
Abstract

Keywords
Introduction
Some US liver transplant centers use abdominal normothermic regional perfusion (A-NRP) techniques for donation after circulatory death (DCD) procurement that limit perfusion via the NRP circuit to the abdominal cavity. 1 One limitation to the use of A-NRP for cardiac DCD donors occurs when the planned heart recovery procedure is direct procurement with normothermic machine perfusion (DP-NMP) because there is a perceived incompatibility of DP-NMP cardiac procurement with A-NRP liver and kidney procurement despite demonstrated feasibility in the United Kingdom.2,3 The challenge with using different procurement techniques in the thoracic and abdominal cavities is that there can be significant volume loss in the chest when thoracic organs are removed, which impacts the ability of the abdominal procurement team to maintain adequate flow rates on NRP. The key to successful dual procurements is meticulous hemostasis and excellent communication between teams to make sure both techniques are progressing as expected. This case report presents the first successful simultaneous rapid recovery heart with A-NRP liver and kidney DCD procurement in the United States. Donor family consent could not be obtained so no identifying characteristics are included.
Presenting Concern
This case concerns a DCD donor in which the liver was accepted with the plan for A-NRP procurement, and the heart was accepted with a plan for direct procurement with ex situ machine perfusion
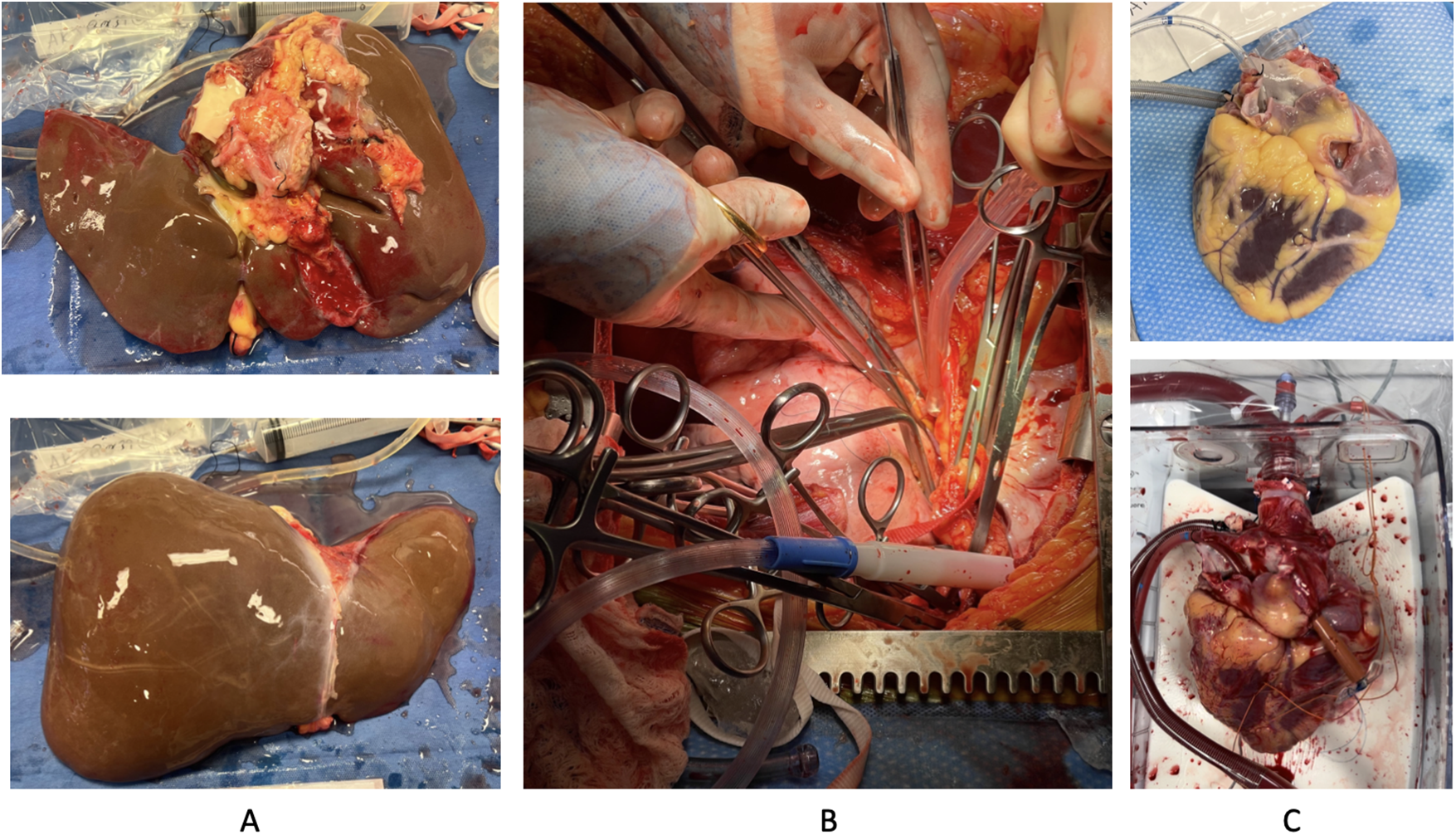
Procurement images of liver and heart recovery using abdominal normothermic regional perfusion. (A) Postflush backtable photographs of liver allograft. (B) Intraoperative image of the thoracic cavity after heart removal while on abdominal normorthermic regional perfusion. Multiple clamps are in place for hemostasis and the clamp on the inferior vena cava above the liver is being sewn into place to avoid being dislodged during liver mobilization. (C) Postflush backtable photographs of the heart allograft cannulated for and on the TransMedics organ care system (OCS™) (TransMedics, Inc, Andover, MA).
