
Abstract
Introduction
Despite the evidence supporting the benefits of physical activity and structured exercise training among solid organ transplant recipients, low physical activity levels persist for years following transplant.1,2 Physical activity encompasses any body movement that requires an expenditure of energy, whereas exercise is a subcategory of physical activity and is defined as planned, structured, repetitive, and purposive activity with the goal of improving or maintaining fitness. 3 Low levels of physical activity have been associated with untoward clinical outcomes such as lower health-related quality of life and greater cardiovascular disease risk.4,5 By engaging in physical activity or exercise training, transplant recipients may reduce the risk of cardiovascular disease and all-cause mortality. 6 Transplant recipients may also mitigate secondary, chronic transplant-related conditions such as high blood pressure, metabolic syndrome, and osteoporosis, as well as improve their health-related quality of life. 4
Transplant recipients encounter a variety of barriers to performing physical activity behaviors. These include physical (eg, lack of energy, medication side effects), psychological (eg, low self-efficacy), and social (eg, lack of social support) barriers.1,7 Digital health interventions are defined as “health services and information delivered or enhanced through the Internet and related technologies,” 8 (p20) such as smartphone applications, some of which are paired with fitness trackers, have the potential to support physical activity behaviors in transplant recipients by increasing self-efficacy and self-management skills.9,10
In our previous work, transplant recipients identified that having the ability to selectively share health information with members of their healthcare team would be helpful in supporting physical activity posttransplant. 11 Engagement of healthcare professionals (HCPs) should be considered in the development and implementation of new technology to ensure acceptance and to promote an optimal user-centered approach and experience.12,13 The purpose of this qualitative study was to explore the perspectives of HCPs regarding the features of a digital health intervention that would support physical activity in transplant recipients, and how an intervention could be integrated into their clinical workflow. We also explored their perspectives on the barriers and facilitators of performing physical activity behaviors to provide context for their viewpoints.
Methods
Settings
This qualitative, cross-sectional study was conducted through 2 Canadian universities, and ethics approval was obtained at each site (University of Toronto Health Sciences REB #36905 in January 2019 and McGill University REB #5020 in February 2019). This study adhered to the consolidated criteria for reporting qualitative research (COREQ).
Sampling
A purposive sampling strategy was employed. Eligible participants included licensed HCPs with at least 1 year of experience providing counseling on physical activity to adult transplant recipients and were working in Canada presently, or within the past 12 months. Efforts were made to recruit participants from various occupations, provinces, practice settings, and exposure to different transplant types. Ethnicity and age were not considered. Potential participants were contacted via individual emails, obtained through the online directory of Canadian transplant rehabilitation programs (CAN-RESTORE) and through an email listserv of the Canadian Society of Transplantation, a professional organization of approximately 400 HCPs. Recruitment also occurred through social media platforms, including Twitter accounts of the investigators and the CAN-RESTORE Facebook page. Snowball sampling was also employed by asking eligible participants to inform their colleagues about the study. Interested participants were asked to contact the investigators by email. The final sample size for our study was determined by thematic saturation, which was estimated to be 10 to 15 participants. 14
Information Collection
Student researchers created the semistructured interview guide based on a literature review and expert knowledge from the research advisors. The interview guide was designed to capture information about experiences with physical activity and exercise counseling for transplant recipients (at any phase posttransplant), barriers to exercise, the potential of digital intervention, and which features would be most useful to support physical activity and exercise. The student interviewers were trained to conduct semistructured interviews by a study investigator, who was experienced in qualitative research and interview methods. The interview guide was pilot tested with 2 members of the research team who were practicing physiotherapists in transplant rehabilitation to provide researchers with feedback and improve the clarity of language. The final interview guide is provided in the Online Supplement.
Interviews were conducted and recorded remotely via videoconferencing software (GoTo Meeting) in English by 2 student researchers or in French by a research assistant according to participants’ language preference. The research assistant was also experienced with conducting interviews. Prior to commencing the interview, verbal consent was obtained by the interviewer and demographic data were collected (eg, gender, occupation, and area of practice). Each interview took approximately 1 h to complete.
For data saturation, the study team adopted the model of information power in making the decision to close the recruitment and interview phase of the study. 15 Acceptable information power was achieved when the study team no longer identified new information from the interview data as it pertained to the primary purpose of the study.
