
Abstract
Although menthol cigarettes are a starter product for youth, menthol was exempted from the 2009 Tobacco Control Act, which banned all other characterizing flavors. Minneapolis and Duluth, Minnesota, implemented menthol tobacco sales restrictions in 2018 to advance health equity for youth, African American, lesbian, gay, bisexual, trans, and queer (LGBTQ), and other communities adversely affected by menthol. This evaluation assesses the policy impact on youth access to menthol tobacco, exposure to menthol advertising, and tobacco use. A core group of youth aged 14 to 17 years (n = 30) was recruited from Minneapolis and Duluth to gather data through photo voice and peer interviews 2 months before and after policy implementation. This evaluation shares the results of focus groups with these core youth where they reflected on what they observed in the community and heard from peers. The core youth identified and categorized emergent themes using the evaluation questions. Following the focus groups, the evaluation staff used these preliminary themes and coded remaining transcripts. The core youth had mixed reactions to the impact of policies on access and use because many tobacco users in their age group obtain tobacco informally through peers, family members, and online. They observed decreases in retail advertising of menthol cigarettes, although many felt e-cigarettes and online advertising were more significant issues for their age group. Findings show a need for increased education and more comprehensive policy approaches, including addressing use of flavored e-cigarettes, online tobacco sales, and informal access, making youth access to tobacco more difficult.
Background
Menthol cigarettes are a known starter product for youth (Hersey et al., 2006). The majority of tobacco users begin smoking in adolescence and with menthol cigarettes (Villanti, Collins, et al., 2017). According to the 2013–2014 Population Assessment of Tobacco and Health study, 59.5% of youth smokers (ages 12–17 years) used menthol cigarettes compared with 37.1% of adult smokers (Villanti, Johnson, et al., 2017). Youth uptake of menthol cigarettes is particularly concerning because youth who smoke menthol cigarettes smoke more frequently and report higher intentions to continue smoking versus youth who smoke nonmenthol products (Azagba et al., 2020). African American (Giovino et al., 2013) and lesbian, gay, bisexual, trans, and queer (LGBTQ) youth (Fallin et al., 2015) are more likely to smoke menthol cigarettes compared with youth smokers in other racial/ethnic groups and heterosexual smokers.
Because flavors in cigarettes appeal to youth, the 2009 Family Smoking Prevention and Tobacco Control Act banned the sale of fruit- and candy-flavored cigarettes; however, menthol-flavored cigarettes were exempted (Center for Tobacco Products, 2009). The cooling sensation and anesthetic effect of menthol makes cigarette smoking more palatable for first-time users. Research shows the tobacco industry manipulated menthol levels to attract and retain youth smokers (Klausner, 2011; Kreslake et al., 2008). Recent data indicate that menthol-flavored e-cigarettes have also gained popularity among youth (Cullen, 2018).
The World Health Organization recommends that menthol cigarettes be banned, given their public health impact (World Health Organization, 2016). In the absence of federal U.S. regulation of menthol cigarettes, local jurisdictions enacted sales restrictions. In 2018, the cities of Minneapolis and Duluth, Minnesota, implemented some of the first ordinances in the country restricting menthol tobacco sales. Menthol tobacco can no longer be sold in convenience stores, groceries, pharmacies, and other retail stores. Although exemptions were made for adult-only tobacco stores in Duluth, and for adult-only tobacco and liquor stores in Minneapolis, the number of outlets where menthol can be sold was significantly limited. The goal of these policies is “to reduce the number of outlets where these products are available, prevent youth from being exposed to seductive tobacco industry marketing, and encourage adults to make a quit attempt” (ClearWay Minnesota & Center for Prevention at Blue Cross and Blue Shield of Minnesota, 2019). This is especially important, given the tobacco industry’s targeting of menthol and its role in exacerbating tobacco-related health disparities among many Black, Indigenous, and other people of color and LGBTQ communities. Although these menthol restrictions apply only to tobacco sales, it is plausible that tobacco marketing may also be affected. For example, advertising and promotions are associated with greater susceptibility and increased smoking initiation among youth (Paynter & Edwards, 2009; Slater et al., 2007).
Menthol sales restrictions in the United States began in 2015 and continue to grow with limited published evidence about the impact of these restrictions, particularly among youth. Evaluation of flavored tobacco sales restrictions (exempting menthol) in New York City found significant declines in the odds of ever trying flavored tobacco or using any type of tobacco among teens between 2010 and 2013 (Farley & Johns, 2017). Other research, from jurisdictions outside the United States, found menthol bans can be effective in reducing menthol sales and tobacco use among adults (Chaiton et al., 2018; Soule et al., 2019). However, there is a need to further document how menthol sales restrictions affect youth smokers and youth perceptions of menthol sales restriction policies.
