
Abstract
Purpose:
Mycotic aneurysms are rare, life-threatening vascular infections that typically result from direct vascular inoculation, including intravenous drug use or vascular access procedures. Hematogenous seeding from a remote musculoskeletal source is distinctly uncommon. This report describes the multidisciplinary management of a mycotic common femoral artery pseudoaneurysm arising from septic ankle arthritis, highlighting key open and endovascular considerations.
Case Report:
A 78-year-old man presented with painful right-groin swelling and septic right-ankle arthritis. Computed tomographic angiography demonstrated a mycotic pseudoaneurysm of the right common femoral artery, and blood and operative cultures grew methicillin-resistant Staphylococcus aureus. He underwent debridement of the infected groin and in situ reconstruction using a reversed femoral vein interposition graft through combined retroperitoneal and thigh exposures. Due to contamination, the groin required secondary wound healing. Chronic popliteal and tibial occlusions were subsequently treated with staged endovascular recanalization and selective stenting using contralateral up-and-over access to avoid stress on the fresh anastomoses. The patient completed a 6-week course of antibiotics, with complete wound healing and return to independent function.
Conclusion:
This case demonstrates the effective combination of autologous in situ femoral vein reconstruction and staged endovascular revascularization for a mycotic pseudoaneurysm in the setting of bacteremia. Multidisciplinary coordination, careful operative sequencing, and rigorous infection control were essential to achieving durable limb salvage.
Clinical Impact
In select cases, complex mycotic aneurysms with peripheral vascular disease can be managed with a staged hybrid approach that combines vascular reconstruction with endovascular intervention, reducing the need for multiple open procedures. Employ a multidisciplinary approach with careful sequencing and access planning to protect grafts, control infection, and optimize limb salvage.
Keywords
Introduction
Mycotic aneurysms represent an uncommon but highly morbid form of vascular infection, accounting for < 1% of all aneurysms and carrying a significant risk of rupture, sepsis, and limb loss if untreated. 1 These infections most frequently arise from bacteremia, contiguous spread, or direct vascular inoculation, with Staphylococcus aureus and Salmonella species among the most commonly implicated pathogens.1,2 Traditional management has involved excision of the infected segment with extra-anatomic bypass. However, contemporary data support in situ reconstruction using autologous vein grafts because of their favorable resistance to reinfection and durable long-term patency.3–5 Endovascular techniques are increasingly used as adjuncts in select patients, though careful attention to infection control remains essential.5,6 Despite these advances, mycotic aneurysms of the common femoral artery (CFA) are rare, and presentations due to hematogenous seeding from remote musculoskeletal infections are exceptionally uncommon. This report describes the multidisciplinary open and endovascular management of a mycotic CFA pseudoaneurysm arising from septic ankle arthritis.
Case Report
A 78-year-old man presented to the emergency department with a 1-week history of progressive swelling and pain in his right groin and right ankle. His medical history included coronary artery disease with a prior right coronary stent placed via radial access, hypertension, hyperlipidemia, non-insulin-dependent diabetes mellitus, stage III chronic kidney disease, and paroxysmal atrial fibrillation on apixaban. He had no history of intravenous drug use, trauma, or recent instrumentation of the affected extremity. He had remote right ankle surgery more than 30 years earlier, with subsequent hardware removal.
On presentation, the patient was afebrile, hemodynamically stable, and nontoxic in appearance. Examination revealed a tender, pulsatile right-groin mass without overlying skin breakdown or erythema. The right ankle was warm, edematous, and significantly tender. Palpable pedal pulses were present only in the left lower extremity; however, in the right foot, Doppler assessment demonstrated a biphasic posterior tibial signal and a monophasic dorsalis pedis signal. The patient was neurologically intact, with no clinical signs of acute limb ischemia.
