
Abstract
The Prenatal Oral Health Program (pOHP) was developed to educate dental students on prenatal oral health and promote access to dental care for pregnant women. Program advancement has occurred in support of quality improvement. This mixed-methods design combined quantitative data from fourth-year dental students who participated the pOHP (N = 81) and qualitative data from a student-faculty-staff focus group discussion (N = 7). Different clinical structures, appropriate leveling in the curriculum, management with a patient care coordinator, and inclusion of interprofessional learning experiences (IPE) were compared. The survey response rate was 96.4% (N = 81). Trends were noted between students who provided clinical care for a pregnant patient (31%) versus those who did not. Results indicated that an integrated clinic was preferred, though students who had treated a pOHP patient showed greater support for a standalone clinic model. Survey and focus group data agreed that pOHP should occur during the third-year dental school training; however, students with patient experience favored second-year placement. Survey and focus group data emphasize the importance of a patient care coordinator for clinical management and IPE as an essential learning element. Innovating new clinical models requires a period of evolution to determine preferred and sustainable infrastructure. Results reveal the advantages and disadvantages of various program implementation models and demonstrate that student perceptions were influenced by their clinical experiences. Study findings will inform implementation and guide other programs as they create and modify existing curricula to enhance prenatal oral health.
Keywords
Pregnancy induces hormonal and physiological changes that increase susceptibility to oral diseases (National Institutes of Health, 2021). Periodontal disease often manifests during pregnancy, with 30%–40% of pregnant women having periodontal disease (Bersell, 2017). Research studies indicate a relationship between poor maternal oral health and an increased risk of preterm delivery, low birth weight, preeclampsia, gestational diabetes, stillbirth, and a link between maternal and infant/child oral health (Boggess & Edelstein, 2006; Daalderop et al., 2018; Hagai et al., 2015; R. S. Lee et al., 2010; National Institutes of Health, 2021; Offenbacher et al., 2009; Strafford et al., 2008; Vergnes & Sixou, 2007).
Pregnant women represent an under-resourced population in the dental health care community. Data indicate that 25%–50% of women in the United States seek care during pregnancy when a problem occurs, the lowest in underserved communities (Bersell, 2017; National Institutes of Health, 2021; VanderWielen et al., 2015). A 2018 systematic review reported prevalence of dental visits during pregnancy ranged from 33% to 68% in United States and Canada (Rocha et al., 2018). Studies concurred that those at a greater risk included ethnic minorities, low income, and those with less education (H. Lee et al., 2022; Marchi et al., 2010; Naavaal et al., 2019; Rocha et al., 2018; Schroth et al., 2015).
Inconsistent prenatal oral health education in dental school curricula exacerbates discrepancies in the standards of care. Academic deans at 65 accredited dental schools in United States and Canada were surveyed and asked to evaluate their prenatal oral health curriculum (Wilder et al., 2009). Of those who responded (N = 50;77%), 26% indicated having sufficient prenatal oral health content. Study results showed a need for increased oral-systemic content and increased interprofessional collaboration. Another study surveyed dental schools and obstetrics and gynecology (OB-GYN) residency programs to explore the amount of time dedicated to prenatal oral health in their respective programs (Curtis et al., 2013). Results found that 94% of dental schools had at least 1 hr, and 61% had 3 or more education hours regarding prenatal oral health. Thirty-two percent of OB-GYN respondents indicated 1 hr of content, and 6% reported 3 or more hours of prenatal oral health education. Although these studies show the presence of prenatal oral health content in their respective programs, it also highlights the varying range of time dedicated to their curricula.
The Prenatal Oral Health Program
The Prenatal Oral Health Program (pOHP) was developed at the University of North Carolina at Chapel Hill (UNC) Adams School of Dentistry to promote evidenced-based care and interprofessional collaboration between medical, dental, and dental hygiene students to provide underserved populations of pregnant women with comprehensive health care (Jackson et al., 2015). Program implementation coincided with American Dental Association and American College of Obstetricians and Gynecologists guidelines, which provided toolkits to address oral health care of women during and after pregnancy (Hartnett et al., 2016; Quinonez & Boggess, 2021).
The pOHP curriculum was designed using evidenced-based practice standards. Subsequent changes included guidance by the Qualis Health: Oral Health Delivery Framework (Phillips & Hummel, 2016). This Framework enhanced a focus on collaborative care, including oral health screening, counseling, and interprofessional partnerships for referral to a dental home. These aspects were critical elements in outcomes assessments with specific constructs on assessing learner knowledge, confidence, and willingness to perform screening, counseling, treatment, and referral of pregnant patients.
The pOHP structure for dental students included a didactic seminar, online access to evidenced-based resources, and clinical learning experiences (Quinonez & Boggess, 2021). The didactic session included a comprehensive presentation detailing care management, oral health information that can benefit the mother and baby, and an outline of the pOHP referral and clinical flow process.
As part of the pOHP, individuals without dental homes could be referred by their medical provider to receive oral health care in dental school clinics. Patient recruitment included promoting the program through fliers and social media advertisements in the dental and medical school, family medicine and obstetrics clinics, and partnering with potential referring physicians in the community.
Previous research demonstrated that pOHP increased dental referrals for pregnant women, promoted oral exams of pregnant women by their primary care providers, enhanced prenatal oral health knowledge and behaviors of involved students, and provided opportunities to treat pregnant women (Brame et al., 2020; Jackson et al., 2015; Leone et al., 2017). Brame et al. (2020) examined the effect of the pOHP program on dental hygiene students. Results confirmed increased student knowledge and confidence in screening and counseling pregnant patients. The investigators also found that clinical experience had an influential role in students’ understanding of the safety of dental care for women during pregnancy. Results indicated that didactic and clinical immersion opportunities enhanced knowledge and practice behavior changes.
pOHP Implementation Evolution
The original clinical design for the pOHP patients included a standalone clinic during designated days and times per week. This layout would create a silo for pOHP care and a dedicated faculty member to oversee their appointments. Eventual adjustments shifted care to the general dentistry student clinics without a dedicated clinical faculty member. The outcome removed dedicated clinical chair space, and instead, the pOHP-referred patients would receive care in the student clinics with all other patients. This change occurred due to competition for resources, such as faculty availability and clinical space.
