
Abstract
Physical activity (PA) is important for managing osteoarthritis (OA), but many patients are inactive. Research is needed on strategies to leverage clinical encounters to engage patients in PA. Guided by the socioecological model of health behavior, this study aimed to engage stakeholders in the process of refining an Osteoarthritis Physical Activity Care Pathway (OA-PCP). Six focus groups and seven individual interviews were conducted with key stakeholders. Focus groups were specific to stakeholder roles and included patients with OA, support partners, and clinic personnel (n = 6 focus groups). Interview participants were local and national PA program representatives (n = 7 interviews). Data were analyzed by thematic analysis. Themes identified in the data included ways the OA-PCP can help patients with OA address challenges to PA engagement, strategies for connecting patients with PA resources, methods for implementing OA-PCP into clinical settings and potential use of PA trackers in the OA-PCP program. Stakeholders’ comments were summarized into key recommendations for OA-PCP. Some recommendations reinforced and led to refinements in planned aspects of OA-PCP, including tailoring to individual patients, involvement of a support partner, and addressing pain with PA. Other recommendations resulted in larger changes for OA-PCP, including the addition of three email- or mail-based contacts and not requiring use of a PA tracker. The refined OA-PCP program is being evaluated in an exploratory trial, with the ultimate goal of establishing a PA program for OA that can be successfully implemented in clinical settings.
Keywords
Background
Osteoarthritis (OA) is a leading cause of pain and disability worldwide (GBD 2015 DALYs & HALE Collaborators, 2016). Physical activity (PA) is an evidence-based, first line strategy for managing OA (Bannuru et al., 2019; Kolasinski et al., 2020; Nelson et al., 2014; Uthman et al., 2013). Unfortunately, the majority of individuals with OA are physically inactive, with only about 10% meeting PA guidelines (Song et al., 2013). Primary care settings, where most patients with OA are regularly treated, present an excellent opportunity to intervene and set patients on a path toward increased PA (AuYoung et al., 2016). Yet evidence shows that providers often fail to discuss PA during conversations with patients about OA management (Do et al., 2011; Hootman et al., 2018; Hunter et al., 2011). There is some evidence for the efficacy of primary care-based PA interventions (AuYoung et al., 2016; Estabrooks & Glasgow, 2006; Heath et al., 2012; Orrow et al., 2012), but no studies have focused on patients with OA, who face specific challenges such as pain, fatigue, and functional limitations. In addition, OA is commonly comorbid with other chronic conditions, such as obesity and hypertension (Caporali et al., 2005; Lementowski & Zelicof, 2008), which can improve with increased PA. Engaging OA patients in PA could have positive benefits for patients in their management of comorbid conditions in addition to OA (Centers for Disease Control and Prevention, 2009, 2011; Sandoval-Rosario et al., 2018).
The present study is informed by the socioecological model, a conceptual framework that describes different levels at which it is possible to intervene to enhance healthy behaviors (McLeroy et al., 1988; Sallis et al., 2006). The levels are often presented as concentric circles, with the innermost circle being intrapersonal factors that are specific to individuals such as knowledge and attitudes, and each progressively larger circle representing wider spheres of social influence, including interpersonal relationships, organizational and community factors, and public policy. Research has shown that interventions that target multiple levels of the socioecological model are more effective than those that target only the intra or interpersonal levels (Kellou et al., 2014). The present study describes the development of a primary care–based intervention to increase PA among people with OA by addressing multiple socioecological levels in order to change patients’ PA behaviors. The socioecological model guided the selection of intervention strategies, which include PA counseling (individual/interpersonal levels), clinic-based PA screening (organizational level), linkage to PA programs (community level), and building evidence for PA initiatives in primary care (public policy level).
Aims
The overall goal of the OA Physical activity Care Pathway (OA-PCP) study is to develop and test a primary care-focused intervention to engage patients with OA in PA. The first aim of this study was to engage key stakeholders representing different levels of the socioecological model, including patients with OA, their support partners, primary care clinicians, and representatives from clinical and community-based PA programs in the process of developing the OA-PCP. This article describes the methods and results of qualitative work to incorporate stakeholder feedback in the development of OA-PCP in preparation for a clinical trial.
Method
This study was reviewed and approved by the institutional review board of the University of North Carolina at Chapel Hill.
