
Abstract
Purpose:
The standard technique for iliac branch device (IBD) deployment involves bilateral femoral access and crossover wire, which may be challenging after previous endovascular aortic repair (EVAR). We present a technique for IBD deployment following EVAR using single femoral access and kissing-balloon angioplasty.
Technique:
An 83-year-old male patient with previous infrarenal bifurcated EVAR presented at 6-year follow-up with left common iliac dilatation and distal loss of seal, leading to type Ib endoleak and aortic aneurysm sac expansion of 13 mm (aortic diameter: 70 mm). A secondary intervention with an IBD was decided. Under general anesthesia, percutaneous left common femoral artery access was achieved. An IBD was successfully advanced and deployed above the left iliac bifurcation. A steerable sheath facilitated access to the hypogastric artery, allowing catheterization, delivery, and deployment of the bridging stent. Using this single access, simultaneous kissing-balloon angioplasty of the main IBD and branch ensured adequate expansion. Completion angiography confirmed patency without endoleak. The access site was secured using a closure device. The postoperative course was uneventful, and the pre-discharge computed tomography angiography confirmed proper device placement without endoleak.
Conclusion:
Single-access IBD deployment using a steerable sheath is feasible after EVAR and may reduce access-related complications.
Clinical Impact
Access site complications affect up to 10% of patients undergoing endovascular procedures and may be even more frequent in patients requiring large-bore sheaths. Single-access iliac branched device placement with a steerable sheath for branch catheterization and bridging stent advancement and deployment reduces the potential risk associated with secondary access site complications, without compromising the final result. With this technique, the performance of kissing balloon to assure adequate expansion of bilateral components is achievable.
Keywords
Introduction
Secondary interventions after endovascular aortic repair (EVAR) are more frequent than those following open abdominal aortic aneurysm (AAA) surgery. 1 A contributing factor to this higher reintervention rate is the failure of distal sealing, often due to enlargement of the common iliac artery (CIA), short landing zones of less than 20 mm, or marked tortuosity, which can lead to loss of distal iliac seal, also known as endoleak type Ib.2,3 Current international guidelines support the use of iliac branched devices (IBDs) to preserve antegrade blood flow to the hypogastric artery (HA), minimizing the risk of buttock claudication, erectile dysfunction, and pelvic and spinal cord ischemia while providing an effective aneurysm exclusion and long-term patency rates above 90%.4,5
The standard implantation technique for IBD typically involves bilateral femoral access and the establishment of a through-and-through wire for crossover access to the HA. For secondary IBD implantation crossover HA access therefore becomes more challenging due to a more acute angle of the aortic bifurcation, requiring either upper extremity access (UEA), with its inherent stroke risk or the up-and-over technique, with a risk of distal migration of the previously placed endograft.6,7
Single-side access for IBD placement may be useful to reduce the number of access sites so to reduce complications, namely when a contralateral access is not available due to occlusive disease, or when there is a scarred groin where percutaneous techniques may pose difficulties, or when brachial access is not desirable. 8 Single-access techniques for IBD placement have been reported previously but not including a technique to perform a kissing-balloon maneuver after bridging covered stent implantation in order to simultaneously expand the iliac bifurcation to create sufficient diameter for both the IBD main body and the IBD-branch.9,10 In bilateral IBD implantation techniques, this step is usually performed using contralateral and ipsilateral access for each of the semi-compliant balloons used.
This technical note describes the technique of using a single femoral access to deploy and successfully complete an IBD placement after a prior EVAR, performing simultaneous angioplasty of the iliac components in a kissing-balloon technique.
Technique
An 83-year-old male with previous aorto-bi-iliac infrarenal EVAR for asymptomatic AAA presented at 6-year follow-up with an aortic aneurysm sac expansion of 13 mm (maximum diameter of the aortic aneurysm 70 mm) due to a type Ib endoleak after concomitant aneurysmal dilatation of the left CIA (25 mm) and loss of the left distal sealing (Figure 1). Due to lack of appropriate distal sealing within the CIA, a distal extension using an IBD was planned to achieve distal sealing and preserve antegrade flow into the left HA. In order to reduce the risk of migration of the previously-implanted bifurcated device during the standard through-and-through wire technique, a single access using a steerable sheath for HA catheterization and bridging stent delivery was decided.
