
Abstract
Background:
Carotid artery stenting (CAS) in the treatment of significant stenosis is a cause of stroke due to both plaque prolapse and cerebral embolization. New types of stents with a double-layer structure have been designed to minimize plaque prolapse and embolization; these double-layer stents (DLSs) should be able to reduce the stroke risk; however, definite data on their performance are scarce in the literature.
Methods:
A systematic search was performed through PubMed, Scopus, and Cochrane Library, according to PRISMA guidelines; all studies on CAS with DLS (Roadsaver/Casper or CGuard) up to January 1, 2022, with a cohort of at least 20 patients were considered eligible. The present meta-analysis was approved and registered on PROSPERO register (CRD42022297512). Patients with tandem lesions or complete carotid occlusion were excluded from the study. The 30-day stroke rate after CAS was analyzed evaluating the preoperative symptomatic status and DLS occlusion. The estimated pooled rate of events was calculated by random effect model and moderators were evaluated.
Results:
A total of 14 studies were included in the meta-analysis for a total of 1955 patients. The estimated overall (95% confidence interval [CI]) stroke rate was 1.4% (0.9%–2.2%, I2 = 0%), which was not influenced by the type of DLS used: CGuard 0.8% (0.4%–1.8%, I2 = 0%) versus Roadsaver/Casper 1.5% (0.7%–3.2%, I2 = 0%), p=0.30. The 30-day estimated stroke rate was 1.5% (0.8%–2.9%, I2 = 0%) in asymptomatic and 1.9% (1.0%–3.6%, I2 = 0%) in symptomatic patients, with no influence by moderators. The 30-day DLS occlusion rate was 0.8% (0.4%–1.8%, I2 = 0%). The publication bias assessment identified asymmetry in the asymptomatic populations.
Conclusion:
The overall 30-day stroke rate in CAS with DLS is low (1.4%), with similar results in symptomatic and asymptomatic patients. Acute occlusion of DLS is rare (0.8%). Further studies are necessary to reduce the publication bias for asymptomatic patients.
Clinical Impact
CAS with DLS is associated to a low rate of 30-day stroke in both symptomatic (1.9%) and asymptomatic (1.5%) patients. The type of DLS (CGuard or Roadsaver/Casper) did not affect the 30-day stroke rate.
Introduction
Carotid artery stenting (CAS) has a well-defined role in the treatment of carotid bifurcation stenosis as an alternative to the gold standard, carotid endarterectomy (CEA). Several randomized controlled trials (RCTs) confirmed the superiority of CEA over CAS in patients with symptomatic carotid stenosis,1,2 due to a higher rate of perioperative cerebral ischemic complications in CAS especially in the early period after the onset of symptoms. 3 On the contrary, asymptomatic carotid stenosis can be treated by either option with comparable results,4,5 validating the role of CAS as an alternative to CEA.
All the CAS procedures in RCTs were conducted with different types of carotid stents, but recently new types of carotid stents have become available. These new devices are characterized by a double-layer stent (DLS), thought to minimize the embolic potential from the plaque, 6 and are represented by two products, Roadsaver/Casper (Terumo Corp., Tokyo, Japan) and CGuard (InspireMD Inc., Boston, Maryland, USA), both of which showed encouraging preliminary results. However, the results reported in the literature are based on composite populations, including both symptomatic and asymptomatic patients, having no neat comparison in previous meta-analyses. 7 Moreover, some authors have hypothesized an increased risk of acute stent thrombosis in DLS. 8
The aim of this study was to perform a meta-analysis of studies regarding CAS with DLS (1) to evaluate the stroke rate in symptomatic and asymptomatic patients and (2) to assess the rate of acute carotid occlusion.
Materials and Methods
The systematic review and meta-analysis were performed according to the Cochrane Collaboration recommendations. 9 A rigorous protocol was established before the analyses, concerning all the objectives, inclusion and exclusion criteria, primary and secondary outcomes, and synthesis methods. We reported the results according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) 10 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 11 recommendations.
Literature Source and Search Strategy
Electronic databases, including PubMed, Embase, and Cochrane Database, were searched up to January 1, 2022 for potentially eligible studies published in English. The reference lists of the gathered reports were manually searched for relevant articles. The following medical subject headings terms or keywords were used: ((( artery stent*[Title/Abstract]) OR (carotid artery stenting [Title/Abstract])) OR (carotid artery[Title/Abstract])) AND ((stent*[Title/Abstract]) OR (stenting[Title/Abstract]))) AND ((((((double layer[Title/Abstract]) OR (double mesh[Title/Abstract])) OR (dual mesh[Title/Abstract])) OR (dual layer[Title/Abstract])) OR (layer[Title/Abstract])) OR (mesh[Title/Abstract])).
The study project was approved and registered in the international prospective register of systematic reviews (PROSPERO 2022 CRD42022297512, Available at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022297512).
Selection Criteria
Two investigators (R.P. and F.C.) independently performed a literature search. The two investigators independently reviewed the titles and abstracts of all citations to identify potentially relevant studies and to exclude duplicates. The investigators reviewed the full text of the corresponding publications to assess if the studies met the inclusion criteria. The references from the articles obtained were also analyzed. The literature search focused solely on articles published in peer-reviewed journals, to enhance the methodological rigor of studies examined. The studies were included if they were cohort studies or case series of at least 20 patients reporting stroke rate after DLS offered for symptomatic or asymptomatic carotid artery stenosis. Only transfemoral CAS procedures were considered: data in the same series of tandem lesions of the proximal common carotid artery or the intracranial arteries (e.g. thrombus removal) were excluded and not considered for the meta-analysis.
Studies including treatment for complete carotid occlusion were not included. Studies were excluded from quantitative pooled analysis if (1) they included only tandem lesions; (2) they overlapped with other papers by the same institution (in such cases, the paper chosen for the meta-analysis was the most recent one, or the one with more useful details); (3) dual antiplatelet therapy was not administrated after carotid stenting (no specific analysis about the type of antiplatelet was performed). If the data allowed to exclude the cases with tandem lesions or acute occlusion, the paper was considered for the meta-analysis; otherwise, the study was omitted from meta-analysis. The final inclusion of the studies was based on agreement between the reviewers. Any disagreement was resolved by discussion and consultation with the other coauthors (G.F. and K.I.P.). The types of stents considered in the present meta-analysis were:
Roadsaver/Casper (Terumo Corp., Tokyo, Japan): This is the same device with two different names. The dual-layer, carotid artery self-expandable stent is an all-nitinol device. The inner layer has pores measuring 375 μm in diameter. It has a rapid exchange delivery system compatible with a 5.2 Fr catheter with a 0.014-inch guidewire. The inner layer acts as a covered stent but the micromesh is inside the stent.
