
Abstract
Introduction
Many studies of Black–White disparities in living donor kidney transplantation hypothesize that they were partially due to Black–White differences in candidate social network access to healthy, willing donors. This differential access hypothesis has not been tested using directly measured social network data.
Research Questions
Do black kidney transplant candidates have perceived lower social network access to health and/or willing living donors than white candidates?
Design
A cross-sectional survey that measured the social network members was collected in 2015. Black–White differences in patient counts of perceived healthy and/or willing potential donors in social networks, and individual network members’ probability of being perceived healthy and/or willing, were compared using logistic and negative binomial regression models.
Results
The survey included 66 kidney transplant candidates reporting on 1474 social network members at a large Southeastern US transplant center in 2015. Black and White patients had similar access to perceived healthy, likely potential donors (86% vs 87% had 1 or more, P = .92; 5.91 vs 4.13 mean counts, P = .20) and perceived healthy, agreed potential donors (56% vs 48%, P = .54; 1.77 vs 1.74, P = .97). Black patients’ network members were individually more likely to be perceived healthy and likely potential donors (26% vs 21%, P = .04), and White patients’ network members were more likely to have agreed (13% vs 9%, P = .03), but these differences were statistically insignificant in demographically adjusted models.
Conclusion
Black and White transplant candidates perceived access to similar numbers of potential donors in their social networks. This result does not support the differential access hypothesis.
Keywords
Introduction
Living donor kidney transplantation is often the optimal therapy for end-stage kidney disease, but relatively few transplant candidates obtain living donors. 1 This is especially true for non-Hispanic Black candidates, whose disparity in living donor rates compared to non-Hispanic Whites is the largest of all major racial/ethnic minoritized groups. 2 Because most living kidney donors are candidates’ family and friends, social network access to healthy, willing (ie, suitable) living donors is a potentially important barrier that may contribute to Black–White disparities.
Due to the broad impact of structural racism on so many aspects of social life, health, and kidney disease,3‐5 a commonly-offered hypothesis is that Black–White disparities may result from relative deficits of suitable potential living donors in Black candidates’ social networks, which we call the differential access hypothesis. This hypothesis has 2 key variations. One variation postulates that these disparities occur because Black candidates have fewer healthy social network members than White candidates (the differential health hypothesis).6‐13 Another variation postulates that racial disparities occur because Black candidates have fewer social network members willing to donate a kidney (the differential willingness hypothesis).6,9,14‐19 Both hypotheses are now factually cited in more recent literature, suggesting these hypotheses have become widely accepted.11,20 Although commonly postulated, the differential access hypothesis typically relies on generalizations from survey or simulation 21 data that may not apply straightforwardly to patients’ family and social networks.
This hypothesis was assessed at the candidate-level (Do Black transplant candidates have fewer perceived healthy, willing social network members than White transplant candidates?) and the network-member-level (Are Black transplant candidates’ social network members individually less likely to be perceived healthy and willing than White transplant candidates’ social network members?). This distinction is illustrated in Figure 1 . The answers to the 2 research questions imply different viewpoints on eradicating these disparities: if the network-member-level version was true but the candidate-level version was not, then both racial groups have equal access, but Black candidates may have greater difficulty identifying suitable donors; if the candidate-level version was also true, the disparity was less readily ameliorated.
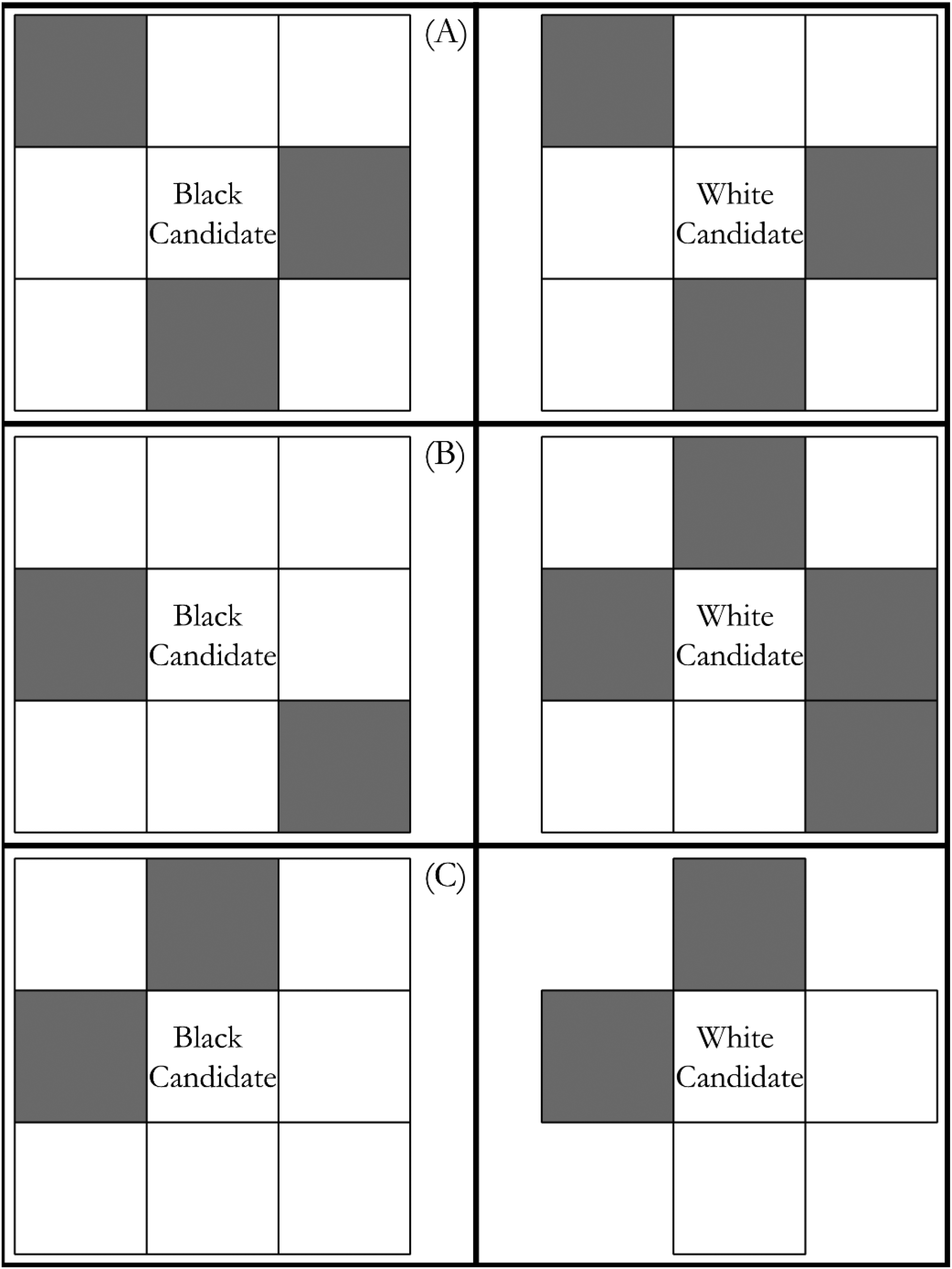
The differential access hypotheses, illustrated. Note: Each panel illustrates hypothetical, typical kidney transplant Black and White patient networks, where each connected box is a network member for the patient. Grey boxes represent suitable potential donors (whether defined as healthy, willing, or both). (A) A scenario with no differential access by race; the Black and White patients have equal numbers of suitable potential donors. (B) A candidate-level differential access scenario; the White patient has a larger number of suitable potential donors than the Black patient. (C) A scenario of network-member-level (but not candidate-level) differential access; the Black patient's network members have half the probability of suitability (25%) as the White patient's network members (50%), but the Black and White patients have equal numbers of suitable potential donors in their networks due to differential network size.
The candidate- and network-member-level versions of the differential health and differential willingness hypotheses were re-examined using candidate-reported social network data on a single-center sample of kidney transplant candidates. An egocentric social network approach was adopted in which kidney transplant candidates were surveyed about their own characteristics and those of their adult social network members. Although this measurement strategy was indirect, previous studies demonstrated that people can reliably report on the health of and relationships with their network members.22‐25 These data offer a new and necessary window into Black and White kidney transplant candidates’ social network access to suitable living donors regardless of living donation behaviors.
