
Abstract
Purpose:
The STABILISE technique has extended the treatment of aortic dissection to the thoracoabdominal aorta to achieve complete aortic remodeling. The aim of this multicenter study was to analyze the short- and midterm anatomical results of the STABILISE technique.
Materials and Methods:
We retrospectively analyzed patients treated with the STABILISE technique for complicated aortic dissection at 3 French academic centers. The aortic diameter at different levels was measured preoperatively, postoperatively, and at 1 year.
Results:
Between 2018 and 2020, 58 patients, including 47 men (average patient age: 60±11 years), were treated for type B aortic dissection in 34 cases and residual aortic dissection after type A repair in 24 cases. Three (5.2%) patients died postoperatively. Complete aortic remodeling (false lumen thrombosis and complete reapposition of the intimal flap) was achieved in 45/55 patients (81.8%), and false lumen thrombosis in the thoracic aorta was achieved in 52/55 patients (94.5%). At 1 year, with a computed tomographic (CT) scan available for 98.2% (54/55) of patients, we observed a significant decrease in the maximal thoracic aortic diameter and a significant increase in the aortic diameter at the bare-stent level compared with the preoperative CT scan. Severe aortic angulation (p=0.024) was a risk factor for incomplete aortic remodeling and significantly increased the aortic diameter (p=0.032). Chronic aortic dissection was associated with an increased risk of incomplete aortic remodeling (p=0.002).
Conclusions:
STABILISE for complicated aortic dissection results in false lumen thrombosis, complete reapposition of the intimal flap, and a decrease in the maximum aortic diameter in most cases. Incomplete reapposition of the intimal flap, which is more frequent in cases of chronic aortic dissection and severe aortic angulation, is a risk factor for a significant increase in the aortic diameter at the bare-stent level, and this risk justifies close follow-up and better patient selection.
Clinical impact
STABILISE technique for complicated aortic dissection results in false lumen thrombosis, complete aortic remodeling and a decrease in the maximum aortic diameter in most cases. At the bare-stent level, incomplete reapposition of the intimal flap, more frequent in chronic aortic dissection and severe aortic angulation, is a risk factor for an increased aortic diameter. This finding justifies close follow-up and better patient selection; thus, the STABILISE technique should be used with care in chronic aortic dissection and severe aortic angulation.
Introduction
Aortic dissection (AD) is a life-threatening disease that is very challenging to treat. 1 Thoracic endovascular aortic repair (TEVAR) has emerged as the first-line therapy for the treatment of AD, with better short-term results than open repair due to a significant decrease in perioperative morbidity and mortality.2–5 The long-term results remain controversial, with a high rate of type IB endoleak linked to distal stent-graft–induced new entry tears and a persistent patent false lumen (FL). Moreover, the thoracoabdominal aorta (TAA) cannot be simply treated with a standard stent-graft, with a risk of long-term aneurysm evolution of 20% to 40% and a risk of reintervention near 60%. 6
The stent-assisted balloon-induced intimal disruption and relamination in AD repair (STABILISE) technique offers a preventive treatment for AD in the TAA, with encouraging short-term results having previously been reported for acute, subacute, and chronic AD.7–9 This strategy has the potential to achieve complete repair of the dissected aorta with complete aortic remodeling, including thoracoabdominal FL obliteration and relamination with intimal flap reapposition, as well as improved long-term outcomes, reducing the need for complex reintervention at the distal TAA in the future.
However, this new technique must be evaluated to confirm that the initial good anatomical results are maintained during follow-up without a significant increase in diameter or the need for reintervention.
Finally, improving indications for treatment with the STABILISE technique by identifying risk factors for treatment failure and incomplete aortic remodeling will improve the management and results of the technique.
The aim of this multicenter study was to report the short- and midterm results of the STABILISE technique and to analyze the anatomical results at the stent-graft and bare-stent levels and the risk of treatment failure.
Methods
Population
All patients included in this study were clearly informed about the use of their data for clinical research. In addition, they were aware that their data would be used anonymously for research purposes. The institutional review board approved the project (N°2020-130 on October 14, 2020) and waived the requirement of informed consent for the use of the patient’s medical data for this study.
In this multicenter retrospective cohort study, we included all patients who underwent a STABILISE procedure for complicated AD at 3 French academic hospitals.
The inclusion criteria for the STABILISE procedure were malperfusion syndrome (malperfusion syndrome was defined as hepatic cytolysis, mesenteric angina or ischemia, acute renal insufficiency or lower limb ischemia), uncontrolled pain( refractory pain defined as persistent pain despite morphine and blood pressure controlled [systolic blood pressure <120 mm Hg]), uncontrolled hypertension, rapid aortic growth or aneurysmal evolution (>10 mm/y or an aortic diameter >55 mm), and aortic rupture.
The exclusion criteria were complete FL thrombosis, an abdominal aortic diameter >42 mm (where the bare-stent should be deployed), and/or an inadequate distal landing zone (<42 mm in diameter in a 20-mm-long segment above the celiac trunk for the proximal stent-graft).
We retrospectively collected data regarding the demographic, clinical, and anatomical characteristics of patients treated with the STABILISE technique.
Perioperative Management
All cases were discussed in a multidisciplinary meeting composed of vascular surgeons, cardiac surgeons, interventional radiologists, cardiologists, and anesthesiologists.
Hybrid treatment with TEVAR and open supra-aortic debranching in at least 2 steps remains the first-line therapy at our aortic center when the AD involves the arch, as previously described. 10
In some cases of contraindications to open repair, complete endovascular treatment was performed with fenestrated or branched endoprostheses.
TEVAR
The TEVAR was performed in a multimodal angiographic suite (Discovery IGS 730; GE Healthcare, Chicago, Illinois). Transesophageal ultrasound was systematically used to ensure correct positioning of the guide in the true lumen (TL).
Stent-grafts were advanced and deployed using standard techniques. We used the following 2 stent-grafts: the C-TAG stent-graft (W.L. Gore & Associates, Inc., Flagstaff, Arizona) and the Valiant Navion stent-graft (Medtronic, Santa Rosa, California).
The decision to extend the proximal landing zone was based on the location of the primary entry tear (aortic arch or descending thoracic aorta).
The stent-graft size was determined by measuring the diameter of the proximal and distal landing zones on an orthogonal view of the total aorta using centerline reconstruction on computed tomography (CT). The diameter of the stent-graft was sized based on both the TL and the FL within the descending thoracic aorta. Proximal oversizing of 10% for native aorta and 20% for graft aorta replacement and distal oversizing of 10% were performed.