The CGuard (InspireMD Inc., Boston, Maryland, USA) is a carotid stent with a self-expandable rapid exchange delivery system compatible with a 6 Fr catheter. The nitinol structure is covered externally with a patented closed cell MicroNet mesh, made of single-knitted polyethylene terephthalate fibers of 20 μm in thickness, designed for improved embolic prevention. With the stent fully expanded, the mesh porosity is 150–180 μm.
Outcome Measure and Moderators
The primary outcome was a quantitative estimated pooled analysis of 30-day stroke rates after CAS. The meta-analysis was also aimed to evaluate the rate of stent occlusion. The type of DLS was evaluated by dividing studies using Roadsaver/Casper stent or CGuard, the two different DLSs available in the market at this time (subgroup meta-analysis). Other moderators considered were patients’ mean age, percentage of males, year of publication, and routine usage of cerebral protection devices. Characteristics of the included studies (period, state, and city of development, design, and enrollment) were also extracted.
Quality Assessment
We assessed interstudy quality by evaluating the inclusion criteria in the studies and the method used to define stroke. The Newcastle–Ottawa Scale (NOS) 12 was applied to evaluate the methodology quality of the included studies. The threshold of six stars or greater was considered as indicative for high-quality studies; studies with NOS <6 were considered for specific sensitivity analysis. Also the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) (https://training.cochrane.org/handbook/current/chapter-25) tool was used: the assessment of risk of bias in a non-randomized study was addressed in pre-intervention, at-intervention, and post-intervention features of the study. Based on answers to the signaling questions, judgments for each bias domain, and for overall risk of bias, can be “Low,” “Moderate,” “Serious,” or “Critical” risk of bias. Studies with “serious,” “critical” and with no information were considered for a specific sensitivity analysis.
Data Synthesis and Heterogeneity Assessment
The statistical analysis was performed using ProMeta 2.0 software (Internovi, Italy, https://www.meta-analisi.it/prometa-software/). Values of proportion outcomes were expressed as proportions and 95% confidence intervals (CIs). The pooled effect estimates were calculated as the back transformation of the weighted mean of the transformed proportions, using DerSimonian–Laird weights of random effects model and expressed as percentage proportions. Because of the heterogeneity of the observational studies, we assessed a priori the random effects model. To test for the overall effect, a Z-test was used, and statistical significance level was set to p<0.05. The data were graphed as a forest plot. Heterogeneity among the studies was estimated by the I 2 test representing the percent value of heterogeneity. An I 2 value <30% was considered as low heterogeneity, between 30% and 49% as moderate, between 50% and 80% as substantial, and >80% as considerable heterogeneity. 13
Meta-regression was performed to assess whether the outcome varied as a function of selected moderators independently from the level of heterogeneity. A subgroup meta-analysis was performed according to the categorical variables, the analysis of variance (ANOVA) Q-Test Random Effect with pooled estimate of T2 (https://www.meta-analysis.com/downloads/Meta-analysis%20Subgroups%20analysis.pdf) was performed to compare the estimated pooled rate of stroke for categorical moderators in subgroup meta-analysis.
Sensitivity analysis and cumulative analysis were performed to test the stability of studies and in cases of outlier studies, identified by the evaluation of studies with NOS <6 and with “Serious” or “Critical” or “No information” risk of bias with ROBINS-I tool.
Study Bias Evaluation
The interstudy bias evaluation (performed by R.P.) focused on the type of evaluation of the outcomes and the NOS and ROBINS-I values of the studies included. The between-studies bias evaluation was performed by the funnel plot visual evaluation. Publication bias was formally assessed using the Egger regression intercept and with the trim-and-fill method. In this method, the tail of the side of the funnel plot with the smaller studies is chopped off to make the funnel plot symmetrical, and it is then replicated and added back to both sides so the plot becomes symmetrical; the center and variability of the filled funnel plot are then estimated.14,15
Results
Study Selection, Characteristics, and Quality Assessment
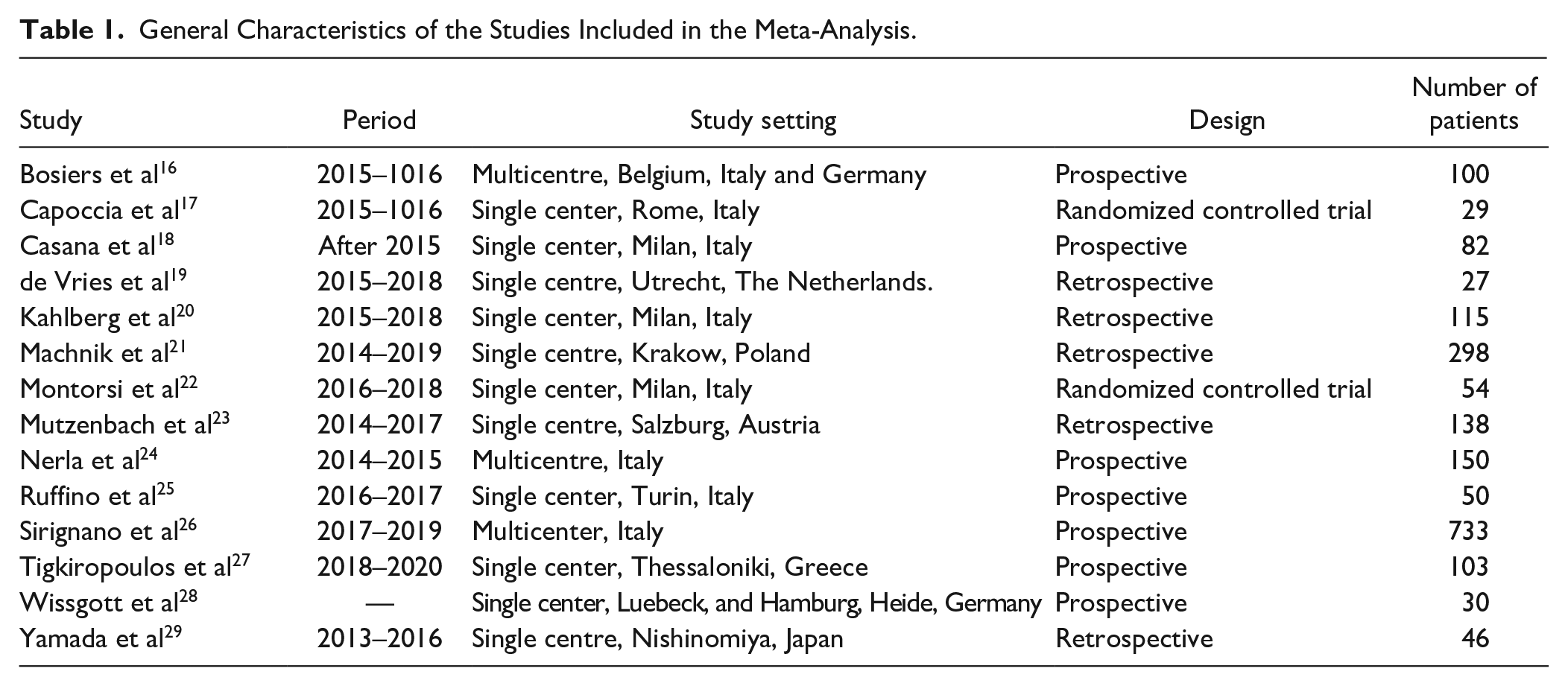
Figure 1 reports the literature search and the process of papers selection for this study. After the screening process and duplicate studies removal, a total of 14 papers16 –29 were included in the analysis. Tables 1 and 2 report the characteristics of the studies included. The median NOS value was 7 (ranging from 6 to 8); no study had an NOS value <6 or “Serious” or “Critical” risk of bias at ROBINS-I tool evaluation. High level of agreement (>90%) was present between the investigators (R.P. and F.C.) in the phases of study selection and data extraction.
