
Abstract
Keywords
Introduction
Living donor kidney transplantation (LDKT) is often the optimal treatment for end-stage kidney disease (ESKD), but only a moderate proportion of kidney transplant candidates receive one. 1 Although numerous steps between incident ESKD and kidney transplantation have been described,2–5 a potentially critical but understudied step is the living donor discussion (LDD) with friends or family. 6 Living donor discussion is defined as the discussions that candidates have with members of their social network about evaluation for potential living donation. Furthermore, it is critical to distinguish between who initiated the LDD—the candidate or the potential donor—and assess the consequences of this difference for mutual agreement for LDKT evaluation.
The discussion stage of kidney transplantation may provide insight into disparities in transplantation by race, gender, and relationship type, which are well-studied but incompletely understood. For instance, women are more likely to become living kidney donors and less likely to receive donations than men.7–10 Although many explanations for this disparity have been offered,10,11 an understudied factor may be gender differences in altruistic behaviors and gendered caregiving social norms, which could make women more likely to offer to donate, and less likely to accept others’ offers, than men.7,11 Similarly, Black candidates are less likely to receive a living donation than White candidates. 5 Previous research has cited lower levels of LDDs as a contributing factor to racial disparities in LDKT,6,12–15 but no previous research has differentiated these discussions by who initiates them or their consequences for racial disparities. Finally, the Scientific Registry of Transplant Recipients annual data reports frequently highlight the high (but falling) concentration of living donations from close family members compared to more distant family or non-family, 16 but the discussion dynamics that underlie this pattern are unclear.
This study aimed to fill the gaps in the current literature by examining 4 key research questions: (1) How common are candidate- and potential-donor-initiated discussions? (2) At what rate do candidate- and potential-donor-initiated discussions result in an agreement for living donation evaluation? (3) What social and demographic characteristics of candidates and potential donors predict candidate- and potential-donor-initiated discussions? (4) What social and demographic characteristics of candidates and potential donors predict the outcomes of candidate- and potential-donor-initiated discussions? To answer these questions, this study used data from a single-center sample of kidney transplant candidates and their descriptions of their social networks.
Methods
Design
The Ego Networks among Candidates for Transplant (ENaCT) study was a 2014-5 cross-sectional survey sample at a single transplant center which recruited 73 kidney transplant candidates. This survey employed an egocentric survey design in which candidates were surveyed both about themselves as well as their social network members. This study was approved by the university Institutional Review Board (protocol # X141121010).
Setting
All recruitment was conducted at a single Southeastern United States transplant center. A member of the research team recruited participants immediately after a presentation by transplant center nurses on kidney transplantation generally with a special focus on LDKT. The survey took place once those who did not participate left the room unless candidates asked that their companion remain with them while they completed the surveys. Participants could answer the survey with the help of their companion or a research team member upon request.
Population
The target population was US kidney transplant candidates in the early stages of evaluation. The accessible population was new candidates at the transplant center. ENaCT participants’ racial/ethnic distribution matched closely to contemporaneous recruitment center new waiting list additions (ENaCT 61% Black, 33% White, and 6% others; center 58% Black, 38% White, 4% others). However, the recruitment center's patient population differed somewhat from the surrounding UNOS region and the United States, with higher shares of Black candidates and lower shares of Latino/a candidates than the UNOS region (47% Black, 36% White, 17% other) and the United States (29% Black, 44% White, 27% other). Candidates age ≥ 65 were somewhat overrepresented, and ages 50 to 64 were somewhat underrepresented, in ENaCT compared to the transplant center (ENaCT 15% 18-34, 39% 35-49, 35% 50-64, 11% 65+; recruitment center 16% 18-34, 35% 35-49, 46% 50-64, 4% 65%). Furthermore, 2014 to 2015 new candidates at the recruitment center were younger than its UNOS region (12% 18-34, 28% 35-49, 40% 50-64, 17% 65+) or the United States (12% 18-34, 27% 35-49, 42% 50-64, 18% 65+).
Sampling
ENaCT is a nonprobability, convenience sample study. Patients were eligible to participate if they could speak and read English and were age ≥ 19. Participants were compensated $10 each.
