
Abstract
We aimed to conduct the first systematic narrative review and quality appraisal of existing evidence on the psychological consequences of crime in older victims in the community and psychological interventions. We searched five databases to identify all peer-reviewed literature published in English on psychological impact and/or interventions for older crime victims and quality appraised these using the Mixed-Methods Appraisal Tool, following Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines (Prospero: CRD42019140137). Evidence from included studies were narratively synthesized, along with their strengths and limitations. We found 20 studies on psychological distress in older victims, four of which included interventions. From these, we identified 30 different impacts including symptoms of anxiety, depression, post-traumatic stress disorder, emotions including humiliation and self-blame, and behavioral changes. Only feasibility interventions have been published, although promising results were reported for cognitive-behavioral informed treatments for depression and anxiety. Studies were wide-ranging in aims, crimes included, and outcomes used. Recommendations for improving the evidence-base and to raise the profile of this neglected population have been provided.
Introduction
Supporting older people after a crime is a growing challenge with global population ageing and is an issue of social concern internationally (Burnes et al., 2017; HMICFRS, 2019; Muhammad et al., 2021; Qin & Yan, 2018). Even in cities considered comparatively safe such as London, an estimated 34,133 adults aged 65 years or over reported a crime in 2019 (Metropolitan Police Service, personal communication, 2019; The Economist, 2022), and as 60% of crimes go unreported, the true figure is likely to be even higher (MacDonald, 2002). Older adults are also at greater risk of specific crimes including fraud and distraction burglary (Laycock, 2020; Qin & Yan, 2018). In the United States, an estimated 1 in 18 older adults in the community suffered fraud each year before Covid-19 (Burnes et al., 2017), and as fraud reports significantly increased during the pandemic, even greater numbers are now likely to have been affected (Office for National Statistics, 2022; Payne, 2020). Internationally, theft and assault are reported to have resurged as lockdown restrictions have eased and social movement resumed (Langton et al., 2021; Nivette et al., 2021) and data on rates of different crimes during Covid-19 are still emerging. With costs of living rising in many countries, there are growing concerns that crime will continue to increase (International Monetary Fund, 2022; Mayor of London, 2022). Globally, the number of older crime victims is likely to be significant.
There is growing recognition of the impact of crime as a public health concern (Burnes et al., 2017; Tan & Haining, 2016) Historically, public health and criminology developed independently of one another meaning the links between crime victimization and health outcomes are poorly understood (Tan & Haining, 2016). Older adults in the community have been further neglected from research on crime and health due to an enduring and disproportionate focus on explaining the “Victim’s Paradox”: the perception that older adults are more fearful of crime than younger age groups despite being at statistically less risk overall (Lindquist & Duke, 1982). This overlooks that large numbers of older adults are still affected and that they are at increased risk of specific crimes (Laycock, 2020). It also implies that fear of crime in older adults is irrational yet impact may be greater in this group because of concurrent life events including declining physical health, bereavement, and reduced income in retirement (Jackson, 2009). Severe and prolonged symptoms of psychological distress have been identified in older victims of all crime types (Serfaty et al., 2016). Burglary and interpersonal violence in older adults has also been associated with accelerated mortality and increased risk of nursing home placement (Donaldson, 2003; Lachs et al., 2006).
Recent reviews have furthered understanding of the psychological impact of domestic violence and elder abuse in older people (e.g., Knight & Hester, 2016; Yunus et al., 2019) but the literature on other crime types has not been synthesized. Domestic and elder abuse should be studied separately as they are typically ongoing and committed by someone in a close existing relationship or with an expectation of trust (WHO, 2017). This is only one aspect of crime which affects older people. For example, ten years of law enforcement data suggest that almost half (43%) of violent victimizations in older people are committed by strangers (Langton & Truman, 2014). Understanding the unique psychological needs and how to support older victims of other crime types, such as burglary, theft, criminal damage, stranger assault, and fraud, is also important.
Study Aims
We aimed to address the following questions: (a) What is the psychological impact of crime in older victims? (b) What psychological interventions are there for distress in older crime victims? (c) What are the strengths and weaknesses of the existing literature and how can the evidence base be improved?
Methods
Study Protocol
Our review adheres to guidance from Cochrane and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) (Higgins et al., 2021; Page et al., 2021). We registered the review protocol on PROSPERO on August 14, 2019 (CRD: 42019140137) and submitted amendments on February 28, 2022, and May 12, 2022.
Inclusion and Exclusion Criteria
We included peer-reviewed studies of any design published in English from 1980 to 2022 that presented data on psychological impact or psychological interventions for community-dwelling older crime victims aged 50 years and over. Psychological impact was defined as any emotional or behavioral response (Ridner, 2004), which could be recorded objectively or subjectively. Psychological interventions could be any format and include any comparator, including treatment-as-usual and no care. As there is no agreed definition of “older adults,” we selected a conservative definition of age 50 years and over, as this was lowest age identified in a review of ageing definitions, and it is recommended that reviews be over-inclusive to capture all relevant literature (Cosco et al., 2014).
We excluded studies on crimes perpetrated by friends, family, or caregivers, unless analyzed and reported separately, as psychological impact may be different when the victim is in a close-existing relationship with the perpetrator (Langton & Truman, 2014). Reviews on psychological impact in older victims of domestic violence and carer abuse have also recently been published elsewhere (Knight & Hester, 2016; Yunus et al., 2019). Studies on dementia, serious mental illness, personality disorder, and intellectual disability were also excluded as the focus is on psychological outcomes rather than preexisting conditions. Studies on alcohol or substance misuse were excluded as these may be considered a consequence of distress rather than a direct outcome.
Search Strategy
We used PsycINFO, MEDLINE, Embase, Cumulative Index to Nursing and Allied Health Literature, and PTSDPubs to search existing literature published between 1980 and August 2019. We updated the search in August 2021 and April 2022. A broad date range of over four decades was chosen to identify as much relevant literature as possible. The key words were “older adult” AND “mental health” AND “crime victim.”
Two reviewers independently screened titles and abstracts of all search results and assessed the full-text of potentially relevant papers before conferring (99.8% agreement, k = 0.66, 95% confidence interval [CI] [0.52–0.79], “substantial agreement”; Cohen, 1960). A third reviewer was nominated to make final decisions on papers where eligibility remained unclear even after discussion. Reference lists of all included papers were also screened. The Cochrane Central Register of Controlled Trials and International Standard Randomized Controlled Trial Number registry were also searched.
Data Extraction and Quality Appraisal
The following data were extracted into pre-populated tables: study design, setting, sample size, sample characteristics, crimes included, mental health outcomes, recruitment procedures, duration between crime occurring and assessment, analytical strategy, lengths, and procedures. Additional data extraction for intervention studies included treatment and comparator characteristics. Missing data was recorded as “not reported.” A second reviewer crosschecked 20% of data extraction and found no errors. Studies were quality appraised using the Mixed Methods Appraisal Tool (MMAT) version 18 (Hong et al., 2018). Low methodological quality was not an exclusion criterion as the review aimed to provide an overview and quality appraisal of existing literature.