A conscience effort was applied when leveling the content and learning experience in the dental school curriculum. The pOHP didactic session and clinical learning experiences were embedded into the final and fourth-year dental school when initially integrated into the dental school curriculum. Challenges with scheduling and anecdotal feedback concerning the proper leveling sparked changes that shifted the program’s curricular timing from fourth-year (D4) to third-year (D3).
Finally, when pOHP began, dental students were responsible for patient management and appointment scheduling. While managing patient care is essential in practice management skill-building, it added stress for students unfamiliar with this referral process and already overwhelmed with existing patient care obligations. In addition, as D4 students, scheduling conflict could arise if an existing patient presented with urgent treatment needs, competing with their clinical availability before graduating. Given these challenges, a patient care coordinator (PCC) was resourced to support the pOHP referrals. The PCC facilitated the referral repository, patient communication, appointment scheduling, and follow-up.
Quality improvement measures were implemented to evaluate the model adjustments. Using the Plan, Do, Study, Act (PDSA) Quality Improvement model (Institute for Healthcare Improvement, 2017), the pOHP team sought to continually gauge the impact of changes. Specifically, these steps included creating a quality improvement plan that included testing changes; documenting observations and feedback; analyzing data to determine modifications; and implementing changes for continuous improvement.
Purpose
This program evaluation aimed to evaluate implementation models and infrastructural systems used to employ pOHP. The intent was to support other institutions implementing educational programs with similar goals to increase learners’ clinical experiences and improve access to care for an under-resourced population.
Method
Study Design
Institutional Review Board approval was obtained from the Office of Human Research Ethics at UNC-CH (#12-1167). This mixed-methods study combined quantitative data from a survey with qualitative data from a focus group. Study participants included dental students, faculty, staff, and dental alums from the UNC Adams School of Dentistry.
Data collection was implemented in the fall of 2018 with survey distribution and the completion of a focus group. In August 2017, all third-year dental students participated in a pOHP orientation. This orientation session encompassed a didactic overview of prenatal oral health and provided details describing the integration of the pOHP into their 2017–2018 academic year. In August 2018, following the conclusion of the 2017–2018 academic year and subsequent pOHP participation, this cohort of dental students (now entering their fourth year of dental school training) were asked to complete a pOHP post-program survey. In addition to this data collection, a focus group with faculty, staff, and dental alums who were integral to the pOHP development, occurred in the fall of 2018 to gather qualitative data.
Survey Design
The survey was revised for dental students following a prior study that examined the perceptions and behaviors of medical students participating in the counsel and referral for dental care aspect of pOHP (Leone et al., 2017).
Kirkpatrick’s Four-Level Training Evaluation Model provided a blueprint for building the survey and focus group questions (Kirkpatrick, 1998). The four levels were integrated into outcomes assessment methods and addressed the following: 1—reaction: What did participants like and dislike; 2—learning: what was the impact on students’ knowledge, skills, and attitudes; 3—behavior: willingness to provide care for pregnant patients; and 4—results: impact on health and educational systems. Additional goals included gaining perceptions of advantages and disadvantages regarding different clinical, curricular timing, and appointment management systems (no PCC vs. PCC).
The survey instrument consisted of 21 questions using a Likert-type-scale design to assess levels of agreement with knowledge, confidence, and willingness to screen, counsel, and treat pregnant patients. Constructs included demographics, clinical experiences, knowledge regarding treatment safety, confidence to provide oral health services to pregnant patients, willingness to implement prenatal care, and perception of resources and practice behaviors.
Surveys were disseminated to all fourth-year dental students in August 2018. Students were informed study completion was voluntary and nonparticipation would not negatively impact their status. No names or identifiers were collected, and responses remained anonymous.
Focus Group Procedures
In August 2018, faculty, staff, and dental alumni involved with pOHP formation were invited to participate in a focus group. Of the 11 people invited, 7 agreed to participate. The focus group occurred in October 2018 and included students who had previously participated in pOHP (N = 3), staff (N = 2), and faculty (N = 2). Each focus group participant was given a letter of invitation, introductory information including the rationale and process for assessing the advantages and disadvantages of various iterations of pOHP over time, research participation information, and a consent form. A focus group mediator utilized a guide with prompts designed to capture their perceptions of the advantages and disadvantages of pOHP aspects.
Data analysis
The focus group session was audio-recorded and later transcribed for analysis. No identifiers were used in the transcription to protect participant anonymity. The focus group mediator prepared a summary to include main points and ideas, with supporting quotes, which was compiled and summarized, with representative verbatim key quotes included. For the student survey, summary scores and percentages from questionnaires were compared using two-tailed t-tests with GraphPad Prism Software. Survey responses from students who did and did not see a pOHP patient were compared. The statistical significance criterion was set at p<.05. Analysis of survey and focus group data occurred in the Winter of 2018.
Results
Sampling and Demographic Data
Eighty-one dental students completed the survey (response rate = 96.4%). Demographic data are illustrated in Table 1. All students gained the didactic component of pOHP; however, not every student provided care for a pregnant patient during their clinical learning experiences due to low patient volume, as many patients missed appointments. Of the 81 respondents, 25 cared for one or more pOHP patient(s) (31%; Table 1). The data, therefore, have been categorized into two groups: students who did not provide treatment to a pOHP patient (NO PT; N = 56) and students who did provide therapy to a pOHP patient (PT; N = 25). Students in the two groups did not differ significantly in age (p = .72), gender (p = .06), whether they have children (p = .35), or intended career path (p > .09 for all categories) (Table 1).