Methods
Design
The Ego Networks among Candidates for Transplant (ENaCT) study was a single-center, cross-sectional survey sample of 73 kidney transplant candidates collected in 2014-2015. In this survey, candidates reported on their own characteristics as well as those of their social network members, also known as an egocentric survey design. This study was approved by the university Institutional Review Board (protocol # X141121010).
Setting
Patients were recruited from a single large transplant center in southeastern United States. Surveys were completed in a conference room following a nurse-led early-phase candidate education session on kidney transplantation, including the process and benefits of kidney transplantation generally and living donor transplantation specifically. A researcher was always present to invite participation, provide informed consent, and answer questions. Non-participants were asked to leave the room before the surveys began, but respondents who wished to complete the survey with the help of a companion (eg, spouse or close family member) or research assistant were permitted to do so.
Population
The target population was early-phase US kidney transplant candidates. The accessible population was new transplant candidates at the transplant center. The ENaCT's racial/ethnic distribution was similar to new waiting list additions at the recruitment center in 2014-2015 (ENaCT 61% Black, 33% White, and 6% others; center 58% Black, 38% White, 4% others). However, it is noteworthy that the recruitment center somewhat overrepresented Black candidates and underrepresented Latino/a candidates compared to contemporaneous new waiting list additions in its UNOS region (47% Black, 36% White, 17% other) and in the United States (29% Black, 44% White, 27% other). The age distribution in ENaCT was somewhat less similar to the recruitment center's contemporaneous new waiting list additions, with patients age ≥ 65 overrepresented in ENaCT and patients 50 to 64 underrepresented (ENaCT 15% 18-34, 39% 35-49, 35% 50-64, 11% 65+; recruitment center 16% 18-34, 35% 35-49, 46% 50-64, 4% 65+). Furthermore, the recruitment center had a younger new waiting list addition age distribution than its UNOS region (12% 18-34, 28% 35-49, 40% 50-64, 17% 65+) or the United States (12% 18-34, 27% 35-49, 42% 50-64, 18% 65+).
Sampling
A non-probability, convenience sampling procedure was used to recruit kidney transplant candidates. Patients were eligible to participate if they were age ≥ 19 and could speak and read English and were compensated $10 each. Because the focus of this analysis was on Black–White differences in access to suitable potential living donors, the analytical sample was restricted to non-Hispanic White and non-Hispanic Black transplant candidates. Four Latino transplant candidate respondents (N = 69) were dropped. The analytical sample was further restricted to those with complete data on the 4 primary independent variables—race, gender, education, and age, dropping 3 additional respondents (N = 66).
Data Collection
The ENaCT survey consisted of 2 components. In the candidate survey component of this study, transplant candidates were asked about themselves. For instance, questions posed were demographic characteristics and views on transplant-related issues. Candidate race (non-Hispanic White vs non-Hispanic Black), age (19-50 vs 51+), sex (male vs female), and education (attended college vs did not attend college) were measured in this instrument. In the network member survey, transplant candidates were asked to describe all adult members of their family and friendship network. Following standard practice, 26 candidates first reported a list of network members in each relationship category. A series of network-member-specific questions were then asked about each network member, including network member age, sex, and relationship to candidate (parents, children, siblings, aunts/uncles, nieces/nephews, grandparents, grandchildren, cousins, other family, spouse/partner, or friend). Additionally, network member health was measured by candidate perception that the network member was healthy enough to donate a kidney (yes vs no or don’t know; hereinafter, healthy). Perceived network member likelihood to donate was measured by candidate perception that they would be evaluated for donation if asked (recoded to 1 if very likely, 0 if somewhat likely, not very likely, or don’t know; hereinafter, likely). Network member agreement to be evaluated was measured distinguishing network members who had discussed living donation and agreed to an evaluation versus those who have either not discussed or not agreed to evaluation (hereinafter, agreed). Healthy & likely network members were both healthy and likely in the sense defined above; healthy & agreed network members were both healthy and agreed in the sense defined above. Each of the 5 dependent variables (healthy, likely, agreed, healthy & likely, healthy & agreed) were modeled in both counts of network members meeting these criteria and whether the candidate had 1 + network members meeting these criteria. Missing values of these measures were addressed using multiple imputation because nonresponse rates on network member items were higher than for candidate items.
