
Abstract
Chronic venous disease (CVD) of the lower extremities comprises a spectrum of venous disorders leading to ambulatory venous hypertension and inflammation due to obstruction, reflux, or both. Chronic venous disease is the leading cause of venous leg ulcers. This case report presents a 72-year-old man who presented with recurrent bilateral malleolar venous ulcers associated with 3 pathological processes, each contributing to ambulatory venous hypertension.
Clinical Impact
This case report suggests that numerous factors can contribute to ambulatory venous hypertension and by extension venous ulceration.
Case Report
A 72-year-old male with an extensive medical history, including hypertension, paroxysmal atrial fibrillation on oral anticoagulation, heart failure with preserved ejection fraction, a history of aortic aneurysm with aortic root replacement and aortic valve replacement, and chronic venous insufficiency with recurrent bilateral venous ulcers since 2016. He was treated in the wound care clinic for a bimalleolar venous ulceration. Treatment included 3-layer compression and Unna boots. The ulceration would heal for a time but recur.
For superficial venous reflux, the patient underwent bilateral great saphenous vein (GSV) ablations in 2016. The patient had temporary minimal improvement in the ulceration. For recurrence of ulceration, the patient underwent multiple interventions, including a bilateral small saphenous vein (SSV) ablation in 2020 and sclerotherapy in 2021 to the sub-ulcer plexus and associated varicose veins. The ulceration regressed for approximately 6 months before recurring. Repeat reflux studies revealed incompetent anterior GSVs, which were ablated in 2022. The patient was followed closely in the wound care clinic, receiving evidence-based ulcer management and adhering to 30 to 40 mm Hg compression stockings or 3-layer bandages.
Despite compression, wound care, and multiple superficial venous interventions detailed above, there were repeat flares in the bilateral medial malleolar ulcers. Bilateral lower extremity edema with venous stasis changes and ulceration was noted (Figure 1).

The recalcitrant venous ulcer of the left ankle, with surrounding inflammation. The right ankle ulcer had a similar appearance.
Computed tomography venogram of the abdomen-pelvis to evaluate for deep venous disease revealed no venous stenosis or occlusion. The inferior vena cava and iliac veins were dilated, with marked cardiomegaly and right atrial enlargement (Figure 2).
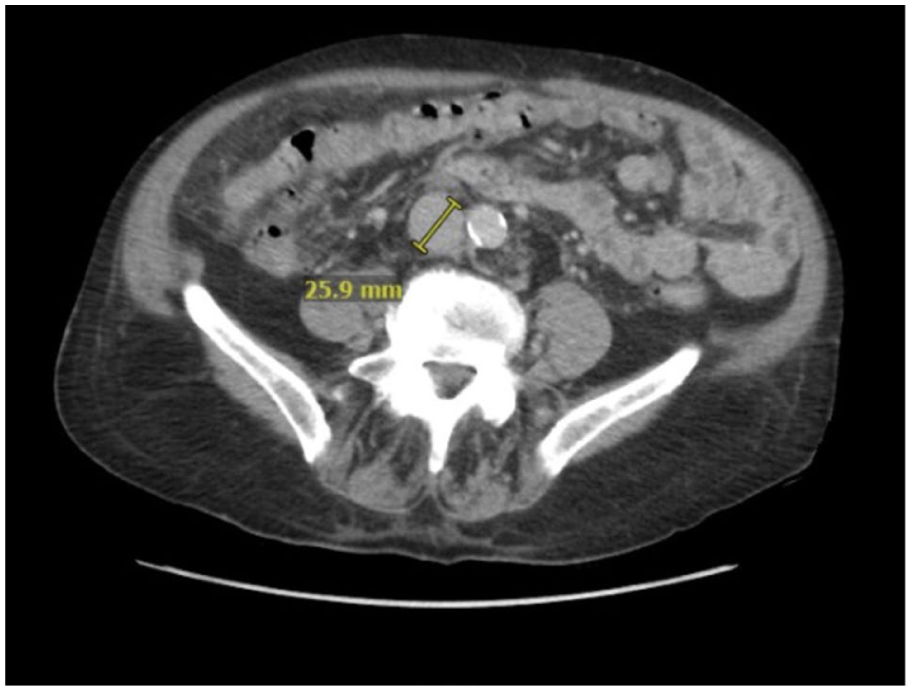
Computed tomography of abdomen-pelvis demonstrating a dilated inferior vein cava.
The patient was also followed by cardiology, with complaints of progressive dyspnea at exertion, paroxysmal nocturnal dyspnea, and abdominal congestion for a year.
Repeat venous duplex studies revealed the absence of superficial reflux with occluded saphenous veins bilaterally. However, severe bilateral femoral and popliteal vein reflux was noted. Arterial duplex studies and pulse volume recordings and computed tomography angiography did not suggest significant peripheral arterial disease, arteriovenous fistulae, or arteriovenous malformations.
The patient underwent transthoracic echocardiography that reported severely increased right ventricular cavity size, elevated right ventricular systolic pressure (53 mm Hg, normal <35 mm Hg), and severe tricuspid regurgitation (Figure 3).