In elective patients, systematic revascularization of the left subclavian artery was performed to prevent the risk of spinal cord ischemia and cerebrospinal fluid drainage was performed when there was extensive coverage of the thoracic aorta with a stent-graft (>250 mm) in the absence of contraindications.
STABILISE Technique
We deployed bare-stent in the TAA to induce remodeling of the distal dissected aorta according to the STABILISE technique (Supplemental Video), as described by Faure et al.8,9
The distal part of the stent-graft should end up in an area where the diameter does not exceed 42 mm over a length of at least 20 mm. When feasible, proximal stent-graft coverage should usually extend 100 to 150 mm above the celiac trunk to preserve the intercostal arteries.
Distal aortic bare-stent deployment
The Zenith dissection endovascular stent (ZDES; Cook Medical, Bloomington, Indiana) was deployed with a 1-stent body overlap in the stent-graft and extension as far as the infrarenal aorta. The 36-mm-diameter ZDES was used in the case of a maximum external aortic diameter up to 32 mm, and the 46-mm-diameter ZDES was used in the case of a maximum external aortic diameter between 32 and 42 mm.
Management of visceral arteries
In cases of visceral or renal branches arising from the FL or signs of static malperfusion on preoperative CT scans, we catheterized the targeted vessels before inflating the balloon.
Balloon dilatation of the bare-stent
Subsequently, a trilobed balloon catheter (W.L. Gore & Associates, Inc.) was inserted. Between the distal end of the stent-graft and the proximal end of the ZDES, balloon expansion was performed to the point of intimal flap disruption, leading to reapposition of the intimal flap on the aortic wall. On completion of balloon angioplasty, an angiogram was performed to ensure adequate proximal and distal seals of the FL to assess FL obliteration and branch vessel patency in the TAA. In cases of visceral or renal artery malperfusion, a bare-stent can be deployed.
Balloon pressures ranged from 1 to 2 atmospheres with manual inflation to reach the total aortic size (guided by image fusion) and enable intimal disruption without applying pressure to the outer aortic wall. In cases of incomplete flap reapposition, the balloon was not reinflated more than once.
Radiological Analysis
All patients underwent a postoperative CT scan before discharge, at 3 and 6 months postoperatively and annually thereafter. Scan image analysis and measurements were performed by 2 independent vascular surgeons using 3-dimensional (3D) imaging software (OsiriX software, Geneva). Diameter measurements were performed on the perpendicular axis according to the centerline using a semiautomated centerline algorithm preoperatively, postoperatively, and on the last available CT scan during follow-up at the 6 different levels (Figure 1). Angulation was also measured preoperatively on 3D CT reconstructions at the level of the aortic arch and at the level of the thoracoabdominal junction by defining a point upstream and downstream of the angulation in a rectilinear zone and measuring the angle between these 2 points.
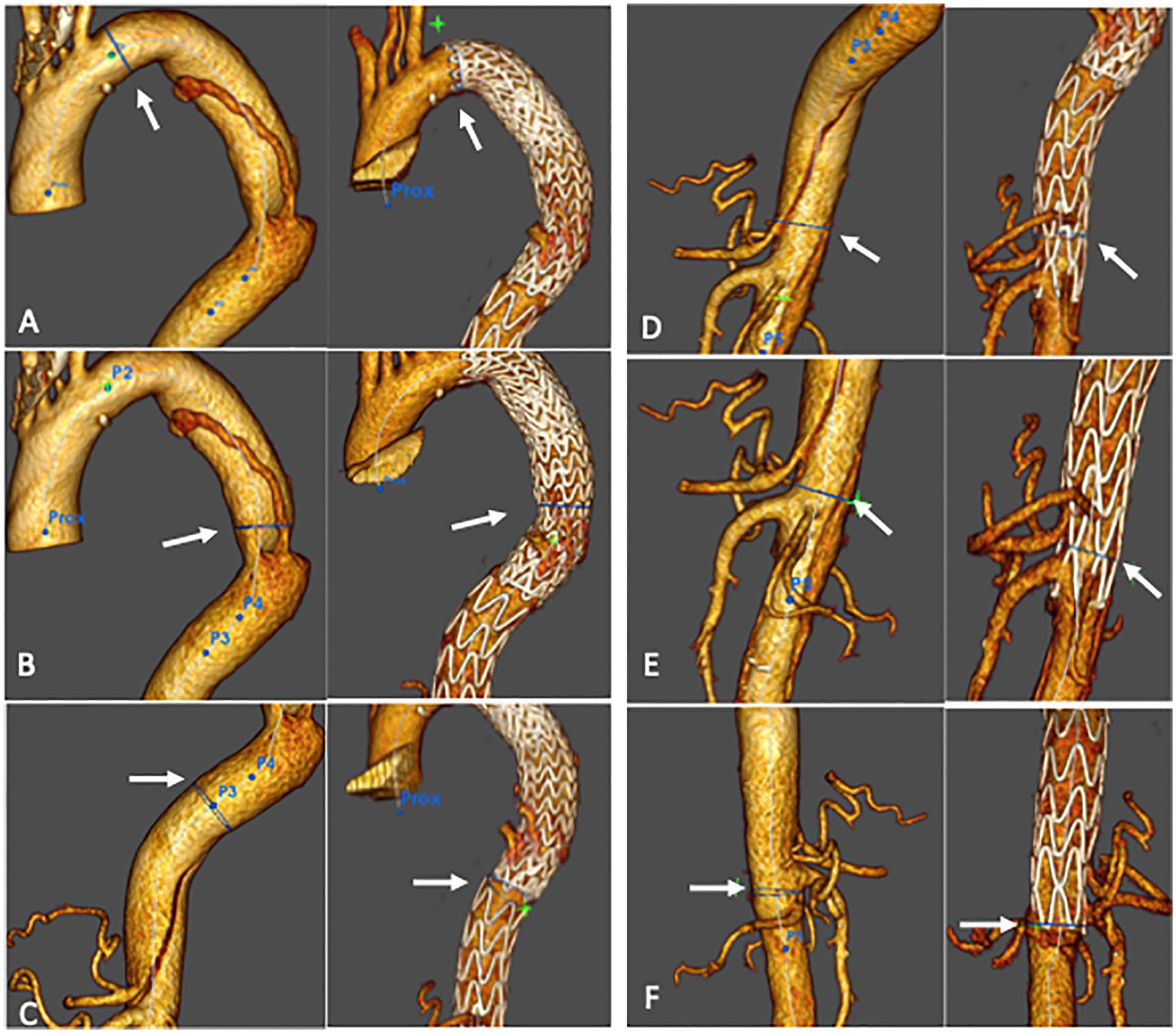
The aortic diameter was measured on computed tomography (CT) preoperatively, postoperatively, and at the last follow-up at the 3 stent-graft level: (A) at the proximal region of the stent-graft; (B) at the descending thoracic aorta (maximum aortic diameter); (C) at the distal part of the stent-graft; and at the 3 bare-stent level: (D) at the ostium of the celiac trunk; (E) at the junction of the last 2 bare-stent segments; and (F) at the terminal part of the bare-stent.
