
Abstract
Maltreated children are at risk of exhibiting attachment disorders: The reactive attachment disorder (RAD) and the disinhibited social engagement disorder (DSED). Determining overall proportions for these disorders, however, is difficult. Assessment methods have varied across studies and over time due to a shift in diagnostic criteria from the Diagnostic and Statistical Manual of mental disorders - 4th Edition (DSM-IV) to the DSM-5. This study examines the overall proportion of RAD-DSED combined (34 studies with 47 independent samples, 8994 participants), RAD (16 studies with 19 independent samples, 1,924 participants), and DSED (16 studies with 21 independent samples, 2,018 participants). Inclusion criteria were all empirical English studies reporting on at least one RAD or DSED classification/diagnosis in children 9 months to 18 years old. Moderators included child age and sex, sample type, measure type, nosological system type, year of publication, study geographical region, and study quality. Random-effects meta-analyses with logit transformation of event proportions were conducted. Publication bias was not tested, given that symmetry assumptions do not apply to proportion data. Results set the overall proportions of attachment disorders in at-risk samples (RAD-DSED combined) at 18.4% [13.4%, 24.9%], 9.6% for RAD [6.6%, 13.7%], and 20.1% for DSED [12.2%, 24.7%]. Some RAD-DSED combined, RAD, and DSED proportions varied according to types of measures, nosological systems, and geographical region of study. Results indicate a decline in RAD proportions since the advent of the DSM-5 in 2013 (from 8.4% [6.5%, 10.9%] to 4.6% [1.4%, 5.6%]), and the DSM-5 algorithm for RAD is markedly more restrictive than that of the Research Diagnosis Criteria (RDC).
Keywords
Introduction
The DSM-5 lists two distinct attachment disorders, namely, the reactive attachment disorder (RAD) and the disinhibited social engagement disorder (DSED), which can be diagnosed in children as of age 9 months. Children with RAD rarely seek comfort when distressed and are minimally responsive to caregiver comforting efforts. Children with DSED tend to actively approach and interact with unfamiliar adults in a manner that is overly familiar and inconsistent with culturally sanctioned and age-appropriate social boundaries (APA, 2013, 2022). The etiology of RAD and DSED has been linked to extreme neglect and severe deprivation in infancy, as observed in many institution-reared or maltreated children (Zeanah & Gleason, 2015, 2021). To gain a clearer understanding of attachment disorders, the current study aims to synthesize the overall proportions of RAD and DSED as reported across various studies.
Since the publication of the DSM-III in 1980, the diagnostic criteria for these disorders have undergone numerous revisions. Some 15 years ago, the diagnostic criteria for attachment disorders differed considerably across nosological systems: the DSM-IV (APA, 2000), the International Statistical Classification of Diseases and Releated Health Problem – 10th Revision (ICD-10; World Health Organization, 1994–2019), the Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood: 0-3 (DC:0-3; Zero to Three, 2005). Today, criteria of the ICD-11 (World Health Organization, 2022) and the DC:0–5 (Zero to Three, 2016) are more convergent with those of the latest DSM-5 (see Supplemental Tables 1 and 2 for behavioral diagnostic criteria for RAD and DSED in the DSM-5, DSM-IV, ICD-10, and DC:0–3R). Before publication of the DSM-5 in 2013, RAD and DSED were classified as subtypes of a single disorder: (a) RAD of the inhibited type (RADi), which became RAD in the DSM-5; and (b) RAD of the disinhibited type (RADd), which became DSED in the DSM-5. Overall, although DSM-5 changes are grounded in research (e.g., Zeanah & Gleason, 2015) showing that RAD and DSED have different correlates (i.e., intervention response, associations with other symptoms), they raise questions about the proportions of these disorders over time, underscoring the need for a meta-analytic review that also examines whether proportions vary according to certain moderators. In the current study, the acronym RAD refers to all RAD variants (e.g., RAD in the DSM-5, RADi in the DSM-IV, RAD in the ICD-10), DSED to all DSED variants (e.g., DSED in the DSM-5, RADd in the DSM-IV, DAD in the ICD-10), and RAD-DSED combined to unspecified attachment disorders (RAD or DSED), as some studies do not report separate proportions for RAD and DSED.
Sample-Level and Study-Level Moderators of RAD and DSED Proportions
Proportions for attachment disorders can fluctuate depending on various factors specific to children (sample type, age, and sex), study methods (type of measure used to assess each of these diagnoses, study design, and quality), and study context (country of study, year of publication). These factors may explain the wide range of proportions reported across studies. The following subsections, organized by moderator type, describe the variability observed across studies and the potential impact of each moderator on the reported proportions.
