
Abstract
Globally, maternal mortality, and morbidity rates have consistently decreased throughout the years, except in the United States, where rates have increased (World Health Organization, 2021). This increase is especially marked among Black women, where disparities have existed for centuries and continuously worsened in the last few decades (Essien et al., 2019; Singh, 2010). Studies show that Black women are 2.6 times more likely to die from pregnancy-related complications than any other race or ethnicity (Hoyert, 2021). According to the Centers for Disease Control and Prevention, over half of pregnancy-related deaths occur during the postpartum period, when women face a range of physical and emotional challenges and systems of coordinated care are limited. Black women giving birth experience a significantly higher rate of postpartum deaths, extending up to 1 year after childbirth, in comparison to their White counterparts (14.9% vs 10.2%; Scott & Davis, 2022). Postpartum cardiomyopathy was the leading cause of late maternal death among all races, with Black women having a six-times-higher risk than White women (MacDorman, 2021). Black women face a significantly elevated risk of severe maternal morbidity compared to White women, with Black women being twice as likely to encounter life-threatening complications during childbirth and the postpartum period when contrasted with their White counterparts (Estriplet et al., 2022; K. F. James et al., 2021). In addition, 29%–44% of Black women experience postpartum depressive symptoms, yet few are properly identified and/or connected to mental care services (Conrey et al., 2019; Howell et al., 2016). Black women often face barriers in accessing quality postpartum care due to disproportionate rates of poverty, limited access to social support networks, which can be crucial for postpartum recovery, persistent structural racism, and decreased access to resources like insurance, transportation, hospitals, and health care providers in their communities (Daw et al., 2020; Georgia State University Center for State and Local Finance, 2017; Oliver & Muntaner, 2005; Perry et al., 2013; Yale Global Health Justice Partnership, 2018). These social and structural determinants lead to implicit bias among providers, imposing barriers to communication between patients and their providers regarding treatment options and follow-up care (Essien et al., 2019; Hall et al., 2015; Jain & Moroz, 2017; Prather et al., 2016, 2018). This disconnection between providers and patients can result in delayed or inadequate care, increasing the possibility of life-threatening or fatal maternal health outcomes (Bryant et al., 2010; Essien et al., 2019; Holdt Somer et al., 2017; Shahul et al., 2015). It is essential that Black women receive the highest standard of care, one that not only meets their unique care requirements but also empowers them with a sense of agency and self-efficacy throughout their health care journey (Julian et al., 2020; Scott & Davis, 2022).
The first few weeks of the postpartum period, beginning the moment after delivery, are critical for establishing the mother and baby’s long-term health and well-being (Aber et al., 2013; The American College of Obstetricians and Gynecologists, 2018; Fowles et al., 2012; Tully et al., 2017). Postpartum maternal health care is a crucial component of women’s health that is often overlooked and neglected (Cheng et al., 2006; Cornell et al., 2016; Sardi et al., 2020). Many women do not see a provider until 3–6 weeks after hospital discharge, and immediate health concerns may be missed during this interval. However, approximately 40% of women do not attend postpartum visits, with higher percentages among Black and low-income women and those living in rural areas, as well as those with public insurance and residing in rural communities (Essien et al., 2019; The American College of Obstetricians and Gynecologists, 2018; Henderson et al., 2016; Yale Global Health Justice Partnership, 2018). This could be due to distrust in the medical and scientific communities rooted in perceived racism and adapted behaviors (survival and resilience) stemming from the historically oppressive nature of the country (Lekan, 2009). Current literature shows little about the effects of Black women’s experiences in clinical settings on childbirth (McLemore et al., 2018). This lack of research explains the limited scope of health systems and the need for public health interventions to combat inequities in postpartum care, particularly for Black women.
Mobile phones and technology have become increasingly popular as a source of health information; therefore, mobile health (mHealth) applications can have the potential to provide a wealth of access to resources in communities with limited access to direct care from providers with functions like automated text messaging, tailored medical advice, or personalized notifications aimed at promoting specific health practices, such as regular exercise or medication adherence. In the United States, a greater percentage of Black women own smartphones (80%) compared to White women (72%), and although prior research has demonstrated high acceptability among Black women regarding the use of smartphones for health research, they remain underrepresented in mHealth research (D. James et al., 2016, Joseph et al., 2019; The Nielsen Company, 2022).
