
Abstract
Purpose:
In Paget-Schroetter Syndrome (PSS), subclavian vein thrombosis is caused by external compression of the subclavian vein at the costoclavicular junction. Paget-Schroetter Syndrome can be treated nonoperatively, surgically, or with a combination of treatments. Nonoperative management consists, in most cases, of anticoagulation (AC) or catheter-directed thrombolysis (CDT). With surgical management, decompression of the subclavian vein is performed by resection of the first rib. No prospective randomized trials are available to determine whether nonoperative or surgical management is superior. We report our long-term outcomes of both nonoperative and surgically treated patients.
Materials and Methods:
We retrospectively analyzed all patients with PSS who were treated between January 1990 and December 2015. Patients were divided based on primary nonoperative or primary surgical therapy. Long-term outcomes regarding functional outcomes were assessed by questionnaires using the “Disability of the Arm, Shoulder, and Hand” (DASH) questionnaire, a modified Villalta score, and a disease-specific question regarding lifestyle changes.
Results:
In total, 91 patients (95 limbs) were included. Seventy patients (73 limbs) were treated nonoperatively and 21 patients (22 limbs) surgically. Questionnaires were returned by 67 patients (70 limbs). The mean follow-up was 184 months (range, 43–459 months). All functional outcomes were better in the surgical group compared with the nonoperatively treated group (DASH general 3.11 vs 9.86; DASH work 0.35 vs 11.47; DASH sport 5.85 vs 17.98, and modified Villalta score 1.11 vs 3.20 points). Surgically treated patients were more likely to be able to continue their original lifestyle and sports activities (84% vs 40%, p=0.005). Patients with recurrence of thrombosis or the need for surgical intervention after primary nonoperative management reported worse functional outcomes.
Conclusion:
Surgical management of PSS with immediate CDT followed by first rib resection leads to excellent functional outcomes with low risk of complications. The results of nonoperative management in our non-matched retrospective comparative series were satisfactory, but resulted in worse functional outcomes and more patients needing to adjust their lifestyle compared with surgically treated patients.
Clinical Impact
Patients with Paget-Schroetter Syndrome and their attending physicians are burdened by the lack of evidence concerning the optimal treatment of this entity. Case series comparing the outcomes of non-operative treatment with surgical treatment are scarce and often not focussed on functional outcomes. Data from this series can aid in the shared decision making after diagnosis of Paget-Schroetter Syndrome. Functional outcomes of non-operative management can be satisfying although high demand patient who are not willing to alter their daily activities are probably better off with surgical management.
Keywords
Introduction
Paget-Schroetter Syndrome (PSS) is effort-induced subclavian vein thrombosis and can be classified as a separate entity within venous thoracic outlet syndromes (vTOS). Paget-Schroetter Syndrome can be treated nonoperatively, surgically or by a combination of treatments. Nonoperative treatment can be anticoagulation (AC), catheter-directed thrombolysis (CDT), or other comparable catheter-based therapies. Surgical therapy is aimed to prevent recurrence of thrombosis and consists of decompression of the subclavian vein by resection of the first rib after patency is restored with AC or CDT. Currently, there is no consensus on the optimal management of PSS. 1 Published reports are predominantly retrospective in design and limited by short follow-up and/or not well-documented functional outcomes. Therefore, we investigated the long-term functional outcomes of both nonoperative and surgically treated patients with PSS.
Methods
Current Local Treatment Protocol
After presentation at the emergency department or referral by a general practitioner, patients are seen by a vascular surgeon or internist. Diagnosis of PSS is preferably made by duplex ultrasound examination or computed tomography (CT) venography (if duplex is not available, out of office hours). Considering the lack of evidence on superiority of nonoperative management or intervention, both treatment strategies are discussed with the patient and a decision is made using shared decision-making. Nonoperative management consists of oral anticoagulation with vitamin K antagonists or direct oral anticoagulant (DOAC). For nonoperative treatment, no standard follow-up imaging was performed and clot resolvement was not investigated as standard practice.
Surgical management consists of CDT followed by scheduled first rib resection (FRR). Preoperative percutaneous transluminal angioplasty (PTA) was performed in case of persistent venous wall irregularities. Postoperative duplex or venography was performed to asses patency and assess the need for additional PTA.