Participants and Recruitment
Focus Groups
We aimed to conduct two focus groups each with patients with OA and their spouses or support partners. We also planned to conduct two focus groups with clinical personnel at two different primary care clinics that are part of the North Carolina Network Consortium. One clinic was in a rural area (Clinic 1) and one was in an urban area (Clinic 2). Potentially eligible patients were identified from University of North Carolina electronic medical records, followed by telephone screening. Support partners were referred to the study by OA participants and were invited to participate in focus groups separate from the patients with OA. Inclusion and exclusion criteria for patients and support partners are shown in Table 1. We also conducted focus groups with primary care clinic personnel at each clinic. All clinical and administrative personnel were invited to participate in order to include staff with a variety of roles.
Inclusion and Exclusion Criteria for Patients With OA and Support Partners
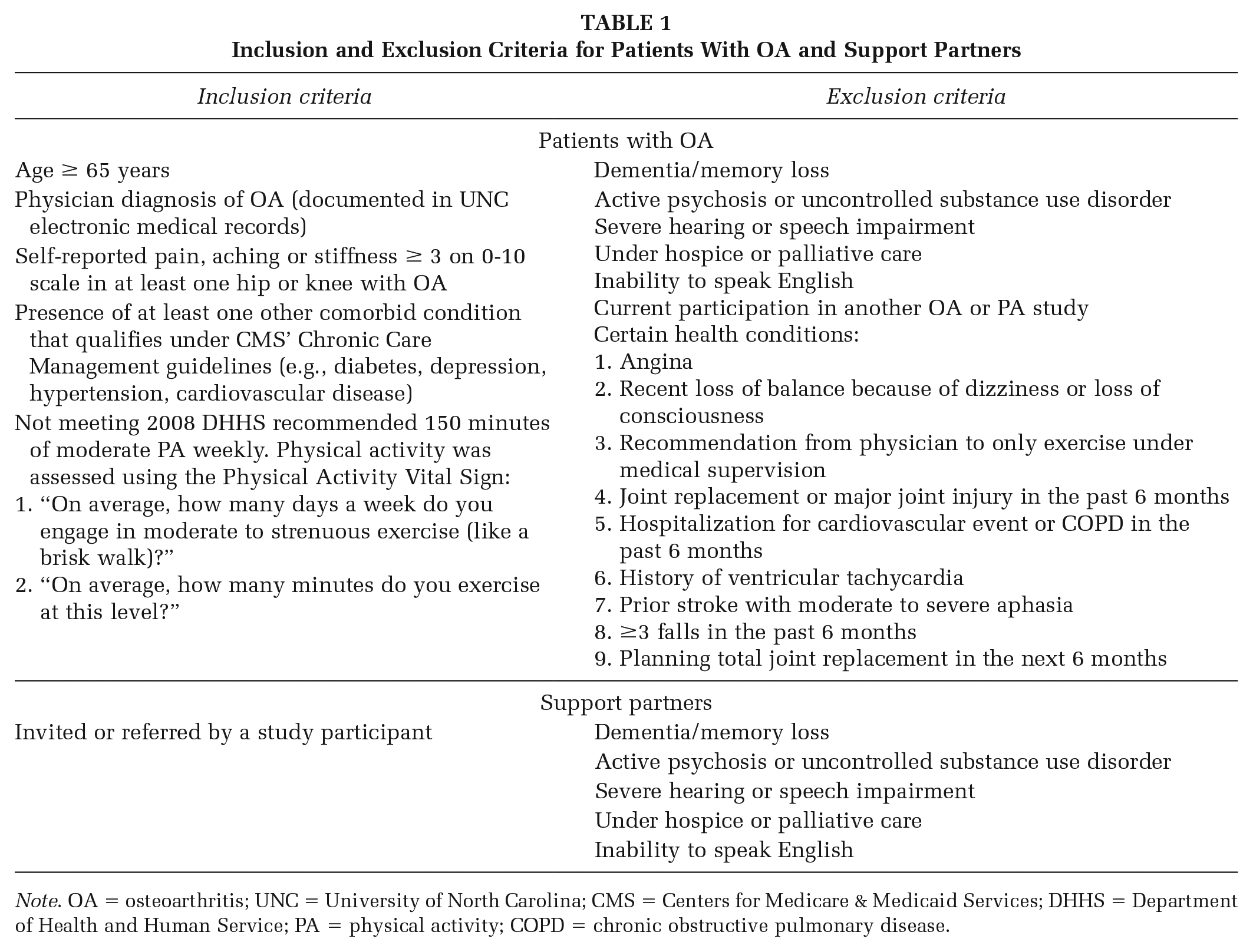
Note. OA = osteoarthritis; UNC = University of North Carolina; CMS = Centers for Medicare & Medicaid Services; DHHS = Department of Health and Human Service; PA = physical activity; COPD = chronic obstructive pulmonary disease.
