
Abstract
The Black Men’s Health Forum, a 6-week online health education intervention for African American men and accountability partners of African American men, was conducted to increase awareness of health issues that disproportionately affect African American men. In this article, we describe the intervention and report on the immediate benefits of the intervention, including changes in health knowledge and perception of research participation. Participants completed a pre-evaluation prior to participating in the forum and a post-evaluation after each session to capture data on sociodemographic information, medical history, health knowledge, and health behaviors. A total of 60 participants (30 African American men and 30 accountability partners) completed the forum. African American men had a mean age of 61.1 years while accountability partners had a mean age of 57.6 years. Overall health knowledge increased by 6.9 points for African American men and 2.8 points for accountability partners. Before the forum began, nine African American men reported ever participating in a research study. The proportion of African American men who reported that they would definitely participate in research in the next 12 months after participating in the forum increased by 40%. Through culturally tailored programming, the Black Men’s Health Forum increased access to health information as well as African American male medical professionals and health researchers for African American men in the community. Exposure to health information resulted in significant increases in health knowledge and willingness to participate in health research among African American men.
Introduction
Morbidity and mortality have improved across the United States (U.S.); however, African Americans (AAs), who only represent 13.7% of the U.S. population, are at an increased risk of death from all causes (Centers for Disease Control and Prevention [CDC], 2017; U.S. Census Bureau, 2021). Younger AAs are living with diseases commonly found among older populations, including high blood pressure, diabetes, and stroke (CDC, 2017). Within the AA population in the U.S., men experience a lower life expectancy than women. Compared with women and their male counterparts, non-Hispanic Black men have one of the lowest life expectancies in the U.S. At birth, non-Hispanic Black men are only expected to live to 68.3 years of age (Black women: 75.8 years; White women: 80.6 years; Hispanic women: 83.3 years; White men: 75.5 years; Hispanic men: 76.6 years; Arias, 2021). For AA men less than 45 years of age, premature mortality is largely due to homicide and unintentional injuries while AA men 45 years of age or older succumb to diseases such as heart disease and cancer (Center for Disease Control and Prevention, 2022). In addition, the COVID-19 pandemic had a negative impact on mortality among AA men, decreasing life expectancy by almost 4 years (Aburto et al., 2022). Despite poor health outcomes and life expectancies, health-insured AA men are 50% less likely to visit a physician (Hammond et al., 2011), and AA men are underrepresented in health research (U.S. Food and Drug Administration, 2020; Whyte, 2022). Barriers to engagement with medical institutions among AAs include socioeconomic status, cost, masculinity, racism, medical mistrust and distrust, lack of health awareness, cultural and linguistic differences, religious beliefs, and peer influences (Cheatham et al., 2008; Ravenell et al., 2008).
Community-based approaches have been proposed to improve health, health education, and engagement in health research. Through these approaches, community members are incorporated in the planning and implementation of health projects. Often, medical institutions and the community collaborate to meet people where they are in the community and bring health information and resources to communities in need. Examples of community-based interventions may include activities such as health programs, health fairs, and mobile clinics held in the community that focus on a population of interest. Communal spaces (e.g., community centers, churches, and other community spaces) versus health care settings may yield greater participant engagement (Okoro et al., 2020). Interdisciplinary stakeholders such as community members, faith-based leaders, policymakers, and health researchers may be involved in these health education efforts (Mitic, 2012). In addition, female peers and relatives may facilitate healthy behaviors among AA men. Women may positively impact health behaviors by influencing diet; monitoring health behaviors; providing motivation, support, and encouragement; and being a source for health information (Allen et al., 2013; Felder et al., 2019; Okoro et al., 2018, 2020). Previous community-based health education interventions have been successful in engaging AA men (Graham et al., 2018; Joseph et al., 2022; Okoro et al., 2020). A total of 245 men completed the Men of Color Health Awareness (MOCHA) project from 2011 to 2015, a project that aimed to improve men’s overall health, including physical, mental, emotional, and spiritual health (Graham et al., 2018). Similarly, Okoro et al. (2020) and Joseph et al. (2022) engaged 29 and 74 AA men, respectively, in health education intervention to address health disparities found among AA men. Not only were these interventions successful in engaging AA men in community settings, but the interventions also provided a health space for AA men, improved health knowledge, and increased access to health care.
Improving health knowledge and healthy behaviors within the AA community is a key aspect of achieving health equity, especially among subgroups who experience worse health challenges (Logan et al., 2015). AA men have some of the worst overall health outcomes for any race or gender and experience traumatic health outcomes across every domain of physical health (Gilbert et al., 2016). In this article, we describe a health education intervention tailored to AA men, the Black Men’s Health Forum, and report on the immediate benefits of the intervention, including changes in health knowledge and perception of research participation.
Method
The Black Men’s Health Forum
The Black Men’s Health Forum, a 6-week online health education intervention for AA men and accountability partners of AA men, was conducted by the Maya Angelou Center for Health Equity at Wake Forest University School of Medicine in April and May of 2022. An accountability partner was defined as a friend or relative who participated in the forum with the AA male and who could play a supportive role in improving their partner’s health. The purpose of this forum was to (1) increase knowledge and awareness of AA men’s health issues among AA men and accountability partners of AA men; (2) improve AA men’s attitudes, intentions, and behaviors toward improving overall health and seeking health-related information and resources; (3) improve AA men’s attitudes and intention to participate in health research; and (4) leverage family and friends in AA men’s lives to influence healthy behavioral changes among AA men.
