
Abstract
Several studies suggest that the quality of the therapeutic relationship (TR) between the patient and their therapist plays a significant role in predicting the outcomes of various forms of psychotherapy. However, it remains unclear whether the TR also influences the outcomes of treatment programs for justice-involved populations. Therefore, this systematic review aims to identify the impact of the TR on treatment outcomes with justice-involved individuals. A comprehensive search was conducted in B-on, Scopus, Web of Science, PubMed, PsycInfo, and Scielo for peer-reviewed quantitative studies providing data on individuals who committed crimes, available in English, Portuguese, or Spanish. A total of 18 studies that met the inclusion criteria were included in the final synthesis. Most of the included studies comprised predominantly male samples convicted of sexual offenses or intimate partner violence–related crimes. Regarding therapists, both genders were represented, along with a diversity of academic backgrounds. In terms of effectiveness, the findings suggest that the TR may exert a stronger influence on proximal, intrapersonal outcomes—such as motivation to change and well-being—than on more distal, behavioral outcomes, including aggression or recidivism. However, the existing studies are scarce and present several methodological limitations. Although the findings suggest the relevance of considering therapists and their training as potential responsivity factors in treatment, further research is needed to draw firm conclusions.
Keywords
Introduction
Over the past few decades, numerous psychotherapies have emerged and evolved, including many evidence-based approaches supported by structured treatment manuals demonstrating effectiveness across a range of mental health conditions (e.g., Alkan et al., 2025; Liu et al., 2023). In this regard, the predominant approaches used with individuals who have committed crimes have also evolved over the years, showing positive effects (e.g., Beaudry et al., 2021; Cunha, Pereira, et al., 2024; Koehler & Lösel, 2024; Sousa et al., 2022; Sousa, Gonçalves, et al., 2025; Sousa, Gouveia, Cunha, et al., 2024). However, challenges such as treatment dropout and lack of patient response persist, and these difficulties are often even more pronounced within populations who committed crimes (e.g., Cunha, Pedrosa, et al., 2024; Pinto e Silva et al., 2024). The literature has shown that between 9% and 67% of individuals who have perpetrated intimate partner violence (IPV) drop out of treatment (Cunha, Pedrosa, et al., 2024), and 27.6% of individuals who committed sex crimes (Olver et al., 2011). To enhance adherence and outcomes, a deeper understanding of psychotherapy’s mechanisms is essential. One mechanism influencing treatment outcomes is the therapeutic relationship (TR).
Therapeutic Relationship
Although researchers differ in their conceptualizations of the TR, most theoretical definitions share three common themes: the collaborative nature of the relationship, the emotional bond between patient and therapist, and the mutual agreement on treatment goals and tasks (Bordin, 1979; Martin et al., 2000; Wampold, 2015). Other terms are often used interchangeably with this concept, such as therapeutic alliance, working alliance, or helping alliance (Catty et al., 2007). However, the term TR will be used predominantly in this work, as it is broader and more inclusive (Catty et al., 2007; Gelson & Kline, 2019; Norcross & Lambert, 2011).
The quality of the interaction between client and therapist constitutes a key determinant of the therapeutic process (e.g., Crits-Christoph & Gibbons, 2021). Historically, this idea emerged in Freud’s (1912/1958) works, where he emphasized the importance of the personal and conscious bond between patient and analyst, while also highlighting the role of the unconscious and transference—the projection of unresolved past relationships onto the therapist. Years later, Rogers et al. (1967) contributed to the development of work about TR by applying empirical methods to study the facilitative conditions of the TR—such as empathy, positive regard, and authenticity—paving the way for the scientific investigation of relational factors. In his seminal work, Bordin (1979) described the TR as being defined by the feelings and attitudes that both the therapist and the client have toward one another and the way these are expressed.
Currently, evidence from several empirical studies, systematic reviews, and meta-analyses conducted with adult populations indicates a consistent and significant link between the TR and treatment outcomes, showing that a stronger TR is associated with more positive therapeutic results (e.g., Cameron et al., 2018; Flückiger et al., 2018; Martin et al., 2000). Specifically, Flückiger et al. (2018) conducted a comprehensive meta-analysis comprising 295 independent studies examining the link between TR and treatment outcomes in face-to-face therapies. Their findings revealed a moderate positive association between TR and symptom improvement. Several potential moderators—such as diagnosis, therapy type, methodological factors, and study context—were tested, but only the timing of alliance assessment significantly influenced results, with stronger correlations observed when TR was measured later in treatment (Flückiger et al., 2018). In a follow-up study, Flückiger et al. (2020) confirmed that this TR–outcome association persisted, even after accounting for patient characteristics and therapist adherence or competence.
The literature has also emphasized that the TR is a reciprocal one—alliance influencing subsequent symptoms and symptoms shaping the quality of the alliance (Flückiger et al., 2020)—as well as dynamic and subject to change over time (e.g., Prusiński, 2024). Specifically, some studies have shown that the TR tends to strengthen as therapy progresses (e.g., Piper et al., 2005; Wu et al., 2024), whereas others have found that it follows a U-shaped pattern: a strong alliance in the early phase, a weaker one during the middle phase, and a renewed strengthening toward the end of therapy (e.g., Luo et al., 2022).