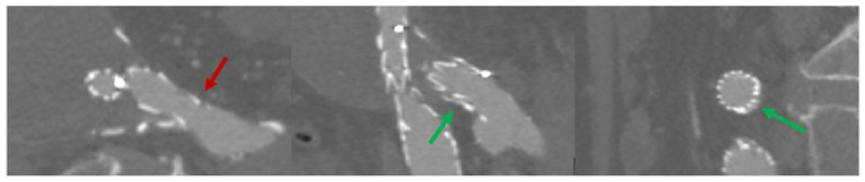
Multiplanar reconstruction of pre-operative computed tomography, demonstrating the type Ib endoleak. Red arrow: common iliac artery dilation with lack of appropriate sealing; Green arrows: lack of graft apposition to the wall of the common iliac artery and endoleak.
Ultrasound-guided puncture of the left common femoral artery was performed using the Preclose technique (Prostar XL, Abbott Vascular Inc, Santa Clara, California). An extra-stiff double-curved Lunderquist wire (Cook Medical, Bjæverskov, Denmark) was positioned in the proximal thoracic aorta, and after initial angiography for HA visualization, a 12-45-41 Zenith Branch Endovascular Graft (ZBIS, Cook Medical, Bjæverskov, Denmark) was advanced. The device was fully deployed, and the preloaded wire and catheter were discarded (Figure 2A).
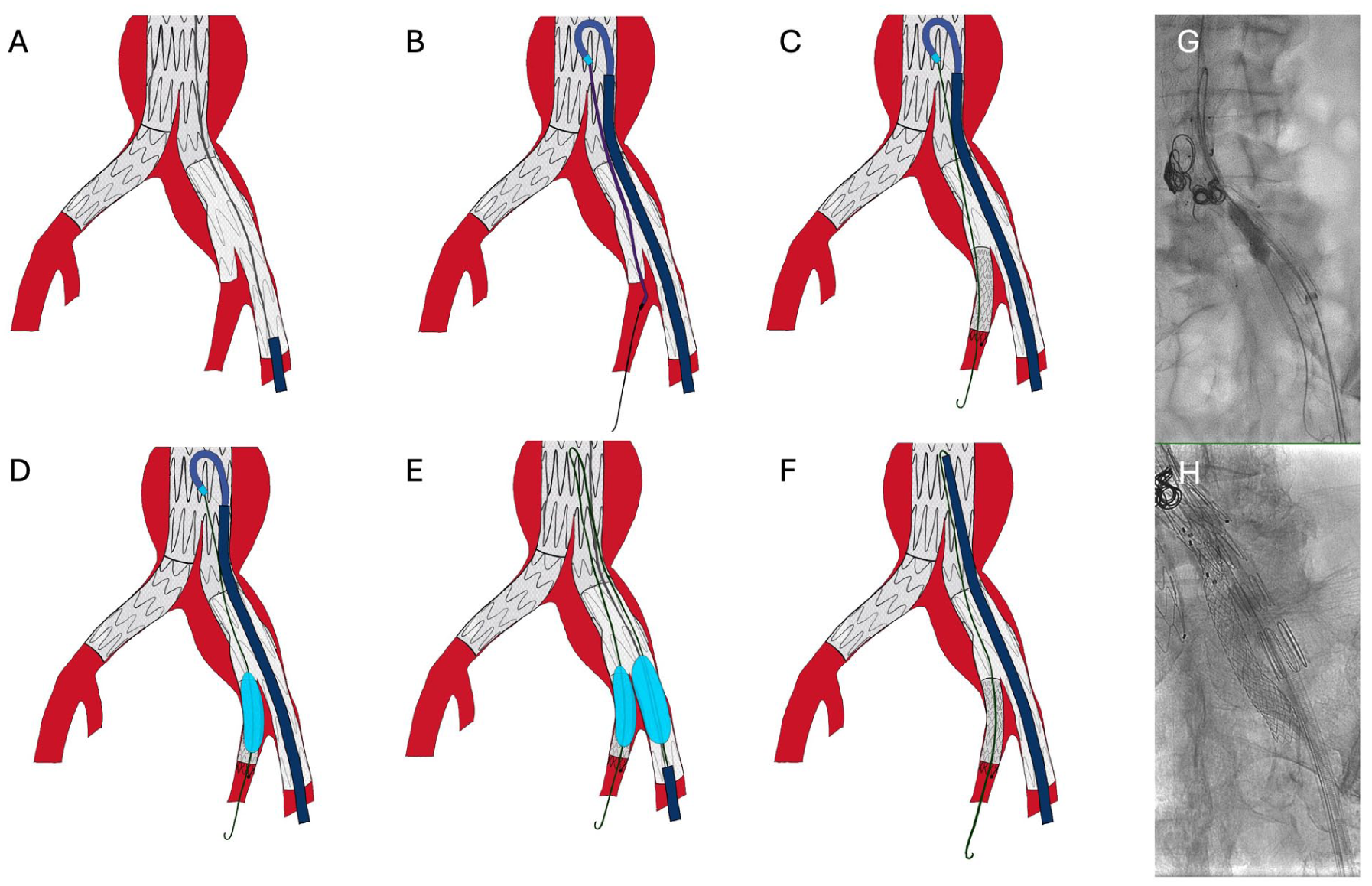
(A) IBD deployment under stiff wire (Lunderquist), without through-and-through wire. (B) A 14F sheath is advanced, and a supported steerable sheath and catheter allow hypogastric artery access. (C) After exchange for a stiffer wire (Rosen), internal iliac artery stent is deployed. (D) A balloon is left inflated, and the steerable sheath is withdrawn and the 14F sheath is retracted, maintaining the loop. (E) Using buddywire technique, a second balloon is inflated in the external component of the IBD, thus performing kissing balloon. (F) Advancement of the 14F sheath up to the level of the loop to allow withdrawal of the internal balloon catheter without loss of hypogastric artery access. (G and H) Intraoperative view of the applied technique.