Study Design
Approval for this research was obtained from the Medical Ethics Review. Our institutional Research Data Platform provided all patients diagnosed with upper extremity deep venous thrombosis (UEDVT) during the period January 1, 1990, and December 31, 2015, using financial and medical coding information from the Departments of Surgery and Internal Medicine. An additional search identified all patients who underwent FRR during the same period. All identified patients were screened for the diagnosis of PSS. Paget-Schroetter Syndrome was defined as UEDVT without any secondary cause: active malignancy, central intravenous line, pacemaker leads, pregnancy, hormonal hyperstimulation during fertility treatment, related to arterovenous fistula in chronic kidney disease, or trauma. The medical files of all patients with PSS were further reviewed. All patients eligible for inclusion were contacted by phone and were asked to participate in this study. If patients were willing to participate, informed consent forms and the following questionnaires were sent by mail. Overall functional outcomes were assessed using the validated Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire. 2 Post-thrombotic complaints were self-assessed with a 7-point modification (symptoms only) of the Villalta score (supplemental document 1). Additional information regarding any changes in lifestyle or sporting activity was obtained with a disease-specific question (supplemental document 2). Patients were reminded several times to return their questionnaires. All patients who did not return their questionnaires before April 1, 2021, were considered not willing to participate in this study.
Statistical Analysis
Descriptive statistics were used for analyzing patients’ characteristics. Statistical analysis was performed using SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp). The DASH scores and Villalta scores of both groups were compared with a Mann-Whitney U test. The disease-specific question was analyzed with a χ2 test. A p-value of 0.05 or less was considered statistically significant. A 10-point DASH difference was considered a minimal important change. 3
Results
In total, 94 patients were identified (98 limbs, 52 men, 60 right-sided, mean age: 33 [range 16–63] years). Two patients were excluded because they were included in our robot-assisted transthoracic FRR case series as reported previously. 4 One patient was excluded because he received no treatment at all. In 76.9% (70/91 patients, 73 limbs) of patients, a nonoperative treatment was instituted as the initial management of their first PSS episode. Twenty-one patients (22 limbs) were treated with CDT followed by FRR. Twenty-four patients (nonoperative n=21, surgical n=3) were lost to follow-up (untraceable n=11, did not return their questionnaires n=7, did not want to participate n=5, deceased n=1). Questionnaires were returned by 73.6% of patients (67/91), reporting on 70 limbs.
Outcomes of Nonoperative Treatment
In total, 70 patients (73 limbs) were treated nonoperatively with anticoagulation (AC, n=43) or CDT followed by AC (n=30) (Table 1). In 8 limbs (11.0%, CDT n=4, AC n=4), initial therapy was unsuccessful in restoring patency. Of the remaining 65 limbs, recurrent thrombosis was reported in 26 (40.0%). Median time to recurrence was 32.4 months (range, 0.5–168 months) . Eventually 20 limbs underwent surgical decompression (27.4%), at a mean interval of 19 months (range, 6–168 months). Forty-nine patients returned the questionnaires corresponding with 51 limbs and were further analyzed (AC n=32, CDT n=19). The mean follow-up was 175 months (range, 43–459 months). Mean DASH scores were as follows: General 9.86 (SD, 12.81; range, 0–56.7); Work module 11.47 (SD, 19.85; range, 0–68,8); Sport module 17.98 (SD, 23.06; range, 0–87.5). The mean modified Villalta score was 3.20 (SD, 3.18; range, 0–12) with 15 (29.4%) of 51 patients scored 0 points, which corresponds with the absence of any post-thrombotic complaints. Sixty percent of patients (30/50, 20 moderate, 10 severe) altered their normal daily living or sporting routine to adjust for physical limitations after their PSS episode. A perfect minimum score of 0 points at both questionnaires and no alterations needed in daily activities were reported in 6 (11.5%) of 52 treated limbs. No statistical or clinical relevant difference was seen between patients receiving AC or CDT as primary management. Of the 20 patients who underwent FRR because of recurrent or persistent complaints, 10 needed a venous reconstruction. Patients who needed surgical treatment after failed nonoperative treatment more often had to make lifestyle adjustments (11/14 vs 19/36, p=0.004). Although also a trend was seen regarding a worse General DASH, Work-related DASH, and Villalta scores, this was not statistically significant.