Because only 4 respondents marked they were Hispanic in the ENaCT survey, the analytical sample was restricted to non-Hispanic White and non-Hispanic Black candidates, reducing the analytical sample from N = 73 to N = 69. The analytical sample was further restricted to those with complete data on the 4 primary independent variables—race, gender, education, and age, dropping 3 additional respondents (N = 66).
Data Collection
Candidates described themselves and their social networks in 2 survey instruments (the candidate survey and network member survey). Among other variables, the candidate survey measured candidate race (non-Hispanic White vs non-Hispanic Black), age (19-35, 36-50, 51+), sex (male vs female), and education (attended college vs did not attend college) were measured in this instrument.
In the network member survey, candidates described their adult family and friends. Candidates first reported a list of network members in each relationship category, then a series of network-member-specific questions were asked about each network member, including network member age, sex, and relationship to candidate (parents, children, siblings, aunts/uncles, nieces/nephews, grandparents, grandchildren, cousins, other family, spouse/partner, or friend). This relationship variable was recoded into 3 categories: nuclear family (parents, children, siblings, spouses/partners), extended family (aunts/uncles, nieces/nephews, grandparents, grandchildren, cousins, other family), and non-family (friends). The dependent variables (LDD direction and evaluation agreement) for this analysis were measured in the network member survey. For each network member, the candidate was asked about the LDD direction: Have you asked them or they have volunteered to be medically evaluated for donating a kidney to you? with the response options Yes, they volunteered (potential-donor-initiated discussion); Yes, I asked (candidate-initiated discussion); and No, haven’t discussed (no discussion). If the respondents marked 1 of the first 2 options, they were prompted to describe the outcome of the LDD: If you have asked them or they have volunteered to be medically evaluated for donating a kidney to you, what happened? with the response options: I/they said yes (evaluation agreement); and I/they said no or Don’t know (no evaluation agreement).
Data Analysis
First, the candidate and network member variables’ distributions were described. Second, the association of discussion direction and evaluation agreement was descriptively assessed. Third, the distribution of discussion direction across candidate race, candidate gender, and network member relationship type was described. Fourth, average marginal effects (i.e., differences