
Abstract
Objectives:
Living with severe lung disease like chronic obstructive pulmonary disease (COPD) is a very stressful situation. The way patients cope may impact their symptoms of anxiety and depression and physical function as well. We studied how ways of coping are associated with levels of emotional distress and lung function in patients with COPD being evaluated for lung transplantation.
Methods:
Sixty-five (mean age 57 years, 46% females) patients completed the General Health Questionnaire-30 (GHQ-30) assessing emotional distress and the Ways of Coping Questionnaire. Measurements of lung function and 6-minute walk test were included.
Results:
Seventeen (26%) patients had elevated emotional distress. Logistic regression of chronic GHQ score with gender, age, body mass index, lung function, and coping scales as covariates showed that escape avoidance and self-controlling coping and forced vital lung capacity were significantly associated with high emotional distress. Odds ratio of emotional distress increased with 5.2 per tertile (P = .011) in escape avoidance coping score. Moreover, we revealed that emotionally distressed patients cope with their current situation by refusing to believe the current situation and taking their distress out on other people.
Conclusion:
Among patients with COPD, a high level of emotional distress was uniquely associated with escape-avoidance coping and lung function. Future work should ascertain whether coping style predicts distress or whether distress increases the use of escape-avoidance coping. Nevertheless, our findings indicate that if either element is present, health care professionals should be attentive to the need for interventions to improve patients’ well-being.
Introduction
Living with end-stage lung disease like chronic obstructive pulmonary disease (COPD) and being assessed for lung transplantation are potent stressors. Knowing that one’s health will gradually deteriorate, continuously struggling with breathing due to impaired lung function, and additionally knowing that premature death will occur in the absence of a transplant, create an untenable situation for most patients. 1 –3 Stressors associated with evaluation for transplant maybe not knowing if one will be accepted for listing, worrying about changes to future life plans and financial strain. 4,5
We previously reported that 35% of individuals presenting for lung transplant evaluation had symptoms of anxiety and depression. 6 Such emotional distress has been reported to increase the frequency of physical symptoms among lung transplant candidates. 7 However, to the best of our knowledge, no previous studies have addressed the way patients cope with living with severe COPD when being assessed for lung transplantation.
Lazarus and Folkman hypothesized that people primarily use 2 broad classes of coping strategies—problem focused (active) and emotion focused (passive). They also hypothesized that the way individuals assess a situation will influence their ways of coping. Literature on coping with physical illness suggests that individuals with high levels of emotional distress apply different ways of coping than those without distress; like more frequent use of avoidant coping (passive coping strategies). 8,9 Studies of patients with COPD have found that better quality of life is associated with more active coping strategies, and this association is independent of COPD severity as assessed by objective lung function. 10 Emotion-focused strategies, such as escape-avoidance coping, has been associated with increased emotional distress in patients awaiting lung transplant 9 and are thus regarded as maladaptive. Few data are available to fully characterize the range of coping strategies used by patients in need of lung transplantation and further how maladaptive coping may affect medical outcomes after transplantation. We believe that more information on how patients cope with living with severe COPD such as the emotional impact of the disease and the associated physical impairment may provide important knowledge that might be used to tailor interventions. 11
Given these gaps in the knowledge base, the first aim of this study is to describe the associations between ways of coping and emotional distress in patients with COPD undergoing evaluation for lung transplantation. As found in our previously published report, COPD was the most common lung disease and meets what is known worldwide. 6,12 Our second aim is to study associations between avoidance-focused coping and high level of distress. To provide detailed information about ways of coping, we also wanted to analyze key items included in the coping scales in relation to levels of distress.
Material and Methods
Design
Data included in this cross-sectional, descriptive study constitute part of the routine assessment of patients evaluated for lung transplantation. Patients provide general informed consent for the requisite medical and psychological-psychiatric assessments needed as part of their workup for possible listing for transplantation. In Norway, routinely collected data, such as for this cohort, may be published without additional informed consent. The compilation of data for this publication was approved by the Hospital’s data protection officer.