Patient Characteristics and Management.
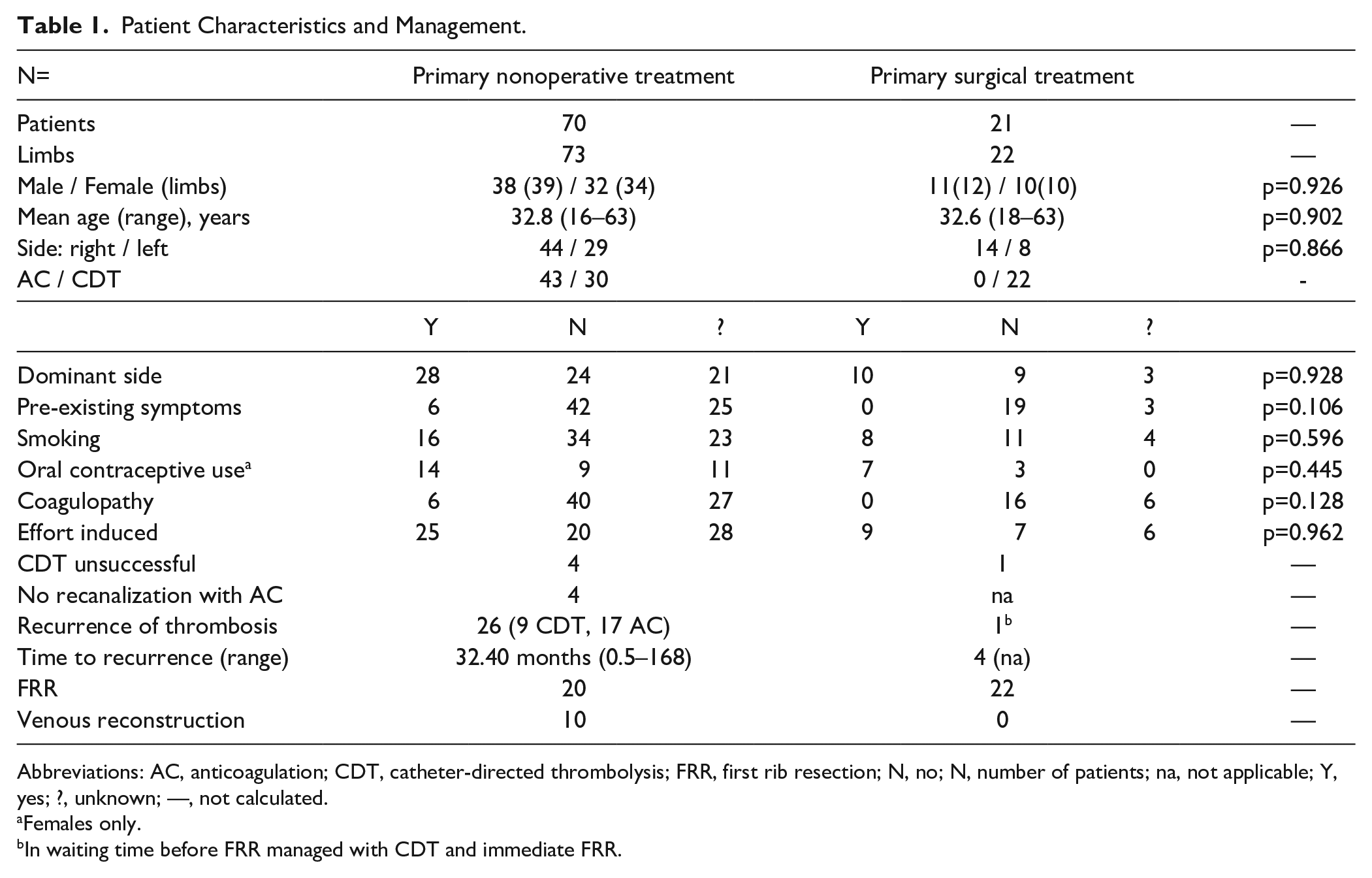
Abbreviations: AC, anticoagulation; CDT, catheter-directed thrombolysis; FRR, first rib resection; N, no; N, number of patients; na, not applicable; Y, yes; ?, unknown; —, not calculated.