Data Analysis
The variables’ distribution at the candidate- and network-member-level for full and race-stratified samples were described. The candidate-level differential access hypothesis was assessed descriptively, summarizing White and Black transplant candidates’ access to suitable potential living donors measured both dichotomously and as counts. These comparisons were adjusted for candidate age, gender, and educational attainment, with effects presented as average marginal effects (changes in outcome probability. In these adjusted comparisons, logistic regression was used to analyze dichotomous dependent variables and negative binomial regression was used to analyze count dependent variables. Negative binomial regression was used because it was the best fitting count model of the 4 models tested (see Supplemental Table 1 ). The network-member-level differential access hypothesis was assessed descriptively, comparing the proportion of White and Black candidates’ network members deemed: (a) healthy, (b) likely, (c) agreed, (d) healthy & likely, or (e) healthy & agreed. The network-member-level differential access hypothesis was assessed with race comparisons adjusted for candidate age, gender, education, the network member's relationship type to the candidate, network member age, and network member gender, using candidate-clustered standard errors to adjust for observations’ non-independence.
Procedure
Kidney transplant patients were asked to complete a survey describing themselves and the members of their social networks.
Results
Sample Characteristics
The top half of Table 1 describes the transplant candidates’ characteristics in the unimputed analytical sample. Sixty-five percent were Black and 35% were White. Forty-six percent of the sample were aged 51 or older. Sixty-two percent of the sample were female. A plurality of respondents (56%) attended college.
Descriptive Statistics, ENaCT Study.
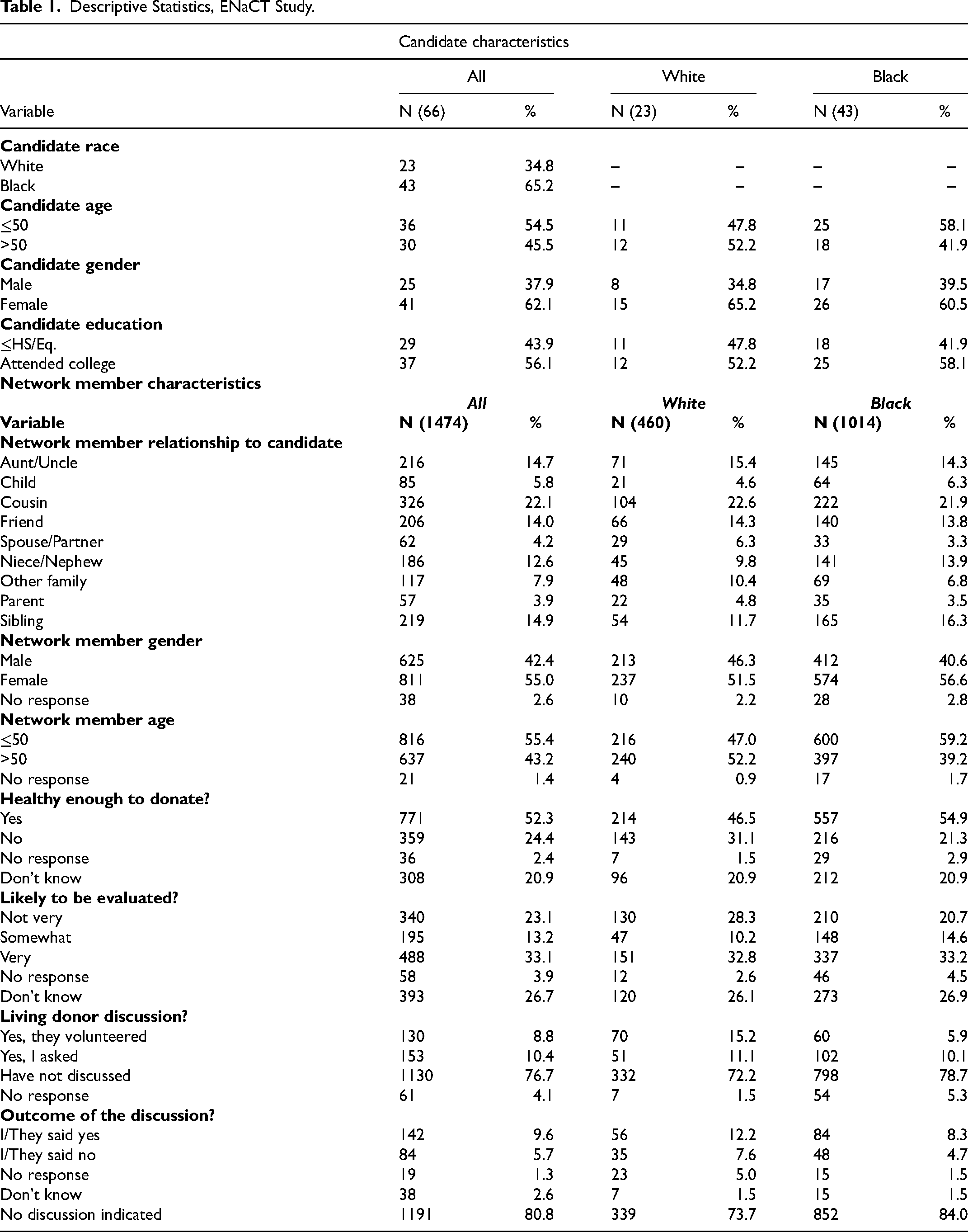
The majority (58.1%) of non-Hispanic Black candidates are under the age of 50 compared to 47.8% of non-Hispanic White candidates. Sixty-five percent of White candidates and 60.5% of Black candidates are female, and 52.2% of White candidates have attended college compared to 58.1% of Black candidates.