Subsequently, the access was downsized and a 30 cm 14F CheckFlo sheath (Cook Medical, Bjæverskov, Denmark) was placed in the infrarenal aorta. A 55 cm 10F Fustar steerable sheath (Lifetech Scientific Inc, Shenzhen, China) was modified as previously described by puncturing the valve and inserting a 0.014-in. wire to obtain a through-and-through wire to stabilize the sheath’s curve. 11 This system was introduced in the 14F sheath and positioned proximal to the previous EVAR main body bifurcation, where it was adequately steered and stabilized (Figure 2B and C). Through this antegrade access, the IBD branch and the left HA were catheterized, and a Rosen wire (Cook Medical, Bjæverskov, Denmark) was positioned. An 8×59 mm VBX stent graft (Gore Medical, Flagstaff, Arizona) was deployed to bridge the HA (Figure 2C). The control angiography showed adequate sealing.
Subsequently, a 10×40 mm Armada semi-compliant balloon (Abbott Vascular, Redwood City) was advanced inside the bridging covered stent and inflated, while the steerable and the CheckFlo sheaths were retracted into the external iliac artery (Figure 2D). Additional access was obtained by puncturing the 14F sheath valve, and a 12×40 mm Armada semi-compliant balloon (Abbott Vascular) was advanced over a standard wire and inflated in the main IBD, thus, performing a kissing-balloon maneuver (Figure 2E). The 14F sheath was advanced over the deflating 12 mm balloon into the common iliac segment to safely remove the balloon of the HA without tearing the fabric at the IBD bifurcation (Figure 2).