in probability associated with a 1-unit change in independent variables) of candidate characteristics were calculated for discussion direction outcomes using a random-effects multinomial logistic regression model (with no discussion as the reference category). Finally, among network members who had discussed donation with the candidate, the evaluation agreement outcomes were also modeled using random-effects multinomial logistic regression analysis (comparing evaluation agreement and don’t know responses to the no evaluation agreement reference category) and effects presented as average marginal effects.
Procedure
Kidney transplant patients were asked to complete a survey describing themselves and their adult family and friends. Patients had up to 90 min to complete the survey, and study staff or patient companions were permitted to assist them when needed (e.g., for limited vision or reading ability).
Results
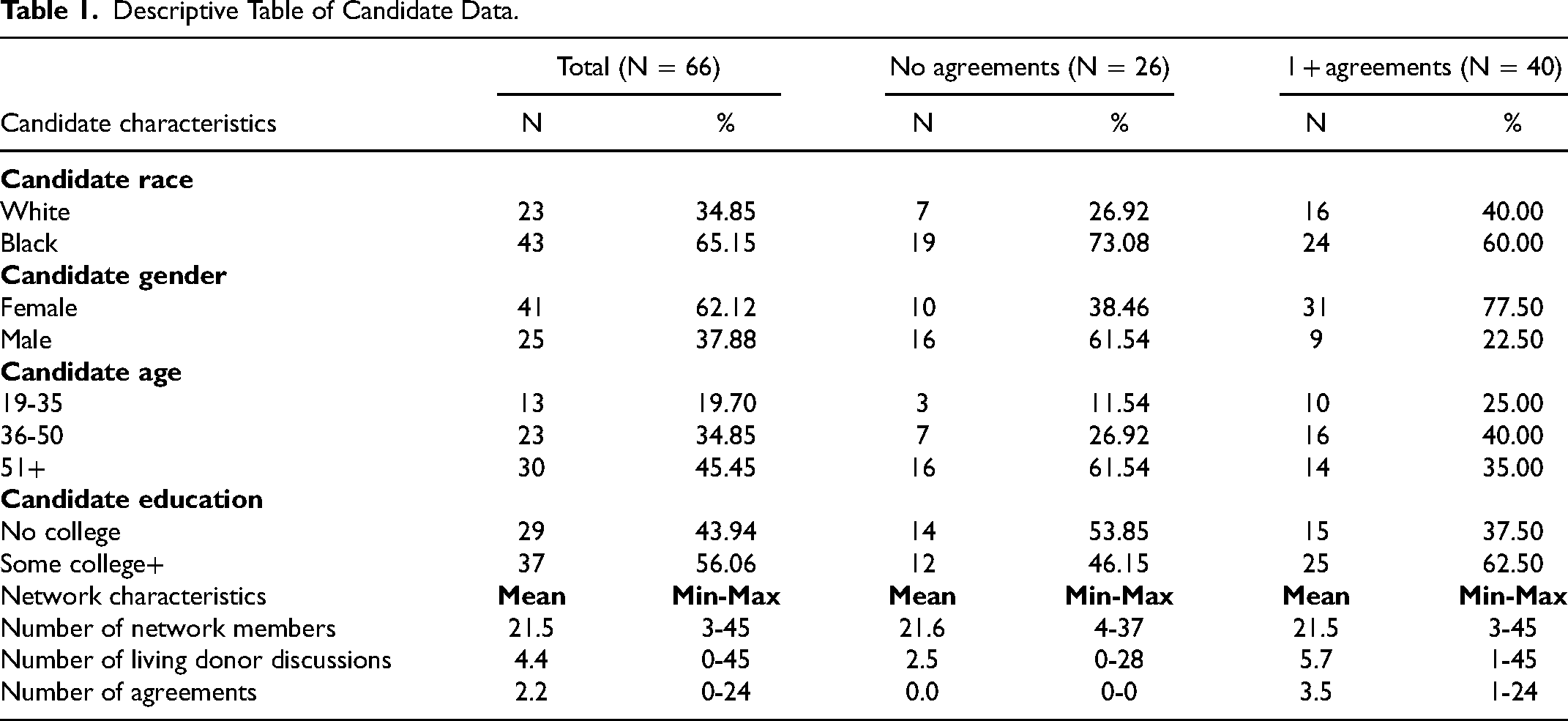
Candidate Characteristics
Descriptive Table of Candidate Data.
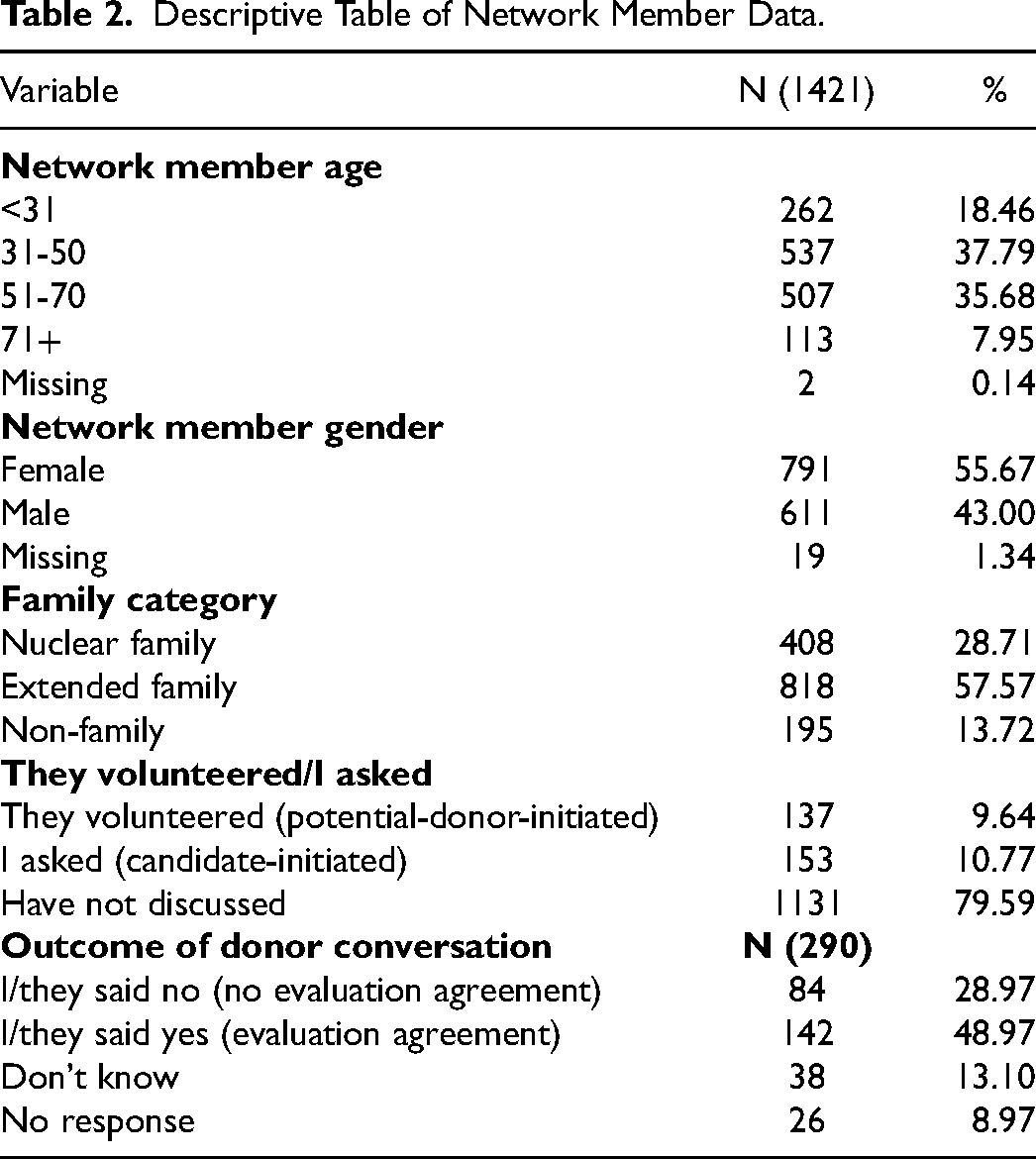
Network Member Characteristics
Descriptive Table of Network Member Data.
Relationship Between Discussion Type and Evaluation Agreement
Discussion Outcome by Living Donor Discussion Direction.a
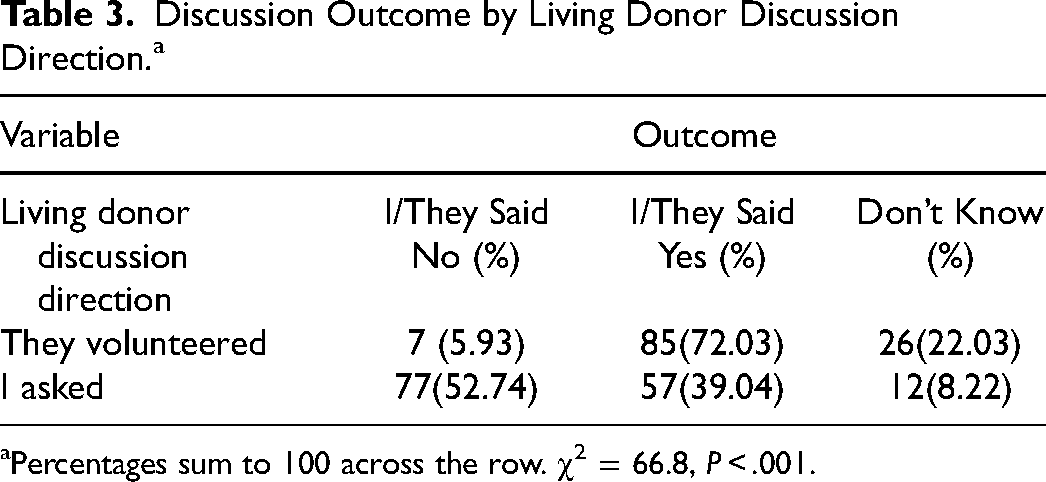
Percentages sum to 100 across the row. χ2 = 66.8, P < .001.