Thematic analysis was grounded in Braun and Clark's guidelines. 16 Audio files were transcribed verbatim by 3 research team members. For the French interviews, the research assistant transcribed the interview and translated it into English. Transcripts were then reviewed by 5 research team members. Codes were generated to identify relevant information and were developed using an iterative-inductive analytical strategy, which was highly suited for health-related research.15,17 Once an inductive coding framework was developed, codes were entered into NVivo (QSR International). Codes were organized into possible themes, and thematic mapping was completed to group patterns and develop connections between themes. Codes were reviewed and refined until the respective study team members agreed that they were inclusive of patterns in the data that addressed the research question. 17
Findings
Fifteen individuals contacted the study team to participate; 2 were excluded (1 only worked with pediatric transplant recipients and the other could not be contacted for an interview), resulting in 13 participants (3 men and 10 women). Many of the participants were physical therapists (n = 6), and the majority had experience working in lung transplant (n = 11); however, they had experience with other organ groups as well. Nine participants had 10 or more years of experience working in transplant and most worked with transplant recipients during the early postoperative phase after transplant (ie, <6 months posttransplant) (see
Characteristics of Healthcare Professionals (N = 13).
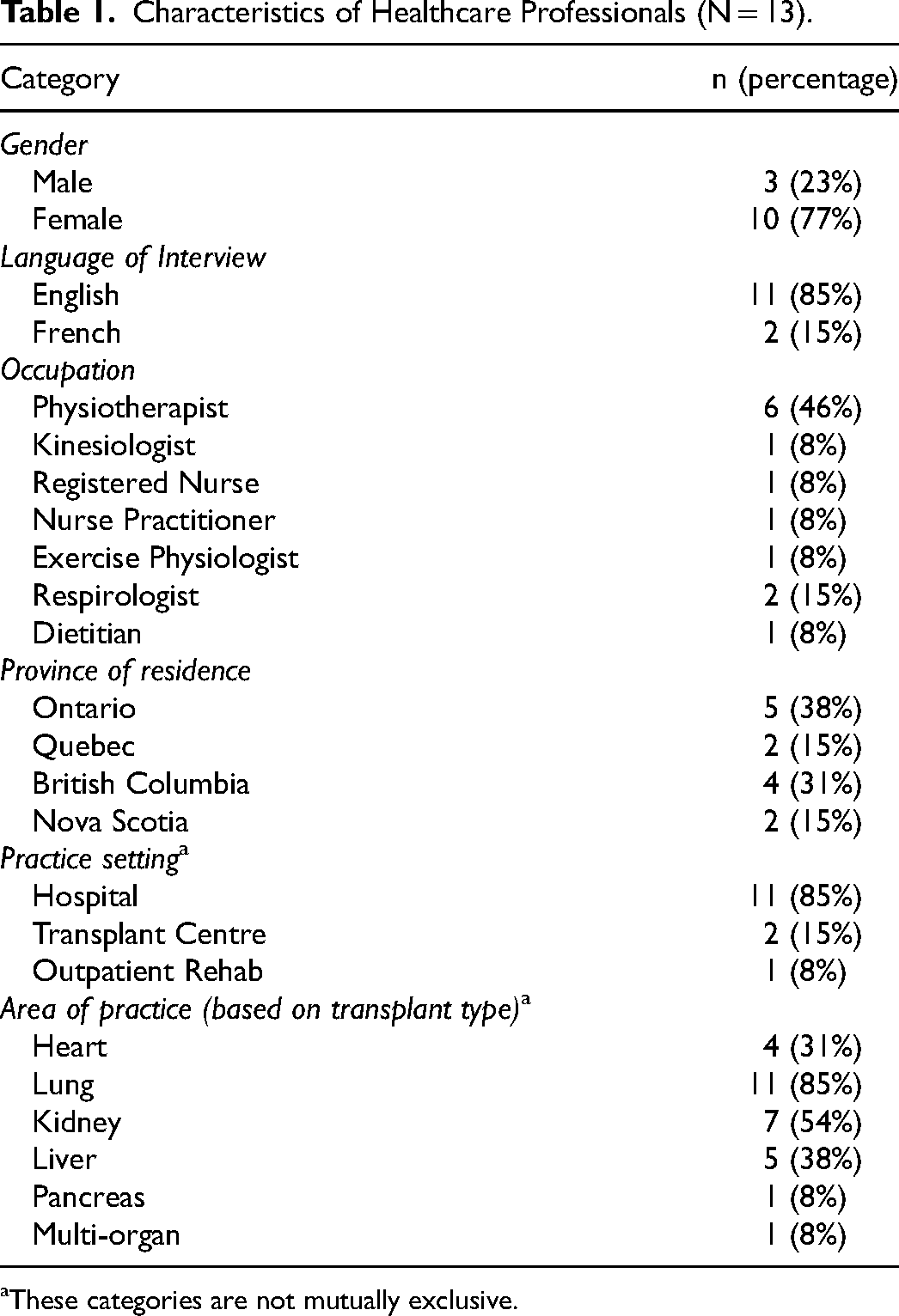
These categories are not mutually exclusive.