Individual Interviews
We recruited representatives from clinical and community-based PA programs for individual telephone interviews. Representatives were identified through our existing contacts with local organizations, a systematic search of local PA programs, and recommendations from the Osteoarthritis Action Alliance (https://oaaction.unc.edu).
Data Collection
Focus groups for patients, spouses or support partners, and clinic personnel were held at their respective clinic locations. Individual interviews with representatives from PA programs were conducted by telephone. Focus groups and interviews were conducted by a senior PhD trained qualitative researcher (MV) and master level research team member with qualitative experience (KH). Neither interviewers had prior relationships with the participants which facilitated candid discussions.
During each focus group and interview, the facilitator described the OA-PCP model, using the model shown in Figure 1. The OA-PCP is based on a previously developed, general primary care-based PA intervention (Boehler et al., 2011; Bull & Milton, 2010). The socioecological model–informed intervention aims to incorporate individual, interpersonal, organizational, and community components and includes: (a) brief PA screening, using the two-item Physical Activity Vital Sign measure (Coleman et al., 2012; Joseph et al., 2016; Young et al., 2014), (b) a brief telephone-based PA counseling session, (c) a 2-week check-in call from the counselor to address questions and review progress toward PA goals, (d) linkage of participants with preferred PA resources and programs (facilitated by the PA counselor), and (e) a 3-month follow-up call from the PA counselor to review participants’ goals, barriers, and engagement with PA programs or resources. Content of the counseling calls is tailored based on participants’ readiness to engage in PA (Prochaska & DiClemente, 1982; Williams & French, 2011).
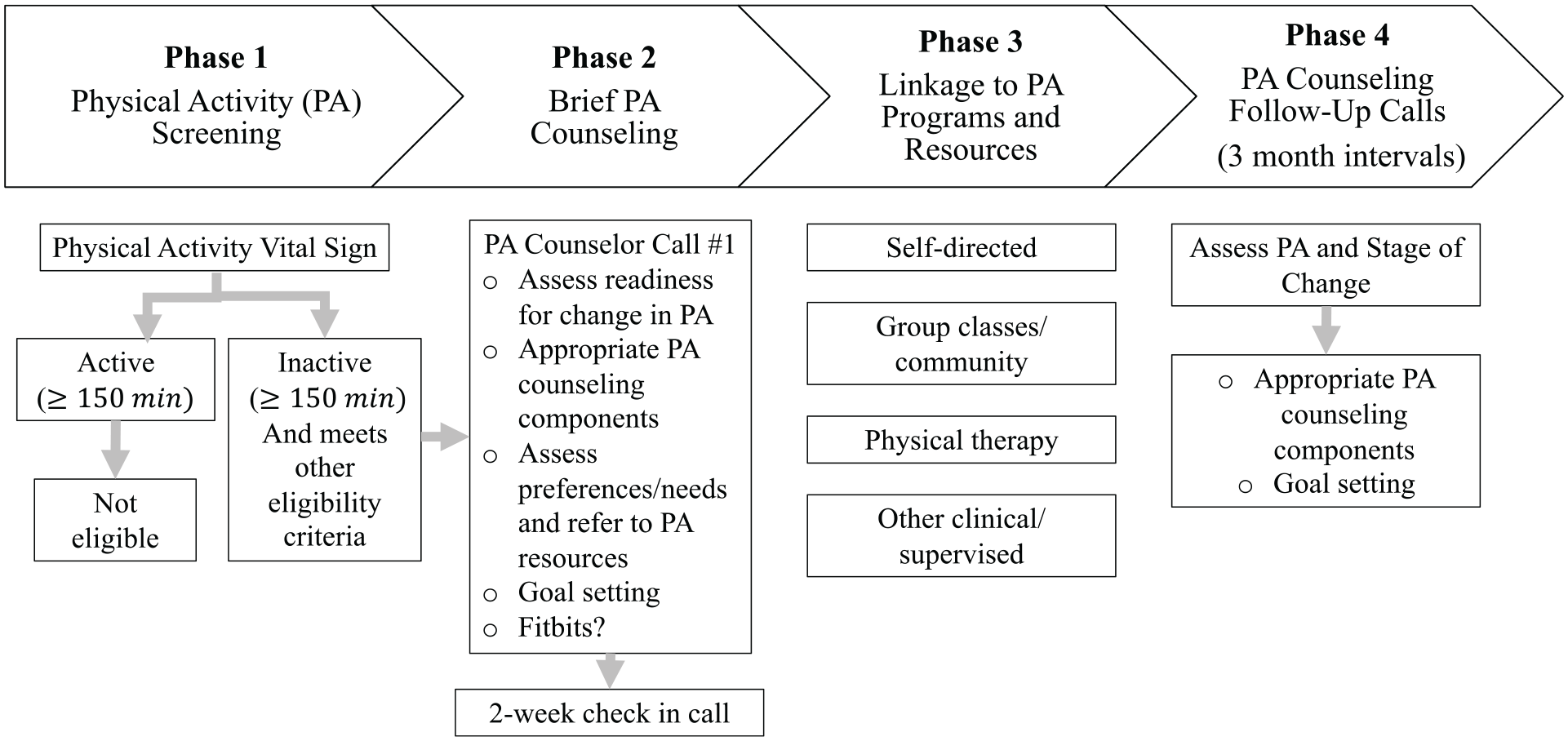
Osteoarthritis Physical Activity Care Pathway
Overlapping focus group and interview topics included: challenges to PA for patients with OA and ways the OA-PCP can address these, strategies for connecting patients with PA resources, methods for implementing PA screening in primary care settings, and patients’ interest in using activity trackers (e.g., Fitbits) as part of the OA-PCP program. Focus groups and interviews were audio-recorded for subsequent analysis. Patients, spouses or support partners, and PA program representatives received $75, and each participating clinic received $500. Focus groups and interviews were conducted from September to November 2018.