Computed tomographic angiography (CTA) demonstrated a large, irregular 6.2-cm right CFA pseudoaneurysm extending from the inguinal ligament to the femoral bifurcation. The aortoiliac and superficial femoral segments showed scattered, non-flow-limiting atherosclerosis. The right popliteal artery was chronically occluded, with distal reconstitution of the posterior tibial artery in the proximal calf (Figure 1). Radiographs of the right ankle revealed extensive bony erosions and adjacent soft-tissue infiltration, concerning for osteomyelitis and magnetic resonance imaging confirmed a complex 6-cm soft-tissue collection involving the right tibiotalar joint (Figure 2). Laboratory evaluation revealed mild leukocytosis with markedly elevated inflammatory markers (erythrocyte sedimentation rate, 123 mm/h; C-reactive protein, 174.6 mg/L). Blood cultures obtained at admission subsequently grew methicillin-resistant Staphylococcus aureus (MRSA). The patient was admitted to the vascular surgery service and started on vancomycin and piperacillin-tazobactam. Orthopedic surgery and infectious disease specialists were engaged early. Electrocardiogram and echocardiogram demonstrated atrial fibrillation but no valvular pathology or evidence of endocarditis.
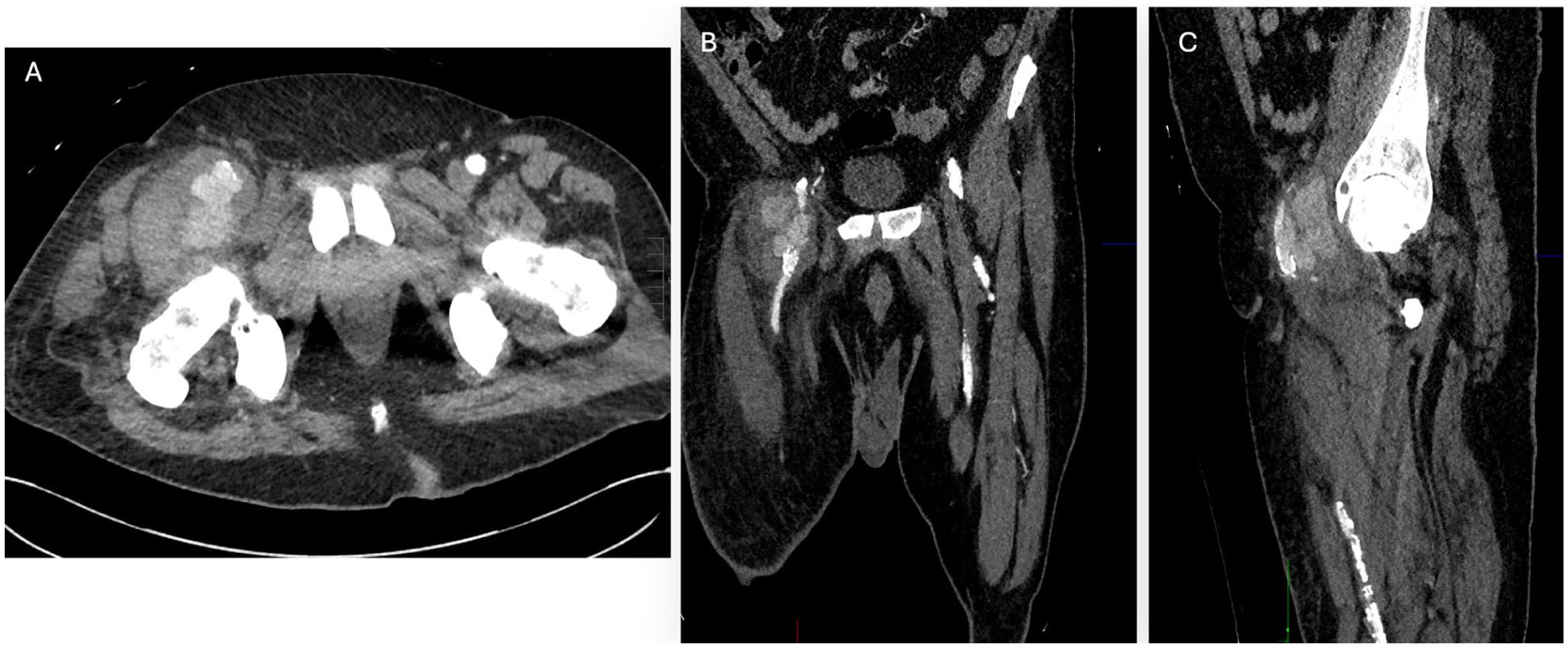
A 6.2 cm right common femoral artery pseudoaneurysm extending from the inguinal ligament to the femoral bifurcation, with scattered, non-flow-limiting atherosclerotic calcification in the aortoiliac segment and superficial femoral artery in (A) axial view, (B) coronal view, and (C) sagittal view.