Endpoints
False lumen patency was assessed as FL enhancement anywhere in the downstream aorta on arterial or venous-phase CT. The FL was also considered patent if only partial thrombosis was observed, while disappearance of the FL was considered to indicate complete FL thrombosis.
A significant increase in diameter at the end of follow-up was defined as aortic growth >5 mm.
Complete aortic remodeling was defined as FL thrombosis in the thoracic aorta and complete reapposition of the intimal flap on the aortic wall at the bare-stent level (Figure 2A and B).
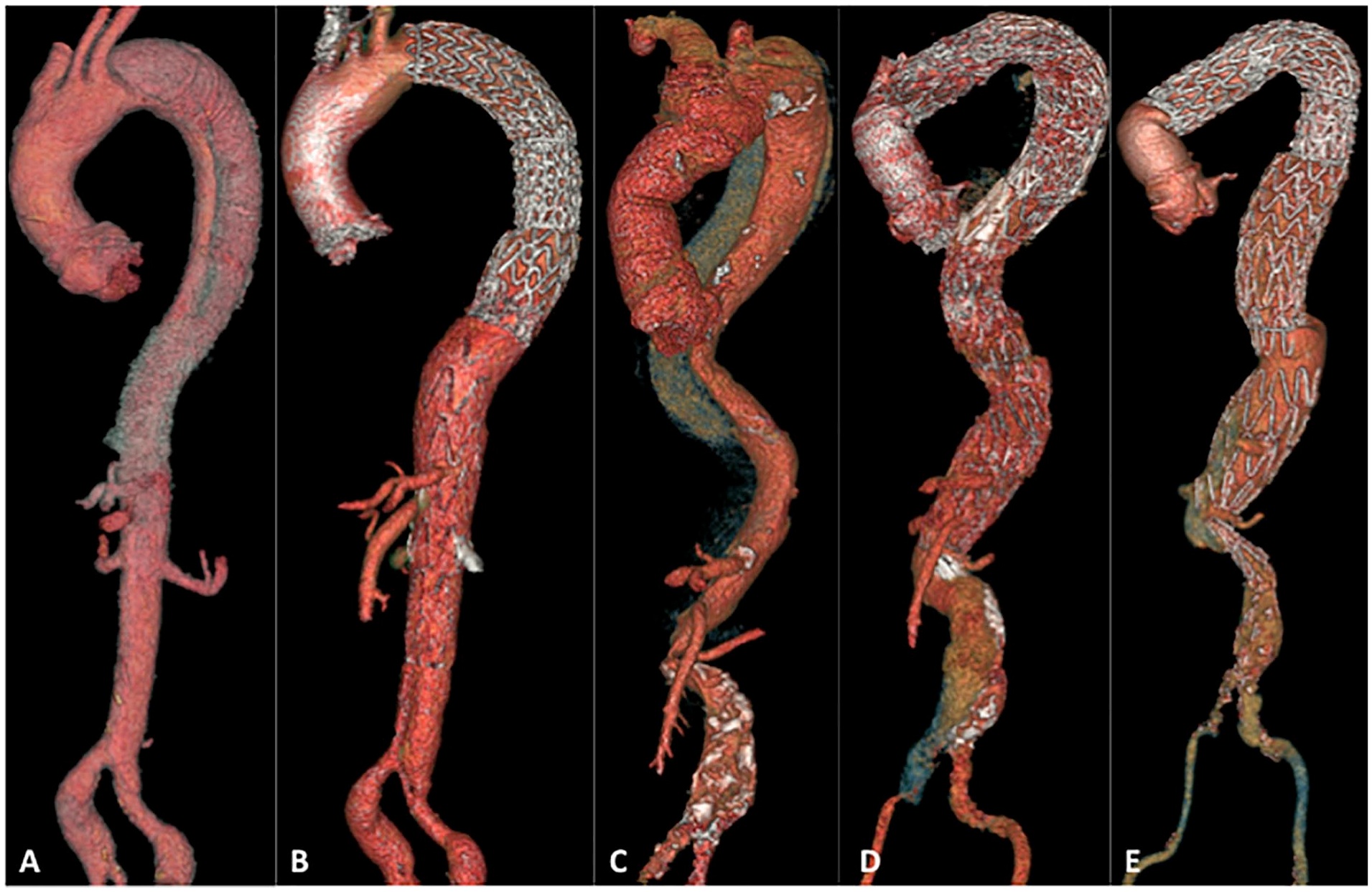
Example of complete aortic remodeling after the stent-assisted balloon-induced intimal disruption and relamination in aortic dissection repair (STABILISE) technique and incomplete aortic remodeling with aneurysm evolution due to significant angulation at the thoracoabdominal junction. (A) Preoperative computed tomographic (CT) scan of a patient treated for subacute type B aortic dissection (AD). The left renal artery arose from the false lumen (FL).(B) Two-year postoperative CT scan of the same patient showing complete remodeling of the thoracoabdominal aorta (TAA) with stent patency in the left renal artery and no aortic aneurysm development. (C) Preoperative CT scan of a patient treated for chronic residual type B AD (hemiarch replacement). Before performing STABILISE-TEVAR, we performed iterative replacement of the ascending aorta + supra-aortic (SA) debranching to create a satisfactory proximal neck. The angle at the level of the thoracoabdominal junction was 95°. (D) Early postoperative CT scan of the same patient showing a stent-graft apposition defect at the level of the distal neck with an FL permeable to the significant angle at the thoracoabdominal junction. (E) CT scan of the same patient at 1.5 years postoperatively showing a permeable FL channel with aneurysm evolution.
Incomplete aortic remodeling in the TAA was defined as incomplete reapposition of the FL without relamination of the intimal flap.