The bottom half of Table 1 describes the living donor-related characteristic distribution of ENaCT candidate-network member pairs. This table shows the unimputed distributions for network member characteristics to aid the reader in understanding how these data were recoded and imputed. Network member non-response rates were <5% for all items.
Transplant candidates reported on a wide variety of network ties, with cousins, siblings, aunts/uncles, friends, and nieces/nephews among the most numerous, while spouses/partners and parents were among the least numerous. A majority of reported network members were female (55%) and age 50 or younger (55%). Transplant candidates believed that a majority of their network members were healthy (52%), though they did not know for a significant minority (21%). Just 33% of network members were very likely to be evaluated for donation, 13% somewhat likely, and 23% as not very likely, with 27% receiving don’t know responses. Nineteen percent of candidate-network member pairs reported living donor discussions (10% candidate-initiated discussions, 9% donor-initiated discussions), while 77% of all candidate-network-member pairs had not discussed living donation. More of these discussions resulted in no agreement (9.6% of all pairs) than agreed outcomes (5.7%).
Transplant candidates’ social network characteristics varied by race. Black candidates reported more siblings, nieces/nephews, and children than White candidates, while White candidates reported more aunts/uncles, cousins, friends, spouse/partners, other family, and parents than Black candidates. Fifty-two percent of White candidates’ network members are over the age of 50 compared to 39.2% of Black candidates’ network members. Fifty-five percent of Black candidates’ network members were rated “healthy” compared to 46.5% of White candidates’ network members, but similar percentages are rated “likely.” The majority of both White and Black network members had not discussed living donation, but White candidates had more network members volunteers (15.2%). White candidates had 12.2% of network members who agreed, compared to 8.3% for Black candidates. Finally, the distribution of reported social network ties was similar for White (mean = 20.0, median = 23, SD = 9.9, range = [3,37]) and Black (mean = 23.6, median = 22, SD = 9.6, range = [4,51]) candidates.
Testing the Candidate-Level Hypotheses
Unadjusted Estimates
Figure 2 presents the descriptive tests of the differential access hypothesis, and the top half of Supplemental Table 2 presents the underlying numbers. The left-hand side of Figure 2 depicts the probability that Black or White transplant candidates had at least 1 suitable potential living donor, variously defined as described above. This demonstrated that, across 5 indicators of access to ≥1 suitable donors, there were no statistically significant Black–White differences. Comparable proportions of Black and White transplant candidates reported that they had at least 1 healthy (96% for Whites, 100% for Blacks), likely (96%, 88%), agreed (65%, 56%), healthy & likely (87%, 86%), or healthy & agreed (48%, 56%) network member.
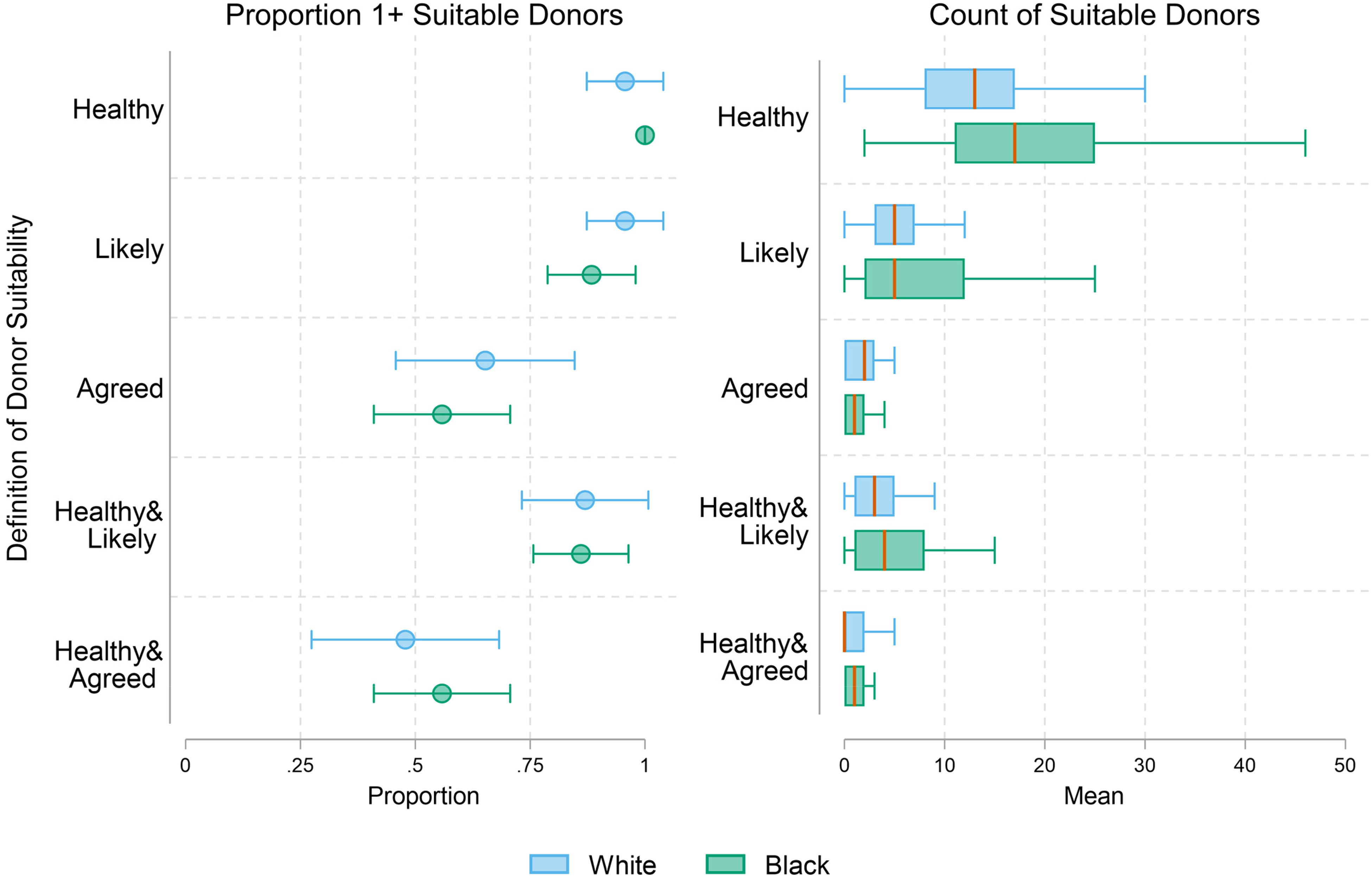
Access to suitable living kidney donors by race in ENaCT. Note: No race differences were statistically significant (using logistic regression models for 1 + suitable donors and negative binomial regression models for count of suitable donors, each specified with no controls). N = 66 kidney transplant candidates (23 non-Hispanic White, 43 non-Hispanic Black).