Setting
All organ transplantations are performed in a single center that serves the entire Norwegian population. For lung transplantation selection, a standard protocol recommended of the International Society for Heart and Lung Transplantation was followed. 13 Patients were evaluated over a 12-day period by the Lung Transplantation Unit at the hospital. When patients meet medical criteria for lung transplantation, they were referred for psychosocial evaluation performed by a mental health professional from Division of Mental Health and Addiction. The present study was performed using a data collection protocol that was integrated into patients’ evaluation for transplant candidacy in 2006.
Population
Yearly, approximately 30 to 35 lung transplantations take place. The 5-year survival rate in the years 2000 to 2013 was 67.6% in a Scandinavian study. 14 All patients at the transplant center were Caucasians, adults, with end-stage lung diseases like COPD, idiopathic pulmonary fibrosis, cystic fibrosis, pulmonary hypertension, sarcoidosis, and lymphangioleiomyomatosis. Most transplants were double.
The inclusion criteria for the current study were patients with COPD evaluated for lung transplantation. Among the 121 Caucasian patients who acquired lung disease as adults, undergoing evaluation for lung transplantation between 2006 and 2010, 118 patients were included in our sample. Of the patients, 74% had COPD, while 14% had idiopathic fibrosis and 12% had rare lung diseases. Mean age for the total group was 54.4 years. 6
Data Collection
Ways of Coping
Coping was measured by The Ways of Coping Questionnaire (WCQ). The WCQ was translated from English to Norwegian and back-translated to ensure accuracy. The 66-item WCQ assesses thoughts and behaviors people use to deal with the internal and/or external demands of specific stressful situations. Respondents were asked to think about their current situation, that is, living with severe lung disease, and rate how often they used each coping activity (0 = does not apply or not used, 1 = used somewhat, 2 = used quite a bit, 3 = used a great deal). Items are summed, with higher score indicating more frequent use. The WCQ includes 8 different coping scales. Four scales reflect active, problem-focused (adaptive) coping: seeking social support (ie, seek informational support, tangible support, emotional support), accepting responsibility (ie, acknowledging one’s own role in the problem), planful problem-solving (ie, deliberate problem-focused efforts to alter the situation), and positive reappraisal (ie, efforts to create positive meaning by focusing on personal growth). Four scales reflect emotion-focused passive (maladaptive) coping: confrontive coping (ie, aggressive and potentially antagonistic efforts to alter the situation), distancing (ie, cognitive efforts to detach oneself and to minimize the significance of the situation), self-controlling (ie, efforts to regulate one’s feelings and actions), and escape-avoidance (ie, wishful thinking and behavioral efforts to escape or avoid the problem).
In our sample, 3 scales (1 reflecting active coping and 2 reflecting passive coping) had adequate internal consistency reliability (α ≥ .60) for inclusion in our analyses: planful problem-solving (6 items; α = .65), self-controlling (7 items; α = .72), and escape-avoidance (8 items; α = .69).
General Health Questionnaire-30
Emotional distress was measured by the 30-item General Health Questionnaire (GHQ-30), addressing the past 2 weeks. The GHQ-30 is a widely used measure of distress that is particularly useful for assessing psychological distress in patients with chronic physical disease because it does not include somatic items. Each GHQ item is rated on a Likert scale (0 = less distress than usual, 1 = same as usual, 2 = more distress than usual, 3 = much more distress than usual). Rather than the typical approach of summing the items to yield an overall measure of distress, we calculated the chronic score (cGHQ-30). This approach takes into account the possibility that the patient’s usual status for the 15 GHQ items that are worded in a negative direction (Likert scale ratings of 1 on the 0-3 scale) would reflect experiencing the symptom on an ongoing or chronic basis. If a person rates their feeling that “life is entirely hopeless” is the “same as usual,” this indicates the presence of chronic distress. In contrast, for the 15 GHQ items that are not worded negatively (eg, feeling “able to concentrate on whatever you are doing”), a rating of “same as usual” would not necessarily indicate the presence of chronic, ongoing distress. The cGHQ score is calculated to reflect the level of chronic distress an individual is experiencing. It is calculated by (a) dichotomizing each negatively worded GHQ items into “less distress than usual” (a value of 0) versus either the “same,” “more,” or “much more” distress than usual (a value of 1) and (2) dichotomizing the remaining positively worded GHQ items into “less distress than usual” or “same as usual (a value of 0) versus “more” or “much more” distress than usual (a value of 1). The 30 dichotomous items are summed and the range of total cGHQ-30 score is 0 to 30 and with Cronbach α in the present sample of .89.
