
Abstract
Objective
This study sought to identify factors associated with (1) situational awareness (i.e., daily recognition of situations to make choices to act in the best interest of one’s health) and (2) the self-care gap (i.e., not acting in one’s best interest despite having recognized at least one opportunity to perform healthful behaviors).
Methods
Data from 1,761 non-Hispanic Black (58.4%) and Hispanic (41.6%) men aged 40 years or older with chronic conditions were collected using an internet-delivered questionnaire. Two linear regression models were fitted to assess factors associated with situational awareness and the self-care gap, respectively. Regression models were adjusted for sociodemographics, disease symptomatology, preventive screening activity, health behaviors, and health-related perceptions.
Results
Situational awareness levels were lower for older individuals (B = −.03, p < .001). Men who had higher fatigue (B = .11, p = .002), more stress (B = .07, p = .032), utilized more prevention screenings (B = .13, p = .001), adhered to physical activity guidelines (B = .36, p = .044), and received more social support (B = .89, p < .001) reported higher situational awareness. The self-care gap was more pronounced among non-Hispanic Black men (B = −.32, p = .026). Men who reported higher fatigue (B = .06, p = .041), clinical depression (B = .39, p = .039), more barriers to self-care (B = .11, p < .001), and higher frustrations with health care (B = .12, p < .001) were associated with greater self-care gaps.
Conclusions
Men’s recognition of healthful opportunities was largely driven by their disease symptomatology, greater engagement in preventive screenings, and receiving social support. However, the self-care gap was seemingly driven by mental health and challenges with disease self-management and health care interactions. Efforts are needed to narrow disparities in the self-care gap between non-Hispanic Black and Hispanic men.
Keywords
Background
In the United States, significant health disparities persist among non-Hispanic Black and Hispanic adults (Jr, 2021; Odlum et al., 2020). An estimated 52% of American adults are estimated to have one or more chronic health conditions (e.g., heart disease, diabetes, cancer), with predominant rates existing among non-Hispanic Black (52.4%) and Hispanic (38.5%) adults (Control & Prevention, 2020). These racial and ethnic groups experience a disproportionate burden of chronic diseases, often developing long-term health conditions earlier in life and at an accelerated rate compared with non-Hispanic White populations (Quiñones et al., 2019). This disparity underscores the critical need for effective self-care strategies to manage these health issues (Smith, Bergeron, Riggle, et al., 2017).
Self-care is a multidimensional concept that has evolved over the past few decades (Riegel et al., 2019), becoming increasingly acknowledged as an essential component of both individual health management and health care systems (Riegel et al., 2021). Scholars provide a comprehensive definition, whereby self-care encompasses a range of intentional activities that individuals learn and implement across physical, psychological, social, and spiritual domains to achieve optimal health (Matarese et al., 2018; Richard & Shea, 2011). Situational awareness, defined as the ability to perceive environmental elements (perception), comprehend their meaning and interconnections (comprehension), and project their future states (projection) (American Psychological Association, 2018), can significantly influence self-care practices (Riegel et al., 2022). In the context of health behaviors, situational awareness involves an individual recognizing health-related cues in their environment and understanding their implications for their own well-being (both proximal and distal outcomes). For individuals with chronic conditions, situational awareness is crucial for effective self-care because it enables them to identify opportunities for health-promoting actions throughout their daily lives. For example, a person with diabetes might perceive the availability of healthy food options (perception), understand how these choices impact their blood sugar levels (comprehension), and foresee the need to adjust their insulin dosage accordingly (projection). This continuous process of awareness and decision-making forms the foundation for proactive self-care behaviors. However, it is widely recognized that men are less likely than women to routinely seek preventive care and engage in self-care behaviors (Smith et al., 2018).
Health disparities experienced by non-Hispanic Black and Hispanic men with chronic conditions are influenced by individual-level factors and broader community- and systemic-level barriers. At the community level, evidence shows that social networks, cultural norms, and peer influences significantly impact health behaviors and health management practices (Fisher et al., 2014; Laranjo et al., 2015). For instance, culturally influenced perceptions of masculinity often discourage men from engaging in preventive care, leading to delayed health care utilization and poorer chronic disease management (Evans et al., 2011; Hammond et al., 2010). In addition, systemic-level barriers such as limited health care access, insufficient availability of culturally appropriate health care services, and perceived discrimination within health care settings disproportionately affect men in minoritized groups (Togioka & Young, 2024; Walker et al., 2016; Williams et al., 2023).
