these national recommendations on DCC practice were introduced, several other consensus meetings, guidelines, and recommendations have been published. These included articles related to pediatric DCC organ donation,
14
withdrawal of life-sustaining measures,
15
,
16
ethical concepts,
17
family discussions,
18
cardiac donation,
19
and quality improvement measures,20-22 which are all described in
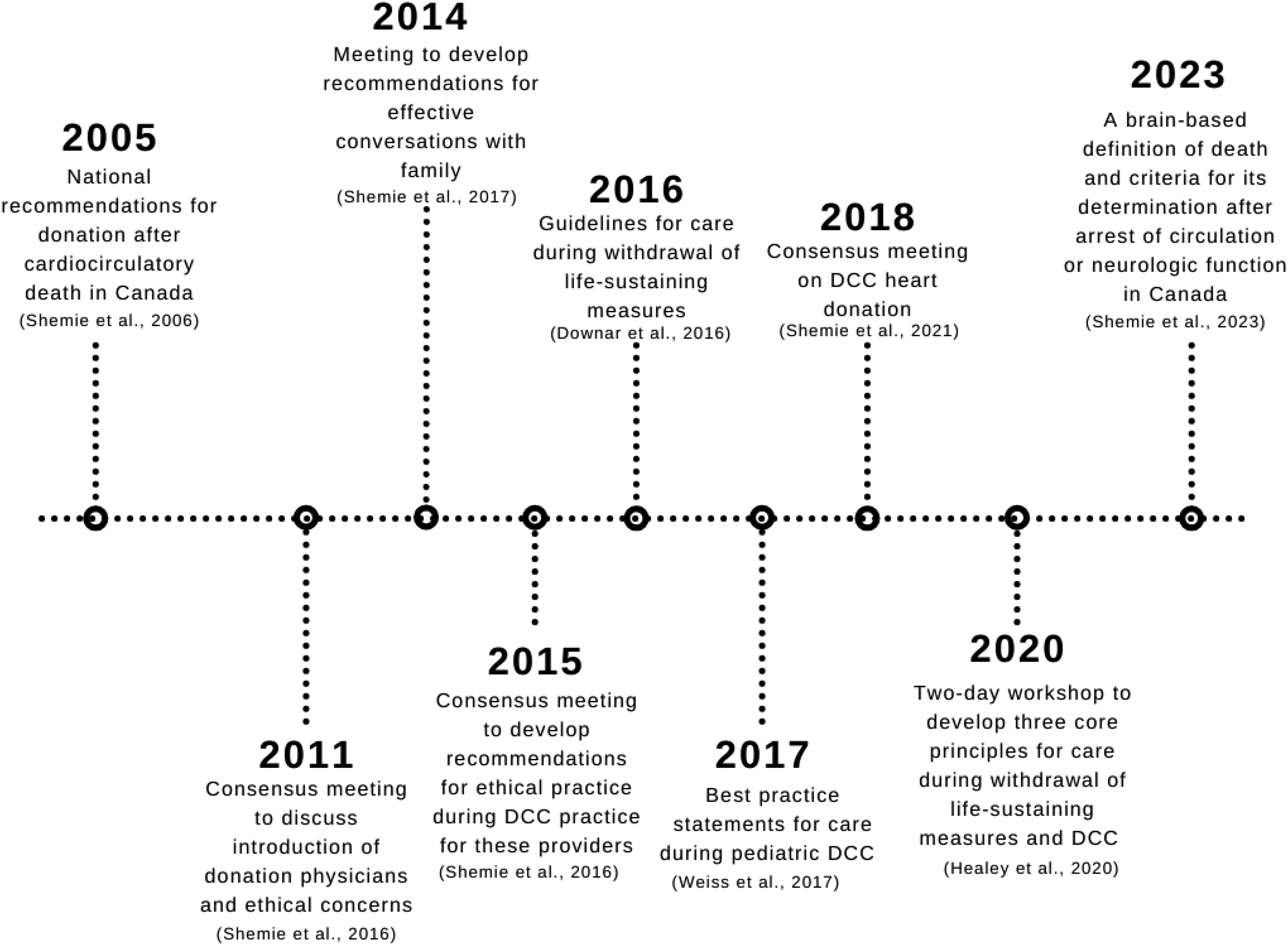
Timeline of guidelines, recommendations, and meetings on DCC.