The cGHQ-30 has 5 subscales including 25 of the 30 items: (1) anxiety, reflecting worry and tension (8 items); (2) well-being, reflecting feelings of lack of competence and low self-esteem (4 items); (3) depression, reflecting unhappiness and hopelessness (5 items); (4) difficulty in coping, reflecting inability to manage problems (5 items); and (5) social dysfunction, reflecting difficulties in interpersonal relationships (3 items). Only the 3 subscales with α ≥ .60 were used in our study (depression, α = .76; anxiety, α = .81; and well-being, α = .73).
Based on our previous studies of cGHQ, 6 we dichotomized the patients in 2 groups. Patients with a total score of ≥17 were considered to have high levels of emotional distress (n = 17; 26%). Mean cGHQ-30 score was 20.2 (SD = 3.1). The remaining patients were considered to have low distress (n = 48; 74%); mean cGHQ-30 score 9.3 (SD = 4.4). Finally, we dichotomized cGHQ with cutoff at 15 and 19 to explore whether these cutoff points would yield different results.
Lung function
Lung function was assessed by spirometry: Forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) were reported as percent of predicted values. The principal variable, FEV1, is a measure of airway obstruction. The 6-minute walk test (6MWT) measures the maximum distance (in meters) a patient can walk on a flat hard surface in 6 minutes. 15 The 6MWT is currently the best indicator for physical function for patients awaiting lung transplantation. 16 The spirometry data and 6MWT were collected at the hospital’s pulmonary laboratory by trained nurses.
Procedure
The data were collected as part of the routine evaluation. At time of assessments, none of the patients knew if they would be accepted for the waiting list.
Statistical Analyses
We compared high emotional distress (cGHQ-30 ≥ 17) versus low distress (cGHQ-30 < 17) groups on relevant covariates by emotional distress using χ2 tests for categorical covariates and t tests for continuous covariates. Given our limited sample size, we required Covariates to be associated with emotional distress with a corresponding P value <.2 or smaller to be included in a multivariate logistic regression analysis using emotional distress as the outcome variable. A P value <.20 is frequently used as an inclusion criterion for this purpose. 17 Variables included in the initial logistic regression model were self-controlling coping, escape-avoidance coping, planful problem-solving coping, FEV1, FVC, and covariates to be controlled including age, gender, and body mass index (BMI). We chose to categorize continuous explanatory variables into tertiles to reveal a dose–response relationship between the outcome and the explanatory variables. This initial regression model was then reduced by backward elimination, provided that the covariate was not significant (P < .05) and that removal did not change the association between emotional distress and coping variables more than 20%.
Examining the effect of using the alternative cut-points for dichotomizing the cGHQ-30 score, we repeated the multivariate regression analyses with these alternative outcomes.
To reduce type 1 error, we applied Bonferroni correction (P = .05) when we studied associations between escape-avoidance coping scale and cGHQ-30 single items and between cGHQ total score and single items in the escape-avoidance and the self-controlling scales. The adjusted Bonferroni P value required for significance was < .006 for escape-avoidance single items (ie, P of .05/8 items) and < .007 (.05/7) for self-control single items. The adjusted Bonferroni P value required for cGHQ single item scale (P of .05/30 items) was <.002. Data were analyzed using Stata version 14.2 (StataCorp LP).