Purpose
The passage of restrictions in Minneapolis (passed August 4, 2017, implemented August 1, 2018) and Duluth (passed January 22, 2018, implemented June 12, 2018) created an opportunity to evaluate changes in youth perceptions and behaviors on access to menthol tobacco and tobacco product marketing. This study addresses the following evaluation questions:
Evaluation Question 1 (EQ1): What are the changes to youth access to menthol tobacco following policy implementation?
Evaluation Question 2 (EQ2): What are the changes to youth exposure to menthol tobacco advertising following policy implementation?
Evaluation Question 3 (EQ3): What are the changes to youth use of tobacco following policy implementation?
Method
Participants
For this evaluation, a pretest–postest design was used following a youth participatory framework, grounded in the belief that youth are experts in their own lives, experiences, and communities, and when they are given opportunities to shape evaluation processes, the authenticity of the evaluation in reflecting the lived experiences of youth improves (Sabo Flores, 2007). Similarly, to ensure that the voices of youth populations targeted by menthol advertising were included in this evaluation, participants were recruited at community-based organizations that work with LGBTQ youth and youth of color. Evaluation staff presented the purpose and study methods to potential participants aged 14 to 17 years at three youth-serving agencies in Duluth and four in Minneapolis. A core group of 30 youth (hereafter referred to as “core youth”) enrolled in the study. Because only a small percentage (3.9%) of high school students report past 30-day menthol cigarette use (Minnesota Department of Health, 2019), both smokers and nonsmokers were eligible to participate. Core youth either were a resident or enrolled in a school located in Minneapolis (n = 19) or Duluth (n = 11).
Procedure and Youth Participation
In alignment with youth participatory practices (Couch et al., 2014; Harper & Carver, 2016), core youth were trained in research methods and participated in cocreating study protocols with the evaluation staff. Core youth were compensated at a rate of US$50 per reflective focus group (described in the following; totaling five to six meetings). All core youth across the three Duluth agencies met together for the duration of the project. Based on program timing and site-specific needs, core youth from each of the four Minneapolis partnering agencies met separately. Partnering with youth-serving agencies helped in the recruitment of participants, provided convenient meeting space and project coordination, as staff at each of the agencies coordinated transportation, handled parent communication, and were present at meetings to foster core youth engagement.
During prepolicy data collection (April–May 2018 in Duluth; June–July 2018 in Minneapolis), core youth completed a short survey, conducted peer interviews, and captured photo documentation of menthol tobacco in their communities. The core youth survey included questions on demographics, tobacco use, and ease of access. The peer interviews included questions about smoking behavior, access points for menthol tobacco, perceptions of ease of access, and awareness of menthol advertising. Each core youth was instructed to interview two to four peers, resulting in a total of 228 peer youth across Duluth (n = 101) and Minneapolis (n = 127). This process was repeated 2 months postpolicy implementation (July–August 2018 in Duluth; October–November 2018 in Minneapolis). Evaluation staff also facilitated reflective 90-minute focus groups with core youth (two prepolicy and two postpolicy). The focus group guide included questions to engage core youth in sharing their experiences, reflections from their peer interviews, and community photo-voice observations. This evaluation focuses on the qualitative findings gained from the reflective focus groups with core youth (quantitative peer interview data will be reported separately).
Analysis
Meetings with the reflective focus groups participants, in which core youth recounted their interviews and data collection activities, were audio-recorded, transcribed verbatim, and uploaded to NVivo 12 Pro (www.qsrinternational.com), a qualitative data management software, to facilitate analysis. Analysis was guided by the DEPICT model for participatory qualitative health promotion research, which emphasizes a process for community members most affected by an issue being studied to cocreate the code book and guide analysis (Flicker & Nixon, 2015). In the reflective focus groups, evaluation staff utilized a modified DEPICT model in which all core youth participants collectively reviewed their collected data and identified and categorized emergent themes, using the evaluation questions as a guide. Two members of the evaluation team used this as the preliminary coding list and coded all remaining transcripts. Emerging themes and subthemes were then identified from the data. A framework matrix was generated with core youth quotes representing each key theme. Findings were synthesized and selected quotes were identified for reporting. This study received IRB determination as nonhuman subjects research through the Minnesota Department of Health.
Results
Participant Characteristics
The core youth in Duluth (n = 11) were primarily White (58%), compared with Minneapolis (n = 19), where the majority of core youth were African American (78%). Just more than half of all core youth were female (63%), 13% identified as LGB+ and 27% reported ever using tobacco.
Major Themes
Themes from the focus groups are organized by each research question, first with themes from prepolicy implementation discussions followed by themes from postpolicy implementation discussions.