Barriers to Physical Activity Participation
Several barriers to physical activity were identified including physical, social, behavioral, psychological, and environmental barriers. Precarious health status following transplant was considered the most impactful physical barrier and included low exercise tolerance (n = 7), posttransplant complications (n = 8), and posttransplant oxygen requirements in lung recipients (n = 4). Social barriers included lack of social support (n = 6), limited financial resources (n = 7), and time (n = 6). Behavioral barriers included a low desire to change (n = 5) and established inactivity habits (n = 3). Psychological barriers included risk aversion surrounding physical activity and illness (n = 9), lack of knowledge about exercise (n = 6), and low motivation to partake in physical activity (n = 11). Environmental factors included lack of access to equipment, transportation, or formal programming (n = 10), weather (n = 5), and risk of infection (n = 3). Overall, HCPs perceived digital intervention as a possible mode to help recipients overcome barriers to participation in physical activity by increasing access to information, reducing costs associated with physical activity participation, and improving access for individuals living in rural areas.
Desired Features of a Digital Health Intervention
Four key themes were identified regarding the development and implementation of a physical activity supportive, digital health intervention. The desired features include features about exercise, credibility, self-management, and user engagement. Participants’ illustrative quotes for each theme are shown in
Quotes Illustrating the Opinions of Healthcare Professionals on Key Features of a Digital Health Intervention to Support Physical Activity among Solid Organ Transplant Recipients.
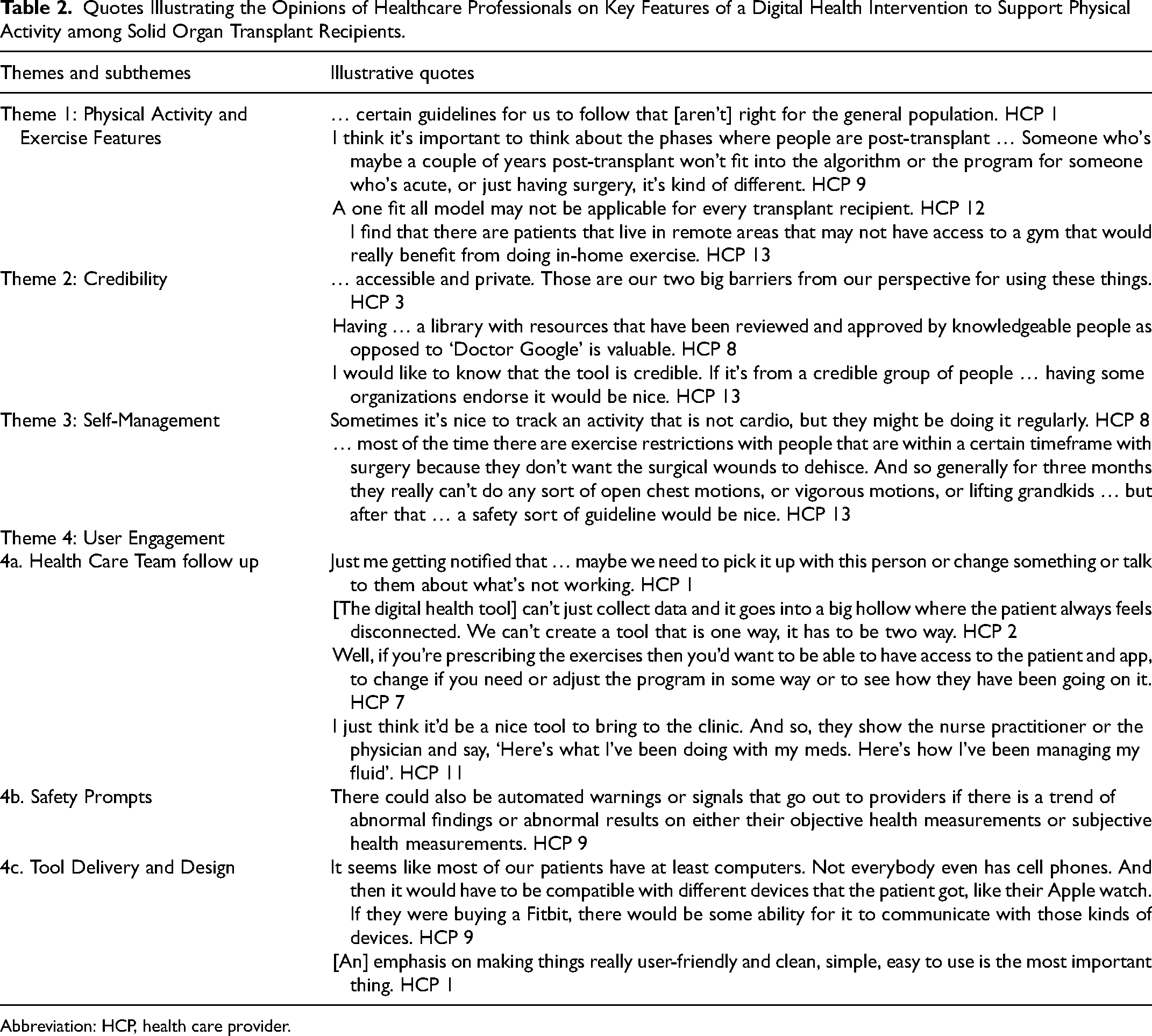
Abbreviation: HCP, health care provider.
Theme 1—Physical activity and exercise features
Participants overwhelmingly pointed out that an effective intervention must offer support in concrete ways that may help mitigate the barriers to physical activity. Namely, it should share information and guidelines specific to exercise (eg, type and parameters of exercise, and instructions on how to perform exercises correctly). Most HCPs (N = 12/13) indicated that features, such as access to physical activity guidelines, would be valuable and should be organ group specific. Further, participants felt that the intervention must provide individualized exercise programs that can be adapted to various phases of recovery and provide tailored progressions, as required. Additionally, they suggested that images and exercise videos be used to provide instructions. The HCPs also emphasized that access to a home exercise program may help in navigating environmental barriers to physical activity.
