
Abstract
Introduction
While survival following liver transplantation has improved over the past 3 decades, few studies have examined the changes over time in hospital length of stay (LOS), a surrogate for healthcare expenditure and an important short-term outcome measure.
Research question
The purpose of this study was to compare post-transplantation LOS over the last 3 decades.
Design
A cross-sectional analysis of 150 603 adult liver transplant recipients between September 1987 and July 2021 from the UNOS database was conducted. The patients were placed into 3 eras (1987-1989, 1990-1999, and 2000-2021) based on a Join point regression analysis of significant time points of change in LOS trends. Risk factors that were significant in univariate analysis (P < .05) were included in the multivariable Cox regression analysis, which controlled for 29 donor/recipient characteristics.
Results
Among adult patients, the average LOS following liver transplantation changed from 51.5 days in 1987 to 16.3 days in 2021, with a relatively steeper decline prior to 2000. On multivariable Cox regression, patients in both the 1987-1989 cohort (hazard ratio [HR]: 0.54, 95% confidence interval [CI]: 0.52-0.57) and the 1990-1999 cohort (HR: 0.77, CI: 0.76-0.78) had significantly prolonged lengths of stay (HR < 1 associated with later hospital discharge) compared to the 2000-2021 cohort.
Conclusions
This analysis found that mean LOS decreased over time in adult liver transplant recipients, even after controlling for donor and recipient-level factors. Future studies are needed to elucidate root cause factors for this decline in LOS over time.
Keywords
Introduction
Over the past several decades, mortality following liver transplantation has improved considerably, due in part to advances in surgical techniques as well as improvements in the medical and critical care of transplant recipients. 1 In addition to this increase in post-transplant survival, metrics beyond mortality are critical to improving patient outcomes and gauging the improvements in liver transplantation. For example, while the model for end-stage liver disease (MELD) and pediatric end-stage liver disease (PELD) scoring systems have led to improvements in waitlist mortality, their implementation has also been linked to increased medical costs, demonstrating that the sole consideration of survival metrics in clinical decision making may provide a limited perspective in evaluating overall transplantation outcomes. 2
Recently, several studies have indicated that hospital length of stay (LOS) is both an important short-term outcome measure and a surrogate for healthcare expenditures. 3 Several studies have established LOS as a measure of operational success, directly associating prolonged LOS with adverse post-transplantation outcomes and increased complications.4,5 Likewise, some studies have linked LOS to center-level characteristics, such as program experience and administrative support.6,7 Furthermore, LOS has been used as a measure of healthcare resource utilization, since prolonged LOS required more critical care and financial resources. 8 As healthcare facilities face increased economic and resource constraints, this facet of LOS has become increasingly relevant to the delivery of care.
Most research in the field has focused on associations between LOS and pre/posttransplant patient-level predictors.9–12 For example, the LOS index used 22 donor and recipient factors to predict hospital LOS following liver transplantation. 13 Similarly, several studies have used LOS in predictive models to forecast clinical outcomes following surgery.14,15 Although there is existing literature on LOS as an outcome measure, there is limited research on long-term changes in LOS over time. Examining longitudinal trends in LOS can provide additional insight into the trajectory of liver transplantation practices in the United States while offering actionable avenues for improvements in clinical and financial domains.
The primary objective of this observational study was to identify general trends in hospital LOS following liver transplantation from 1987 to 2021. A second objective was to identify patterns in LOS over time for high- and low-acuity patients and for specific Organ Procurement and Transplantation Network (OPTN) regions.
Design/Methods
Design
This study was a retrospective, cross-sectional analysis of liver transplant patients in the United States. Institutional Review Board (IRB) approval was obtained prior to the analysis of data and drafting of the manuscript.
Population
This analysis used the liver registry with de-identified patient-level data collected by the Organ Procurement and Transplantation Network (OPTN). The database included all patients listed for liver transplantation in the United States.
Sampling
A retrospective analysis was performed of all adult recipients who underwent liver transplantation between September 30, 1987, and June 30, 2021. All transplant recipients older than 18 years were included in the analysis. Donor and recipient characteristics were reported at the time of transplant. Follow-up information was collected at 6 months and then yearly after transplantation. Recipients undergoing multivisceral transplants (n = 11 248) were excluded from the study. Recipients with a missing discharge date were also excluded (n = 6767). Traditional measures of patient health such as the MELD score lacked sufficient data for the earlier years in the study; therefore, the LOS index, which accounts for a comprehensive list of patient risk factors with relatively complete entry completion through time, was used to define relatively low (<10th percentile LOS index) and high (>90th percentile LOS index) acuity patients for potential hospital LOS.