Youth Access: Prepolicy Implementation
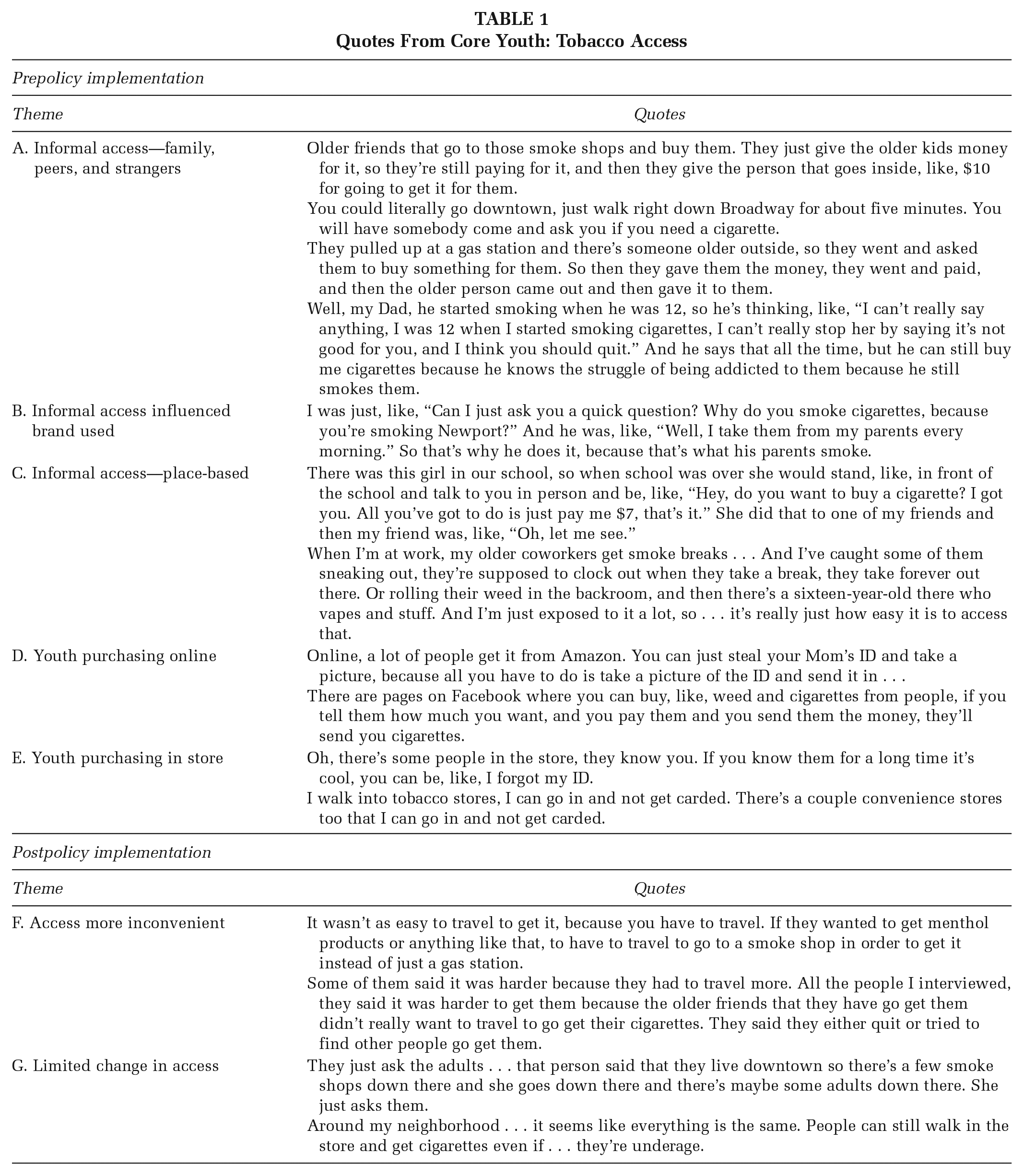
See Table 1 for representative quotes from core youth.
A. Informal access—family, peers, and strangers: Most core youth reflected that they and their peers obtained tobacco through informal means, such as family members, friends and strangers whom they approached. For example, a common source of access to tobacco was school peers and other friends; this included asking older friends to purchase tobacco. Youth also reported that many people within their age group accessed tobacco by buying “loosies” (single cigarettes) from strangers in public or asking strangers to purchase tobacco for them. Other youth described the complex relationship some family members have with tobacco as contributing to access for young people (Table 1A).
B. Informal access influenced brand used: Core youth described how access through family and friends influenced brand use among their peers; they use the same brand as the family/friends who helped them access tobacco, specifically Newport, which was mentioned repeatedly (Table 1B).