Results
Fifteen of the 87 patients with COPD included in this study did not complete questions about coping. Among the 72 patients with available coping data, 7 patients did not complete questions about distress, leaving 65 (75%) to be included in our analysis.
There were no significant sociodemographic or clinical differences between the 65 patients included and those patients not included, except that those 22 not included had a higher level of education (P = .004; see Supplement Table 1).
Table 1 presents the distribution of sociodemographic variables among the 65 patients with either high (cGHQ ≥ 17) or low (cGHQ < 17) emotional distress. The FVC (% of predicted) and FEV1 (% of predicted), but not 6MWT, were significantly lower in patients reporting high emotional distress. Patients reporting high distress had significantly higher mean scores on the coping scales self-controlling and escape-avoidance. Both self-controlling and escape-avoidance scales were also significantly associated with the 3 cGHQ-30 subscales: anxiety, depression, and well-being. Self-controlling scale: anxiety β = .15 (95% CI: 0.07-0.24, P = .001), depression β = .14 (95% CI: 0.04-0.24, P = .007), and well-being β = .11 (95% CI: 0.02-0.21, P = .019). Escape-avoidance scale: anxiety β = .13 (95% CI: 0.04-0.22, P = .004); depression β = .20 (95% CI: 0.11-0.29, P < .001), and well-being β = .11 (95% CI: 0.01-0.20, P = .027).
Demographics, Lung Function, and Coping Scales Scores Among Patients With High Versus Low Emotional Distress (CGHQ-30 cutoff ≥17).
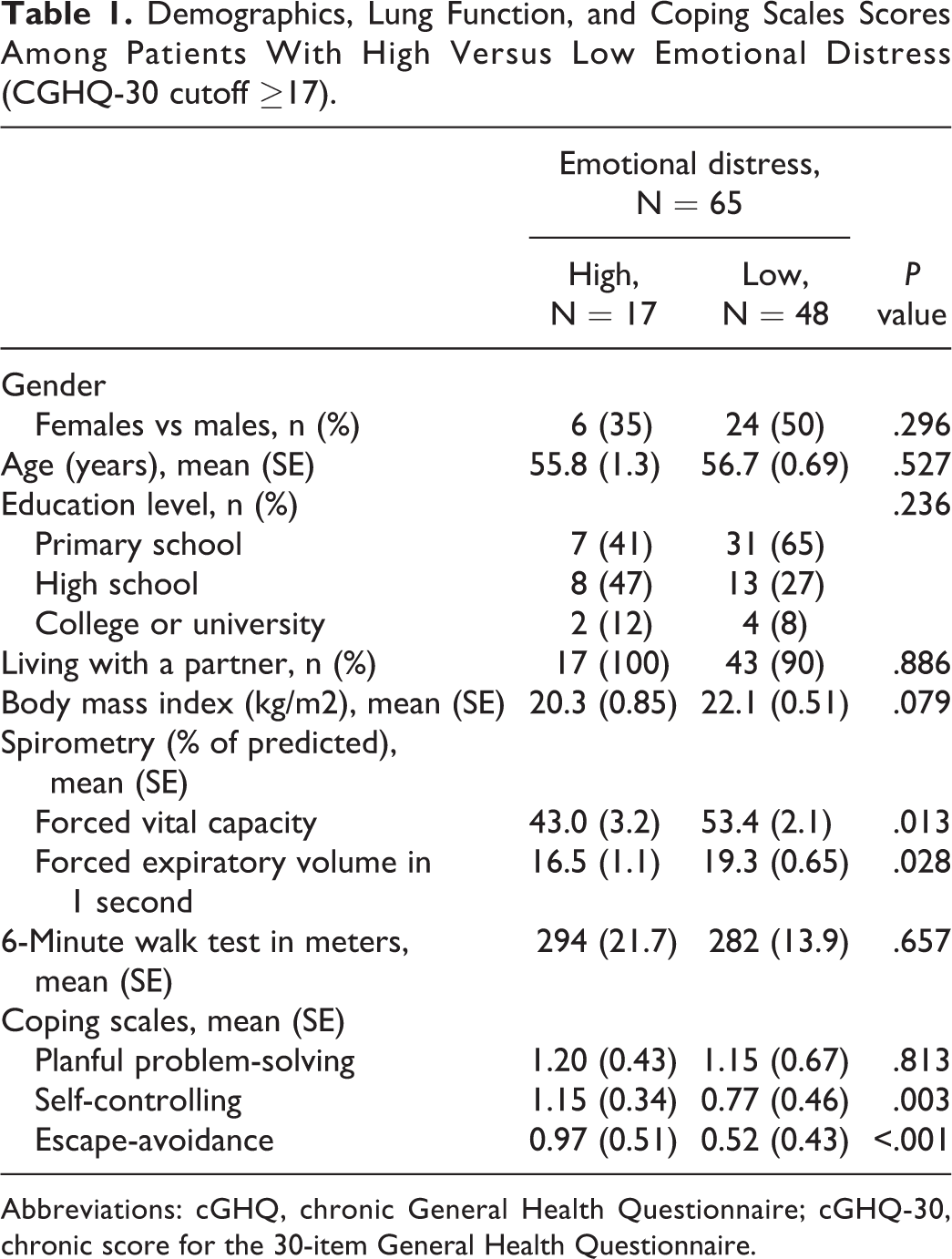