Many women in the postpartum period have reported using the internet and mHealth applications to obtain health-related information (Bernhardt & Felter, 2004; Gibson & Hanson, 2013; Guendelman et al., 2017; Slomian et al., 2017). However, although many women access and utilize various health sources during pregnancy, they do not tend to look up the information as frequently during the postpartum period (Cheng et al., 2006; Fogel, 2017; Guerra-Reyes et al., 2017; Kanotra et al., 2007). Therefore, utilizing mHealth applications to engage with women shortly after discharge can help customize and establish resources and support for women during the early postpartum period. mHealth applications may present an avenue for the scalable dissemination and broadening of health care resources to individuals and communities that are often overlooked or confronted with profound social challenges (such as historical trauma, discrimination, and marginalization) and systemic barriers (including systemic racism, implicit bias, insurance coverage, time constraints, transportation; Hughson et al., 2018; Nimo-Sefah et al., 2023). Therefore, there is a need for further research on the use of mHealth applications in its ability to provide culturally relevant postpartum content to Black women. For this reason, the purpose of this scoping review is to examine the perceptions about mHealth applications and their utility in this population. Likewise, this review acknowledges the multitude of challenges Black women experience during the postpartum period and looks to mHealth applications as a potential solution.
Method
Search Strategy
Three reviewers conducted a comprehensive literature search to obtain relevant articles using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) extension for scoping review guidelines. Peer-reviewed articles published between 2010 and 2022 were searched on PubMed, while gray literature was searched using Google Scholar and other library catalogs (Tricco et al., 2018). We used the following search terms and their combinations when selecting relevant articles: African American women, Black women, Black, mHealth, mHealth application, mHealth interventions, technology, postpartum health, women’s health, access, resources, risk reduction, morbidity, and mortality. Peer-reviewed articles were filtered to only include results published in English within the last 12 years.
Eligibility Criteria
Eligible studies were peer-reviewed, written in English, utilized mHealth applications as a primary intervention, and focused on postpartum health and access to resources, primarily among Black women in the United States. For the purpose of this study, the postpartum period was defined as the period from the birth of the child up to 1 year after delivery (Romano et al., 2010). Abstracts, commentaries, editorials, and presentations were excluded from the search. We also excluded articles that did not measure the effects of mHealth applications on the postpartum period, articles older than 2010, and articles with study populations outside of the United States.
Study Selection
From our search, 77 articles were uploaded to Covidence, a web-based collaboration software platform that streamlines the production of systematic, scoping, and other literature reviews. Duplicated articles were screened out, leaving 69 articles for review. The titles and abstracts of the 69 articles were screened by two reviewers and mutually decided upon based on eligibility criteria. Following the initial screening of the 69 articles, 23 were found to be systematic reviews or qualitative articles, leaving 46 articles for full-text review. Upon completion of the full-text review, 30 articles were excluded due to the intervention not involving mHealth applications (n = 14), not focusing on the postpartum period (n = 7), having the wrong patient population (n = 6), and being located outside of the United States (n = 3). We then selected the remaining 16 articles for use. However, of the 16, only 8 articles discussed the impact of their mHealth application interventions on the specified population. We decided to use these eight articles for further discussion. The eight articles were assessed for quality based on their study methodology, results, and relevance of concluding statements. Of the included articles, their study strategy, sample size and type, study design and measures, major findings, and future implications were examined to determine their relevance to disparities in postpartum health, the effects of mHealth applications on mothers, mother’s adherence to mHealth applications, and therefore reduction in maternal mortality and morbidity rates.
Results
Overall results showed that when designed and tailored to meet target population needs, mHealth interventions have the ability to influence behavior change and lead to improved health outcomes in Black and minority women. Figure 1 shows the number of studies screened for eligibility, selected for full-text review, and then selected for inclusion in our study. Table 1 shows the study characteristics.
