
Abstract
Objectives:
This study evaluated the feasibility and safety of zone 1 thoracic endovascular aortic repair (TEVAR) with fenestrated surgeon-modified stent-graft (SMSG) for aortic arch pathologies.
Methods:
Between March 2016 and November 2020, 34 consecutive patients underwent zone 1 TEVAR with fenestrated SMSG for aortic arch pathologies. Outcomes included technical success, perioperative, and follow-up morbidity and mortality.
Results:
During the study period, 34 patients were treated with zone 1 TEVAR with fenestrated SMSG. Twenty-four (70.6%) patients presented with type B aortic dissections, 9 (26.5%) patients presented with aneurysms (7 located on the lesser curvature side of aortic arch), 1 (2.9%) patient presented with type Ia endoleak after previous TEVAR owing to traumatic aortic dissection. The proximal landing zone for all patients were in zone 1, and all supra-aortic trunks were reconstructed, except for one left subclavian artery. Technical success was achieved in all cases. The 30-day estimated survival (±SE) was 90.9% ± 5.0% [95% confidence interval (CI): 77.0%–97.0%]. The 30-day estimated freedom from reintervention (±SE) was 87.9% ± 5.7% (95% CI: 73.4%–95.3%). At a median follow-up of 48 months (range, 12–68 months), 2 patients died, including 1 aortic-related death and 1 non-aortic-related death. One patient had reintervention 13 months after the operation owing to type Ia endoleak. All supra-aortic trunks were patent. The estimated survival (±SE) during follow-up was 85.1% ± 6.2% (95% CI: 69.9%–93.6%). One (2.7%) patient had stroke. The estimated freedom from reintervention (±SE) during follow-up was 84.2% ± 6.5% (95% CI: 69.9%–93.5%).
Conclusions:
Zone 1 TEVAR with fenestrated SMSG is an alternate option for treatment of aortic arch pathologies in experienced centers.
Keywords
Introduction
The development of endovascular techniques and devices has extended the use of thoracic endovascular aortic repair (TEVAR) to treatment of aortic arch pathologies. With specially designed delivery systems, preloaded fenestrations, and inner branches, results of TEVAR have been significantly improved, and now has become a viable option for aortic arch pathologies, offering another treatment for high-risk patients who historically could not have gone open surgery. 1
Hybrid procedure with debranching of supra-aortic vessel is an alternative for open surgery, which creates an adequate proximal landing zone for endovascular exclusion of the pathology. Debranching can be performed with various approaches, while all requiring clamping of supra-aortic trunks and sometimes in a staged approach, which raise the concern of stroke. 2 Custom-made branched or fenestrated stent-graft has been widely used for aortic arch pathologies (no off-the-shelf products currently available).3–5 Custom-made stent-grafts allow personalized treatment for patients with different arch types and various aortic arch anatomy. The essence that custom-made stent-grafts require 1 to 3 months to design and manufacture holds back its application in emergency and increases the costs. Parallel graft, including chimney graft, the periscope, and sandwich technique, is another option. 6 The advantages of parallel graft included available off-the-shelf products and lower cost compared with custom-made stent-grafts. The major concern of parallel graft is a confirmed higher risk of type I endoleak owing to the inevitable gutter.
A further alternative is fenestrated surgeon-modified stent-grafts (SMSGs) for aortic arch pathologies. Fenestrated SMSGs allow personalized treatment with off-the-shelf products. The objective of the study is to report outcomes of zone 1 TEVAR with fenestrated SMSGs to revascularize left common carotid artery (LCCA) and left subclavian artery (LSA).
Materials and Methods
Population
A single-arm, retrospective review was conducted for 34 consecutive patients with aortic arch pathologies who underwent TEVAR with fenestrated SMSGs to revascularize LCCA and LSA. Informed consents were obtained from all patients before operations. Protocol and informed consent were approved by the institutional review board. Indications for TEVAR with fenestrated SMSGs were (1) zone 2 or zone 3 aortic arch pathologies, including aortic dissection and aneurysm and (2) zone 1 aortic arch pathologies, and the distance between pathologies and distal edge of ostium of innominate artery (IA) was more than 20 mm. Exclusion criteria were (1) zone 0 aortic arch pathologies; (2) zone 1 aortic arch pathologies, and the distance between pathologies and distal edge of ostium of IA was less than 20 mm. Preoperative high-resolution computed tomography angiography (CTA) of each patient was acquired to assess anatomical features. Demographic, anatomic, intraoperative, and postoperative data were extracted from a routinely updated database.