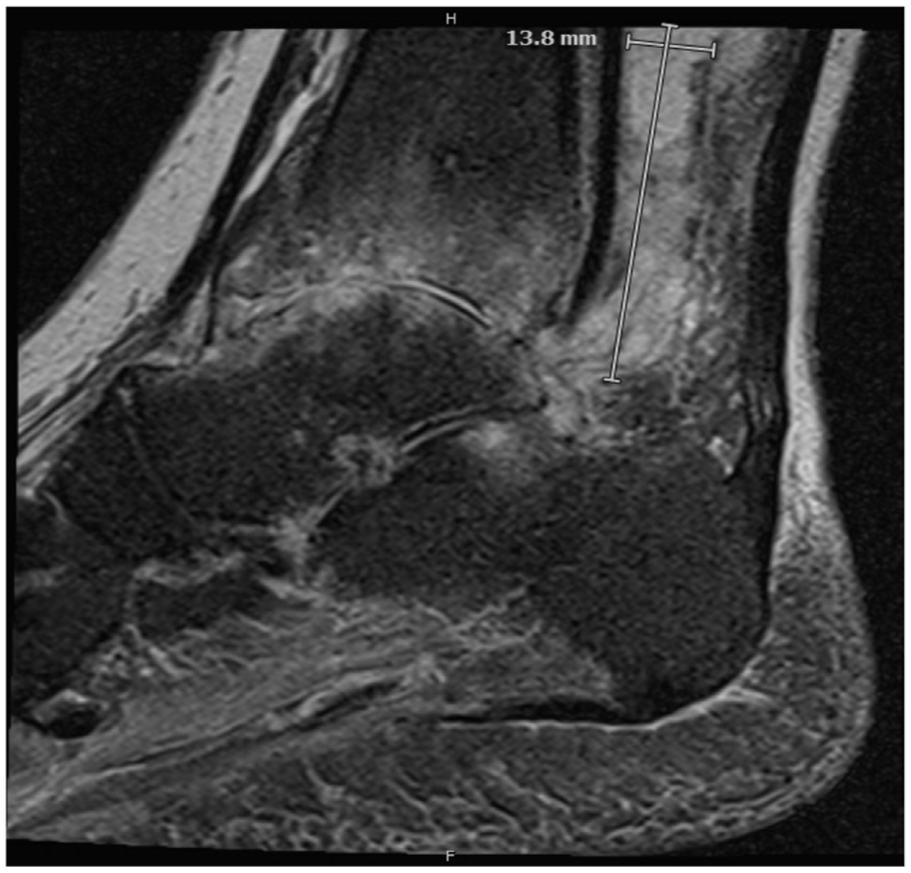
T2 magnetic resonance image of the right ankle showing a complex 6.2 cm (craniocaudal) × 1.4 cm (anteroposterior) × 3.1 cm (transverse) soft-tissue collection involving the tibiotalar joint.