Females only.
In waiting time before FRR managed with CDT and immediate FRR.
Outcomes of Surgical Management
Twenty-one patients (22 limbs) were treated with CDT followed by scheduled FRR (Table 1). Two patients did not want to participate in this study, and one patient was untraceable. The median time between PSS and FRR was approximately 4 months (122 days, range, 24–731). The transaxillar approach was used in all but 1 patient in which a paraclavicular approach was used because a venous reconstruction was performed in the same procedure. The mean operation time was 86.2 minutes (range, 55–160 minutes). The median hospital stay for FRR was 4 days (range, 1–10 days). The mean follow-up was 206 months (range, 60–370 months). The mean general DASH score was 3.11 (range, 0–30), the mean work-related DASH score was 0.35 (range, 0–6.3), and the mean sport-related DASH score was 5.86 (range, 0–37.5). The mean modified Villalta score was 1.11 (range, 0–5). Alterations in their normal daily living or sporting routine to adjust for physical limitations after their PSS were reported by 15.8% of patients (3/21, 2 moderate, 1 severe). More than half of all patients (11/21) had a perfect minimum score of 0 points at both questionnaires and were able to maintain their daily activities as before their episode of PSS.
Nonoperative Versus Surgical Management
All functional outcomes were in favor of surgical management: General DASH module (−6.75 points, p=0.005), DASH Work module (−11.12 points, p=0.013); DASH Sports module (−12.12 points, p=0.057); Villalta score (−2.09 points, p=0.006) (Table 2). Surgically treated patients were more often able to maintain their pre-existent functional and sporting activities (40% vs 85%, p=0.005). No clear relation between time and functional outcome could be identified as shown in Figure 1.
Functional Outcome of Included Patients.
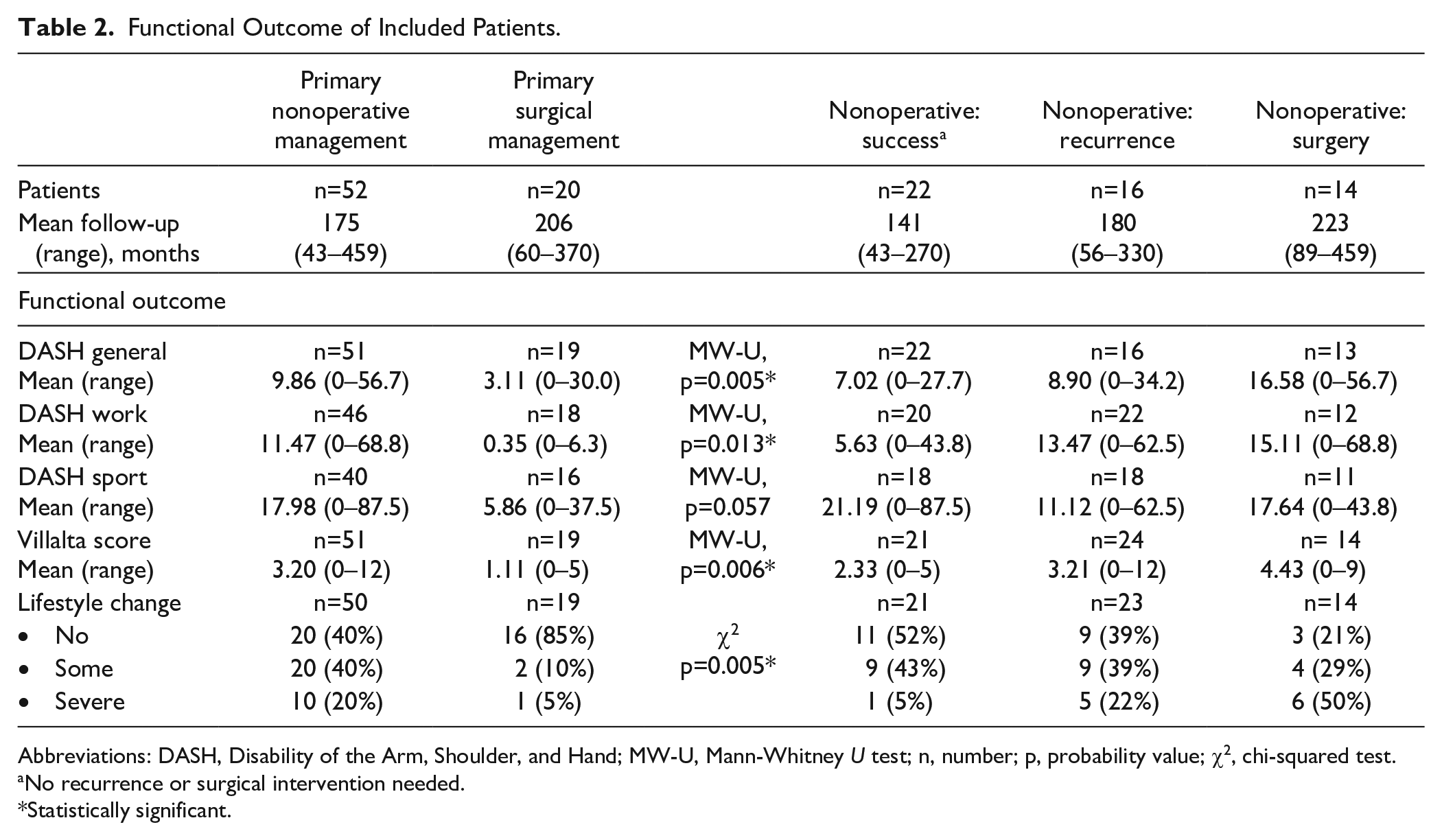
Abbreviations: DASH, Disability of the Arm, Shoulder, and Hand; MW-U, Mann-Whitney U test; n, number; p, probability value; χ2, chi-squared test.
No recurrence or surgical intervention needed.
Statistically significant.
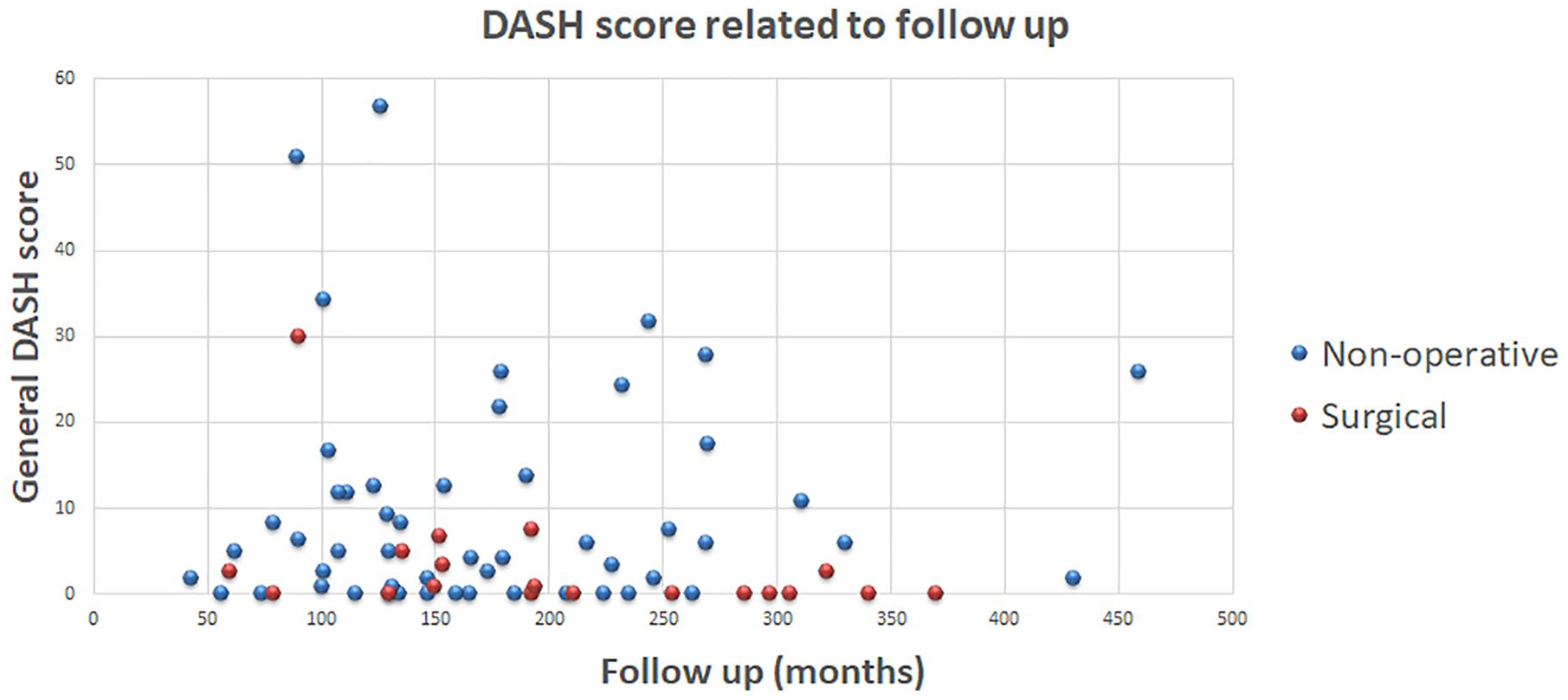
Relation between mean general DASH score and time of follow-up. DASH, Disability of the Arm, Shoulder, and Hand.