Demographic Characteristics and Intended Career Path of Dental Students Surveyed by Treating or Not Treating a Perinatal Oral Health Program (pOHP) Patient
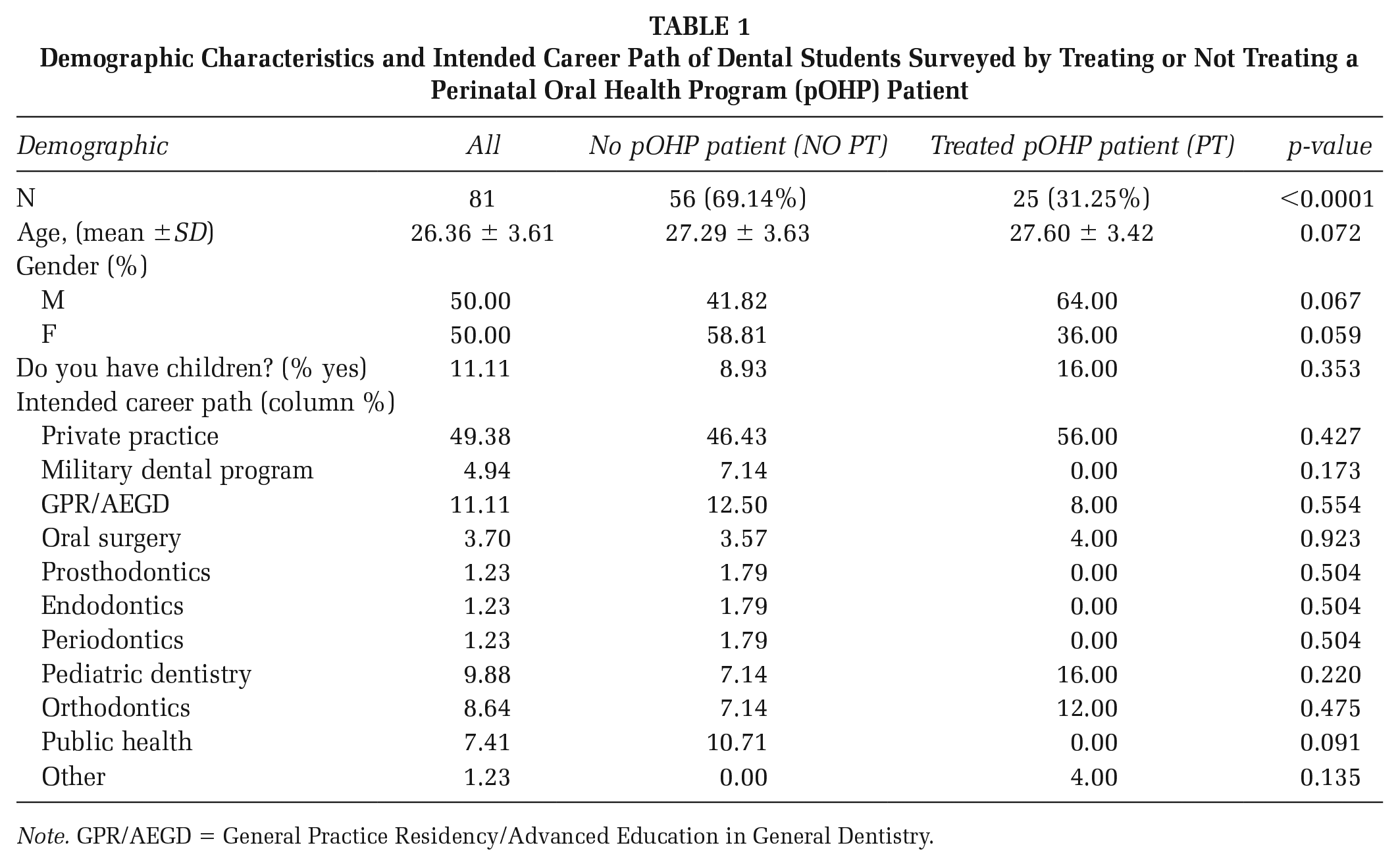
Note. GPR/AEGD = General Practice Residency/Advanced Education in General Dentistry.
Clinical Format for pOHP
Focus group participants were asked for opinions regarding the pOHP as a standalone clinic versus being integrated into the student general dentistry clinic. Participants agreed that integration was convenient for an existing system with a well-established structure. Noted advantages included the feasibility of care, smoother student experience, interprofessional interactions, and reinforcement of pOHP values regarding the safety of dental procedures for pregnant women.
A reported disadvantage to this model was that faculty might not be as focused or knowledgeable on pOHP’s goals and protocols. Some faculty may perceive that pOHP patients increase clinical teaching responsibilities. Despite this issue, focus group participants agreed that a standalone clinic had disadvantages with workflow and unsustainability. Table 2A summarizes participant perceptions.