Preoperative Planning and Design
In our center, vascular imaging workstation Aquarius (TeraRecon, Foster City San Mateo, CA, USA) with center-line luminal reconstruction was used for CTA evaluation and 3-dimensional reconstruction. Diameter of the aorta at proximal and distal landing zone, diameter and clock position of ostia of LCCA and LSA, and diameter of LCCA and LSA were measured under center-line luminal reconstruction. The distance between LCCA and LSA was measured under the greater curvature line. The oversizing rate for aortic dissection was 0% to 5%, and 15% to 20% for other pathologies. Three different strategies were applied to revascularize LCCA and LSA: if the pathology is aortic arch aneurysm or aortic dissection on the greater curvature side, 2 small fenestrations for LCCA and LSA, respectively would be used; if the pathology is located on the lesser curvature side, one large fenestration for LCCA and LSA would be used; and if LSA was involved in the pathology, a small fenestration combined with bypass surgery would be used. Stent strut within a small fenestration should be avoided in case of implantation of bridging stent-graft.
Procedural Details
Details about the endovascular procedure, especially how to align fenestrations with target arteries accurately, has been described previously. 7 In brief, all operations were performed under general anesthesia in a hybrid operating room. Valiant Captivia (Medtronic, Minneapolis, MN, USA) devices were used for modification in all cases. The modification was performed on a sterile operating table. After the stent-graft partially unsheathed, the operator created the fenestration in the designated position (in the same direction of the white point in the front grip when fenestrations were in 12’o clock) with a scalpel (electrotome available), then the fenestrated SMSGs would be resheathed. Access points were common femoral artery for the fenestrated SMSG, left brachial artery and left external carotid artery for the bridging stent-graft. Systemic heparin 100 units/kg was administered after access was obtained [target activated clotting time (ACT) > 250 seconds]. A large sheath (mostly 24 French) was introduced retrogradely through common femoral artery. In cases where bridging stent-grafts were implanted into LCCA and LSA, a sheath was introduced retrogradely through left brachial artery into the ostium of LSA, and a sheath was introduced retrogradely through left external carotid artery into the ostium of LCCA. After ascertaining that the white point in the front grip was pointing to the ground, the fenestrated SMSG was advanced over the Lunderquist wire. The systolic blood pressure was lowered to approximately 100 mmHg, and the fenestrated SMSG was deployed under visualization. Rapid pacing was not used. An angiography would be performed to confirm that fenestrations were aligned with target arteries, and all supra-aortic trunks patent. Bridging stent-grafts [Fluency (CR Bard, Murray Hill, NJ, USA; n = 12, all for LSA), Viabahn (WL Gore, Flagstaff, AZ, USA; n = 1, LCCA), and E-luminexx(CR Bard, Murray Hill, NJ, USA; n = 5, all for LCCA)] were advanced through left brachial artery or left external carotid artery into fenestrations, approximately 15 mm protruding into lumen of SMSGs, with the remaining in the LCCA and LSA. Completion angiography was performed to verify the position of fenestrated SMSGs and patency of all supra-aortic trunks.
Follow-up
Follow-up surveillance was performed with serial CTA in the first week, then 3, 6, and 12 months, and annually thereafter. Mortality and adverse events occurred within 30 days after the operation or during hospitalization were reported in 30-day outcomes. Technical success was defined as successful alignment of all fenestrations with target arteries, patent supra-aortic trunks, and complete exclusion of pathologies without type I or III endoleak. Chronicity of aortic dissection is in accordance with latest reporting standards published by Society for Vascular Surgery. 8
Statistical Analysis
Categorical data are reported as the absolute number and percentage; continuous data are reported as the mean ± standard deviation; nonparametric data (eg, follow-up time) are given as median and range. Statistical analysis was performed with SPSS software (26.0 v; SPSS, Inc.). The Kaplan–Meier analysis was used for follow-up data.