C. Informal access; place-based: Core youth also discussed how their peers informally obtain tobacco on or around school grounds and youth workplaces (Table 1C).
D. Youth purchasing online: Core youth also reported that purchasing tobacco (particularly e-cigarettes) online was another common and easy source of tobacco. The most common sites named were Amazon, eBay, Facebook Marketplace, and Instagram. Online age restrictions can easily be bypassed, by using parents’ credit cards (Table 1D).
E. Youth purchasing in store: Less frequently, core youth discussed purchasing tobacco in person at corner stores, gas stations, and tobacco shops. They described having familiar connections with people who work in these stores, intentionally building trust with employees, by coming in often with older people who can legally purchase tobacco or flirting with store employees. In addition, core youth reported knowing which stores do not routinely check IDs; they indicated that smaller, independently owned locations were more likely to sell to underage youth directly than chain stores (Table 1E).
Quotes From Core Youth: Tobacco Access
Youth Access: Postpolicy Implementation
In focus groups, youth in Duluth and Minneapolis had a range of reactions to changes in access following policy implementation.
F. Access more inconvenient: Core youth indicated that the menthol restrictions are causing an inconvenience for their peers who smoke menthol cigarettes because of additional travel needed to purchase, either for themselves or those purchasing for them (Table 1F).
G. Limited change in access: Other core youth shared that because many of the peers they interviewed reported that they and their peers vaped and already accessed these products through informal means, they had not yet experienced a significant reduction in access to menthol tobacco following the restrictions. Those who were already illegally purchasing from tobacco shops were continuing to do so and, although convenience stores could no longer legally sell menthol tobacco, some youth knew of corner stores that would continue selling to regular customers (Table 1G).
Advertising: Prepolicy Implementation
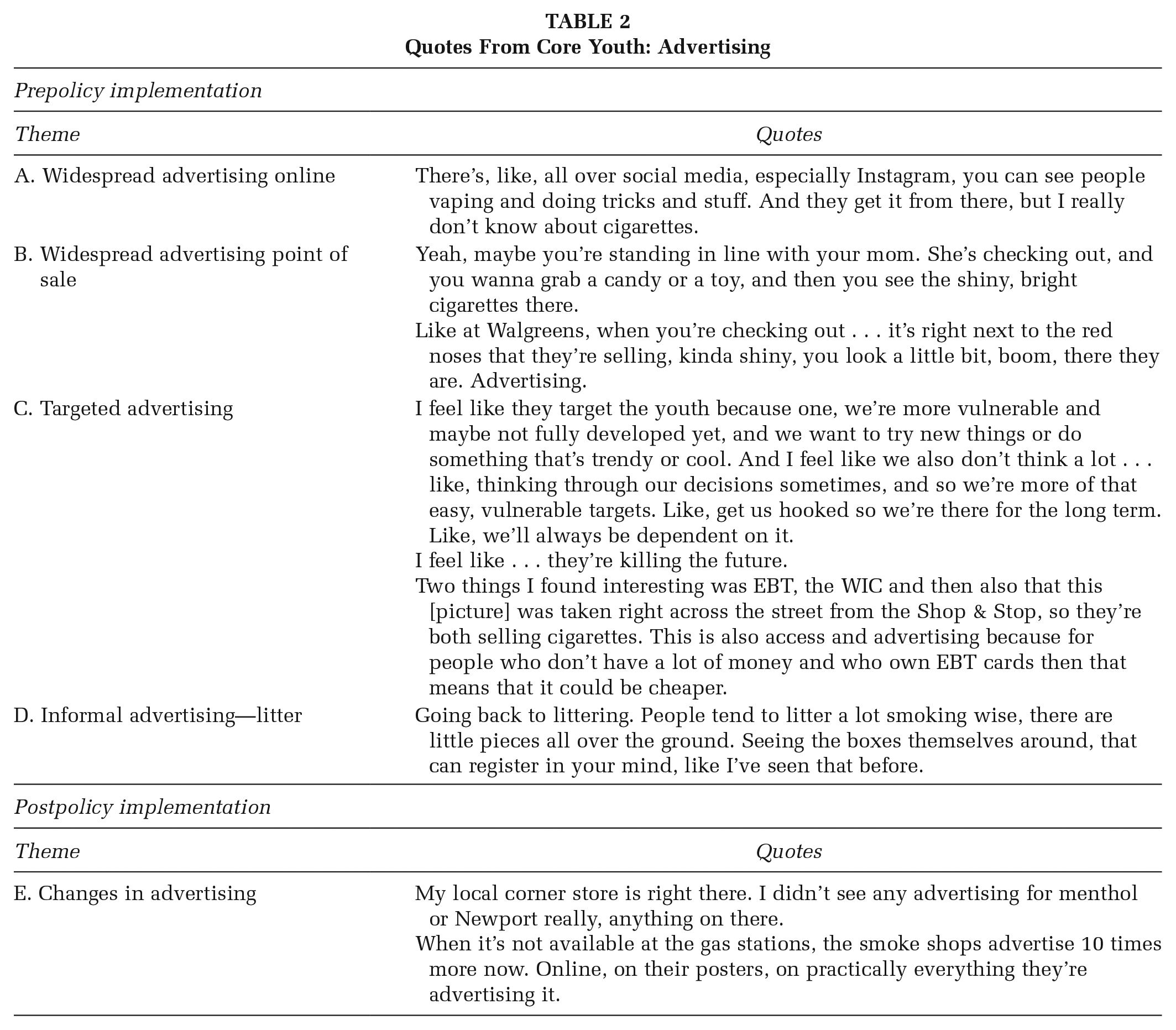
See Table 2 for representative quotes from core youth.
