
Abstract

Introduction
Lung transplant recipients have a high risk for invasive fungal infections. This is due to the allograft being directly exposed to environmental fungi with lung and airway defenses impaired. High levels of immunosuppression also places patient at risk. 1
A 64-year-old, who underwent bilateral lung transplant in March 2021 due to interstitial lung disease, presented with severe lung infection. The patient gave permission for the case to be written for publication.
Presenting Concern
In February 2023, during a routine followup, the patient reported a month long complaint of asthenia, hyporexia, generalized pain and low-grade fever. This case was complex as there were multiple resections done after transplantation for size discordance between lungs and thorax cavity, leaving the patient with reduced lung capacity.
Clinical Findings
Chest computed tomography (CT) scan, showed a 9 mm rounded nodule in left lower lobe
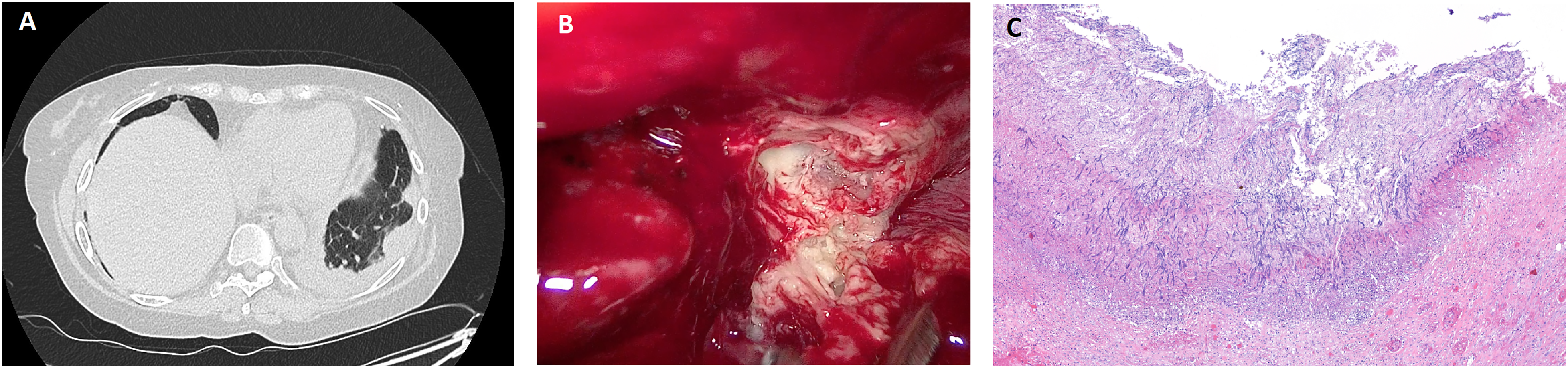
Patient computed tomography, image from video-assisted thoracoscopic surgery (VATS), and biopsy from nodule. (A) Chest CT scan showing nodular thickening of the left basal pleura with tumor-like appearance. (B) Image of VATS decortication showing nodularities with caseum inside. (C) Histology of left lower lobe nodule showing abundant fungal infiltration by filamentous fungi.
Outcome
Patient was clinically stable despite all the events. Good clinical, analytical, and radiological evolution was observed after surgery and after another couple of weeks of two intravenous antifungal therapies, the patient was switched to oral therapy with isavuconazole for 3 more months after hospital discharge.
Discussion
Invasive pulmonary aspergillosis is the most severe form of the spectrum of diseases caused by fungi of genus Aspergillus and one of the main death causes in immunosuppressed patients, such as lung transplant recipients. Broad spectrum of clinical features involving upper and lower respiratory tract are the most common presentations since it is generally the main gateway to the rest of the organism. Pleural involvement is an atypical manifestation and presented without any signs of parenchymal involvement is extremely rare. After a literature review, only 1 case report was found. 2
Neoplasms, granulomatous inflammatory diseases, and other opportunistic infections should be considered in differential diagnosis. Sometimes, biopsy specimens must be obtained to establish definitive diagnosis of invasive pulmonary aspergillosis. This report shows necrotizing and purulent inflammation with vascular invasion of small caliber arteries by septate hyphae. The microbiological differential diagnosis should be carried out with other filamentous fungi (Fusarium, Mucor, etc). Approximately 50% of patients present therapeutic failure with first-line drugs (voriconazole, isavuconazole and liposomal amphotericin B), so current trend is to use combination therapy with an echinocandin for its synergistic effect. 3
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.