Although health disparities between racial and ethnic groups in chronic disease prevalence and management are well-documented, the literature remains limited regarding specific psychosocial factors driving these disparities among non-Hispanic Black and Hispanic men. Previous research indicates that non-Hispanic Black men frequently encounter systemic barriers including racial discrimination, mistrust of health care providers, limited culturally competent care, and socioeconomic inequalities, significantly impacting their engagement in preventive and self-care behaviors (Griffith et al., 2024; Williams et al., 2023). Hispanic men face additional challenges, such as language barriers, immigration-related stress, and cultural expectations regarding masculinity that may limit their use of health services and self-management practices (Sherman et al., 2021). Furthermore, masculinity norms often discourage men from seeking medical advice, thereby increasing their vulnerability to adverse chronic disease outcomes (Smith et al., 2018; Zwolinsky et al., 2016). Given these multifaceted barriers, there is a critical need to better understand the intersection of situational awareness (i.e., an individual’s daily ability to recognize opportunities for health-promoting decisions) and the gap between this awareness and actual health behaviors (i.e., the “self-care gap”). Therefore, efforts are needed to identify the drivers of situational awareness for health and understand the factors driving healthful inaction (despite the individual knowing that the healthful option is present).
This study aims to identify (1) levels of situational awareness for healthful behaviors; (2) gaps between situational awareness and actual healthful actions geared toward self-care; and (3) factors associated with wider self-care gaps by race and ethnicity among a sample of non-Hispanic Black and Hispanic men with chronic conditions. The current study is conceptually guided by Situated Cognition Theory, which asserts that real-world behaviors are best understood within the specific contexts and situations in which they naturally occur. According to this theory, cognition is inherently context-bound, meaning that individual actions and decisions are influenced by personal mental processes and significantly shaped by social interactions, cultural expectations, and the immediate physical environment (Choi & Hannafin, 1995; Korthagen, 2010). Lave and Wenger (1991) describe situated cognition as a generative social process in the lived-in world (Lave & Wenger, 1991). Applying this framework to our study helps clarify why situational awareness (i.e., recognizing opportunities to engage in self-care) is influenced by daily lived contexts and social-cultural environments. It also can explain the need for culturally and socially relevant interventions, designed explicitly around the daily realities and lived experiences of non-Hispanic Black and Hispanic men (Choi & Hannafin, 1995; Korthagen, 2010; Lave & Wenger, 1991).
Methods
Sample and Procedures
Data collection utilized a Qualtrics web-based panel, employing an internet-delivered questionnaire incorporating validated scales. The survey aimed to investigate the interrelationships among health status, preventive health behaviors, and health service utilization in Black and Hispanic men aged 40 years and older with chronic conditions (Smith et al., 2022). Qualtrics web-based panels, characterized by opt-in participation, offered access to pre-identified research participants with specific demographic characteristics. Recruitment and compensation were managed by Qualtrics. Upon recruitment through Qualtrics, potential participants were provided with a brief study description and information sheet (which required acknowledgment) prior to being able to access the survey. A total of 2,028 eligible men completed the online questionnaire. Additional details about the survey content and methodology have been previously reported (Kew et al., 2023; Merianos et al., 2023; Oloruntoba et al., 2024; Sherman et al., 2021, 2023; Smith et al., 2022). Institutional Review Board approval was obtained. Prior to analyses, further exclusion criteria were applied; men who self-reported being both non-Hispanic Black and Hispanic (n = 47) and men with missing data pertaining to lifestyle behaviors (n = 36) were omitted. Further, men without insurance were intentionally removed from analyses to alleviate biases associated with health care access and health provider interaction variables of interest (n = 184). All 1,761 men reported their situational awareness regarding health-related decisions. To examine the “self-care gap,” men (n = 199) who reported not recognizing any daily situations to act in their best health interest were omitted. The resulting analytic sub-set comprised 1,562 non-Hispanic Black and Hispanic men aged 40 years and older with chronic conditions.