Synthesis
The results were summarized using narrative synthesis as recommended for systematic reviews that include non-RCT studies (Popay et al., 2006). We considered meta-analysis but deemed it unsuitable due to heterogeneity in study and sample characteristics.
Results
Study Selection
The searches combined produced 19,856 results which, once duplicates were removed, left 11,980 results which were screened by two reviewers. Most (n = 11,575) were excluded based on titles and abstracts, but a full-text review was completed for 56. Of these, 36 were excluded because: (A) the crime was committed by a perpetrator in a close relationship with the victim; (B) the study focused on younger victims; (C) the study was a review or protocol paper that did not present data; (D) the outcome was not psychological, or (E) the intervention was not psychological. One intervention study (Acierno et al., 2004) included older victims of domestic violence but clearly reported that this was the minority of the sample and that no differences were found compared to other crime groups in any analyses. As such, we decided to include this study and a protocol amendment explaining this was submitted to Prospero.
This resulted in 20 papers for inclusion in this review. Figure 1 illustrates the full selection process using the PRISMA 2020 flow diagram (Page et al., 2021).
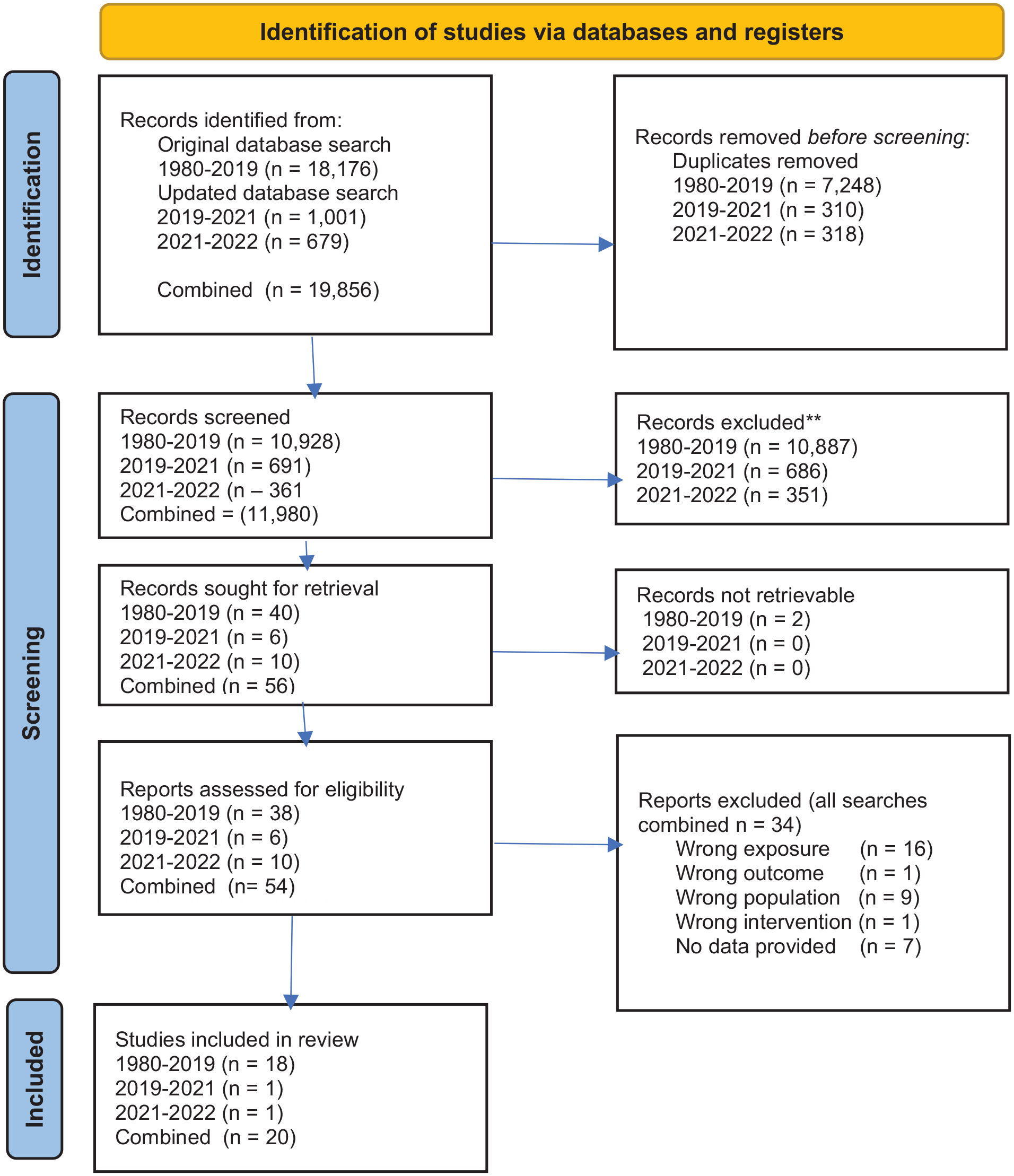
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
Study Characteristics
Study and sample characteristics of included studies are summarized in Table 1. Of the 20 studies, four included intervention research. The studies were published between 1985 and 2021 and were cross-sectional (n = 9), case studies (n = 2), qualitative (n = 4), randomized controlled trial (n = 2), descriptive intervention (n = 1), prospective longitudinal (n = 1), and secondary analysis (n = 1). Most (n = 17) were from Western countries except for two in India and one in China (Muhammad et al., 2021; Tripathi et al., 2019; Qin & Yan, 2018). The mean sample ages ranged from 60 to 79 years. Crimes included across studies were burglary, vandalism, robbery, mugging, physical assault, sexual assault/ rape, distraction burglary, transphobic hate crime, racial hate crime, fraud, cybercrime, and other scams.
Summary Characteristics of Studies.