Living Donor Discussion Direction by Candidate Race and Sex, and Family Category.a
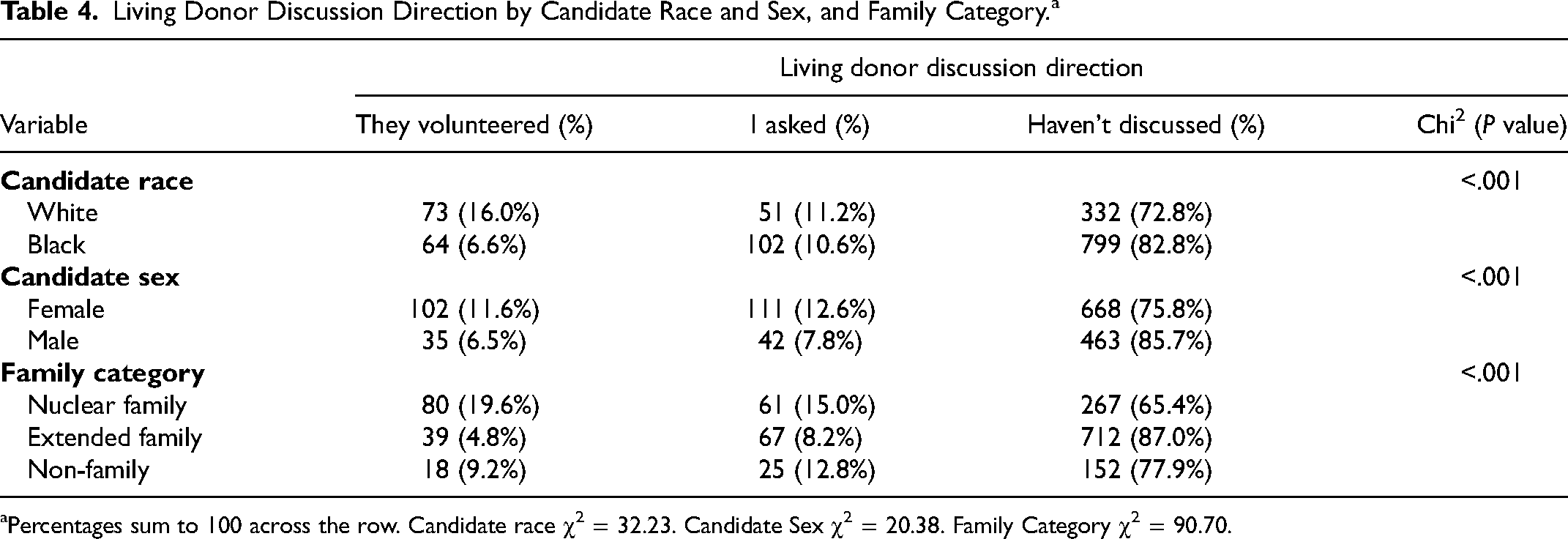
Percentages sum to 100 across the row. Candidate race χ2 = 32.23. Candidate Sex χ2 = 20.38. Family Category χ2 = 90.70.
Sociodemographic Characteristics That Predict LDDs
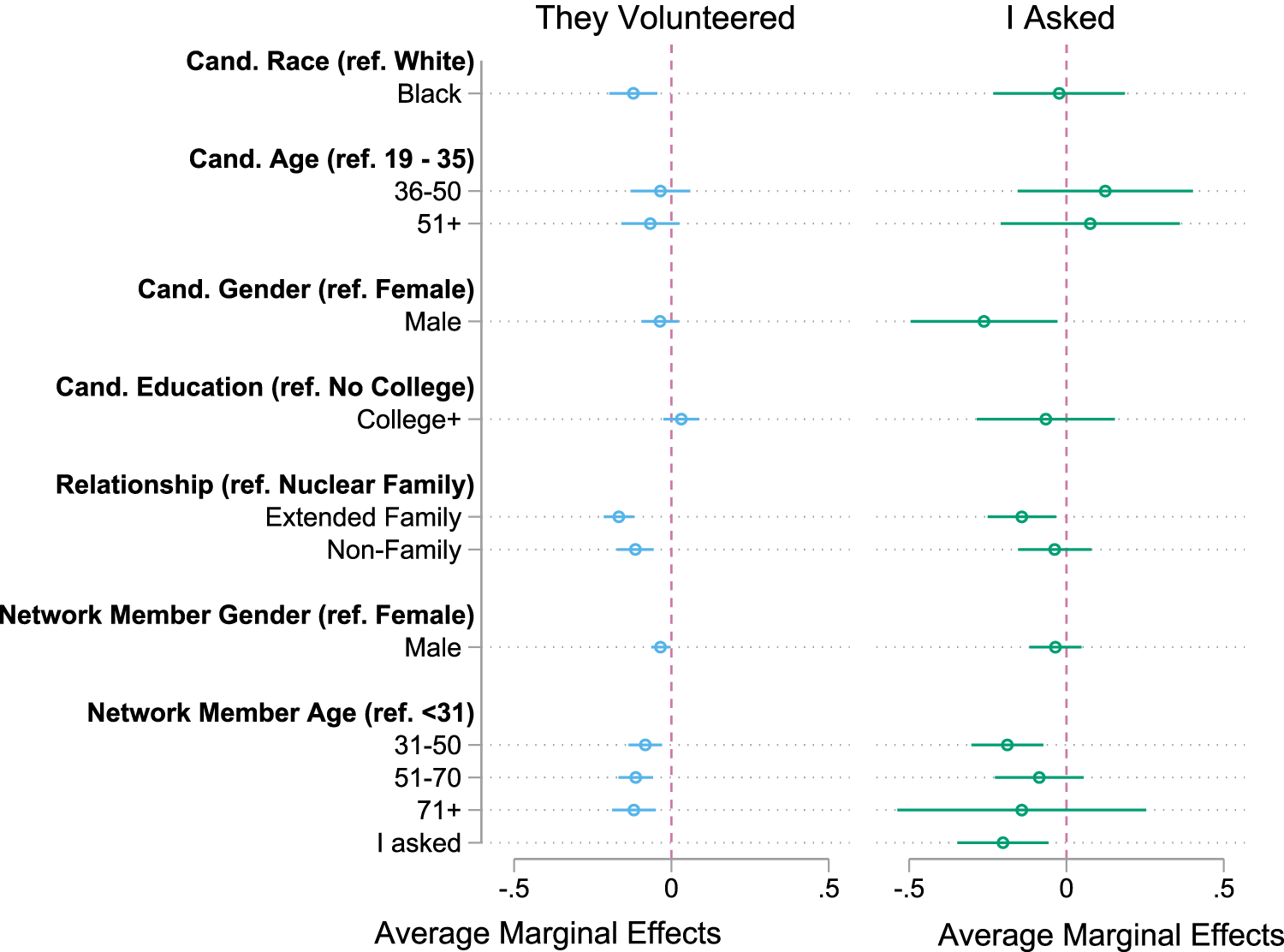
Average marginal effects of the random-effects multinomial logistic regression model of discussion direction. Cand., candidate.
Network member characteristics also predicted discussion direction. Compared to nuclear family members, extended family members have a 17% lower probability of potential-donor-initiated discussions and a 10% lower probability of candidate-initiated discussions (P = .000). Also compared to nuclear family members, non-family have an 11% lower probability of potential-donor-initiated discussions and a 9% lower probability for candidate-initiated discussions (P = .000). Male network members have a 3% lower probability of potential-donor-initiated discussions (P = .019), but there was no statistically significant difference for candidate-initiated discussions (P = .621). Finally, network member age predicted discussion direction. Compared to network members age < 31, network members aged 31 to 50 had an 8% lower probability of potential-donor-initiated discussions (P = .002) but no statistically significant difference for candidate-initiated discussions (P = .482). Network members aged 51 to 70 had the same pattern with a larger probability difference, as compared to network members aged <31 they had a 11% lower probability of potential-donor-initiated discussions (P = .000), but no statistically significant difference for candidate-initiated discussions (P = .945). Finally, compared to network members aged <31, network members aged >70 had a 12% lower probability of potential-donor-initiated discussions (P = .001) but no statistically significant difference for candidate-initiated discussions (P = .654).
