
Abstract
Vietnamese Americans experience high rates of infectious disease-related cancers, specifically cervical cancer caused by Human Papillomavirus (HPV) and liver cancer linked to Hepatitis B (Hep B). Vaccination is critical for cancer prevention, but HPV and Hep B vaccine uptake remains suboptimal among this group. This qualitative study examined factors influencing Vietnamese American young adults’ decisions to receive elective vaccines, including HPV, Hep B, flu, and COVID-19. Twenty-one participants, aged 18 to 26, were recruited through social media platforms and participated in semi-structured interviews. The findings revealed high levels of vaccine acceptance, with common themes including family influence, cultural values, and concerns about side effects. While COVID-19 and flu vaccines were generally accepted due to work or school requirements, family protection, and trust in health care providers, HPV and Hep B vaccines had more hesitancy, particularly due to misconceptions around reproductive health and lack of awareness. Results highlight the cultural importance of familial responsibility, particularly the concept of filial piety, in COVID-19 vaccine uptake. The study suggests future cancer vaccine interventions should integrate cultural and familial dynamics to position HPV and Hep B vaccines as essential cancer prevention tools. Engaging families, health care providers, and community networks in vaccine promotion efforts may help improve coverage rates and reduce cancer disparities in the Vietnamese American population.
Keywords
Vietnamese Americans (VAs) are among the fastest-growing Asian ethnic groups in the United States (Budiman & Ruiz, 2021). This community has elevated rates of cervical cancer caused by Human Papillomavirus (HPV) and liver cancer linked to Hepatitis B (Hep B) infection (R. J. Lee et al., 2021). VA women have one of the highest age-adjusted cervical cancer incidence rates (16.8%), more than double that of non-Hispanic White (NHW) women (8.1%; Ma et al., 2015), and are nearly twice as likely to die from the disease (Nguyen-Truong et al., 2018). VAs also have the highest age-adjusted liver cancer incidence (47.3% in males, 14.4% in females) and mortality rates among Asian Americans (AAs; Pham et al., 2018).
Cancer-preventing vaccines for HPV and Hep B are effective, yet vaccination remains low among VAs (A. W. Lee et al., 2019; Vu et al., 2022). In contrast, VAs have high annual influenza (flu) vaccination rates (61%) compared with other AA groups (45%; Tse et al., 2018). They are more willing to be vaccinated for flu and COVID-19 (Wu et al., 2022), and show fewer negative COVID perceptions than other AA groups (Ta Park et al., 2021).
This positive vaccine perception contrasts with the lower HPV and Hep B vaccine rates. VA adolescents have a 52% HPV vaccination initiation and only 35% complete the series, far below the national averages (75% and 59%, respectively; Vu et al., 2023). Hep B vaccination rates are similarly low at 26%, a 10% decline since 2006 (T. T. Nguyen et al., 2010). Although VAs exhibit positive attitudes toward flu and COVID-19 vaccines, little is known about their perceptions and self-efficacy regarding cancer-preventing vaccines.
Recent media-based interventions identified family influence and health care provider recommendations as key factors increasing HPV (Duong & Hopfer, 2021) and Hep B (Chu et al., 2022) vaccine uptake among VAs. A gap remains in the literature. Prior studies examined the drivers of HPV and Hep B vaccines separately, despite their similar age-based immunization schedules and roles in cancer prevention (Constable & Caplan, 2020). Given the high risk of cervical and liver cancer in this population, this study examines VA young adults’ perceptions, facilitators, barriers, and potential connections to elective vaccines.
Method
In summer 2023, we conducted a qualitative cross-sectional study of VA young adults to explore perceptions of elective vaccines (HPV, Hep B, flu, and COVID-19). The study was informed by the Health Behavior Model (HBM), which predicts health beliefs and behaviors, including vaccine acceptability (Fallucca et al., 2022; Gutierrez & Wolfe, 2022). The HBM’s five constructs—perceived severity, perceived susceptibility, perceived barriers, perceived benefits, and self-efficacy—were used to examine vaccination perceptions (Jones et al., 2015). We consulted literature on vaccine decision-making, including knowledge, doctor’s recommendations, and culture (Chen et al., 2022; C. Nguyen et al., 2022; Vu et al., 2023).