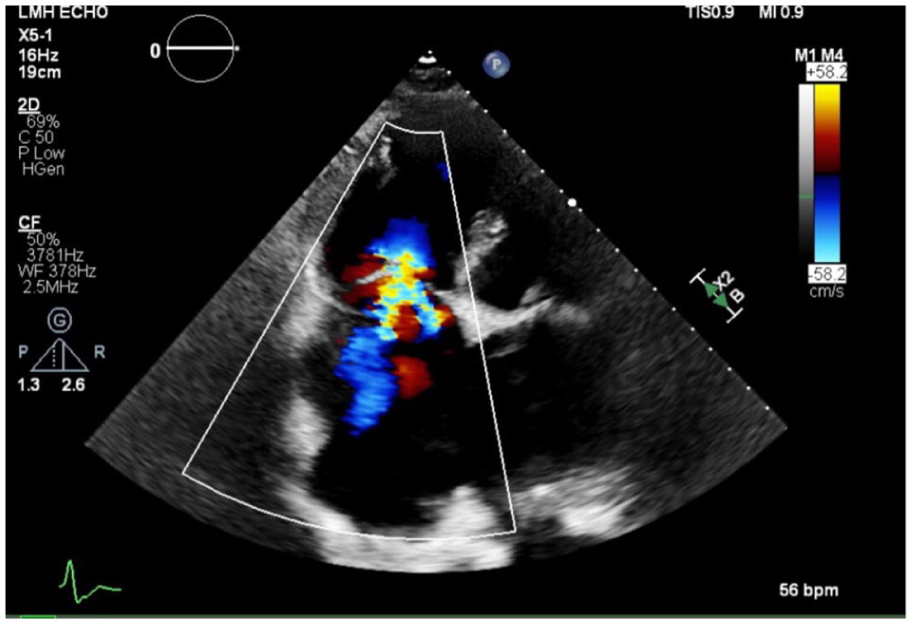
Echocardiogram revealing severe tricuspid regurgitation and increased right ventricular size.
The patient was diagnosed with recalcitrant venous ulceration associated with ambulatory venous hypertension, in turn associated with deep vein reflux, pulmonary hypertension, and severe tricuspid regurgitation. The presence of deep vein reflux likely further exacerbated the ambulatory venous hypertension.
Phosphodiesterase-5 inhibitors were not initiated, as the primary etiology for pulmonary hypertension was deemed to be left-sided heart disease. Biopsy was considered but not performed, as the treating team felt that removing tissue in a patient with ambulatory venous hypertension may further enlarge the ulcer and not heal. The patient’s ulcers would only regress and remain healed following a course of oral corticosteroid therapy that was then maintained. Cessation of steroids would be followed, within 2 weeks, by ulcer recurrence.
The patient provided consent for the publication of this manuscript.
Discussion
Chronic venous disease is the leading cause of venous leg ulcers. Treatment includes compression therapy and, where possible, correction of the causes of ambulatory venous hypertension. 1
This case illustrates a patient with pulmonary hypertension with right heart failure who had an initial presentation with bilateral venous ulcers. He underwent multiple invasive procedures including bilateral truncal vein ablations that did not lead to long-term ulcer healing. Despite these interventions, the persistence of venous ulcers and emergence of deep vein reflux indicated that superficial vein ablation alone was insufficient to improve the underlying venous hypertension.
From the cardiac standpoint, the findings of marked cardiomegaly and right heart enlargement, alongside with elevated right ventricular systolic pressure, pointed toward the diagnosis of pulmonary hypertension, which can be a consequence of chronic heart failure and valvular disease. 1 The severe tricuspid regurgitation observed on the echocardiogram, secondary to the right ventricular dilation and increased pressure, further complicates the patient’s clinical status. Tricuspid regurgitation can exacerbate venous congestion, leading to worsening lower extremity edema and formation of ulcers. The patient experienced a vicious cycle of venous and cardiac dysfunction with resultant ambulatory venous hypertension and recalcitrant ulceration. The patient received medical therapy including diuretics for his chronic heart failure. He was not deemed a suitable candidate for tricuspid valve repair due to his frailty. The potential correlation between chronic venous insufficiency and congestive heart failure has been suggested in the literature, although it is unclear whether this relationship is attributable to shared risk factors among those affected.2,3
Compression therapy with multi-layer bandages (30-40 mm Hg) was employed for this patient without adverse cardiovascular effects. Studies on stable patients with heart failure have supported the safety of compression therapy.4,5
Ambulatory venous hypertension is associated with inflammation. By extension, as treating the venous hypertension remained challenging, we sought to medically treat the inflammation with oral corticosteroids. The only treatment strategy that showed a positive effect was oral corticosteroid therapy.
Management strategies for similar patients with multifactorial disease should include optimizing heart failure treatment, interventions to address deep vein reflux, and employing wound care.
Conclusion
Pulmonary hypertension, when occurring in the setting of tricuspid regurgitation and deep vein reflux in the lower extremity veins, is associated with ambulatory venous hypertension and can lead to recalcitrant ulceration.
Footnotes
Author Contributions
All 3 authors contributed to the conception, writing, editing, and literature search for this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.