Measures
Dependent Variables
This two-stage study had two dependent variables. First,
Chronic Disease Profile and Symptomatology
Chronic conditions were evaluated using a detailed self-reported checklist comprising 18 chronic physical and mental health conditions, including asthma/emphysema/chronic breathing or lung problems, arthritis/rheumatic disease, cancer or cancer survivorship, chronic pain, diabetes, heart disease, high cholesterol, hypertension, kidney disease, memory problems, obesity, osteoporosis, obstructive sleep apnea, schizophrenia or other psychotic disorders, stroke, thyroid problems, urinary incontinence, and other unlisted chronic conditions. Participants were instructed to select the conditions applicable to them from the list provided. The endorsed items were then combined to calculate a composite score representing the total number of chronic conditions experienced by each participant, with scores ranging from 1 to 18.
Current depressive symptomatology was assessed using the Patient Health Questionnaire–2 (PHQ-2), consisting of two questions regarding feelings of depression and interest in usual activities (Kroenke et al., 2003). Response options for each item ranged from “never” (scored 0) to “nearly every day” (scored 3), with summed scores ranging from 0 to 6. This variable was dichotomized, with scores of 3 or higher indicating the presence of depression (Kroenke et al., 2003).
Participants assessed the severity of the following symptoms using a scale spanning from 0 to 10: fatigue, pain, stress, and sleep (Smith et al., 2022). Within this scale, participants indicated their level of concern or problem, with 0 representing “no problem/concern” and 10 indicating “major problem/concern.”
Prevention Screenings and Activities
Participants were asked to report their engagement with eight recommended health practices. Participants reported if they received the following in the past year (coded “yes” or “no”): routine check-up with a physician; flu vaccination; blood cholesterol test; blood sugar tests; colon cancer screening; eye examination; and dental check-up (Centers for Disease Control and Prevention [CDC], 2020). Respondents were also asked to report if they ever received a prostate-specific antigen (PSA) test (coded “yes” or “no”). Then, the number of prevention screenings and activities was calculated by summing the number of recommended health practices in which men engaged (range = 0–8).
Health Behaviors
Participants were asked to report their physical activity, alcohol consumption, and tobacco and cannabis use (Smith et al., 2022). These variables were each dichotomized into “yes” and “no” responses based on whether the participant met recommended guidelines for weekly physical activity (i.e., weekly over 150 minutes of moderate-to-vigorous activity [U.S. Department of Health and Human Services, 2018]), engaged in problem drinking (i.e., consuming 14 + alcoholic drinks per week), used any tobacco product in the past 30 days, and used cannabis in the past 30 days (Rolle-Lake & Robbins, 2020).
Health-Related Perceptions
The
The
A single-item measure assessed participants’
Participants’ overall
The frequency of participants’
Sociodemographic Factors
Sociodemographic variables in this study included age (range = 40–93 years), race and ethnicity (classified as non-Hispanic Black or Hispanic), educational attainment (scored as: 1 = Less than high school, 2 = High school graduate, 3 = Some college, 4 = 2-year degree, 5 = 4-year degree, 6 = Professional degree, and 7 = Doctorate), partner status (differentiated between married/partnered individuals and those who were never married, divorced, separated, or widowed), and annual household income (reported in approximately $10,000 USD increments).
Data Analysis
All statistical analyses in this study were analyzed by using SPSS version 28 (Statistics, 2021). Descriptive statistics were computed to summarize the characteristics of the participants. Sample characteristics were compared across race and ethnicity using independent sample t-tests for continuous and count variables and chi-square tests for categorical variables. An ordinary least squares (OLS) regression model was fitted to identify factors associated with higher situational awareness (i.e., the number of times daily that men recognized situations to make choices to act in their best health interest). Then, after omitting men with no reported situated awareness, an OLS regression model was fitted to identify factors associated with wider “self-care gaps” (i.e., the number of times daily that men recognized situations to act in their best health interest, but they did not do so). Statistical significance for all analyses was set at p < .05.
Results
In Table 1, the sample characteristics of the 1,761 male individuals aged 40 years and older are presented by race and ethnicity. Among these men, 58.4% identified as non-Hispanic Black, and 41.6% identified as Hispanic. The mean age of the participants was 57.31 years (±9.97), ranging from 40 to 93 years. Most participants had achieved a college degree or higher, 53.5% were married/partnered and had average annual household incomes of approximately $62,000 (±$34,000). On average, participants reported 4.01 chronic conditions (±2.90). Clinical depression was reported by 23.2% of the participants. Large proportions of men reported receiving routine check-ups (87.8%), blood cholesterol tests (78.7%), blood sugar tests (74.0%), PSA tests (57.8%), eye exams (60.8%), and dental exams (56.4%). Smaller proportions reported getting flu vaccines (43.3%) and colon cancer tests (32.2%). About two-thirds of participants (75.2%) did not meet the recommended guidelines for general physical activity, with smaller proportions reporting problem drinking (10.7%), using tobacco (34.2%), and using cannabis (20.2%). Participants reported an average of 4.30 (±3.16) situations per day they were aware of situations they had the choice to act in their best health interest. Of those who recognized one or more situations daily (n = 1,562), participants reported an average of 2.99 (±2.81) situations in which they knew they had a choice but did not act in the best health interest.