Data Collection Instruments
A pre-interview questionnaire collected demographic information (age, gender, ethnicity, education, and state of residence) and assessed health care and vaccination status, including insurance, regular doctor, and elective vaccine uptake. The HBM guided the development of the semi-structured interview guide. Sample questions included: (1) How would you describe your attitude toward vaccines? (2) What do you know about cancer vaccines? (3) Do you have any family history of cancer? (4) What do you think are the advantages of receiving the vaccine? (5) If you were eligible for a booster, would you get one in the next 6 months? Questions were asked for each of the four vaccines and tailored based on participants’ pre-interview responses. Participants’ vaccine statuses guided follow-up probes, enabling the interviewer to explore beliefs, knowledge, and decision-making processes specific to each individual’s experience.
Participant Recruitment and Data Collection
Participants were recruited online through public and private VA social media groups on Facebook and Instagram, identified through keyword searches for Vietnamese-centered pages. We posted digital flyers with study information, eligibility criteria (identified as Vietnamese American, 18 to 26 years old, residing in the United States, and English-speaking), and a link to the pre-interview questionnaire. Eligible participants completed the questionnaire on Qualtrics and scheduled a Zoom interview via Calendly to ensure anonymity. The study was approved as exempt research by the University of California, Irvine’s Institutional Review Board (IRB). A sample size target of n = 15 was determined based on projected data saturation, defined as no new themes emerging after five consecutive interviews (Guest et al., 2020). Participants received a U.S. $50 Walmart or Amazon gift card, and each 45- to 60-min interview was audio-recorded.
Data Analysis
The primary author interviewed the participants via Zoom. Zoom’s Live Transcript feature and integrated Otter.ai transcription add-on generated interview transcripts, a validated approach in prior qualitative research (e.g., Vedapudi et al., 2024). The primary author conducted a post-interview clean-up to ensure transcript accuracy. Dedoose 9.0.46 was used to organize and code the data. Steps were taken to minimize subjectivity and potential biases in the interpretation of a single coder. In the first coding round, each transcript was reviewed and coded in short passages to identify emergent themes and subcodes. The HBM informed a clear coding scheme to mitigate concerns associated with a single coder (Campbell et al., 2013). A deductive coding approach was used to categorize data according to HBM constructs to identify initial themes related to individual factors influencing vaccine perceptions and behaviors.
An inductive approach captured unanticipated insights. Subsequent coding rounds systematically categorized themes within HBM constructs to allow for flexibility and theoretical alignment. This iterative analysis allowed for deductive model confirmation and inductive subcode refinement. This modeled techniques in the literature (McDonald et al., 2019), such as triangulation, to enhance single-coder qualitative analysis, allow for deeper data engagement, and reduce reliance on multiple coders.
In the final round, subcategories within each construct were refined to capture the nuances of participants’ perceptions and behaviors. The recursive nature allowed emergent themes to be thoroughly captured using systematic reflection and transparent methods to maximize reliable and valid results (Belotto, 2018). The overall process facilitated researcher reflexivity and consistency, and minimized single-coder bias since the same researcher returned to the data multiple times (Cofie et al., 2022).