Results
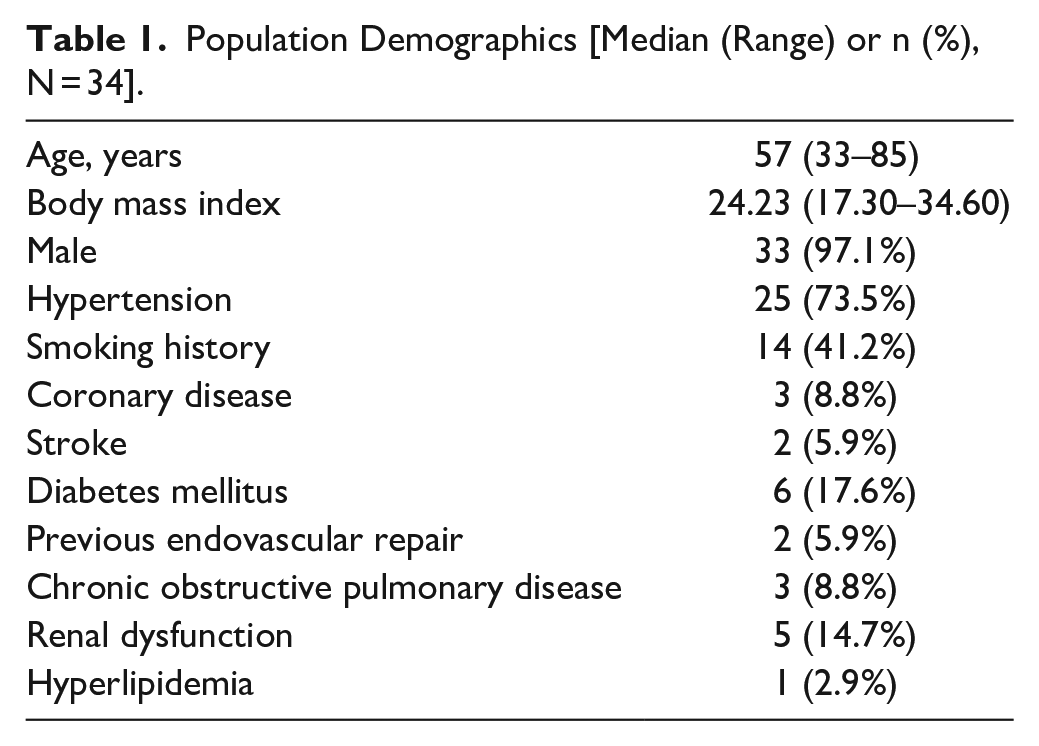
Between March 2016 and November 2020, 34 consecutive patients met the inclusion criteria and underwent zone 1 TEVAR with fenestrated SMSGs. Median age was 57 (range, 33–85). Median BMI was 24.23 (range, 17.30–34.60). Details about baseline characteristic and comorbidities are listed in Table 1.
Population Demographics [Median (Range) or n (%), N = 34].
In this study, 24 (70.6%) patients presented with type B aortic dissections, 9 (26.5%) patients presented with aneurysms (7 located on the lesser curvature side of aortic arch), and 1 (2.9%) patient presented with type Ia endoleak after previous TEVAR owing to traumatic aortic dissection. For aortic dissections, 15 cases were treated in acute phase (1–14 days), 4 cases were treated in subacute phase (15–90 days), and 5 cases were treated in chronic phase (>90 days). Disease details were listed in Supplemental Table 1.
In total, 68 arteries were revascularized successfully, including 34 LCCA, 30 LSA, 1 aberrant left vertebral artery revascularized with fenestrations, 2 LSA revascularized with chimney, and 1 LSA revascularized with LCCA-LSA bypass in the same stage. In a case with type B aortic dissection, LSA was involved in the dissection and was embolized with coil. An average of 1.56 stent-grafts was deployed. The median duration to modify the stent-graft was 18 minutes (range, 15–23 minutes). Technical success was achieved in all cases (Figure 1).
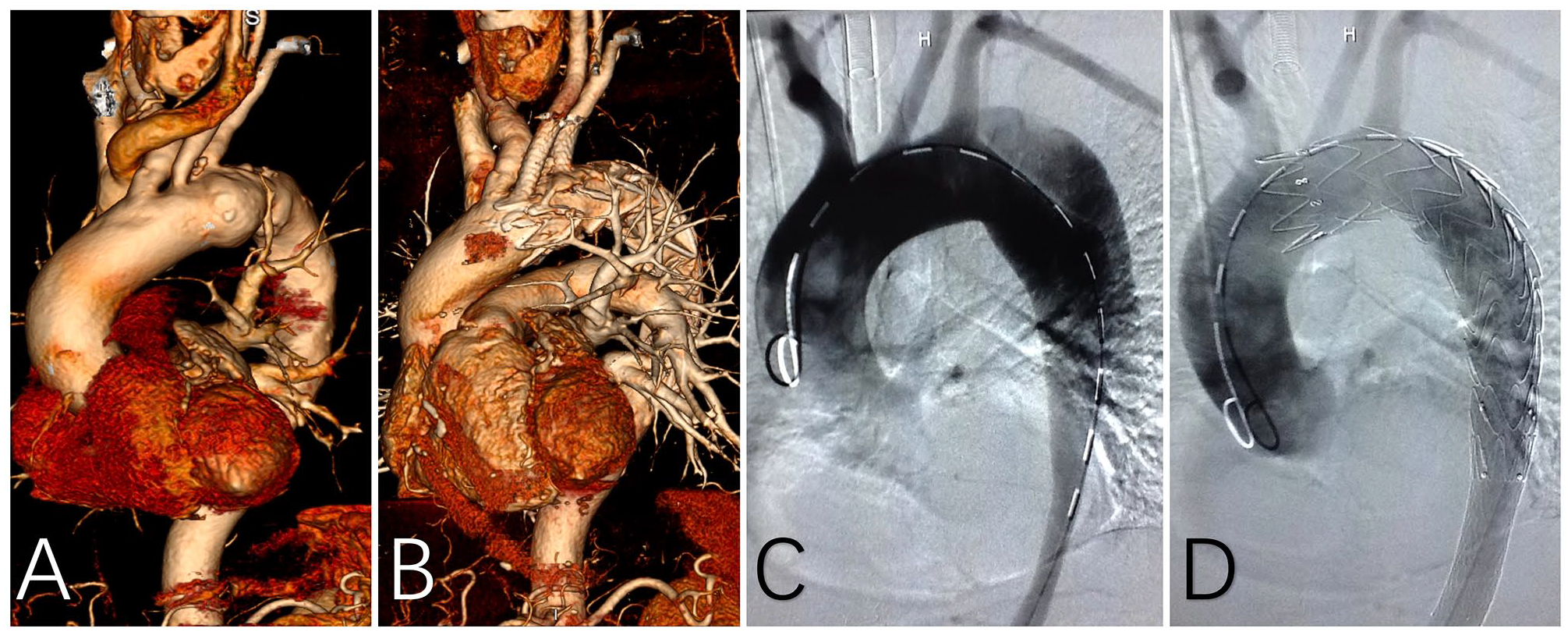
TEVAR with fenestrated SMSG. (A) Preoperative 3-dimensional CTA reconstruction for a patient with aneurysm. (B) Three-dimensional CTA reconstruction for a patient with aneurysm 1 year after the operation. (C) Digital subtraction angiography (DSA) for a patient with aortic dissection. (D) Complete angiography for a patient with aortic dissection.