Theme 2—Credibility
Credibility (ie, trustworthy, factual, and secure) was identified as critical in the development of a digital health intervention. According to HCPs, it was paramount that all information users might receive or share through the device was credible, has the backing of relevant and reputable organizations, and contain up-to-date, evidence-based information. In addition, the digital intervention must maintain its credibility by ensuring the privacy and security of its users. The importance of data security was strongly emphasized. That said, regulations from various institutions and governing bodies around ownership and security approval required for use across healthcare settings and provinces were seen as a barrier to development and implementation (N = 4).
Theme 3—Self-management
All HCPs believed that a suitable intervention should include features that promote self-management such as physical activity and health data tracking, tracking of subjective measures, tailored education, and access to behavioral change strategies. Physical activity monitoring should include step counts as well as frequency, intensity, duration, and type of activity. An ideal activity intervention should have an interface where users are provided with an overview of trends in their health data. Health data should also include heart rate, blood pressure, oxygen saturation, diet, hydration, weight, sleep, and medication. Desired patient-reported outcome measures included rate of perceived exertion during physical activity, quality of life, pain, and mood.
Behavioral change strategies, in-line with some of those listed under the Behavior Change Technique (BCT) Taxonomy, such as feedback and monitoring (BCT 2.1-2.7), goal setting (BCT 1.1), rewards (BCT 10.3), social support (BCT 3.1-3.3), scheduling of activities (BCT 1.4), and activity reminders (BCT 7.1) should also be incorporated to effectively promote self-management and physical activity participation. 18 The HCPs perceived low motivation to use a digital intervention as a potential barrier (n = 5), and therefore, perceived the use of behavior change strategies as essential for success. Lastly, this service should provide lifestyle and wellness education to promote self-management, such as information on proper nutrition, sleep, exercise, and safe adaptation to any comorbidities and complications.
