
Abstract
Background:
Patients with lower extremity arterial disease (LEAD) frequently require revascularization procedures. Currently used diagnostic methods are insufficient in predicting successful outcomes and focus on macrovascular rather than microvascular state. Several promising modalities to increase diagnostic accuracy are emerging, including maximal systolic acceleration (ACCmax), measured by duplex ultrasound (DUS). For the assessment of tissue perfusion, near-infrared fluorescence (NIR) imaging using indocyanine green (ICG) demonstrates promising results. This study aims to identify the usefulness of combining these two methods for macrovascular and microvascular perfusion assessment to predict successful clinical outcomes.
Methods:
A retrospective study was performed collecting preinterventional and postinterventional DUS and ICG NIR fluorescence imaging measurements from LEAD patients undergoing revascularization. The correlation between the preinterventional and postinterventional perfusion parameters, described as the delta (Δ) ACCmax and ΔICG NIR fluorescence parameters, were analyzed. Improvements in perfusion parameters were compared to clinical outcomes, defined as improvement in pain-free walking distance, freedom from rest pain, or tendency toward wound and ulcer healing.
Results:
A total of 38 patients (42 limbs) were included. ACCmax and ICG NIR fluorescence perfusion parameters improved significantly after revascularization (p<0.001). Patients with a poor clinical outcome had a significantly lower improvement of both parameters after revascularization (p<0.001–0.016). Lack of correlation was found between the delta of ACCmax and ICG NIR fluorescence imaging. Multiple non-congruent improvements of macrovascular parameters (ACCmax) and perfusion (ICG NIR fluorescence) were seen within patients. However, for all patients with a successful clinical outcome, at least one parameter improved.
Conclusion:
Combining ACCmax and ICG NIR fluorescence imaging revealed improvement in at least one parameter within all patients with a successful clinical outcome. This study highlights the potential of assessing both the macrovascular state and tissue perfusion following lower extremity revascularization, as both appear to reflect different aspects of vascularization.
Clinical Impact
Numerous techniques have been developed to assess tissue perfusion to predict clinical outcomes following revascularization in patients with peripheral artery disease. However, none are widely implemented in clinical practice. This study emphasized the importance of employing multiple modalities from different perspectives for more accurate prediction. By focusing on both the macrovascular state and tissue perfusion, clinicians can better guide themselves in their treatment strategies.
Keywords
Introduction
Lower extremity arterial disease (LEAD) is characterized by decreased perfusion, mostly due to atherosclerotic plaques. It is estimated that over 230 million people worldwide are affected by LEAD and this number is expected to increase.1,2 The most severe form, known as chronic limb-threatening ischemia (CLTI), carries a 5-year mortality risk of 60%. 3 These patients typically require revascularization procedures to preserve limb function. Despite successful revascularization, high reintervention rates persist due to post-operative occlusions and the multilevel disease patterns of CLTI patients.3,4 Currently, the prediction of clinical outcome following revascularization remains inadequate using existing modalities and mainly focuses on assessment of the macrovasculature instead of perfusion 5 Combining assessment of the macrovascular state with perfusion after revascularization could be a promising method to better guide physicians in their treatment decisions by initiating or preventing reinterventions and amputations more promptly. 6
The maximal systolic acceleration (ACCmax) is a new emerging bedside test that corresponds to macrovascular flow proximal to the measurement point.7–9 ACCmax is measured through duplex ultrasonography (DUS) and has shown excellent diagnostic accuracy to detect and rule out LEAD, independent of patients prone to medial arterial calcification 8 ACCmax seems to be a reliable diagnostic modality and can provide insights into the severity of a stenosis, yet only depicts macrovascular state.10,11 Especially in LEAD patients with impaired wound healing or diabetes mellitus, a combined assessment of the microvascular status could be very helpful for physicians. 12
To assess tissue perfusion, near-infrared (NIR) fluorescence imaging with indocyanine green (ICG) can be used. ICG is a fluorescent dye that binds to plasma protein albumin after intravenous injection and provides visualization and quantification of perfusion when recorded with a specialized NIR camera. 13 Studies have shown that NIR fluorescence imaging has the potential to predict clinical outcomes after revascularization procedures using the extracted inflow and outflow perfusion parameters.14,15
This study aims to identify the usefulness of combining two emerging methods for macrovascular and microvascular assessment to predict successful outcomes after revascularization. Therefore, the primary objective of this study is to investigate whether there is a correlation between ACCmax and ICG NIR fluorescence or if they independently assess different aspects of vascularization. It is hypothesized that ACCmax corresponds with macrovascular flow and that ICG NIR fluorescence imaging assesses perfusion. A secondary objective is to analyze how combining the two modalities, ultimately leads to an improved prediction of clinical outcome after revascularization.