Complications
Two complications related to CDT were observed (Table 3). Hemoptysis in one patient and a vaginal bleeding in another patient warranted cessation of CDT and prevented complete restoration of flow in the subclavian vein. No further treatment was instituted at the patient’s requests. No other CDT-related adverse events were reported. Information regarding postoperative complications after FRR could be retrieved in 38 of 42 FRR (nonoperative n=18, surgical n=20). In total, 27 complications or adverse effects of FRR were recorded in 19 of 38 procedures (11/18 nonoperative, 8/20 surgical). No Clavien-Dindo grade IV (life-threatening) or grade V (death) complications were observed.
Complications of First Rib Resection.
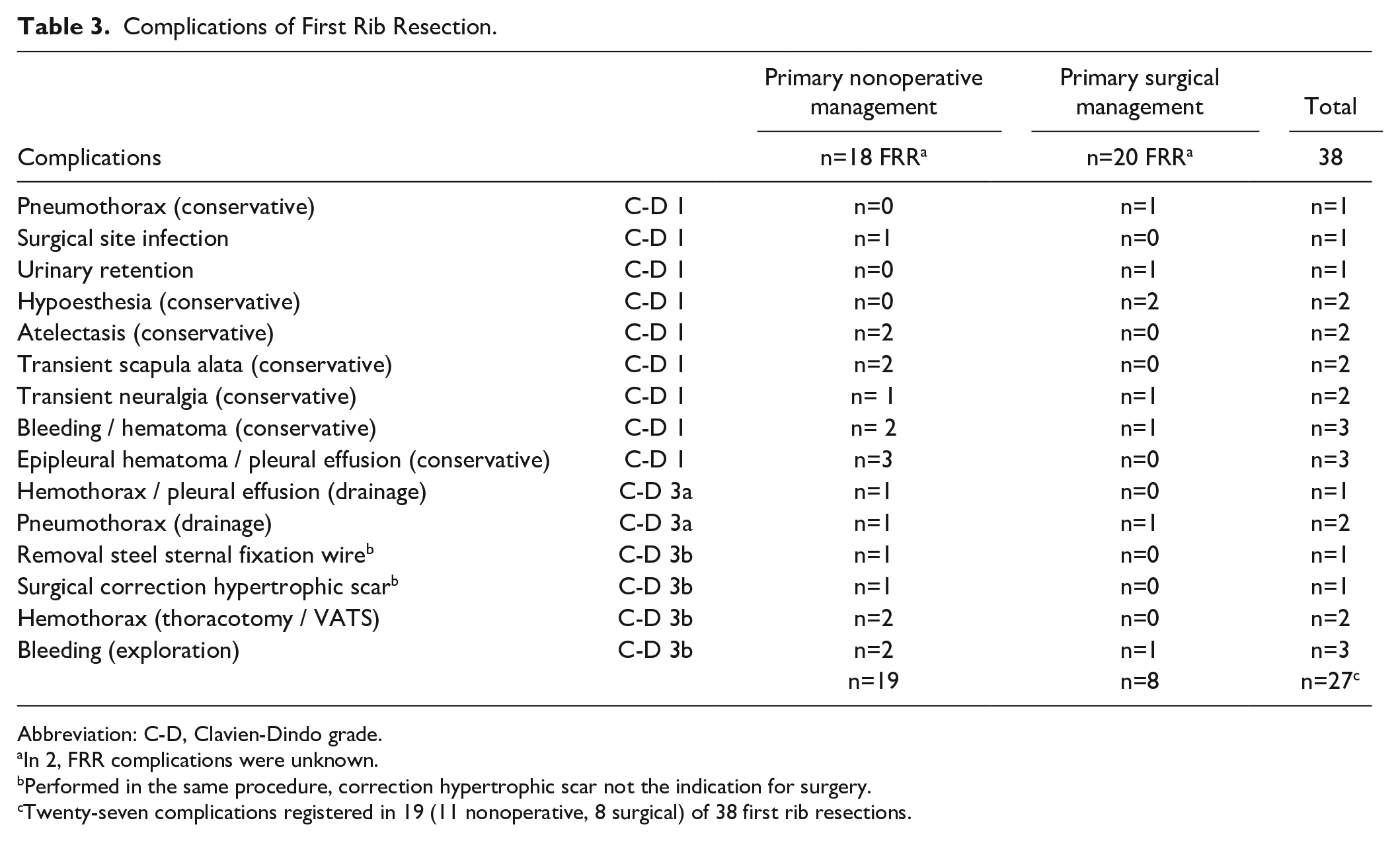
Abbreviation: C-D, Clavien-Dindo grade.
In 2, FRR complications were unknown.
Performed in the same procedure, correction hypertrophic scar not the indication for surgery.
Twenty-seven complications registered in 19 (11 nonoperative, 8 surgical) of 38 first rib resections.
Discussion
Our study provides insight into long-term functional outcome after nonoperative and surgical management of PSS. Surgical treatment results in better DASH scores and modified Villalta scores. Furthermore, surgically treated patients are less often required to change their daily activities. All DASH scores of surgically treated patients and the General DASH scores of nonoperatively treated patients are comparable to the normative population. 5 The work-related and sport-related DASH scores of nonoperatively treated patients are worse. 6 Patients treated with nonoperative therapy have a substantial risk of persistent complaints or recurrence of PSS and frequently undergo FRR eventually. In our series, persistent occlusion (n=8) or recurrence (n=26) was reported in 46.6% (34/73). Twenty patients did undergo FRR (27.4%), which is in line with the rates reported by others in literature 6 Failure of nonoperative treatment results in worse functional outcomes (Table 2).
Our recurrence rate (26/73, 35.6%) after nonoperative treatment is high compared with the recurrence rate reported in literature of 23%. 6 A possible explanation may be that our institution serves as a referral center, and therefore, the possibility of selection bias is present. This may also lead to worse functional outcomes. Patients with the need for surgical intervention after failed nonoperative management have the worst outcomes. Venous reconstruction is often needed, resulting in a more extensive procedure. The risk for postoperative complications is much higher compared with the FRR performed in the surgical group (61% vs 40%) (Table 3).