Guidelines for Donation After Death by Circulatory Criteria (DCC).
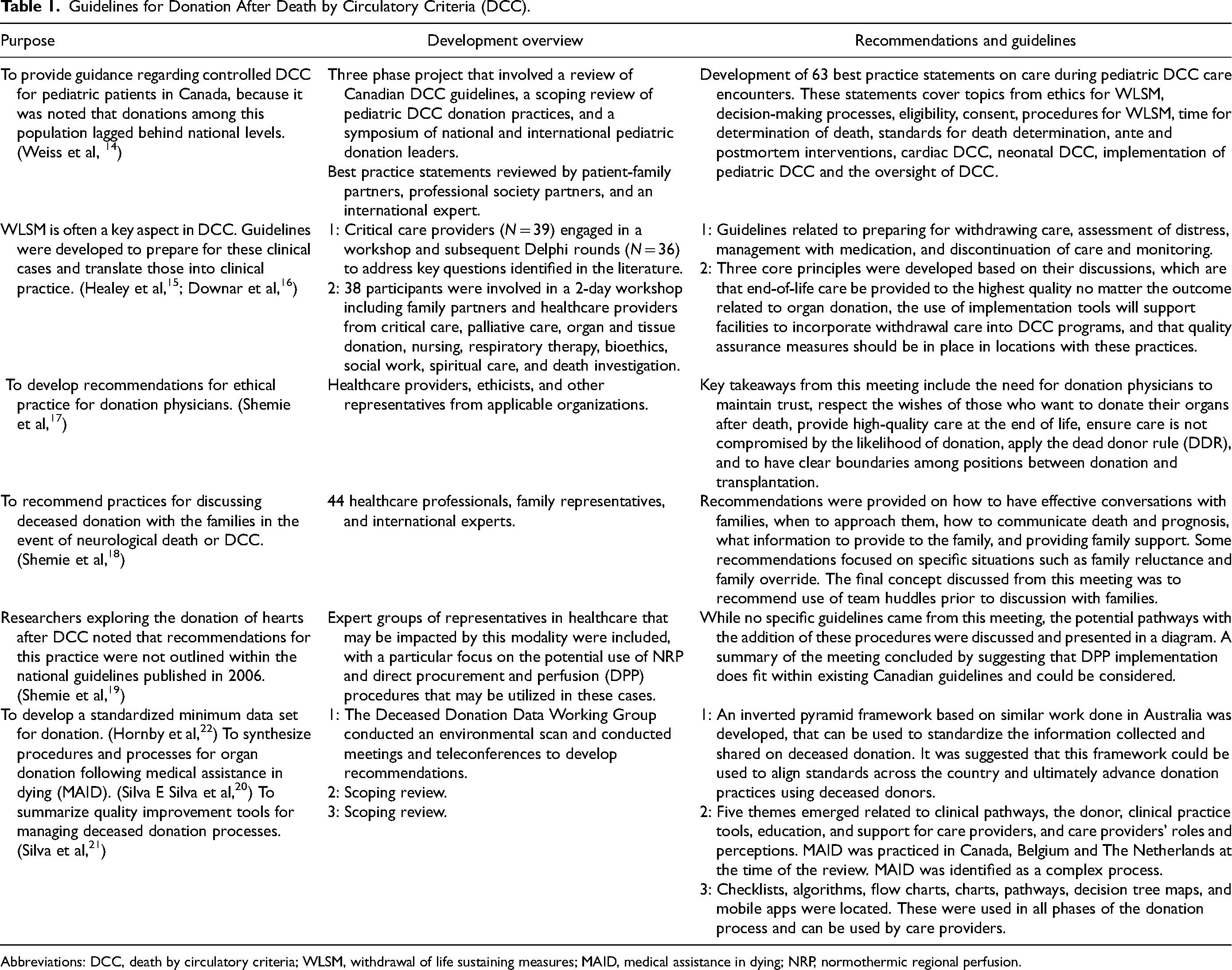
Abbreviations: DCC, death by circulatory criteria; WLSM, withdrawal of life sustaining measures; MAID, medical assistance in dying; NRP, normothermic regional perfusion.