Materials and Methods
This retrospective cohort study was performed between February 2019 and December 2023 in a single academic hospital. Patients were included if they underwent a technically successful revascularization procedure and had complementary preinterventional and postinterventional DUS and ICG NIR fluorescence imaging measurements. Successful clinical outcome was defined, as in a previous study, depending on Fontaine's classification of the limb, by either improvement of pain-free walking, reduction of rest pain, or tendency toward wound and ulcer healing assessed by the treating physician. 15 Follow-up was performed according to the revascularization protocol in the outpatient clinic within 6 weeks measurement. Patients included before implementation of ICG NIR fluorescence as the standard of care gave written informed consent. All patients provided permission for data usage.
ICG NIR Fluorescence Measurement
Indocyanine green NIR fluorescence measurements were performed before the revascularization and within 5 days after the intervention, according to previously described methods. 15 During ICG NIR fluorescence imaging, patients were taken into a room that could be cleared of ambient light, where a bolus of ICG (Verdye) 0.1 mg/kg was administered intravenously in the cubital vein. Subsequently, the NIR fluorescence intensity change over time was recorded for 5 min by the Quest Spectrum 2.0 (Quest Medical Imaging, Middenmeer, the Netherlands), which was aimed perpendicular to the dorsum of the feet at a distance of 50 cm. This system uses a visible light engine and an NIR light source (700–820 nm). All videos were recorded using fixed camera settings.
DUS Measurement
ACCmax values were measured by DUS and calculated at the maximal slope of the upstroke (expressed in m/s 2 ). A detailed description can be found in previous literature. 8 Patients with preinterventional and postinterventional measurements of the arteria tibialis posterior (ATP), arteria tibialis anterior (ATA), or arteria dorsalis pedis (ADP) were included. When measurements in multiple arteries were available, the artery demonstrating the greatest improvement was selected. Patients with a preinterventional ACCmax longer than 6 months prior to the revascularization or post-interventional ACCmax longer than 3 months after the revascularization were excluded. Patients who displayed a newly formed stenosis on the post-interventional duplex were excluded as well. The DUS measurements were performed by the same sonographer, using the Siemens Acuson Sequoia Ultrasound System. Figure 1 gives a schematic overview of both techniques and their corresponding location of measurement.
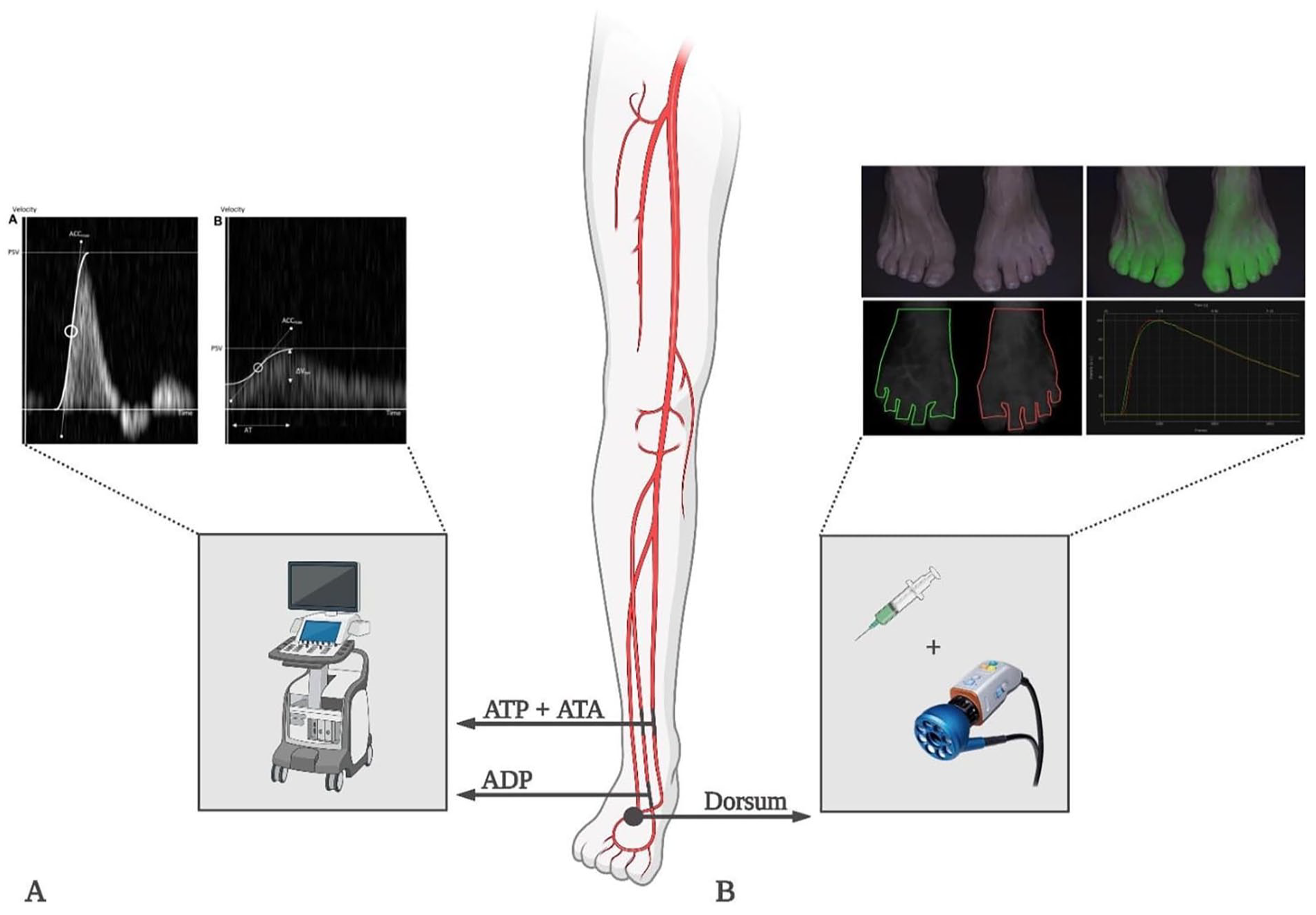