Advantages and Disadvantages of Two Different pOHP Clinical Structures
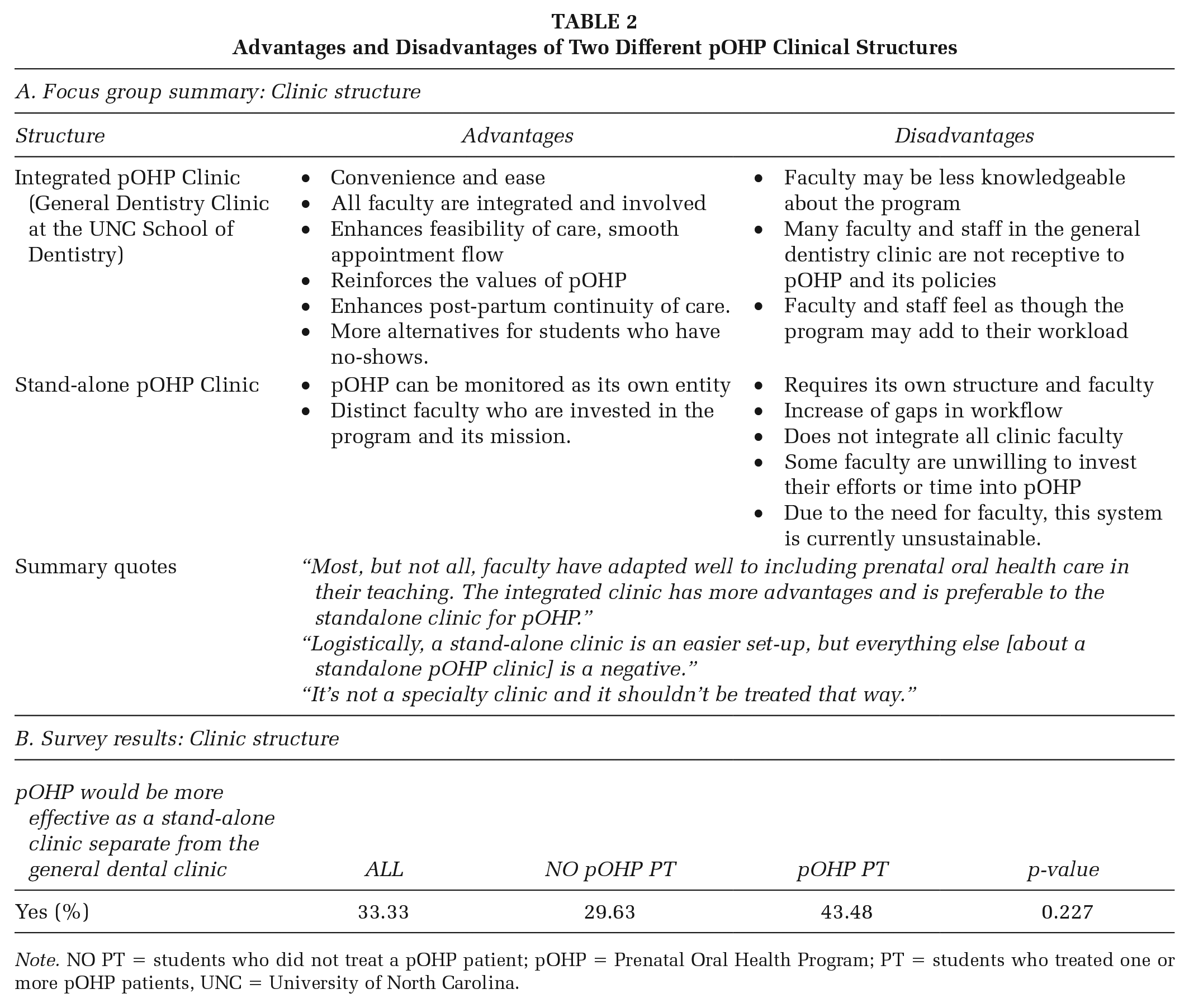
Note. NO PT = students who did not treat a pOHP patient; pOHP = Prenatal Oral Health Program; PT = students who treated one or more pOHP patients, UNC = University of North Carolina.
Survey results demonstrated agreement with focus group feedback. Only 33.3% of students responded that pOHP should be a standalone clinic. Students with clinical patient experiences preferred a standalone clinic, though differences were not significant (NO PT 29.6% vs. PT 43.5%; p = .23; Table 2B).
Program Timing in the Curriculum
The pOHP was initially embedded into the D4 curriculum and re-sequenced to D3 after two years. Focus group participants agreed it was more valuable in D3. D3 students were more receptive, and as a result, both patients and students benefited. Though D3 students may be less experienced and require more guidance and clinical supervision, participants agreed this was appropriate. Table 3A summarizes the findings.
pOHP Curriculum: Advantages and Disadvantages by Year of Dental Student Training
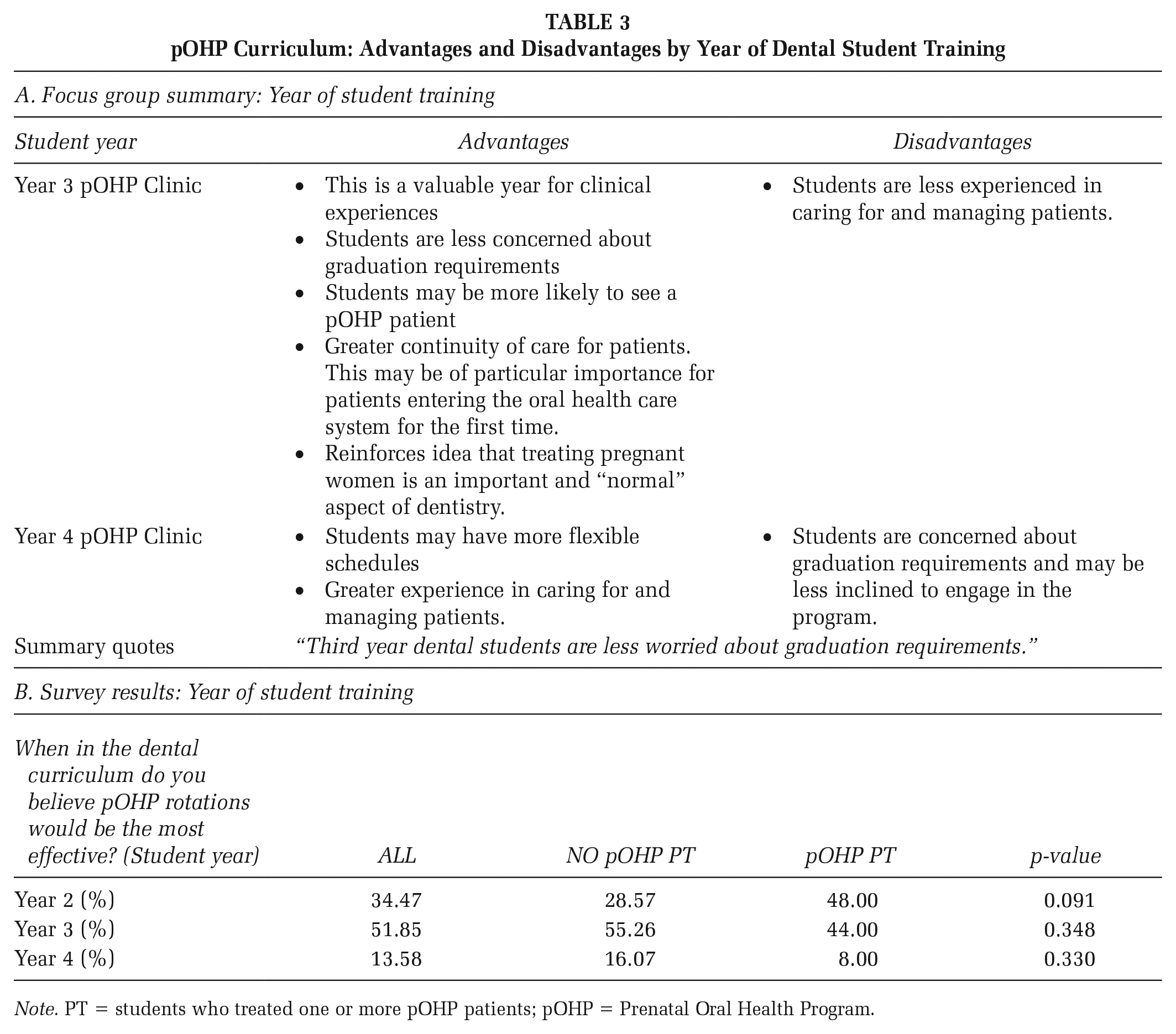
Note. PT = students who treated one or more pOHP patients; pOHP = Prenatal Oral Health Program.