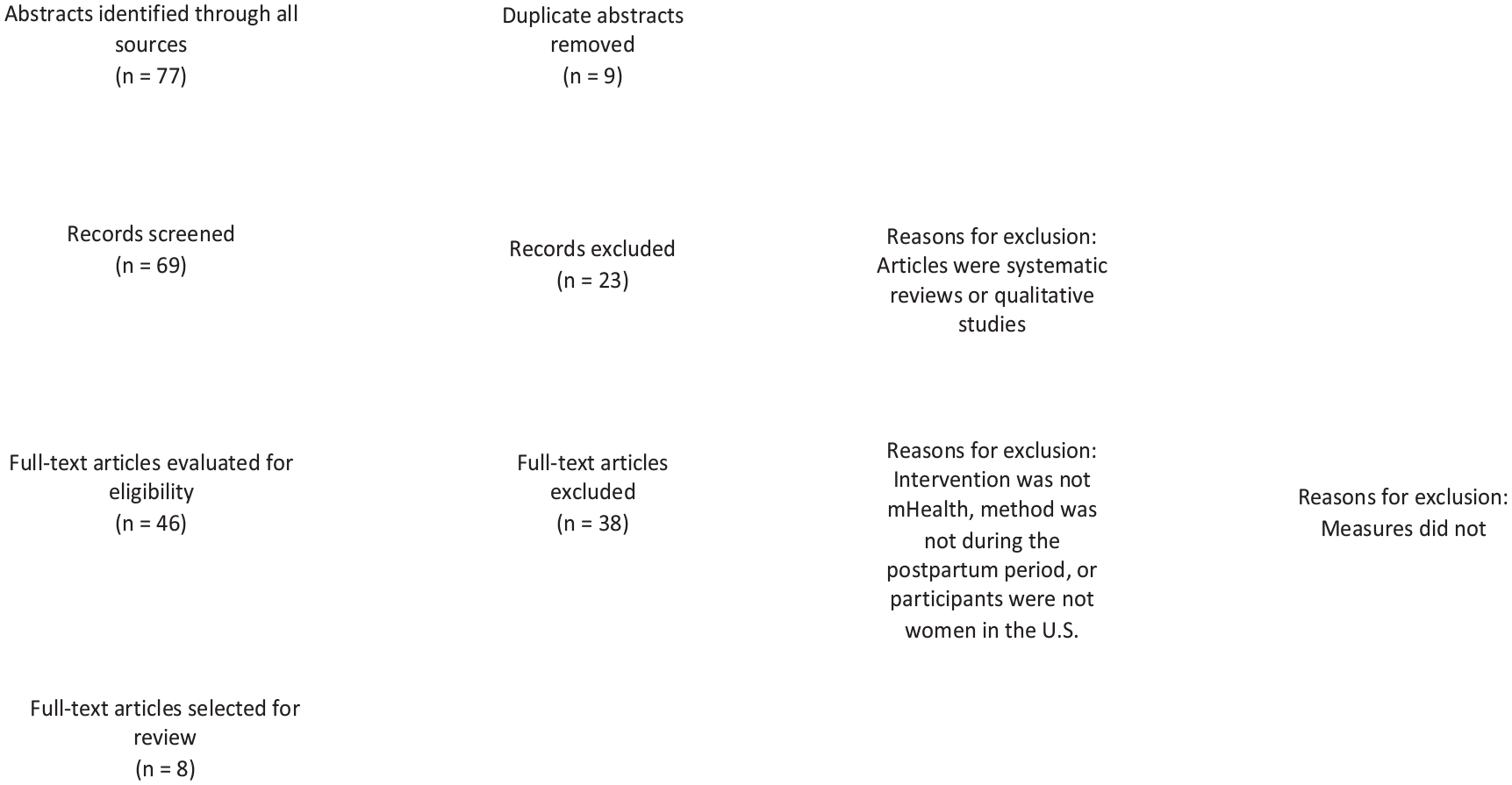
PRISMA Flow Diagram Showing the Number of Articles Identified, Screened, Excluded, and Included in the Scoping Review
Summary Table of Study Characteristics, Findings, and Implications for Practice (N = 8)