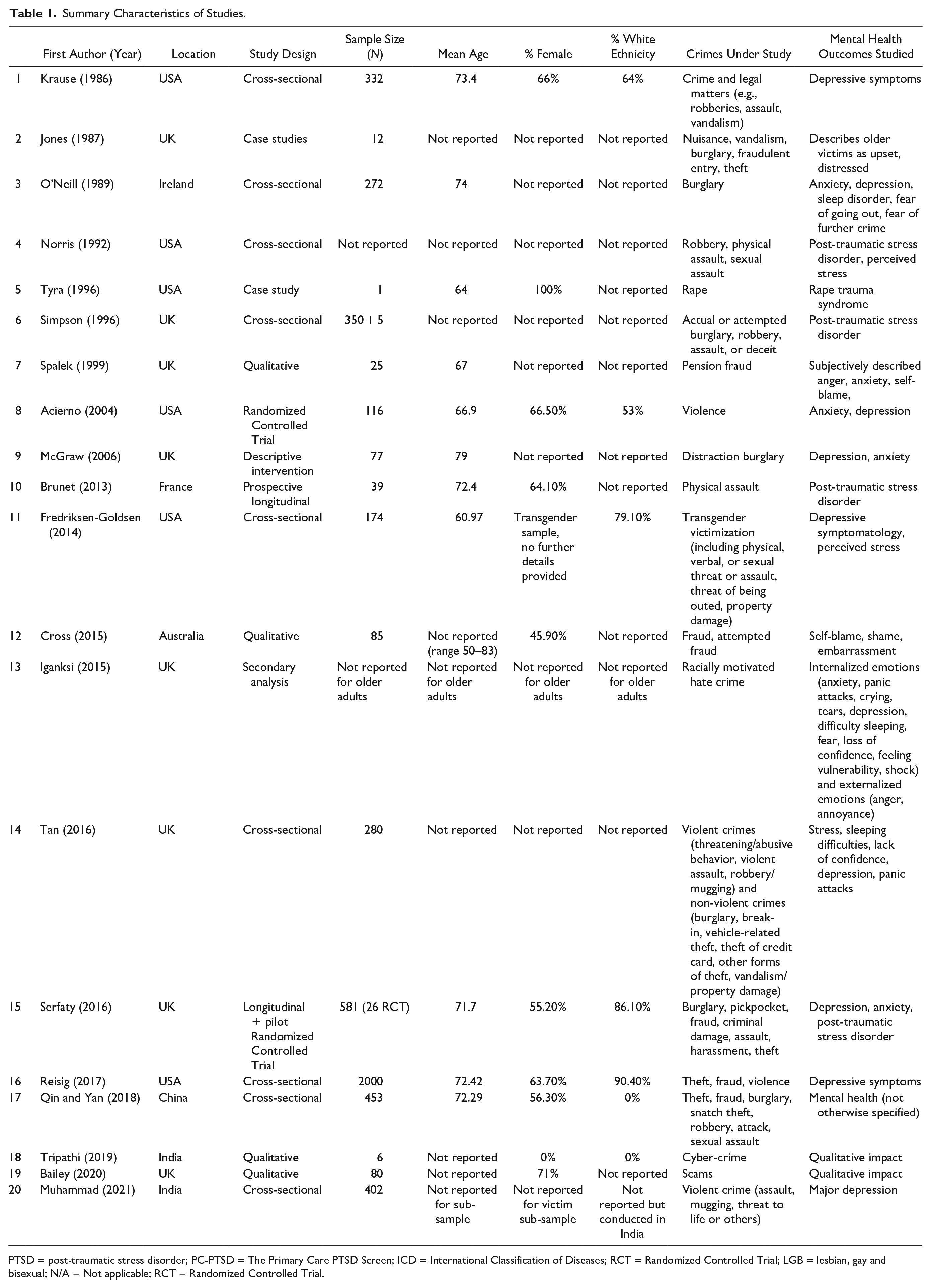
PTSD = post-traumatic stress disorder; PC-PTSD = The Primary Care PTSD Screen; ICD = International Classification of Diseases; RCT = Randomized Controlled Trial; LGB = lesbian, gay and bisexual; N/A = Not applicable; RCT = Randomized Controlled Trial.
Quality Appraisal
Quality appraisal using the MMAT (Hong et al., 2018) was conducted for the 20 studies, an overview of which is presented in the supplementary material. Studies of low methodological quality were not excluded as we aimed to appraise the strengths and limitations.
Observations across the literature included: (a) Many studies lack detail on methods. (b) It was often unclear which crimes were included in studies. (c) Reporting of sample characteristics (including mean age, gender, and ethnicity) was inconsistent. (d) Of the studies that did report ethnicity, samples were predominantly white. (e) Studies varied on how long after the crime the outcome was measured; in some cases, the crime may have occurred much earlier in life. (f) Different definitions of psychological impact made comparisons across studies challenging. (g) Four studies included older victims alongside other populations or traumas, meaning examination of psychological impact in older crime victims was brief. (h) There was little consideration of how differences in frailty, physical health, and global functioning may influence outcomes. (i) Stranger-perpetrated and known-perpetrator crimes were often not clearly distinguished. (j) No studies obtained data on pre-crime psychological health limiting inferences around causality and direction thereof. (k) Studies often did not declare whether ethical approval was obtained or outline ethical considerations in their research. (l) Only feasibility intervention data has been published. (m) The challenges of timely identification and recruitment of older victims meant psychological impact studies were often based on convenience samples or randomly selected samples with low response rates, risking bias, and limiting generalization. Intervention studies addressed this by collaborating with police or healthcare agencies, although this limited samples to those known to those services.
Narrative Synthesis
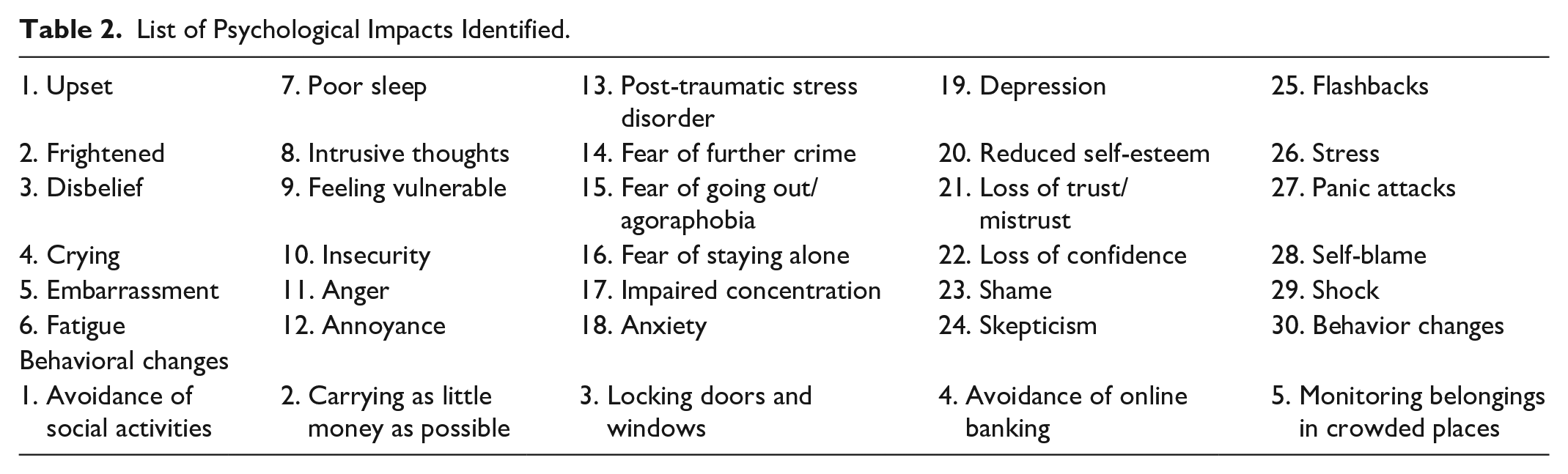
Our synthesis is divided into psychological impact and psychological intervention findings, with psychological impact studies further organized by study aims. The psychological impacts we identified across studies are summarized in Table 2, psychological impact methods and data are in Table 3, psychological intervention methods and data are in Table 4, and implications of this review for practice, policy, and future research are in Table 5.