Clinical Findings
Before donor extubation, sheaths were placed in the left femoral artery and vein for rapid wire exchange to cannulas postmortem. Following confirmation of death, the femoral venous sheath was wire exchanged for a 25-French multistage venous cannula. Via a preconnected Y-connector in the venous tubing, 1.5 L of blood was collected into a drainage bag for postrecovery warm reperfusion of the heart. Two units of packed red blood cells were used to prime the NRP circuit to replace the volume collected for heart reperfusion. The arterial sheath was wire-exchanged for a 19F cannula.
Simultaneously, the cardiac team opened the chest and cross-clamped the descending aorta to isolate NRP to the abdomen. The inferior vena cava (IVC) was clamped directly above the diaphragm. The superior vena cava (SVC) was clamped caudal to the azygos vein initially and the ascending aorta was clamped, completely isolating the heart. NRP was initiated at 2:50 s from the start of the procedure. The heart was perfused with cold cardioplegia after venting the left pulmonary veins and the IVC leaving a 2 mm cuff above the clamp. The azygos vein was clipped with 3 large ligaclips and divided. Another SVC clamp was placed cranially just below the innominate-SVC junction and the SVC was divided below it. Cardiectomy was completed and the IVC clamp was oversewn to prevent any risk of it slipping during liver mobilization.
A-NRP was continued for 44 min, for a total pump time of 57 min. Flow was maintained above 4.5L, and lactate down-trended from 11.1 to 8.38
Lactate Trend Over Time on Abdominal NRP.
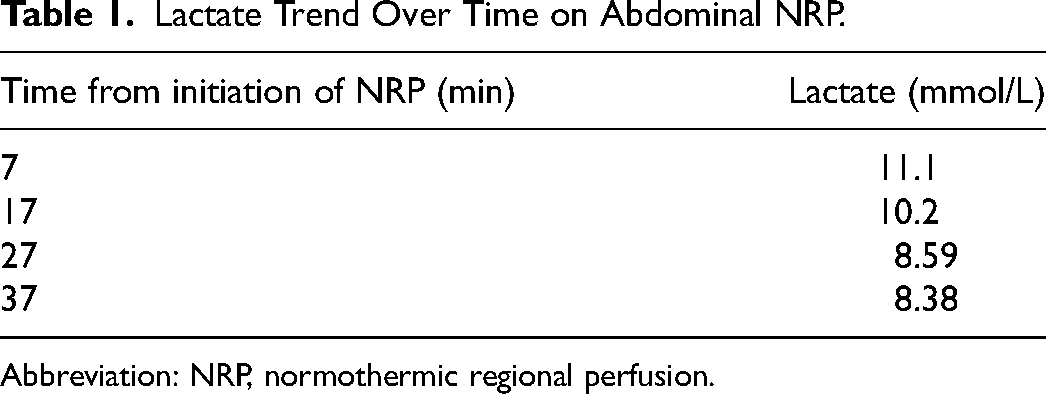
Abbreviation: NRP, normothermic regional perfusion.
Outcome
The liver and heart recipients both had uneventful operative courses. The liver recipient spent 1 day in the intensive care unit and 5 total days in the hospital before discharge. At the time of this submission, the heart recipient remains hospitalized and is expected to fully recover.
Discussion
This case demonstrates the feasibility of A-NRP with cardiac rapid recovery DCD procurement. This approach is an option for donor hospitals that have ethical concerns about thoracoabdominal NRP. It can also be done with direct intra-abdominal IVC and aortic cannulation when premortem interventions are not allowed.