Analysis
Data were analyzed using a standard statistical software package, Stata® 17.0 (Stata Corp, College Station, TX, USA). Continuous variables were reported as a mean (standard deviation) and compared using the Student's t-test. Contingency table analysis was used to compare categorical variables. Results were considered significant at a P-value of <.05. All reported P-values were 2-sided. The primary outcome measure was discharge from the hospital. Time to discharge was assessed as time from the date of transplantation to the date of discharge. A Poisson regression model and Monte Carlo Permutation Test for model selection were used to determine 3 statistically significant eras for the study using the Joinpoint Regression Program, Version 4.9.1.0. Excel was used to generate mean LOS and transplant volume graphs with trendlines. Kaplan-Meier analysis was used for time-to-event analysis. The LOS was the dependent variable in the Cox regression analysis. The 3 eras (1987-1989, 1990-1999, 2000-2021) and recipient and donor risk factors were the independent variables.
Twenty-nine recipient, donor, and center-level factors found to be significant in prior analyses (P < .05) were used in the univariate analyses. 13 Continuous variables were categorized using clinically relevant groupings. Normally distributed continuous variables were analyzed using ANOVA, while non-normally distributed continuous variables were analyzed using the Kruskal-Wallis test. Pearson's chi-square test was used to analyze binary and categorical variables. Recipient risk factors were collected at the time of transplantation. ICU and hospital admission refers to the type of admission at the time of transplantation.
Missing variables were imputed using predictive mean matching imputation method for incomplete predictors in the OPTN database. The following donor variables were imputed: functional status at transplant (0.44% missing entry completion), donor age (0.02%), recipient's bilirubin concentration at transplant (0.01%), distance from donor hospital to transplant center (1.35%), recipient BMI (1.67%), recipient weight (0.79%), donor weight (1.8%), recipient's albumin levels at transplant (1.86%), recipient height (0.66%), donor height (4.99%), cold ischemia time (5.33%). A sensitivity analysis coding missing entries as an absence of the risk factor was