
Abstract
Introduction
Organ transplantation is administratively complex and involves multiple stakeholders. The perioperative period alone involves donor and recipient coordination and several care teams. The operation is performed in time-sensitive conditions. These circumstances heighten the medico-legal risk for physicians, increasing susceptibility to malpractice claims. 1 Yet, suits against medical centers and surgeons only comprise a portion of total litigation. For instance, new organ allocation policies implemented by the Organ Procurement and Transplantation Network (OPTN) have led to action against several non-medical entities. 2 Unfortunately, there is little literature that characterizes the legal landscape of transplantation comprehensively and cohesively. Even less literature outlines which parties are susceptible to involvement in a suit that progresses to court.
Few malpractice cases go to trial. 3 Often, claims were dismissed as frivolous or lacking merit. 4 When tort was more obvious, those implicated in the lawsuit were often interested in settling out of court. This process may take 2-3 years to resolve and was associated with greater settlement awards, 5 notwithstanding the emotional impact on those involved. 6 Agreeing to settlement during pre-trial motions may not always be in defendants’ best interest. 7 Even when proof of strong medical negligence exists, physicians have been found to receive a favorable verdict in half of these trials. 4 It is unclear how well these findings translated to transplant surgery. Similarly, even a robust description of medical malpractice in the field would only be relevant to some stakeholders.
This study aimed to fill knowledge gaps by analyzing court proceedings involving kidney, heart, liver, lung, and pancreas transplantation. These cases included an analysis of outcomes from trials and pre-trial motions. This study also sought to characterize common case themes and defendant types. This analysis offers a comprehensive overview of the current medico-legal landscape in solid organ transplantation.
Methods
Design
This study was a retrospective analysis of court cases related to organ transplantation occurring in the US state and federal courts from 2000 to 2019.
Setting
This study was conducted by accessing The Caselaw Access Project (CAP). CAP is an online repository of published US court decisions maintained by the Harvard Law School Library.
Sampling
The search query on CAP was performed using the keywords: liver, kidney, pancreas, heart, lung and transplant. This yielded 2053 court files. Cases were included if they directly pertained to organ allocation, transplantation, or transplant-related services. Cases were excluded if they did not meet these criteria, or if they were appeals without impact on outcomes, including evidence admission or witness testimony.
Data Collection
Four main litigation themes were identified with associated subcategories: Policy, Discrimination, Poor or Unsuccessful Outcomes, and Other. Policy allegations encompassed insurance coverage disputes, disability benefits, and worker's compensation for transplant-related costs. Discrimination involved denied access to transplant-evaluation/transplantation due to incarceration and claims against employers of discriminatory firing or hiring based on transplant history or living donation. Poor or unsuccessful outcomes included malpractice, donor-derived malignancy or infection, and other errors leading to injury or compromise of the graft itself. The other category included various litigation grounds without a unifying theme. These topics ranged from allegations of sub-potent or counterfeit medications against pharmaceutical entities to foreign individuals seeking asylum for organ transplantation access.
Cases were organized by defendant type. This included transplant surgeons, medical centers, governmental organizations, pharmaceutical entities, insurance companies, employers, or a combination thereof. Defendants were placed in one category.
Data Analysis
Percentages were used to gain statistical insight into the frequency of recurring themes, verdict outcomes, and differences across defendant outcomes in different transplant cases.
Procedure
From May to September 2022, professors, post-doctoral researchers, graduate, and medical students examined court materials to determine each suit's relevance to organ transplantation. Cases were organized into themes by senior reviewers. At least 2 senior team members independently reviewed to ensure inter-rater reliability. Periodic meetings were held to reconcile discrepancies and clarify details. Ultimately, 164 cases had organ transplantation as a central element.
The outcome of cases was evaluated. These ranged from pre-trial motions – including granting summary judgment to a party that provided a verdict without advancing to trial – to reviewing appeals with eventual resolution.