Results
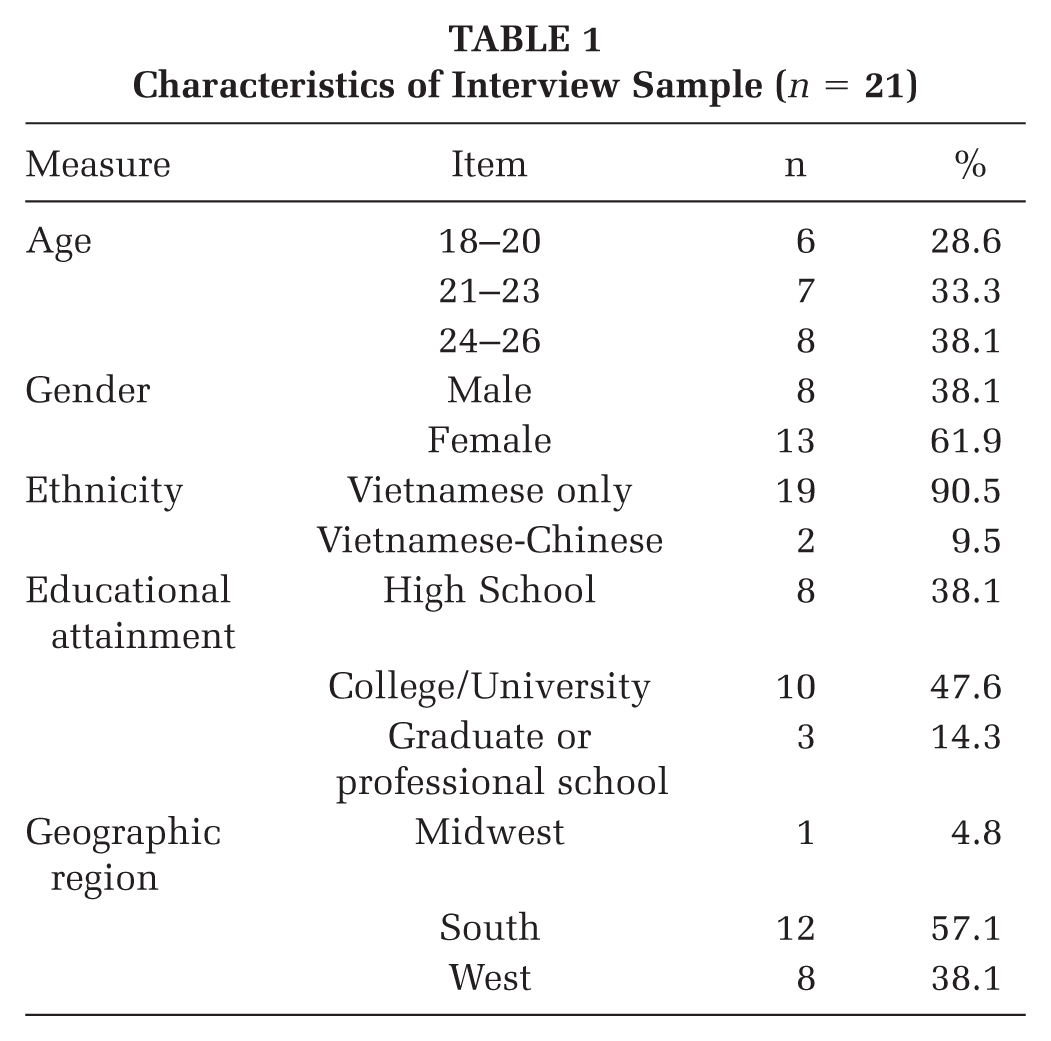
A total of 21 participants were interviewed, with the majority aged 24 to 26 (n = 8). Most identified as VA (n = 19), while two identified as Vietnamese-Chinese American. The majority were female (n = 13) and had completed higher education (n = 13; see Table 1).
Characteristics of Interview Sample (n = 21)
Most participants had a regular medical provider (n = 18) and insurance (n = 18). While most received the HPV and Hep B vaccines, nearly a quarter did not receive the flu vaccine. All participants received the COVID-19 vaccine, though a few did not receive the booster (see Table 2).