Considering the relevance of the TR in treatment outcomes, as well as its variation throughout the therapeutic process, comprehensive models have been developed to better understand this phenomenon. Ribeiro et al. (2013) proposed the Therapeutic Collaboration Model, which conceptualizes therapeutic collaboration as a joint process in which therapist and client work together within the so-called Therapeutic Zone of Proximal Development (TZPD). This concept, adapted from Vigotsky’s (1978) original framework and introduced to psychotherapy by Leiman and Stiles (2001), represents the gap between what clients can currently manage independently and what they can achieve with therapeutic guidance (Ribeiro et al., 2013, 2021). Because clients’ abilities evolve over the course of therapy, both members of the dyad continuously negotiate and adjust their work within this zone. The therapist assesses whether interventions fall inside or outside the client’s TZPD by observing how the client responds—either validating (accepting) or invalidating (rejecting) the therapist’s input. As clients make progress, their TZPD gradually expands upward, reflecting developmental growth. To promote this progress, therapists alternate between supportive interventions, which consolidate the client’s existing understanding, and challenging interventions, which introduce new perspectives to foster change. The degree of collaboration is inferred from clients’ reactions: validation signals that the interaction is within the TZPD, invalidation indicates work beyond it, and mixed reactions suggest the dyad is operating near its boundary (Ribeiro et al., 2013, 2021).
TR Within the Forensic Context
While TR has been extensively studied in clinical settings, research within forensic contexts, particularly concerning individuals who have committed crimes, remains scarce (e.g., Blasko & Jeglic, 2016; Blasko et al., 2015; Kozar & Day, 2012; Polaschek & Ross, 2010; Santirso et al., 2020).
Developing a TR with individuals who have committed crimes can be challenging (Blasko et al., 2018). First, some crimes evoke negative attitudes even among therapists, as is the case with sexual offenses (e.g., Hardeberg Bach & Demuth, 2018), which influences the development of a TR. More specifically, a study by Sousa, Félix, et al. (2025) found that some participants, prior to taking part in an intervention program, feared they would not be understood because of previous negative experiences with therapists. Second, the fact that intervention with these individuals is often court-mandated may make the development of an RT more difficult (e.g., Hachtel et al., 2019). In this way, research has shown that the development of a strong TR is grounded in a “firm but fair” approach, combining care and fairness with an authoritative style. This relationship is further strengthened when professionals promote interactions based on respect, dignity, fairness, the opportunity for individuals to express themselves, validation of their perspective, clear information, and a genuine concern for their well-being (Hachtel et al., 2019; Wittouck & Vander Beken, 2019; Stinson & Clark, 2017). In fact, research on therapist characteristics in forensic treatment has demonstrated that therapists who display empathy, warmth, and directiveness, as well as reward their clients’ good behavior, have been found to impact changes in the client-therapist relationship with those individuals (Blasko et al., 2018). Nevertheless, the available evidence suggests that even populations considered more challenging can develop positive and robust TRs. This is exemplified by a study by DeSorcy et al. (2016), which examined TR and its associations with psychopathy, treatment completion, and recidivism in a correctional context. Participants with both high and low levels of psychopathy reported strong working alliances with their therapists. Notably, even those with elevated psychopathy scores demonstrated the capacity to establish effective TRs within the context of treatment for sexual offenses (DeSorcy et al., 2016).
Nevertheless, existing studies suggest that the TR is important in interventions with individuals who have committed crimes, significantly influencing treatment outcomes (Blasko et al., 2018). In addition, available evidence indicates that a strong therapeutic alliance plays a key role in reducing treatment dropout rates (Brocato, 2013).
Current Study
Considering the well-established influence of the TR on treatment outcomes in clinical settings (e.g., Cameron et al., 2018; Flückiger et al., 2018), and given that, to date, only one systematic review exists in forensic contexts—focusing exclusively on juvenile populations and treatment-related outcomes (Papalia et al., 2022)—there is currently no systematic synthesis examining this association among justice-involved adults across diverse settings.
Moreover, existing research has not fully examined the impact of the TR on outcomes of interest, such as clinical measures and recidivism. The systematic review of justice-involved youth highlighted the role of treatment readiness and expectations in shaping the TR (Papalia et al., 2022), but did not attempt to examine how these factors relate to key outcomes, including clinical improvement or recidivism.
The present systematic review, therefore, focuses on adult males and females who perpetrated crimes across diverse settings (prisons, psychiatric hospitals, and community programs) and includes both clinically relevant outcomes and recidivism. In doing so, it provides a comprehensive synthesis of how the TR relates to key outcomes in adult forensic populations, addressing important methodological and conceptual gaps in the literature and offering insights relevant for clinical practice and intervention planning. Specifically, this systematic review seeks to investigate how the TR relates to recidivism reduction, improvements across various therapeutic domains, and treatment dropout. Furthermore, the review adopts a broad scope by including studies conducted in both custodial (prison) and non-custodial (community and/or forensic hospitals) settings, where men and women who committed crimes are engaged in therapeutic interventions.
Methods
Protocol and Registration
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021), and was pre-registered on OSF REGISTRIES (reference: 10.17605/OSF.IO/4Z7TN).