Results
One hundred-sixty-four cases met inclusion criteria. Across all organ types, policy coverage was the most common recurring theme (N = 55, 33.5%). Next was poor outcomes (N = 51, 31.1%), discrimination cases against prison systems and employers (N = 37, 22.6%), and the other category (N = 21, 12.8%). Not all briefs reached a verdict. Occasionally, suits were remanded to lower courts for ongoing trial. In others, no clear outcome occurred. In cases with discoverable final verdicts, defendants involved in discrimination trials won most often (N = 29, 90.6%). Those implicated in policy suits won 65.3% (N = 32) of cases. Cases related to poor outcomes won 62.2% (N = 28) of the time. The other category won 70% of cases (N = 14). Lastly, a recurring claim against medical centers and transplant surgeons was lack of informed consent (N = 23, 45.1%).
Kidney
Of the 563 court proceedings obtained, 89 were included (
Summary of Overarching Case Categories Represented as Percentage of Each Organ Type.*
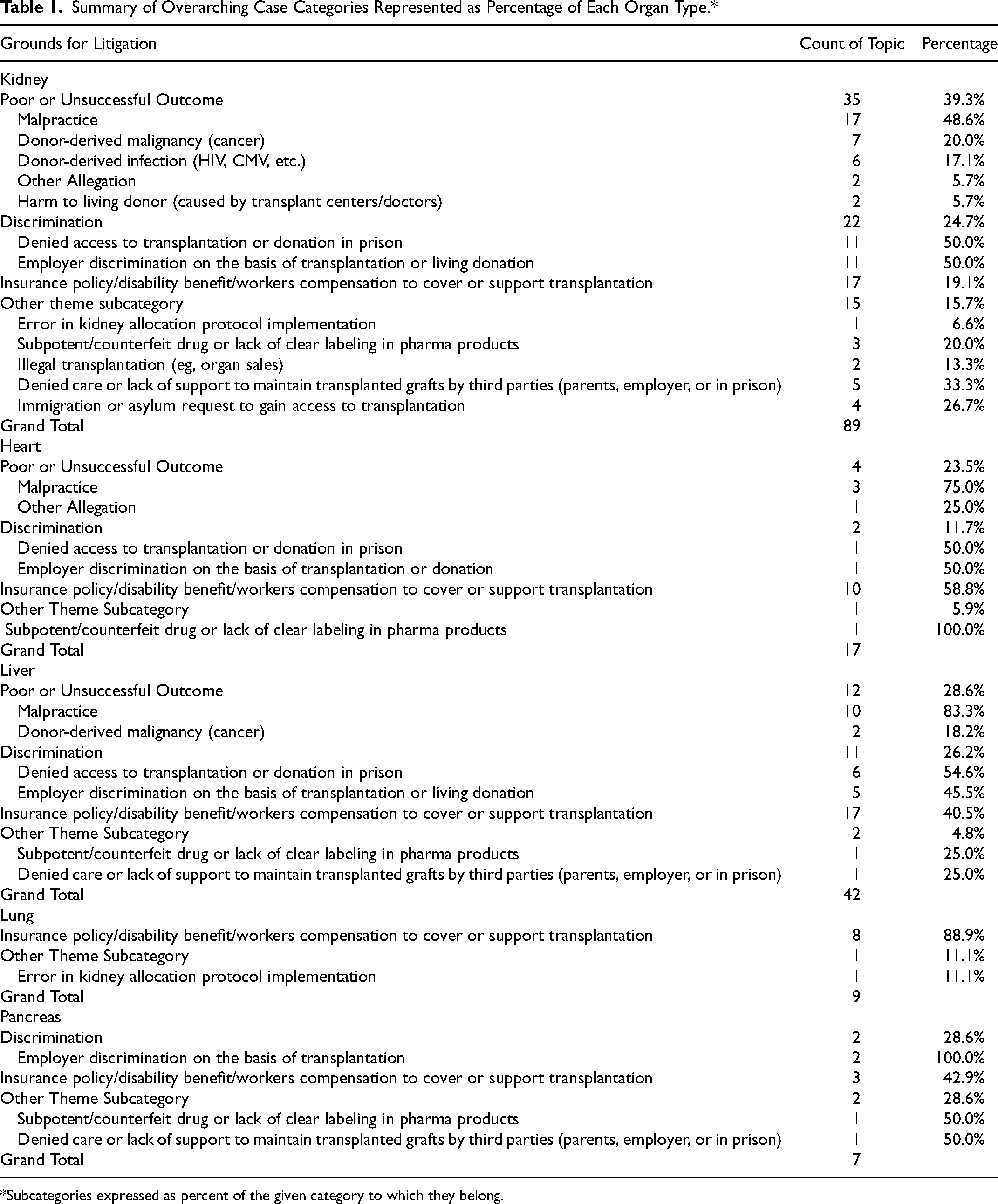
Subcategories expressed as percent of the given category to which they belong.