Schematic overview of the two techniques and their corresponding location of measurement. (A) Duplex ultrasound with maximal systolic acceleration was visually measured and calculated as the maximal slope of the upstroke of a Doppler wave. [10] (B) Near-infrared fluorescence with indocyanine green measurement of two feet, including two drawn regions of interest and corresponding time-intensity curves. Abbreviations: ATA, arteria tibialis anterior; ATP, arteria tibialis posterior; ADP, arteria dorsalis pedis.
Data Analysis
Quantification of ICG NIR fluorescence data was performed using Quest Research Framework (Quest Medical Imaging, Middenmeer, the Netherlands). The entire dorsum of the foot was selected as a region of interest, from which time-intensity curves were extracted. The parameters normalized max ingress slope (Normalized slope in %/s) and time to maximum intensity (Tmax in s) were extracted from these curves for further analysis, as these inflow parameters are most reliable in clinical settings.16,17 Statistical analyses were conducted using IBM SPSS Statistics 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Versions 25.0 Armonk, NY, USA; IBM Corp.). Preinterventional and postinterventional parameters were compared using the Wilcoxon signed-rank test. Delta (Δ) ACCmax, ΔNormalized slope, and ΔTmax were correlated using the Spearman’s rank correlation coefficient (Spearman’s ρ). Subgroup differences were analyzed using the Mann–Whitney U test and the Kruskall–Wallis test. p-Values <0.05 were considered statistically significant. Based on clinical outcome, 2 × 2 tables were generated, aligning improvement or no improvement of ACCmax and ICG NIR fluorescence parameters to each other. Improvement was defined by an increase of >1.5 m/s 2 of ACCmax, >2 s of Tmax, and >0.2%/s of Normalized slope by consensus of the authors.
Results
Patient Characteristics
Thirty-eight patients were included with a mean age of 68.5 (±8.2) years, and 58% (n=22) were male (Table 1). Reported comorbidities include hypertension (60%), diabetes (33%), and kidney failure (12%). Of all patients, 88% had a history of smoking, of which 29% were active smokers. A successful clinical outcome was seen in 37 limbs (88%). Most limbs (n=21) were classified as Fontaine stage 2B, corresponding to Rutherford (RF) stage 3. One limb was stage 2A (RF 2), 11 limbs were Fontaine stage 3 (RF4), and 9 limbs were classified as Fontaine stage 4 (RF 5/6). Endovascular revascularization was performed in 23 limbs (55%), whereas surgical treatment (bypass or thrombendarteriectomy of the common femoral artery or infrarenal aorta) was conducted in 9 (21%) and 10 (24%) patients, respectively. Sixteen limbs (38%) were revascularized at the aortoiliac level, 22 (52%) limbs were treated at a femoral-popliteal level, and four limbs (10%) were treated at a crural level. The ATA was assessed by ACCmax in 14 (33%) instances; subsequently, the ATP and ADP were assessed in 25 (60%) and 3 (7%) instances, respectively.
Patient and Revascularization Characteristics.