Abbreviations: cGHQ, chronic General Health Questionnaire; cGHQ-30, chronic score for the 30-item General Health Questionnaire.
When exploring the alternative cutoff points for the cGHQ score, we found a cutoff at 15; 25 (38%) patients were classified with high distress. The association between cGHQ and escape-avoidance was P = .002 (95% CI: 0.45-1.91), β = 1.2. When the cutoff was set at 19, 11 (16.9%) patients were classified with high distress. The association between cGHQ and escape-avoidance was P = .011 (95% CI: 0.29-2.31), β = 1.3.
In the final logistic regression model of cGHQ-30 score (dichotomized at 17) with gender, age, BMI, lung function, and coping scales as covariates, high scores on escape-avoidance and self-controlling coping scales were significantly associated with high cGHQ-30 scores. The FVC was also significantly associated with cGHQ-30 (Table 2). With this logistic regression model, we calculated that 90% of the sample was correctly classified based on these predictors (sensitivity 81%, specificity 93%).
Odds Ratio of Emotional Distress With Gender, Age, Body Mass Index, Lung Function, and Emotional Coping Scales as Covariates Using Multivariate Logistic Regression.a
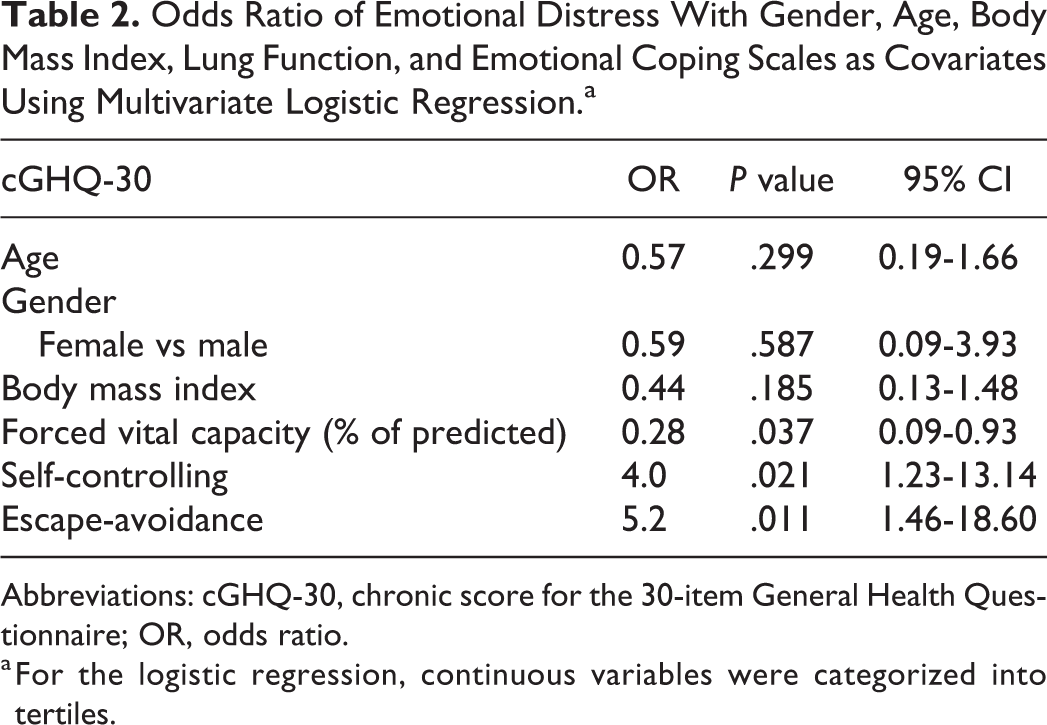
Abbreviations: cGHQ-30, chronic score for the 30-item General Health Questionnaire; OR, odds ratio.
a For the logistic regression, continuous variables were categorized into tertiles.
Similarly, multiple linear regression model with cGHQ-30 score as the dependent variable (see Supplement Table 2) revealed a strong positive association between cGHQ-30 score and escape-avoidance coping scale β = 4.8 (95% CI: 1.66-7.95, P = .003), respectively for self-controlling β = 3.6 (95% CI: 0.33-6.93, P = .032). The FVC was not significant in this model β = .10 (95% CI: 0.20-0.002, P = .054).
To explore feelings connected to escape-avoidance coping, we studied the associations between the escape-avoidance scale and single items from the cGHQ scale. After Bonferroni correction (P = .002), a multivariate model for escape-avoidance as a predictor of single items from the cGHQ-30 scale showed that escape-avoidance was associated with difficulties in managing oneself to keep busy and occupied β = .445 (95% CI: 0.17-0.72, P = .002) and that life was completely hopeless β = .409 (95% CI: 0.19-0.63, P = .001).
To find out how patients with high level of distress may cope with their distress, we looked at differences in scores on the single items of the 3 coping scales (planful problem-solving, escape-avoidance, and self-controlling) between those with high and low emotional distress. We found no significant differences in the planful problem-solving scale. Among the 8 escape-avoidance single items, 5 had higher mean scores among those with high levels of distress. Three of the escape-avoidance single items survived Bonferroni correction (Table 3). Among the self-controlling scale, 3 of 7 single items were significantly different, but none of the self-controlling single items survived the Bonferroni correction.
Mean cGHQ-30-Score in the Total Cohort (N = 65) for Patients With High (N = 17) Versus Low (N = 48) Emotional Distress in 3 of 8 Single Items From Escape-Avoidance Scale That Are Significantly Different After Bonferroni Correction.
