
Abstract
Black men in the United States have a lower life expectancy than Hispanic and White populations due to elevated morbidity and mortality from various health conditions. This is partially attributable to the experience of systemic racism and earned mistrust toward health professionals, the majority of whom are not Black. Despite recognition of this issue, limited progress has been made to improve Black men’s health trajectories. Thus, there is an urgent need for health care organizations to reach more Black men and address existing health inequities through innovative means. Larry Wallace Sr., an experienced health care executive, recognized this issue in his community and created the Black Men’s Health Clinic (BMHC) with his son, Larry Wallace Jr., to improve health care delivery to Black men in and around Austin, Texas. BMHC has successfully reached Black men in its catchment area through its strategic community engagement efforts and a unique financial model to increase health care accessibility for a population that has historically experienced poor health outcomes. Furthermore, they offer a comprehensive range of services that acknowledge the impact of social and structural determinants of health and address social needs to provide Black men with access to vetted, high-quality health care. Consequently, BMHC’s health care model offers a useful framework for other health care organizations that are aiming to achieve health equity. The BMHC model is presented herein, highlighting strategies for other health care organizations to reach Black men and deliver trusted care. Implementing suggestions discussed in this work may lead to improved health outcomes for Black men in the United States.
In the United States, Black men bear a disproportionate disease burden based on premature morbidity and mortality rates. Life expectancy for White men, Hispanic men, and even Black women are all 75 years or greater, whereas Black men are expected to only live to 68 years (Arias et al., 2021). Myriad pathologies underlie this disparate mortality. Among them is that Black men are more likely to die from heart diseases and cancer than Black women or White men (Giaquinto et al., 2022). Among Black men aged 20 years and above, 58.4% have hypertension, a higher proportion than Black women or White, Asian, or Hispanic men (National Center for Health Statistics, 2021). Furthermore, compared to Black women and White men, Black men are more likely to be diagnosed with diabetes (Office of Minority Health, 2022).
Many of these health inequities are driven by disparities in social and structural determinants of health experienced by historically marginalized Black communities in the United States, such as higher uninsurance rates, lower incomes, and less education—all of which are associated with less accessibility to quality health care (Carter et al., 2024). Meanwhile, the same Black communities are situated in food deserts frequently overrun with stores peddling alcohol, tobacco products, and calorie-dense food, facilitating access to and the salience of products that damage their health (Wallace et al., 2021). Among Black adults who can access health care, many are reluctant to do so due to earned medical mistrust. This reluctance, albeit understandably rooted in past and present experiences of systemic racism (Nuriddin et al., 2020), jeopardizes the health of Black individuals. This reluctance may also be exacerbated among Black men due to masculine notions of self-reliance (Griffith et al., 2012).
With these barriers in mind, the Black Men’s Health Clinic (BMHC) was launched in May 2022 and is changing the way that Black men in and near Austin/Travis County, the fifth most populous county in Texas, interact with the city’s health care resources. BMHC was formed by Larry Wallace Sr., a retired health care executive with more than 35 years of experience in health care administration. BMHC’s strategic efforts are substantially overseen by his son, Dr. Larry Wallace Jr., former mayor of nearby Manor, Texas. Although there has been limited focus on understanding why Black men (rather than on all men or all Black adults) experience poorer health outcomes (Jack & Griffith, 2013), Wallace Sr. noticed throughout his career that the health care system and conventional health promotion campaigns failed to reach Black men. Rather than resigning to the intractability of the problem, he founded BMHC as part of the solution. Unlike health care organizations that acknowledge disparities affecting Black men but provide race- and sex-neutral programs and policies, BMHC is intentionally unapologetic in its focus on Black men because it aims to be a place where Black men consider their health care home. However, BMHC will never deny patient services or assistance based on race/ethnicity.
BMHC is largely a personal health care navigator, leveraging partnerships to innovate both service delivery and outreach/engagement. Its approach to health care stands out as a “jack-of-all-trades,” transcending limitations often found in clinics specializing in specific areas. The clinic’s service delivery efforts have evolved over time (Figure 1) into the comprehensive care model it is today (Figure 2). BMHC considers social determinants of health in all aspects of its operation, providing physical and mental health services alongside financial support for those who need it while leveraging innovative community engagement strategies to connect with Black men that traditional U.S. health care organizations struggle to reach.