Health Care and Vaccination (n = 21)
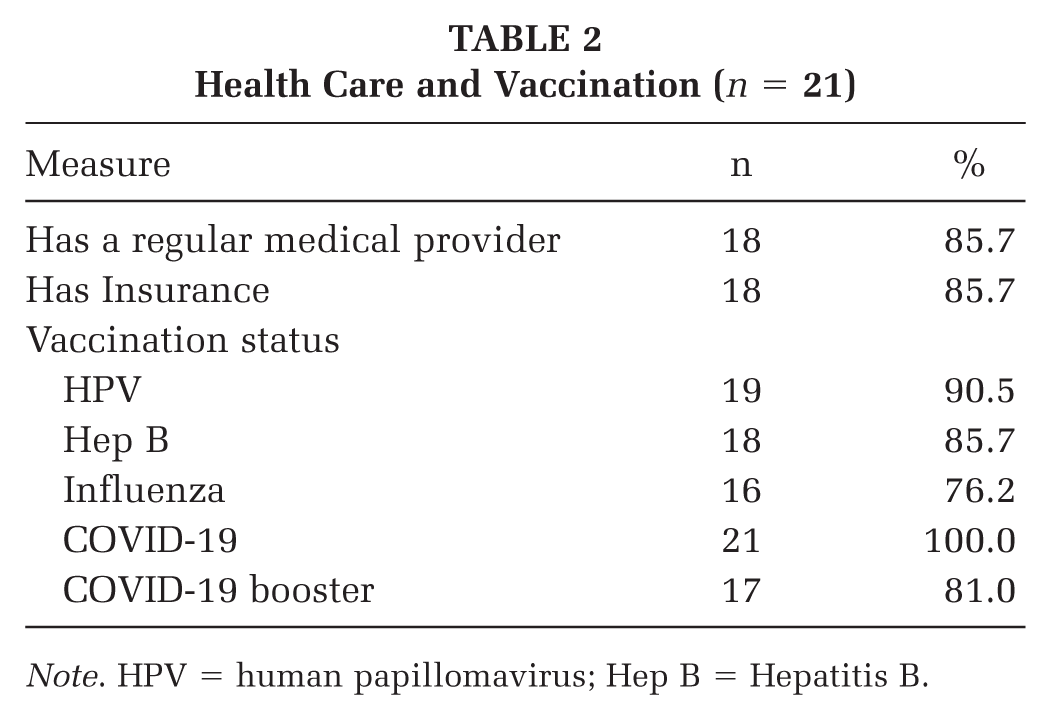
Note. HPV = human papillomavirus; Hep B = Hepatitis B.
Themes Regarding Vaccine Perceptions
Table 3 shows the shared and unique themes influencing each vaccine.
Themes Influencing Vaccine Uptake
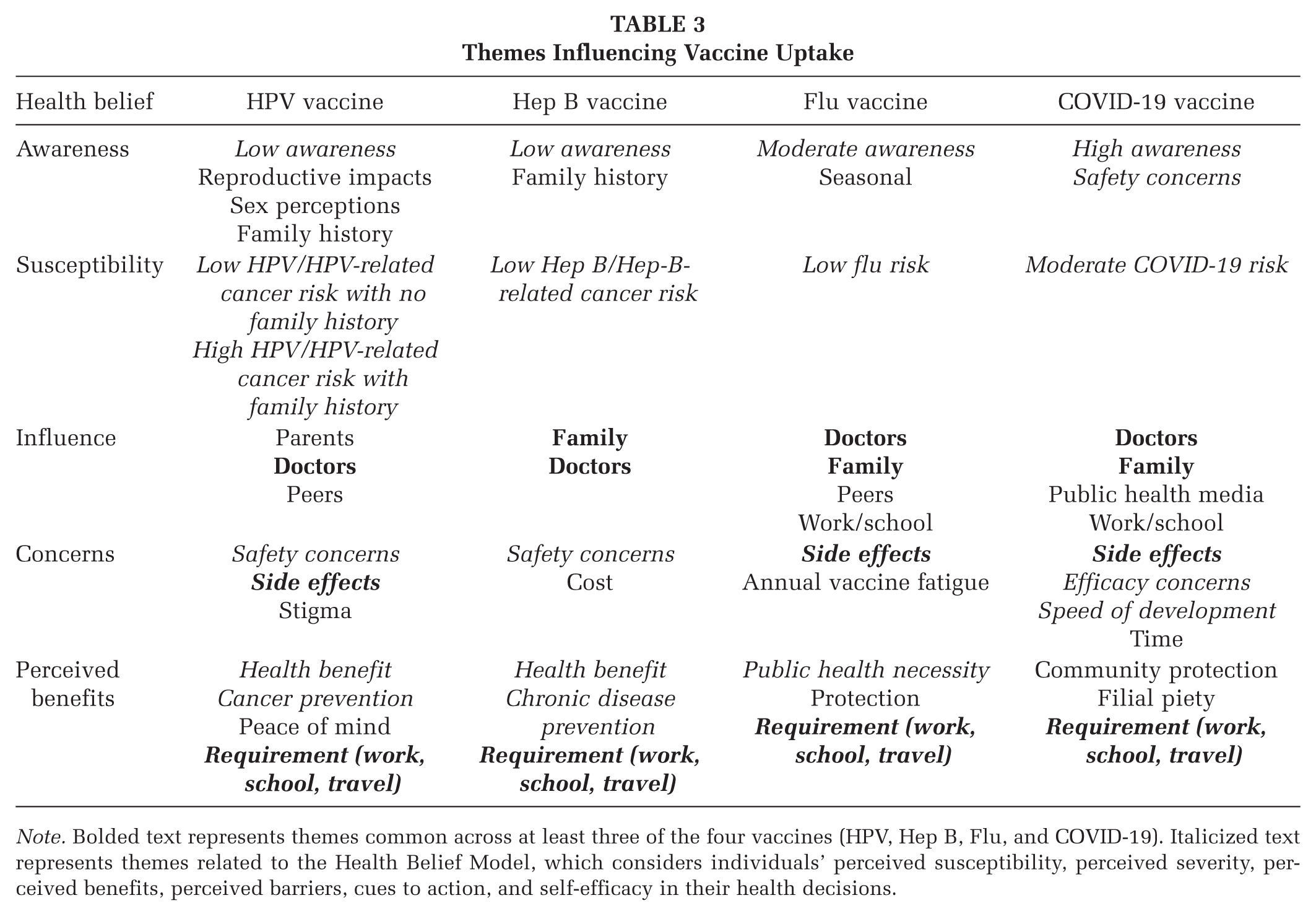
Note. Bolded text represents themes common across at least three of the four vaccines (HPV, Hep B, Flu, and COVID-19). Italicized text represents themes related to the Health Belief Model, which considers individuals’ perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy in their health decisions.
HPV Vaccine
Nearly all participants (n = 19) received the Human Papillomavirus (HPV) vaccine, with most (n = 16) recalling receiving it during adolescence. However, many were not well-informed about the vaccine’s necessity. Several participants were unsure about the recommended age and number of doses required. Fifteen participants displayed low knowledge or held misconceptions about the vaccine, believing it was only for those sexually active or that receiving it implied a desire to be sexually active. One 18-year-old woman in Washington shared, “I don’t think it came into my mind because I’m not sexually active for like it to come near me (sic).” Five female participants expressed concerns about its impact on reproductive health, with one 21-year-old woman from Alabama noting, “I’ve heard people really being concerned with just like how safe it is because I think they hear about infertility.” Unlike other vaccines, misconceptions about the HPV vaccine pertained to sexual and reproductive health, reflecting societal stigmas and misinformation about its safety and effects on women’s health.