Survey data revealed that most students agreed that D3 was the most effective time for a pOHP rotation (51.6%) as compared with the second (34.6%) or fourth (13.6%) years. Most students who provided care for a pregnant patient responded that pOHP would be most effective as a second-year rotation (48%) as compared with students who did not see a patient (28.6%) though there was no statistically significant difference (p = .09; Table 3B).
Patient Management Systems
Students were initially responsible for managing patient appointments. The pOHP was modified and utilized a PCC as a consistent point of contact and resource for patients and students. The PCC was bilingual (English and Spanish), which was necessary to support the full patient population. Focus group participants agreed that having a PCC supported efficiency. No additional costs were associated with the pOHP PCC, as roles were integrated as an extension of current duties.
When asked about perceptions regarding a PCC, most students felt neutral about the topic; however, students with a patient experience were significantly more likely to say that having a PCC was beneficial as compared with students who did not have a pOHP patient experience (PT 56% vs. NO PT 18.2%; p<.001; Table 4B). Most students who treated one or more pOHP patients were not in contact with the PCC (55.3%; Table 4B).
pOHP Management Systems: Advantages and Disadvantages of Inclusion of Patient Care Coordinator (PCC)
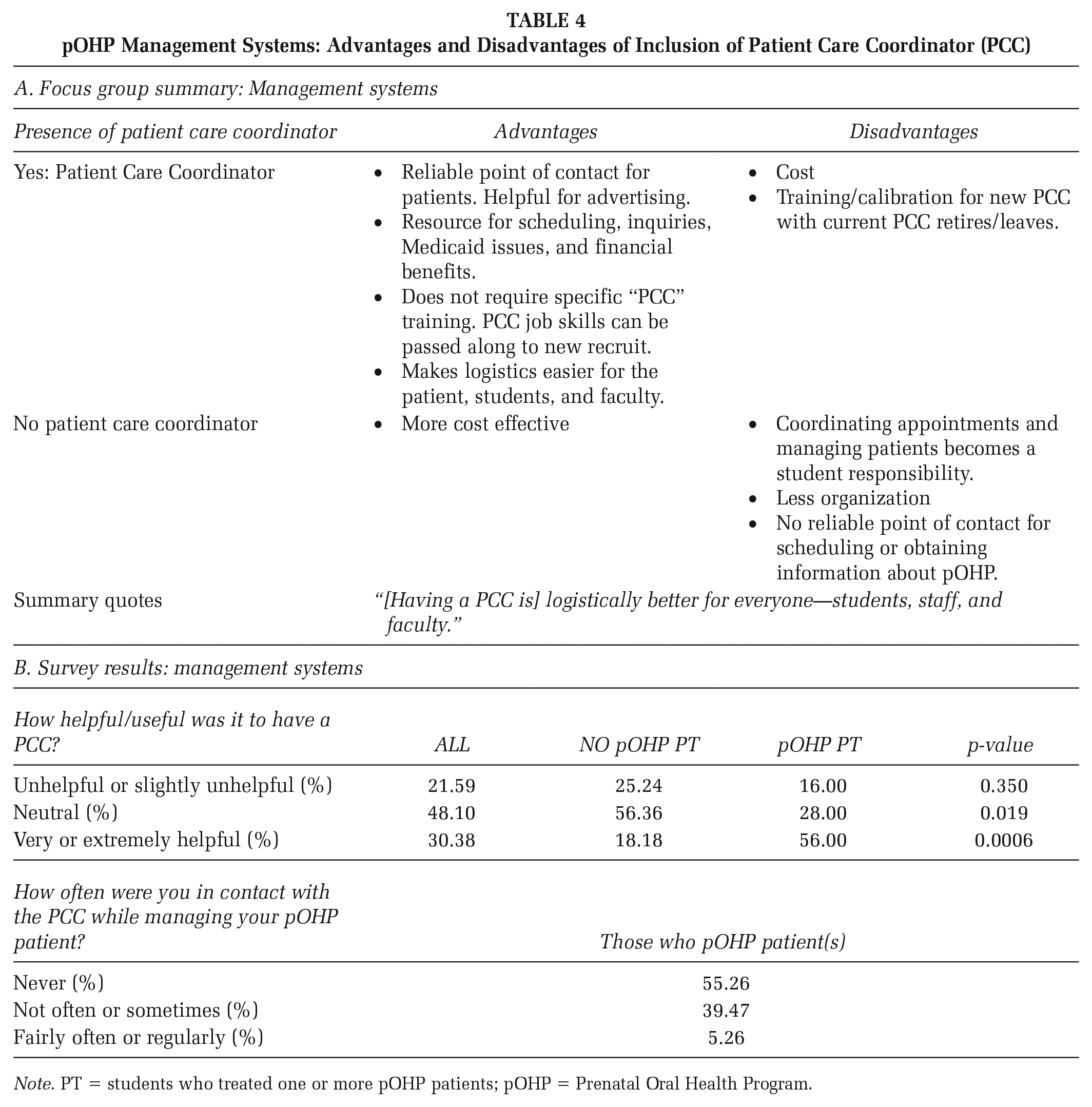
Note. PT = students who treated one or more pOHP patients; pOHP = Prenatal Oral Health Program.