Sociodemographic Characteristics That Predict Evaluation Agreement
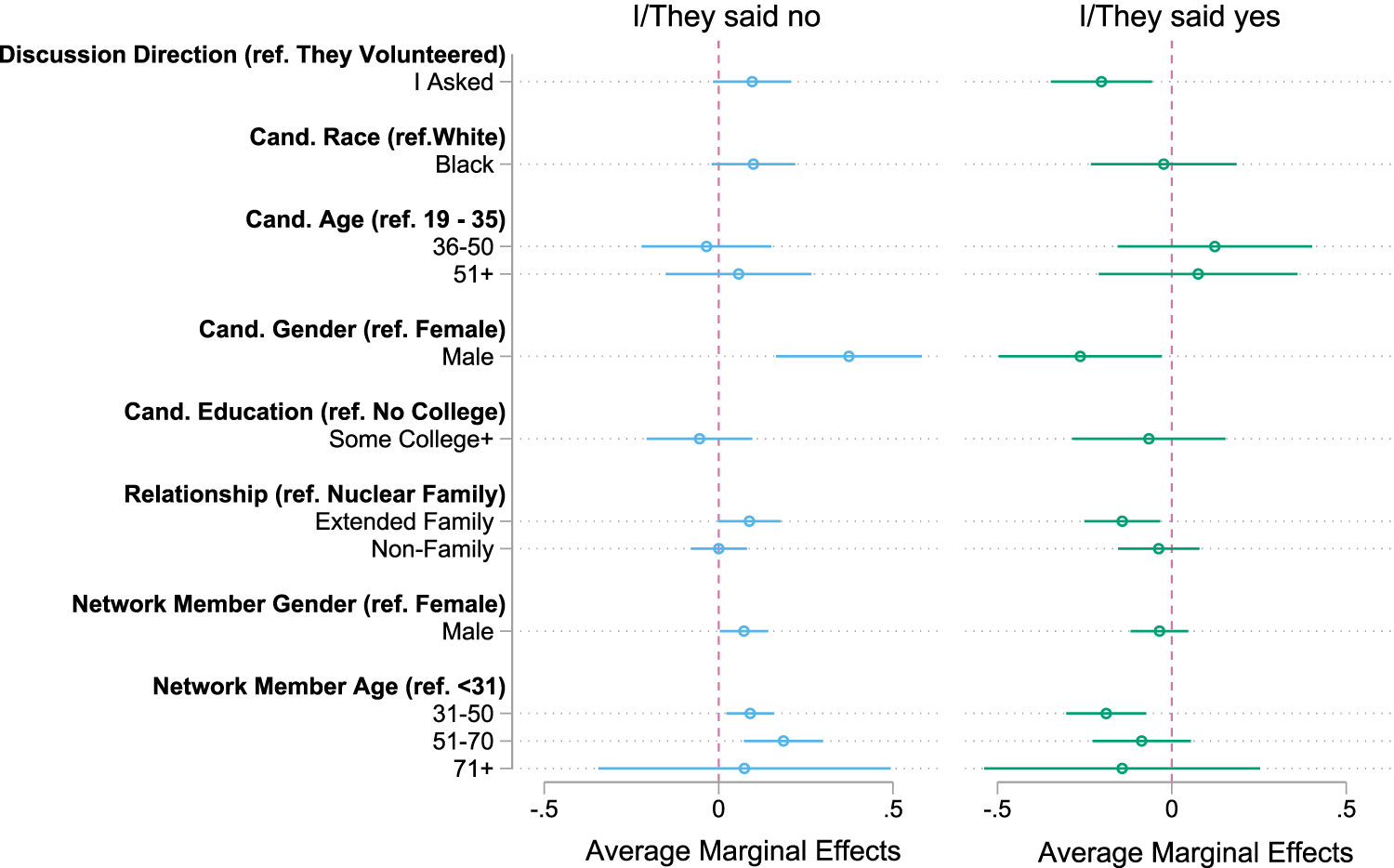
Average marginal effects of the random-effects multinomial logistic regression model of evaluation agreement outcomes among candidate-network member pairs. Cand., candidate.