The curriculum for the forum was developed based on the results of a community health assessment conducted among AA, male faith leaders in North Carolina. These leaders provided data on health topics of concern among AA men. The forum was culturally tailored for AA men by discussing health topics that disproportionately affect AA men, creating a health space just for AA men, and inviting AA male clinicians and researchers to engage with AA male attendees during forum sessions. Based on the needs of AA men in the Triad area of North Carolina, the following topics were selected for the forum: Black Men’s Health and Black Masculinity, Mental Health and Coping Strategies, Cancer, Sexual Health, Cardiovascular and Metabolic Health, and Brain Health and Healthy Aging. Each week, a health topic was presented to participants by an AA male researcher or physician with an emphasis on increasing health knowledge of medical issues that disproportionately affect AA men and health research participation. All sessions were facilitated by an AA male faith leader. Over 6 weeks, AA men synchronously attended virtual sessions each week, lasting 90 minutes each. An AA male expert in the selected topic area for the week gave a presentation for up to 60 minutes and participants were allowed to ask the speaker questions during the remainder of the session to further the discussion on the selected health topic for the week. Weekly sessions were recorded, and accountability partners viewed recordings of the sessions asynchronously. All identifying information of the men was removed from the recordings. Participants attended a total of six sessions and completed seven surveys via REDCap® (Research Electronic Data Capture), including a pre-evaluation prior to participating in the first session of the forum and a post-evaluation taken after each session (a total of 6). Informed consent for the study was obtained in a REDCap survey prior to completing the pre-evaluation for the forum. For participation in the forum, AA men received a $200 gift card for attending weekly sessions and completing pre- and post-evaluations. Accountability partners received a $125 gift card for participating in the forum asynchronously and completing pre- and post-evaluations. The compensation received by AA men in the study was slightly greater than that of accountability partners in the study to offset increased participant burden. AA men were asked to participate in the study synchronously and complete additional survey items. This study was approved by the Wake Forest University School of Medicine Institutional Review Board (IRB00063666).
Population
Recruitment followed a convenience sampling approach. Participants in the forum were recruited through a partnership between the Maya Angelou Center for Health Equity and the Triad Pastors Network, a network of community faith leaders. This partnership was created to establish or advance health ministries in churches, with a long-term goal of improving AA health. Members of the network distributed fliers to their congregations and referred community members to the study by word of mouth.
To participate in this forum, participants were required to enroll as a pair including a male who identified as AA and an accountability partner. Due to the influence of women on the health of AA men, the population of interest for the accountability partners were female relatives and peers; however, we understood that some men may not have a female accountability partner. Therefore, we did not exclude AA men from the forum who wanted to include a male as their accountability partner. In addition, participants were required to be 18 years of age or older, attend all six online sessions, and complete pre- and post-evaluations.
Measurements
Instruments were developed to measure changes in health attitude, knowledge, and health behaviors, to understand the impact of educational programming on willingness to engage in research, and to assess acceptability of the health education intervention. A conceptual framework integrating the knowledge, attitude, and practice (KAP) methodology was incorporated in the health education intervention through pre-evaluations and post-evaluations administered directly after the forum (knowledge) and 6 months following the forum (attitude and practice). This article describes immediate benefits of the forum, including changes in knowledge. According to a systematic review by Rav-Marathe and colleagues (2016), the KAP model has been extensively used in health education research as a guide to better comprehend how health education can influence behavioral change and health outcomes. Three constructs make up the components of the KAP model, namely, knowledge, attitude, and practice. Knowledge is defined as the “acquisition, retention, and use of information or skills.” Attitude is defined as “a psychological tendency that is expressed by evaluating a particular entity with some degree of favor or disfavor.” Attitude comprises cognition, affect, and behavior. Practice is defined as actions that may prevent or delay an unwanted outcome due to the attainment of knowledge and positive changes in attitude toward a health outcome. The KAP framework posits that health educational interventions enhance knowledge and attitude about health that leads to improved self-care practices (Rav-Marathe et al., 2016).
Pre- and post-evaluation instruments were designed based on questions from national and community health surveys as well as validated scales for health attitude and health behaviors (Balanzá-Martínez et al., 2021; Center for Behavioral Health Statistics and Quality, 2018; Cottler, McCloskey, et al., 2013; Cottler, Striley, et al., 2013; DuBenske et al., 2009; Hong, 2011; Kessler et al.,2002, 2003; Mincey et al., 2014; PhenX Toolkit, n.d.). Sociodemographic measures included age, race, ethnicity, sexual orientation, marital status, education, income, and employment. AA men were also asked to report data on their health, including self-reported health status, past 12-month physical exam, past 12-month dental exam, health insurance status, lifetime health conditions, family history of Alzheimer’s disease, psychological distress, and research participation. To assess health knowledge, the study team created questions based on the content of the speaker presentations. Furthermore, AA men were asked to report their top 3 health concerns, top 3 barriers to health care, and top neighborhood concern in open-ended questions. All developed instruments were designed and tested in the Research Electronic Data Capture (REDCap) system.