Eligibility Criteria
Studies were considered eligible for inclusion if they met the following criteria: (a) involved adult participants (male, female, or mixed samples); (b) were empirical and used a quantitative method; (c) provided data on individuals who have perpetrated crimes and were receiving services to support their mental health and/or prevent recidivism; (d) used a validated measure of therapeutic alliance; (e) examined the therapeutic alliance between the client and a mental health professional in the context of a TR, even if the intervention was not exclusively individual therapy (e.g., psychosocial interventions, group therapies); (f) were published in peer-reviewed journals; (g) were written in English, Portuguese, or Spanish; and (h) were accessible online. This review adopted a broad scope by including both forensic interventions aimed at reducing offending-related risk and psychological interventions targeting mental health difficulties in people who have offended, given the recognized role of psychopathology in offending trajectories and the increasing emphasis on outcomes beyond recidivism alone (see Lutz et al., 2022; Willis & Ward, 2024). Studies were excluded if they met any of the following criteria: (a) were review studies, including systematic reviews, meta-analyses, scoping reviews, psychometric studies, theses, or research protocols; and (b) were case reports.
Search Strategy
The initial search was conducted in February 2025, and an additional search was performed in October 2025, without any date restrictions, by two independent researchers. The following search equation was applied to identify relevant studies: (“therap* relationship” OR “working relationship” OR “helping relationship” OR “therap* alliance” OR “therap* collaboration” OR “helping alliance” OR “working alliance”) AND (offend* OR aggres* OR batterer OR perpetrat* OR “criminal*” OR “felon*” OR “Inmate*” OR “Incarcerat*” OR “Prison*” OR “Sentenced” OR “Detainee*” OR “forens*”) AND (treatment OR intervention OR program* OR rehab* OR therapy). The search was conducted across five electronic databases: B-on, Scopus, Web of Science, PubMed, PsycInfo, and Scielo, focusing on titles, abstracts, and keywords. In addition, the reference lists of relevant and key studies were reviewed to identify any further studies that might meet the inclusion criteria.
Literature Selection Process and Data Extraction
Studies identified through the equation-based search were imported into Rayyan software (Ouzzani et al., 2016), where duplicate entries were removed. Two independent reviewers then screened titles and abstracts against the eligibility criteria, selecting articles for full-text analysis. Any discrepancies were discussed until a consensus was reached, with a third reviewer available if needed.
For the selected articles, a structured codebook was developed to extract relevant data. The development of the coding categories followed a hybrid approach, informed by the objectives of the review and by existing literature. Specifically, categories were defined based on prior research highlighting the relevance of these aspects in the TR, as well as on existing systematic reviews in the field of clinical psychology. Coding was limited to information explicitly reported in the articles; no inferences were made when data were not clearly stated. When relevant information was missing or ambiguously described, it was coded as “not reported.” Specifically, when studies reported multiple intervention components or therapeutic approaches, all modality identified by the authors was coded. Similarly, when more than one therapeutic alliance measure was used, all reported instruments were recorded.
The codebook including reference details (e.g., authors and year of publication); study characteristics (e.g., country of the study, sample size; inclusion and exclusion criteria, study setting), participant demographics (e.g., age, gender; ethnicity; type of crime perpetrated); therapist characteristics (e.g., number of therapists, age, gender, professional qualifications, years of service), intervention details (e.g., type of therapy [e.g., cognitive-behavioral therapy, schema therapy], number of sessions, length of sessions; intervention setting [e.g., prison, community]), therapeutic alliance measure (the instrument used in each study to assess TR); methodological details (e.g., study design, follow-up period); and outcome measures relevant to the review’s objectives. To ensure accuracy, extracted data were cross-checked between the reviewers. All extracted data were cross-checked between the reviewers independently, and any disagreements were resolved through discussion until consensus was reached or, when necessary, by consulting a third reviewer.
Quality Assessment
The methodological quality of the included studies was evaluated using the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018). This tool assesses different study designs (e.g., qualitative research, randomized controlled trials, non-randomized studies, quantitative descriptive studies, and mixed-methods studies). Each study was screened using two preliminary questions (“Are there clear research questions?” and “Do the collected data allow to address the research questions?”), followed by five criteria rated as “yes,” “no,” or “don’t know,” according to methodological rigor. The five quality criteria, adapted to the study design, focused on the population (e.g., representativeness), participant recruitment (e.g., appropriate randomization), measurement tools (e.g., suitability for outcomes and interventions), completeness of data, and data analysis (e.g., control of confounders). Consistent with previous steps, two independent reviewers conducted the quality assessment. Discrepancies were addressed through discussion, with a third reviewer consulted when necessary. No study was excluded from the present review based on its quality level, in accordance with the recommendations of the scale itself (Hong et al., 2018).
Data Analysis
This study was conducted as a systematic review, with meta-analytic quantitative pooling performed when sufficient and comparable data were available across the included studies. The data were analyzed using a narrative synthesis approach, where both descriptive text and tables were employed to provide a concise summary of the collected data. This method enables reviewers to assess the findings, considering variations in study designs and potential biases across the studies included in the systematic review.
Results
Screening and Selection of Studies
A total of 3,922 articles were retrieved from database searches and supplementary sources. Following the removal of duplicates, 1,499 titles and abstracts were screened for eligibility. From these, 77 studies were retained for detailed evaluation. Fifty-nine studies were excluded as they did not satisfy the inclusion criteria. Specifically, most studies were excluded because they did not relate TR to an indicator of intervention effectiveness (n = 37). In addition, 12 studies were excluded for not being quantitative empirical articles, 4 for not being written in English, Portuguese, or Spanish, and 2 for not being accessible online. Ultimately, 18 studies were included in the final review. Figure 1 illustrates the PRISMA diagram, detailing study inclusion across all screening phases and reasons for exclusion.