The right-hand side of Figure 2 presents box-plots of the number of suitable potential living donors in Black and White candidates’ networks. This shows that Black and White candidates’ suitable potential living donor count distributions were either comparable or indicate Black candidates had higher typical counts.
Demographically Adjusted Estimates
Table 2 presents the demographically adjusted analysis of Black–White differences in candidate-level suitable potential living donor access. As with the unadjusted estimates in Figure 2 , no statistically significant race differences were found. In contrast, compared to female candidates, male candidates had a 0.29 lower probability of access to one or more healthy & agreed donors (P = .032), and 1.5 fewer healthy & agreed donors on average (P = .009). Supplemental Table 3 presents the results of these same tests for the healthy, likely, and agreed measures, where the findings were substantively identical Black–White differences in access to suitable potential living donors were never statistically significant.
Multivariate Analyses of Access to Suitable Living Donors.
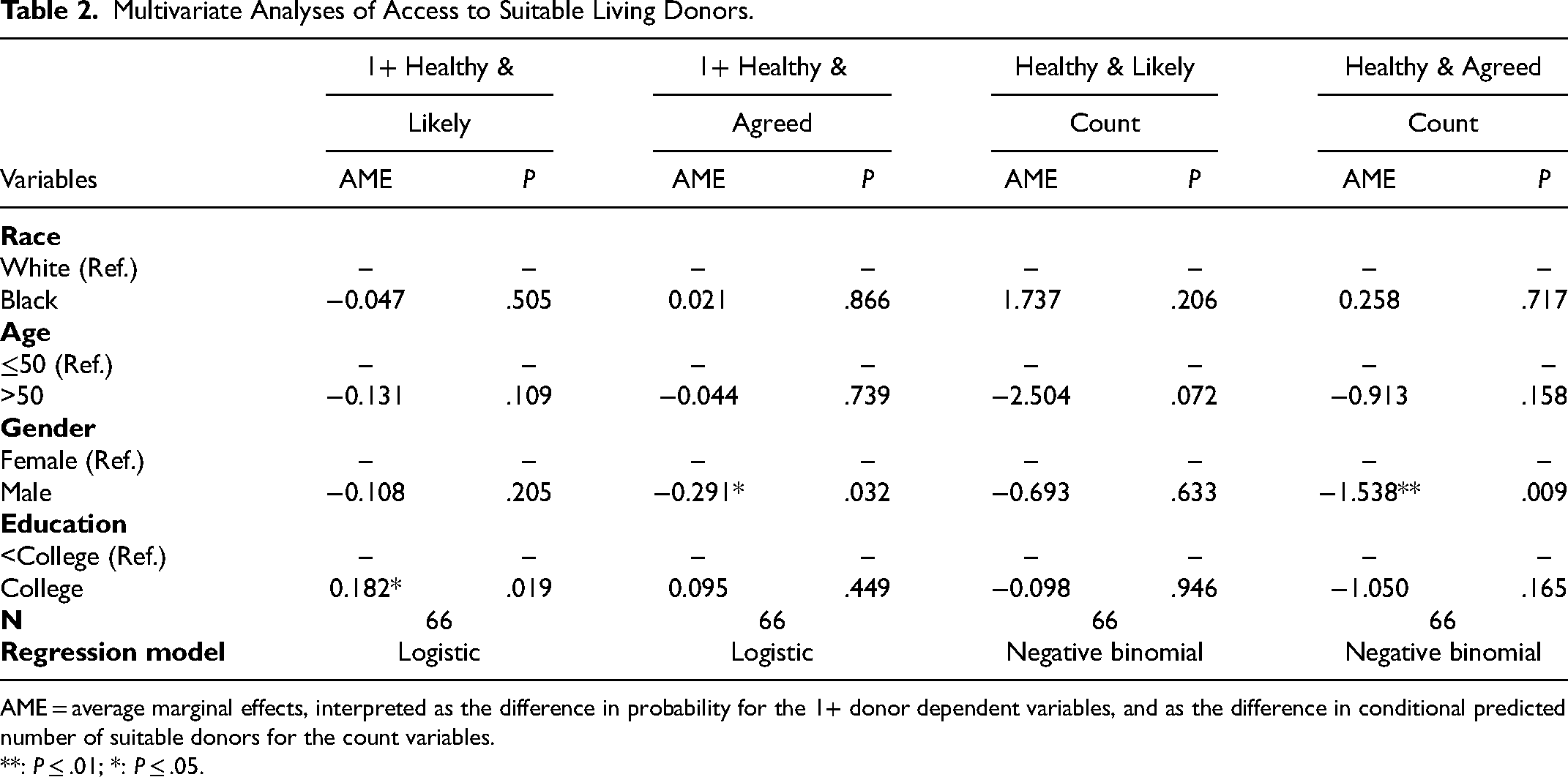
AME = average marginal effects, interpreted as the difference in probability for the 1+ donor dependent variables, and as the difference in conditional predicted number of suitable donors for the count variables.