Thirty-Day Outcomes
The average diameter and length of fenestrated SMSG was 199.41 ± 2.38 mm and 32.97 ± 3.45 mm, respectively. The median duration of the operation was 94 minutes (range, 81–176 minutes). The median duration of hospitalization was 10 days (range, 4–28 days), and the median duration of ICU stay was 1 day (range, 0–12 days). The estimated survival (±SE) was 90.9% ± 5.0% [95% confidence interval (CI): 77.0%–97.0%]. The mortality rate was 8.8% (n = 3). One patient died of retrograde type A aortic dissection (RTAD) 1 week after the operation despite another open surgery was performed. The new entry tear was in the proximal bare stent at the lesser curvature side with ostium of right coronary artery proximally involved. One patient died of severe pulmonary infection and multiorgan failure during hospitalization. The other patient had bloody pleural effusion after the operation, and the condition kept getting worse and finally died of multiorgan failure. The estimated freedom from reintervention (±SE) was 87.9% ± 5.7% (95% CI: 73.4%–95.3%). The rate of reintervention was 11.8% (n = 4), including one described in the mortality. Two patients accepted reintervention because of RTAD, both had the new entry tear located in the proximal bare stent at the greater curvature side with IA involved in the dissection. Aortic root reconstruction, transposition of ascending aorta, and aortic arch and stent-graft implantation for descending aorta were performed. The other patient had reintervention because of severe aortic insufficiency and ascending aortic aneurysm. Bentall procedure, transposition of aortic arch, and frozen elephant trunk implantation were performed. All supra-aortic trunks were patent (Figure 2).