Theme 4—User engagement
User engagement describes how the potential users (transplant recipients and HCPs) may engage with the digital intervention, with an emphasis on accessing data and communication across diverse groups of transplant recipients. All HCPs reported that clinician involvement, and the opportunity for clients to follow-up with their clinician using the intervention is critical.
Subtheme 4a—Health care team follow-up
Many HCPs emphasized the importance of using digital health intervention posttransplant to aid recovery and transition out of acute care toward self-management. Three distinct roles were highlighted regarding their level of involvement with a digital program. First, some HCPs wanted the digital intervention to provide real-time prompts to check in with the transplant recipient when their data indicated low participation or a change in their health status. Second, some were interested in the possibility of increasing their engagement with patients via a digital health intervention such that they could provide exercise progressions based on health data. Third, other HCPs wanted to use intervention during in-person follow-ups. Participants also reported that it would be ideal for health data to be integrated with electronic health records. Although HCP follow-up consistently emerged as a desired component of the intervention, staffing requirements were perceived as a challenge to implementation.
Subtheme 4b—Safety prompts
The HCPs believed that the digital intervention should include safety prompts for the patient and healthcare team to contact each other. They believed that the program should flag safety concerns if they arise from inputted user data and send prompts to the appropriate clinician or clinical team as per the severity of the safety issue.
Subtheme 4c—Tool delivery and design
The HCPs anticipated that recipients may face a variety of barriers pertaining to the use of the digital intervention, including a lack of access to the internet or devices (n = 10) and related usage costs (n = 6). Thus, the method of delivery was a key consideration. The most consistent perception was that digital health interventions should be delivered through a variety of devices (eg, mobile phones, tablets, computers, and wearable technology) and compatible across technologies (n = 9).
Lastly, HCPs emphasized the importance of having a user-friendly design that is aesthetically pleasing and convenient to access with a simple navigable interface, accessible information, adjustable font and image size, and downloadable information for printing. Difficulty using the service due to limited technological proficiencies (n = 10) and medical complications following the transplant, such as decreased dexterity and vision changes (n = 4), was identified as potential barriers to implementation.
Discussion
We found that HCPs had a positive attitude toward digital health interventions to support physical activity in transplant recipients. They indicated that digital programs may increase access to information and reduce costs, which could overcome common barriers to physical activity.1,7 An increase in familiarity with electronic devices and better internet access provides an opportunity for a digital intervention to reach populations for whom access to in-person physical activity counseling, fitness facilities, and qualified exercise personnel can be a challenge. 17 Many desired features such as evidence-based physical activity information, individualized exercise programs, self-monitoring abilities, a secure digital platform, and so much more that could support physical activity among transplant recipients were highlighted by HCPs in this study. These data are valuable to the development of a digital health intervention that supports physical activity among transplant recipients.