**: P ≤ .01; *: P ≤ .05.
Testing the Network-Member-Level Hypotheses
Unadjusted Estimates
Figure 3 presents the proportion of Black and White candidates’ network members rated to be healthy, likely, agreed, healthy & likely, and healthy & agreed. Unlike Figure 2 tests of the candidate-level differential hypothesis, this figure shows results of the network-member-level tests and finds 3 statistically significant Black–White differences in these assessments: (a) Black candidates (57%; see bottom half of Supplemental Table 2 ) were statistically significantly more likely than White candidates (47%) to rate each network member as healthy; (b) White candidates (13%) were statistically significantly more likely than Black candidates (9%) to rate each network member as agreed; and (c) Black candidates (26%) were statistically significantly more likely than White candidates (21%) to rate their network member as healthy & likely.
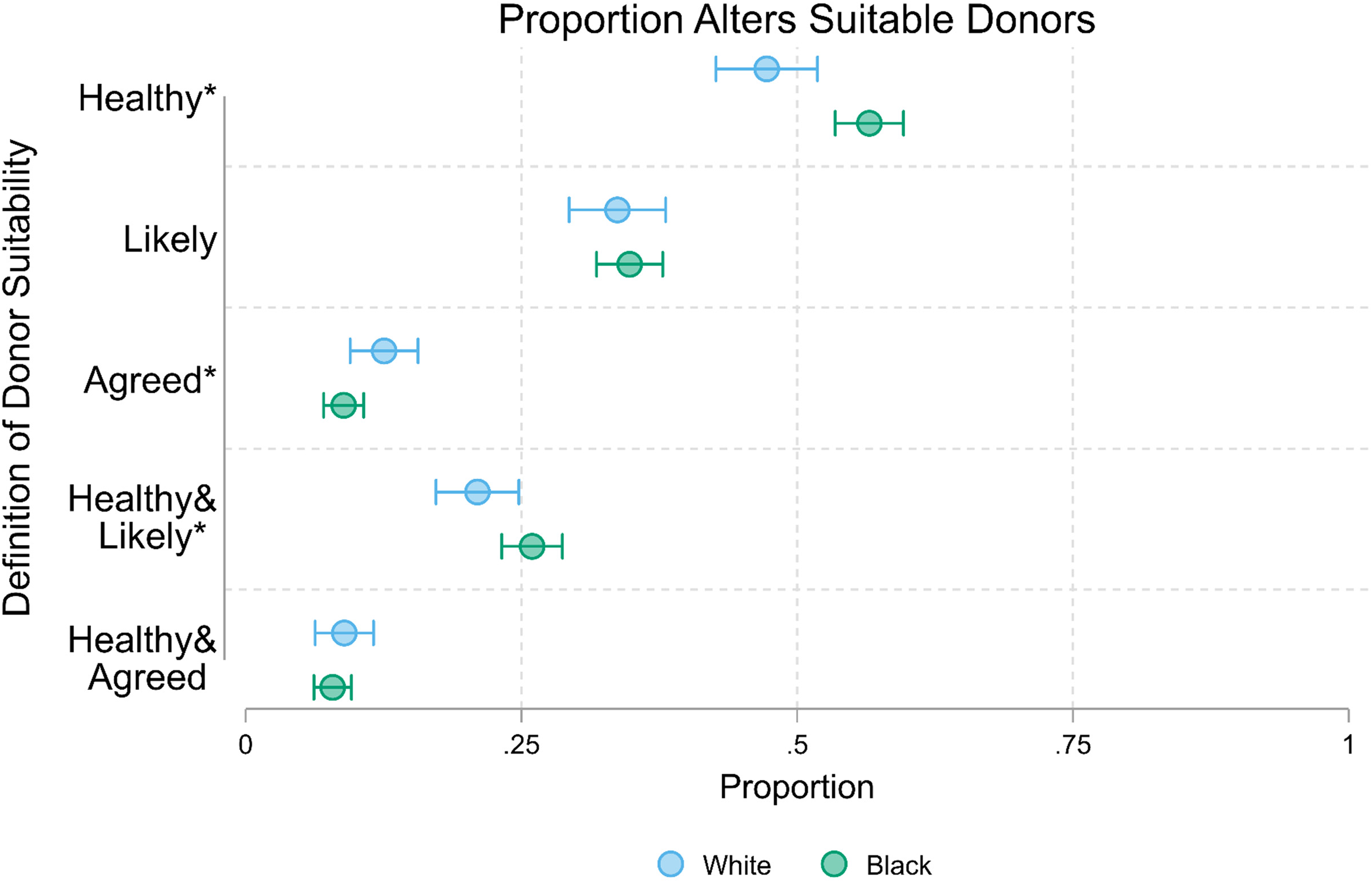
Proportion network members suitable living kidney donors by race in ENaCT. Note: *: Black–White difference in 2-group proportion test statistically significant at P ≤ .05.
Regression-Adjusted Estimates
Table 3 tests the network-member-level differential access hypotheses, adjusted for candidate and network member demographic characteristics. These results did not support the differential access hypotheses for any of the 5 measures of potential donor suitability, as no Black–White differences were substantively or statistically significant with demographic controls.
Multivariable Analyses of Network Member Living Donor Suitability.