Sample Characteristics by Race and Ethnicity
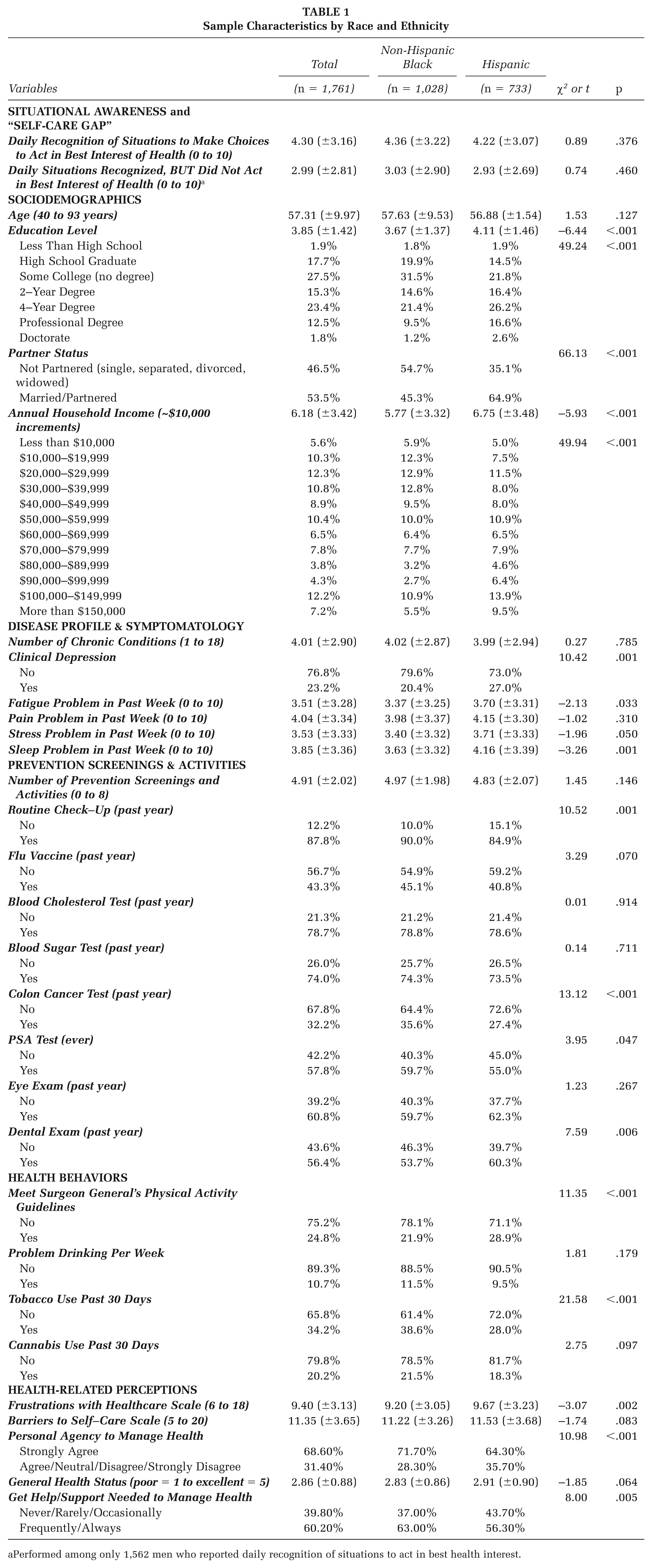
Performed among only 1,562 men who reported daily recognition of situations to act in best health interest.