Referring to main defendant types, transplant surgeons were sued in 15.7% (N = 14) of proceedings while hospitals/transplant centers were implicated in 23.6% (N = 21). Policy dispute cases involved insurance companies most commonly (N = 9, 10.1%), then employers involved in coverage disputes (N = 6, 6.7%), and lastly governmental agencies (Federal Bureau of Prisons/Social Security Administration) (N = 2, 2.3%). Prison systems were involved in most discrimination lawsuits (N = 11, 12.4%). Eight employers were defendants (9%)
A final verdict was discoverable in 80 of 89 total cases related to kidney transplantation (89.9%) (
Final Outcome for Defendants Grouped by Dispute Type in Each Organ Type.*
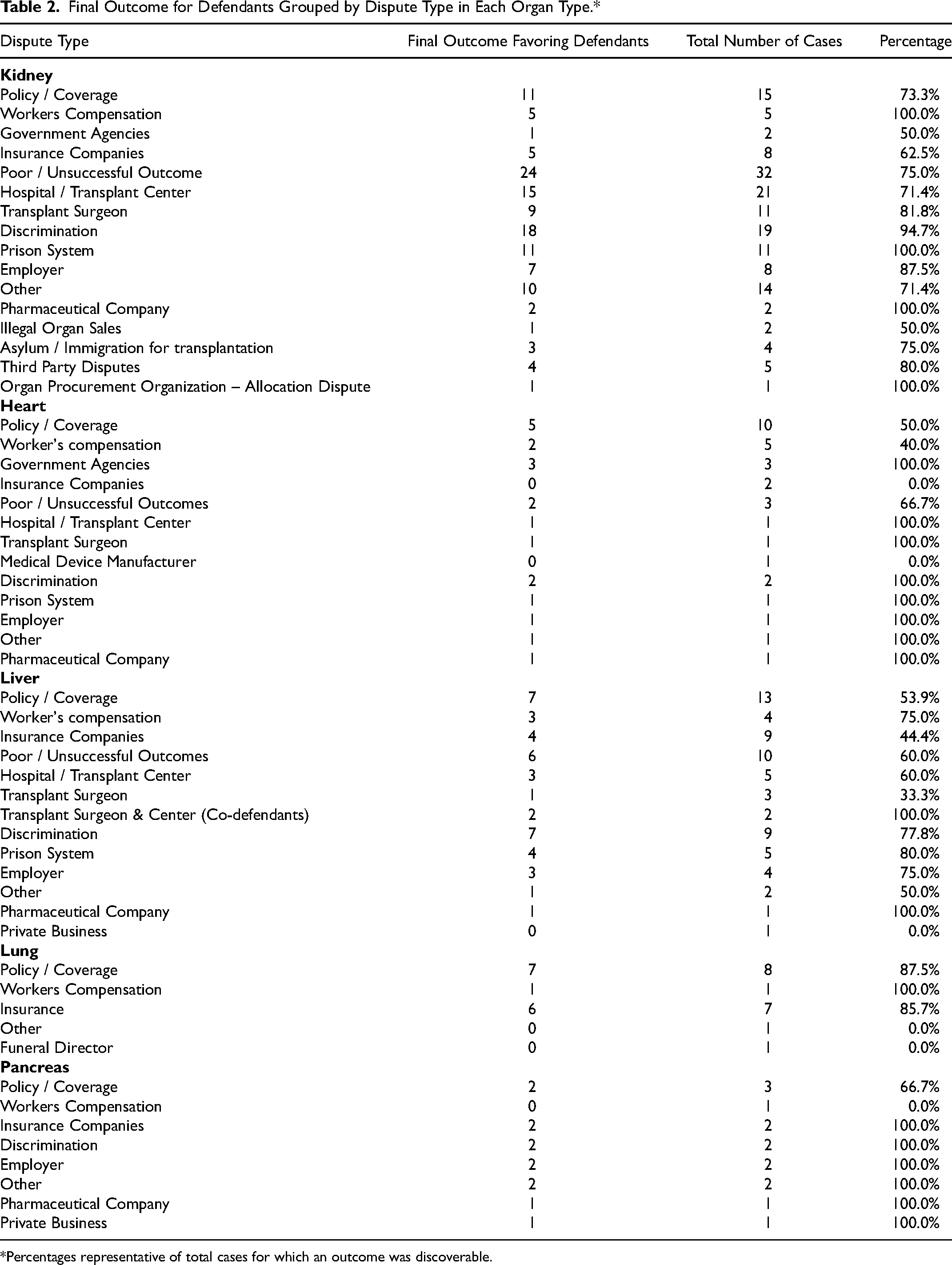
Percentages representative of total cases for which an outcome was discoverable.
Heart
Of the 842 court proceedings obtained, 17 were included for analysis
Most defendants were involved in policy disputes (N = 10, 58.8%). Employers involved in workers’ compensation claims represented the most common type (N = 5, 50%). Next was government agencies such as the Federal Bureau of Prisons or Social Security Administration (N = 3, 30%) and insurance companies (N = 2, 20%). Of the 4 poor outcome suits, transplant facilities were involved in 2 cases. One case involved a transplant surgeon and another involved a medical device manufacturer. There were 2 defendants in discrimination cases. One was a prison system, and the other was an independent employer. Finally, a pharmaceutical entity was involved in 1 suit.
In the 17 cases reviewed, all but 1 had a final verdict (94.1%)
Liver