BMHC Key Milestones
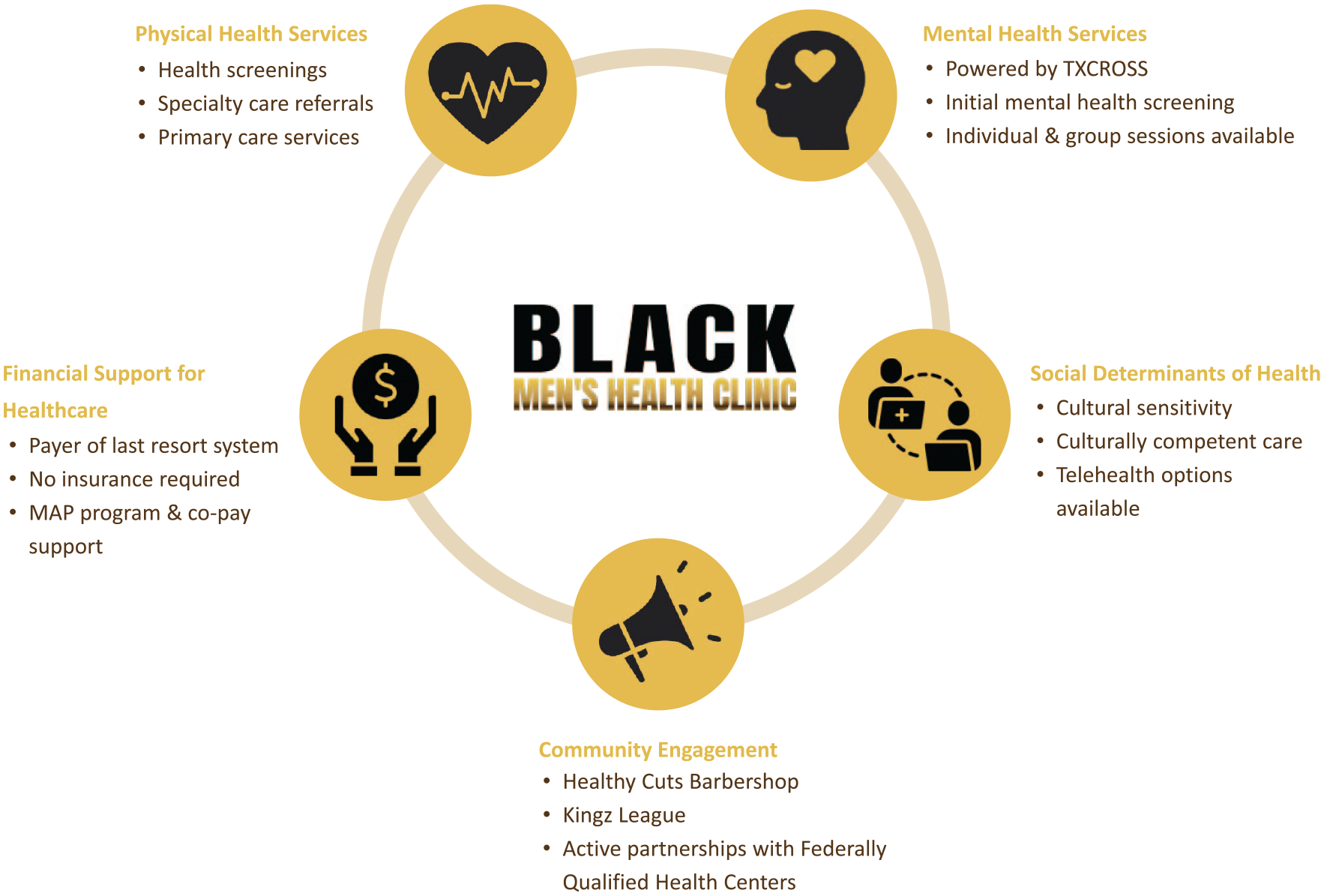
BMHC Comprehensive Care Model
Physical Health Services
Each patient’s relationship with BMHC begins with a health screening, after which a personalized health care action plan is constructed. BMHC partners with CommUnityCare™, the second largest community health center system in Texas, to offer primary care services (e.g., physical exams, immunizations, nutritional counseling, and chronic illness management) and specialty care referrals out of BMHC’s brick-and-mortar location. Sickle cell trait testing and blood pressure, cholesterol, and diabetes management are offered by other partners, such as Austin Public Health, and BMHC will help the patient connect with services, make an appointment, and so on. Aware that 17.7% of Black men smoke cigarettes (National Center for Health Statistics, 2023), BMHC is partnering with Taking Texas Tobacco Free—a program based at The University of Texas MD Anderson Cancer Center—to design and acquire culturally appropriate print materials that encourage tobacco cessation. The clinic is also partnering with the American Heart Association to implement an annual skill assessment designed to ensure that blood pressure measurements are consistently being taken accurately. In addition to specialist referrals offered by CommUnityCare™, BMHC staff work with patients to identify more appropriate providers if they feel an existing one is unsuitable. As with its patients, not all BMHC-affiliated providers are Black. If a patient is uncomfortable seeing a racially discordant doctor, however, BMHC will connect them with a concordant provider, even if that requires telehealth visits. Telehealth visits are also made available to patients who are unable to take time away from work to travel to health care appointments and may not have access to transportation.