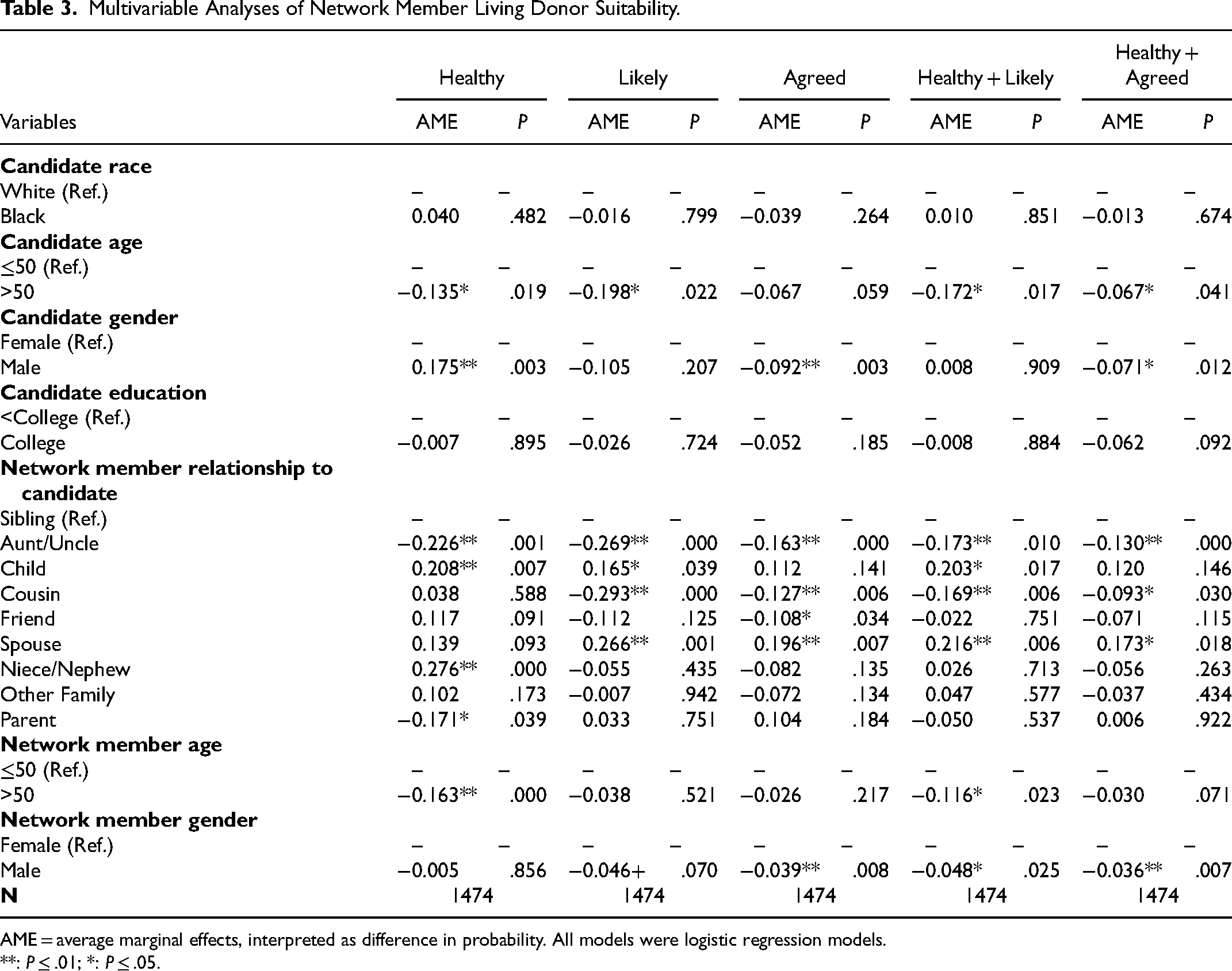
AME = average marginal effects, interpreted as difference in probability. All models were logistic regression models.
**: P ≤ .01; *: P ≤ .05.
Robustness Checks
Additional results demonstrated the robustness of these findings and are available upon request. When candidate-level analyses were reproduced using only nuclear family social network ties (parents, siblings, spouses/partners, and children) since these are the most common living donors, no statistically significant Black–White differences were observed. Similarly, when network member-level analyses were reproduced using only nuclear family social network ties, White candidates’ network members were still agreed at higher rates than Black candidates’ network members (28% vs 18%, P = .018). However, unlike the primary results, there were no statistically significant differences in other measures. In other robustness check analyses, candidate income was substituted for candidate education as a measure of socioeconomic status. As in the primary analyses, there was no evidence for the differential access hypothesis.
Discussion
Arguments for the differential access hypotheses currently rely on multiple plausible but previously untested extrapolations from limited clinical and population health evidence. First, the differential health hypothesis was based on researchers’ frequent extrapolation from population-level racial/ethnic health disparities to disparities in transplant candidate network members’ health.6,8,9 Relatedly, many researchers extrapolate from clinical studies showing higher rates of potential donor health-related disqualification for Black patients than White patients7,10‐13 to generalizations about their full social networks regardless of living donor evaluation. This evidence was inconsistent with this claim, showing instead that Black candidates’ network members were perceived as healthy at higher rates than White candidates’ network members. This finding suggests that differential selectivity into living donor evaluations is a plausible alternative interpretation of these clinical findings, 11 suggesting that interventions promoting healthiest network member evaluations may ameliorate racial/ethnic living donor disparities.
The differential willingness hypothesis was based on a similar extrapolation from population- or patient-level differences in medical institutional trust or kidney transplant knowledge to Black transplant candidates’ network members being less willing to become a living kidney donor.15‐19 The evidence did not support this conclusion either, as Black candidates reported similar rates of access to likely and agreed donors at the candidate-level. Although this hypothesis was partially supported by White candidates’ higher agreed rate at the network-member-level, this difference was not statistically significant in demographically adjusted models. This finding suggests that there are no Black–White differences in candidate-reported willingness to donate among otherwise similar network members.