We analyzed risk factors for incomplete aortic remodeling and a significant increase in diameter using demographical data (Table 1), perioperative data (Table 2), and anatomical data obtained from the radiological analysis.
Baseline Characteristics.
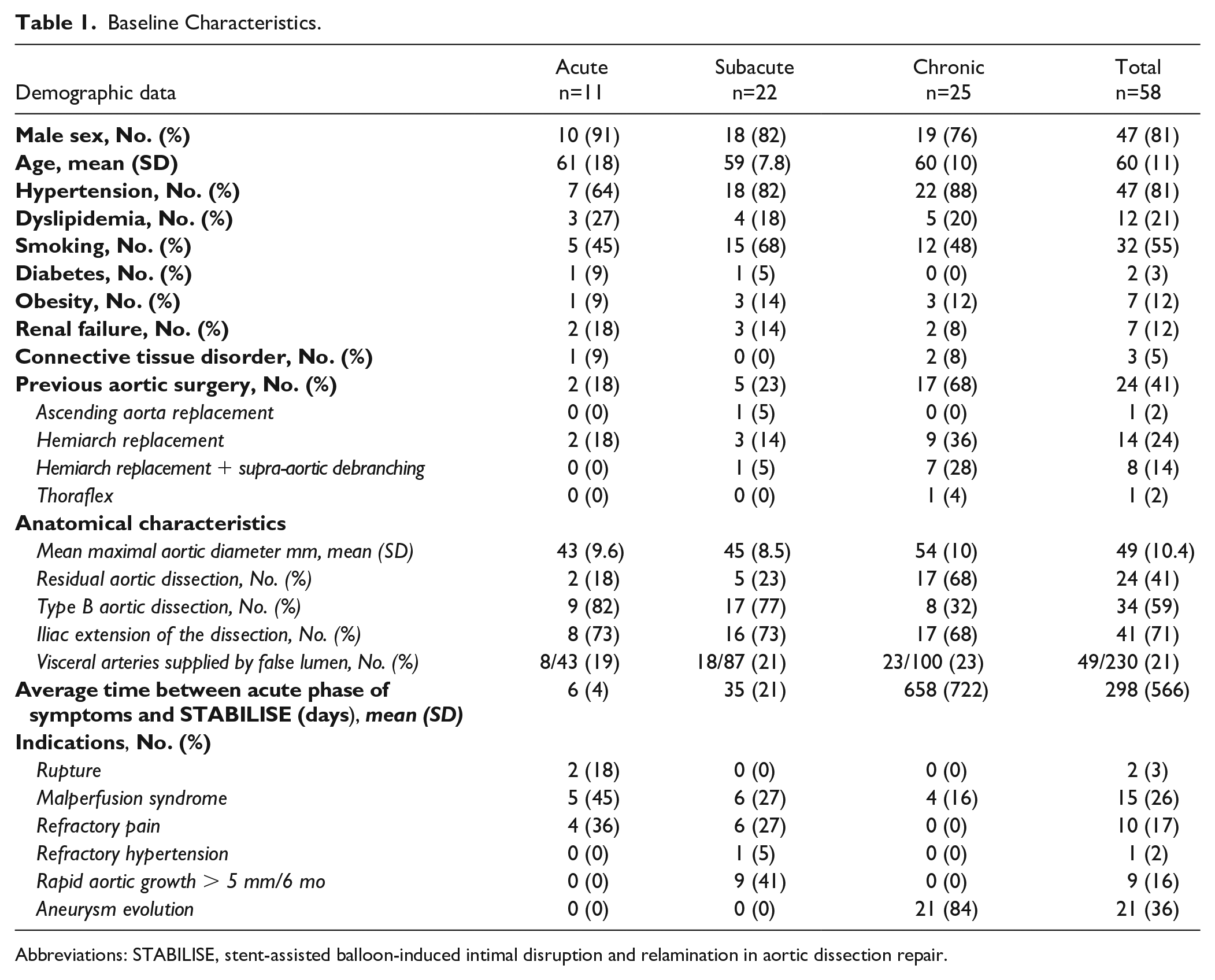
Abbreviations: STABILISE, stent-assisted balloon-induced intimal disruption and relamination in aortic dissection repair.
Procedural Details.
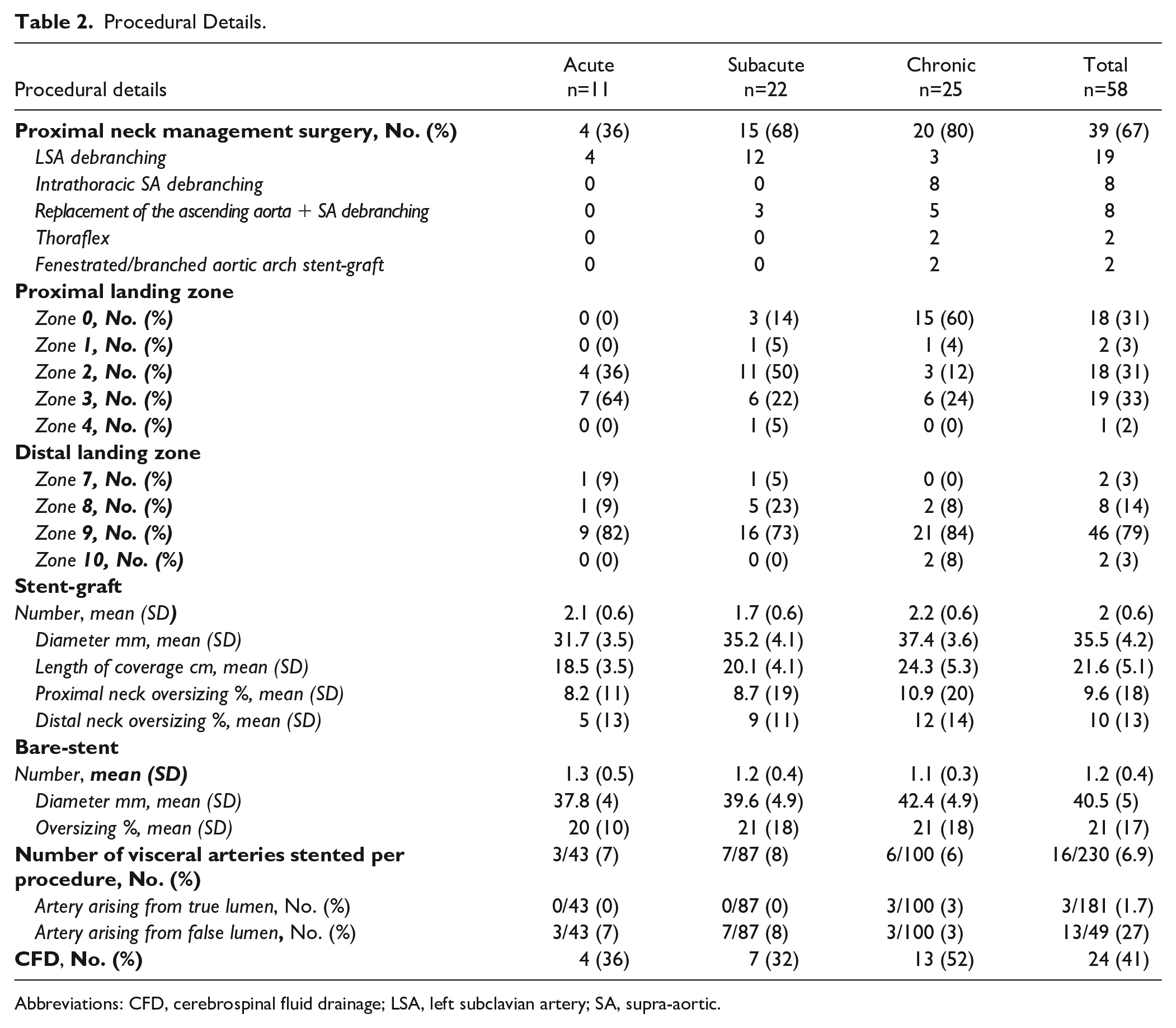
Abbreviations: CFD, cerebrospinal fluid drainage; LSA, left subclavian artery; SA, supra-aortic.