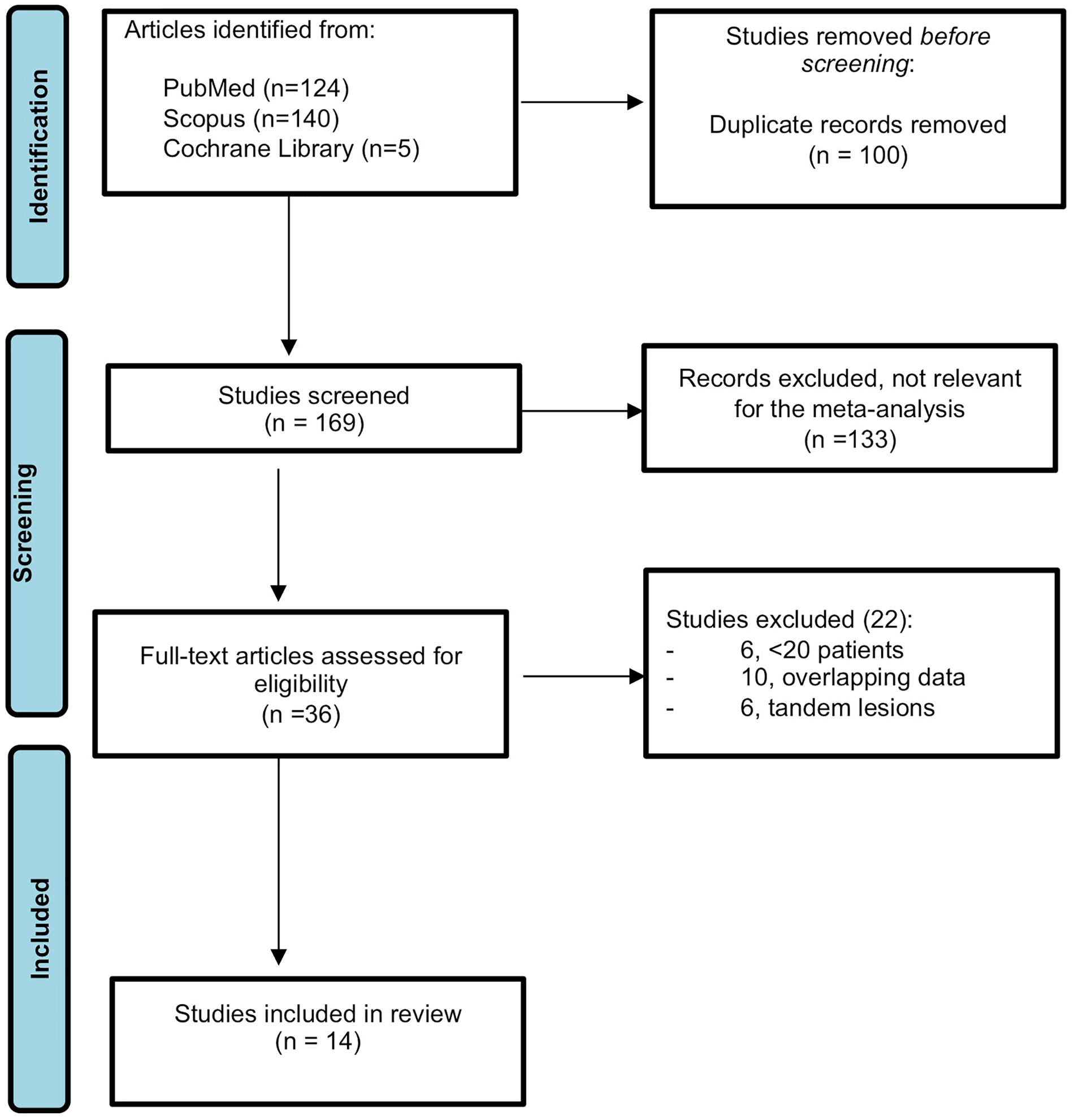
Flow-chart of selected studies.
General Characteristics of the Studies Included in the Meta-Analysis.
Results of Studies Included in the Meta-Analysis.