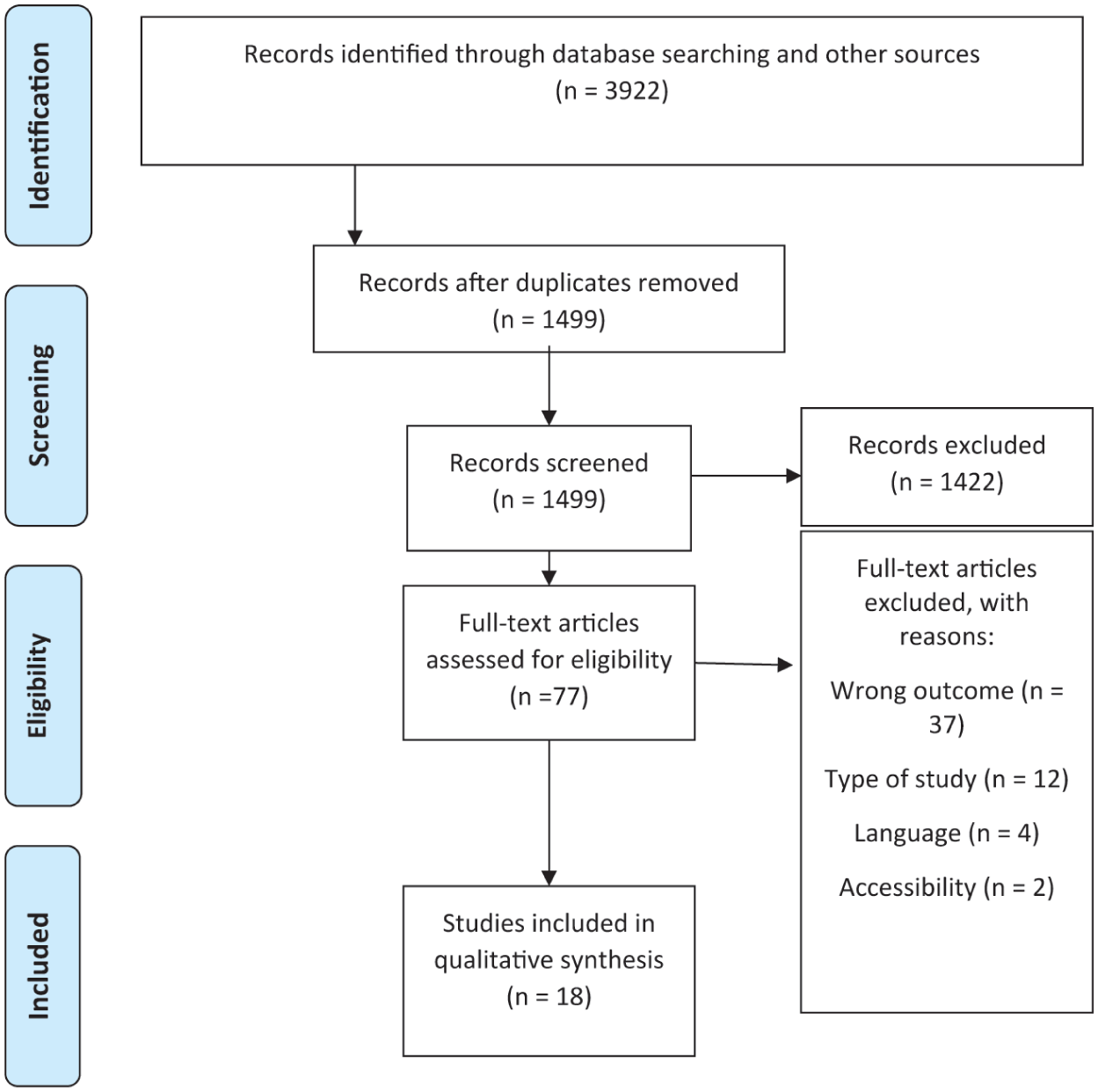
PRISMA flow diagram of the study selection process.
Quality Assessment
Of the included articles, the majority employed quantitative non-randomized designs (n = 15), while the remainder consisted of randomized controlled trials (n = 2), and one was a mixed-methods study (n = 1; see Table 1). Two studies met four out of five criteria of excellent (DeSorcy et al., 2016; Singh et al., 2024), eight met three out of five criteria (Bélanger & Higgs, 2024; Blasko & Jeglic, 2016; Brocato, 2013; DeSorcy et al., 2020; Miles-McLean et al., 2019; Taft et al., 2003; van Tilburg et al., 2025; Walling et al., 2012), five studies met two out of five criteria (Brocato & Wagner, 2008; Brown & O’Leary, 2000; Coleman et al., 2024; Olver et al., 2024; Scanlon et al., 2022), and two studies met one out of five criteria (Polaschek & Ross, 2010; Watson et al., 2018). One study did not meet any of the excellence criteria (Clercx et al., 2021). The majority of the included studies present samples that are not representative of the population under study or omit information regarding the procedure, namely, whether the intervention was administered (or the exposure occurred) as intended. In some cases, the studies include instruments without providing information on their psychometric properties.
Characteristics of the Included Studies.

Note. RCT = randomized controlled trial; TR = therapeutic relationship; RNR = risk-need-responsivity; EERSS = Enhanced Engagement Relational Support Service; RP = Relapse Prevention; CBT = Cognitive Behavioral Therapy; n/a = not applicable; ST = Schema Therapy; WiP = Women in Prison; MI = Motivational Interview.