Learning Styles
As part of pOHP, medical students and residents were instructed to screen, counsel, refer pregnant patients, and review prenatal oral health information and protocols regularly. Dental hygiene students learned to counsel, educate, and treat pregnant women alongside dental students. Focus group participants agreed that intra- and inter-professional experiences benefited pOHP, mainly when working with medically complex patients. Though participants supported these interprofessional experiences unanimously, barriers such as scheduling created challenges. Participants expressed optimism that curriculum innovation may increase interprofessional experiences. See the summary in Table 5A.
pOHP Learning Styles: Advantages and Disadvantages.
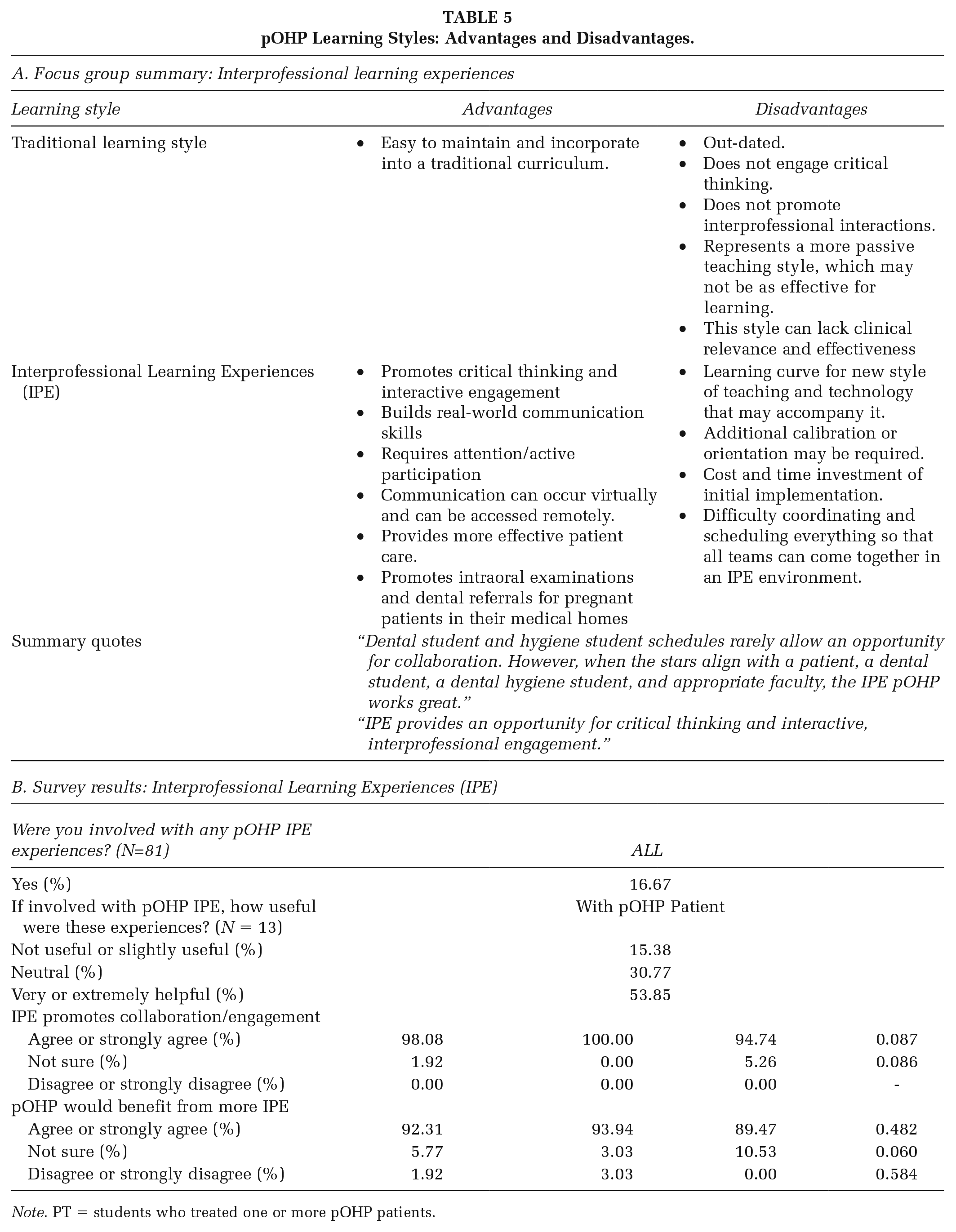
Note. PT = students who treated one or more pOHP patients.
Survey results indicated that 16.7% were involved in interprofessional experiences. Most agreed that experiences were very or extremely helpful (53.9%; Table 5B). Almost all students agreed that interprofessional experiences promoted collaboration and engagement (98.1%; Table 5B) and that pOHP would benefit from more integrated interprofessional opportunities (92.3%; Table 5B).
Program Educational Effectiveness
Most respondents rated their prenatal oral health training good or very good (74.1%). Students with patient experience were significantly more likely to rate their training as good or very good when compared with students who did not (PT 32.1% vs. NO PT 4%; p<.01), demonstrating the importance of clinical patient experiences in addition to didactic content (Table 6A).