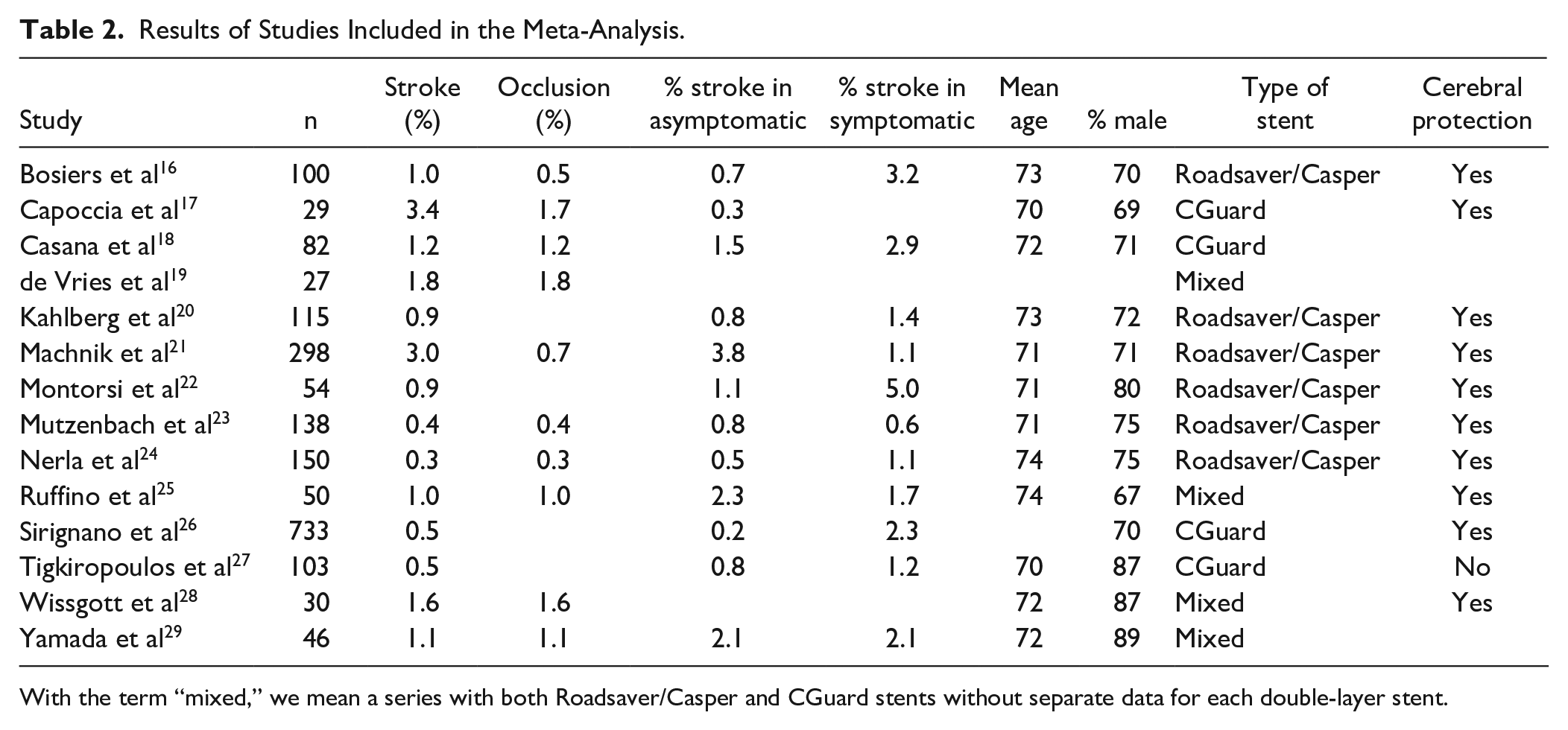
With the term “mixed,” we mean a series with both Roadsaver/Casper and CGuard stents without separate data for each double-layer stent.
Estimated Pooled Proportions of the Different Meta-Analysis and Moderators Analysis Performed for Outcome Measurement.
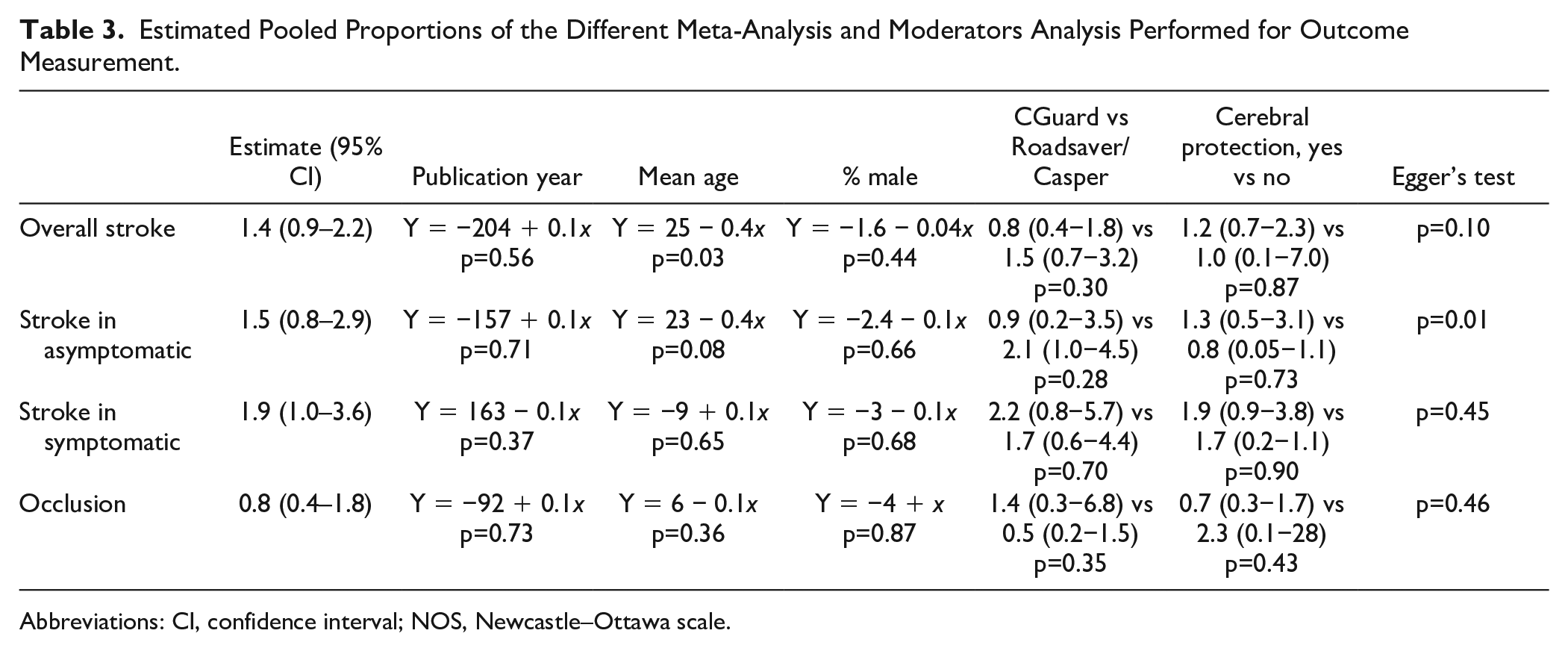
Abbreviations: CI, confidence interval; NOS, Newcastle–Ottawa scale.