Experiences With Death by Circulatory Criteria Program Development and Delivery
Subsequent to the inception of DCC practice in 2006, the implementation of programs has been gradual. 26 Despite this, there are several articles (N = 10) describing healthcare organizations experiences with developing and implementing organ donation following DCC programs. Some challenges were described from the experience, such as airway issues, acute organ rejection, arrhythmias, and hypotension. 27 , 28 Alternatively, several recommendations were made from the experiences, related to increasing referrals and awareness, clear communication, good leadership, transparency, preparation, incorporating patient–family partners, and collaboration as some examples.27-30
Several studies have also shown the variability in DCC practice, another item that has been recognized since the adoption of DCC in 2006.7,26,31 Variations were noted with medication use, nutrition support, time from hypotension to death, diagnostic procedures, airway management, and even for the existence of policies and procedures for the practice.26,32-36
Experiences With Donation After Death by Circulatory Criteria Program Development and Delivery in Canada.
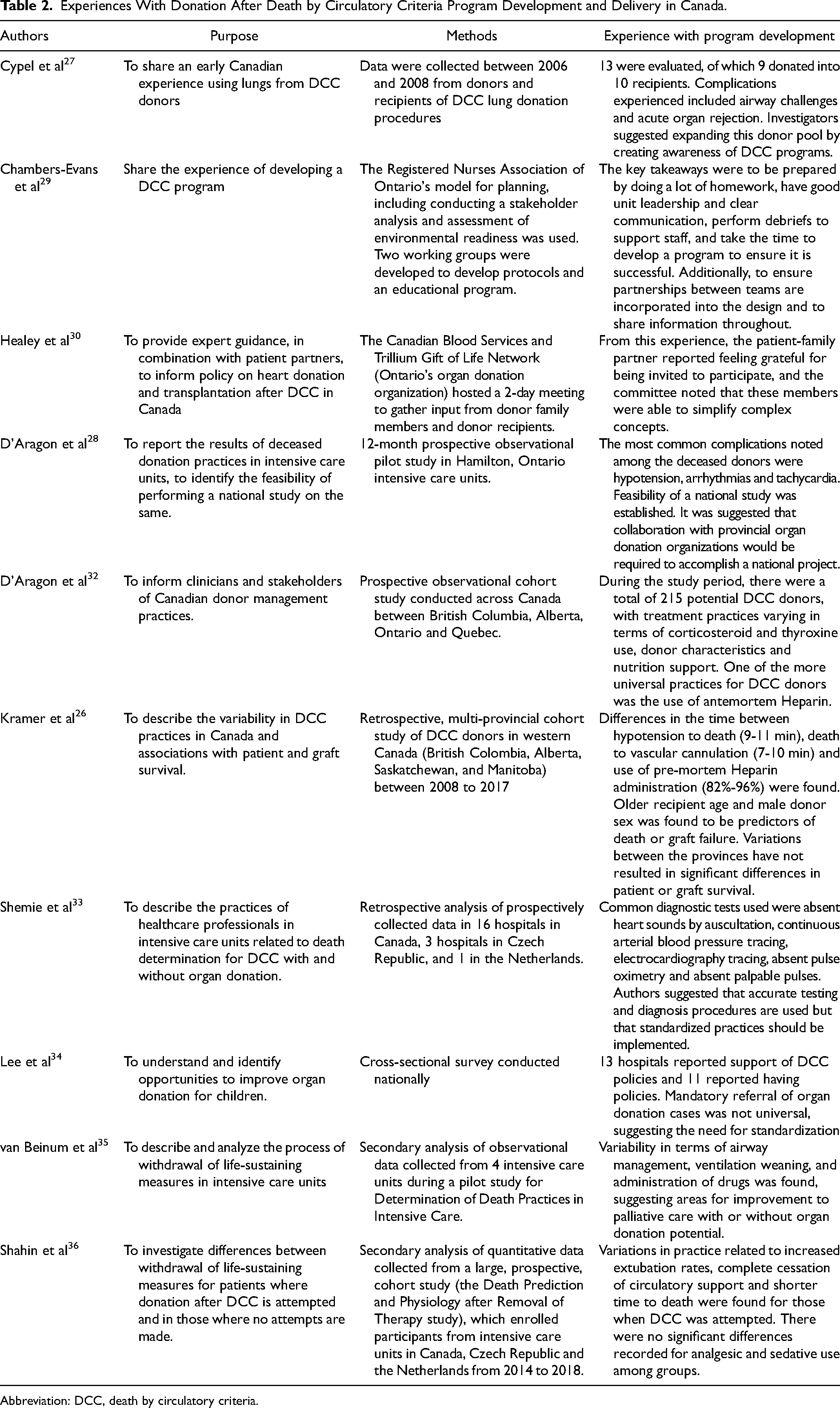
Abbreviation: DCC, death by circulatory criteria.