The study included couples; however, since the intervention targeted the man, only information regarding the male participant was reported.
Study Characteristics
The publication years of the included studies ranged from 2003 (Taft et al., 2003) to 2025 (van Tilburg et al., 2025). The year 2024 had the highest number of publications (n = 3), followed by 2016 (n = 2; Blasko & Jeglic, 2016; DeSorcy et al., 2016; see Table 1). The majority of the studies were conducted in the United States (n = 8), followed by Canada (n = 4; see Table 1). The remaining studies were conducted in the United Kingdom, the Netherlands, Australia, and New Zealand. Only one study did not explicitly report this information (Brown & O’Leary, 2000).
The sample sizes included in this review range from 34 (Singh et al., 2024) to 317 participants (Olver et al., 2024), with mean ages varying between 28.6 years (Brocato, 2013) and 47 years (Bélanger & Higgs, 2024). Regarding the samples, most studies (n = 15) included only men, while the remaining ones consisted of participants of both sexes. Concerning the crimes committed, there is a greater representation of studies with participants convicted of sexual offenses (n = 5) and IPV (n = 5; see Table 1).
Intervention and Therapist Characteristics
Nine studies applied a cognitive-behavioral program, although some interventions included additional theoretical components such as relapse prevention, motivational interviewing, and the risk-need-responsivity (RNR) model (see Table 1). One study applied schema therapy (Clercx et al., 2021). Some studies were even more specific, mentioning the intervention program used, such as the Clearwater Sex Offender Program (DeSorcy et al., 2016, 2020), the Sexual Offense Treatment Program (SOTP)/Clearwater Program (Olver et al., 2024), the “Te Whare Manaakitanga” (Polaschek & Ross, 2010), the Changing Lives and Changing Outcomes Program (Scanlon et al., 2022), the Enhanced Engagement Relational Support Service (EERSS; Singh et al., 2024), and the “Not Losing It Anymore” (van Tilburg et al., 2025). Four articles did not specify the name of the intervention or the therapeutic approach used (Brocato, 2013; Brocato & Wagner, 2008; Coleman et al., 2024; Watson et al., 2018). Seven programs were implemented in the community, five in prison settings, five in forensic hospitals, and one was implemented both in prison settings and in the community.
The number of professionals implementing the intervention programs ranged from 2 (Miles-McLean et al., 2019) to 30 (van Tilburg et al., 2025), with 6 studies not reporting any information regarding the professional team. All seven studies that reported the gender of these professionals included both genders. The average age of these professionals ranged from 25.7 years (Coleman et al., 2024) to 39.94 years (Blasko & Jeglic, 2016). The basic training of these professionals varied across the included articles, involving intervention with a multidisciplinary team with psychologists, psychiatrists, nurses, staff members of institutions such as parole officers, and social workers (e.g., Blasko & Jeglic, 2016; Coleman et al., 2024; DeSorcy et al., 2016, 2020; Miles-McLean et al., 2019; Olver et al., 2024; Polaschek & Ross, 2010; van Tilburg et al., 2025), and psychologist and/or psychologist students (e.g., Brocato & Wagner, 2008; Taft et al., 2003; Walling et al., 2012). Regarding years of experience, only two studies reported the average number of years, which ranged from 1.83 years (Coleman et al., 2024) to 5.2 years (Polaschek & Ross, 2010). On the other hand, the study by Brocato and Wagner (2008) mentioned that the professionals had at least 2 years of experience, and Blasko and Jeglic (2016) reported a minimum of 3 years of experience. The van Tilburg et al. (2025) study included therapists with varying levels of experience: 3 with fewer than 5 years, 8 with 6 to 10 years, 4 with 11 to 15 years, and 15 with more than 15 years of professional experience.
Instruments Used to Assess TR
Most studies (n = 16) used the Working Alliance Inventory (WAI; Horvath, 1981, 1982) or the short version of WAI (Hatcher & Gillaspy, 2006). Within these studies, eight used only the version of the scale focused on the client’s perspective; five used both the client and therapist versions; one used only the version reflecting the therapist’s view of the TR (Brocato & Wagner, 2008); one used only the observer-rated version (Brown & O’Leary, 2000); and one used all three versions of the scale (Polaschek & Ross, 2010; see Table 1).
One study used the California Psychotherapy Alliance Scale (Bélanger & Higgs, 2024), which allows the assessment of the client’s perspective. Another study used two scales to obtain information from both clients and therapists: the patient-rated alliance scale—the Session Rating Scale, and the therapist-rated alliance scale—the Therapist Satisfaction Scale (van Tilburg et al., 2025).
Intervention Outcomes
Recidivism and risk of recidivism were the most common outcomes (n = 6), followed by retention/ dropout/treatment non-completion (n = 5), aggression/institutional incidents/abusive behavior (n = 4), motivation to change (n = 3), and distress and well-being (n = 3). Four studies focused on miscellaneous problems such as marital satisfaction, alcohol abuse, criminal thinking, and treatment gain (see Table 2).
Conclusions of the Included Studies.

Note. IPA = intimate partner abuse; GV = general recidivism; TR = therapeutic relationship.
Recidivism and Risk of Recidivism
The findings across studies were inconsistent regarding the relationship between TR and risk: Blasko and Jeglic (2016) reported that TR is not correlated with risk of recidivism, whereas the study by Polaschek and Ross (2010) showed the opposite. Specifically, their study found a positive small-to-medium correlation (r = .32).