Data Analysis
Quantitative analyses were completed using SAS® software version 9.4. Descriptive statistics, including frequency and percentage, were conducted for sociodemographic characteristics of both men and accountability partners who participated in the study. Additional descriptive statistics on the medical history and perception and willingness to participate in health research was conducted among AA men in the study. To assess change in health knowledge, the number of correct responses for the overall assessment and for each health topic (Black Men’s Health and Black Masculinity, Mental Health and Coping Strategies, Cancer, Sexual Health, Cardiovascular and Metabolic Health, and Brain Health and Healthy Aging) were calculated for each participant in the pre- and post-evaluations. Participants could receive a maximum score of 30 for the full assessment and a total score of 5 for each health topic. Paired t tests were used to assess significant changes in health knowledge scores overall and by health topic as well as for trust in researchers and research.
Qualitative data in open-ended questions in the evaluations were quantified using categorical themes for AA men’s top health concerns, barriers to health care, and neighborhood concerns. Two members of the research team reviewed responses to the questions completed by the 30 men who completed the forum and organized the data into groups. Similar concerns were grouped in the same category. For example, “Mental,” “Mental Health,” and “PTSD/Vietnam Veteran” were categorized as Mental and Emotional Health. The frequency in which a respondent reported a concern for each category was documented.
Results
On average, approximately 36 AA men attended the sessions each week. To complete the forum, a pair of participants completed all six study sessions and all seven evaluations. A total of 88 participants (44 pairs) enrolled in the study and 60 non-Hispanic AAs (30 pairs; 30 AA men and 30 accountability partners) completed the forum (Table 1). Approximately 68% of participants were retained in the forum. AA men had a mean age of 61.1 years while accountability partners had a mean age of 57.6 years. Only two accountability partners reported being male; 93.3% of accountability partners reported being female. The majority of AA men and accountability partners were married. More than 50% of AA men and accountability partners had a bachelor’s degree or higher. About 53% of AA men and nearly 43% of accountability partners reported an income of $50,000 or higher. More AA men reported being retired (46.7%), and most accountability partners reported being employed full-time or part-time (70.0%).
Sociodemographic Summary of Participants in the Black Men’s Health Forum.
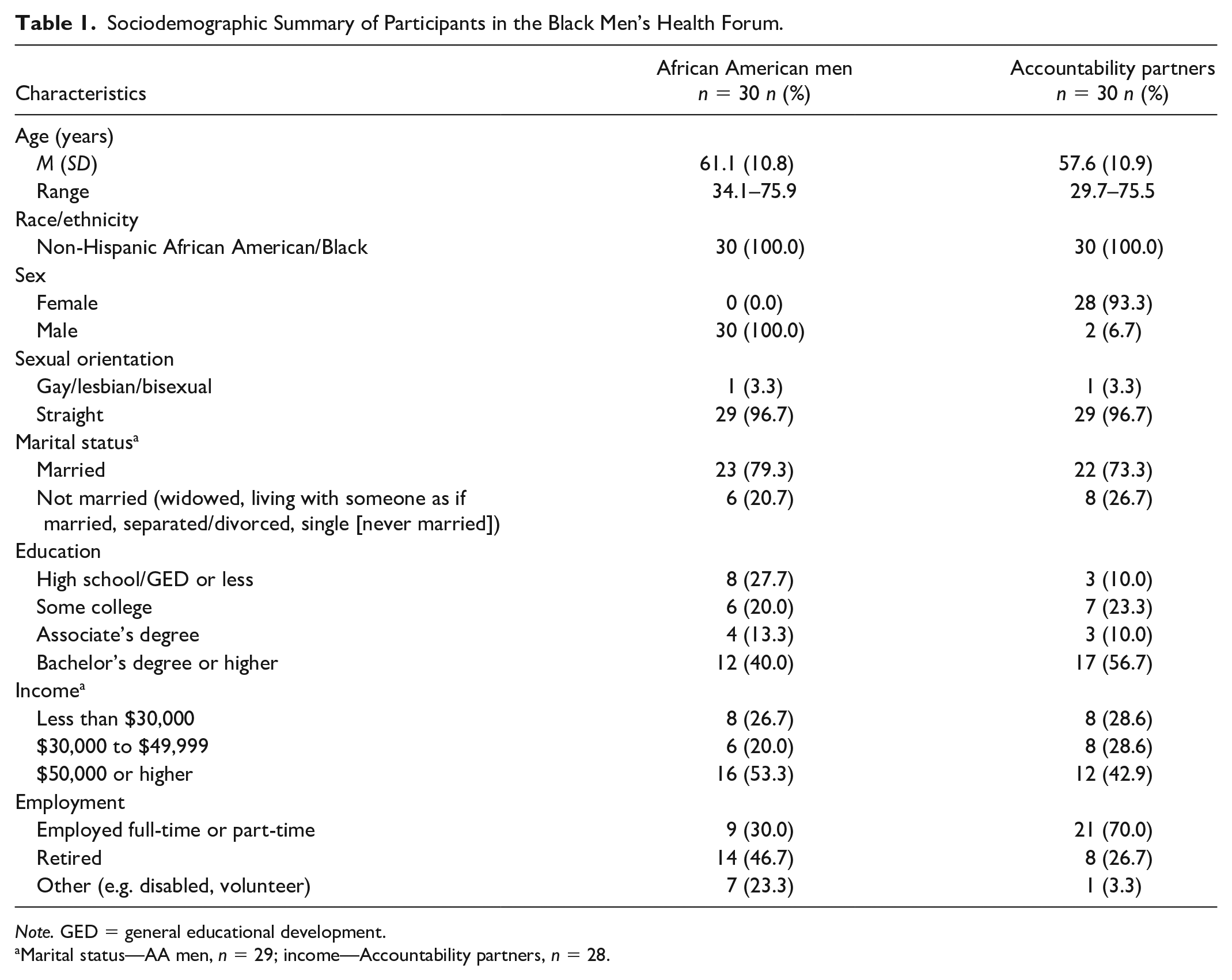
Note. GED = general educational development.