Sample Type
Proportions of RAD and DSED vary considerably across sample types. Studies on community-living children report very low rates, never exceeding 1% (Minnis et al., 2020, Skovgaard et al., 2008, Upadhyaya et al., 2019). In socioeconomically high-risk samples, rates are also generally low, ranging from 0% to 13% (Boris et al., 2004; Minnis et al., 2013; Kay et al., 2016; Pritchett et al., 2013). In other high-risk samples, rates tend to be higher, with substantial variability across studies. For example, in psychiatric care samples, often involving parental separation, maltreatment without placement, or children with severe regulation problems and special education needs, rates vary widely, ranging from 4% to 42% (Bosmans et al., 2019; Dowdy-Hazlett & Boel-Studt, 2021; Equit et al., 2011; Giltaij et al., 2017; Kay et al., 2016; Løkkegaard et al., 2019; Scheper et al., 2016, 2019). Among children placed in foster care (FC) following maltreatment, studies report low to high rates, ranging from 2% to 51%, with DSED generally higher than RAD (Allen & Schuengel, 2020; Archambault et al., 2024; Boris et al., 2004; Bruce et al., 2019; Herd et al., 2023; Lehmann et al., 2013; Jonkman et al., 2014; Jorjadze et al., 2023; Kay et al., 2016; Kliewer-Neumann et al., 2018; Leloux-Opmeer et al., 2017; Schröder et al., 2019; Scheper et al., 2016; Strijker et al., 2008; Wiefel et al., 2005; Zeanah et al., 2004). In residential care (RC), such as in group homes, youth care centers or intensive youth justice service facilities, rates range from 7% to 30% (Archambault et al., 2024; Moran et al., 2017, 2024; Seim et al., 2020). In children reared in institution (orphanages) during early childhood, deprived of parental care prior to being placed in FC or adopted, studies also show low to high rates, ranging from 1% to 27%, with DSED again being the highest (Ayaz et al., 2012; Gleason, Fox et al., 2011; Jorjadze et al., 2023; Kroupina et al., 2023).
Child Age and Sex
Differences in RAD and DSED proportions may be related to child age. In samples of institution-reared children, one study has shown RAD to be more frequent before age 5 and to decline as children developed, particularly when placed in an adequate substitute home setting (Zeanah & Gleason, 2015, 2021). In contrast, another study found that the proportion of DSED remained relatively stable across childhood, even after placement in an adequate substitute home setting (Gleason, Fox et al., 2011). Consequently, it is difficult to determine whether RAD and DSED proportions are influenced by the age of the child or by changes in caregiving quality (Rutter et al., 2007). Furthermore, few studies have examined whether RAD and DSED rates vary by child sex. Some studies report similar RAD and DSED rates for boys and girls (Guyon-Harris et al., 2019; Guyon-Harris et al., 2018; Lehmann et al., 2013; Rutter & O’Connor, 2004). However, one study showed that boys benefited more quickly from positive changes in caregiving (Kliewer-Neumann et al., 2023), suggesting that boys may be at lower risk of exhibiting DSED behaviors than girls. Another study showed a higher DSED rate among girls (17%) than boys (5%) in RC (Archambault et al., 2024).
RAD and DSED Measures
The practice parameters of the American Academy of Child and Adolescent Psychiatry for attachment disorders (Zeanah et al., 2016) recommend clinical evaluations using standardized and validated tools, and adopting a multi-informant, multi-method approach (i.e., combining questionnaires, observation, and diagnostic interviews) to establish these diagnoses. Specifically, Zeanah et al. (2016) emphasize that systematic observation of the child interacting with primary caregivers should be part of the evaluation process, although this is not consistently implemented in practice. To date, various questionnaires (e.g., Relationship Problems Questionnaire [RPQ]: Minnis et al., 2009), interviews (e.g., Disturbance of Attachment Interview [DAI]: Zeanah et al., 2005; preschool age psychiatric assessment [PAPA]: Seim et al., 2020), and observational measures (e.g., Waiting Room Observation [WRO]: Minnis et al., 2009; Rating for Infant-Stranger Engagement [RISE]: Lyons-Ruth et al., 2009) for DSED have undergone varying degrees of validation. However, only one questionnaire (Early TRAuma-related Disorders Questionnaire [ETRAD-Q]: Monette et al., 2022), one semi-structured interview (Reactive Attachment disorder and Disinhibited social engagement disorder Assessment [RADA]: Archambault et al., 2024; Lehmann et al., 2018), and one observational measure (Rating of inhibited Attachment Behavior [RinAB]: Corval et al., 2019; Spangler et al., 2019) for RAD are based on DSM-5 diagnostic criteria. Notably, the DAI interview (Smyke & Zeanah, 1999) was developed prior to DSM-5, and its items played a key role in shaping the DSM-5 criteria. The types of measures used to diagnose or classify RAD and DSED have likely moderated proportions of these disorders reported in the literature.