When comparing sample characteristics by race and ethnicity, Hispanic participants reported higher educational achievement (t = −6.44, p < .001) and higher annual household incomes (t = −5.93, p < .001) compared with their non-Hispanic Black counterparts. Relative to non-Hispanic Black participants, significantly larger proportions of Hispanic men were married/partnered (χ2 = 66.13, p < .001) and reported depressive symptomatology (χ2 = 10.42, p = .001). On average, Hispanic men reported more fatigue (t = −2.13, p = .033) and sleep (t = −3.26, p = .001) problems in the past week. Compared with Hispanic men, significantly larger proportions of non-Hispanic Black men reported routine check-ups (χ2 = 10.52, p = .001) and colon cancer tests (χ2 = 13.12, p < .001), yet a significantly smaller proportion of non-Hispanic Black men reported dental exams in the past year (χ2 = 7.59, p = .006). A significantly larger proportion of Hispanic men reported meeting physical activity guidelines (χ2 = 11.35, p < .001), whereas a significantly larger proportion of non-Hispanic Black men reported using tobacco in the past 30 days (χ2 = 21.58, p < .001). On average, Hispanic men reported higher health care frustrations compared with non-Hispanic Black men (t = −3.07, p = .002). Significantly larger proportions of Hispanic men reported worse personal agency to manage their health (χ2 = 10.98, p < .001), whereas a significantly larger proportion of non-Hispanic Black men reported getting the help and support needed to manage their health (χ2 = 8.00, p = .005).
Table 2 reports findings from the two OLS regression models. In the model including all men (n = 1,761), age was negatively associated with men recognizing more daily situations to make choices to act in their best health interests (B = −.03, p < .001). Fatigue problems (B = .11, p = .002) and stress problems (B = .07, p = .032) were positively associated with men recognizing more daily situations to make choices to act in their best health interests, respectively. Reporting more barriers to self-care was positively associated with men recognizing more daily situations to make choices to act in their best health interests (B = .05, p = .047). Engaging in more preventive screening and activities (B = .13, p = .001), meeting physical activity guidelines (B = .36, p = .044), reporting better general health status (B = .20, p = .037), and reporting getting more frequent help and support to manage health (B = .89, p < .001) were positively associated with men recognizing more daily situations to make choices to act in their best health interests, respectively.
Linear Regression Models
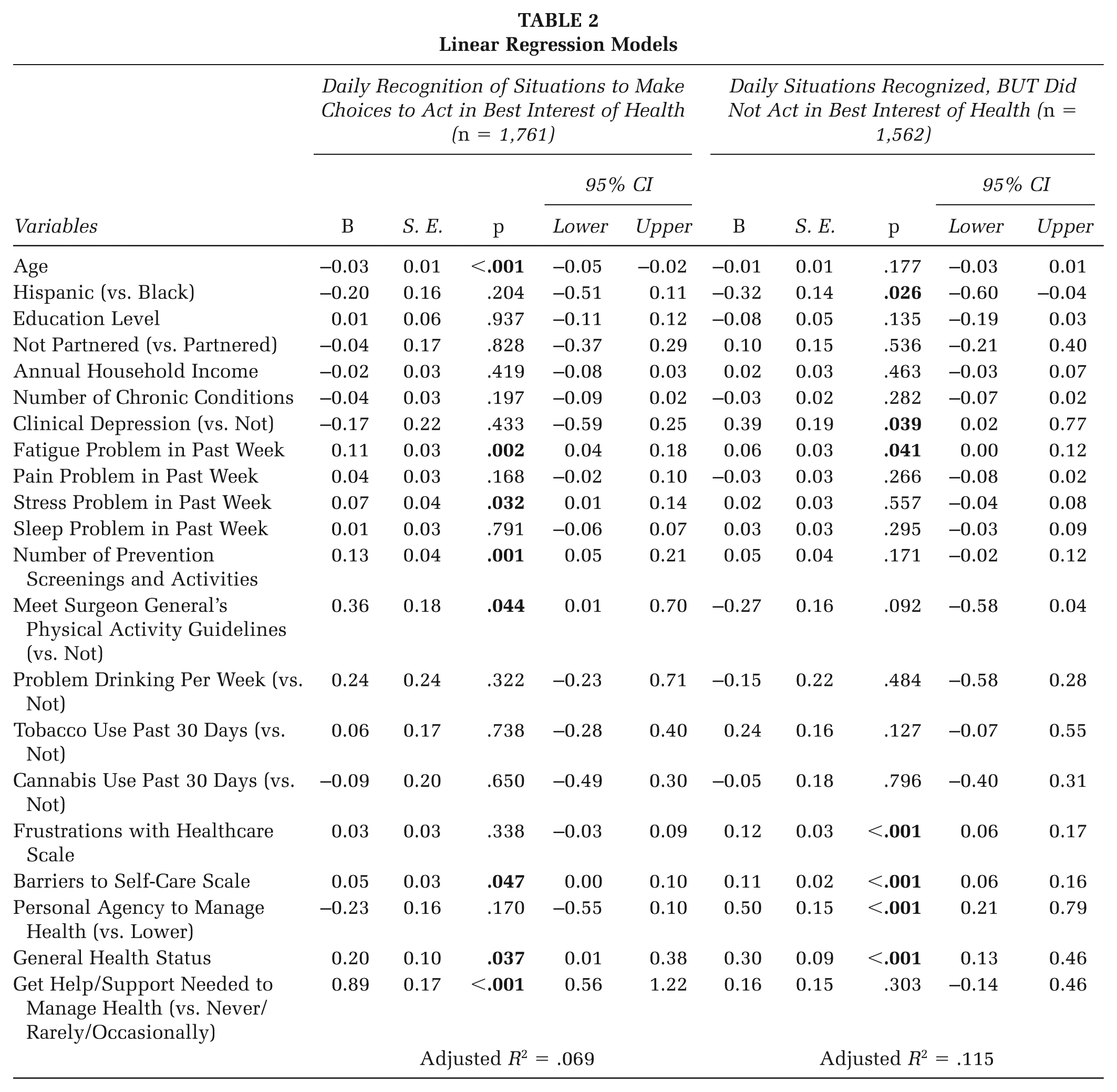
In the model including only men who reported at least one instance of daily situational awareness (n = 1,562), Hispanic men (B = −.32, p = .026) reported a narrower “self-care gap” (i.e., recognizing daily situations to act in their best health interest, but not doing so). Reporting clinical depression (B = .39, p = .039), fatigue problems (B = .06, p < .041), frustrations with health care (B = .12, p < .001), and barriers to self-care (B = .11, p < .001) were positively associated with greater “self-care gaps,” respectively. Conversely, reporting strongest personal agency for managing health (B = .50, p < .001) and better general health (B = .30, p < .001) were positively associated with greater “self-care gaps.”