Mental Health Services
BMHC’s mental health services are provided by various partners, such as Texas Christian Recovery and Other Support Services, an Austin-based counseling and education agency that operates from BMHC’s offices throughout the week. The first step is a mental health screening. Next, a personal care plan is developed and, if necessary, an appropriate ongoing provider is identified. Mindful of stigmas associated with mental health treatment, BMHC’s physical space, includes a private entrance that allows patients to enter the clinic and reach the counselor’s office inconspicuously. In addition to individual sessions, BMHC offers group sessions and healing circles for those patients who benefit from a sense of community. They also extend their support to military veterans by offering free access to resources, including online yoga classes.
Financial Support for Health care
Financial affordability is at the top of mind at BMHC. Health insurance is not required to receive care at BMHC, and patients with health insurance may be eligible for copay support. Central Health (where Wallace Sr. formerly served as Chief Operating Officer [COO] and Interim Chief Executive Officer [CEO]) administers the Medical Access Program (MAP), which serves as a health coverage program for uninsured, low-income residents of Travis County, Texas. Ordinarily, MAP only covers services if patients are enrolled in the program prior to the appointment being scheduled. BMHC, realizing the danger of turning away a patient who is prepared to make a health care appointment, negotiated an exemption whereby MAP will cover the cost of services even if the patient was not enrolled at the time the appointment was scheduled. Other efforts to increase health care affordability have included the adoption of an innovative financial model that deviates from the common sliding fee scale. BMHC has a payer-of-last-resort system. This is designed to ensure that health care remains accessible by covering the gaps that insurance fails to pay, thereby removing financial barriers that often hinder access to health care services. Finally, BMHC’s collaboration with Federally Qualified Health Centers also helps expand its reach in socioeconomic terms and enhances its health care provision capabilities. Its approach is particularly relevant in its community where a substantial portion of the population, 47.8% of BMHC patients, have incomes that are at or below the federal poverty level and may not otherwise be able to afford health care.
Community Engagement
BMHC’s community outreach and engagement initiatives, led by Cameron Morgan, are broad in their settings but remain narrowly tailored to reach Black men. BMHC’s Healthy Cuts is a grant-funded initiative that engages potential patients in a place that is brimming with trust: the Black barbershop. Barbers are trained to administer non-intrusive wellness checks and to encourage patrons to seek routine health care, including at BMHC. Patrons are granted a US$25 credit toward their next haircut if they make and attend an appointment at BMHC. They have also partnered with Kingz Social League, a local, predominantly Black adult basketball league that is a place where men can let their guard down to enjoy recreation. BMHC is a league sponsor and offers onsite blood pressure and blood sugar screenings to both players and spectators, who can schedule an appointment with BMHC on the spot. Looking toward the future, BMHC plans to extend engagement with the league to provide pre-participation physical evaluations to each player. Not only could health risks be proactively identified and addressed but all players would be encouraged to establish ongoing relationships with BMHC. Morgan also reached out to the local school district to expand BMHC’s community outreach after he recognized the significant amount of time spectators spent staring at the jumbotron during youth sports games. Consequently, BMHC is now the first health care organization to advertise its services on the jumbotron during youth football games, with future aims to expand this marketing campaign to basketball games.