Perspectives and Understanding of Death by Circulatory Criteria Donation
The integration of DCC has sparked many researchers to explore perspectives regarding these practices (N = 12). A majority of these studies aimed to gather information regarding the attitudes, opinions, and knowledge of healthcare professionals specifically regarding DCC, while others considered the perspectives of the general public. Findings from 1 study that explored both populations’ perspectives found that healthcare workers were more likely to donate organs than receive them, whereas the public were more likely to receive organs than donate. 37 It was also found that healthcare providers reported having more knowledge on withdrawal of life-sustaining therapies than the general public. 37
Several studies had specific focuses when considering perspectives and understanding regarding DCC, such as specific procedures for DCC, facilitators and barriers, knowledge and education needs, and the family experience. Many of which are corroborated by other articles located from this review.
Procedures/Protocols for Donation After Death by Circulatory Criteria. The use of certain procedures during DCC organ donation, such as NRP, direct procurement and perfusion (DPP), and extracorporeal cardiopulmonary resuscitation (ECPR) was often required, of which researchers have aimed to gain perspectives. One study collected and analyzed the attitudes of healthcare providers and the general public regarding DPP and NRP, finding overall acceptance of these procedures among these populations. 38 , 39 A related study was conducted by Brooks et al considering use of ECPR within clinical settings for out-of-hospital cardiac arrests. 40 Experts within the field proposed several considerations for this procedure about fair access, cost, candidates, feasibility, readiness, safety, and training. 40 The group reported a generalized support for this procedure but suggested it should only be implemented in large facilities that have the potential opportunity to learn from the use. 40 Results from a study aimed to explore pediatricians’ confidence in declaration of death among DCC donors, revealed that many of these care providers were not confident that these donors were actually dead, with variations depending on the given scenario. 41
Facilitators and Barriers. There were barriers identified regarding DCC organ donation. One of these barriers included the confusion regarding practices for DCC, primarily due to the unclear guidelines and variability in front-line practices and policies. 42 The concept of role ambiguity, due to multiple healthcare professionals involved in the DCC process with sometimes overlapping or conflicting roles, was also described.5,42-45 Additional barriers described included education, resources, such as operating room spaces and staffing, communication, and support. 42
Several recommendations and facilitators for DCC organ donation were found. One of these included the importance of obtaining public perspectives on the speciality practice of DCC. 42 A scoping review that summarized the DCC literature found no results and ultimately suggested this to be a gap that may be important to research further. 46 A study that aimed to understand the experiences of families during the deceased organ donation process, suggested that comprehensive support and information about the outcome of the transplant case could be provided. 47 A recommendation for the concept of role conflict was to have separate care providers responsible for patient care and organ donation, preventing competing priorities.42-45,48
Knowledge Assessments. The needs assessment on education for healthcare providers on organ donation and DCC was conducted within several studies.49,50 Gaps in resident's knowledge and limited learning on DCC, as well as a need for training and a standardized curriculum to learn about organ donation was identified by Sarti et al 49 Hancock et al 50 surveyed intensive care and emergency room physicians and nurses and found that competency comfort levels were between 8% and 85.6% depending on the care provider, of which emergency care providers and nurses identified lower levels overall. Robert et al found that 69% of medical students surveyed were not aware of the concept of DCC. 51 Likewise, critical care residents’ education on end-of-life was explored in Arora et al's study. 52 Residents reported a discrepancy between certain organ donation-related skills, including identifying potential DCC donors and conducting the DCC process, where many reported effective teaching methods, yet reported not being comfortable with the skills themselves. 52
Discussion
The results of this integrative review provide a summary of how Canada has evolved in the development of DCC programs. Several guidelines and recommendations have been proposed by lead researchers and key stakeholders within the field of organ donation, that focus on a range of concepts from front-line practices, pediatric DCC, end-of-life care, withdrawing treatment, core values, family conversations, and ethical aspects. Lessons from organizations that have implemented DCC were provided, emphasizing the importance of preparedness, communication, and standardization. Other factors that were highlighted include the complexity of the procedures that may be used during DCC and the educational needs for those directly and indirectly involved in this practice.