Stroke rate
For the primary outcome of stroke, all 14 studies were considered, for a total of 1955 patients. The pooled rate of stroke was 1.4% (95% CI = [0.9%–2.2%]; I2 = 0%; Figure 2). The analysis of moderators did not identify any factor associated with stroke (including the type of stent used, Figure 3) except for mean age (Table 3). The between-study bias evaluation was performed by the funnel plot analysis and showed a good level of symmetry, with a p=0.1 at the Egger test. The trim-and-fill method did not identify any asymmetrical study and confirmed the pooled event rate. The sensitivity analysis confirmed the outcome.
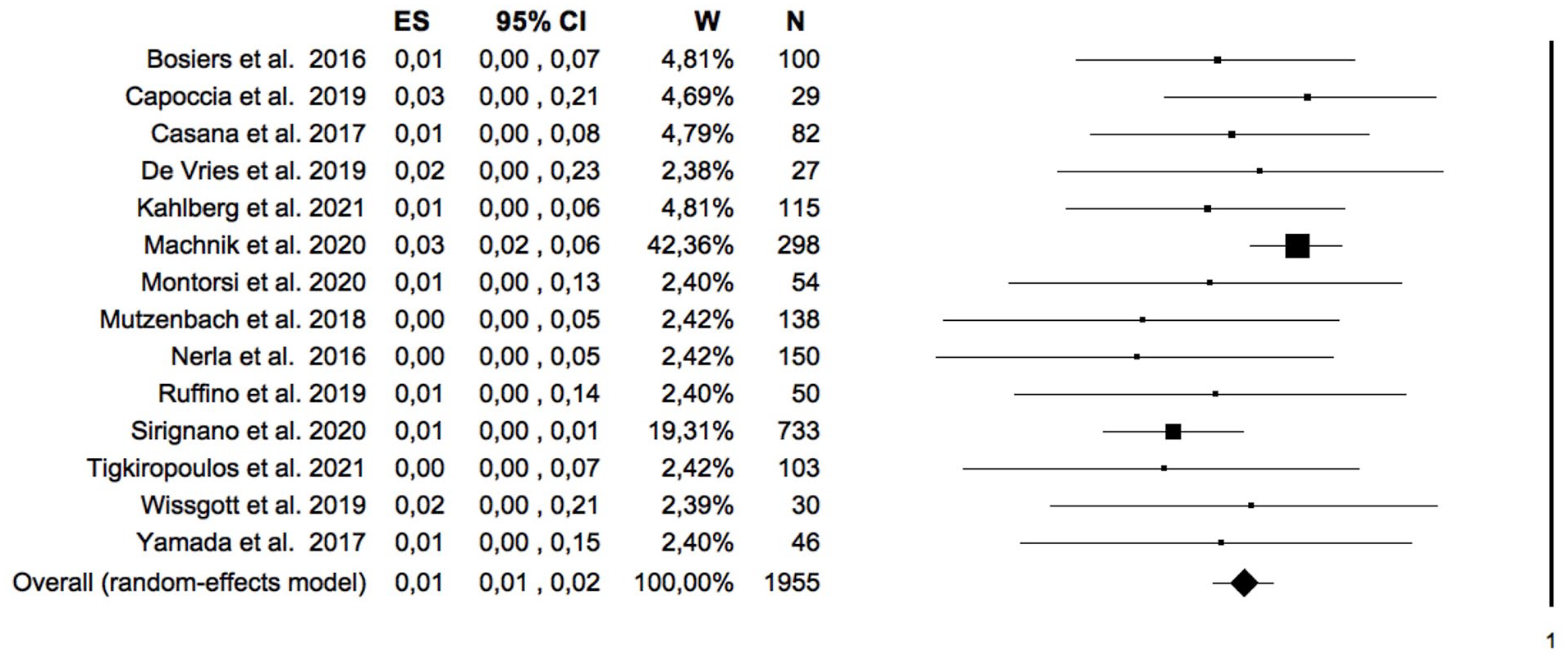
Forest plot of the pooled estimate rate of 30-day stroke after double-layer carotid stent. Heterogeneity analysis: Q=12.9; df=13; Sig.=0.45; I2 = 0%. CI, confidence interval; ES, effect size; W, weight; N, number.