Operative Reconstruction of the Mycotic Pseudoaneurysm
Given the size, location, and infected nature of the lesion, operative repair was undertaken. Proximal control of the right external iliac artery was achieved through a supra-inguinal Gibson-type retroperitoneal approach. Distal control of the profunda femoris and superficial femoral artery was obtained via a separate anteromedial thigh incision guided by intraoperative ultrasound. Preoperative duplex mapping confirmed a suitable, compressible contralateral femoral-popliteal vein, which was harvested to serve as an autologous conduit because of its superior caliber match and durability in an infected, high-flow arterial position.
To address the aneurysm, a longitudinal incision was made over the right groin, extended to join the distal anteromedial thigh incision. The pseudoaneurysm was opened, evacuated, and extensively debrided. An in situ reversed femoral vein interposition graft was constructed from the external iliac artery to the CFA bifurcation. A rotational sartorius flap was transposed to augment soft-tissue coverage. The groin incision was partially closed, and a negative pressure wound therapy device was applied for delayed closure given the contaminated operative field.
Postoperatively, the patient was extubated on postoperative day (POD) 1. He required brief vasopressor support during the first 24 hours but stabilized quickly.
Management of the Infected Ankle
To confirm the ankle as the source of bacteremia, a diagnostic aspiration was performed, yielding gram-positive cocci. On hospital day 6 (POD 4 from femoral reconstruction), the patient underwent right ankle arthrotomy with irrigation and debridement and partial tibial resection. Intraoperative cultures confirmed MRSA, concordant with blood and groin cultures.
Endovascular Revascularization
On hospital day 11, endovascular intervention was performed to treat the chronic popliteal and tibial occlusions and promote wound healing. At this point, the patient had received 11 days of targeted intravenous antibiotics, with clinical stabilization following wide debridement and negative pressure wound management of the right groin. When planning endovascular access, the surgeons took particular care to avoid disrupting the fresh femoral vein interposition graft and its anastomoses. Due to the recent reconstruction, access was obtained from the contralateral left CFA, allowing an up-and-over approach that entered the reconstructed right CFA lumen with the direction of flow, avoiding retrograde passage across the fresh anastomoses. The graft appeared widely patent on angiography without kinking or narrowing (Figure 3). To protect the suture lines, advancement was performed using a soft-tipped hydrophilic wire with minimal forward pressure under continuous roadmap guidance, supported by a low-profile angled catheter.

Completion angiogram following open repair of the common femoral artery pseudoaneurysm. The interposed graft is seen as a smooth reconstructed segment with restored inline flow into the profunda femoris and superficial femoral arteries. No residual pseudoaneurysm or contrast extravasation is present.
A combination of hydrophilic guidewires, angled glide catheters, and support catheters were sequentially used to traverse the chronically occluded popliteal artery and tibio-peroneal trunk, requiring subintimal passage in several segments. Iatrogenic dissections created during recanalization were successfully treated with drug-coated balloon angioplasty and selective stenting. Three stents were placed overall: a 7-mm × 150-mm drug-eluting stent in the above-knee popliteal artery for residual dissection and high-grade stenosis; a 6-mm × 60-mm drug-eluting stent extending into the below-knee popliteal artery; and a 10-mm × 88-mm self-expanding stent in the external iliac artery for multifocal stenoses (Figure 4).