Discussion
The findings from this study provide insights into LDDs, particularly the impact of candidate- versus potential-donor-initiated discussions on the probability of evaluation agreement and the influence of sociodemographic characteristics on these processes. The results indicated that candidate-initiated discussions were more likely to be associated with no evaluation agreement than potential-donor-initiated discussions—that is, who asks matters. Furthermore, sociodemographic characteristics played a large role in who was more likely to have a candidate- or potential donor-initiated conversation. Black candidates, non-nuclear familial donors, and donors over the age of 31 were less likely to have potential-donor-initiated discussions, while older and extended family donors were less likely to have candidate-initiated discussions. These findings suggested that interventions that promoted potential-donor-initiated LDDs were likely to be more effective at promoting potential donor evaluations than those that promoted candidate-initiated LDDs.
Besides the discussion direction, several additional sociodemographic characteristics predicted evaluation agreement, including candidate gender, relationship type linking candidate and network member, network member race, and network member age. These findings suggested that LDDs and their direction may be potentially critical contributors to, and intervention points for, social disparities in LDKT, such as women's higher propensity to become living kidney donors, Black patients’ lower odds of receiving an LDKT, and more educated patients’ higher odds of receiving an LDKT. Future research should investigate these questions with larger, more representative samples of candidates and their social networks.
The findings add to the literature about LDDs and the influence of social and demographic factors for discussions. The candidate's race and gender all influenced the likelihood of having candidate- or potential donor-initiated discussions, and candidate-initiated discussions had a higher likelihood of ending in potential donors’ refusal to be evaluated for donation. Although these findings do not address candidates or network members’ reasoning for agreeing to be evaluated or not, several studies have addressed barriers to living donation that are important for understanding the results. Previous research has cited differential access to healthy donors,17,18 lack of knowledge regarding transplantation,19,20 and mistrust as potential barriers to living donation for Black candidates. 17 Moreover, research has posited that the overrepresentation of women as living donor may be due to traditional gender norms for women to be more altruistic. 11
The main result was that candidate-initiated discussions were more likely to end in negative outcomes. This may be interpreted to mean that while candidates rarely decline evaluation offers, network members who do not volunteer have low rates of willingness to donate. One approach to redress this reality would be to promote a more effective discussion about living donation. One such intervention is Communicating about Choices in Transplantation (COACH), a behavioral communication intervention aimed at providing candidates with information and strategies for approaching transplantation with potential donors. 21 Results from this pilot study provided positive and support for the impact of such interventions. Another education-based intervention found that a house-call intervention—where a trained health educator spoke directly to the candidate and their invited potential donors at the candidate's home—were more likely to result in evaluation. 22 The positive results from these interventions suggest that more widespread interventions with aims at arming candidates with tools to have more effective discussion or having the help of trained transplant educators may help reduce disparities in LDKT. Public educational campaigns to promote greater awareness of the low risks and strong benefits of LDKTs and who is eligible to donate may also prove effective at promoting greater and more equitable LDKT access.
This study had limitations that should be taken into consideration when interpreting the results. First, the sample was drawn from a single, large transplant center in the southeastern United States, and the analytical sample was exclusively Black and White. Thus, future research should investigate whether these results are generalizable to the larger kidney transplant population, particularly those in other regions or members of other racial/ethnic groups. Additionally, the analyses did not measure candidate or potential donor attitudes or beliefs that may be important for the outcomes of the LDDs. Future research on LDDs would benefit from a more in-depth investigation of the role of candidate and donor beliefs and attitudes in determining the outcome of discussions and whether they vary between candidate- and potential-donor-initiated discussions.
Conclusion
This study adds to the growing literature as one of the first to directly test if the outcome of LDD is associated with who initiates the discussion, the candidate or potential donor. The results found that candidate-initiated discussions were more likely to end in the potential donors’ refusal to be evaluated and call attention to the need for interventions that promote more effective LDD. Additionally, the results found significant differences in who initiated LDDs and discussion outcomes by race and gender, suggesting that differences in LDDs may contribute to disparities in LDKT.
Footnotes
Acknowledgments
The authors thank Shawn Bauldry, PhD, Chenoia Bryant, PhD, Katie McIntyre, PhD, Sara Rutland, PhD, and Ashton Verdery, PhD for their assistance designing and implementing the survey analyzed in this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIDDK grant R01DK114888 and the University of Alabama at Birmingham Comprehensive Transplant Institute, the Penn State Social Science Research Institute, and the Population Research Institute at Penn State University, which is supported by an infrastructure grant by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2CHD041025).