Three-hundred and sixty-seven total court proceedings were reviewed; 89 met inclusion criteria
Insurance companies were the primary defendants in 13 suits (N = 13, 31%). Transplant surgeons or transplant medical centers were defendants in 28.6% of cases (N = 12). Further analysis of this category showed that transplant surgeons (N = 3), transplant surgeons with transplant centers as co-defendants (N = 2), and transplant centers as sole defendant (N = 7) accounted for 7.1%, 4.8% and 16.7% of the total defendant cohort, respectively. Governmental agencies were present in 4 cases (9.5%). Other defendant types included prison systems (N = 6, 11.5%), employers (N = 5, 11.9%), a pharmaceutical company (N = 1, 2.4%), and a private business entity (N = 1, 2.4%).
Final verdicts were discoverable in 35 of 42 suits (83.3%) (
Lung
Nine lung cases were analyzed
Insurance companies were the primary defendant type (N = 7, 77.8%). Funeral directors (N = 1, 11.1%) and employers (N = 1, 11.1%) were the remaining defendants.
A final verdict was discoverable in all cases (N = 9)
Pancreas
Seven pancreas transplant-related court briefs were reviewed
Insurance companies were defendants in 28.6% of cases (N = 2). A similar number involved employers involved in allegations of work-related discrimination (N = 2, 28.6%) and once in workers’ compensation disputes (N = 1, 14.3%). One suit targeted a governmental agency, another involved a pharmacy, and another implicated a private business entity (N = 1, 14.3%, respectively).
Defendants won 80% of cases (N = 7)
Twenty-three of the 51 total cases concerning poor or unsuccessful outcomes revealed a failure by the defendant to properly obtain informed consent (45.1%).