List of Psychological Impacts Identified.
Summary Findings of Studies Reporting on Psychological Impact.
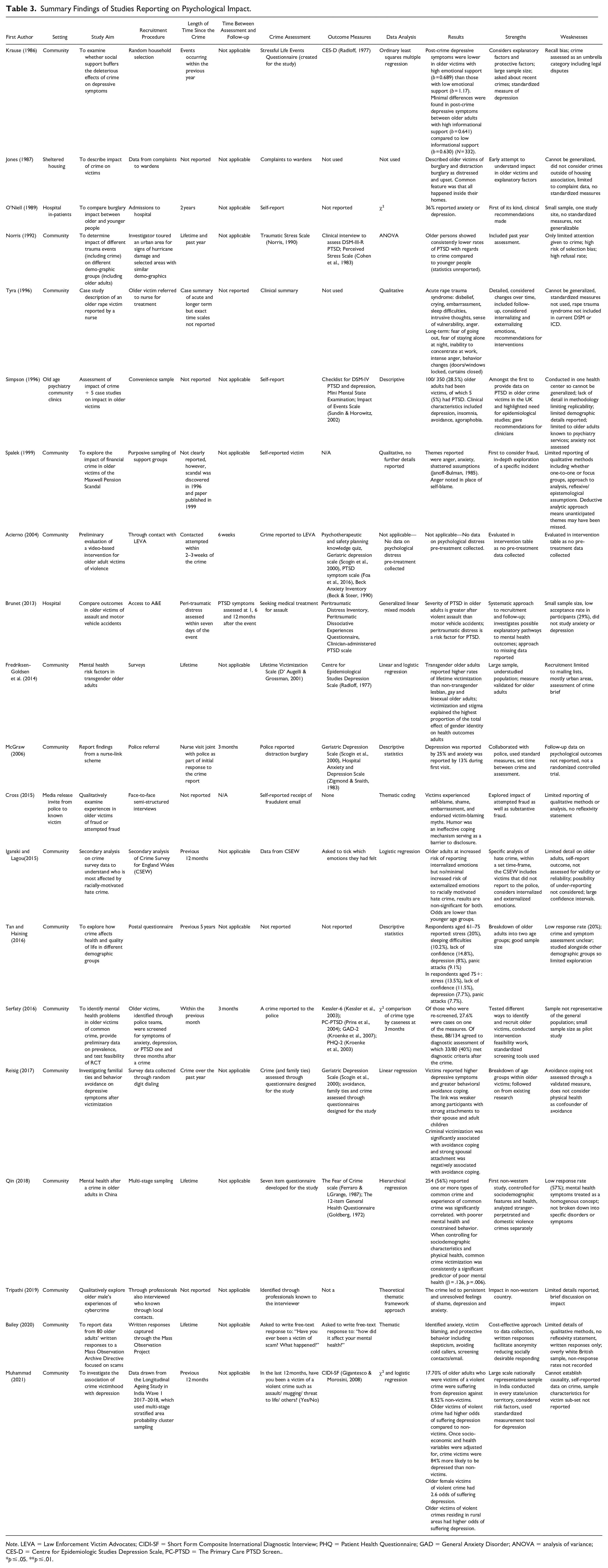
Note. LEVA = Law Enforcement Victim Advocates; CIDI-SF = Short Form Composite International Diagnostic Interview; PHQ = Patient Health Questionnaire; GAD = General Anxiety Disorder; ANOVA = analysis of variance; CES-D = Centre for Epidemiologic Studies Depression Scale, PC-PTSD = The Primary Care PTSD Screen..
p ≤ .05. **p ≤ .01.
Summary Findings of Studies Reporting Interventions.
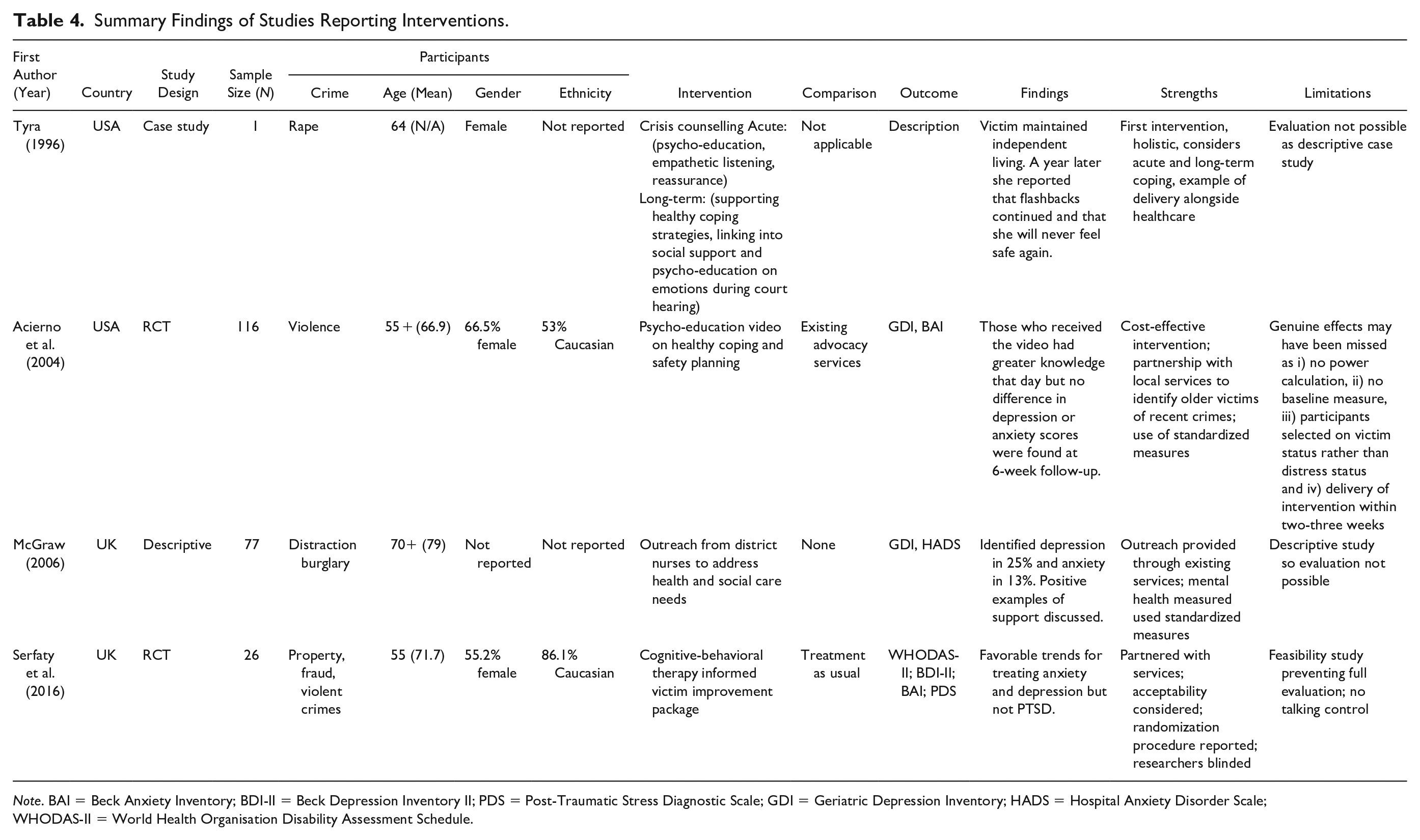
Note. BAI = Beck Anxiety Inventory; BDI-II = Beck Depression Inventory II; PDS = Post-Traumatic Stress Diagnostic Scale; GDI = Geriatric Depression Inventory; HADS = Hospital Anxiety Disorder Scale; WHODAS-II = World Health Organisation Disability Assessment Schedule.