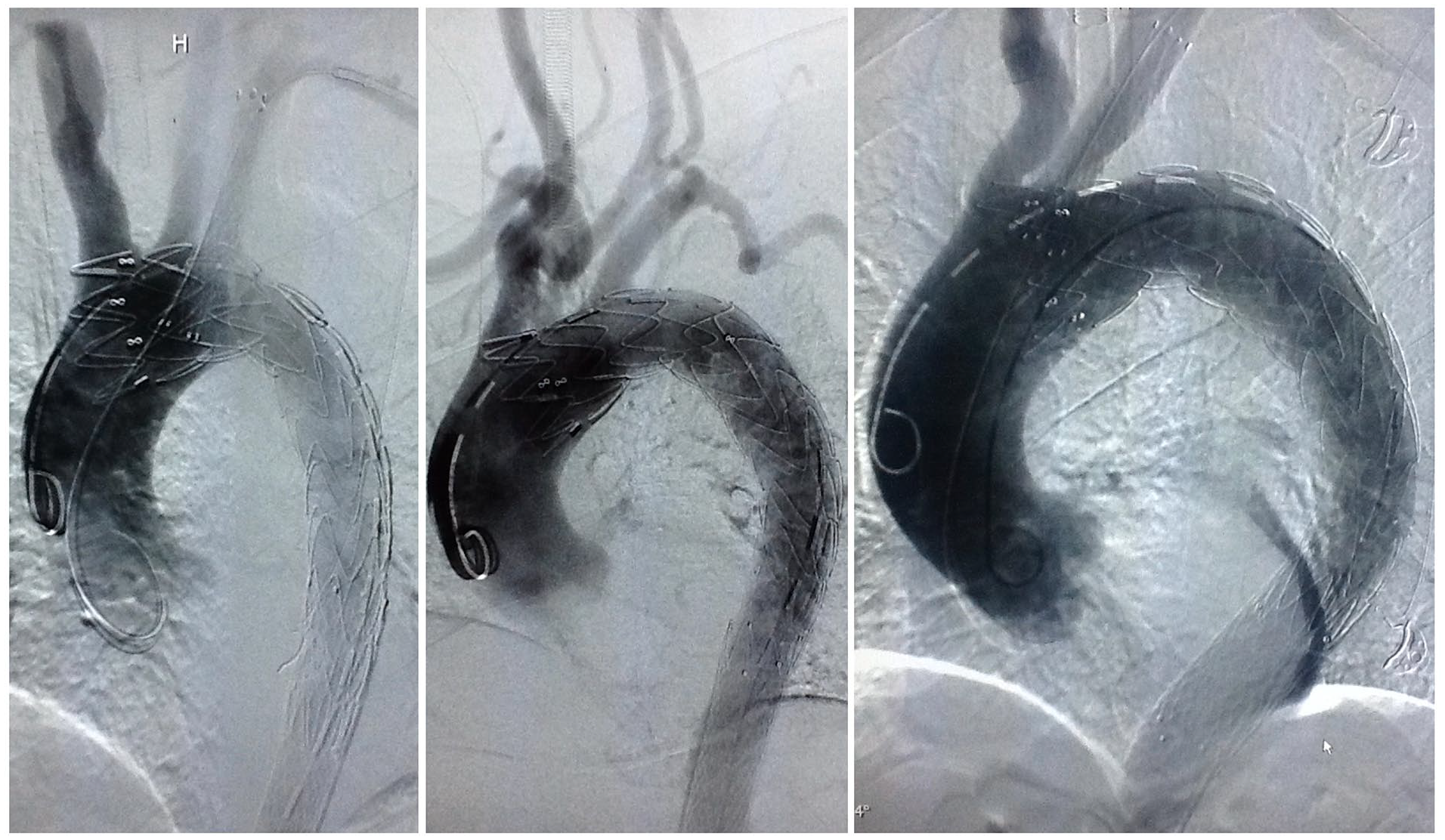
Complete DSA of 3 patients who later developed retrograde type A aortic dissection.
Follow-Up Outcomes
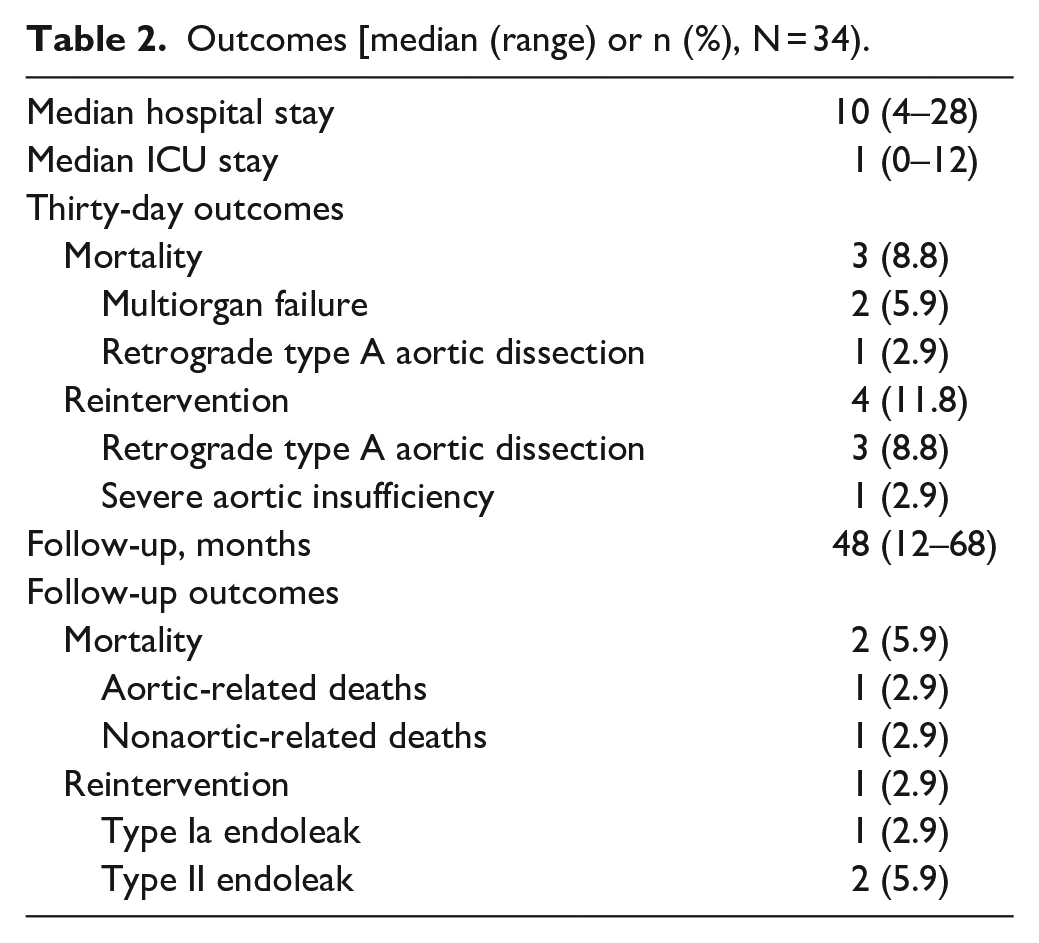
The median follow-up was 48 months (range, 12–68 months) (Figure 3). The estimated survival (±SE) was 85.1% ± 6.2% (95% CI: 69.9%–93.6%). Two patients died during the follow-up, including one aortic-related deaths and one non-aortic-related death. One patient died of rupture of aneurysm 13 months after the operation. The other patient died of bilateral stroke 7 months after the operation. The estimated freedom from reintervention (±SE) was 84.2% ± 6.5% (95% CI: 69.9%–93.5%). One patient had reintervention 13 months after the operation owing to type