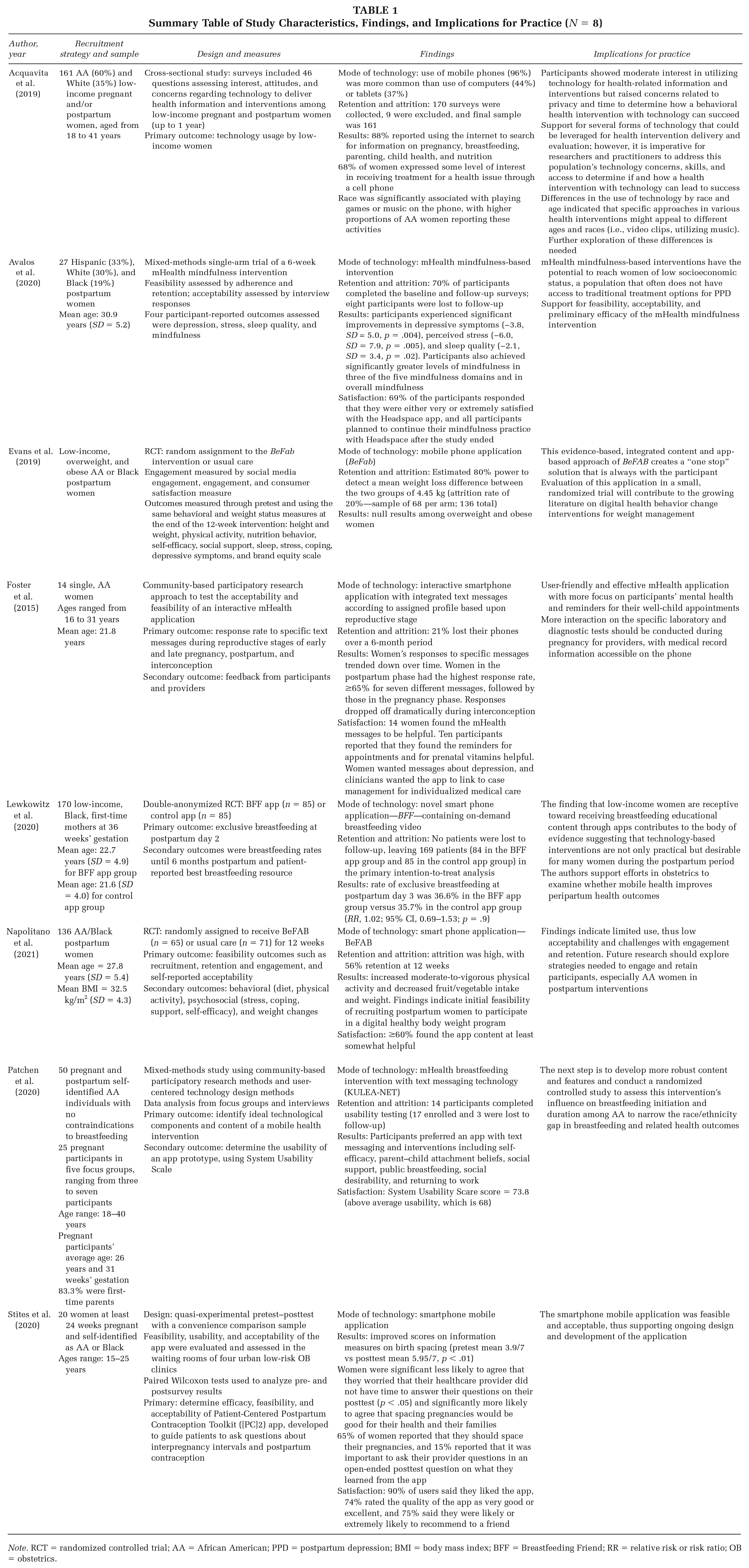
Note. RCT = randomized controlled trial; AA = African American; PPD = postpartum depression; BMI = body mass index; BFF = Breastfeeding Friend; RR = relative risk or risk ratio; OB = obstetrics.