Dental Student Ratings of pOHP Program Effectiveness
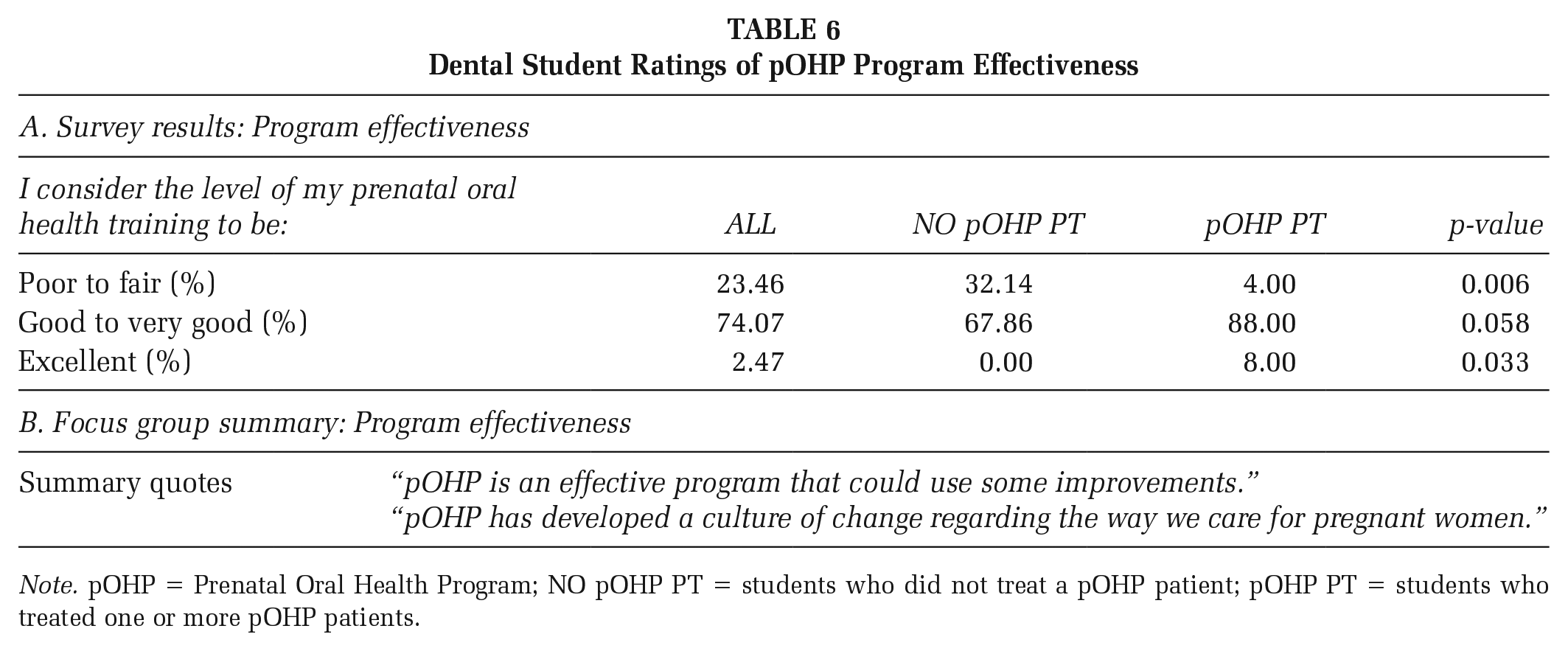
Note. pOHP = Prenatal Oral Health Program; NO pOHP PT = students who did not treat a pOHP patient; pOHP PT = students who treated one or more pOHP patients.
Focus group participants agreed pOHP was practical and should continue to advance (Table 6B). Participants agreed the most significant achievement was increasing access to care while simultaneously developing a culture of change about treating pregnant women. Participants discussed barriers that included full faculty engagement and patient barriers such as transportation, child care, and financial issues. The most significant obstacle was a lack of patients.
Discussion
Program evaluation data were gathered to support quality improvement in program implementation. Although data were collected in the fall of 2018, continuing and consistent academic challenges and educational considerations exist for allied health programs in university settings. The lessons learned from this report are applicable to the 2023 academic climate and remain relevant to curriculum and population needs.
A preference for an integrated model was noted. Previous research supports using standalone clinic models, particularly for weak health care systems or delivering complex services requiring a highly skilled workforce (Merzel & D’Afflitti, 2003). Standalone models are also beneficial to address priority populations’ needs that may be hard to reach. Though pregnant women, particularly those of low socioeconomic backgrounds, fall into this underserved category, preventive and standard operative dental services should not deviate from standard protocols. The initial standalone pOHP clinic required its structure and faculty, which was not sustainable.
Evidence supports integrated models for various clinical services, including managing patients with substance abuse, mental health, tuberculosis, and HIV (Church et al., 2013). An integrated model enhances the delivery of care with a lower number of unmet needs. When deciding whether to use an integrated or standalone clinical model, it is essential to consider school policies, planning, training, supervision, monitoring, and financial management (Waddington & Egger, 2008). Results suggest an integrated model is better suited for pOHP at UNC, though standardized training for all involved faculty is essential to ensure maximal consistency, effectiveness, and engagement.
The curricular timing of pOHP has shifted based on learner feedback and alignment with curriculum advancements. Earlier exposure to pOHP could result in more clinical opportunities, and it is well-known that early exposure and repeated reinforcement of knowledge results in improved learning and confidence (AlHaqwi & Taha, 2015; Ben-Gal et al., 2017; Dunham et al., 2017; Park et al., 2011). Though advantages and disadvantages exist simultaneously, previous research and current data favor D3 over D4. Most students who treated pOHP patients, compared with those who did not, were more likely to suggest second-year (D2) as the most effective pOHP rotation time. Rotation experiences reiterated that treating a pregnant woman should be no different from treating any other patient, and this rotation would be effective even earlier in the curriculum. Individual needs also impact optimal timing. Initial exams and preventive services may be better suited for D2 students, whereas D3 and D4 may be able to provide more comprehensive care and complex procedures.
Findings indicate that a PCC is vital for the highest efficiency of care. PCCs are commonly employed by clinical programs, increasing effectiveness and efficiency, providing a point of contact for patients, and a streamlined, consistent registration process (Bayard et al., 1997). The pOHP PCC was a critical point of contact linking patients, referring physicians, and students, promoting continuity of messaging, appointment scheduling, and follow-up. It also decreased students’ time completing paperwork, scheduling, and other non-educational administrative tasks reported to add stress and deduct from clinical learning (VanderWielen et al., 2015).