Ia endoleak. False lumen of the dissected aorta was embolized with coil, and no endoleak was observed after the operation. There were no conversions to open surgical repair, paraplegia, retrograde dissection, myocardial infarction, graft migration, and graft collapse. All supra-aortic trunks were patent. At the end of follow-up, the maximal diameter of dissected aorta had been reduced from 57.9 ± 9.9 (preoperative) to 38.5 ± 3.0 (p < 0.001). All patients exhibited complete thrombosis of the false lumen in the segment covered by stent-grafts. Detailed information about early and late outcomes are listed in Table 2.
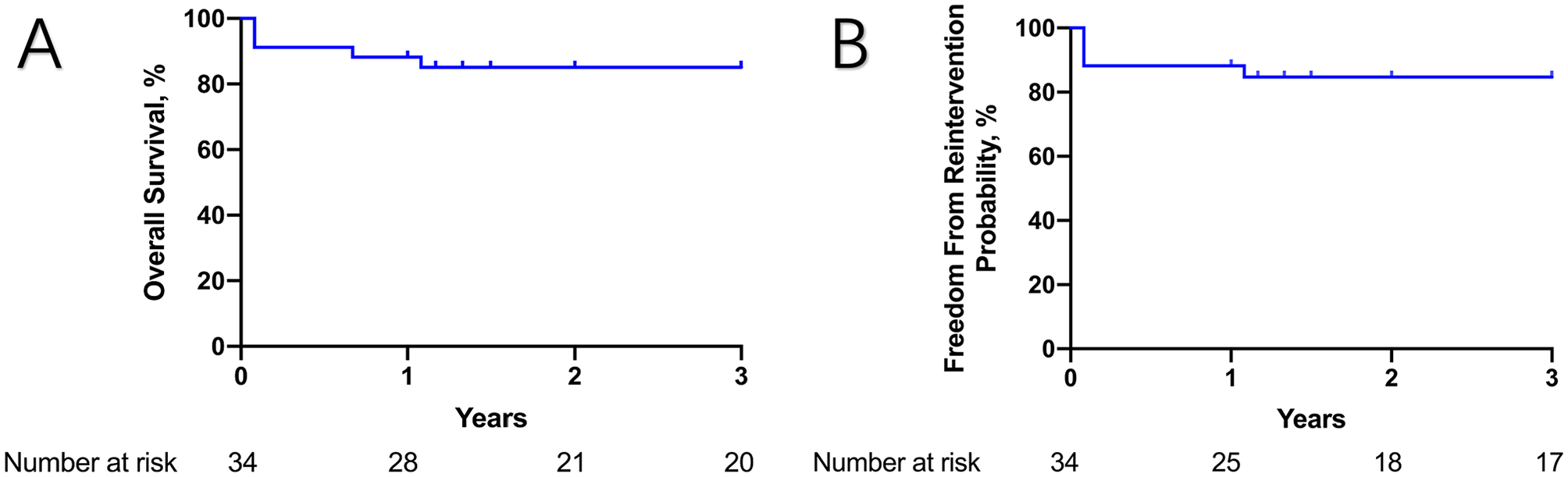
Kaplan–Meier curve of (A) overall survival; (B) freedom from reintervention.