Population
Most of the studies (n = 7) included a large percentage of Black participants, with at least 60% of this group represented in the samples (Acquavita et al., 2019; Evans et al., 2019; Foster et al., 2015; Lewkowitz et al., 2020; Napolitano et al., 2021; Patchen et al., 2020; Stites et al., 2020). One study focused on a mixture of minorities, 33% Hispanic and 19% Black (Avalos et al., 2020). Most participants were recruited from obstetrics offices and other health-related settings and used electronic medical records to preview characteristics of eligible participants. The majority of studies (n = 7) focused on women of reproductive age, spanning from 15 to 41 years, with mean ages ranging between 21.8 and 30.9 years (Acquavita et al., 2019; Avalos et al., 2020; Lewkowitz et al., 2020; Napolitano et al., 2021; Patchen et al., 2020; Stites et al., 2020).
Study Quality
Three (Evans et al., 2019; Lewkowitz et al., 2020; Napolitano et al., 2021) of the eight studies were randomized controlled trials, one was a cross-sectional study (Acquavita et al., 2019), three were mixed-methods studies (Avalos et al., 2020; Foster et al., 2015; Patchen et al., 2020), and one was quasi-experimental (Stites et al., 2020). Two mixed-methods studies utilized a community-based participatory research approach (Foster et al., 2015; Patchen et al., 2020), while the other was a single-arm trial (Avalos et al., 2020). All studies utilized quantitative methodology (Table 2).
Summary of the Systematic Search Strategy
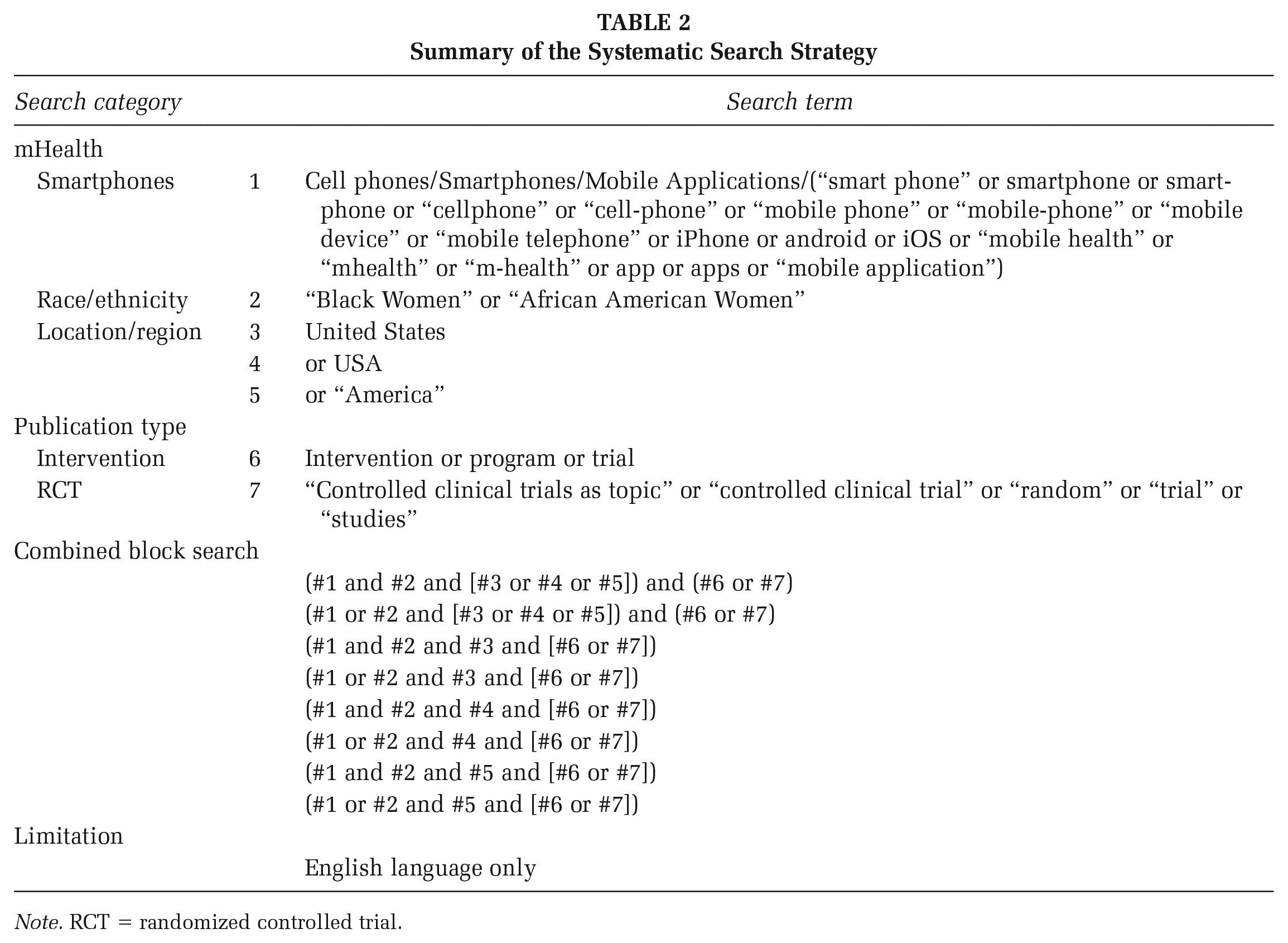
Note. RCT = randomized controlled trial.
Outcome Measures
Increased acceptability and feasibility for the various mHealth interventions were commonly reported among studies, highlighting the importance of the role of mHealth applications in improving disparities in Black postpartum mothers (Avalos et al., 2020; Napolitano et al., 2021; Patchen et al., 2020; Stites et al., 2020). A study by Acquavita et al. (2019) focused on usage of mobile phone technology stratified by age or race as the primary outcome (Acquavita et al., 2019). One study reported behavioral, psychosocial, and weight outcomes as the primary outcome