Instead, these findings suggest that Black–White disparities may be explained by differences in other previously documented barriers to living donor transplantation, such as the rate and determinants of completed living kidney donor evaluation and donation. One possible interpretation is that White candidates’ suitable potential living donors may also be more likely to be evaluated than Black candidates’ suitable potential living donors, perhaps due to differences in their ability to afford lost wages, living donor evaluation indirect costs, travel to transplant clinics, or dependent care during recovery.27,28 Racial differences in each of these key determinants of living kidney donation emphasize the potentially broad role of structural racism in Black–White disparities. This interpretation also suggests that the living kidney donor support provisions of the Advancing American Kidney Health executive order may ameliorate racial/ethnic living kidney donor disparities, though survey evidence suggested this may not be the case. 29 Future research should measure candidate family and friendship networks to assess these hypotheses prospectively, linked to clinical data on potential donor evaluations and outcomes.
Other factors may explain these findings. First and most importantly, transplant candidates’ perceptions of network members’ health were likely measured with some error. However, egocentric reporting such as this study's has been shown to be accurate in reporting many health statuses and behaviors such as HIV positive status, 22 abortion, 24 multiple sex partners, 24 and adolescent smoking. 23 Nonetheless, measurement error could bias these comparisons if its degree differed by race in this sample, which is plausible due to Black–White differences in access to diagnostic medical care. 30 However, this is not the most likely explanation for these results for 2 reasons. For one, transplant candidates participating in ENaCT did so immediately following a presentation about living donor benefits and medical contraindications, so these participants’ contraindication knowledge likely exceeded the general population's. Furthermore, these findings accord with previous simulation work linking national data on kinship structures, contraindication probabilities, and ABO and HLA distributions by race to assess the differential access hypothesis. 21 Although this simulation study and the present study both have limitations, their convergent conclusions suggest that this finding is likely to be robust.
Second, transplant candidates’ reports on network members’ willingness to donate may also have been measured with error that could bias comparisons. Although previous research has shown that both sides of network pairs could reliably report relational characteristics such as sexual and drug-sharing histories as well as the existence of social ties, 25 whether patients’ perceptions of network members’ willingness to donate a kidney was equally reliable merits future investigation. Regardless, it is possible that candidates’ perceptions of network members’ willingness to donate may be just as consequential as network members’ self-reported willingness, since candidates’ perceptions could structure with whom they initiate living donor discussions. Future research should compare transplant candidate network data with health and willingness measures directly reported by network members to extend these findings.
Third, the characteristics measured for each network member were limited to avoid overly burdening respondents. Future research should gather more information about network members to understand their barriers to living kidney donation.
Fourth, the ENaCT sample’s candidate racial/ethnic and age distributions were similar but not identical to those of the recruitment center, and the center's demographics did not exactly match those of its UNOS region or the United States at the time. We argue it is reasonable to generalize this study's findings to non-Hispanic White and Black patients in the southeast United States, but these findings’ national generalizability warrants further investigation.
Conclusion
This study was the first attempt to comprehensively assess the candidate- and network-member-level differential access hypotheses using data on transplant candidates’ directly measured social networks rather than the smaller, selective subset of network members who were evaluated for kidney donation. The patient-level differential access hypothesis received no support in this analysis; Black candidates had access to suitable potential living donors at highly similar rates as White candidates across a variety of metrics. In contrast, the network-member-level differential access hypothesis did receive some support, as White candidates’ network members have agreed to medical living kidney donation evaluation at higher rates than Black candidates’ network members. This finding was counterbalanced by findings that Black candidates’ network members were perceived to be healthy and healthy & likely at higher rates than White candidates’ network members. Furthermore, no network-member-level Black–White differences in potential donor suitability were statistically significant in demographically adjusted models.
Black and White transplant candidates’ descriptions of their social networks’ structure and characteristics did not systematically differ in indicators of access to healthy, willing donors. These findings were inconsistent with either version of the differential access hypothesis.
Supplemental Material
sj-docx-1-pit-10.1177_15269248231164174 - Supplemental material for Testing the Differential Access Hypothesis That Black Kidney Transplant Candidates Perceive Social Network Access to Fewer Potential Living Donors Than White Candidates
Supplemental material, sj-docx-1-pit-10.1177_15269248231164174 for Testing the Differential Access Hypothesis That Black Kidney Transplant Candidates Perceive Social Network Access to Fewer Potential Living Donors Than White Candidates by Jonathan Daw, Mary Roberts, Avrum Gillespie, Ashton M. Verdery and Tanjala S. Purnell in Progress in Transplantation
Supplemental Material
sj-docx-2-pit-10.1177_15269248231164174 - Supplemental material for Testing the Differential Access Hypothesis That Black Kidney Transplant Candidates Perceive Social Network Access to Fewer Potential Living Donors Than White Candidates
Supplemental material, sj-docx-2-pit-10.1177_15269248231164174 for Testing the Differential Access Hypothesis That Black Kidney Transplant Candidates Perceive Social Network Access to Fewer Potential Living Donors Than White Candidates by Jonathan Daw, Mary Roberts, Avrum Gillespie, Ashton M. Verdery and Tanjala S. Purnell in Progress in Transplantation
Supplemental Material
sj-docx-3-pit-10.1177_15269248231164174 - Supplemental material for Testing the Differential Access Hypothesis That Black Kidney Transplant Candidates Perceive Social Network Access to Fewer Potential Living Donors Than White Candidates
Supplemental material, sj-docx-3-pit-10.1177_15269248231164174 for Testing the Differential Access Hypothesis That Black Kidney Transplant Candidates Perceive Social Network Access to Fewer Potential Living Donors Than White Candidates by Jonathan Daw, Mary Roberts, Avrum Gillespie, Ashton M. Verdery and Tanjala S. Purnell in Progress in Transplantation
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIDDK grant R01DK114888 and the University of Alabama at Birmingham Comprehensive Transplant Institute, the Penn State Social Science Research Institute, and the Population Research Institute at Penn State University, which is supported by an infrastructure grant by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2CHD041025).
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.