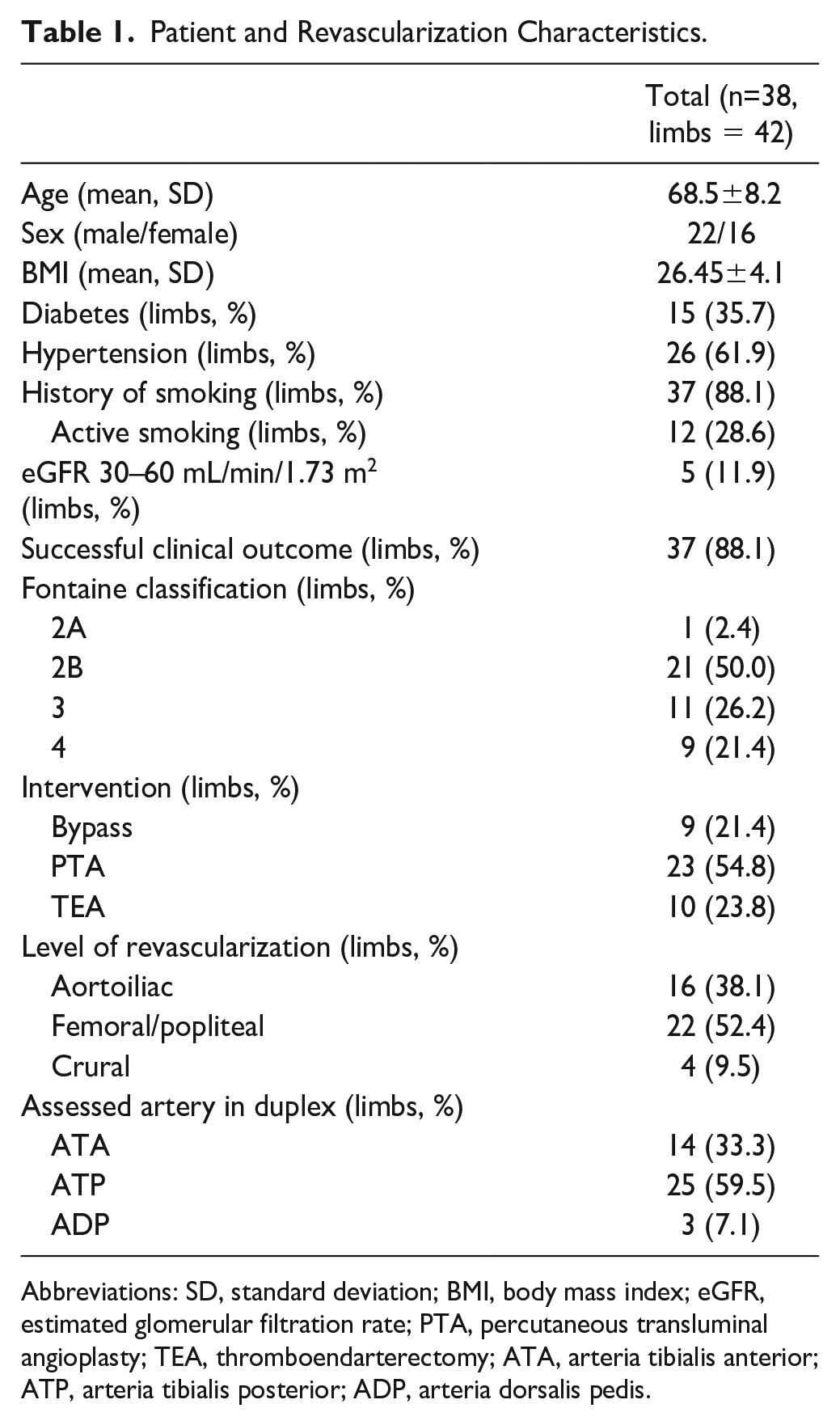
Abbreviations: SD, standard deviation; BMI, body mass index; eGFR, estimated glomerular filtration rate; PTA, percutaneous transluminal angioplasty; TEA, thromboendarterectomy; ATA, arteria tibialis anterior; ATP, arteria tibialis posterior; ADP, arteria dorsalis pedis.
Intervention
Preinterventional and postinterventional delta’s of ACCmax and ICG NIR fluorescence imaging are displayed in Table 2. Normalized slope increased from a median of 2.7 %/s (1.8–4.2) to 5.8 %/s (3.8–7.8). Time to maximum intensity (Tmax) increased from a median of 102.2 s (60.2–151.9) to 38.8 s (20.3–66.0). Median ACCmax improved from 1.6 m/s² (0.6–3.2) to 9.3 m/s² (4.1–10.8).
Preinterventional and Postinterventional ICG NIR Fluorescence Parameters and ACCmax With Absolute Improvement.
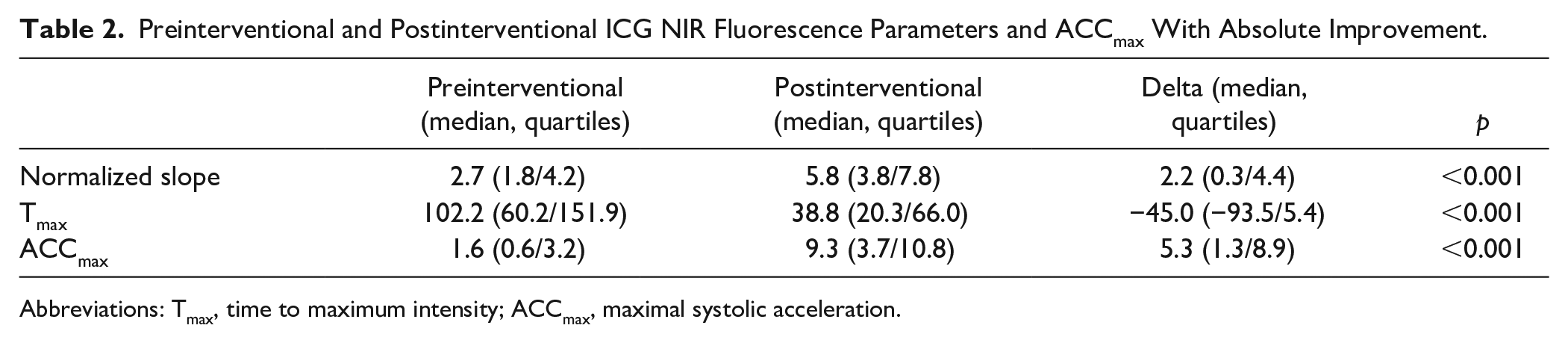
Abbreviations: Tmax, time to maximum intensity; ACCmax, maximal systolic acceleration.