Discussion
Medical centers and transplant surgeons were frequently subject to cases due to lack of informed consent. This was particularly prominent in kidney transplantation wrongful death suits. While risk disclosure is often stressed to reduce malpractice exposure, it remains a frequent basis for litigation.1,8,9 The inadequate transparency of information has been specifically recognized by patients undergoing donor nephrectomy.
Donors have reported feeling ill-informed and unprepared for all aspects of donation. 10 Candidates cited poor explanation of the evaluation process, insufficient preparation information, and minimal understandings of risks, testing, and surgical procedures.10,11 Many also felt that explanations about the donation process did not match their experiences.10,12 These findings suggest measures may be taken to decrease litigation risk.
Recognizing the need for informed consent guidance, OPTN/UNOS established donor requirements in 2013. 13 Little policy or recommendation exists on how to approach the recipient. This is problematic for its legal implications. Solid organ transplantation consent is also more complex than other surgeries. 14 This raises a complicated question of how best to meet a patient's expectations. A discrepancy exists regarding the legal standard for patient information, a physician-centered or a patient-based standard. In short, these can be reduced to: what would a colleague deem necessary to disclose? And, what information would a patient require to adequately comprehend the risks and benefits necessary to decide on a treatment? 15 Presumably, orienting ourselves towards the informational needs of patients rather relying on colleagues’ presumptions portends the greatest means of mitigating risk. To our knowledge, there is no literature, comparing these two legal standards. Still, a few practical considerations exist.
Foremost, transplant center consent forms are written at a freshman college level. This surpasses the education level attained by many US dialysis patients. 16 Policymakers recommend writing at a fifth-eighth grade reading level. 17 But even more simplistically, the surgeon can empower patients with a sense of control over their care. 18 Beyond its alignment with our ethical duty to promote patient autonomy, a shared-decision-making approach may reduce the likelihood of patients filing complaints or lawsuits. 19
Disputes over insufficient insurance coverage, disability benefits, or workers’ compensation were the primary reasons for litigation in most organ transplant types. Although not the most common in kidney transplant related suits, these disputes comprised 19.1% of cases. Given transplantation costs, this is a major theme of the analysis. Beginning with the least costly, pancreatic transplantation bills approximately $350 000, while heart transplantation costs $1 300 000. 20
Combining all allegations of insufficient cost coverage against the various defendants, they won 65.3% (N = 32). A misleading inference from this is that transplant patients should accept any settlement given lower success in court. There are both internal and external appeal processes for individuals to pursue the compensation they feel entitled to. 21 One should not attempt to extrapolate these findings to the winning probability in these preliminary steps. Nevertheless, these claims highlight the financial vulnerabilities recipients and donors incur.
Even when patients are eligible for Medicare, recipients may still be liable for various costs for transplant facility charges, and 20% of immunosuppression costs. 22 Prior to 2020, medication coverage ended 36 months after successful kidney transplantation. 23 However, with the Immunosuppressive Drug Coverage for Kidney Transplant Patients Act (H.R.5534), coverage lasts the recipient's lifetime. 24 Despite this, patients continue to experience economic burden because of limited coverage.
The policy's restriction to kidney recipients is a drawback. Additionally, this lifetime coverage is limited to those eligible for Medicare Part B. 25 This may leave those receiving other forms of Medicare financially vulnerable. 23 This limited insurance is also associated with worse patient outcomes. In heart transplantation, an association has been made between public insurance and worse long-term outcomes compared to those with private insurance. 26 Presumably, this is due to differences in access to care and coverage. While warranting scrutiny for confounding factors, the significance of inadequate policy coverage is emphasized throughout the literature and was a major theme of this analysis. This dialogue raises an additional concern of the presence of structural injustices in organ transplantation.