Statistical Analysis
Data are presented as the mean±standard deviation for continuous variables and as counts (%) for categorical data. For categorical variables, the relationship between variables was studied using the chi-square test or Fisher exact test, as appropriate. The Mann-Whitney U test was used for continuous variables. The normality of the distribution of variables was assessed with the Shapiro-Wilk test. Nonparametric Friedman test for paired samples was used to compare changes in diameters at different aortic levels between the preoperative CT scan, the postoperative CT scan, and the 1-year CT scan. The diameters of the thoracic and thoracoabdominal aortas are presented as box-and-whisker dot plots. The upper and lower borders of the box represent the upper and lower quartiles. The middle horizontal line represents the median. The upper and lower whiskers represent the maximum and minimum values of nonoutliers. Extra dots represent outliers. All statistical analyses were performed using IBM SPSS Statistics 20.0 (IBM, Inc., New York).
Results
Population
Between August 2018 and July 2020, 58 patients (33, 12, and 13 patients at the Marseille, Angers, and Tours centers, respectively), including 47 men (average age: 60±11 years), were treated with STABILISE for type B AD (34 cases) and residual AD after type A repair (24 cases).
The median interval between the onset of acute symptoms and the procedure was 298±566 days (0-3110).
Eleven patients were treated during the acute phase (<14 days), 22 during the subacute phase (14-90 days), and 25 during the chronic phase (>90 days). Indications for treatment and demographic data are described in Table 1.
For proximal landing zone management, we performed a hybrid treatment with supra-aortic trunk debranching in 35 cases, open surgery with a thoraflex in 2 cases, and fenestrated or branched aortic arch endoprosthesis in 2 cases (1 branched endoprosthesis for a chronic type B AD treated for aneurysmal evolution and 1 homemade in situ laser fenestration for a chronic residual AD treated for pain and rapid aortic growth). In other cases, TEVAR alone was performed.
Perioperative Results
Procedural details are presented in Table 2.
Three patients (5.2%) died postoperatively. All deaths occurred in patients who underwent emergency treatment for complicated acute AD (2 cases of aortic rupture and 1 case of malperfusion syndrome).
In 1 case of aortic rupture in acute type B AD without perioperative complications, the patient died on the 13th postoperative day (sudden death of unknown cause).
In 1 case of aortic rupture in acute type A AD treated with hemiarch replacement, supra-aortic debranching, and TEVAR-STABILISE, the patient died at the time of balloon inflation of aortic rupture.
In 1 case of malperfusion syndrome (cerebral and mesenteric malperfusion) in acute type A AD treated with hemiarch replacement, supra-aortic debranching, and TEVAR-STABILISE, the patient died on day 3 secondary to pulmonary sepsis with multiple-organ failure.
We observed 2 postoperative strokes (3.4%):
One ischemic stroke with hemorrhagic transformation in a patient treated emergently for type A AD and malperfusion syndrome by ascending aortic replacement and TEVAR STABILISE with subsequent hemiparesis.
One minor ischemic stroke (probably due to navigation) in a patient treated in the subacute phase of a residual dissection with complete recovery.
In 1 case of postoperative spinal cord ischemia (1.7%) (acute type B AD with malperfusion syndrome), the patient was treated emergently with extensive coverage of the thoracic aorta but no left subclavian artery revascularization. Complete recovery was achieved using cerebrospinal fluid drainage.
In 2 patients (3.4%), perioperative acute superior mesenteric artery (SMA) dissection occurred after balloon inflation; in 1 patient, treatment was performed with a proximal stent in the SMA, and in the other patient, with distal dissection, medical treatment was performed with curative anticoagulation.
Five patients presented renal infarct (8.6%) on preoperative CT, with a postoperative increase in the creatinine level in all patients; complete regression occurred in 4 patients, and none of the patients required dialysis. There were no renal complications related to the STABILISE procedure.
We performed early reintervention in 8 cases (Supplemental Table 1) and late reintervention in 5 cases (Supplemental Table 2).
Postoperative Anatomical Results
Complete aortic remodeling (FL thrombosis and complete reapposition of the intimal flap) was achieved in 45/55 patients (81.8%), and FL thrombosis in the thoracic aorta was obtained in 52/55 patients (94.5%) (Figure 2A and B; Table 3).
Anatomical Results.