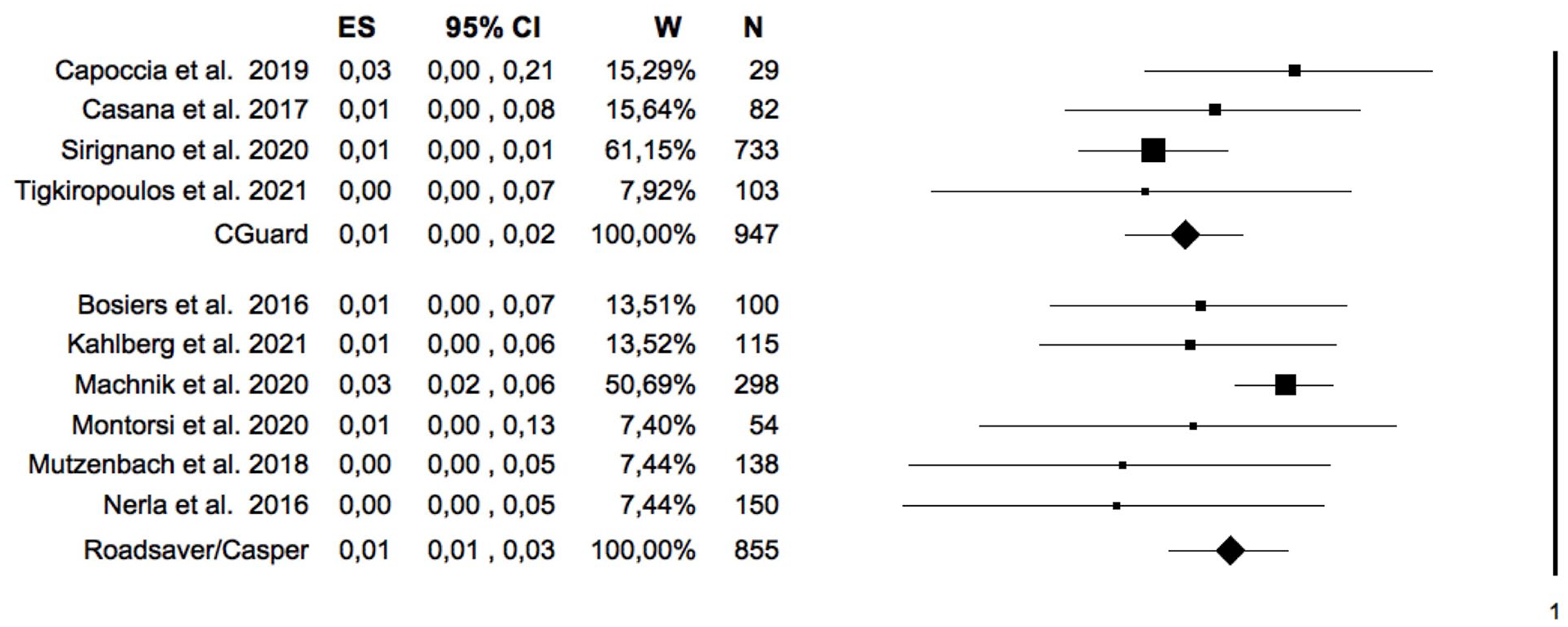
Forest-plot of the pooled estimate rate of 30-day stroke after double-layer carotid stent with Roadsaver/Casper and CGuard. ANOVA Q-Test Random Effect with pooled estimate of T2: P = .30. CI, confidence interval; ES, effect size; W, weight; N, number.
Stroke in asymptomatic patients
A separate meta-analysis was performed for only asymptomatic patients including 12 studies for a total of 1358 patients. The pooled rate of stroke was 1.5% (95% CI = [0.8%–2.9%]; I2 = 17%). The analysis of moderators did not identify any factor associated with stroke (Table 3).
The between-study bias evaluation was performed by the funnel plot analysis and showed a low level of symmetry, with a p=0.01 at the Egger test. The trim-and-fill method did not identify any asymmetrical study and confirmed the pooled event rate.
Stroke in symptomatic patients
A separate meta-analysis was performed for only symptomatic patients including 11 studies for a total of 525 patients. The pooled rate of stroke was 1.9% (95% CI = [1.0%–3.6%]; I2 = 0%). The analysis of moderators did not identify any factor associated with stroke (Table 3). The between-study bias evaluation was performed by the funnel plot analysis and showed a good level of symmetry, with a p=0.45 at the Egger test. The sensitivity analysis confirmed the outcome.
DLS occlusion
Data on stent occlusion were reported in 10 studies (930 patients) and the pooled rate was 0.8% (95% CI = [0.4%–1.8%]; I2 = 0%), Figure 4. The analysis of moderators did not identify any factor associated with stroke (Table 3). The between-study bias evaluation was performed by the funnel plot analysis and showed a good level of symmetry, with a p=0.46 at the Egger test. The trim-and-fill method did not identify any asymmetrical study and confirmed the pooled event rate (Figure 5). The sensitivity analysis confirmed the outcome.
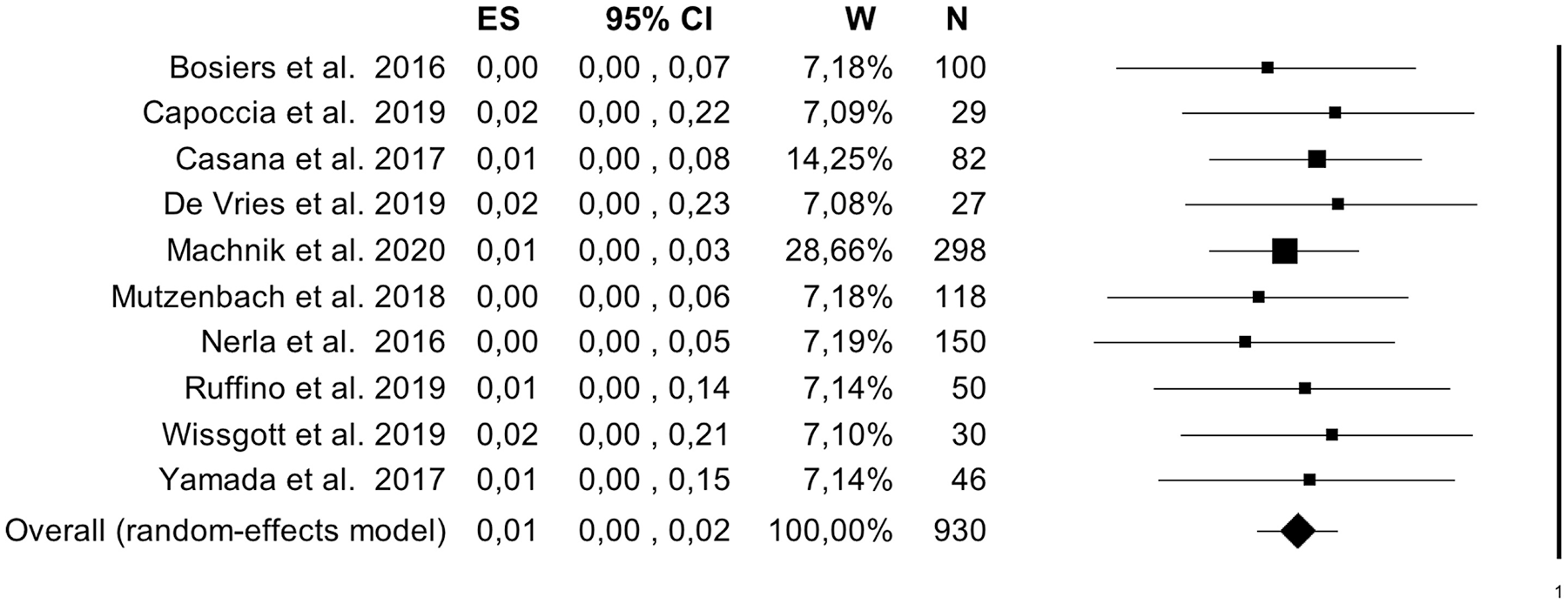
Forest plot of the pooled estimate rate of 30-day stent occlusion after double-layer carotid stent. Heterogeneity analysis: Q = 1.84; df = 9; Sig. = 0.99; I2 = 0%. CI, confidence interval; ES, effect size; W, weight; N, number.