Marital status—AA men, n = 29; income—Accountability partners, n = 28.
AA men who participated in the forum were asked additional questions about their health (Table 2). More than half (56.7%) of AA men reported a self-rated health status of “Very Good” or “Good” while 43.4% of AA men reported a health status of “Fair” or “Poor.” Approximately 84% and 86% of AA men had a physical exam and a dental exam in the past 12 months, respectively. Almost all AA men reported having health insurance (96.7%). Hypertension, erectile dysfunction, and diabetes were the most common lifetime health conditions reported by AA men. Most AA men did not have a high level of psychological distress; 10% of AA men reported high psychological distress.
Health Status of African American Men in the Black Men’s Health Forum, n = 30.
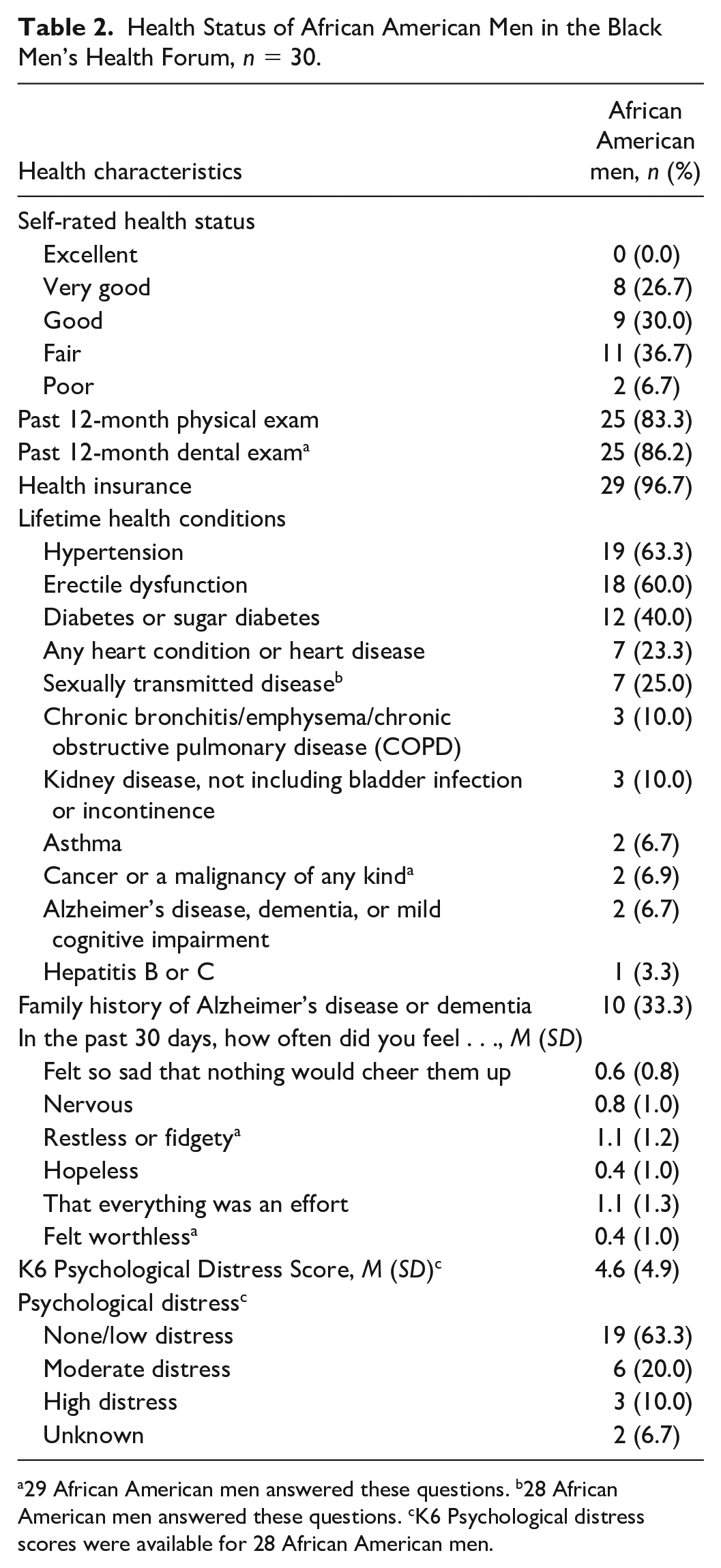
29 African American men answered these questions. b28 African American men answered these questions. cK6 Psychological distress scores were available for 28 African American men.