performed. Among the factors with the highest missing entry completion, such as cold ischemia time and donor-recipient height difference, none were significant in multivariable analysis.
Results
Study Characteristics
The sample included 150 603 transplant recipients. Recipients were placed into 3 time periods: 1987-1989 (2389 patients), 1990-1999 (28 083 patients), and 2000-2021 (120 131 patients). Mean hospital LOS was 17.9 days. The overall average LOS index of recipients decreased significantly over the 3 eras. In contrast, the average donor and recipient age increased significantly over time. The proportion of patients admitted to the ICU and on a ventilator decreased significantly across the 3 eras, while the proportion of patients on dialysis increased (
Demographic Characteristics of Adult Liver Transplant Recipients from 1987 to 2021.
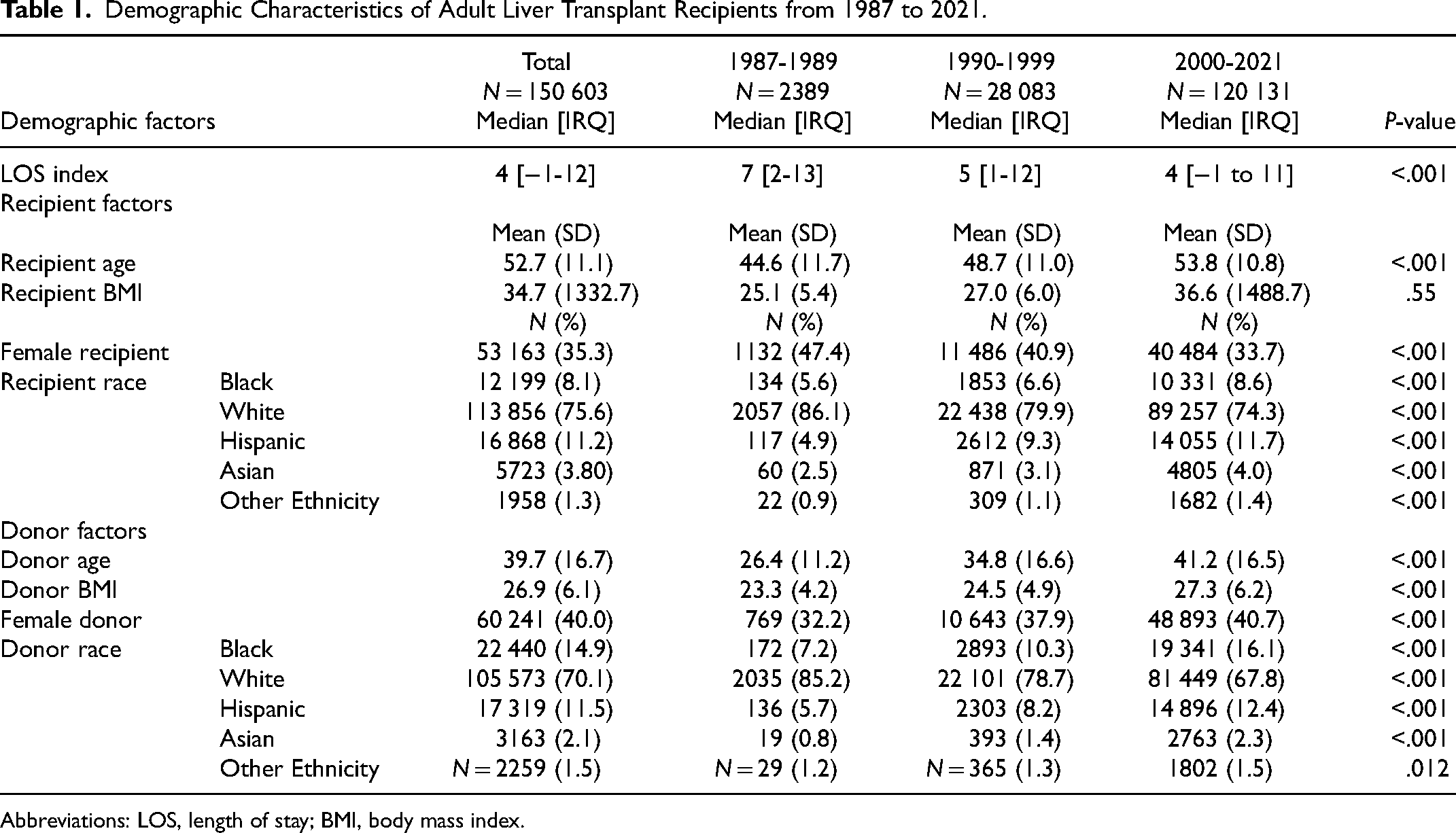
Abbreviations: LOS, length of stay; BMI, body mass index.
Data Entry Rate
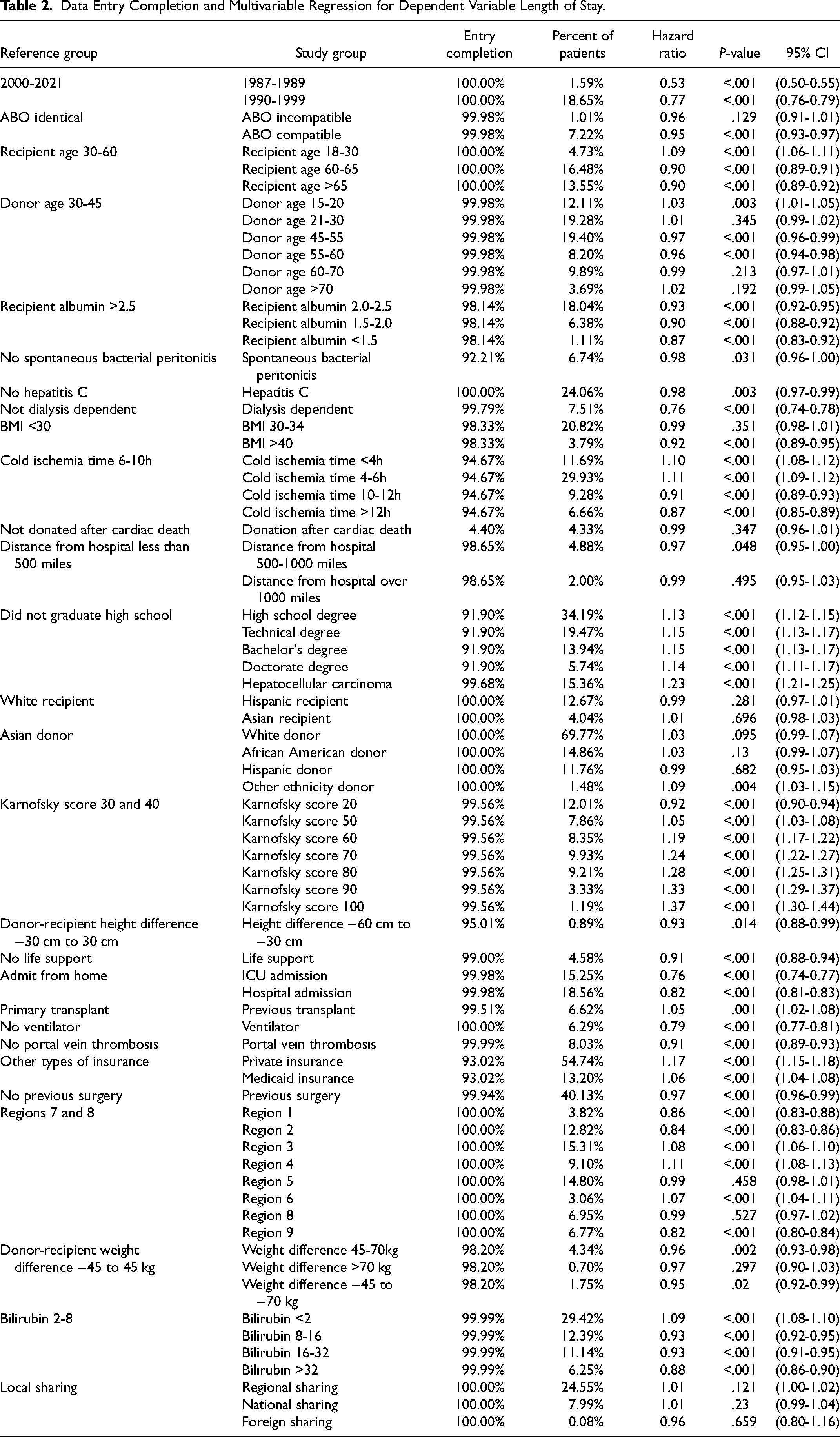
Data entry completion for variables is listed in
Data Entry Completion and Multivariable Regression for Dependent Variable Length of Stay.
Computation of Length of Stay Groups