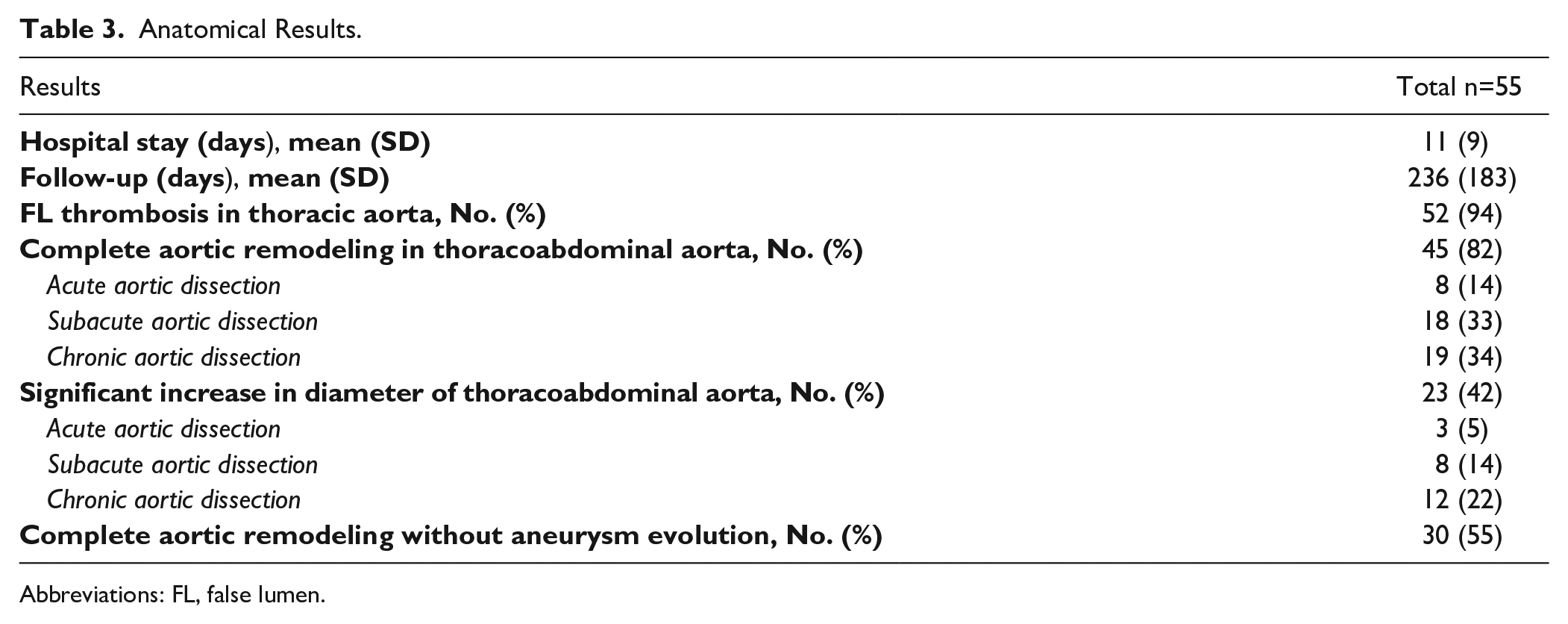
Abbreviations: FL, false lumen.
In 1 case of type IA endoleak, the patient was treated emergently after type A repair for malperfusion syndrome without coverage of the main entry tear at the distal anastomosis of the previous ascending aorta replacement.
There were 2 cases of type II endoleak from the intercostal arteries and 10 cases of incomplete reapposition of the intimal flap with a remaining short segment of patent FL at the bare-stent level.
The maximal thoracic aortic diameter was stable on the postoperative CT scans.
There was a significant increase in the aortic diameter on CT preoperatively to postoperatively at the bare-stent levels (see Figure 1): 31.7±4.4 mm to 32.8±4.4 mm (p<0.01).
One-Year Results
At 1 year, with late CT scans available for 98.2% (54/55) of patients, the results are as in Table 4.
Diameter Evolution.
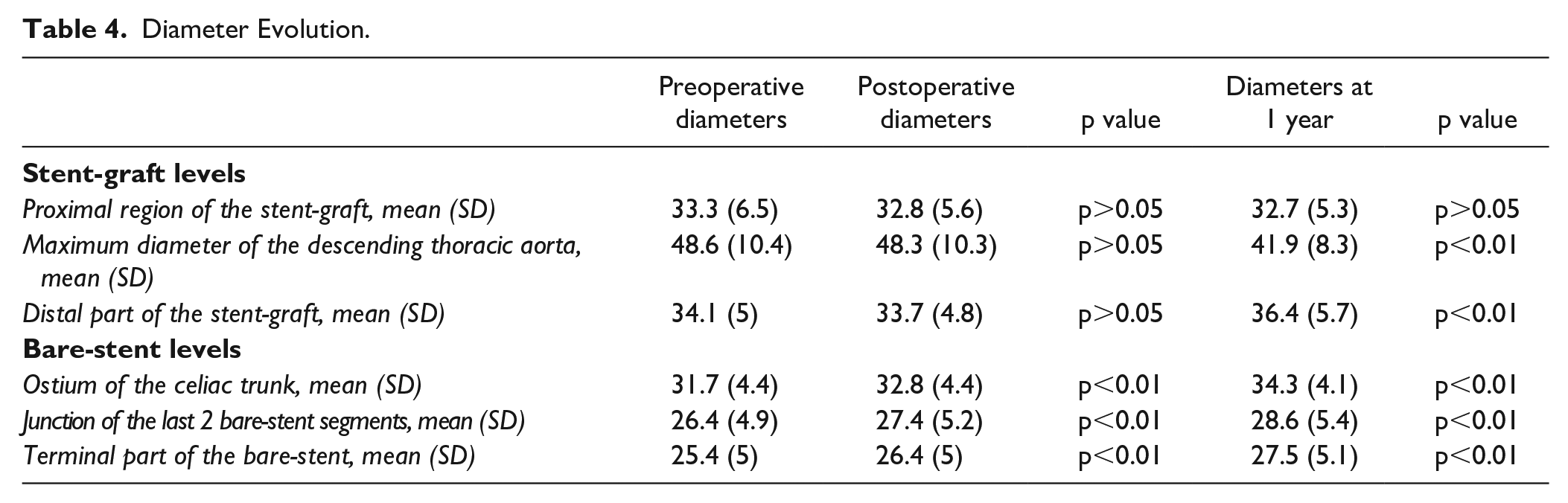
We observed a significant decrease in the maximal thoracic aortic diameter at the stent-graft level (48.6±10.4 mm to 41.9±8.3 mm; p<0.01). Regression of the aortic diameter was present in 49% (27/55) of patients, and stabilization was present in 51% (28/55) of patients.