Finally, a 10×38 mm Advanta V12 covered stent (Getinge/Atrium Medical Corporation, Merrimack, New Hampshire) was deployed and post-dilated to 12 mm to bridge the IBD with the previous EVAR iliac extension and a 14 × 60 mm Protegé stent (Medtronic, Minneapolis, Minnesota) was placed to smoothen the transition between the IBD and the external iliac artery. The completion angiography demonstrated adequate position and patency of the IBD with endoleak type Ib resolution. The catheters and sheaths were retrieved, and the left common femoral access was successfully closed. Total radiation of the procedure was 17.5 Gycm3.
The postoperative course was uneventful, and the patient was discharged 4 days later under chronic apixaban 2.5 mg 2id for atrial fibrillation and adjusted to glomerular filtration rate plus clopidogrel 75 mg id for 6 months. The pre-discharge computed tomography angiography showed exclusion of the aorto-iliac aneurysm, with a patent IBD and HA (Figure 3). At 6 months follow-up, the aneurysm sac dimension was 63 mm with no evidence of endoleak, with fully patent endografts.
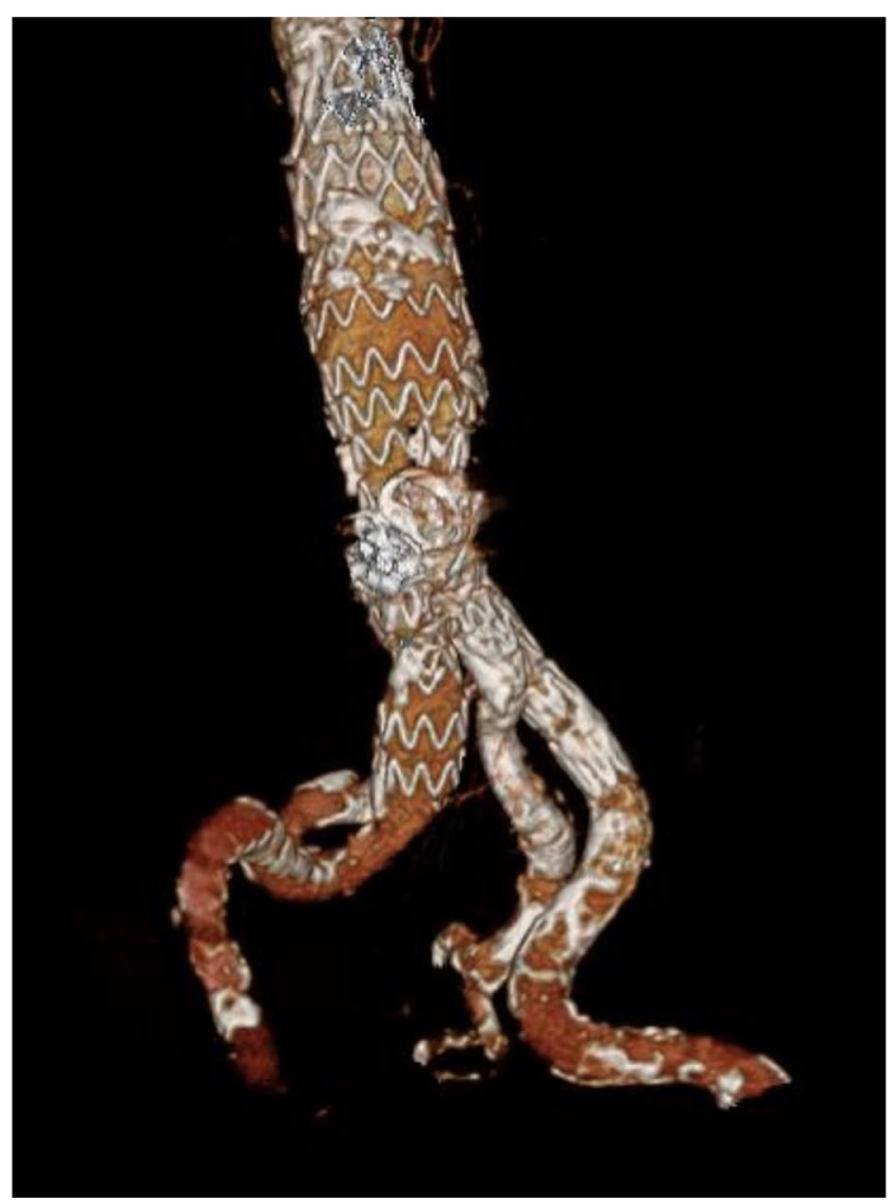
Post-operative CTA with adequate deployment of the IBD without endoleak.