Implications for practice/policy
Increasing Interprofessional Collaboration
Oral health needs during pregnancy are best addressed with an interdisciplinary team adapting a specialized approach to care. The pOHP has progressed with changing curricula, adjusting to modern, collaborative, and forward-thinking teaching styles. The pOHP partnerships have expanded with local primary and obstetric physicians so they may provide women with a direct referral to pOHP services. This collaboration has increased oral examinations provided by medical providers and subsequent referrals, encouraging communication between dental and medical homes (Leone et al., 2017). As of January 2020, UNC School of Dentistry implemented a new dental record branch of the EPIC® medical record system shared by UNC health care network. This integrated electronic health records system has the potential to support pOHP by facilitating interprofessional communication and streamlining referrals from medical practitioners to dental providers. The extent EPIC is used for this purpose could be measured in the future.
As the findings from the data suggest, there is a need to continue implementing prenatal oral health learning opportunities in professional and health education programs using a team-based model. Pregnant women remain underserved in dental care, and academic challenges for resource allocation continue to drive curriculum and programmatic changes (Stephens et al., 2020). In addition, the criticality of interprofessional learning experiences continues to drive curricular changes that advance teaming and tailor care for person-centered treatment deliveries. Therefore, while data from this report are pre-COVID, the implications of these primary findings remain consistent with 2023 educational trends and population needs. Future studies will benefit from including various types of learners and practice structures.
Increasing Access to Care
The number of students with clinical experience was below optimum. Unfortunately, many referrals did not seek dental care. In 2016, <20% of North Carolina pregnant women visited the dentist during pregnancy, and 33% had active caries (Stephens et al., 2020). These statistics prompted a call to action for NC patients, providers, and policymakers to help resolve this public health issue.
Social determinants of health left unaddressed and adverse health policies contribute to oral health disparities. Out-of-pocket fees for costly services may discourage patients from seeking care, especially those who are uninsured or underinsured. At UNC, access to care may be limited by the social security number (SSN) requirement for all patients. Student clinics offer care for a broad community of patients, including some who may be undocumented. Requiring SSNs limits their access to care.
Future educational changes could include the implementation of external student rotations to community dental clinics, such as Federally Qualified Health Centers, that offer dental care to pregnant patients. Students who acquire experience caring for underserved populations gain an understanding of social responsibility, learn to address and conquer socioeconomic barriers, and are more likely to practice in underserved areas following graduation (Curtis et al., 2013; Ferguson et al., 2009; VanderWielen et al., 2015). Over 1,000 free clinics exist in the United States, offering medical, dental, pharmacy, and mental health services; and providing over 3.5 million medical and dental visits to over 1.8 million people (Darnell, 2010). Reassessing and reducing fees associated with pOHP or incorporating pOHP into a sliding-scale clinic may be necessary to enhance program participation from pregnant women with limited resources.
Policy Changes Needed
Limitations exist for pregnant women who qualify for Medicaid, as their dental coverage may end at delivery. Policy changes have recently occurred, including a 12-month extension of dental Medicaid coverage post-pregnancy in North Carolina (Eke et al., 2019; SB 105, 2020). Continued policy changes are necessary to improve the completion of care for enrolled women. Many other states only include emergency or minimal adult dental Medicaid coverage; an increase in dental coverage would benefit those residents. Increasing low dental Medicaid reimbursement rates would help increase low provider participation (National Institutes of Health, 2021; Stephens et al., 2020). In Michigan, dental hygienists can care for pregnant patients in the OB suite during prenatal appointments (Atchison et al., 2018). Workforce supervision regulations in other states inhibit this type of collaborative model.
Study Limitations
The primary goal of this quality improvement study was to gain feedback from program changes and hear reflections on what should stop, start, and continue in ongoing efforts for programmatic improvement. The authors intended to report on outcomes data from several PDSA cycles, yet this report focuses on pre-COVID-19 data. Multiple unforeseen challenges occurred that influenced the limitation of more current data. Of most significance, when the COVID-19 pandemic erupted, dental schools closed the student clinics, halting all patient care. Academic leadership had to change course on existing initiatives, refocus priorities on urgent needs in health and safety, and reimagine the curricular structure to support student success during a global pandemic. This critical redirection reduced the allocation of resources that would have been invested in a continued expansion of the pOHP clinical experiences. The reduction of resources limited faculty and staff distribution and clinical space for this project and delayed analysis and report writing.
Although efforts to rebuild this project are underway, there remains value in the pre-pandemic findings from this quality improvement project. The results presented in this report illustrate perspectives that are transferable to today’s educational climate. Barriers and challenges, such as clinical space and financial backing, remain consistent in implementing prenatal clinical learning experiences for dental and allied dental programs. IPE and appropriate leveling of content are also mainstays in the academic progression. This analysis provides additional and novel information on a program that has the potential to offer solutions to barriers that continue to exist in prenatal oral health promotion and education. Furthermore, the lessons learned during pOHP implementation may be applied to other clinical programs and initiatives, helping to enhance their effectiveness and impact.
Conclusion
In this article, the authors reviewed the evolving infrastructure of the novel pOHP. We found that pOHP functions best when integrated with the general dental clinic during the third year of dental school. We also found that pOHP benefits from interprofessional collaboration and having a PCC. Dental students who provided dental treatment to pregnant women reported their training to be better than those who did not have clinical experience. Based on the data generated from the PDSA cycle, a strategic priority is to explore ways to increase patient enrollment and decrease broken appointment rates. Although the data in this report are from pre-COVID, many of the same challenges continue to resonate with allied health academicians; hence the lessons learned still show relevance in today’s academic setting. The pOHP will continue implementing quality improvement efforts to enhance its quality and impact the prenatal patient population.
Footnotes
Authors’ Note:
The authors thank Abigail Shapiro (UNC Gillings Schools of Global Public Health), for mediating the focus group session, the focus group participants for their participation and assistance with program development over the years, and Monty Tellez for her coordination of pOHP.