Eras were delineated by joinpoints, which were generated by the Joinpoint Regression Program, Version 4.9.1.0. These time ranges are not equal in duration or sample size; they were selected based on a Poisson regression model, which identified statistically significant points at which the trends in LOS changed. The optimal number of joinpoints was determined using a Monte Carlo Permutation method for significance. The modeled annual percent change in mean LOS over time was found to be: −14.19 (CI: −18.3 to −9.9, P < .001) from 1987 to 1989, −6.01 (CI: −7.1-4.9, P < .001) from 1990 to 1999, and −0.74 (CI: −1.1 to 0.3, P = .001) from 2000 to 2021.
Mean Length of Stay
Among adult recipients, the average LOS following liver transplantation changed from 51.5 days in 1987 to 16.3 days in 2021, with a relatively steeper decline prior to 2000 (
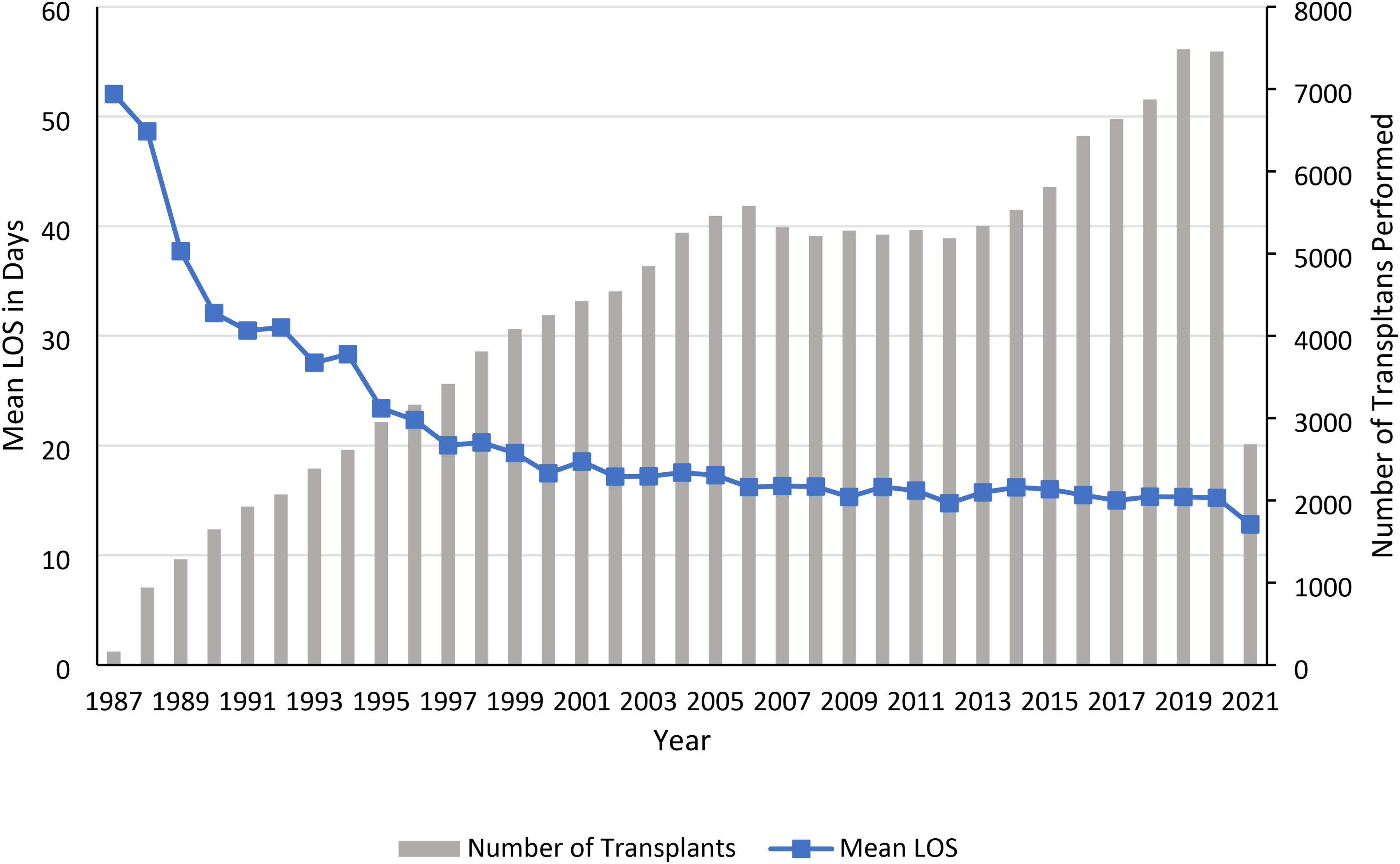
Mean length of stay and number of transplants in adults, 1987-2021.
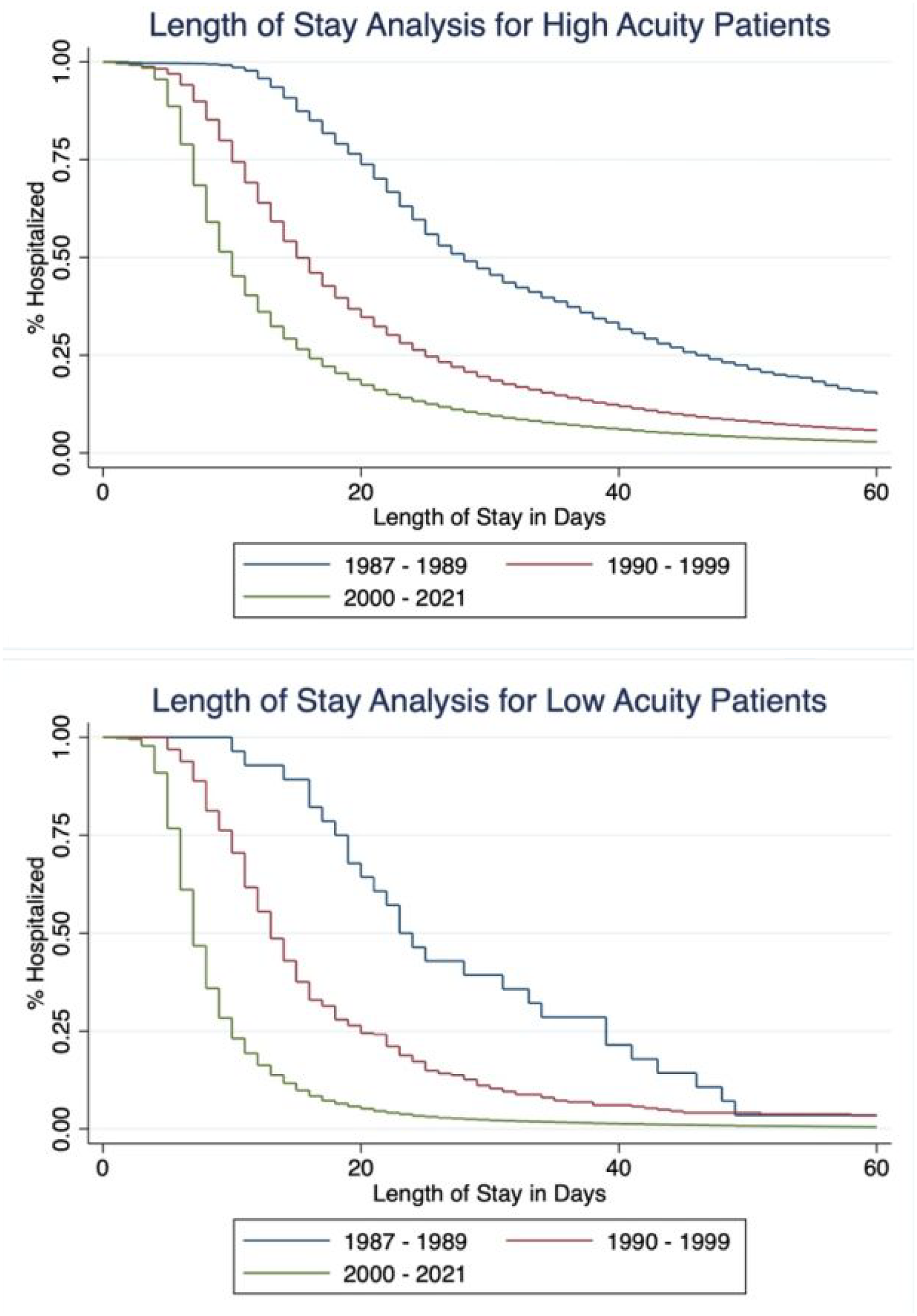
Differences in length of stay among high- and low-acuity patients. (A) LOS trends from 1987 to 2021 in high-acuity adults (>90th percentile in LOS index), (B) LOS trends from 1987 to 2021 in low-acuity adults (<10th percentile in LOS index). Abbreviation: LOS, length of stay.
In OPTN Region 9, a high transplant demand region, mean LOS decreased irregularly over time from 44.7 days in 1988 to 17.0 days in 2021. Transplant volume also fluctuated significantly, peaking in 2006 and 2020. In contrast, OPTN Region 3, a low transplant demand region, had a much steeper and smoother decline in mean LOS over time, from 79.7 days in 1987 to 11.8 days in 2021. In contrast to Region 9, Region 3 had a steady increase in the number of transplants performed over the last 4 decades. The abnormalities in transplant volume and mean LOS from 2020 to 2021 can be explained by incomplete data collection for 2021.
LOS Comparison Between Eras
Twenty-nine recipient, donor, and center-level factors were considered. Risk factors that were significant in univariate analysis (P < .05) were included in the multivariable Cox regression analysis, which controlled for 29 donor- and recipient-level characteristics. The risk factors that were included in multivariable analysis are presented in
Recipient, Donor, and Center-Level Risk Factors of Adult Liver Transplant Recipients from 1987 to 2021.