There were 2 major categories in the thematic analysis related to allegations of discrimination. Twenty claims involved prisoners alleging they were wrongfully denied transplant-related care. An additional 19 suits concerned claims of unlawful termination by an employer or prejudicial hiring practices. Of note, only 1 case brought by prisoners had a successful outcome (5%), suggesting prisoners are unlikely to win rulings. Similarly, only 2 lawsuits brought against employers were successful (10.5%). Prisoners may be experiencing constitutional torts precluding them from liver transplantation. 27 Given most cases favored the various prison systems, the findings fortunately did not substantiate this. Nevertheless, a favorable legal ruling does not necessarily indicate that prisoners received the care they deserved. One case in the analysis exemplifies this point.
Hubbard v. Taylor (2006) involved an incarcerated individual making such constitutional claims against the Delaware Department of Correction. The plaintiff developed end-stage renal disease in 1994 from unspecified pathology and was maintained on hemodialysis since. In 1998, he was found ineligible for transplantation by Prison Health Services because of his incarcerated status. In subsequent appeals, he was deemed stable on dialysis and therefore did not appear to need a kidney. He attempted to subpoena his medical records, which allegedly contained documentation that he was eligible for transplantation yet was denied his medical records. In 2006, the defendants were again granted summary judgment closing the claim against them on grounds that the plaintiff remained stable on hemodialysis. 15
It is beyond the scope of this paper to argue that this did not constitute deliberate indifference, and in turn, violate a constitutional right afforded by the Eighth Amendment. The conclusion that the plaintiff was stable on dialysis does not acknowledge that patients experience less mortality and improved quality of life following kidney transplantation. 28 Therefore, if transplantation is reasonable for these patients, it is difficult to argue against their right to desired care. Additionally, the legality of this ruling might have rested on an erroneous medical premise which brings the former under scrutiny.
There are several strengths to this analysis. The outcomes of litigation related to solid-organ transplantation is severely limited in existing literature. The examination of cases in this analysis indicated this may be the most thorough analysis of litigation related to solid-organ transplantation. The findings provided insight that is relevant to many different stakeholders and has more practical implications for transplant surgeons and hospitals engaged in non-frivolous lawsuits that are likely to progress to trial.
A major weakness is citation age. Yet, inferences gained from these citations remain pertinent to the manuscript's goal. In addition, more up-to-date information was not available, making this a modern update given the dearth of current literature on the topic.
As noted by Tapper et al who engaged in a similar undertaking, only published legal proceedings are searchable. 27 Thus, it is possible that this analysis excluded relevant, lower court trials. Also, suits involving undocumented immigrants seeking organ transplantation were not fully captured. As they lack standing in court, they are often absent in searches. The investigator's ability to construct a comprehensive overview of all litigation involving organ transplantation was therefore limited.
This study might also be subject to criticism of relevance. Given that 95% of malpractice cases do not progress to trial, 3 this work may not seem important to typical transplant professionals. Although informed consent was a recurrent theme of malpractice trials, it was beyond the scope to extract granular detail on what the shortcomings were. Copious literature exists addressing ideas of informed consent and malpractice in general. Future work should be oriented towards defining common shortcomings in the disclosure process, which makes transplant surgeons and institutions vulnerable to litigation.
Conclusion
This analysis provides a comprehensive thematic analysis of litigation on organ transplantation, the most implicated parties to such suits, and their outcomes. Fewer cases than expected were brought against transplant centers and surgeons. Cases brought against them specifically mentioned plaintiffs’ lack of informed consent as partial grounds for claim. This suggests that reevaluating the process of educating patients about transplantation risks may help mitigate future legal action. Similarly, future OPTN/UNOS recipient guidelines of consent may provide a schema for providers to highlight risks in a more complete manner.
Additionally, this work did not substantiate claims of structural injustice in transplant surgery. This does not preclude the possibility of inequity within the field. Insufficient policy coverage claims were the most common theme. This may be reflective of financial vulnerability donors and recipients incur. The absence of legal rulings demonstrating discrimination or insufficient policy coverage does not necessarily prove a perfectly just system. Ongoing investigations are necessary to ensure the equitable allocation of organs given the nature of these suits. Additionally, it is hoped that the gift of transplantation does not come at the cost of financial ruin.
Footnotes
Acknowledgements
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.