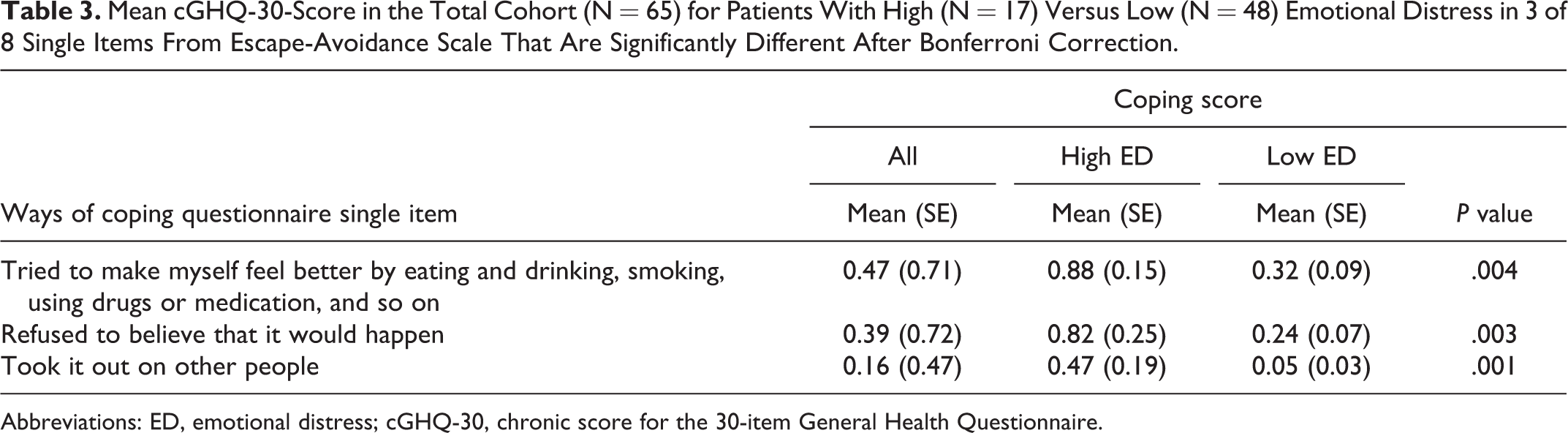
Abbreviations: ED, emotional distress; cGHQ-30, chronic score for the 30-item General Health Questionnaire.
Discussion
The main findings in this study are that high emotional distress was significantly associated with escape-avoidance and self-controlling coping as well as lung function in patients with COPD being evaluated for lung transplantation. Our hypothesis about the association between emotional distress and escape-avoidance coping was supported.
Given the multiple uncontrollable stressors associated with advanced lung disease and the lung transplant evaluation, it is not surprising that patients would experience psychological distress and that such distress would be associated with efforts to use emotion-focused coping. Specifically, we found significant associations between cGHQ-30 subscale well-being (ie, low self-esteem) and escape-avoidance coping and self-controlling coping. Low self-esteem and maladaptive coping may have impact on how patients assess their situation on waiting list. 18 Low self-esteem may also affect medical adherence after transplantation and thereby indirectly impact posttransplant outcomes. 18 Tailored psychological support using strategies to empower self-esteem on waiting list might be explored in future studies.
The nonsignificant associations between level of distress and 6MWT are noteworthy but may stem from lack of individual variation in walking distance in the sample. Although we did not find an association between FEV1 and emotional distress in our final regression analyses, we did observe that poorer FVC was associated with emotional distress. To the best of our knowledge, this is a novel finding that needs an explanation: Whereas FEV1 is mostly determined by airways resistance, FVC is mostly determined by static lung volumes. It may be possible that patients with high emotional distress stop their expiration before they reach their total lung capacity and thereby have lower FVC. This interpretation must be taken with caution since we did not measure static lung volume.
Interestingly, we found that a subgroup of patients with high levels of distress cope with their current situation by avoiding being with people, refusing to believe the current situation, and taking their distress out on other people. No previous study has addressed ways of coping in patients being evaluated for lung transplantation. Our finding is along the same line as those reported in a study of patients with COPD being accepted for transplantation. Myaskovsky et al 9 found that avoidant coping was associated with depression and Taylor et al 19 differentiated between active coping and disengagement. The latter was defined as behavioral and mental disengagement, denial, and venting. This concept overlaps partly with the concept escape-avoidance coping.