measures (Evans et al., 2019). Another study reported the response rate to specific text messages during various reproductive stages as the primary outcome measure (Foster et al., 2015). A study by Lewkowitz et al. (2020) reported exclusive breastfeeding at postpartum day 2 as the primary outcome (Lewkowitz et al., 2020). Secondary outcome measures varied widely among studies and included feedback from participants and providers, the usability of an app prototype, breastfeeding rates until 6 months postpartum, and patients’ feedback on breastfeeding resources (Foster et al., 2015; Lewkowitz et al., 2020; Patchen et al., 2020).
Mobile Phone-Based Interventions
All eight studies employed mobile phone app-based interventions, given that was one of the primary inclusion criteria. The mobile phone application interventions integrated text messaging (Foster et al., 2015; Patchen et al., 2020) and on-demand videos (Lewkowitz et al., 2020). Most (n = 5) of these interventions incorporated content tailored toward culture and gender (Evans et al., 2019; Foster et al., 2015; Lewkowitz et al., 2020; Napolitano et al., 2021; Patchen et al., 2020).
In Avalos et al.’s (2020) study, the theoretical basis for mindfulness is derived from a model rooted in studies of the influence of mindfulness on learning, memory processes, and emotional regulation—all in support of recent research suggesting that mindfulness mHealth interventions may promote efficacious nonpharmacological treatment for postpartum depression. Two other articles utilized social cognitive theory and health branding as a theoretical framework for their studies (Evans et al., 2019; Patchen et al., 2020). Another study utilized pre- and postsurvey instruments modeled on the information–motivation–behavior framework (Stites et al., 2020).
Attrition and Loss to Follow-Up
Overall, retention was high among the studies, with the majority reporting retention rates of at least 70% (n = 5). Among included studies that utilized mobile phone-based mHealth interventions, a common cause of loss to follow-up was participants losing their phones (Foster et al., 2015) or changing their phone numbers (Acquavita et al., 2019).