Doctors played a notable role in HPV vaccine uptake. Nine participants recalled that their health care provider recommended the vaccine when they were of age. Consequently, parental influence was also significant in vaccine uptake. Twelve participants noted that their parents’ decisions affected their vaccination status. One 22-year-old man from Alabama recalled, “Whenever I went to my doctor as a child growing up, they always just kind of told me what kind of vaccines I needed at that specific age, and my parents and I just consented to it.”
Safety was another key concern. Two participants did not receive the HPV vaccine due to their parents’ concerns about safety. Eight participants—including those who received the vaccine and those who did not—expressed hesitancy due to safety concerns. A 25-year-old woman from Alabama, who received the HPV vaccine as a child, shared, “I would like to say it’s safe, but I’m not sure just because everyone’s different and how people react is different.” Seven participants acknowledged the vaccine’s importance for public health, particularly cancer prevention and school requirements.
Participants’ risk perceptions varied, with some expressing a lower perceived risk of developing HPV or HPV-related cancers, partly due to a lack of awareness about the cancers prevented by the vaccine. Perceived risk was higher among those with a family history of cancer. One 25-year-old woman in California shared, “Because my mom had cervical cancer, my parents were more adamant about me getting the HPV vaccine.” In addition, eight participants expressed openness to receiving an HPV booster if offered, showing a willingness to pursue further vaccination if recommended by health care providers.