Widespread advertising online: After observing and photographing menthol advertising, the core youth noted that tobacco advertising on social media (particularly Facebook, Instagram, and Snapchat) was widespread, especially for e-cigarettes. Common social media advertising approaches were either paid advertising, or “tricks” using tobacco products, which often became viral challenges. Examples of this include vaping in school without getting caught or making smoke rings (Table 2A).
Widespread advertising at point of sale: Youth reported seeing a large number of physical ads within their communities, in locations such as gas stations and corner stores as well as sandwich board signs on sidewalks. The frequency and intensity of ads at the point-of-sale was also mentioned by core youth (Table 2B).
Targeted advertising: Core youth recognized that some of the ads were specifically intended to get youth attention. They also observed that some of the corner stores that sell tobacco also accept Women, Infants, and Children (WIC) and Electronic Benefits Transfer (EBT) modes of payment. The youth recognized this as targeting individuals with low income (Table 2C).
Informal advertising—litter: Finally, core youth identified butt and carton litter as an informal type of advertisement—particularly as it collected in community locations and was repeatedly for the same few brands, including Newport (Table 2D).
Quotes From Core Youth: Advertising
Advertising: Postpolicy Implementation
Decreases in advertising were observed where sales were restricted after the policy was implemented but not at other locations or online.
E. Changes in store advertising: Core youth reported observing differences in menthol advertising following policy implementation, with fewer menthol ads in corner stores or gas stations, and significant increases in menthol advertising from tobacco shops that continue to sell menthol tobacco (Table 2E).
There were no reported changes in online advertising following the policy implementations.
Youth Tobacco Use: Prepolicy Implementation
Overall, 26.7% of core youth participants indicated they had ever used any tobacco, with (23.3%) reporting they used e-cigarettes (also described as “vape” or JUUL), compared with 16.7% who had ever smoked cigarettes, and 13.3% who had ever smoked cigars or cigarillos. In Duluth, more core youth participants reported using e-cigarettes (27.3%) than cigarettes (9.1%), whereas in Minneapolis participants reported equal prior use of e-cigarettes and cigarettes (21.1%; Table 3).