Discussion
This study examined factors associated with situational awareness for healthful behaviors and the self-care gap among non-Hispanic Black and Hispanic men with chronic conditions. In general, younger men were more likely to recognize situations requiring healthy choices. Previous research has highlighted age-related differences in awareness of lifestyle factors that affect chronic diseases (Okobi et al., 2023). This suggests that younger men may be more health conscious than older men. Their heightened situational awareness may also be attributed to their greater participation in the labor force, where they could possibly be exposed to workplace health promotion programs. Younger men tend to use technology more frequently (Bünning et al., 2023; Chidiac et al., 2022) and have better access to health information (Gandrakota et al., 2021; Onyeaka et al., 2021), further enhancing their situational awareness.
Our findings suggest that men who reported higher levels of fatigue and stress also noted an increase in situational awareness. Fatigue and stress are interrelated concepts, with fatigue sometimes considered a type of physical stress (Kocalevent et al., 2011). While some studies suggest that acute stress can enhance general alertness (Qi & Gao, 2020), potentially leading to improved situational awareness among men, most of the literature contradicts this finding. Both fatigue and stress are typically associated with reduced cognitive functioning, including diminished situational awareness (Ibrahim et al., 2023; Valent et al., 2016). Zhou and colleagues push this reflection further by examining the three levels of situational awareness and proposing that perception may not be affected by fatigue (Zhou et al., 2023), but comprehension and projection of future events might be.
In the current study, men who reported better overall health, engaged in more preventive screenings, and met physical activity guidelines demonstrated higher situational awareness. Research indicates that individuals with better health status tend to have better cognitive function (Caserta & Abrams, 2007), which contributes to situational awareness. Those who maintain good health are also more likely to be proactive about their health, more aware of health-promoting environments, and participate in health screenings (Teo et al., 2016). Identifying more barriers to self-care and receiving help and support needed to manage their health conditions were associated with more recognition of situations to make choices to act in the best interest of their health. Men with self-care difficulties or who rely on others may already be more conscious of their health needs, which could easily be extended to being more aware of their environments.