Hep B Vaccine
Like the HPV vaccine, nearly all participants (n = 18) received the Hepatitis B (Hep B) vaccine. However, awareness about the Hep B vaccine varied among participants. Thirteen participants were unaware of the vaccine or its benefits. Some participants knew more about the HPV vaccine than about Hep B. A 20-year-old woman from California stated, “I knew about HPV before you mentioned it, but I didn’t realize that Hepatitis B is a cancer-related thing.” Others had no background on the vaccine, with one 21-year-old woman from Washington, a public health undergraduate student, sharing, “It’s kind of a shame for me to have to say this, but I don’t know much about them.”
Doctors also played an important role in vaccine uptake, with 10 participants reporting that their health care provider recommended the Hep B vaccine to their parents. Parental influence was also significant. Fourteen participants recalled that their parents opted for the Hep B vaccine, leading to their initiation of the series.
The vaccine was considered necessary by 11 participants for its role in preventing chronic liver disease. Two participants had a family history of liver cancer, and three participants had a family history of Hepatitis B virus, which heightened their awareness of the vaccine’s importance. A 22-year-old man in Missouri shared, “I know there is a family history of Hepatitis B, and because of that, I know a little bit more about Hep B and the importance of prevention.” Similarly, a 25-year-old man from Florida, whose mother and paternal uncle have liver cancer, shared that family history played a “big factor” in ensuring he received the Hep B vaccine. In addition, eight participants noted that school or work requirements contributed to their perception of the vaccine’s necessity.
In contrast to perceptions of sexual promiscuity related to the HPV vaccine, concerns about the Hep B vaccine focused more on cost. A 20-year-old woman from Virginia shared that although she received the Hep B vaccine as an adolescent, affordability was still a concern, stating, “It sounds like an expensive vaccine.” Similarly, eight participants expressed that if they had not received the vaccine as children, they would be worried about the expense of paying for the series as adults.
Flu Vaccine
Of the four vaccines assessed, the flu vaccine had the most variability in uptake. Sixteen participants received their annual flu vaccine, citing protection for themselves and others. Twelve participants mentioned familiarity with the vaccine’s seasonal nature and positive past experiences. A 21-year-old woman from Alabama shared, “I think it’s just like a precaution. I don’t think I’ve ever had the flu before, but as a preventive measure, I always get it every year.”
Among recipients, the flu shot was viewed as necessary for both public health and personal protection. A 21-year-old woman from Washington, who got it annually, shared, “I feel like it’s an obligation for myself to get it to maintain my healthy status.” Fourteen participants emphasized its importance during flu season and for school or work requirements, particularly those in health care, who cited their field as the key motivator for annual vaccination.
Doctors were less influential in the decision-making process for the flu vaccine compared with cancer-preventing vaccines. Only three participants mentioned their doctor’s recommendation for the flu shot. Instead, interpersonal influences, such as family (noted by 10 participants) and school/work requirements (mentioned by 15 participants), were significant factors in the decision to receive the annual flu vaccine.
Hesitancy was present among the five participants who did not receive their annual flu vaccine. They cited reasons such as vaccine fatigue due to its seasonal nature or feeling that it was unnecessary, as they rarely got sick. One 25-year-old man from Florida noted,
I didn’t feel that it was necessary. I didn’t go out of my way to get them (flu shots) because I felt like it was a secondary thing to handle. The flu and any exposure to it sit in the back of my mind because I just never get it.
Overall, the flu vaccine’s annual nature and routine familiarity contributed to its acceptance, though not without varying degrees of skepticism.
COVID-19 Vaccine
Awareness of the COVID-19 vaccine was nearly universal, with all 21 participants receiving it and acknowledging its importance. Many trusted science and health care providers. An 18-year-old woman from Washington shared, “A lot of people are recommending it, like health officials, so I trust them and I want to prevent myself from getting COVID.” While 12 participants expressed concerns about the vaccine’s side effects and the speed of its development, they still trusted the science. Twelve participants also cited work and school requirements as reasons for vaccination.