A total of 19 health concerns, 12 barriers to health care, and 10 neighborhood concerns were observed based on AA men’s responses. In this article, we report the top 3 health concerns, barriers to health care, and neighborhood concerns most frequently reported by AA men who participated in the forum (Table 3). Top health concerns included obesity/weight management, hypertension, diabetes, heart problems, and mental and emotional health. Common barriers to health care were cost, no barriers to health care, options for health care, and going to and remembering appointments. Neighborhood concerns included no neighborhood problems, crime, and safety.
Top Health Concerns, Barriers to Health Care, and Neighborhood Concerns Among African American Men.
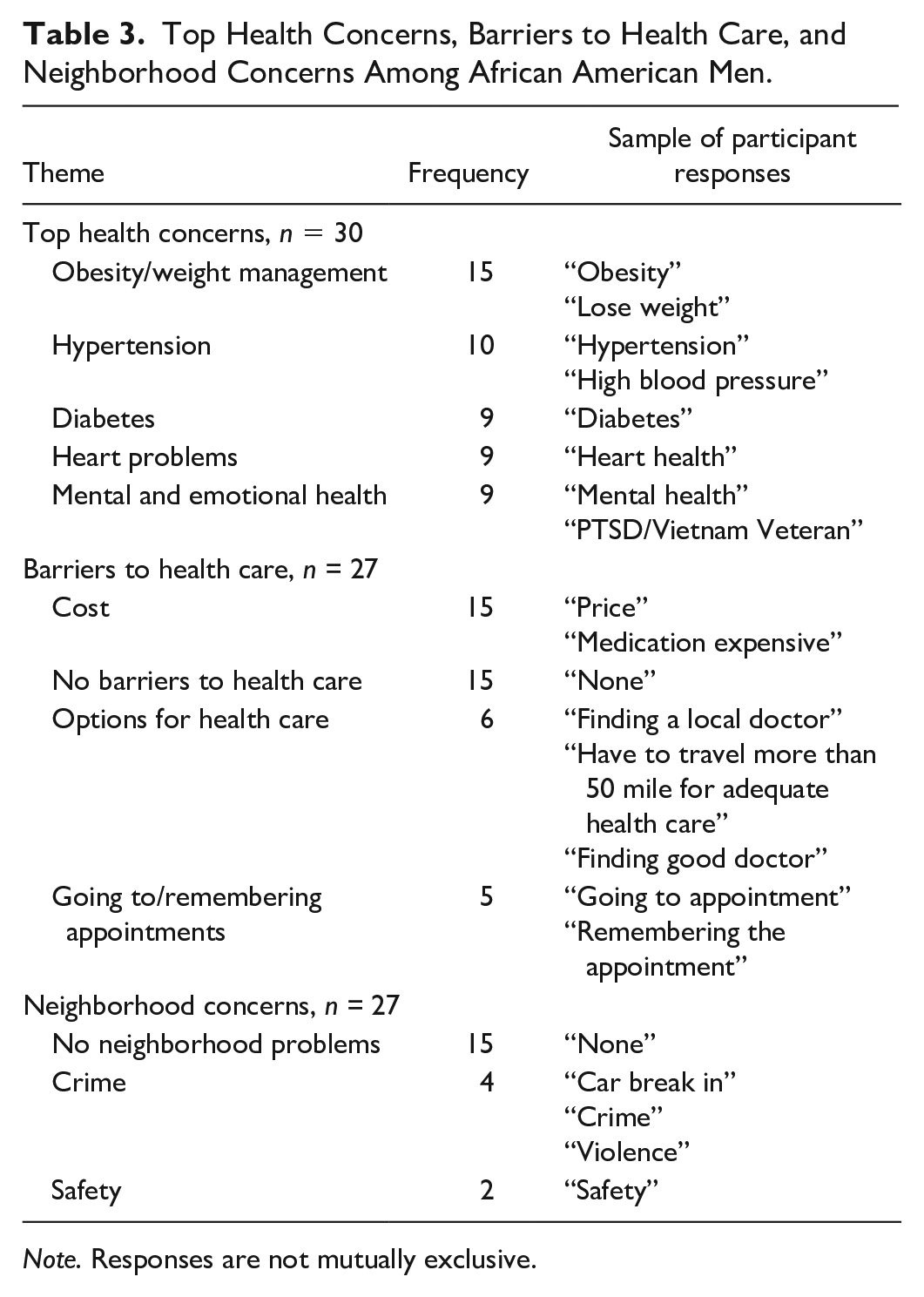
Note. Responses are not mutually exclusive.
The overall change in health knowledge before and after the forum increased significantly for AA men and accountability partners (Table 4). Overall health knowledge increased by 6.9 points for AA men and 2.8 points for accountability partners. Accountability partners also scored higher on the pre-evaluation than AA men in the study (19.8 vs. 15.5). AA men had significant increases in health knowledge in the areas of mental health, sexual health, cancer, cardiometabolic health, and brain health and healthy aging. Accountability partners significantly increased their knowledge in sexual health, cancer, and brain health and healthy aging after the forum.