There was a significant increase in diameter at the bare-stent level (31.7±4.4 mm to 34.3±4.1 mm; p<0.01). We observed a significant increase in the aortic diameter in 41.8% (23/55) of patients and stabilization in 58.2% (32/55) of patients.
Anatomical Results According to the Time of Treatment (Acute Subacute and Chronic Phase)
A decrease in the maximal aortic diameter was observed for each group of patients treated, which was significant at the chronic phase (Figure 3A).
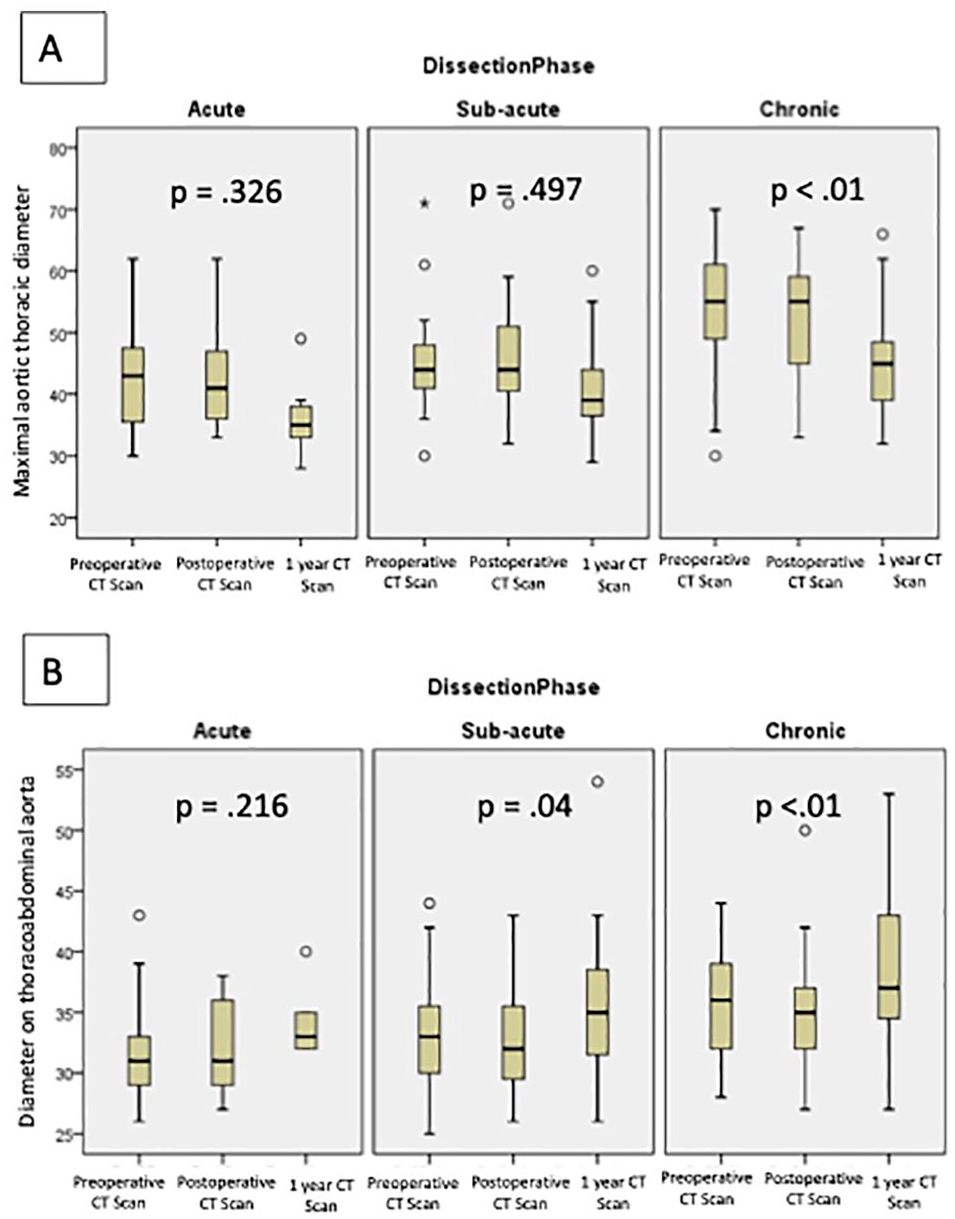
Evolution of the diameter of the thoracic aorta and thoracoabdominal aorta (TAA).
An increase in the diameter of the TAA at the bare-stent level was observed for each group; it was significant at the subacute (p=0.04) and chronic phases (p<0.01) (Figure 3B).
Risk Factors for Significant Aortic Diameter Increase and Incomplete Aortic Remodeling at the Bare-Stent Level
Incomplete aortic remodeling at the bare-stent level was significantly associated with a risk of increased diameter at 1 year (+5.8 mm vs +1.4 mm, p<0.01).
Severe aortic angulation at the bare-stent level was significantly associated with an increased risk of incomplete aortic remodeling (112° vs 60°, p=0.024) and a significant increase in diameter (95° vs 57°, p=0.032) (Figure 2C–E).
Compared with type B AD, residual AD (after type A repair) was significantly associated with an increased risk of incomplete aortic remodeling—36% (8/22) vs 3% (1/33), p=0.002. There were significantly more cases of chronic AD in the residual AD group than in the type B AD group—70.8% (17/24) vs 23.5% (8/34), p<0.001.
Chronic AD was associated with an increased risk of incomplete aortic remodeling (28% vs 10%, p=0.08).
Discussion
Herein, we report the short- and midterm results of the STABILISE technique in 58 patients with type B AD. This is the first multicenter study on this technique in such a population.
In the present study, the STABILISE technique provided excellent short- and midterm anatomical results, with complete aortic remodeling in 82% of patients, FL thrombosis in 94.5% of patients, and a decrease or stabilization of the thoracic aortic diameter. Similarly, Faure et al reported 100% FL thrombosis at the stent-graft level and 100% complete aortic remodeling in acute dissection, whereas TEVAR alone fails to prevent aneurysm development at the level of the thoracic aorta in most cases, with complete FL thrombosis achieved in only 10% to 30% of cases.11–16
The STABLE technique (proximal stent-grafting with distal bare-stenting) yields better results than TEVAR alone,17–19 with re-expansion of the TL and reduction of the FL.20,21 However, complete FL thrombosis in the thoracic aorta is achieved in only 30% to 60% of cases,20,21 and Sobocinski et al 22 observed a significant increase in the volume of the abdominal aorta at 12 months.