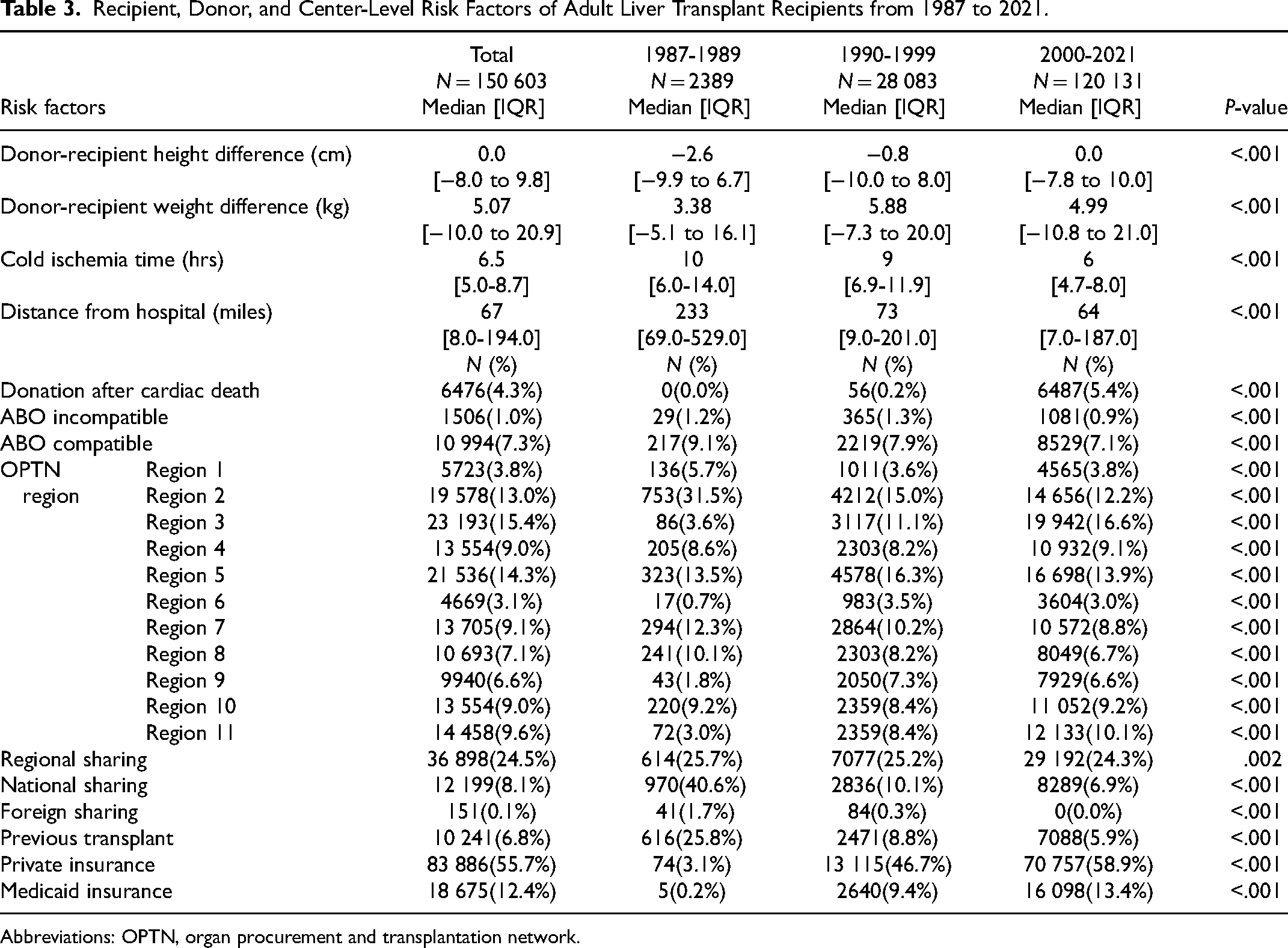
Abbreviations: OPTN, organ procurement and transplantation network.
In the multivariable Cox regression, recipients in both the 1987-1989 cohort (hazard ratio [HR]: 0.53, 95% confidence interval [CI]: 0.50-0.55) and the 1990-1999 cohort (HR: 0.77, CI: 0.76-0.79) had significantly prolonged lengths of stay (HR < 1 associated with later hospital discharge) compared to the 2000-2021 cohort. The most significant risk factors for prolonged hospital LOS were ICU admission (HR: 0.76, CI: 0.74-0.77), dialysis in the week prior to transplant (HR: 0.76, CI: 0.74-0.78), and being on ventilator (HR: 0.79, CI: 0.77-0.81). The most significant risk factor for shorter hospital LOS was increased functional status at transplant. Overall, recipients from Region 9, an area with high organ demand and relatively low supply, had significantly prolonged LOS (HR: 0.82, CI: 0.80-0.84), while recipients from Region 3, an area with low demand and relatively high supply, had a slightly shorter LOS (HR: 1.08, CI: 1.06-1.1).
Discussion
In providing a longitudinal view of LOS over the last 4 decades, this analysis demonstrated that the changes in LOS over time happened in the context of changes in the overall field of liver transplantation. There has been a great improvement in LOS from 1987 to 2021, with the greatest declines occurring mostly prior to 2000. Since the late 20th century, the field of liver transplantation has witnessed a huge expansion in the number of procedures performed, as well as an evolution in surgical and allocation techniques. For example, the method of preserving the inferior vena cava was popularized in the late 80s, while the Child-Turcotte-Pugh and MELD scores altered liver allocation methods.1,16 Thus, this pattern of decreasing LOS was supported by the transformative historical advances in the field prior to 2000 and furthermore reflects a maturation period of the field. Likewise, both low- and high-acuity recipients witnessed a decline in LOS over the last 4 decades along similar patterns, which was also expected given the advances in the field.