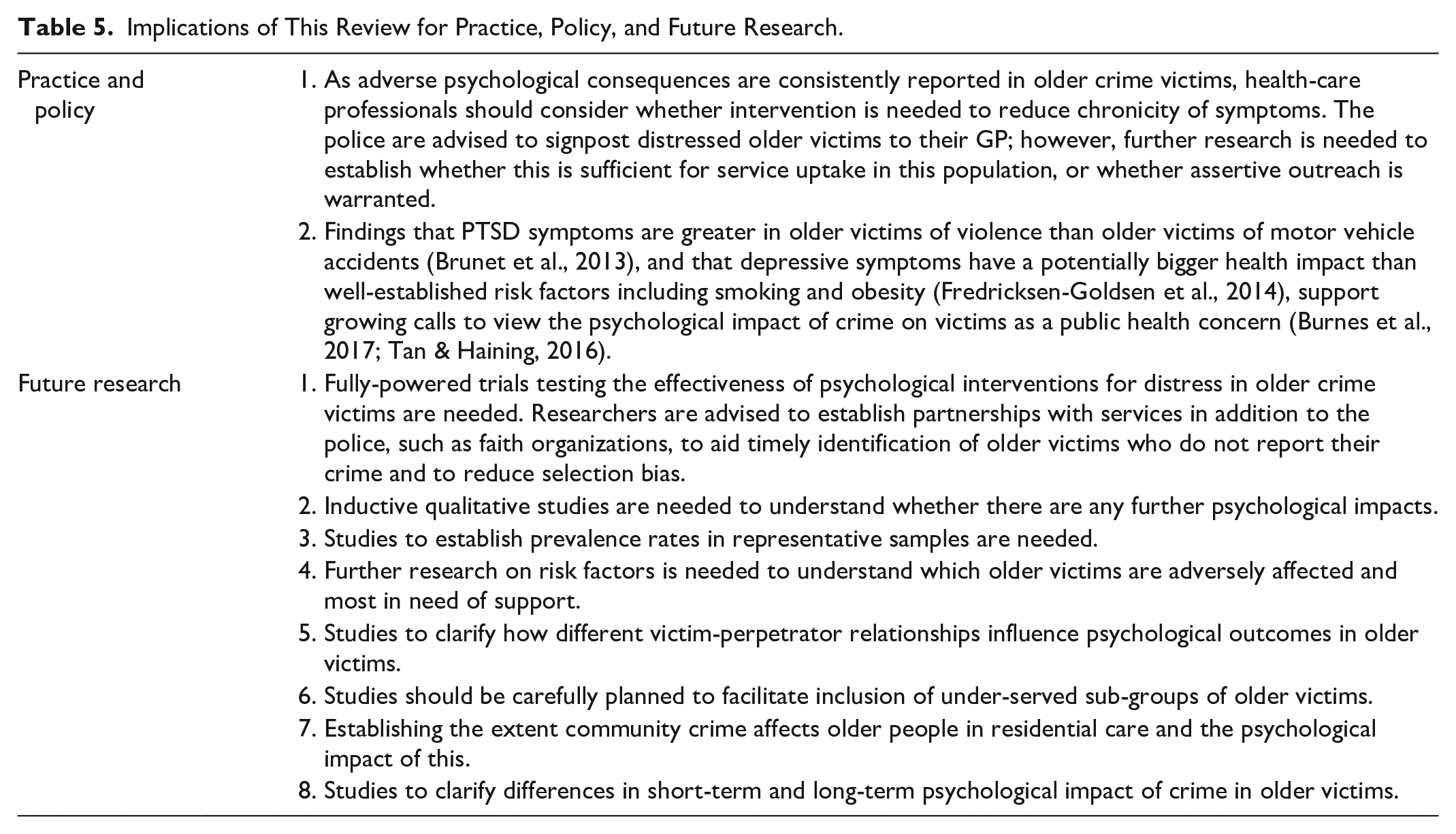
Implications of This Review for Practice, Policy, and Future Research.
Psychological Impact
Through synthesis of all study data, we identified 30 different psychological impacts, outlined in Table 2.
Case Studies
Two early studies from the United Kingdom and United States provided case study data (Jones, 1987; Tyra, 1996). The UK study summarized twelve crime-related incident reports from wardens of sheltered accommodation, which described older victims of burglary and vandalism as “upset” and “frightened” (Jones, 1987). Fraudulent entry and theft was reported to “affect them profoundly,” and it was suggested this may be because of emotional attachment to their home (Jones, 1987, pp. 195–96). The U.S. study described acute and chronic experiences of “rape trauma syndrome” in an older rape victim (Tyra, 1996). Acute experiences included disbelief, recurrent crying, embarrassment, fatigue, poor sleep, intrusive thoughts, feeling vulnerable, insecurity, and intense anger. Chronic experiences included fear of going out at night or staying alone, poor concentration, intrusive thoughts, and ongoing anger. Together, these studies provide insight into the nature of psychological impact in older victims but cannot be generalized due to insufficient numbers.