Core Youth Participant Demographics and Smoking Characteristics (n = 30)
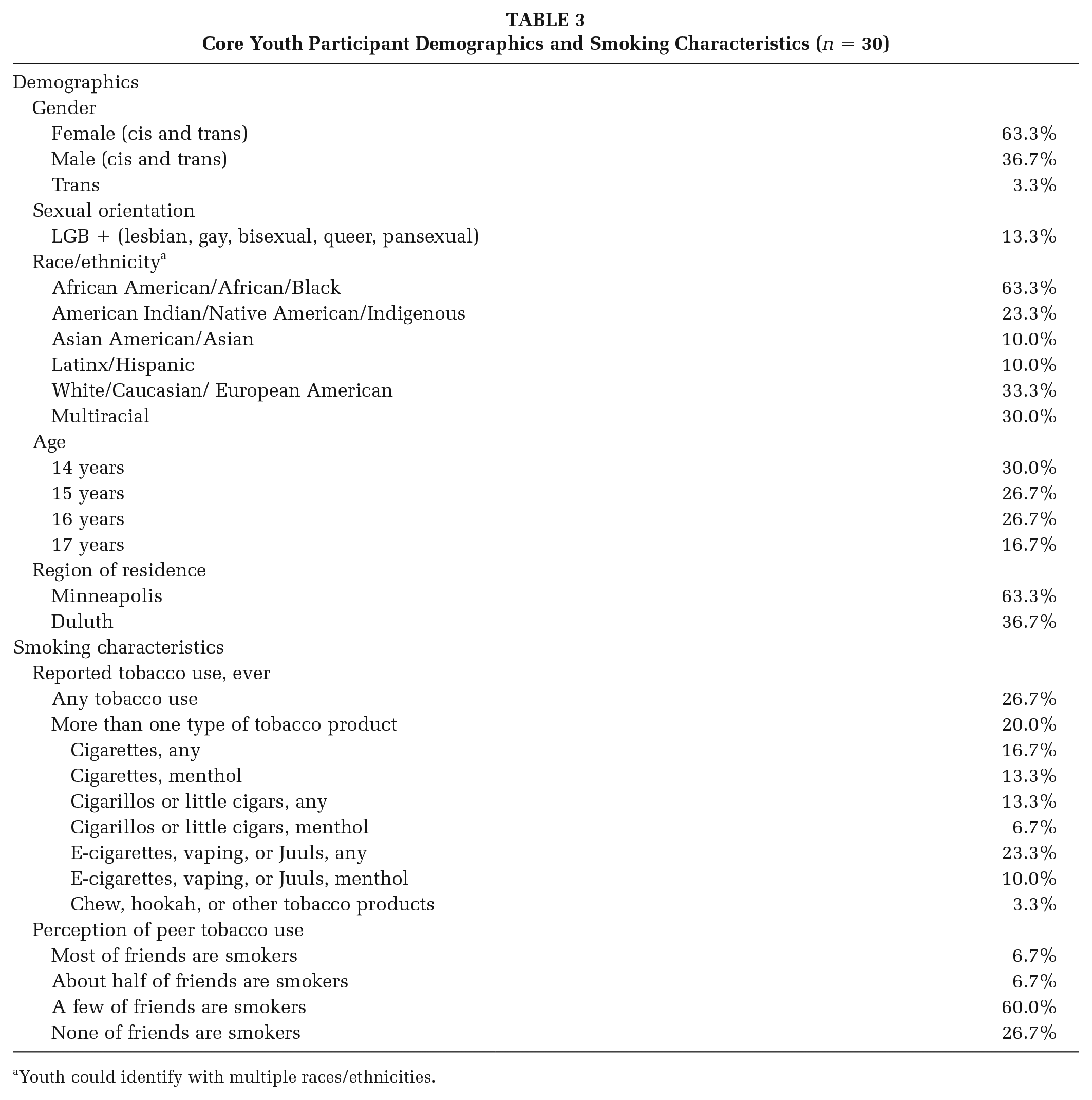
Youth could identify with multiple races/ethnicities.
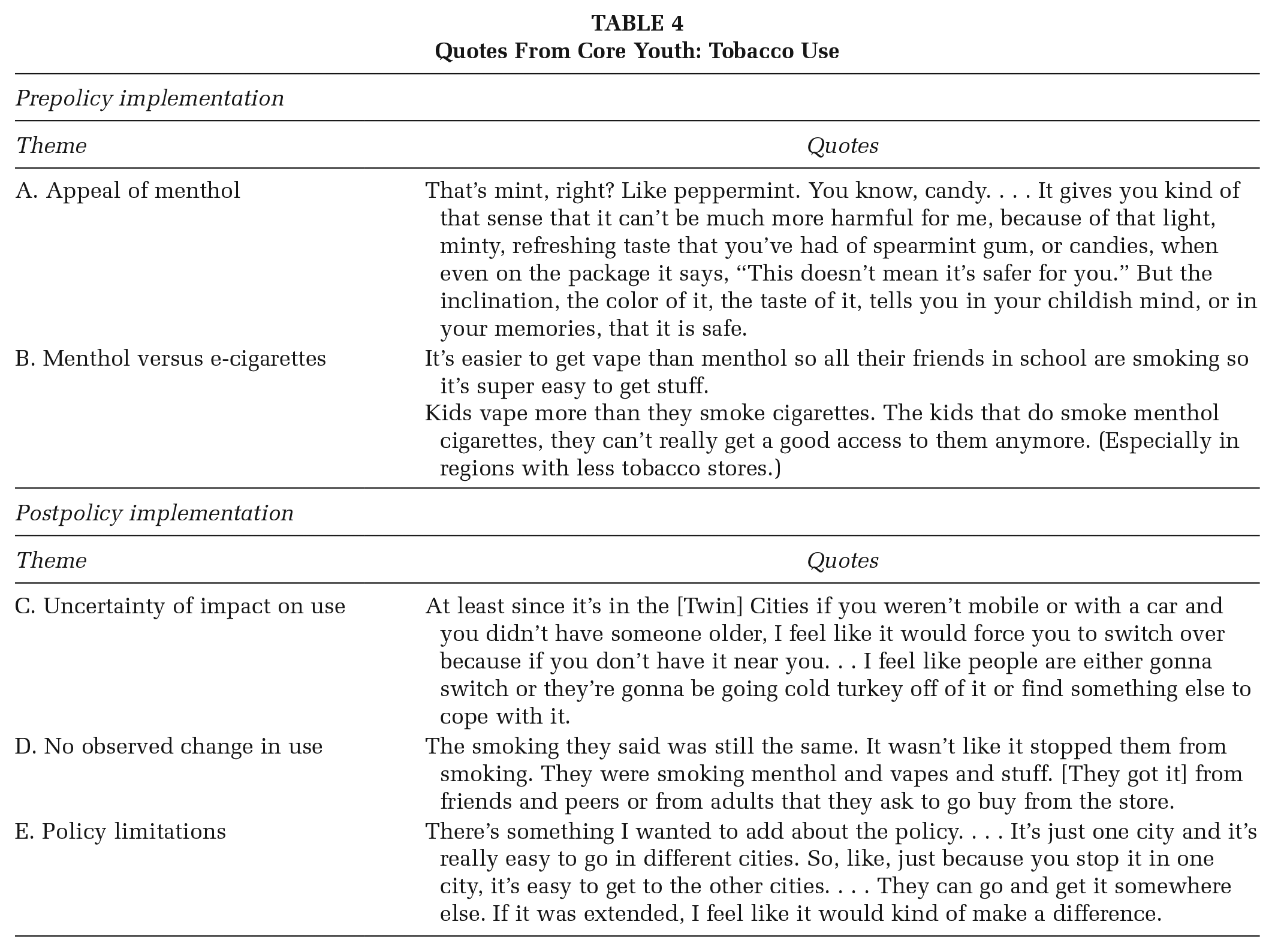
See Table 4 for representative quotes from core youth.
Appeal of menthol: Some participants felt menthol had a particular appeal to their age group because of the unique sensation or “buzz” menthol tobacco products have. One participant made the connection to how menthol tobacco may contribute to reduced risk perceptions among young people (Table 4A).
Menthol versus e-cigarettes: Core youth reported more vaping than smoking among their peers because access to cigarettes is becoming more difficult. Some participants discussed vaping and menthol (cigarette) use as distinct preferences, perhaps not aware that menthol is a specific flavor not only for cigarettes but also for e-cigarettes (Table 4B).
Quotes From Core Youth: Tobacco Use
Youth Tobacco Use: Postpolicy Implementation
Youth had mixed responses about the impact of policy implementation on youth tobacco use.
C. Uncertainty of impact on use: Some core youth were uncertain of the impact on peer tobacco use following policy implementation. Some felt that, although it might influence certain menthol tobacco users to quit, it also had the potential to encourage switching to other products that were more easily available (Table 4C).
D. No observed change in use: Other core youth reported not seeing a change in smoking habits, as a result of underage smokers already accessing tobacco through informal means (Table 4D).
E. Policy limitations: In addition, there was the feeling among some of the core youth that effects on tobacco use may be limited because the policy was implemented in localities (vs. more widespread, such as a statewide menthol restriction) and in many cases youth regularly navigated between localities with menthol restriction policies and localities without menthol restrictions (Table 4E).
Discussion