Correlation
Scatterplots of absolute ΔACCmax, ΔNormalized slope, and ΔTmax were generated. ACCmax and ICG NIR fluorescence parameters did not exhibit equivalent improvement as no significant correlations between change in macrovascular ACCmax and microvascular ICG NIR fluorescence parameters were observed (Figure 2).
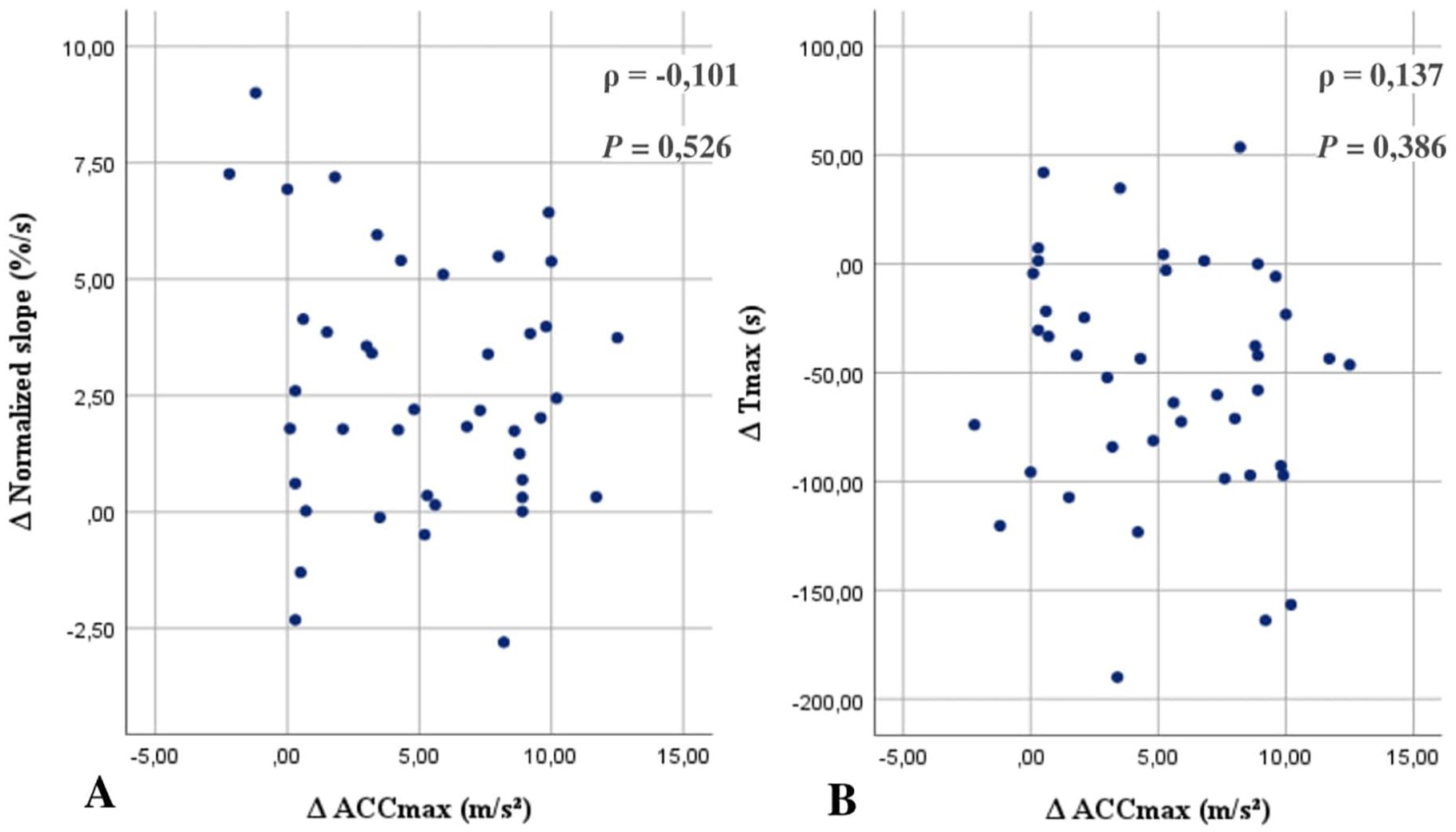
Scatterplot of change in normalized slope against change in ACCmax with associated correlation coefficient (A), scatterplot Of change in Tmax against change in ACCmax with associated correlation coefficient (B). Abbreviations: ACCmax, maximal systolic acceleration Spearman’s correlation coefficient. Tmax, time to maximum intensity; A, deltas; ρ, Spearman’s correlation coefficient.