Discussion
A case of successful single-access complete IBD implantation for type Ib endoleak after previous infrarenal EVAR using a steerable sheath technique is presented. This strategy allowed not only to avoid an additional contralateral femoral access but also to maintain adequate support for device advancement and accurate deployment during the procedure. The ability to perform the kissing-balloon maneuver despite the single access is important for full expansion of all components. Minimizing the number of access sites during endovascular procedures may be beneficial in terms of complications’ reduction, as access-related adverse events seem to occur in 5% to 10% of patients undergoing endovascular procedures, while they are even more frequent in patients requiring large-bore access. 8
Iliac sealing loss and type Ib endoleak after EVAR have been recorded in up to 8% of cases. 3 Treatment strategies focus on the extension of the repair into more distal iliac segments and include several alternative approaches to IBD, such as embolization of the HA and distal extension to the external iliac artery, or techniques with preservation of antegrade flow to the HA such as parallel grafts, with the drawback of gutter endoleak and possible worse long-term outcomes. 12 By contrast, IBD enables preservation of antegrade hypogastric flow while mitigating the complications inherent to parallel configurations. 12
Reinterventions with IBD implantation in patients who have undergone previous EVAR have been reported, with studies presenting various access approaches, such as concomitant UEA and bilateral femoral access for catheterizing and bridging the HA.13-15 Limited data comparing UEA and the up-and-over technique in patients with type Ib endoleak after previous EVAR showed similar success rates but with upper access being related to higher stroke rates and longer operative times. 15 The up-and-over technique seems to provide a valuable alternative in cases of previous failed EVAR, as it has been related to high technical success and low complication rates. 13
Techniques for single transfemoral access IBD placement have previously been reported.9,10 However, these techniques did not include a kissing-balloon maneuver as we describe. We believe the described technique can be beneficial in patients with reasons to avoid contralateral femoral access as in patients with distal bypasses, with groin scar tissue from previous surgeries or in those with diseased iliac arteries. The use of the stabilized steerable sheath seems to be crucial in single-access IBD implantation. According to the previously published experience of steerable sheaths for antegrade branch catheterization and bridging stent deployment in complex aortic repairs, it provides an effective platform, further reducing the need for UEA.
There are several important technical considerations regarding single-access IBD cases. Single access should be avoided in cases where the contralateral side also requires intervention or when significant iliac tortuosity is present. A steerable sheath with robust support is generally preferred to facilitate accurate stent delivery. If additional stability is needed, a 0.014-inch through-and-through wire exiting through an outer sheath can be employed. Ideally, the bridging covered stent intended for HA should have a 7Fr or smaller profile, allowing continued use of the 0.014-inch wire within a 10F Fustar sheath. This configuration also accommodates the introduction of an additional 7Fr sheath and minimizes friction along the sharp curvature of the steerable sheath. Stable access to the HA can be maintained until it is no longer required. If repeated antegrade access to the HA is required after sheath withdrawal while maintaining wire position within the HA, the sheath can be positioned up to the point where the wire curves back toward the HA, thus preserving a pulley-shaped configuration of the HA wire (Figure 2F).
Conclusion
The IBDs can be deployed after previous EVAR using a single access and including a kissing-balloon maneuver, avoiding the potential complications derived from a second access site. This approach may be considered on an individual patient basis and be specifically of value in cases with compromised contralateral access.
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
According to the local ethics committee, ethical approval is not required for this manuscript.
Consent for Publication
Consent was taken from the patient for publication of this technical note and the accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.K. receives consulting, proctoring, and intellectual property fees, royalties, and research and travel grants from Cook Medical Inc.
Data Availability Statement
The data sets used during the current study are available from the corresponding author on reasonable request.