Men who reported clinical depression and higher levels of fatigue were not likely to act in the best interest of their health, despite their situational awareness. Clinical depression significantly impacts daily functioning and an individual’s ability to take care of themselves (Hindmarch et al., 2013; Lawlor et al., 2020). Symptoms such as fatigue—a common symptom of depression—lack of energy, and difficulty making decisions can hinder an individual’s ability to act on their awareness (Abuse & Administration, 2016; National Institute of Mental Health, 2024). This finding is consistent with previous research showing that depression is associated with decreased self-care behaviors, including medication adherence, healthy diet, and physical activity (Egede et al., 2009; Stamoulis et al., 2024). Poor self-care can also exacerbate depressive symptoms, further reducing the likelihood of engaging in healthy behaviors. Effective treatment of depression using a combination of psychotherapy and medication (Simon et al., 2024) and fatigue management would be essential to support non-Hispanic Black and Hispanic men with chronic conditions to engage in self-care activities.
The strength of this study lies in its examination of the self-care gap. Results indicate that non-Hispanic Black men experience a larger self-care gap compared with their Hispanic counterparts. Although non-Hispanic Black men with chronic conditions recognized opportunities to engage in healthful behaviors, they were less likely to act on this situational awareness and perform self-care activities. Compared with Hispanic individuals, Black individuals face additional barriers, such as perceived race- and insurance-based discrimination (Walker et al., 2016; Williams et al., 2023), which can result in reduced access to care and fewer opportunities for self-care activities (e.g., attending medical check-ups; taking medication). Considering these differences, further examination is needed to assess the cultural and environmental influences of the self-care gap among non-Hispanic Black men in the United States. Targeted interventions at the micro, meso, and macro levels are needed to address specific barriers faced by non-Hispanic Black men with chronic conditions to encourage self-care. As examples (Boyd et al., 2023), at the micro level, health care providers could implement culturally tailored health education programs that address the unique needs and perspectives of non-Hispanic Black men, incorporating elements of their cultural beliefs and practices into self-care recommendations. At the meso level, community-based organizations could establish peer support groups or mentorship programs specifically for non-Hispanic Black men with chronic conditions, fostering a sense of community and shared experience in managing health. These programs could also involve family members to strengthen social support networks. At the macro level, policymakers could work to address systemic barriers by implementing policies such as expanding Medicaid coverage or incentivizing health care providers to practice in underserved areas.
The self-care gap identified among non-Hispanic Black and Hispanic men who reported better general health highlights an unexpected finding. While this association may seem counterintuitive, it may be explained by masculine norms emphasizing toughness, self-reliance, and risk-taking behaviors such as alcohol consumption (Zwolinsky et al., 2016). Thus, tailoring interventions and framing public health awareness campaigns with culturally meaningful messages specifically for men who perceive their health positively could effectively bridge the self-care gap between awareness and actual performance of health-promoting behaviors (Griffith et al., 2024). For example, framing self-care behaviors as ways to maintain strength and independence could align with masculine ideals while promoting health. Community-based interventions could leverage existing social networks, such as sports teams or faith-based organizations, to promote health awareness in familiar, comfortable contexts. Workplace wellness programs could be designed to offer health screenings and education, emphasizing the importance of maintaining health for career success and family responsibilities (Haynes et al., 2022).
Men did not engage in healthful behaviors when they faced more barriers to self-care, weaker personal agency, and increased health care frustrations. Barriers to self-care can lead to feelings of being overwhelmed, distressed, and powerless (Konlan & Shin, 2023; Yu et al., 2008), which can reduce motivation to adopt healthier habits. Men with weaker personal agency may also experience feelings of helplessness (Shankar et al., 2019); this can result in an over-reliance on others for health-related decisions and actions, leaving them vulnerable when support is not available. Finally, frustrations with the health care system can lead to dissatisfaction and avoidance of medical encounters (Smith, Bergeron, Adler, et al., 2017), medication nonadherence (Konstantinou et al., 2020), and overall difficulty in effectively managing chronic conditions (Smith, Bergeron, Riggle, et al., 2017).