Qualitative Studies
Four qualitative studies were identified, all focusing on fraud, indicating an evidence gap for qualitative research in older victims of other crimes. These included older victims of the Robert Maxwell Pension scandal in the United Kingdom (Spalek, 1999), attempted and completed scams in Australia and the United Kingdom (Bailey et al., 2020; Cross, 2015), and cyber-scams in India (Tripathi et al., 2019). Reported themes on psychological impact in these studies included: anxiety, depression, reduced self-esteem, loss of trust and confidence, embarrassment, shame, increased skepticism, mistrust, and behavior changes (e.g., avoiding online banking). Self-blame was observed in older victims who felt personally responsible but was absent in older victims scammed by a trusted pension provider; anger was noted instead (Spalek, 1999). It is a strength that two studies considered both attempted and completed scams, but contradictory findings were observed: one observed psychological distress in victims who suffered severe financial losses only (Cross, 2015), the other reported that malicious intention was more distressing (Bailey et al., 2020).
Notable across all four studies was limited detail on interviewing approach (e.g., one-to-one, focus groups), topic guide (e.g., semi-structured), analytical approach, theoretical assumptions, and reflections on researcher background and possible personal biases. All four appeared to approach the data deductively, seeking evidence to support existing ideas on psychological impact, but did not inductively explore whether there were other impacts not yet considered. Taken together, these studies support that fraud adversely affects older victims but inductive analysis with older victims of different crime types is needed to understand the full range of impact.
Descriptive Surveys
Three studies conducted surveys in larger samples of older people asking whether they had been a victim previously and, if so, what psychological impacts they had experienced. The first was in older hospital inpatients in Ireland (N = 272) (O’Neill et al., 1989), which found that of those who reported having been burgled in the previous two years (n = 72, 26%), almost all (90%) reported a psychological impact. These included fear of further crime (n = 57, 79%), anxiety or depression (n = 36, 50%), sleep disturbance (n = 32, 44%), and agoraphobia (n = 32, 44%). The second study was in older adults accessing a community mental health clinic in Manchester, United Kingdom (N = 350) (Simpson et al., 1996). This study found that 100 participants reported having been crime victims; of whom, five (5%) met diagnostic criteria for PTSD. It was not reported when the crimes occurred nor what the clinical presentation of the 95 victims who did not meet diagnostic criteria for PTSD was like, limiting comparisons between these two studies. These two surveys were also conducted in convenience samples of older people accessing healthcare so cannot be generalized to all older victims.
The third study tried multistage sampling 800 older people living in urban China; however, the response rate was low (n = 453, 57%) (Qin & Yan, 2018). Over half of respondents had experienced one or more types of crime (n = 254, 56%). Theft (n = 198, 44%), fraud (n = 140, 31%), and burglary (n = 253, 56%) were most frequently reported while physical assault (n = 5, 1%) and rape (n = 1, 0.2%) were least reported. Experience of crime was a consistently significant predictor of poor mental health on the General Health Questionnaire (Pan & Goldberg, 1990), even when physical health and sociodemographic characteristics were controlled for.
Taken together, these three studies suggest high levels of distress is associated with being a victim of crime, although they cannot be generalized to all older victims. As psychological health before the crime was not known, it is unclear whether poor mental health was because of the crime or preexisting.
Psychological Impact in Older Victims Compared to Older Non-Victims
One recent study of depression using data from a large national survey on ageing in India (N = 31,646) showed that 1.32% of respondents (n = 402) reported having been victims of violent crime, such as assault or mugging, in the previous 12 months (Muhammad et al., 2021). Using the Short-Form Composite International Diagnostic Interview for major depression, 17.7% scored positive compared to 8.52% of non-victims (Unadjusted odds ratio (UOR): 1.54, 95% CI [1.05–2.26]). After controlling for sociodemographic and health variables, the adjusted odds ratio increased to 1.84 (95% CI [1.15–2.95]). A strength of this study is that it reports a representative sample and it sought to measure the association between crime and depression within a defined time-period. However, the direction of association remains unclear, and findings may not be generalizable to nonviolent crime.
Psychological Impact of Crime Compared to Other Trauma Types in Older Victims
One study compared psychological outcomes after crime with another trauma-type in older victims (Brunet et al., 2013). Older adults seeking emergency medical treatment for either physical assault or motor vehicle accidents were assessed for peritraumatic distress symptoms, and followed up 1 week and 1, 6, and 12 months post-incident. Older victims of physical assault scored significantly higher across time-points on the Clinician Administered PTSD Scale (CASP) (mean = 36.1, 95% CI [22.8–49.3]) than older victims of motor vehicle accidents (mean = 15.2, 95% CI [10.8–19.7]) (t = 2.23; p = .03). Consistent with the ageing survey in India, this demonstrates severity of psychological impact in older victims of violence. By using the gold-standard assessment tool for PTSD (CASP) and partnering with a local hospital, assessment was at clearly defined time-points. However, research to understand the severity of psychological impact in older victims of less violent crimes is also needed.
Older Victims Compared to Younger Victims
Three studies investigated psychological distress across age groups. One found no difference between younger and older victims (Tan & Haining, 2016) and two found lower symptoms in older adults than younger adults (Iganski & Lagou, 2015; Norris, 1992). However, these retrospective studies asked participants whether they had been a victim anytime in their lives, meaning acute distress was not measured in older adults and responses may have been affected by recall biases. Results may also have been conflated in these studies. For example, one study (Tan & Haining, 2016) found that female victims of all ages were more likely to report psychological symptoms than males but did not provide a gender breakdown within age groups; lower distress scores in older males may have skewed higher distress scores in older females. Researchers should consider whether there is clinical value in investigating whether one age group is more affected than another as erroneous conclusions in either direction risks excluding vulnerable populations from research.
Risk Factors for Adverse Psychological Outcomes in Older Victims
While studies often analyzed older victims as one group, some have begun to consider the factors that may contribute to distress within this population.
Type of Crime
Psychological distress was reported in older victims of assault (Acierno et al., 2004; Brunet et al., 2013), rape (Tyra, 1996), fraud (Bailey et al., 2020; Cross, 2015; Spalek, 1999; Tripathi et al., 2019), burglary (Jones, 1987), distraction burglary (McGraw & Drennan, 2006), mugging (Muhammad et al., 2021), and vandalism (Jones, 1987), but there is less on the impact of low-value high-frequency crimes such as petty theft. It therefore remains unclear whether psychological distress arises from all crime or specific crime types. Equivocal findings in the fraud studies (Bailey et al., 2020; Cross, 2015) also raise the question whether it is the crime itself or the malicious intent that is distressing in older victims.