Knowledge of Black Men’s Health, n = 60.
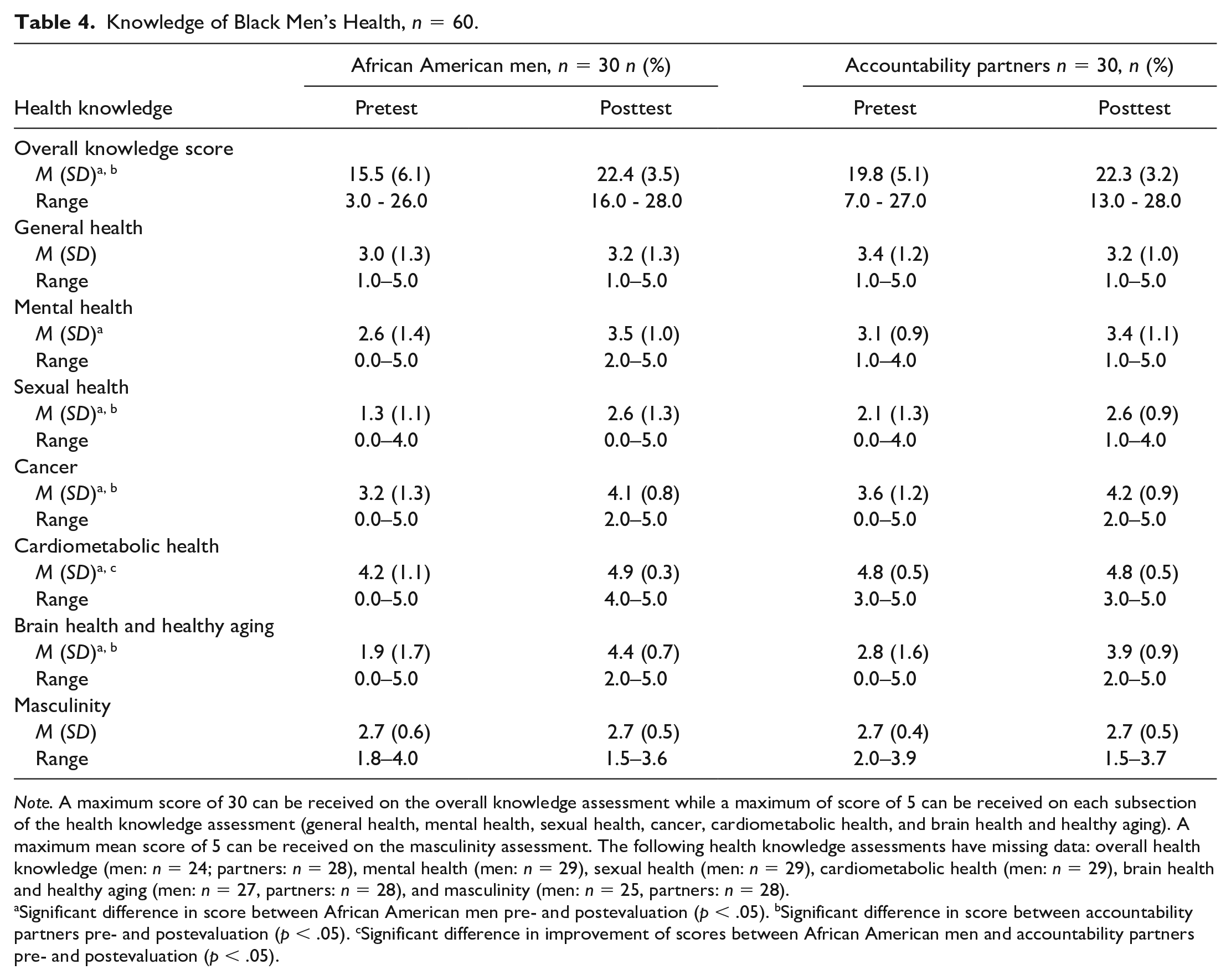
Note. A maximum score of 30 can be received on the overall knowledge assessment while a maximum of score of 5 can be received on each subsection of the health knowledge assessment (general health, mental health, sexual health, cancer, cardiometabolic health, and brain health and healthy aging). A maximum mean score of 5 can be received on the masculinity assessment. The following health knowledge assessments have missing data: overall health knowledge (men: n = 24; partners: n = 28), mental health (men: n = 29), sexual health (men: n = 29), cardiometabolic health (men: n = 29), brain health and healthy aging (men: n = 27, partners: n = 28), and masculinity (men: n = 25, partners: n = 28).
Significant difference in score between African American men pre- and postevaluation (p < .05). bSignificant difference in score between accountability partners pre- and postevaluation (p < .05). cSignificant difference in improvement of scores between African American men and accountability partners pre- and postevaluation (p < .05).
Before the forum began, 30.0% of AA men reported never participating in a research study (Table 5). Trust in researchers and research increased from 7.1 on a scale of 1 to 10 to almost 8 on a scale of 1 to 10. Trust in researchers significantly increased after the forum (p < .05). In addition, the proportion of AA men who reported that they would definitely participate in research in the next 12 months increased by 40%.