Discussion
Leveraging mHealth interventions may present innovative prospects to advance equitable health outcomes for Black postpartum women; however, as this scoping review suggests, there is limited information on how Black women are engaged in these interventions. A particular challenge prevalent in the application of mHealth among Black women is long-term user retention and promoting user engagement. This challenge is of the utmost importance for Black women, given that there is an overall lack of inclusion in mHealth research. Consequently, there are significant gaps in the literature and, thus, limited knowledge regarding recruitment and retention of Black women in mHealth interventions.
In addition, the pool of health care systems and public health interventions to address inequalities in postpartum care for Black women is severely limited. Given the discrepancies in attention to postpartum care, coupled with the critical importance of the postpartum period for preventing adverse maternal health outcomes, optimizing postpartum care and addressing barriers to care for Black women during this period are essential for alleviating maternal health disparities (Yale Global Health Justice Partnership, 2018). Although women tend to access and utilize a variety of health sources during pregnancy, many of these sources of information and care do not transfer into the postpartum period (Cheng et al., 2006; Fogel, 2017; Guerra-Reyes et al., 2017; Kanotra et al., 2007).
This scoping review identified and summarized literature published on the use of mHealth interventions to address postpartum health among Black women. Among the studies included, mobile phones were the only platform used to implement mHealth interventions, with various integrations of text messaging and on-demand video. Integrative mHealth interventions are pivotal, as data suggest that mobile phone availability among women in low-resource settings is related to improved health outcomes during the postpartum period. Lefevre et al. (2020) state that mobile phone availability improves women’s decision-making, access to health services, and effective health communication. These improvements may positively impact a woman’s decision to advocate for herself during the postpartum period, which could address provider bias and communication barriers.
However, it is important to consider the validity and accuracy of health information presented in mobile apps, which can vary widely and, thus, more widespread education to users, particularly Black women, is crucial. Some considerations for verification can include seeking professional advice and recommendations, seeking the developer’s credibility, reviews and ratings, and checking the source of information being disseminated.
Implications for Research, Practice, and Policy
mHealth applications have grown increasingly popular as sources of health information. Given the near-ubiquitous use of mobile phones in the United States, mHealth applications offer accessibility alongside versatility to specific audiences that may otherwise not be reached. Recent studies have demonstrated that postpartum women frequently use mobile phones and the internet to search for health information (Hughson et al., 2018). Although participants reported using mobile applications throughout their pregnancy, they also reported that applications were unavailable or did not address their concerns during the postpartum period, given that these studies were examining different types of mHealth information (Gibson & Hanson, 2013; Guendelman et al., 2017; Slomian et al., 2017). The available literature on the use of mHealth interventions during the postpartum period is severely limited (Guerra-Reyes et al., 2017). mHealth applications have predominantly been concentrated on the dissemination of health information, serving as valuable sources of knowledge and guidance. However, to fully harness their potential, future interventions must broaden their utility. One promising avenue for expansion lies in utilizing these applications to connect Black mothers and address the critical social determinants of health that disproportionately affect them (Rogers et al., 2023). These platforms may be instrumental in linking these mothers to essential services, helping to bridge gaps in their unmet social support needs. Moreover, mHealth applications present a vital opportunity for remote monitoring of critical health metrics, including conditions like embolism, preeclampsia, and cardiomyopathy that disproportionately impact Black women, contributing to the primary causes of pregnancy-related deaths within this demographic (Mendez et al., 2019; Vernon & Yang, 2022). This capability equips Black women and health care providers with an invaluable tool to track and respond to health concerns in real time. The implementation of remote monitoring programs specific to Black women has the potential to mitigate disparities in maternal mortality and morbidity (Vernon & Yang, 2022). By extending the reach and capabilities of mHealth applications, we can create a more comprehensive and inclusive health care ecosystem that better serves the needs of Black mothers and, by extension, the broader community.