Social and traditional media influenced 16 participants’ perceptions, with consistent and prevalent messaging increasing their confidence in the vaccine’s safety and efficacy. One 24-year-old man from Arizona was motivated to get vaccinated because of its television coverage, sharing, “I think the biggest factor outside of hearing and learning about it (online) was the news. I specifically got it because of what the news was saying.” Three participants felt that the popularization of the vaccine on platforms like Facebook and Instagram made them perceive it more positively. A 20-year-old woman from Alabama mentioned, “I got most of my news about the vaccine through social media, like the CDC’s social media.”
Family was a significant factor in the decision to receive the COVID-19 vaccine. Eight participants expressed a strong sense of responsibility to safeguard their family members, particularly their parents and elders. One participant said they felt the need to care for their family’s well-being before their own, as part of their cultural background. A 21-year-old woman from Washington stated, “I care more about my family than my own health. I think that’s the main part of Vietnamese culture too, like your family is above most other things.” Ten participants specifically mentioned their grandparents as a primary reason for getting vaccinated, as they wanted to safeguard their health and be able to visit them. A 19-year-old man from California stated,
I was scared of getting it (COVID-19) myself, but I live with my grandparents, so most of the stress was towards not getting them sick because of their poor health. Getting COVID for me might be like getting a cold, but for my grandparents, it would be worse. I worried about my grandparents and my parents too.
Familial selflessness and responsibility only emerged in discussions about the COVID-19 vaccine.
Conversely, some participants prioritized getting vaccinated for personal health, believing that by protecting themselves, they could better protect their family members. Ten participants shared this perspective. A 21-year-old woman from Alabama shared, “I think that [personal health] would probably be above all because if I can’t do anything with my own health, there’s nothing I can do about the others.”
Uptake of the COVID-19 booster showed more variability. Most participants (n = 17) received the booster in the last 6 months. Among those who did not, common reasons included feeling sufficiently protected or lacking time to get the shot. While five participants did not receive the flu vaccine, all participants received the COVID-19 vaccine.
Overall, family history, cultural values, and institutional requirements shaped vaccine decisions across all four elective vaccines.
Culture and Family on Health
All 21 participants discussed themes related to family and culture’s impact on health and well-being. Key themes surrounding family and health care access included language barriers among older adults, the influence of social media within the Vietnamese community, political alignment perpetuated on social media, and the reliance on younger family members to navigate the health care system.
Six participants highlighted how language barriers affected their families’ understanding of medical information, communication with health care providers, and access to accurate vaccine information. A 22-year-old woman from Oregon shared that her grandparents’ limited English impeded their accessibility, noting, “They don’t have the language to navigate public transportation, much less the doctor’s office.” A 26-year-old woman from Texas echoed this sentiment, recalling, “When they (parents) switch between languages, maybe they don’t understand, and it’s not being fully translated correctly, and so they don’t understand what the vaccines can do to help them.” Participants recognized that although they did not face language barriers, such barriers affected their older family members’ ability to communicate health matters, thereby affecting their access to and navigation of health care services.
Seven participants discussed how social media platforms, specifically Facebook and YouTube, influence Vietnamese families’ understanding and uptake of health prevention and resources. A 22-year-old man from Missouri noted that his mom primarily got her news on Facebook and YouTube, especially from non-science channels and/or creators. Four participants discussed how political alignment and conservative values are heavily tied to popular VA media, influencing health care utilization, especially vaccine uptake. One 23-year-old woman in Alabama shared, “They [parents] are conservative, and they stigmatize [cancer] vaccines because they think that it’s like an STD vaccine,” highlighting how political values, often shared on social media, influence health behaviors in this community.
Eight participants noted that younger people often help the older generation navigate vaccine information and make informed choices, highlighting the role of intergenerational support in the decision-making process for vaccinations. One 21-year-old woman from Alabama, who works in health care, noted that many older VAs attend appointments with a younger family member who would translate the visit. Thus, familial relationships shape VAs’ health care access and decision-making.
Discussion
To our knowledge, this is the first study to examine Vietnamese American young adults’ elective vaccine perceptions and decision-making processes. Most participants received all four vaccines, but attitudes, knowledge, and understanding varied across vaccine types. The most salient HBM constructs influencing vaccine uptake were perceived susceptibility, perceived benefits, and self-efficacy, particularly when shaped by family.