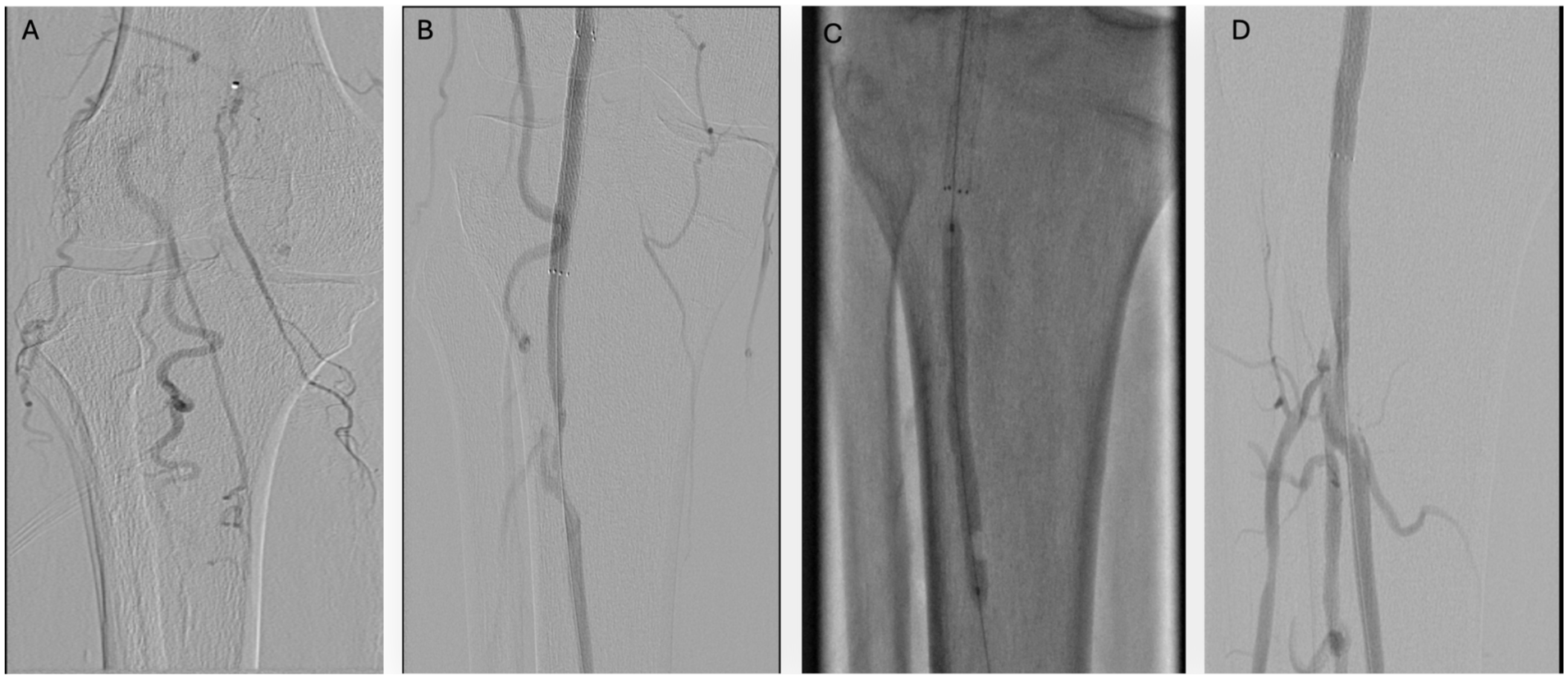
Endovascular revascularization of the chronically occluded tibio peroneal trunk (TPT) and popliteal artery. (A) Pre-intervention angiogram demonstrating chronic occlusion of the TPT with reconstitution of distal branches via collateral flow. (B) Advancement of the guidewire through the occluded TPT and popliteal artery with deployment of a stent across the diseased segment. (C) Drug-coated balloon angioplasty of the stented segment, followed by drug-eluting stent placement. (D) Post-intervention angiogram showing restored inline flow through the TPT and popliteal artery, with improved perfusion of downstream vessels.
Intraoperative cultures from both the ankle and groin confirmed MRSA. A peripherally-inserted central catheter was placed, and the patient was started on a 6-week course of intravenous vancomycin. He was discharged to a short-term rehabilitation facility on hospital day 12.
Follow-up
At the 1-month postoperative visit, his groin and ankle wounds were completely healed. Follow-up at 3 and 6 months demonstrated normal right ankle–brachial indices, a widely patent femoral vein bypass on duplex ultrasound, and patent popliteal and iliac stents on surveillance CTA. Mild dependent edema in the contralateral (harvest) leg improved with ambulation and compression. The patient returned to independent living and resumed normal activities by approximately 2 months postoperatively.