Clinical Outcomes
Table 3. presents the median delta’s of ACCmax and ICG NIR fluorescence parameters within specific subgroups. In patients with an unsuccessful clinical outcome, all three parameters exhibited a significantly lower delta after revascularization. Based on Fontaine classification, ΔTmax significantly differed, indicating that CTLI patients classified as Fontaine 4 experienced less improvement of perfusion after revascularization. No significant differences between diabetics and non-diabetics were observed.
Delta’s of ICG NIR Fluorescence Imaging and ACCmax in Patients Based on Clinical Outcome, Fontaine Classification and Presence of Diabetes.
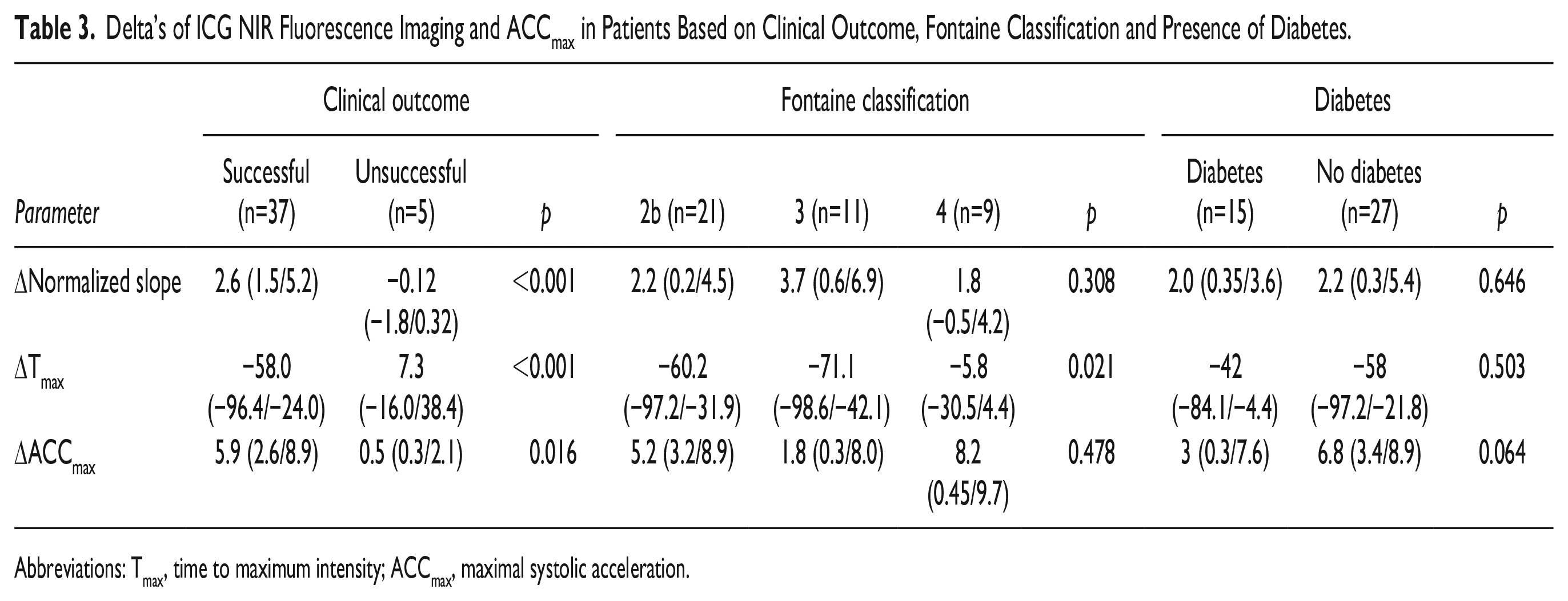
Abbreviations: Tmax, time to maximum intensity; ACCmax, maximal systolic acceleration.
Figure 3 shows improvement or no improvement of ACCmax against either Normalized slope or Tmax. Among patients with an increase in both ACCmax and normalized slope (n=27), all eventually experienced a successful clinical outcome. Within this group, zero patients showed no improvement in both parameters, whereas ten patients showed improvement in only one parameter. Similar results were observed when examining the parameter Tmax. Among patients with a poor clinical outcome, three cases exhibited no improvement in both ACCmax and Normalized slope, while two patients exhibited improvement in one parameter.