This evaluation focused specifically on youth and their perspectives related to sales restrictions of menthol tobacco. There is moderate evidence demonstrating significant observed reductions in store-level flavored tobacco availability in communities with sales restrictions of these products (Rogers et al., 2021). However, the perceived impact of the policies on access was limited in our study, potentially because many of the youth are not accessing tobacco products directly from retailers, but rather accessing through informal, unregulated means, including online. For example, core youth reported that tobacco users in their age group regularly access menthol tobacco through peers, a finding supported by the 2019 Minnesota Student Survey, which found 72.3% of 11th-grade and 71.0% of eighth-grade e-cigarette users obtained their e-cigarettes from friends. Similarly, in previous research, youth expressed perceived limited impact of existing tobacco laws that limit access as they believe they can easily acquire tobacco by circumventing the laws, such as getting someone older to buy for them (Crawford et al., 2002).
Participants reported exposure to tobacco advertising both online and at the retail locations they visited. The core youth discussed seeing online promotion of tobacco through paid advertisements on social media and through youth-created content that normalizes or promotes tobacco. In addition to online exposure, core youth also noticed large amounts of advertising at retail locations prior to policy implementation. As anticipated, youth observed that menthol advertising decreased in (physical) places not allowed to sell menthol, following policy implementation, but did not notice a similar reduction in advertising online or in retail places that were allowed to continue menthol sales. This finding aligns with existing evidence that suggests tobacco retailers in locations with comparable policies are less likely to have advertising of flavored products compared with those without these policies (Rogers et al., 2021). Given the postpolicy reduction in retail store advertising and the strong association between tobacco advertising and youth tobacco use (policies restricting the sale of menthol tobacco have the potential to reduce both exposure to advertising and use for youth and other populations, including LGBTQ communities and communities of color who are targeted by menthol advertising. These impacts could be furthered by regulating online advertising.