Perceptions of Research Among African American Men, n = 30.
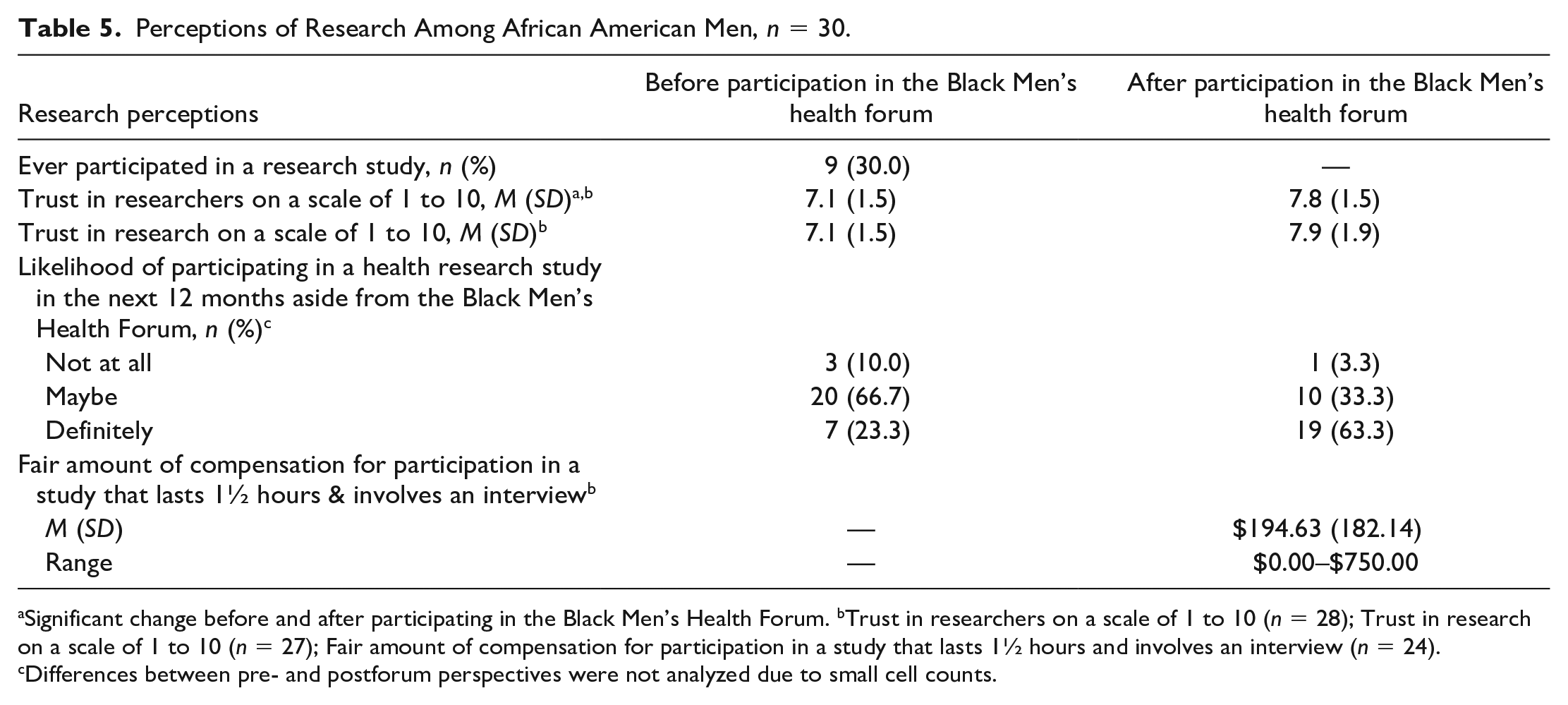
Significant change before and after participating in the Black Men’s Health Forum. bTrust in researchers on a scale of 1 to 10 (n = 28); Trust in research on a scale of 1 to 10 (n = 27); Fair amount of compensation for participation in a study that lasts 1½ hours and involves an interview (n = 24). cDifferences between pre- and postforum perspectives were not analyzed due to small cell counts.
Discussion
The Black Men’s Health Forum reached more than 30 AA men and their accountability partners over a span of 6 weeks to raise awareness and increase knowledge of health issues of concern for AA men and knowledge of health research. Health topics presented in the forum included Black Men’s Health and Black Masculinity, Mental Health, Cancer, Sexual Health, Cardiovascular and Metabolic Health, and Brain Health and Healthy Aging. Health Knowledge significantly increased after participation in the forum for both AA men and their accountability partners. Among AA men, an increase in willingness to participate in health research was also observed.
Although significant increases in health knowledge were observed among AA men and accountability partners in the study, men had a greater increase in knowledge than their accountability partners, on average. When assessed for knowledge of health subtopics, AA men had increases in mental health, sexual health, cancer, cardiometabolic health, and brain health and healthy aging while accountability partners increased their knowledge in sexual health, cancer, and brain health and healthy aging after participating in the forum. Similarly, in a community-based health education intervention, Okoro and colleagues (2020) significantly increased health knowledge among AA men and women in these AA men familial and social networks. In this study, participant health knowledge was assessed in the areas of prostate cancer, heart disease, diabetes, and mental health. Both groups of participants had significant increases in knowledge in all areas of health, excluding AA men in the area of heart disease (Okoro et al., 2020). Offering culturally tailored, community-based health education interventions is a public health approach that enables clinicians and researchers to reach a broader proportion of AA men, especially considering that mistrust of health care systems is commonly cited as a reason for lack of involvement in research and health systems among AAs (Hoyo et al., 2003; Scharff et al., 2010).