Regarding recidivism, the studies showed that TR is not correlated with reoffending for any type of crime (DeSorcy et al., 2016, 2020; Miles-McLean et al., 2019), regardless of whether TR was assessed by the client or the therapist (Miles-McLean et al., 2019). However, this absence of correlation does not apply to TR subscales. For example, the Bond subscale was significantly negatively correlated with risk, regardless of the small effect sizes, r = −.27, p < .001 (Blasko & Jeglic, 2016). Curiously, Olver et al. (2024) reported that TR was actually associated with an increased risk of sexual recidivism (Harrell’s C = 0.62).
All programs were based on a cognitive-behavioral approach; however, no differences were found in TR depending on whether the program adhered to RNR principles (e.g., DeSorcy et al., 2016, 2020) or incorporated motivational approaches (Miles-McLean et al., 2019). Regarding the intervention setting, no specific pattern was observed in the relationship between TR and recidivism or risk of recidivism.
Retention/Dropout/Treatment Non-Completion
The results showed that the TR is not a predictor of treatment retention—that is, staying in or dropping out of therapy (Brocato, 2013; Brown & O’Leary, 2000; DeSorcy et al., 2020). However, the study by DeSorcy et al. (2016) revealed a different pattern: participants with a poorer TR were more likely to drop out of treatment, whereas those with a stronger TR—especially regarding bond and goal alignment—tended to remain in the program for a longer period. In addition, the relationship between TR and treatment completion seems to depend on who evaluates the relationship. Specifically, the study by van Tilburg et al. (2025) found that therapists’ ratings of the TR reliably predicted session attendance and treatment completion, whereas patients’ ratings did not predict either outcome.
No differences were found in the relationship between TR and retention/dropout/treatment compliance across different intervention settings, with studies showing mixed findings.
Aggression/Institutional Incidents/Abuse Behavior
The included studies have produced contradictory findings regarding the impact of TR on aggression variables. Brown and O’Leary (2000) and Taft et al. (2003) found that the TR significantly predicts reductions in psychological aggression and physical aggression after treatment. However, the study by Walling et al. (2012) showed that the extent to which TR influences the decrease in violence depends on racial background. Specifically, for minority participants, an increase in TR was associated with a substantial reduction in violence. In addition, the study by Clercx et al. (2021) examined the effect of TR on the number of institutional incidents involving verbal and physical aggression. The authors found that the impact of TR varied depending on the assessment period and the influence of concurrent variables. Specifically, while baseline TR did not predict incidents during the first 18 months, it significantly predicted incidents in the subsequent 18 months. TR assessed at 18 months was not a significant predictor.
When focusing specifically on outcomes related to aggression, institutional incidents, or abusive behavior, Clercx et al. was the only study to examine a non-cognitive-behavioral intervention, conducted in a forensic hospital setting. This study found no associations between TR, assessed at baseline or post-treatment, and aggressive incidents during the first 18 months. However, the TR assessed at baseline was associated with aggressive incidents occurring after the first 18 months. In contrast, studies of cognitive-behavioral programs conducted in community settings reported significant associations (Brown & O’Leary, 2000; Taft et al., 2003; Walling et al., 2012).
Motivation to Change
The studies indicated that the quality of the TR is associated with motivation to change (Bélanger & Higgs, 2024; Brocato, 2013; Brocato & Wagner, 2008), with studies suggesting that these associations vary depending on the stage of change (Bélanger & Higgs, 2024) or the specific dimension of TR examined (Brocato & Wagner, 2008). Specifically, Bélanger and Higgs (2024) found a positive but weak association between TR and the contemplation stage (i.e., when individuals begin to recognize the need for change), a moderate positive association between TR and the action stage (i.e., when individuals are actively engaged in making behavioral changes), and a moderate negative association between TR and precontemplation (i.e., when individuals do not yet acknowledge a need to change their behavior). Brocato and Wagner (2008), who assessed TR based on therapists’ self-reports, found that only the bond dimension was associated with motivation to change.
TR results did not vary according to the intervention setting (i.e., community or correctional institution).
Distress and Well-being
The included studies showed that TR was moderately associated with lower psychological and relationship distress at the end of treatment (Coleman et al., 2024) and with higher well-being (Singh et al., 2024). Specifically, the study by Scanlon et al. (2022) further showed that TR is a moderator of change for certain dimensions of mental health, such as anxiety, mania, anger, and depression symptoms. The results did not vary by intervention approach or setting.
Other Outcomes
The results indicated that TR did not predict outcomes related to marital satisfaction (Brown & O’Leary, 2000), alcohol use (Miles-McLean et al., 2019), or improvement in treatment (Watson et al., 2018), but it was significantly associated with reductions in general, reactive, and current criminal thinking (Scanlon et al., 2022).
The only program in which TR reached significance was based on a cognitive-behavioral model that also incorporated a psychosocial rehabilitation framework and a social learning paradigm (Scanlon et al., 2022), specifically in relation to anxiety, manic symptoms, anger, depression symptoms, and general, reactive, and current criminal thinking. No differences were observed based on the intervention setting.
Discussion
Building on the previously noted relevance of the TR for clinical outcomes (e.g., Cameron et al., 2018; Flückiger et al., 2018), this review further investigates how this relational factor operates within forensic treatment. In particular, the present study examines the associations between the TR and recidivism, therapeutic progress, and treatment attrition in intervention programs for individuals who have committed crimes.