Finally, the role of volunteerism and community upliftment in BMHC’s operational model cannot be overstated. Through its robust volunteer programs, BMHC enables community members to play a direct role in reducing health disparities. This strategy fosters a strong sense of community ownership and participation in health initiatives, creating a sustainable model for community health. More information can be found at https://blackmenshealthclinic.org/.
BMHC’s Impact
In a year, BMHC served 428 unique clients, with more than 85% being Black. Moreover, BMHC facilitated numerous services, including 63 new MAP enrollments, 59 food boxes, and 3,800 hot meal boxes, and was the payer-of-last-resort assistance for 6 patients. They also provided transportation assistance for 249 individuals, made 27 mental health referrals, coordinated with 17 health specialists, and made 770 physical and health screening appointments through its holistic approach. By leaving the clinic to engage Black men outside of the institutions that have historically perpetrated medical racism in favor of spaces where trust and comfort have been established and building a track record of addressing their physical health, mental health, and social determinants of health, BMHC is innovating the way that Austin’s health care resources approach and treat Black men to address health inequities.
Implications for Public Health Practice
BMHC has developed an effective health care model for reaching Black men, a population that is adversely affected by numerous health inequities. From sponsoring local sports teams to developing strategic partnerships with research organizations at prestigious institutions, BMHC has successfully expanded its reach of Black men in its catchment area and maintained high-quality care through its comprehensive approach. Consequently, BMHC’s model offers valuable insights to other health care organizations that have struggled to reach underserved populations but aim to address pervasive health inequities within their own communities.
Offering comprehensive care that is tailored to patients they serve is an integral part of BMHC’s health care model. Health care organizations dedicated to addressing health inequities affecting Black men should not solely focus on physical health but also on addressing mental health and the adverse effects of social determinants of health that disproportionately affect this group. Furthermore, they should actively work to surmount barriers to health care, such as stigma and medical mistrust, by cultivating a culturally sensitive environment for Black men through sharing their narratives and navigating them to race-concordant providers. Providing telehealth services and discrete health care may also offer a more comfortable experience for patients.
BMHC goes beyond delivering quality health care; integrating itself within the community it serves is essential to its success. Health care organizations looking to expand their reach to Black men within the community can follow in BMHC’s footsteps by reaching out to local organizations and Black-owned businesses that predominantly serve this group. Moreover, they should aim to develop sustainable partnerships by offering health care services to organization members and advertising the services they offer to the broader community.
Health care organizations bear an ethical responsibility to ensure the accessibility of their services to all, irrespective of racial/ethnic identity. It is not enough to recognize disparities; health care organizations must actively participate in dismantling barriers to access and trust that contribute to these inequities (Carter et al., 2024). Therefore, it is imperative that they take actionable steps that foster inclusivity. Employing practices that BMHC has already implemented in other health care settings holds the potential to enhance the accessibility of high-quality health care for Black men and pave the way for a healthier society as a whole.
Footnotes
Authors’ Note:
The Black Men’s Health Clinic is grateful for the support of its collaborators who enable their mission to be accomplished, including but not limited to the Austin Community Foundation, Austin ECHO, Austin Public Health, African American Youth Harvest Foundation, Bigger than Business City of Austin Office of Sustainability, Central Health, Charity Navigator, Hogg Foundation for Mental Health (2023 Healthy Minds recipient), Integral Care, Nextdoor Kind Foundation & NAACP, Shannon Jones, Sir Charles Media, St. David’s Foundation, Larry Wallace Sr. (BMHC Founder), Taking Texas Tobacco Free, and Wallace Brothers & Associates. To learn more about the BMHC, see their website at ![]() . Dr. Larry Wallace Jr. is a co-founder of BMHC and invested in its success; other authors declare no additional conflicts of interest, Work on this manuscript was supported by the National Institutes of Health/National Cancer Institute (award no. P30CA016672) and by The University of Texas MD Anderson Cancer Center through institutional funds for Dr. Lorraine Reitzel
. Dr. Larry Wallace Jr. is a co-founder of BMHC and invested in its success; other authors declare no additional conflicts of interest, Work on this manuscript was supported by the National Institutes of Health/National Cancer Institute (award no. P30CA016672) and by The University of Texas MD Anderson Cancer Center through institutional funds for Dr. Lorraine Reitzel