Analysis
The overall analytic strategy was selected to align with the goal of identifying important adaptations for the OA-PCP program. Audio recordings were reviewed with notes taken during the discussions to assure accuracy and completeness. Key point summary forms capturing main topics and emerging ideas were completed by interviewers (MV and KH) and imported into ATLAS.ti 7.5.18 (Scientific Software Development GmbH), a qualitative software program to facilitate analysis. Separate codebooks were created to analyze data from the focus group discussions and interviews. To enhance trustworthiness, all analyses were conducted independently with no input from sponsors and the lead for analysis had no competing interests (MV). A senior qualitative researcher (MV) with extensive experience developed topical codes from the interview guides (e.g., barriers to support and clinic integration) and participants’ words (e.g., credibility, safety). An inductive approach as described by Strauss and Corbin (1990) was used for codes that emerged on rereading (e.g., values, social opportunities). An audit log of decisions was kept along with codes arising from the focus groups and interviews. We then grouped codes into emergent themes and relationships after iterative reading of the transcripts and discussion with the research team. Because the focus groups and interviews evaluated a similar set of topics, we pooled the qualitative data for the final summarization of findings and chose quotes representative of each theme. This allowed for both emergent and anticipated themes.
Results
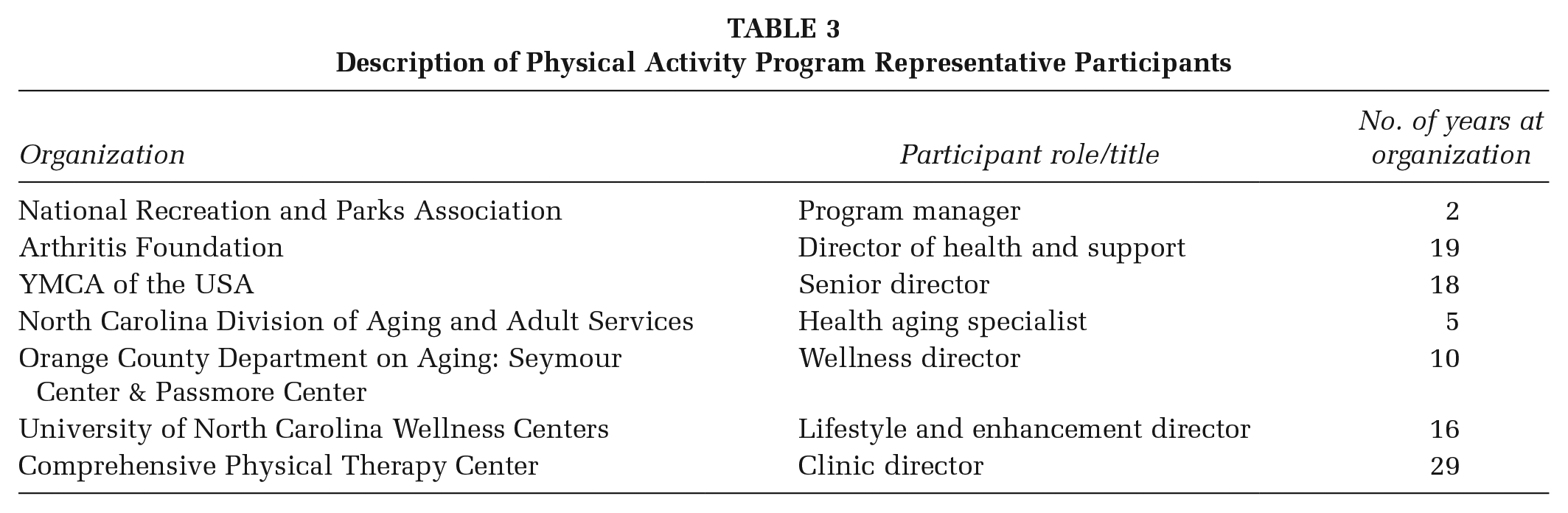
We conducted six focus groups with a total of 13 patients with OA, 10 spouses or support partners, and 18 clinic personnel. Demographic characteristics for the patients and support partners are presented in Table 2. Interviews were conducted with seven representatives from PA programs; their organizations and roles are listed in Table 3.