Outcomes [median (range) or n (%), N = 34).
Discussion
With the development of endovascular techniques and devices, TEVAR has become a viable option for aortic arch pathologies. The European Society for Vascular Surgery had recommended TEVAR in zones 1 and 2 for patients with suitable anatomy. 1 Custom-made branched and fenestrated arch endograft, parallel graft, in situ fenestration, and fenestrated SMSG are available approaches.2–5,9 These techniques have been reported for treatment of aortic arch pathologies with promising outcomes, and currently there is no evidence showing one technique superior to another. Each technique has its advantages and disadvantages. In a meta-analysis regarding outcomes of zone 1 aortic arch hybrid endovascular repair, the in-hospital or 30-day mortality was 10.1%, the overall operative technical success was 89.8%, and the stroke rate was 9.5%. Zone 1 hybrid aortic arch repair is a reliable treatment option, whereas total endovascular repair is less invasive for patients. Chimney graft, which belongs to parallel graft, was used in our center for aortic arch pathologies before the application of fenestrated SMSGs. 10 However, owing to the high incidence of type I endoleak, which is the intrinsic shortcoming of chimney graft, we turned to TEVAR with fenestrated SMSGs. At early stage of the learning curve, misalignment between fenestrations and supra-aortic trunks did occur, and chimney technique was an ideal method as a rescue. Details about misalignment cases have been discussed in previous report. 11 Application of preloaded guidewire for LSA could reduce the risk of misalignment by protruding the guidewire into the fenestration for LSA during modification. With the combination of the technique described in our previous study and preloaded guidewire, misalignment would be avoidable at the early stage of the learning curve. For either double or triple fenestrated SMSGs, the alignment is based only on one fenestration, reducing the manipulation within the arch. When the fenestration is accurately aligned with target arteries, revascularization of supra-aortic trunks is accomplished as soon as fully deployment of fenestrated SMSGs, minimizing the cerebral hypoperfusion time. 12 With aforementioned advantages, fenestrated SMSGs is associated with low incidence of stroke and high technical success rate. In this series, stroke and technical success rate is 0% and 100%, respectively. Chassin-Trubert et al 13 reported low stroke rate and high technical success rate for total endovascular repair with fenestrated SMSGs, which is 4% and 94%, respectively.
Currently, no off-the-shelf stent-graft, either branched or fenestrated, is available in China; thus, various approaches were used in different centers. An understandable concern about off-label use of thoracic stent-graft is the long-term durability and stability. In our previous experience, only 3 cases (2.7%) of stent-graft migration and no stent fractures were identified during a 49.5 ± 18.3 months follow-up period. 14 In this series, no stent-graft migration and fracture were identified during a median follow-up of 48 months (range, 12–68 months). Nonetheless, stent-graft migration and fracture are related to severe complications and poor outcomes; thus, patients treated with fenestrated SMSGs must be under close and strict imaging surveillance in case of any potential stent-graft fracture and migration.
RTAD caused by stent graft-induced new entry is the most fatal complication after TEVAR. The incidence of RTAD after TEVAR could be as low as 1.3%, whereas the mortality rate of this catastrophic complication is up to 37.1%. 15 The incidence of RTAD after zone 1 aortic arch hybrid repair was 4.1%. 2 In our series, the incidence of RTAD was 8.8%, and the mortality rate was 25% in spite that all patients had received a timely open surgery. Compared with the low incidence of RTAD in surgical debranching technique, the incidence of RTAD in TEVAR with fenestrated SMSGs was high, suggesting the manipulation within the arch could have attributed to the occurrence of RTAD. Canaud et al 16 reported that the majority of RTADs occurred intraoperatively (20.9%) or in the postoperative period (50%), which was consistent with our series where all RTAD cases occurred within 30 days after the operation. This phenomenon suggested that most RTADs were triggered when the force was applied on the fragile intima exceeded its biological limitation. Furthermore, all patients developed RTAD were treated in acute phase, during which the aortic wall is more fragile. It has been reported that the odds ratio of RTAD was 10.0 (CI: 4.7–21.9) for acute aortic dissection and 3.4 (CI: 1.3–8.8) for chronic aortic dissection. 16 The dilemma between fragile aorta in acute phase and timely endovascular repair requires a more cautious decision for the treatment of aortic dissection.