These declines in LOS among liver transplant recipients have been mirrored by similar reductions in LOS across various surgical fields and countries. For example, one study conducted in Denmark found that LOS following a cesarean section declined significantly from 4.0 days in 2004 to 2.4 days in 2016. 17 Likewise, another study conducted in the United States found that hospital LOS for total hip arthroplasty procedures decreased significantly from 3.8 days in 2006-2009 to 2.7 days in 2014-2016. 18 Within this context, the analysis illustrated the similarities in LOS trends over time between liver transplantation and other surgical procedures. The decreases in LOS over time have been much more dramatic in the field of liver transplantation.
In recent years, LOS has become an important outcome measure in clinical settings. 14 As a measure of the number of days that a patient stays in an inpatient healthcare facility, LOS can be used as a representative metric of healthcare resource utilization and costs.8,19 From an operational perspective, LOS also serves as a measure of patient flow through a healthcare system. 14 From a medical perspective, LOS has been used as a surrogate for a number of clinical outcomes, from hospital mortality to the health status of a patient.20,21 Because LOS is an important factor in both administrative efficiency and patient experience, it has become an increasingly significant outcome measure in clinical evaluations.
In the field of transplant surgery, limited resources and the significant cost of transplant procedures can place constraints on transplant centers, making LOS a particularly relevant outcome marker. 3 Because of the complex nature of the transplantation process, there were many factors that contributed to postoperative outcomes such as patient and graft survival.22,23 Recently, LOS has been used to predict healthcare expenditures and recipient survival following transplantation.3,8 Several studies have even identified certain patient and transplant factors that predicted a longer hospital LOS.13,24 Understanding the factors that contribute to a longer LOS can help healthcare providers identify best practices and factors to improve transplantation outcomes.
Region 9, a traditionally high-demand region, was associated with a longer LOS, while Region 3, a low-demand region, was associated with a shorter LOS. These findings align with current literature, which has found that high-demand regions have recipients with a higher average MELD score at transplant than low-demand regions with a less limited organ supply. 19 Likewise, several factors identified in this analysis have been previously shown in other literature to be significant for prolonged stay following liver transplant. Specifically, multiple studies have linked longer cold ischemia times with a longer LOS. 4 Previous literature found that patients admitted to the ICU were more likely to have longer hospital LOS, higher mortality, and increased complications. Recipients with an educational degree (high school, bachelor's, technical, or doctoral) had a shorter LOS compared to recipients who did not finish high school. This finding aligns with existing literature, since increased health literacy and education levels have been shown to have a positive impact on transplantation outcomes such as survival.4,25,26 Recipients with private insurance had shorter LOS compared to recipients with other forms of insurance. These findings are supported by previous evidence that private insurance is associated with better transplantation outcomes than public insurance. 27 Although existing literature has found differences in transplantation outcomes by race, this analysis found no significant relationship between donor or recipient race and LOS. 13
Prior to this study, there was no analysis that examined the long-term trends in LOS. This analysis aims to both illustrate trends in LOS over the last 4 decades and identify relevant recipient and donor characteristics associated with changes in LOS. These findings could be used in clinical practice to identify actionable factors to improve patient outcomes and hospital resource utilization. Future potential directions include identifying center-level characteristics associated with prolonged LOS and using a mixed methods qualitative study or a prospective study to further explore avenues for improving clinical practice in transplantation.
Although data entry is mandatory for all US transplant centers, all patient registries have variability in data entry, such as data entry errors or missing data, that may lead to inaccurate findings. Because this analysis was based on a large sample of patients, it is unlikely that small amounts of missing or erroneous data would have significantly impacted the findings. Imputation analysis was performed to correct for missing data. Another limitation of the study was that center-level characteristics could not be analyzed due to the nature of the database. Finally, because the current database only contained data up to July 2021, the values for 2021 may not be as robust compared to other years.
Conclusions
This analysis showed that there has been a statistically significant decrease in the mean LOS over time in adult recipients following liver transplantation, even after controlling for donor and recipient level factors. This study demonstrated the potential to identify actionable root cause factors to avoid prolonged LOS in clinical transplantation settings.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.