Individual Characteristics
Comparatively few studies reported on the influence of individual differences on psychological outcomes. The surveys of older people in urban China (Qin & Yan, 2018) and across India (Muhammad et al., 2021) both found a strong association between experiencing a crime and mental health even after variables such as health, gender, age, education, household finances, and living arrangements were controlled for. Of the victims of violent crime in India, older females living in rural areas had the highest odds of suffering major depression (Adjusted odds ratio (AOR): 2.27, 95% CI [1.25–4.14]) (Muhammad et al., 2021). Further research is needed on the influences of sociodemographic and health variables on psychological outcomes across different crime types.
Two other studies highlight that crimes targeted toward marginalized groups (called “hate crime” in the United Kingdom and “bias crime” in the United States) may be particularly distressing. A study in the United States (Fredriksen-Goldsen et al., 2014) found that transgender older adults (n = 174) reported higher lifetime victimization and depressive symptoms than lesbian, gay, and bisexual (n = 2,201) older adults. Victimization and stigma explained the highest proportion of the total effect of gender identity on health outcomes in transgender older adults, even when compared to other health-related behaviors including smoking and obesity. Another study examining data from the Crime Survey for England and Wales found older victims of racially motivated hate crime were at increased risk of self-reported internalized emotions, although standardized outcomes measures were not used and the findings were not statistically significant (Iganski & Lagou, 2015).
Social Isolation
Two studies suggest that older victims with limited social support may be at risk. An early study (N = 332) found that depressive symptoms were lower in older crime victims with high emotional support than those with low emotional support, although this was not statistically significant and minimal differences were found between those with high informational support and low informational support (Krause, 1986). However, these findings were supported by a more recent study (N = 2,000) which found that although older victims reported increased depressive symptoms after crime, the link was significantly weaker in those with strong attachments to spouse and adult children (Reisig et al., 2017).
Changes in Behavior
Several studies reported behavior changes in older victims including avoiding online banking, avoiding unidentified callers, and increasing home security (Bailey et al., 2020; Qin & Yan, 2018; Tripathi et al., 2019). Crime victimization was found to significantly correlate with “constrained behaviors” in older people in China (Qin & Yan, 2018) and avoidant behaviors in older people in the United States (Reisig et al., 2017). Strong spousal attachments were also found to moderate this link (Reisig et al., 2017). However, while these studies tested a relationship between crime and protective behaviors, and crime and mental health, neither tested a relationship between protective behaviors and mental health. Protective behaviors were also measured based on presence or absence (Qin & Yan, 2018) or frequency (Reisig et al., 2017), which may not be valid in older victims as they were not asked whether this was a change since the crime. In the survey in China, nearly all older people (98.5%) reported engaging in protective behaviors yet only 56% reported having been victims, making it unclear whether these behaviors were in response to the crime or preexisting. The American study (Reisig et al., 2017) also defined avoidance as nonattendance at activities such as the cinema or leisure sports, which may have been confounded by poor physical health. Nonetheless, given several studies observed behavior changes in older victims, further investigation using valid assessment tools to strengthen understanding of these associations is needed.
Taken together, these findings suggest that crime type, sociodemographic characteristics, social isolation, and behavior changes are possible factors that may influence how older victims psychologically respond to a crime.
Interventions
Four feasibility intervention studies for psychological distress in older victims were identified: two nursing schemes (McGraw & Drennan, 2006; Tyra, 1996), a psychoeducation video (Acierno et al., 2004), and an adaptation of cognitive-behavioral therapy (CBT) (Serfaty et al., 2016). There are no published data from fully-powered trials, although further testing of the adapted cognitive-behavioral therapy is in progress (Serfaty et al., 2020).
The first nursing intervention was crisis counselling for an older rape victim (N = 1) delivered alongside medical care (Tyra, 1996). This involved psychoeducation and empathetic listening in the aftermath, longer term linking into social support, and psychoeducation on coping during court proceedings. It was reported that whilst the older victim continued to suffer flashbacks and felt unsafe a year later, crisis counselling meant she was able to continue living independently at home. Standardized outcome measures were not used and, as a case study, the findings cannot be generalized. The aftermath period that crisis counselling was delivered in was not defined, but it is important to note that guidance released since cautions against prematurely intervening before the person has had a chance to recover naturally (NICE, 2018).
The second study described a “nurse-link” collaboration between district nurses (also called “home visiting” nurses) and London police to assess and address health and social care needs of distraction burglary victims aged 70 and over (N = 77) (McGraw & Drennan, 2006). Of these, 19 (25%) scored positive for depression on the Geriatric Depression Scale and 10 (13%) on the Hospital Anxiety and Depression Scale. Health and social care were coordinated for these older victims and follow-up case studies describe successful outcomes. While it is not possible to evaluate the effectiveness of descriptive studies, further feasibility research would be worthwhile as this highlights the possible benefits that could be achieved by embedding support within existing nursing services.
The psychoeducation video was delivered in “real-world settings” by local police for older victims of violence in South Carolina (N = 116) and was compared to existing advocacy in a pilot randomized controlled trial (Acierno et al., 2004). Participants who received the video had greater knowledge when assessed later that day, but no differences were found between treatment groups on the Geriatric Depression Inventory or Beck Anxiety Inventory at 6-week follow-up. Genuine differences may have been missed as power calculations were unreported, inclusion was based on victim status rather than distress scores, the intervention was delivered within a few weeks of the crime, researchers were not blinded, randomization technique was not reported, and missing data was high (29%). Baseline assessment was not conducted so there was no data on pretreatment psychological distress scores, and knowledge retention at follow-up was not collected so within-groups changes could not be assessed. Further feasibility work addressing these limitations is recommended as a psychoeducation video would be low cost to deliver if found clinically effective.
Serfaty et al. (2016) partnered with local police and Victim Support to systematically identify older victims of different crime types within a month of reporting a crime, and screen for depression, anxiety, and PTSD at 1 and 3 months after. As many as 27.6% of older victims were found to have continued distress symptoms 3 months later, but this small feasibility sample was not representative of the general population, providing only a preliminary prevalence estimation. Those who continued to screen positive 3 months post crime were offered a diagnostic interview. Of those, N = 26 participated in a feasibility RCT of modified CBT compared to treatment-as-usual. Modified CBT was found to be acceptable and appeared promising for treating anxiety and depression but not PTSD. It is a strength that this study systematically identified, assessed, and treated older victims using standardized measures within a defined timeframe. Further evaluation through a fully powered RCT is needed to determine the efficacy of this treatment, which is now underway (Serfaty et al., 2020).
Discussion
This is the first systematic narrative review and quality appraisal of existing research on psychological impact and interventions for older crime victims living in the community. Through systematic searching we found 20 studies on psychological distress in older victims, 4 of which included interventions.