Focus Group Participant Demographics
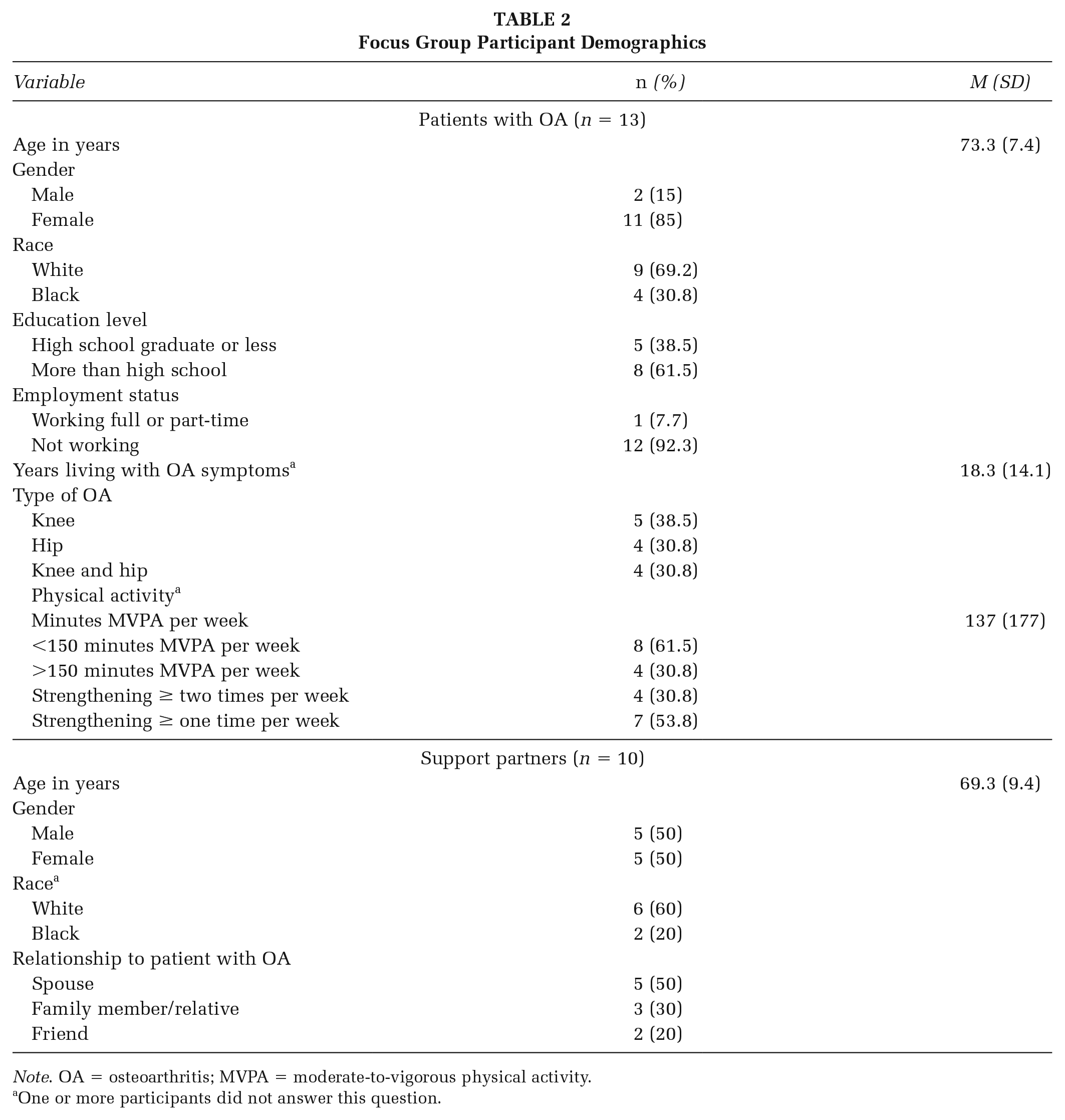
Note. OA = osteoarthritis; MVPA = moderate-to-vigorous physical activity.