Despite the considerable amount of research on intervention with individuals who have committed crimes (e.g., Beaudry et al., 2021; Gannon et al., 2019; Pinto e Silva et al., 2025; Sousa et al., 2022; Sousa, Féliz, et al, 2025; Sousa, Gonçalves, & de Castro-Rodrigues, 2024), in this systematic review, only 18 studies focused on the TR. This reflects the small investment and focus on TR among psychological interventions with individuals who have committed crimes, in contrast to non-forensic settings, where research on TR is of particular importance (e.g., Cameron et al., 2018; Flückiger et al., 2018; Luong et al., 2020). In fact, in clinical settings, more than 300 studies have investigated the alliance-outcome relationship, encompassing over 30.000 patients (Flückiger et al., 2018; Wampold, 2021). The extensive body of research on TR in clinical settings is associated with its recognition as a common factor across all treatments that plays a central role in determining positive therapeutic outcomes and is, at times, considered more influential than the treatment itself (Messer & Wampold, 2002; Norcross & Lambert, 2018; Wampold, 2021). Furthermore, our data further revealed that the included studies were conducted between 2003 and 2025, also reflecting a delay in the study of TR in forensic settings, given that interest in the clinical context dates back to 1978 (see Flückiger et al., 2018). In this regard, the studies conducted also exhibit low methodological quality, with only two studies employing a randomized controlled trial design. The low methodological quality observed is consistent with that of studies included in the systematic review on TR outcomes among justice-involved youth (see Papalia et al., 2022). The limited attention afforded to the TR in forensic contexts may be largely attributable to the dual role of forensic practitioners, who must integrate therapeutic work with risk assessment and legal reporting (Merkt et al., 2021; Ward, 2013), thereby creating tensions with foundational relational principles such as trust and confidentiality. Historically, forensic interventions have prioritized risk management, control, and program fidelity over relational processes, reflecting actuarial and correctional paradigms that conceptualized individuals who committed crimes as resistant, manipulative, or insufficiently motivated for change (Bonta & Andrews, 2023). Furthermore, the coercive nature of treatment, pronounced power asymmetries, and ethical constraints have complicated both the development and empirical examination of therapeutic alliance in forensic settings (Skeem et al., 2007).
In terms of sample characteristics, the included studies predominantly focused on men convicted of sexual offenses or IPV. Although the near-exclusive focus on the male population aligns with trends in scientific research (e.g., Cunha, Pereira, et al., 2024; Sousa et al., 2022; Sousa, Gouveia, Freitas, et al., 2024), it is surprising that there is a particular emphasis on individuals convicted of sexual or IPV-related crimes. This may be due to the continued high prevalence of these crimes and their psychological, physical, and social repercussions for victims, their families, and society both in the short and long term, as well as to their substantial social impact and the associated medical and legal costs (Hailes et al., 2019; Sardinha et al., 2022; Stubbs & Szoeke, 2022). Consequently, there remains an ongoing scientific and political debate regarding the effectiveness of interventions for these populations (e.g., Annison & Guiney, 2022; Gouveia et al., 2025; Sousa et al., 2026), highlighting the need to improve intervention strategies and identify the key components that can maximize outcomes (Lussier et al., 2023).
In relation to the characteristics of therapists, the number of professionals varied across studies, with different professional backgrounds such as psychologists, psychiatrists, nurses, institutional staff members (e.g., parole officers), and social workers (e.g., Blasko & Jeglic, 2016; Coleman et al., 2024; DeSorcy et al., 2016, 2020; Miles-McLean et al., 2019; Olver et al., 2024; Polaschek & Ross, 2010; van Tilburg et al., 2025). These findings are concerning, as a meta-analysis revealed that intervention programs targeting individuals convicted of sexual offenses as well as IPV-related crimes show lower recidivism rates when the programs are delivered by psychologists (Gannon et al., 2019). Although the present review does not allow for an assessment of whether therapists’ professional background has a consistent impact across the included studies, findings from Gannon et al. suggest that this factor may be relevant and, therefore, warrants caution when selecting professionals to deliver intervention programs. The overuse of paraprofessionals to deliver intervention programs, that is, professionals who are not licensed psychologists for clinical practice, has been associated with the growth of the prison population and the need to provide interventions to a larger number of individuals (Gannon & Ward, 2014).
The impact of the TR on treatment outcomes in justice-involved adults showed marked heterogeneity. Mixed findings were observed concerning the influence of the TR on recidivism and the risk of perpetrating new crimes (e.g., Blasko & Jeglic, 2016; DeSorcy et al., 2016, 2020; Miles-McLean et al., 2019; Olver et al., 2024; Polaschek & Ross, 2010), as well as its influence on the reduction of aggressiveness (e.g., Brown & O’Leary, 2000; Taft et al., 2003). Nevertheless, the included studies showed that TR is linked to motivation to change (Bélanger & Higgs, 2024; Brocato, 2013; Brocato & Wagner, 2008), as well as with reductions in psychological and relational distress (Coleman et al., 2024) and improvements in well-being (Singh et al., 2024). In addition, only one study found it to be significant for participants to remain in treatment (DeSorcy et al., 2016). Taken together, these findings suggest that the TR may exert a stronger influence on proximal, intrapersonal outcomes, such as motivation to change and well-being, than on more distal behavioral outcomes, such as aggression or recidivism. The TR did not show a robust link to treatment retention, which is somewhat surprising given evidence from recent qualitative studies suggesting that therapist characteristics are essential for treatment retention in programs for men who have perpetrated child sexual abuse (see Sousa, Félix, et al., 2025). Furthermore, the absence of an effect at the behavioral level may occur because recidivism, risk, and levels of aggression are complex, multifactorial outcomes influenced by a wide range of individual and therapeutic factors beyond the TR (Sturm et al., 2022). However, the available evidence base is too small and limited to allow firm conclusions to be drawn.