Family dynamics, cultural values, provider recommendations, and institutional requirements all played critical roles. These results align with prior research among AA subgroups. Family and provider influence are central to HPV uptake among Korean Americans (Vu et al., 2020) and Hep B uptake among Chinese Americans (Vedio et al., 2017). This study advances the literature by identifying cross-cutting themes across multiple elective vaccines, rather than examining each in isolation. It disentangles the relational mechanisms, such as familial expectations and cultural obligations, that shape how family influences health behaviors.
All participants noted family impact on health decision-making. Filial piety, defined as respect for and duty to one’s family (Li et al., 2021), was particularly salient in motivating COVID-19 vaccination. VA young adults’ health decisions were rooted in collective, culturally-informed values rather than individual autonomy. Provider recommendations and institutional mandates reinforced self-efficacy by offering clear and actionable guidance.
This study’s limitations include the use of a convenience sampling method through social media, which may not fully represent the diverse VA population. The reliance on a single coder for data analysis may introduce interpretive bias, such as overemphasizing themes or overlooking alternative perspectives. However, we implemented multiple strategies, including saturation, systematic reflection, and theoretical triangulation, to minimize this risk. The sample skewed toward participants with higher educational attainment, a factor associated with higher vaccination rates (Lupu & Tiganasu, 2024). These findings may not fully reflect barriers experienced by less-educated individuals. Finally, the uneven geographic distribution of participants across nine states limits the ability to generalize results nationally.
Implications for Practice
Despite the limitations, this study offers key insights into how HBM constructs intersect with cultural and community factors to shape vaccination decisions among VAs. To strengthen overall vaccine uptake, health promotion practitioners should focus on community-level interventions that leverage the central role of family and cultural values. Health promotion practitioners should design communication campaigns that frame HPV and Hep B vaccination as a clear act of familial responsibility and cancer prevention, aligning with the cultural concept of filial piety. These campaigns should utilize trusted community networks, such as faith-based organizations and community health centers, and social media platforms like Facebook and YouTube, to disseminate accurate, culturally competent messaging that explicitly addresses misconceptions around sexual health and affordability.
In addition, medical students and practicing providers should receive ongoing training on vaccination guidelines that leverage key HBM constructs. Providers should be aware of the elevated risk of infection-related cancers in VA communities and their historically lower vaccination rates. In clinical settings, providers and educational materials should incorporate cultural competency, especially regarding family dynamics, to effectively promote vaccines. This includes addressing concerns about safety and side effects while highlighting perceived benefits, such as improved overall health and disease prevention. In general, cancer vaccine messaging should center VA cultural and familial values to enhance vaccine promotion, particularly among individuals who may have missed vaccinations during childhood or immigration.
Implications for Research
Researchers should examine cross-vaccine themes among disaggregated AA subgroups to better understand the nuanced sociocultural drivers of vaccine decision-making. Understanding these within-group variations can help identify culturally specific barriers and facilitators that inform tailored outreach and education strategies. Researchers should also investigate reasons for missed cancer vaccinations and parental opt-outs to clarify gaps in vaccine delivery, communication, and trust. In addition, examining how state and federal policies, such as Medicaid and Medi-Cal, affect vaccine accessibility can inform equitable health coverage nationwide. Comparative policy analyses could highlight how adopting Medi-Cal’s inclusive coverage of all ACIP-recommended vaccines (including HPV and Hep B) may improve vaccination rates and reduce cancer disparities. Finally, researchers should explore multilevel and community-engaged approaches that integrate cultural, familial, and health care system factors to advance vaccine uptake and reduce cancer risks among VAs. Overall, a multi-targeted approach is crucial to increasing vaccination rates and reducing cancer risks among Vietnamese Americans.
Footnotes
Authors’ Note:
We would like to thank the community members who participated in the interview and the University of California, Irvine Joe C. Wen School of Population & Public Health. The study was supported in part by the Cancer Epidemiology Education in Special Populations (CEESP) Program through funding from the National Cancer Institute, Grant # R25 CA112383, and the University of California Presidential Chair fund of Dr. Oladele Ogunseitan.