One or more participants did not answer this question.
Description of Physical Activity Program Representative Participants
We conducted a qualitative analysis of discussions across focus groups and individual interviews to summarize participants’ feedback on the OA-PCP. The following key recommendations, along with illustrative quotes and additional supporting data, emerged from these stakeholders. For each recommendation, we summarize actions taken by the study team in response to this feedback.
Recommendation 1: Hire a Highly Qualified PA Counselor
There were strong sentiments across stakeholders that the PA counselor plays a critical role to the success of this program, as they are the link between the patients and community organizations. Stakeholders said having a genuine interest in working with patients and feeling confident in this role was more important than a background in health or physical therapy. One patient explained that the PA counselor should be a “cheerleader” and genuinely interested in helping them because “If you are into the job, I connect. If you are just into the paycheck [I can tell].” A PA Program Representative noted, “Your program is going to be as successful as the strength and robustness of the resources, including human resources, that you have.”
These comments highlighted the importance of rigorous training of PA counselors. Training procedures will include written and verbal instruction on OA-PCP, followed by multiple practice calls that are reviewed by an experienced study team member.
Recommendation 2: Tailor the Program to Each Patient’s Health and PA Levels
Stakeholders felt that a “one size fits all” model would not work for patients with OA. They indicated it is important to consider patients’ other health conditions and tailor recommendations to their specific needs. For example, a support partner emphasized that some patients may have more functional limitations than others, so giving all patients the same PA recommendations would not be appropriate. They said, “Find out what are the patient’s limitations and share this with the PA coach, so that during the first call the PA coach has some credibility and is not making inappropriate referrals.” Some stakeholders also expressed a preference for paper vs. online resources. As one patient explained, “I am on the computer maybe once a week.” Another patient noted, “For the non-exerciser, it’s hard to get the right form from an online video.” Offering resources in nondigital formats and tailoring delivery based on patient preferences could be important factors in patient engagement with PA resources.
The need for tailoring the OA-PCP for individual patients was also illustrated by differences in what motived participants to engage in PA. One patient noted What motivates me a lot of times is that I do not want to be on a walker . . . So, when I see those people, [who] have much worse health problems than me, it makes me say, “I gotta keep going.”
A PA program representative offered, “If you can reach people on an individual basis and get an idea about what’s important to them and then turn that around and use that as a motivator, I think that’s powerful.”
Stakeholders’ comments on this topic reinforced the planned approach to tailor OA-PCP content based on patients’ health status, PA preferences and stage of change. While most OA-PCP contacts will be conducted via telephone, delivery of some components will be based on patient preferences (email vs. postal mail). The study team ensured that PA resource guides included a variety of programs ranging from online to in-person (see Supplemental Material for example).
Recommendation 3: Provide Optional Activity Trackers
Stakeholders’ comments were mixed regarding the use of activity trackers. Only a small number of patients had used activity trackers, but most said they were “open-minded” and willing to try it because it “could help mentally.” Ease of use was cited as being important. For example, one patient said, “I . . . would try it but make sure everything is already set up,” Some participants noted that comfort with technology may be an issue for older patients, but assistance from the PA counselor could help to overcome this challenge. Some stakeholders recommended using pedometers, which are simpler but still provide instant tracking information. Other concerns regarding activity trackers included their usefulness for people who are already aware of their activity levels and their ability to measure different types of activity. Some stakeholders noted that there may not be one right approach regarding the use of activity trackers, and this can be based on patient preference. A clinician noted, “I think it can go both ways. We have some older folks that would say, ‘what is this device? I’m not wearing it.’ But I also have some that use it as motivation.”
Based on mixed feedback on the utility of using activity trackers in OA-PCP and concerns about the technological aspects in this patient group, the study team decided to not require the use of these devices. Instead, the PA counselor will work with individuals to consider how they can use any tools they currently own (e.g., smartphone, activity tracker) to monitor progress toward goals.
Recommendation 4: Highlight PA as a Safe Strategy to Protect Joints and Reduce Pain
Stakeholders noted that many patients with OA are concerned about increasing pain, and it is essential to highlight that being active will not cause more damage. Stakeholders also expressed a need for information on how to exercise without increasing pain. One patient noted, “Showing the benefits [of PA], even a little can help a lot and more importantly, let them know that being active CAN NOT hurt you,” Similarly, a clinician made the suggestion to “Share information about the direct link between exercise and the pain relief they could receive,” This recommendation supported the planned approach to include information on the safety of PA for patients with OA. Stakeholders’ comments were used to fine-tune the content for the first call with the OA-PCP counselor and the accompanying patient handout.