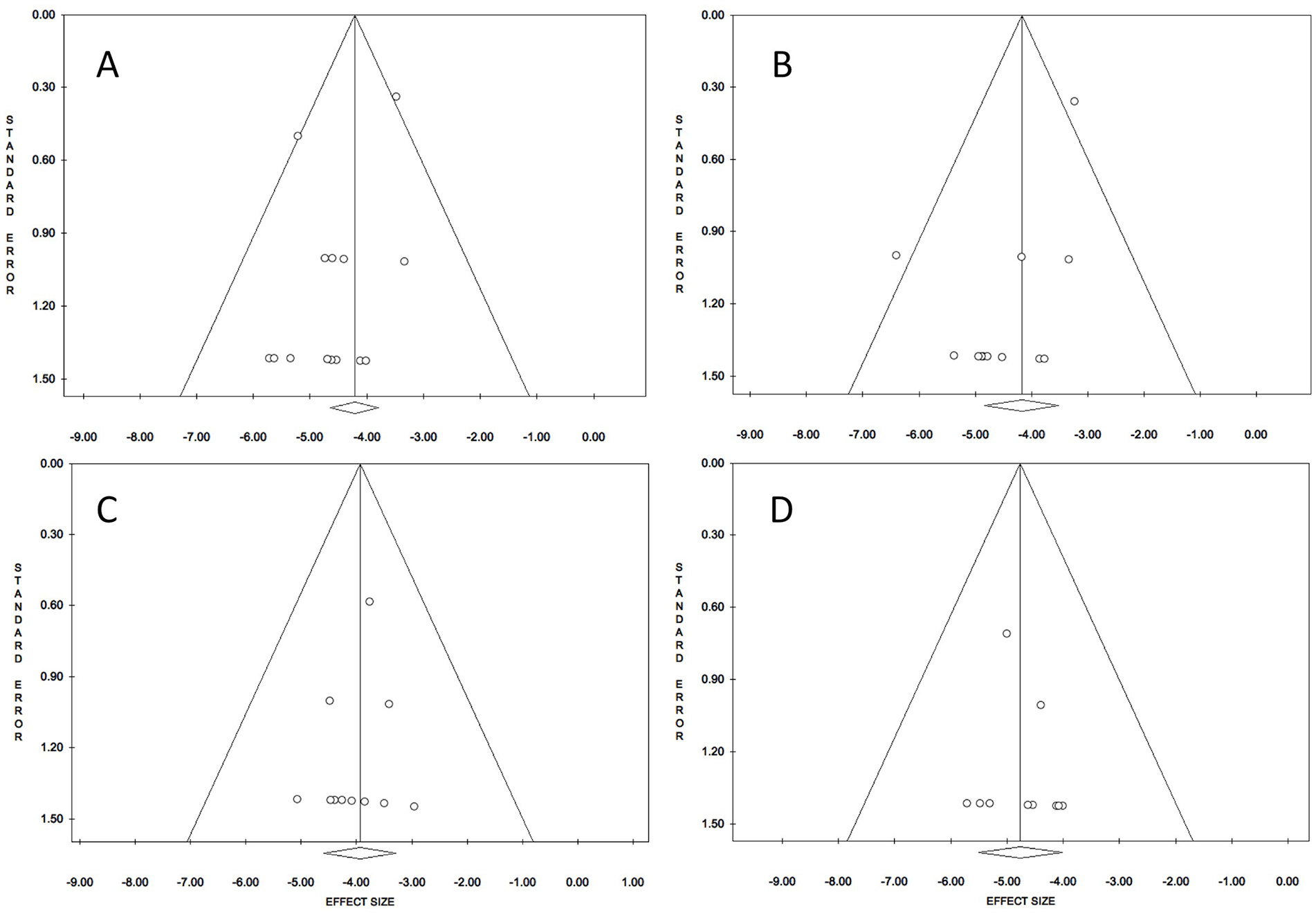
Funnel plot for overall stroke (A), stroke in asymptomatic patients (B), stroke in symptomatic patients (C), and occlusion (D) at 30-day after dual-layer carotid stent.
Discussion
The present meta-analysis reports the 30-day stroke rate of 14 studies on CAS with DLS. These new devices are proposed to reduce the risk of plaque prolapse and, consequently, the stroke rate associated with CAS. However, no large prospective studies comparing classical stents and DLS have been performed to date. In a RCT including 61 patients, Capoccia et al 17 found similar cerebral lesions at diffusion-weight magnetic resonance after CAS with CGuard or carotid Wallstent (Boston Scientific, Marlborough, MA, USA). On the contrary, Montorsi et al 22 randomized 104 patients in four groups according to the type of carotid stent and the type of cerebral protection device; the authors analyzed the micro-embolic signals on transcranial Doppler and identified a lower rate of micro-embolic signals with the use of Roadsaver and proximal occlusion devices for cerebral protection.
With this study, we aimed to evaluate the stroke rate of DLS, analyzing patients and stratifying them according to their symptomatic status. The systematic review identified 14 eligible studies, excluding series with less than 20 cases and studies with concomitant intracranial procedures for tandem lesions where possible overlapping data may have occurred (in particular, the PARADIGM 30 and CARENET 31 trials), for a total of 1955 patients. The overall 30-day stroke rate is 1.4%, with a low level of heterogeneity of the studies (I2 = 0). The low rate of stroke is certainly driven by the asymptomatic patients; the stroke rate in the meta-analysis extrapolating only the asymptomatic patients is 1.5%. The present results are not influenced by moderators and the two types of DLS have a similar outcome (0.9% CGuard and 2.2% Roadsaver/Casper, p=0.28). Similarly, the use of cerebral protection devices, evaluated as a moderator did not affect the outcome. However, only one study did not use routinely the cerebral protection devices without strokes in its series. 27
The data from the present meta-analysis are remarkable since the last available RCTs on asymptomatic patients reported a higher stroke rate, 3.6% in ACST-2 5 and 2.8% in ACT trial. 4 Certainly, the RCTs with a strict follow-up are more accurate in the detection of 30-day stroke compared with retrospective studies; in fact, by evaluating the outcome reported by some registries, the differences between DLS and old stents seem reduced. The United Kingdom Carotid Artery Stent Registry 32 reported a 30-day stroke rate of 2.2% in 201 asymptomatic patients and the Society for Vascular Surgery (SVS) vascular registry 33 a rate of 2.1% in 805 patients.