The participants believed that a digital intervention could be an effective adjunct to current physical activity counseling practices by providing up-to-date, evidence-based information, and empirical data for HCPs to review with patients in hopes to promote self-management. Many HCPs thought that monitoring health data such as physical activity, medications, vital signs, diet, sleep, and mood was necessary, which was similar to transplant recipients. 11 These features have the potential to improve communication between clinicians and transplant recipients by facilitating follow-up when a patient was not exercising appropriately or when the patient had questions about their lifestyle behaviors. Previous studies support the role of digital health interventions in fostering self-management, for a variety of chronic conditions 19 and transplant recipients specifically.9,11 Digital interventions that incorporate behavior change strategies, 18 such as goal setting (BCT 1.1), feedback (BCTs 2.1-2.7), and action planning (BCT 1.4), are particularly effective in promoting self-management and physical activity adherence.13,20 Technological proficiencies, health literacy, and cultural factors must be further investigated to design a successful service that can be utilized by diverse groups.21,22
The features that were identified as most important for physical activity counseling included individualized exercise recommendations, physical activity guidelines specific for transplant recipients, and home programs with images or videos of exercises. The literature consistently suggests that lack of knowledge and access to exercise recommendations and limited access to formal exercise facilities are barriers to participation in physical activity for transplant recipients.1,7 We also found that transplant recipients expressed a need for safe and evidence-based activity guidelines as a desirable feature in a digital health intervention. 11 Based on a recent meta-analysis, there is strong evidence suggesting that exercise training is effective in improving exercise capacity and health-related quality of life in transplant recipients. 4 Current evidence-based recommendations for exercise in transplant 23 can be incorporated into the design of digital health interventions. 23
A clinician's ability to follow-up with transplant recipients is a desired feature of a digital health intervention. However, HCPs in this study had diverse perspectives about the degree to which they wanted to interact with the tool. Some expressed concerns around how the time spent learning to use the technology and monitoring data collected by the tool might negatively impact their workflow. Indeed, time spent interacting with previous digital health interventions regularly surpass staff resources and may not be accepted by HCPs if it impeded or creates duplicative work.24,25 However, a recent study where 26 a telehealth intervention for kidney transplant recipients that were developed with the input of patients and HCPs suggested the implementation of a digital intervention was not disruptive to clinician workflow and helped to create an effective collaboration between patients and HCPs posttransplant. 26
Although digital health interventions provide a convenient and mobile platform, there are potential risks regarding the privacy of health information associated with data sharing. 13 At the same time, many of the transplant participants in our previous study believed that the ability to share data with their HCPs would be an asset in a digital program. 11 Therefore, to gain widespread use, the tool must protect health data and be safe for patients to use. A third-party application developer may be helpful in managing security and data technology risks. 24 Although the respondents consulted in that study did not discuss regulatory bodies, their concerns related to having control over the nature of data that may be shared, and which members may be granted access to that data.
Some limitations of this study should be considered. Our sample may not be fully representative as there were only 2 interviews conducted in French and HCPs from only 4 Canadian provinces were represented in our sample. Additionally, more women than men were included in the sample. Since the professions represented are more dominated by women, 27 this was representative of the population of HCPs in the field. Snowball sampling was employed to help recruit the specialized HCPs required for this study. This type of recruitment may lead to potential sampling bias by limiting the diversity of participants, as subjects tend to refer to individuals within similar organizations. We did not probe specifically on features that may be desired in the early versus late postoperative phases after transplant, and few of HCPs had experience counseling transplant recipients over the longer term (ie, more than 6 months posttransplant); therefore, their responses may pertain more to counseling transplant recipients on physical activity in the early posttransplant phase. There may be differences in how physical activity was supported in the early versus late phases after transplant, which could be explored in future studies. Lastly, this study was conducted prior to the COVID pandemic, and perspectives regarding digital health barriers may have changed as HCPs and patients have become more familiar with using digital health interventions.
Conclusion
Our findings revealed that HCPs perceive that a digital health intervention could be beneficial to promote physical activity in the transplant population, citing physical activity and exercise features, credibility, self-management, and user engagement as the most important features. This information can be used in the design of a digital health intervention to support physical activity. The main perceived barrier to implementing a digital health intervention was the potential increased work demands on HCPs. Future research should be conducted to examine the implementation of a digital health intervention that promotes physical activity behaviors, and its impact on workflow in transplant clinics, as well as health outcomes.
Supplemental Material
sj-docx-1-pit-10.1177_15269248221145039 - Supplemental material for A Qualitative Study of the Perspectives of Healthcare Professionals on Features of Digital Health Interventions to Support Physical Activity in Solid Organ Transplant Recipients
Supplemental material, sj-docx-1-pit-10.1177_15269248221145039 for A Qualitative Study of the Perspectives of Healthcare Professionals on Features of Digital Health Interventions to Support Physical Activity in Solid Organ Transplant Recipients by Lauren Handler, Paula Jaloul, Jessica Clancy, Brittany Cuypers, Jayme Muir, Julia Hemphill, Tania Janaudis-Ferreira, Chaya Gottesman, Lisa Wickerson, Mike Lovas, Joseph A. Cafazzo and Sunita Mathur in Progress in Transplantation
Footnotes
Acknowledgments
The authors acknowledge Catherine Tansey PhD for assistance in conducting interviews in French.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Donation and Transplantation Research Program (CDTRP).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.