Recommendation 5: Build in Multiple Contacts With the PA Counselor
Stakeholders said that it could be beneficial to patients to have contact with the PA every few weeks. One suggestion was to reach back to patients in an email or text, since a patient commented that “Going from two weeks to not hearing again [until the 3-month check-in call] is too long,” This would also be an opportunity for the counselor to acknowledge successes and challenges and re-motivate those experiencing issues. A PA program representative explained, “Touch points . . . are critical to keep people from falling off. I like to focus on what’s going well. How do you do more of that . . .? So you don’t set up more obstacles.”
We added a series of three emails or letters to participants, between the 2-week and 3-month calls. These additional contacts include a reminder of each participant’s PA goals, tips for increasing lifestyle PA, review of the benefits of PA, and tips for dealing with pain that occurs during or after PA.
Recommendation 6: Create a Team Approach, but Ultimately Hold the Patient Accountable
Stakeholders described the intertwined roles that the PA counselor, partner and patient play in the OA-PCP; they recommended a model of “shared responsibility” so it feels like a team. Stakeholders viewed the counselor role as important for helping patients set realistic goals. Stakeholders said it was important for the counselor to involve support partners early in the process of talking about activity levels and goals. One PA program representative said, “In that conversation of goal setting and talking about behavior change, ask ‘who can help you with that?”’ This could provide a change for the PA patient to identify an important support person to help them stay active. In a focus group with support partners, one partner explained: “I’d like to hear what [the PA counselor] is suggesting so I can encourage [my partner] to do it so I can be there and encourage her to at least try.” Support partners also expressed the importance of having patients decide who they want to engage in this process.
Stakeholders noted that the PA counselor’s role should be to hold the patient accountable for engaging in PA. One support partner emphasized the need for the counselor to set clear expectations for the patient at the end of each call. They said, “[The PA coach can say] Ok, when I talk to you next time . . . My mom has to have that extra push,” A PA program representative offered the recommendation to “focus on making the patient feel accountable for their own health.”
Partner involvement is encouraged as an optional component of OA-PCP, aligning with participant feedback. Patients’ “accountability” is a major focus of the goal-setting process. The study team reviewed and modified PA counseling call scripts to ensure that patient accountability was clearly communicated. For example, call scripts included a reminder (at the end of the call) that the PA coach would be asking participants about their progress toward activity goals at the next call.
Recommendation 7: Clinic Personnel Should Deliver the Program
Stakeholders shared that some practices have a “point person” like a dietitian who spends individual time with patients. Therefore, adding PA to those conversations would be one way to integrate OA-PCP into a practice setting. Clinicians also recommended having clinic staff give patients a PA screening form to complete, leading to a “hand off” to a counselor. Although stakeholders thought it was important to involve clinic personnel in OA-PCP, another key message was that providers and practice staff lack time to discuss PA. Clinicians said that without enough time to address PA levels, “most of the time we are just throwing a sheet at them and they are not going to do it.”
For logistical reasons, PA screening in the initial exploratory trial of OA-PCP is being conducted by the study team. However, the eventual goal is for PA screening to be conducted in the clinic, which aligns with these stakeholder recommendations. We also aim for OA-PCP to ultimately be delivered by embedded clinic personnel, such as a chronic care manager or dietician. Stakeholders’ comments on this topic reinforced this approach, as well as the need to limit the amount of time required by primary care providers.
Recommendation 8: Emphasize the Link Between Primary Care Providers and the PA Program
Stakeholders said it was important to know their providers endorsed this program. They felt it was more legitimate if the providers were involved and offered it as an option to improve their health. For instance, with regard to the focus group, one patient said, “That’s the reason I am here, because Dr. X told me about it.” A PA program representative suggested, “Help [the PA counselor] to be set up as a credible support to the physician,” Based on this feedback, we added language at the beginning of the first PA counseling call describing the OA-PCP as a partnership with the patient’s primary care provider.
Recommendation 9: Work With Local Organizations to Identify Community-Based PA Programs
Stakeholders noted the importance of knowing what was available in the area so that any recommendations would be up to date. Stakeholders also said having a “locator” to centralize PA resources and programs would be valuable because the PA counselor would know the details of the programs. A clinic expert offered, “Have a list of all of the physical activity programs and senior centers [available], and dividing it by where they live could be really helpful.”
The study team created detailed PA resource guides, which are tailored to different geographic locations and include a variety of programs (e.g., online, self-directed, in-person). In-person programs included different settings such as general fitness centers, senior centers, YMCAs, and Parks and Recreation programs. These will be provided to participants at the beginning of OA-PCP.