In addition, no differences were observed in the influence of the TR across the different outcomes as a function of the theoretical approach or the intervention setting. This may be because of the lack of variability, as most studies employed a CBT-based approach, which is in accordance with the literature (e.g., Gannon et al., 2019).
Limitations and Strengths
There are some limitations that should be considered. First, the number of included studies was limited, and the resulting evidence was frequently inconsistent. Further research is therefore needed, which would be facilitated by therapists and program evaluators routinely incorporating measures of the TR into interventions with justice-involved adults. Second, the overall quality of the studies is low, with limitations related to sample representativeness, the instruments used, and the procedures employed. In this regard, more randomized controlled trials are needed, with greater rigor in the selection of instruments with good psychometric properties and clearer reporting of procedures. In addition, the diversity of participants in the included studies was limited. Most studies included only men, and where both sexes were included, detailed demographic information such as race/ethnicity or socioeconomic status was generally not reported. This restricts the ability to assess how findings may vary across different populations and limits the generalizability of the results. Future research should aim to include more diverse samples and systematically report demographic characteristics to better understand the applicability of findings across different groups and cultural contexts.
The review also highlighted key knowledge gaps and directions for future research, some of which have already been addressed. From a practical perspective, the findings appear to suggest, albeit based on a limited body of evidence, that the TR functions as a responsivity factor that may influence participants’ engagement, motivation to change, and well-being, as it allows for the creation of a learning environment—considered a crucial element of responsivity—in which change is promoted and initiated and client engagement is enhanced (Bourgon & Bonta, 2014). This variable is particularly relevant, given that motivation to change in this population is generally low because of the mandatory nature of participation, which could influence recidivism rates (Pinto e Silva et al., 2022). In this regard, the findings also point to the importance of ensuring that professionals involved in these interventions receive appropriate clinical training, including training in relational and person-centered skills. Therapists’ person-centered characteristics (i.e., empathy, respect, warmth, and accepting and caring behavior) are associated with the formation of positive TRs, whereas a confrontational approach (i.e., hostility, negative attitudes, therapist rigidity, and arrogance) hinders the development of the therapeutic alliance (Norcross & Lambert, 2014; see Table 3).
Key Findings of the Systematic Review.

Note. TR = therapeutic relationship.
From a research perspective, further studies with greater methodological rigor, particularly randomized controlled trials, are needed to examine the influence of the TR in the treatment of diverse populations of individuals who have committed crimes. Future research should also move beyond examining whether TR is associated with treatment outcomes and instead clarify under which conditions, for whom, and through which mechanisms these associations emerge. Greater methodological consistency in the assessment of TR is needed, including the use of validated measures, repeated assessments across different stages of treatment, and the consideration of both participant and therapist perspectives. It is also important that future studies distinguish between different types of outcomes, such as treatment engagement, dropout, aggressive incidents, psychological well-being, and recidivism, to better understand the specific contribution of TR. Moreover, further research should include more diverse forensic samples, including individuals with different offense profiles and participants from prison, forensic psychiatric, and community-based settings. Finally, qualitative and mixed-methods studies may be particularly useful in clarifying the interpersonal and contextual processes through which TR develops in mandated treatment, including the role of perceived coercion, trust, responsivity, and the balance between care and control.
Conclusion
The primary aim of the present systematic review was to provide an overview of the outcomes associated with the TR in the treatment of adults who have committed crimes. Overall, the findings indicate that the TR plays a significant role in influencing proximal therapeutic factors, such as motivation to change and well-being. Nevertheless, further research with this specific population remains essential. In particular, additional studies are needed to deepen our understanding of the impact of the TR on the effectiveness of individuals’ rehabilitation (see Table 4).
Implications for Research, Practice, and Policy.

Footnotes
Acknowledgements
The authors acknowledge the support of the doctoral student Teresa Pinto e Silva for the draft prepared for the development of the “Introduction” section.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Fundação para a Ciência e Tecnologia (FCT), under HEI-Lab R&D Unit (UID/05380/2025, UIDP/05380/2020, and UID/PRR/05380/2025; ![]() , https://doi.org/10.54499/UIDP/05380/2020, and https://doi.org/10.54499/UID/PRR/05380/2025 https://doi.org/10.54499/UIDB/05380/2020). This work was also conducted at CIPsi, School of Psychology, University of Minho, supported by Fundação para a Ciência e a Tecnologia (FCT; UID/01662/2020) through the Portuguese. This work is funded with national funds from FCT, I.P., in the context of the R&D Unit: UID/04810/2025—William James Center for Research.
, https://doi.org/10.54499/UIDP/05380/2020, and https://doi.org/10.54499/UID/PRR/05380/2025 https://doi.org/10.54499/UIDB/05380/2020). This work was also conducted at CIPsi, School of Psychology, University of Minho, supported by Fundação para a Ciência e a Tecnologia (FCT; UID/01662/2020) through the Portuguese. This work is funded with national funds from FCT, I.P., in the context of the R&D Unit: UID/04810/2025—William James Center for Research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.