Youth expressed unlimited or uncertain impact of policy on tobacco use behaviors. Some felt the policy could encourage users to quit or switch to other products. Previous research found similarly uncertain perceived impact of such a policy on use as some youth reported they would switch to nonmenthol cigarettes if there was a ban on menthol, whereas others indicated it might help them quit (D’Silva et al., 2021; O’Connor et al., 2012; Wackowski et al., 2018). However, current overall evidence for increased quit intentions and attempts due to laws restricting the sale of menthol tobacco is low (Rogers et al., 2021).
Youth participants perceived that vaping was a more pressing tobacco-related concern than menthol cigarette use, which is not surprising given that nationwide (Gentzke, 2020), and in Minnesota (Minnesota Department of Health, 2019), youth report using e-cigarettes at much higher rates than combustible products such as cigarettes. Relatedly, they discussed vaping and menthol (cigarette) use as distinct preferences. Youth and adult smokers do not always realize or identify the cigarettes they are using as menthols (Brennan et al., 2015; D’Silva et al., 2021), which may also be the case for e-cigarettes. Yet youth perception of limited use of menthol-flavored vaping products among peers is in contrast to recent data indicating increasing popularity among youth nationwide (Cullen, 2018). Despite this evidence, because the youth in this study did not necessarily think of themselves or their peers as menthol product users, this perception may have played a role in their awareness of policy impact. Thus, more education within this age group around the use and harms of menthol-flavored tobacco may be needed to increase awareness.
Although the restrictions of menthol sales were constrained to geographical borders, these distinctions were different from the lived experience of how youth think about and define their communities; youth often navigate their communities in ways that are not aligned or constrained by actual city boundaries. Likely, this is similar to how adults navigate city borders as one study found that some young adult tobacco users living in a city with menthol-flavored restrictions purchased tobacco from retailers outside the city (Yang et al., 2020). Thus, to have greater impact, menthol restriction policies should be implemented at the state and/or federal level.
Limitations
Postpolicy data were collected 2 months after policy implementation. Two months may be insufficient time for youth to become aware of the policy, depending on how they access tobacco, or for the policy to have affected smoking behaviors. During the postimplementation interviews, Minneapolis passed an ordinance restricting tobacco sales of tobacco to anyone below the age of 21 years. This policy may have affected our findings related to informal access.
Implications for practice
This evaluation of youth perceptions of menthol policy restrictions revealed there is a need for increased education and comprehensive policy approaches to make access to tobacco more difficult through a variety of channels. Comprehensive approaches to menthol policy restrictions may include actions such as internet sales regulation, limiting targeted advertising to youth online—particularly through social media, policies without tobacco outlet or other retailer exemptions, and policies covering wide (and not just city-by-city) geographical areas. Together, these comprehensive policy approaches and increased education may further the effectiveness of policies that prevent youth use of menthol tobacco.
Future studies should quantitatively analyze youth prevalence of menthol tobacco before and after policy implementation to provide additional insight into their effectiveness on reducing youth use of menthol tobacco, including e-cigarettes. Longitudinal analyses of these or similar policies can reveal potential long-term impacts. Furthermore, these analyses should look at differences across demographic groups to determine whether there are differential policy impacts for communities most adversely affected by menthol tobacco use. Finally, as much of youth access is through informal means, evaluating the impact of Tobacco-21 policies on informal access will determine how a comprehensive policy approach can influence youth use overall.
Footnotes
Acknowledgements
The authors acknowledge the contributions of Selam Tilahun, Beki Saito, Mary McEathron, and the Minnesota Menthol Evaluation Advisory Group. They also thank the advocates in Duluth and Minneapolis for their ongoing efforts to keep our young people healthy and improve the health and lives of our communities. Finally, they gratefully acknowledge the staff at the participating youth-serving agencies and the youth participants who entrusted them with their stories.
Tobacco in this document refers to manufactured commercial tobacco products, and not to the sacred, medicinal, and traditional tobacco use by American Indian people and other groups. This study was funded by ClearWay Minnesota and the Center for Prevention at Blue Cross and Blue Shield of Minnesota (Blue Cross). Support was also provided in part by Truth Initiative. The information contained herein does not necessarily reflect the views and opinions of the Truth Initiative.
No financial disclosures were reported by the authors of this article.