To date, no literature has been published on the use of mHealth applications for postpartum Black women, particularly those living in areas known to experience geographic disparities, such as limited access to health care facilities, leading to delayed or inadequate care (Danbjørg et al., 2015; Osma et al., 2016; McCarter et al., 2019; Shorey et al., 2018). Of the available literature, it is known that current mHealth applications do not provide adequate maternal health information and are not optimally accessible to users in terms of inclusivity or usability (Tucker et al., 2021). This decreases the effectiveness of information provided in mHealth applications and further marginalizes minority populations who already experience the effects of the digital divide (Tucker et al., 2021). Therefore, to ensure the long-term sustainability of health outcomes in Black postpartum mothers, it is crucial that providers understand the lack of relevant health information current applications provide to Black women and are educated on the quality of current mHealth application offerings. With providers knowing the scarcity of relevant mHealth applications, they can accurately recommend mHealth applications to their patients and ensure the maintenance of applications according to their patient’s needs.
mHealth interventions have far-reaching implications for health care policy across local, regional, national, and global levels. They can significantly enhance access to health care, especially in underserved areas, prompting the need for policies that encourage their adoption. In addition, mHealth applications can lead to cost savings by reducing infrastructure and administrative expenses, allowing policymakers to reallocate resources. Moreover, policies can focus on leveraging mHealth applications for preventive care, chronic disease management, patient engagement, data privacy, interoperability, provider training, regulatory oversight, evidence-based practice, telemedicine integration, and global health initiatives. For example, the Whitehouse Blueprint mentions telemedicine and technology as tools to address the maternal health crisis (White House, 2022). Similarly, analysis of federal legislation suggests that implementation of provider training such as implicit bias training, investing in digital tools, and refined data collection processes as potential avenues to improve maternal health outcomes in underserved communities (Black Maternal Health Momnibus Act of 2021, 2022; Carty et al., 2022). Effective policy development is essential to maximize the benefits of mHealth applications while maintaining high standards of care and patient safety.
Given that mHealth technology has the potential to overcome barriers and gaps in postpartum care, there is a need for research on mHealth applications that provide postpartum content to Black women, who face unique challenges during the postpartum period. Evidence reveals a link between the adoption of mHealth interventions, better chances of survival, and fewer postpartum complications for mothers and their newborns (Gayesa et al., 2023). Knowing this, interventions may be implemented and customized to better meet the needs of Black women and those with limited access to resources, support, and communication.
Limitations
Given our search approach, it is probable that relevant articles were not found and hence were eliminated from our analysis. There could have been a loss of data and information on the topic due to our method of obtaining literature. In addition, given the scarcity of literature on the subject, more rigorous recruiting tactics and research are required to examine how mHealth interventions might better fulfill the needs of institutionally underserved Black women. Expanding the search strategy to include more terms related to maternal health could serve as a potential technique to mitigate these limitations in future research. In addition, including relevant articles that are not solely focused on the postpartum period could still be beneficial in assessing the impact of mHealth technology on Black maternal health.
Conclusion
The immediate postpartum period, though fleeting, has many short-term and long-term implications for a woman’s health. It is simultaneously a difficult time to access traditional care given the new responsibilities that arise when caring for a newborn, in addition to all the usual search term barriers to care that Black women face. Leveraging the capabilities of mHealth technologies to expand access to care for postpartum health has the potential to drastically reduce maternal morbidity and mortality, improve the patient experience, and mitigate the racial disparities institutionalized by the health care system (Lefevre et al., 2020). Consistent investment in grouping, refining, and evaluating mHealth technology and applications for postpartum women—with specific attention to mHealth technologies’ ability to provide equitable, personalized care—is a pivotal step toward promoting obstetric health for all women.
Our findings show that when mHealth interventions are designed and adjusted to address and fulfill the needs of target populations, they can successfully inspire behavior change and enhance postpartum health outcomes. More research is needed, however, to determine whether the better health outcomes brought about by mHealth interventions are sustainable in long term.
Interventions that enhance postpartum care knowledge and promote behavior change through interactive material customized to Black women’s distinct needs and experiences will be critical for reducing the health inequalities that exist among this vulnerable demographic. When designed with the target population in mind, mHealth applications have the ability to overcome considerable hurdles and improve postpartum care for Black women who otherwise would not have access to such health material during this time period.