Change in coping may constitute a significant area of focus of change in psychotherapy and other behavioral interventions. 20 It has also been shown that psychological intervention in patients completing a pulmonary rehabilitation program may reduce anxiety and depression and improve physical function (6MWT). 21 Most psychological interventions aim at changing the appraisals of the situation and encourage directly facing anxiety and fears, that is, mainly problem-solving approaches. For most patients, such adaptive coping may reduce distress and improve pain-related functioning. 22 However, some patients find these recommendations too challenging to fulfill. Such difficulties as following prescription for physical activities in order to improve or maintain their physical status as long as possible may be explained by increased emotional distress. 23,24 In line with those findings, lung patients with high level of escape-avoidant coping respond poorly to such approaches. 25 Research has found that external locus of control, that is, feeling that one is under the control of others rather than oneself, is crucial to the outcome and is associated with both dependency on others and helplessness. 26 Those observations are put into perspective by recent research reporting reducing maladaptive coping seems to be more important for outcome than enhancing adaptive coping. 27
We believe that our study may imply that intervention to reduce escape-avoidance may be the most efficient approach to reduce distress. Psychoeducation may be one intervention to improve outcome in patients with lung diseases. 10,28,29 However, given our cross-sectional data, future prospective studies are needed to fully determine whether the factors that we studied are predictive of psychological distress. Nevertheless, given the limited work on the role of coping in relation to distress in lung transplant candidates, and posttransplant outcomes, we believe that our work makes an important contribution in this field.
The main strength of this study is our ability to identify patients from a national cohort who all received a similar, standardized psychosocial evaluation. Another asset is the combination of data on specific coping items with a distress measure less sensitive to concurrent physical symptoms.
The study comes with some limitations as well. The cross-sectional design and that only 3 of 8 coping scales had adequate internal consistency reliability to be included in the current study, limited our ability to examine a full range of coping behaviors. We did not systematically collect data about how patients experienced being on waiting list, including the stressors we have discussed above. Our data collection ended over 10 years ago. However, it should be noted that in Norway, criteria for being accepted for lung transplantation have not changed significantly; thus, our findings should still be of relevance.
The cutoff point of the outcome cGHQ-30 (distress score ≥17) may be questioned. Therefore, we investigated 2 alternative cutoff points at 15 and 19. They did not notably change the findings.
It is possible that advances in pharmacotherapy for COPD may have resulted in a reduction in distress levels in patients evaluated more recently than those in our study, thus potentially reducing the generalizability of our findings. Recent evidence suggests that anxiety remains a significant problem for patients with COPD despite the availability of newer medications. 30
Conclusion
Among patients with COPD undergoing evaluation for lung transplantation, a high level of emotional distress was uniquely associated with escape-avoidance coping and lung function. Future work should ascertain whether coping style predicts distress or whether distress increases the use of escape-avoidance coping. Nevertheless, our findings indicate that if either element is present, health care professionals should be attentive to the need for interventions to improve well-being among patients in need of lung transplantation.
Supplemental Material
Supplemental Material, 5_19-0132_Supplement_Table_1_R2_final_rpw - Coping Patterns and Emotional Distress in Patients With Chronic Obstructive Lung Disease Who Are Undergoing Lung Transplant Evaluation
Supplemental Material, 5_19-0132_Supplement_Table_1_R2_final_rpw for Coping Patterns and Emotional Distress in Patients With Chronic Obstructive Lung Disease Who Are Undergoing Lung Transplant Evaluation by Torunn S. Soyseth, Mary Amanda Dew, May Brit Lund, Gro Killi Haugstad, Vidar Soyseth and Ulrik Fredrik Malt in Progress in Transplantation
Supplemental Material
Supplemental Material, 6_19-0132_Supplement_Table_2_R2_final_rpw - Coping Patterns and Emotional Distress in Patients With Chronic Obstructive Lung Disease Who Are Undergoing Lung Transplant Evaluation
Supplemental Material, 6_19-0132_Supplement_Table_2_R2_final_rpw for Coping Patterns and Emotional Distress in Patients With Chronic Obstructive Lung Disease Who Are Undergoing Lung Transplant Evaluation by Torunn S. Soyseth, Mary Amanda Dew, May Brit Lund, Gro Killi Haugstad, Vidar Soyseth and Ulrik Fredrik Malt in Progress in Transplantation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.