Discussion
Mycotic aneurysms account for < 1% of all arterial aneurysms but are associated with high morbidity and mortality rates if untreated. 1 The most common causative organisms are S. aureus and Salmonella species, although polymicrobial infections can also occur. 1 Typical predisposing factors include endovascular procedures, intravenous drug use, and systemic infections.1,2 Traditional management options include excision with extra-anatomic bypass, but in situ reconstruction with autologous vein grafts has gained favor due to reduced infection risk and improved long-term patency.3–5 Recent literature also highlights the role of adjunctive endovascular techniques in complex cases, particularly in patients with significant comorbidities.5,6
The novelty of this case and several technical considerations merit discussion. This represents an exceptionally uncommon presentation of a mycotic femoral pseudoaneurysm arising from hematogenous spread of septic ankle arthritis. The extensive nature of the aneurysm necessitated separate retroperitoneal and thigh incisions to achieve adequate proximal and distal vascular control before addressing the infected groin. Although the great saphenous vein is frequently used for bypass from the CFA and can reliably tolerate arterial pressure, in this case the contralateral femoral vein was preferred due to its close caliber match to the CFA, thick wall structure, and long-term durability when arterialized in high-flow environments. Prior studies have demonstrated that femoral vein grafts have low rates of aneurysmal degeneration, particularly when placed in infected fields or in large-diameter reconstructions.3,4
The successful endovascular recanalization of a Trans-Atlantic Inter-Society Consensus II (TASC II) class D popliteal trifurcation occlusion is noteworthy. While open surgical bypass is traditionally preferred for such complex lesions, this case highlights that endovascular techniques remain a viable option, particularly in high-risk patients. In this patient, endovascular intervention was chosen over open bypass surgery due to factors including the patient’s advanced age, significant comorbidities, recent groin infection, and complex distal disease. This offered a less invasive, but technically feasible approach while preserving surgical options if later required, minimizing wound complications, and supporting faster recovery in a functional but frail patient who required a stay in the intensive care unit for hemodynamic and respiratory support after the index femoral reconstruction.
Although prosthetic stents are generally avoided in actively infected fields, the endovascular intervention in this case occurred remotely from the contaminated groin and only after wide debridement, open drainage, negative pressure therapy, and clinical stabilization. Since the interventions occurred outside the infected zone and only after substantial infection control, the risk of prosthetic stent contamination was minimized. Furthermore, the patient completed a 6-week course of intravenous anti-MRSA therapy, consistent with the Infectious Diseases Society of America (IDSA) recommendations for MRSA bacteremia. 7
Most importantly, this case underscores the critical role of a multidisciplinary team approach in managing complex vascular infections.6,8,9 Coordinated efforts among vascular surgery, orthopedic surgery, and infectious disease specialists were instrumental in achieving a favorable outcome for this high-risk patient.
Conclusion
This case demonstrates that mycotic CFA pseudoaneurysms, even when complicated by bacteremia and severe distal occlusive disease, can be managed safely with an individualized, staged strategy. Autologous in situ reconstruction provided durable proximal repair, while delayed endovascular intervention restored distal perfusion without jeopardizing the new graft. Coordinated decision-making across specialties allowed for controlled infection management, protection of fresh anastomoses, and effective limb salvage. This experience underscores the value of tailoring operative timing and technique to each patient’s physiology, anatomy, and infectious burden.
Footnotes
Acknowledgements
We would like to thank Dr Rachana Borkar, Chief Resident, Department of Radiology, Yale New Haven Health—Bridgeport Hospital, Bridgeport, Connecticut, for her invaluable contributions to this report. Her dedication and expertise with reviewing imaging was instrumental in bringing this work to fruition.
Ethical Considerations
ethical approval was not required for this case report
Consent for Publication
Patient consented to publication of this report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.