The good outcome in the asymptomatic patients of CAS in the real-world studies can be due to a lower vulnerability of the carotid plaque in these patients; furthermore, a quote of events are probably determined mainly by the aortic navigation and carotid catheterization that are a source of cerebral embolization independently from the carotid stent used. 17
In our meta-analysis, we have also evaluated symptomatic patients, who had a 30-day stroke rate as low as 1.9% in 525 patients. Previous trials reported a much higher rate of stroke: The Carotid Revascularization Endarterectomy versus Stenting Trial (CREST) 1 reported a 30-day stroke rate of 4.1% (even though one-third of the patients were asymptomatic); and in the International Carotid Stenting Study (ICSS), 2 the per-protocol 30-day stroke rate was 7.0%. The reduction of cerebral events seems to be lower with DLS even when compared with national registries: the United Kingdom Carotid Artery Stent Registry reported a 30-day stroke rate of 5.5% in 953 symptomatic patients and the SVS vascular registry a rate of 5.3% in 645 patients.32,33 The low rate of stroke in symptomatic patients treated with DLS can be justified by the design of the stents and the low risk of plaque prolapse or micro-embolization after stent apposition.
Nevertheless, different outcomes of DLS in symptomatic patients are reported in the literature. In particular, the DLSs were commonly used by neuroradiologists in the treatment of tandem lesions of carotid stenosis and intracranial arteries occlusions. In many instances with concomitant intracranial vascular procedures (not included in the present meta-analysis), the rate of perioperative stroke seems to be increased: Foo et al 34 reported a 5.3% stroke rate and a 6.4% DLS acute thrombosis rate in 94 patients submitted to CAS for acute stroke; the extensive involvement of cerebral vessels in these patients justify the higher rate of stroke compared with other studies with no tandem lesions treatment.
De Vries et al 19 reported a different experience with DLS in the emergent stroke treatment. The authors described the treatment of acute stroke also including carotid occlusions and concomitant intracranial procedures (27 patients excluded from the meta-analysis), in which they reported five cases of DLS occlusions (19%) with three (11%) cases of neurological deterioration.
Some authors considered the acute DLS occlusion as a specific complication of the design of these stents. In the present meta-analysis, this particular aspect was separately evaluated. The rate of DLS occlusion reported in the present meta-analysis is 0.8% over a total of 930 patients. These results are strikingly different from the data of Runck et al 8 and Yilmaz et al 35 who reported a 24% and a 45% DLS thrombosis rate in the treatment of acute strokes, respectively (including tandem lesions). The DLS thrombosis rate in the present meta-analysis (0.8%) seems to be similar to the results reported by Moulakakis et al. 36 They described a series of 674 CAS with standard stents, having four cases (0.6%) of acute thrombosis, possibly secondary to carotid dissections and overlapping of a second stent. 37
Current guidelines do not mention DLS, suggesting CAS only in selected cases when CEA is considered at high risk (hostile neck or high surgical risk). The recommendations come from the evidence of higher risk of stroke in CAS compared with CEA for both symptomatic and asymptomatic patients. Therefore, the results from the present meta-analysis should be taken into account from future guidelines considering the extremely low rate of stroke after carotid stenting with DLS.38,39
The TCAR is a new technology that was considered in the updated 2022 SVS guidelines. 40
The SVS guidelines underlined the absence of a large RCT but analyzed the vascular quality initiative registry. More specifically, the paper by Schermerhorn et al reported the results on 3200 patients, with a lower rate of in-hospital stroke/death after TCAR compared with transfemoral CAS (1.6% vs 3.1%, p=0.001); the study by Malas et al showed similar outcomes comparing TCAR with CEA for symptomatic patients (2.2% vs 2.6%; p=0.46).41,42
The DLS can be used both in transfemoral CAS and in TCAR and it is plausible that DLS can further reduce the stroke rate of TCAR.
Another possible thrombotic complication associated with DLS use is the thrombosis of the external carotid artery. In the IRONGUARD 2 study (only CGuard DLS), Sirignano et al 26 reported a 1.1% rate of external carotid artery thrombosis without any associated neurological event; due to the low rate of occurrence and the absence of neurological complications, the latter seems to be a benign complication.
The present meta-analysis has some limitations, namely the retrospective nature of most studies and the absence of a standardized neurological evaluation, leading to a possible underestimation of stroke rates. Moreover, in the meta-analysis of asymptomatic patients, the Egger’s test and the asymmetry in the funnel plot suggest possible publication bias; thus, further studies are necessary to confirm the present results. The experience and the volume of the centers have a determinant role in the CAS outcome, with a reduction of neurologic events in high experience centers; however, it was not possible to investigate this moderator in the present meta-analysis. 43 The cerebral micro-embolization detected by diffusion weight magnetic resonance imaging can be considered a surrogate of a cerebral event; it can be investigated further to broadly evaluate the effect on the reduction of embolization risk; however, the aim of the present meta-analysis was to evaluate only the clinical effect of DLS; for this reason, this specific aspect was not investigated.
Conclusion
The present meta-analysis of DLS for CAS suggests that the stroke rates with these new devices are low in both symptomatic and asymptomatic patients. The rate of acute thrombosis is also low; however, further studies are necessary to confirm the findings of these retrospective series with prospective data.
Supplemental Material
sj-docx-1-jet-10.1177_15266028221126940 – Supplemental material for Carotid Artery Stenting With Double-Layer Stent: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jet-10.1177_15266028221126940 for Carotid Artery Stenting With Double-Layer Stent: A Systematic Review and Meta-Analysis by Rodolfo Pini, Gianluca Faggioli, Kosmas I. Paraskevas, Federica Campana, Gemmi Sufali, Cristina Rocchi, Sergio Palermo, Enrico Gallitto and Mauro Gargiulo in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.