Based on results from the pre-evaluation for the forum, 70.0% of men enrolled in the study reported that they had never participated in a research study. Yet, by the end of the forum, the proportion willing to participate in research in the next 12 months increased by 40%. This increase in willingness to participate in research may have been influenced by the presence of AA clinicians and researchers who encouraged research participation during each forum session. Diversity of clinicians and researchers who interact with AA men can have a significant impact on AA men’s engagement with health systems and research. Comparably, Alsan et al. (2019) conducted an experiment in which AA men were randomized to Black or non-Black male physicians to assess the effect of physician workforce diversity on AA men’s decision to engage in preventive services. This study found that AA men who were matched with an AA male physician were more likely to select every preventive service, including more invasive procedures. It was estimated that increased preventive screenings may result in an 8% decline in the White–Black life expectancy gap and as much as a 19% decline in the White–Black cardiovascular mortality gap (Alsan et al., 2019). Moreover, speakers provided participants with factual health information; however, participants were not inundated with dire information about health disparities. AA men were provided with advice on how to improve their health and positive affirmations. Nicholson et al. (2008) found that AAs responded positively to messages of hope and negatively to information on cancer disparities. The delivery and deliverer of health messaging are critical to successfully promote the engagement of AA men into health research.
There are limitations to this study that should be noted. The findings of this study may not be generalizable to all AA men. Participants for the study were recruited via convenience sampling and were recruited from faith-based organizations. Therefore, AA men who are not engaged in faith-based organizations may differ from participants in the study. In addition, participants in this study were largely well educated and insured. Moreover, volunteer bias may be present in this study. AA men who were approached to participate in this study and chose not to participate may have different sociodemographic and health backgrounds. Moreover, there were restrictions in the eligibility criteria, which may have limited who could participate in the study. AA men had to enroll in the study with an accountability partner. Some men did not have anyone in their network who could serve as a partner and could not participate in the study. Access to internet and a device to stream the forum sessions on were also requirements to attend the live weekly sessions, which restricted some AA men and accountability partners from participating in the study.
Despite limitations of this health education intervention, there were several strengths that should be noted, which enabled the successful engagement of AA men in health research and enhancement of their health knowledge. We capitalized on an established network of trust by partnering with faith-based organizations serving AAs to engage with and recruit clusters of AA men to participate in the Black Men’s Health Forum (Graham et al., 2018; Hoyo et al., 2003; Scharff et al., 2010). The endorsement of our study by faith leaders in the community aided in building trustworthiness among AA men and increased interest for participation in the study. The Black Men’s Health Forum provided a culturally tailored health intervention just for AA men. This forum created a safe space for AA men to learn about health issues that disproportionately affect them and to openly discuss their health concerns with other AA men. The facilitators and all speakers for the forum were AA male researchers and clinicians who (1) understood the everyday experience of the AA men, (2) were aware of the importance of increasing healthspan and lifespan among AA men, and (3) were experts in medicine and research. There is a paucity of AA male physicians in the United States, and AA men in the community have limited opportunities to interact with clinicians who look like them and share some of their social experiences. Less than 3% of physicians in the United States are Black men (Ly, 2022). In addition to placing AA men from the community in a space to discuss health with speakers of corresponding racial and gender backgrounds, the forum was hosted over a virtual platform. The virtual platform ameliorated some of the barriers that AAs often face when considering participation in health research such as transportation issues, time to travel to study sites, and mistrust of medical environments (Scharff et al., 2010). AA men were able to participate in the study in the comfort of their own home. Furthermore, accountability partners were able to watch the forum sessions asynchronously, which decreased the inconvenience of study participation (Scharff et al., 2010). We leveraged the influence of family and friends, the majority of which were female, to support AA men in their health journeys. Anecdotally, some research participants shared that participating in the forum initiated conversations around health with their partner.
Through culturally tailored programming, the Black Men’s Health Forum increased access to health information as well as AA male medical professionals and health researchers for AA men in the community. AA men are interested in learning about health and participating in research; however, additional efforts may be necessary to engage AA men in health programming and research in the community. Exposure to health information for AA men resulted in significant increases in health knowledge and willingness to participate in health research. Future efforts will focus on engaging AA men in the community and meeting them where they are to disseminate health information, with a specific focus on the AA male experience in the U.S., and to increase linkages to health resources in the community.
Footnotes
Acknowledgements
The authors would like to thank all men and women who participated in and completed the Black Men’s Health Forum. In addition, we would like to acknowledge Tyrone Bethune, MPH, for his contributions to the development, writing, and editing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All aspects of this research are funded by the National Institutes of Health (National Institute on Aging) via an administrative supplement affiliated with the Wake Forest Alzheimer’s Disease Research Core (P30AG049638-03) and a grant from the Bank of America Charitable Foundation, Inc.