Despite the good initial anatomical results of the STABILISE technique, the incidence of a significant increase in diameter on CT scan at the bare-stent level was 41.8% at 1 year. This finding suggests that such increases in diameter are linked to the operating technique (the self-expanding stent continued to conform to the arterial wall, becoming fragile due to forced aortic remodeling) and to the natural evolution of AD. Indeed, more than 60% of patients with AD, regardless of the initial treatment modality, develop aneurysm growth in the 5 years following the procedure. 23
All patients were treated for complicated AD, more often aneurysmal evolution (52% of cases), which is a well-known complication of type B and residual AD, in approximately 50% of cases.
The inclusion of all patients with complicated AD treated with the STABILISE technique at 3 academic French centers allows for the analysis of prognostic criteria, and for the first time, we identified risk factors for failure of the STABILISE technique and an increase in the aortic diameter at the bare-stent level. Incomplete reapposition and chronic AD of the intimal flap at the bare-stent level were significantly associated with a risk of a significant increase in diameter. We found that residual AD was significantly associated with this risk of negative results and was directly linked to the large number of chronic AD cases in this group (70.8% vs 23.5%, p<0.01). During the chronic phase, the intimal flap is stiffer, and disruption by balloon inflation is more difficult, which could explain the better results observed in acute and subacute AD. In the literature, the results of the STABILISE technique for chronic AD are reportedly worse than those for acute and subacute AD.24,25 Hofferberth et al 26 reported the first series, with only 1 case of failure in the TAA in a patient treated for chronic AD. Faure et al reported 100% FL thrombosis at the level of the stent-graft in 17 chronic type B AD patients but only 88% at the bare-stent level, 9 whereas in their experience with 41 acute type B AD patients, complete aortic remodeling was obtained in all patients at the thoracoabdominal level. 7
In addition, we observed that aortic angulation (>90°) at the bare-stent level was a significant risk factor for incomplete aortic remodeling and a significant increase in diameter during follow-up. This could be due to incomplete reapposition of the intimal flap in the aortic angulation leading to a large new entry tear, which is a well-known risk factor for aneurysm evolution. 27 Moreover, aortic angulation is at risk of disconnection between the stent-graft and bare-stent when the overlap is in this zone.
The bare-stent used here had a low radial force, and we believe that a large diameter yields improved results by increasing the effect of the stent on the aortic wall and promoting complete reapposition of the intimal flap.
In cases involving a high risk of incomplete aortic remodeling, alternatives should be considered: candy plugs, the knickerbocker technique or direct FL occlusion by coil, plug, or glue embolization.28–31
Regarding the short-term results, the 30-day mortality rate in this study was 5.2%, but all deaths occurred in patients treated during the acute (n=2) or subacute (n=1) phase for complicated AD. One patient died because of balloon inflation, and we think it is better to avoid the STABILISE technique at the acute phase, in agreement with other previous studies, as the 30-day mortality also increased among patients treated at the acute phase.2–4 Moreover, it is essential to perform the procedure in a multimodal angiographic suite with image fusion guidance to obtain the targeted aortic size with balloon inflation.
Spinal cord ischemia seems to be the most frequent complication, occurring at a rate of 0-10%, and it is regressive in most cases.7,24,25 In our study, we observed only 1 case of spinal cord ischemia, and we believe that limiting the coverage of the thoracic aorta and performing cerebrospinal fluid drainage in cases of extensive coverage and systematic left subclavian artery revascularization in elective patients would prevent this complication.
Limitations
This study has several limitations, including its observational design and lack of a comparative group, small number of patients, lack of long-term follow-up, and heterogeneity among the included patients. The multicentric nature of this study introduces heterogeneity bias but makes it possible not only to confirm that the technique is safe and reproducible but also to identify prognostic criteria according to the type of pathology and timing. Moreover, to overcome this bias, we separated the anatomical results into 3 groups: acute, subacute, and chronic AD.
Studies comparing the STABILISE technique with TEVAR alone in AD are also needed to confirm that immediate aortic remodeling reduces long-term aneurysm development.
Prospective follow-up of patients included in this study is necessary to confirm the good results of the STABILISE technique in the long term.
Conclusion
STABILISE for AD results in FL thrombosis, complete reapposition of the intimal flap, and a decrease in the maximum aortic diameter in most cases.
Incomplete reapposition of the intimal flap, which is more frequent in cases of chronic AD and severe aortic angulation, is a risk factor for a significant increase in the aortic diameter at the bare-stent level, and this risk justifies close follow-up and better patient selection.
Supplemental Material
sj-docx-1-jet-10.1177_15266028221111984 – Supplemental material for Risk Factors for Incomplete Aortic Remodeling With Stent-Assisted Balloon-Induced Intimal Disruption and Relamination in Aortic Dissection Repair for Complicated Aortic Dissection: Results of a Multicenter Study
Supplemental material, sj-docx-1-jet-10.1177_15266028221111984 for Risk Factors for Incomplete Aortic Remodeling With Stent-Assisted Balloon-Induced Intimal Disruption and Relamination in Aortic Dissection Repair for Complicated Aortic Dissection: Results of a Multicenter Study by Fabien Vecchini, Gautier Haupert, Anna Baudry, Julien Mancini, Lucie Dumur, Robert Martinez, Philippe Piquet, Jean Picquet and Marine Gaudry in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028221111984 – Supplemental material for Risk Factors for Incomplete Aortic Remodeling With Stent-Assisted Balloon-Induced Intimal Disruption and Relamination in Aortic Dissection Repair for Complicated Aortic Dissection: Results of a Multicenter Study
Supplemental material, sj-docx-2-jet-10.1177_15266028221111984 for Risk Factors for Incomplete Aortic Remodeling With Stent-Assisted Balloon-Induced Intimal Disruption and Relamination in Aortic Dissection Repair for Complicated Aortic Dissection: Results of a Multicenter Study by Fabien Vecchini, Gautier Haupert, Anna Baudry, Julien Mancini, Lucie Dumur, Robert Martinez, Philippe Piquet, Jean Picquet and Marine Gaudry in Journal of Endovascular Therapy
Footnotes
Authors’ Note
All patients included in this study were clearly informed of the use of their data for clinical research, but we did not obtain written consent, since the institutional review board did not require it.
IRB approval number: 2020-130 on October 14, 2020
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.