The incidence of RTAD fluctuated for many years while continuing to decline, ultimately reaching a valley in 2016 to 2017. 17 The recognition of connection between oversizing rate and RTAD should have made an important contribution to the decrease of RTAD. In recent years, 5% oversize rate has been widely accepted, and 0% oversize rate for aortic dissection has been suggested. 18 Ma et al 19 set up a computational model to investigate the interaction between valiant thoracic stent-graft and aorta in RTAD after TEVAR and found that higher oversize rate is associated with higher stress on aortic wall, showing a 2-fold increase in 15% oversize rate than that of 0% oversize rate. This inferred that if 0% oversize rate could provide a stable fixation of stent-graft in the long run, it would carry along the lowest rate of complications (mostly caused by the radial force for fixation of stent-graft) compared with any other oversize rate.
Ma et al. also suggested maximal aortic stress as the main cause of RTAD, which was 2- to 3-fold than that of 50% distal oversize rate. Maximal aortic stress was found on the proximal bare stent contacting the greater curvature side of the arch. The conclusion was later verified in canine models, whether developed RTAD or not. 20 The canine model developed RTAD had significantly higher maximal aortic stress at the greater curvature side of the aorta than the model without RTAD. The development of RTAD requires the maximal aortic stress to exceed the tolerance of aortic wall, further emphasizing the importance of a comprehensive understanding about the interaction between stent-graft and aortic wall, including biomechanical property of aortic wall, relation between angulation (that of stent-graft and aortic wall) and maximal aortic stress, and material property of stent-graft.
In our series, a new entry tear was found near the proximal bare stent at the greater curvature side in 2 RTAD cases, which was consistent with the point of maximal aortic stress suggested by Ma et al. Compared with another series with zone 0 landing in our center where no RTAD occurred, it can be inferred that zone 1 and zone 3 landing, where the curvature is larger, carried with higher risk of RTAD. The maximal aortic stress should be lowest when the stent-graft is released in a straight artery. Kudo et al 21 also found that zone 0 landing had significantly fewer, shorter, and less angulated bird-beak configurations than zones 1 and 2 landing. At a mean follow-up of 4.2 years, the rate of stent-graft migration was significantly lower for zone 0 landing than zones 1 and 2 landing. Compared with zones 1 and 2 landing, zone 0 landing is associated with lower incidence of RTAD, type Ia endoleak, and device migration according to our experience and previous report. Moreover, our experience and study from other centers presented with promising early outcomes of zone 0 landing TEVAR in high-risk patients for open surgery. These evidence suggested the idea of extending proximal landing zone into zone 0 instead of zones 1 and 2 landing in selected cases, but only can be performed in centers capable of revascularizing all supra-aortic trunks.
Limitations
This is a retrospective study with a small sample size. There is no control group to compare fenestrated SMSG with other techniques including parallel graft, custom-made branched or fenestrated stent-graft, and in situ fenestration. Comparison of cost-effectiveness among different strategies deserves evaluation to benefit lower-income patients. Further follow-up is required to verify long-term durability and stability of off-label use and outcomes of this technique.
Conclusions
Outcomes of the study revealed zone 1 TEVAR with fenestrated SMSGs as a feasible method for aortic arch pathologies. The relative high incidence of RTAD alerts the importance to consider the aortic wall–stent-graft interaction when choosing proximal landing zone. Individualized design of fenestrations enables precise treatment for patients with different anatomical and morphological features. Spatial transformation of fenestrations when crossing the arch reduces the difficulty in aligning fenestrations with target arteries and cerebral hypoperfusion time. The short modification time and application of off-the-shelf stent-graft allows usage of fenestrated SMSGs in emergency.
Supplemental Material
sj-docx-1-jet-10.1177_15266028221108903 – Supplemental material for Outcomes of Zone 1 Thoracic Endovascular Aortic Repair With Fenestrated Surgeon-Modified Stent-Graft for Aortic Arch Pathologies
Supplemental material, sj-docx-1-jet-10.1177_15266028221108903 for Outcomes of Zone 1 Thoracic Endovascular Aortic Repair With Fenestrated Surgeon-Modified Stent-Graft for Aortic Arch Pathologies by Xiaoye Li, Lei Zhang, Chao Song, Hao Zhang, Shibo Xia, Longtu Zhu, Wenying Guo, Haiyan Li, Zaiping Jing and Qingsheng Lu in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.