Discussion
We conducted a comprehensive qualitative exploration of multiple groups of stakeholders in the process of refining a PA intervention for patients with OA, with a view toward integrating the program within primary care settings. As highlighted in the socioecological model (McLeroy et al., 1988; Sallis et al., 2006), health behaviors are influenced by factors occurring at multiple levels, including individual, interpersonal, organizational (e.g., primary care clinic) and community. Therefore, we sought feedback on the OA-PCP program from representatives from each of these levels. The resulting recommendations facilitated the refinement of the OA-PCP program across multiple levels of the socioecological model. Recommendations 1 to 6 are pertinent to the individual and interpersonal levels and the counseling aspect of the program. These recommendations focus on characteristics of the counselor, and patients’ individual needs and communication preferences. Recommendations 7 to 8 focus on the organizational level, describing the importance of incorporating clinic personnel into program delivery. Recommendation 9 centers on the community level by focusing on community-based resources offered in the program. Overall, the intention of the OA-PCP program is to build evidence for best practices for enhancing PA in this population, which could influence the policy level of the socioecological model by creating support for health care policies that emphasize integration of PA interventions in primary care settings.
Some recommendations from stakeholders reinforced aspects or components that were already planned for the OA-PCP program. Examples of this included the emphasis on tailoring the intervention based on individuals’ needs and preferences, involvement of support partners and connection of patients with existing PA programs and resources. In these cases, we made minor modifications (described above) to address specific recommendations of stakeholders. There were also several recommendations that resulted in more substantial changes to the OA-PCP program. First, stakeholders emphasized the importance of health care provider endorsement of the OA-PCP program; though primary care providers typically have limited time for PA counseling, they have an important role in giving a “credible” recommendation to engage in PA (AuYoung et al., 2016; Grandes et al., 2009). To address this feedback, we added language to the PA counselor scripts that emphasizes partnership with the patient’s primary care provider. Second, stakeholders thought patients would benefit from additional contacts with the PA counselor. The study team considered this recommendation alongside the goal of developing a program that can be implemented feasibly in primary care settings, where personnel resources are limited. To address these competing priorities, we added three emails or letters between the 2-week and 3-month phone calls, to provide encouragement, reminders on patients’ specific goals and tips for reducing pain during or after PA. Third, stakeholders provided mixed feedback on the use of activity trackers with some expressing reservation about dealing with the technology. Based on this feedback, activity trackers are not being given as part of the pilot study of OA-PCP, but the PA counselor will work participants to explore methods for activity monitoring, based on their preferences.
Limitations
This study involved patient, partner, and clinical stakeholders from two clinics within one health system, which may limit generalizability. The average physical activity level of patients was relatively high, which may have influenced perspectives on the OA-PCP program; however, our sample still included patients with a wide range of PA levels, with some reporting 0 minutes of weekly moderate-to-vigorous activity. The majority of participants (85%) were female, and the low proportion of males may have limited the male perspective on aspects of OA-PCP.
Implications for Practice and Research
Information obtained from this project directly informed modifications to the OA-PCP program. This is a first step in our long-term goal to test and implement this program widely in clinical settings. Findings from this study can also inform other research and practice efforts related to clinic-based PA programs. Specifically, others seeking to support PA among patients with OA can implement these stakeholder recommendations, particularly emphasizing patient-centered tailoring, engagement of support partners and connections with primary care providers as well as community-based programs.
Supplemental Material
OA-PCP_PA_Resource_Guide_Durham – Supplemental material for Developing a Primary Care–Focused Intervention to Engage Patients With Osteoarthritis in Physical Activity: A Stakeholder Engagement Qualitative Study
Supplemental material, OA-PCP_PA_Resource_Guide_Durham for Developing a Primary Care–Focused Intervention to Engage Patients With Osteoarthritis in Physical Activity: A Stakeholder Engagement Qualitative Study by Ida Griesemer, Maihan B. Vu, Leigh F. Callahan, Rebecca Cleveland, Yvonne M. Golightly, Kimberlea Grimm, Katie Huffman, Amanda E. Nelson, Jennifer Rees and Kelli Allen in Health Promotion Practice
Footnotes
Authors’ Note:
The authors have no conflicts of interest to disclose. Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number R21AG056568. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Drs. Allen, Callahan, Cleveland, Golightly, and Nelson are supported by the NIAMS Core Center for Clinical Research (P30AR072580). Dr. Allen is supported by the VA HSR&D Center of Innovation to Accelerate Discovery and Practice Transformation (CIN 13-410).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.