The stereotypical case presentation in literature is an adolescent male athlete experiencing sudden complaints after strenuous physical exercise. This image is not entirely reflected in this series; gender distribution is nearly 1:1 with 46.2% female patients. Physical activity was reported in our series in 56%. The average age in our series was 32.8 years, but it ranged from 16 to 63 years. Primary care physicians and emergency medical staff therefore need to have a high index of suspicion in any patient with a swollen upper extremity. Besides the aforementioned possible inclusion bias, several methodological shortcomings have to be addressed. Because of the retrospective design of this study, we have no information about the severity of complaints before the initiation of treatment. Furthermore, we do not have data on which ground they were chosen for nonoperative or surgical management. A substantial part of our patients were referred from other hospitals; we do not know exactly why they were referred for further management. Therefore, due to the possibility of unobserved confounders, we have to be cautious not to overvalue our results. Also, data about clot lysis after initial nonoperative treatment with anticoagulation and patency at last follow-up are lacking. A large proportion of our patients were referred from other institutions, and after our management, the follow-up was frequently carried out by the referring hospitals. It is well known that there is a lack of association between venous hemodynamics, venous morphology, and post-thrombotic complaints.7,8 In line with this discrepancy, several authors mention patients with a complete occlusion without any complaints.9–12 Patient-reported outcome measures (PROMs) are therefore the most important modality to evaluate treatment success. Although we do see a correlation between DASH and Villalta scores (Figure 2), we did also see a remarkable incoherency in our series. The nonoperatively treated patient with the worst modified Villalta score (12 points) had a better than average General DASH score (8.3 points) and reported no alterations in his daily activities.