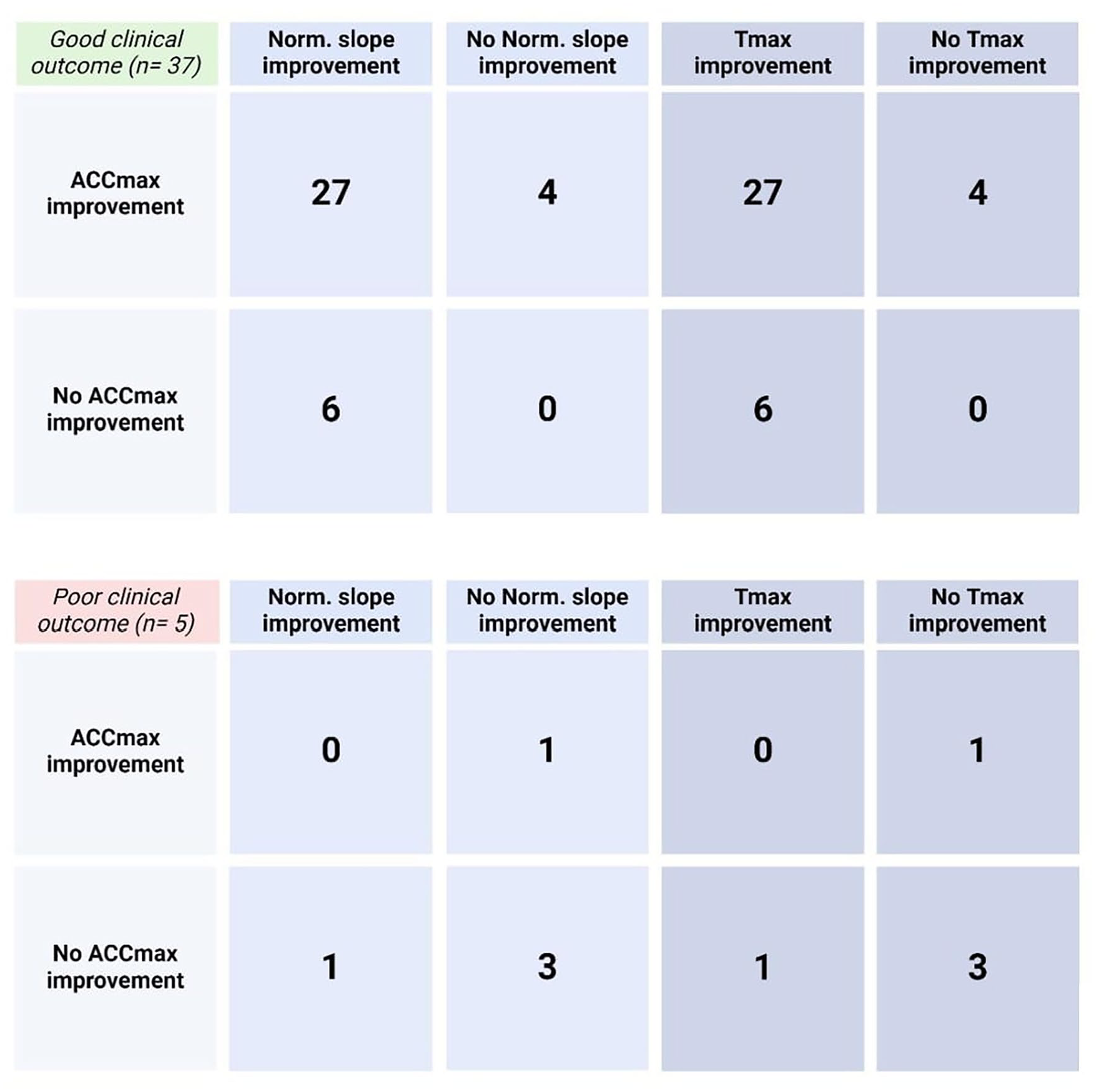
2 × 2 tables of improvement of ACCmax and ICG NIRF parameters (Normalized slope and Tmax) in patients with a good or bad clinical outcome. Abbreviations: ACCmax, maximal systolic acceleration; Norm. slope, Normalized slope; Tmax, time to maximum intensity.
Discussion
This study was designed to identify the usefulness of combining ACCmax and ICG NIR fluorescence imaging to predict successful outcome after revascularization of the lower extremity. For all patients with a successful clinical outcome at least one parameter improved. Complementary use of these two modalities can give optimal information to predict clinical outcomes after revascularization.