It is evident that there are several variations in the way that DCC practices and protocols were implemented. Research from other countries reveals similar differences in DCC program delivery, suggesting that this may be more of a global challenge than anticipated. An evaluation of DCC programs in Europe reported that there were significant differences between the categories used, legislation, and the way death was determined between the 10 countries using this method of donation. 53 Similarly, Elsiesy et al reported regional variations in organ donation practices across Saudi Arabia, particularly related to the implementation of a Mobile Action Donor Team initiative in some regions. 54 Description of these dispersed programs have been considered fragmented; therefore, it may be beneficial to consider more standardization of these practices across provinces.
Despite these variabilities, it is promising that many were receptive to this form of organ donation, providing a unique opportunity to potentially continue to enhance this practice. Education on this topic is required first, primarily for those in healthcare roles that may be impacted by such advancements. While several training needs were identified among the literature, how to deliver such education was not thoroughly described. An integrative review considering training methods for healthcare professionals’ communication skills and decision-making in deceased organ donation were explored by Potter et al. 55 Results from this review demonstrated the array of delivery methods that can be used to educate healthcare providers on organ donation concepts, including those offering theory, role-playing and reflection as some examples. Commonly used were simulated-based exercises, with incorporation of debriefing. Therefore, incorporation of such techniques to educate healthcare providers on DCC practices may enhance comfortability and delivery of care for these donor cases.
Several other recommendations were highlighted among the literature, including the use of designated healthcare providers to prevent role conflict and the involvement of the public when considering new practices. Wall et al emphasized this practice when developing the protocol to consider expanding DCC donation to uncontrolled cases, 56 which may be considered advancement. Similarly, Parent et al described the importance of informing the public how such programs could impact wait times and how decisions will be made. 57 Dhanani et al considered this from a Canadian perspective, encouraging open dialogue with the public, medical, and policy communities. 58 It is essential then, for researchers to continue to engage the public in discussions on DCC practices within Canada, especially if advancements in practices in any capacity are being considered.
Ultimately, the knowledge gained from this review on DCC organ donation highlights some of the critical components that must be considered if expansion of DCC organ donors continues. Insights are being used to guide a study exploring leaders and key stakeholders’ perspectives on uncontrolled-DCC policy development. Future research may also wish to incorporate some of the other key recommendations described, such as through the conduction of a study to gain the perspectives on the public and healthcare providers on uncontrolled-DCC organ donation.
Limitations
There were a few limitations to this integrative review. The first was the heterogeneity among the included studies, including differences in the study designs, populations, and contexts. The variability made it difficult to compare findings and limited approaches to synthesize the results. While the inclusion of mixed designs allowed for a broad review of the literature, there is a risk of bias in the way data were selected and analyzed due to use of this approach, which may have been reduced with use of a more systematic-type review with stricter inclusion and exclusion criteria. Since there was variability in the quality of the included articles, it is possible that some of the results and information presented may not be reliable and may need to be interpreted with caution.
Conclusion
The evolution of DCC organ donation demonstrates the great strides that have been made in this specialty field, however, also underscores the need for further development of guidelines for this practice and standardization across provinces. While there have been numerous challenges to delivering care through DCC organ donation, various strategies have also been provided to enhance these practices and continue providing this life-saving treatment. These strategies may also be used to support continued advancements in this field that could allow for the use of practices such as uncontrolled DCC organ donors, or other methods, further increasing the number of organs available to save and improve lives.
Footnotes
Acknowledgments
The authors would like to thank Research and Scholar Communication Librarian Elizabeth Yates MLIS, for their support in the development of the search strategies for this review, and Bachelor of Science in Nursing student Isabelle Boudreau for their support with the quality appraisal.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with the research, authorship, and/or publication of this article.