Our study advances literature by specifically measuring the “self-care gap.” This measurement uniquely captured the disconnect between recognizing health-promoting situations and actual engagement in healthful behaviors among non-Hispanic Black and Hispanic men with chronic conditions. The significance of this approach—examining both situational awareness and the self-care gap—lies in its potential to inform focused interventions addressing cognitive and behavioral barriers simultaneously. Unlike previous studies focusing solely on barriers or outcomes, this research integrates both awareness and action components within the same framework. Moreover, programs should aim to enhance recognition of health-promoting opportunities while simultaneously supporting the actions that follow this recognition (e.g., culturally tailored behavioral interventions addressing practical barriers like access or stigma reduction). Further, the use of a large, diverse sample of underrepresented minority groups, coupled with comprehensive psychosocial, behavioral, and systemic measures, allowed for a multidimensional understanding of the determinants influencing health behaviors. This approach provides actionable insights on intervention design highlighting the need for support establishing a foundation for reducing persistent health disparities in chronic disease management among minoritized populations.
Implications for Practice
Addressing the self-care gap among non-Hispanic Black and Hispanic men with chronic conditions requires a multifaceted approach that considers individual, social, and systemic factors. At the individual level, enhancing health literacy, self-efficacy, and mental health support is pivotal. For example, culturally sensitive cognitive-behavioral interventions effectively address mental health barriers such as depression and chronic fatigue, which improve self-care practices (Simon et al., 2024; Stamoulis et al., 2024). This could involve culturally tailored education programs and cognitive-behavioral interventions to help men overcome barriers to self-care. At the social level, efforts should be made to leverage existing support networks and challenge harmful masculine norms that discourage help-seeking behaviors. Community-based peer-support initiatives can provide social reinforcement for positive health behaviors, thus reducing stigma around help-seeking among men (Griffith et al., 2024; Haynes et al., 2022). At the systemic level, enhancing health care provider training in cultural competence and expanding access through policy changes, such as increased Medicaid coverage and health care incentives in underserved communities, are crucial for bridging health disparities (Boyd et al., 2023; Walker et al., 2016). In addition, digital health solutions, including mobile apps and telemedicine services tailored to non-Hispanic Black and Hispanic communities, can offer accessible and personalized support, effectively bridging the gap between awareness and health-promoting actions (Gandrakota et al., 2021; Sherman et al., 2021).
Public health approaches that incorporate situational awareness principles can enhance surveillance, epidemiology, and preparedness capabilities. Policies that promote a holistic approach addressing both physical and cognitive aspects of health may lower the burden on health care systems by reducing the incidence and severity of chronic illnesses. Such integrated strategies represent a sustainable path toward achieving broad-scale improvements in population health outcomes. By recognizing and leveraging the connection between situational awareness and health behaviors, policymakers can design more effective interventions that simultaneously enhance cognitive functioning, encourage preventive health practices, and create resilient health care systems capable of addressing both current and emerging public health challenges.
Limitations
The study findings should be interpreted in consideration of the following limitations. The study relied on a self-reported, cross-sectional survey. This methodology is subject to potential biases such as social desirability and recall bias and limits the ability to establish causal relationships. Participant recruitment and data collection using a Qualtrics panel may have biased the sample in that participants were required to have internet access and be able to read English, which may have excluded certain less affluent men or those experiencing the “digital divide.” Although the study aims focused on non-Hispanic Black and Hispanic men, not collecting data from women or men of other races and ethnicities limited our ability to make broader comparisons by gender, race, and ethnicity. The broad concepts of situated awareness and self-care gap could have benefited from more precise measurement techniques. The ecological momentary assessment (EMA) methods could have captured more nuanced, objective, and context-specific information in real-time (Price et al., 2016). Other study variables could have also benefited from clearer definitions (e.g., acute or chronic stress, physical or cognitive fatigue). Future research on situational awareness and the self-care gap among non-Hispanic Black and Hispanic men with chronic conditions should consider using longitudinal designs, more objective measures, and incorporating real-time data to enhance the validity and reliability of the findings.
Conclusion
This study highlights the need to enhance situational awareness and bridge the self-care gap among non-Hispanic Black and Hispanic men with chronic conditions. Men’s recognition of healthful opportunities was largely driven by their disease symptomatology, greater engagement in preventive screenings, and social support. However, the self-care gap was seemingly driven by mental health and challenges with disease self-management and health care interactions. By identifying these barriers and addressing them at multiple levels across the socioecological model, better support can be provided to these men in translating their situational awareness into effective self-care practices, ultimately leading to improved overall health outcomes.
Footnotes
Authors’ Note:
This work was supported by Texas A&M University through their Texas A&M Triads for Transformation (T3) initiative.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved for a waiver by the Institutional Review Board at relevant University (IRB ID: 2018-1684).
Consent to Participate
Informed consent was obtained from all potential participants prior to being able to access the survey.