ICG NIR fluorescence has been used extensively for various indications, including perfusion assessment in oncologic, reconstructive, and vascular surgery. 13 ICG has long been recognized for its ability to bind to plasma proteins following intravenous administration, making it feasible for perfusion assessment.18–20 Recently, the focus has shifted to quantification of this fluorescence signal, which results in an objective and reproducible evaluation of tissue perfusion. 19
This is the first study to describe the relationship between quantified ICG NIR fluorescence and ACCmax measured with DUS in patients with LEAD and linking this to clinical outcomes. Previously, poor correlation has been observed between the microvascular oxygenation parameter StO2 and the macrovascular ankle-brachial index.21–23 Geskin et al. 24 compared acceleration time, measured by DUS, of the medial and lateral tarsal artery to near-infrared spectroscopy. Similar to our findings, no significant correlations were observed between differences of microvascular and macrovascular assessment following revascularization. The efficacy of ICG NIR fluorescence as a quality control measure post-revascularization and as a predictive value on clinical outcome has already been demonstrated in previous studies.14,15,25–28 DUS is already recommended by current guidelines as standard surveillance after endovascular interventions for detection of newly formed in-stent stenoses. 29 As these guidelines on follow-up after surgical or endovascular revascularizations do not include ICG NIR fluorescence or any type of (microvascular) perfusion assessment, considerable prognostic advantages can be obtained in the future. 30
Non-congruent improvements in ACCmax and ICG NIR fluorescence, seen in multiple patients, show that an enhanced macrovascular state following revascularization does not necessarily result in improved tissue perfusion and vice versa (Figure 3). However, in the clinical improvement group, all patients showed improvement of at least one parameter. This suggests that observing lack of improvement of both ACCmax and ICG NIR fluorescence, a more rapid evaluation of the patient might be necessary. Adding ICG NIR fluorescence imaging to standard monitoring after revascularization enables more accurate identification of patients without improved perfusion. This is particularly crucial in patients with CLTI, as early identification of those with unimproved perfusion can significantly aid in preventing reinterventions or amputations. ICG NIR fluorescence imaging appears to more directly reflect the endpoint in CLTI patients, which in this case is actual wound perfusion. Patients with a poor clinical outcomes showed significantly less improvement in both ACCmax and ICG NIR fluorescence parameters (Table 3). However, more interestingly, Fontaine stage 4 patients in this cohort demonstrated less improvement of the Tmax compared to Fontaine stage 2b and 3, which is consistent with findings from a previous study. 31
The poor correlation between the delta of ACCmax and ICG NIR fluorescence imaging suggests that both modalities evaluate different aspects of vascularization. However, this lack of correlation could be attributed to several other factors. It is important to note that significant changes in perfusion may take several weeks to become noticeable.32,33 Current study design involves conducting a second NIR fluorescence imaging measurement shortly after the intervention, which may not allow enough time for changes in perfusion to manifest. Additionally, diabetes mellitus could potentially lead to disparities in microvascular and macrovascular statuses. However, it does not appear to be the primary factor behind the poor correlation observed in this cohort, as no significant differences in improvement are seen between diabetic and non-diabetic individuals (Table 3). The absence of significant differences among these individuals may be attributed to the small sample size. Considering that diabetes mellitus is a known contributor to microvascular disease, different changes in perfusion patterns after revascularization are expected. Improved tissue perfusion measured by ICG NIR fluorescence imaging without enhancement of macrovascular flow, as depicted by ACCmax is not in line with expectations. This discrepancy can be most logically explained by the likelihood that inline flow was not attained through the analyzed artery. As improvement in foot perfusion might have taken place through an alternative pathway, such as collateral vessels or through another crural vessel.
It appears that ACCmax and ICG NIR fluorescence both reflect different aspects of vascularization and combining both modalities could provide more prognostic insight into macrovascular and microvascular pathology. However, these findings should be interpreted with caution, due to the retrospective nature of the study, patient heterogeneity, and variations in the timing of ACCmax measurements. Nevertheless, the heterogeneous presentation observed is typical for PAD patients, and the underlying pathophysiology is consistent across all patients. Furthermore, although various revascularization techniques were employed, they all share the common objective of augmenting blood flow to the lower extremities.
Future studies should focus on simultaneous ACCmax and ICG NIR fluorescence imaging measurements in CLTI patients, as this group stands to benefit most from such combined assessment. This exploratory study is an important first step toward more comprehensive research into predicting successful revascularization by employing multiple modalities from a different perspective. Prospective studies are necessary to establish the utility of combining these two promising modalities and translate these findings into clinical care. Ultimately, this could result in intra-operative assessments involving both preinterventional and postinterventional measurements of the macrovascular state and actual tissue perfusion to evaluate the effectiveness of treatment. If necessary, immediate adjustments could be facilitated to deviate from a “wait-and-see” approach by revascularizing more extensively or deciding to amputate more promptly.
Conclusion
Combining ACCmax and ICG NIR fluorescence imaging revealed improvement in at least one parameter within all patients with a successful clinical outcome. This study highlights the potential of assessing both the macrovascular state and tissue perfusion following lower extremity revascularization, as both appear to reflect different aspects of vascularization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is co-funded by the PPP Allowance made available by Health∼ Holland regarding the RULER and IMPULSE-project. Top Sector Life Sciences & Health, to stimulate public-private partnerships.