Our first aim was to synthesize existing evidence on psychological impact in older victims. While studies varied across aims, outcome definitions, and included crimes, adverse impacts in older victims were consistently reported. Thirty different psychological impacts were identified, with particular emphasis on internalized anxious and depressive symptoms. Initial prevalence estimates that 28% of older victims of different crime types continue to suffer depression and/or anxiety 3 months later (Serfaty et al., 2016) is considerably higher than rates for depression (7%) and anxiety (4%) in older people globally (WHO, 2017). For violent crime, depressive symptoms are even higher (Muhammad et al., 2021) and greater PTSD symptoms have been reported than in older victims of motor vehicle accidents (Brunet et al., 2013). Depression attributed to victimization has a potentially bigger health impact than well-established risks including smoking and obesity (Fredriksen-Goldsen et al., 2014). Our findings follow on from earlier physical health studies which found older victims of violence and burglary are at increased risk of nursing home placement and accelerated mortality (Donaldson, 2003; Lachs et al., 2006). Together, this supports growing calls to acknowledge the impact of crime on victims as a public health concern (Burnes et al., 2017; Tan & Haining, 2016).
Our second aim was to identify existing interventions for psychological distress in older victims. While intervention research is in its infancy, it is encouraging that modified CBT was acceptable and favorable for treating anxious and depressive symptoms (Serfaty et al., 2016) and that this is now being further tested (Serfaty et al., 2020). Partnering with local healthcare and police services also appears promising for timely identification, recruitment, and intervention delivery (Acierno et al., 2004; McGraw & Drennan, 2006). As not all crimes are reported, and uptake of mental health services is low in both older adults and crime victims of all ages (MacDonald, 2002; McCart et al., 2010; Nair et al., 2019), future research should consider other partnerships to engage older victims not known to these services. This may include faith organizations, as promising results have been found for spiritually-focused group interventions in older female victims of domestic violence (Bowland et al., 2012). Interventions targeted toward social inclusion and enhancing quality of social connections may also be beneficial (Zagic et al., 2021) given findings that social support moderates distress in older victims (Reisig et al., 2017). While randomized controlled trials are the gold-standard for intervention research, single case experimental design may be more cost-effective for testing interventions in older crime victims as statistical power can be achieved through repeat-testing fewer participants compared to conventional trials (Brysbaret, 2019).
Our third and final aim was to quality appraise the literature so that recommendations to strengthen the evidence can be made. Priorities for future research include establishing prevalence in representative samples, understanding how different crime types and victim-perpetrator relationships influence outcomes, understanding both the short-term and long-term impact of crime, and further feasibility and evaluation of interventions. Inductive qualitative research is needed to explore whether there are further impacts not yet identified. Few studies discussed externalized emotions such as anger, yet this was found to be an important part of the phenomenology of crime-related PTSD in violence victims aged 18 years and over (Andrews et al., 2000). Further research on risk factors is recommended as understanding which older victims are most adversely affected will ensure effective allocation of resources and development of targeted interventions. Studies should also be carefully planned to ensure accessibility to under-served groups (NIHR-INCLUDE, 2020). This may include older victims from ethnic minorities, who do not speak English, who lack trust in statutory services, are without permanent residency, or have mobility or sensory disabilities (Bodicoat et al., 2021).
Consistency of outcome definitions can be improved by adhering to DSM or ICD diagnostic criteria (American Psychiatric Association, 2013; WHO, 2004). Use of standardized assessment tools would strengthen study comparability. Validated tools include the Patient Health Questionnaire (Arolls et al., 2010) or Beck Depression Inventory (Beck et al., 1996) for depression, the General Anxiety Disorder (Plummer et al., 2015) or Beck Anxiety Inventory (Beck & Steer, 1990) for anxiety, and the Clinician Administered PTSD scale (Weathers et al., 2015) for PTSD. Use of the Traumatic Events Scale is also advised as it can discriminate between people with severe and mild distress to detect which individuals would most benefit from treatment (Sundin & Horowitz, 2002). Standardizing assessment and intervention to 3 months post-incident has been recommended in other trauma populations as it allows time for natural recovery without prolonging suffering in victims with continued symptoms (McNally et al., 2003). This would also build on existing research identified in this review (Serfaty et al., 2016, 2020).
While reporting guidelines were not available when many of the studies were published, future research should follow these to reduce missing detail, including CONSORT for RCTs, STROBE for observational studies, and SRQR for qualitative studies (The Equator Network, 2022). We recommend that researchers also specify which crimes have been included, when the crimes occurred, and whether the victim had a preexisting relationship with the perpetrator or not. As older adults range from individuals in good health and living independently to those who are frail and nearing end of life, clarifying which phase of late adulthood the study findings are most relevant to will help inform treatment decisions (Jaul & Barron, 2021). Finally, studies should confirm research ethics approval has been obtained and outlined how procedures adhere to ethical research guidance for older trauma victims (McGuire, 2009; Seedat et al., 2004). This includes obtaining informed consent, ensuring confidentiality, and safeguarding procedures if a participant were to disclose ongoing abuse.
Our systematic review is a comprehensive synthesis of a limited evidence base. While many studies included have bias risk, recommendations to improve methodological quality have been made. Only studies published in English were included, however, few studies published in other languages were noted during screening meaning the number of studies missed is likely to have been small. We purposefully included only peer-reviewed studies as recommended for reviews with limited resources as non-published studies often have more methodological issues and introduce further bias rather than reduce it (Egger et al., 2003). Our included studies focused on older victims living in the community as this is where most of these crime types occur, however, understanding the extent of such crime and its impact in older people in nursing homes and long-term residential care may be an important area to include in future research.
To conclude, there is growing evidence that older adults are adversely psychologically impacted by crime. Further research following methodological recommendations outlined in this review is urgently needed to improve outcomes in this neglected population.
Footnotes
Acknowledgements
Thank you to Professor Gloria Laycock, Professor Chris Brewin, and Dr. Martin Blanchard for providing feedback on the review protocol in preparation for submission to Prospero and to Jacquie Smith for advising on the search strategy.
Author’s Note
Marc Serfaty is also affiliated to The Priory Hospital North London, London, UK.
Author Contributions
JS designed the review, coordinated, and performed all review activities, and wrote the manuscript. TC was a second reviewer for screening, data extraction, and quality assessment. VMD was nominated as the third reviewer with final decision where study eligibility was unclear. MS and JB supervised the review. All authors read, commented on, and approved the final manuscript.
Data Availability
Details on search strategy, data extracted from included studies and quality assessment are provided in this review. Further supplementary materials including complete search strategy and full-text review decision log are available from the corresponding author on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JS and MS are funded by the NIHR-PHR Victim Improvement Package Trial (grant number 13/164/32), a study which is referenced in this review (Serfaty et al., 2020). The views expressed are those of the authors and not necessarily of the NIHR or the Department of Health and Social Care. The funders had no other role other than financial support.