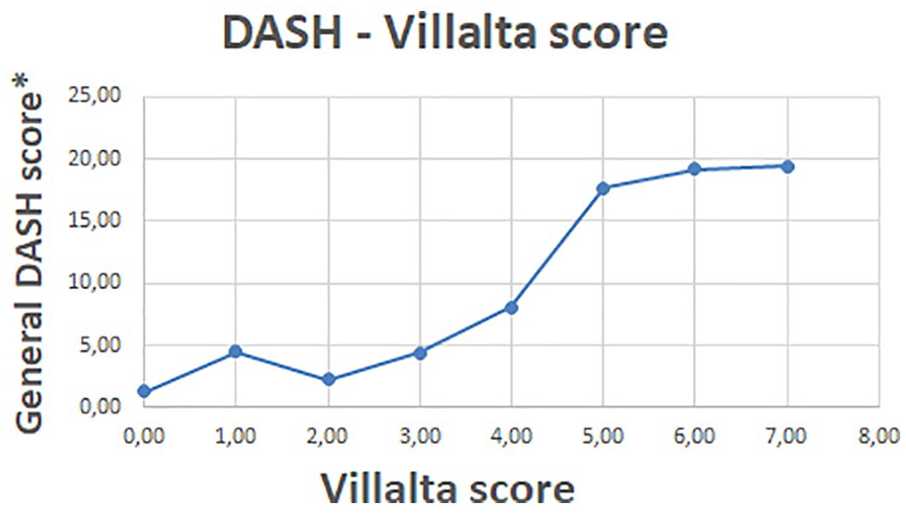
Relation between mean general DASH and Villalta score. DASH, Disability of the Arm, Shoulder, and Hand.
Although we do acknowledge the conceptual superiority of surgical management with immediate recanalization with CDT followed by scheduled FRR, we have to point out that a substantial part of all nonoperatively treated patients are experiencing none to minimal complaints. In our series, 67% of nonoperatively treated patients had a DASH score of ≤10 and can be therefore be in grades from good to excellent. This has to be taken into account when advising patients which management is most appropriate for their specific case. Shared decision-making is essential in the management of PSS.
Conclusion
Surgical management of PSS with immediate CDT followed by FRR leads to excellent functional outcomes with low risk of complications. The results of nonoperative treatment in our non-matched retrospective comparative series were satisfactory, but resulted in worse functional outcome and more patients needing to adjust their lifestyle.
Supplemental Material
sj-docx-1-jet-10.1177_15266028221120360 – Supplemental material for Long-Term Outcomes of Nonoperative and Surgical Management of Paget-Schroetter Syndrome
Supplemental material, sj-docx-1-jet-10.1177_15266028221120360 for Long-Term Outcomes of Nonoperative and Surgical Management of Paget-Schroetter Syndrome by Frank Hoexum, Vincent Jongkind, Hans M. E. Coveliers, Willem Wisselink and Kak Khee Yeung in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028221120360 – Supplemental material for Long-Term Outcomes of Nonoperative and Surgical Management of Paget-Schroetter Syndrome
Supplemental material, sj-docx-2-jet-10.1177_15266028221120360 for Long-Term Outcomes of Nonoperative and Surgical Management of Paget-Schroetter Syndrome by Frank Hoexum, Vincent Jongkind, Hans M. E. Coveliers, Willem Wisselink and Kak Khee Yeung in Journal of Endovascular Therapy
Research Data
sj-docx-3-jet-10.1177_15266028221120360 – Long-Term Outcomes of Nonoperative and Surgical Management of Paget-Schroetter Syndrome
sj-docx-3-jet-10.1177_15266028221120360 for Long-Term Outcomes of Nonoperative and Surgical Management of Paget-Schroetter Syndrome by Frank Hoexum, Vincent Jongkind, Hans M. E. Coveliers, Willem Wisselink and Kak Khee Yeung in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.