Nosological Systems, Geographical Region, and Year of Publication
The DSM-5 introduced two major changes to diagnostic criteria for RAD and DSED. First, it proposed a more restrictive diagnostic algorithm compared to the DSM-IV-TR and the ICD-10, which previously described behaviors without specifying a required number of criteria (see Supplemental Tables 1 and 2). Second, the description for both disorders changed considerably. For example, for DSED, the DSM-IV-TR was characterized by the absence of selective attachment (e.g., diffuse attachment, lack of selectivity in the choice of attachment figure), whereas in the DSM-5, these symptoms are no longer part of DSED and are instead associated with RAD. Similarly, the DSM-IV-TR described RAD as generally involving problematic social behavior (persistent failure to initiate or respond in a developmentally appropriate fashion to most social interactions), post-traumatic symptoms (hypervigilant, frozen watchfulness), and disorganized attachment behaviors (contradictory responses to caregivers). These features were removed from the DSM-5 criteria for RAD.
The number of studies of attachment disorders has increased substantially since the early 2000s. However, most of these studies used instruments developed before publication of the DSM-5 and were conducted primarily in Western Europe than in North America. Consequently, the proportion of children with RAD or DSED could have been overestimated on account of the absence of the more restrictive diagnostic criteria in the DSM-IV-TR and the ICD-10, especially in Western European samples. In 2011, Gleason, Fox et al. (2011) proposed alternative criteria to those of the DSM-IV-TR, known as the Research Diagnostic Criteria (RDC), which have been used in the studies such as those by Bosmans et al. (2019), Gleason, Fox et al. (2011), Jorjadze et al. (2023), and Scheper et al. (2016, 2019). Based on items of the DAI, criteria of the RDC are akin to those of the DSM-5, though markedly less restrictive (see Supplemental Tables 1 and 2). Given the differences in conceptualization across DSM-IV-TR, DSM-5, ICD-10, and RDC, the nosological system used in the studies, their year of publication, and the geographical region of studies represent three (inter-related) potential moderators that may have influenced the proportions of children diagnosed with these disorders.
The Current Study
The objective of this study was to synthesize meta-analytically the overall proportion of children with RAD-DSED combined, RAD, or DSED, and to examine the conditions under which these proportions may vary. We hypothesized that the proportions of RAD-DSED combined, RAD, and DSED would be lower in community samples than in at-risk samples, and that among at-risk samples, proportions would be higher in samples of children with a history of maltreatment, deprivation, placement, or with mental health problems than in samples at socioeconomic risk. Also, we hypothesized that observation-based assessments would yield lower proportions than interview-only assessments. Moreover, given the more restrictive DSM-5 criteria, we expected DSM-5 to produce lower proportions than other nosological systems (DSM-IV/DSM-IV-R, ICD-10, and DC: 0-3R) and the RDC research system. Because the DSM-5 studies have been published more recently, we also expected a decline in proportions in more recent studies. Finally, we explored whether proportions of RAD and DSED differed significantly. We also hypothesized that RAD-DSED combined, RAD, and DSED proportions would be more often diagnosed in Western Europe than in North America.
Method
This meta-analysis was conducted following the recommendations outlined in the PRISMA guidelines (Page et al., 2021).
Protocol and Registration
The protocol for the meta-analysis was not pre-registered.
Eligibility Criteria, Information Sources, and Search Strategy
To be included in the meta-analysis, empirical studies had to have at least one RAD or DSED classification or diagnosis (no continuous score or odds ratio; dichotomous variable: presence or absence of RAD or DSED), involving children 9 months to 18 years old, and had to be drafted in English. Articles published in scientific journals, book chapters, and doctoral dissertations were found through the PsycINFO, PubMed, Scopus, ProQuest Dissertations and Theses search engines, and in works of reference. The reference lists of these documents were reviewed to ensure no articles relevant to our research question were omitted. The following keywords were used: “Abstract: ‘attachment Disorder’ OR Abstract: ‘Disinhibited attachment’ OR Abstract: ‘Reactive Attachment’ OR Abstract: ‘inhibited attachment’ OR Abstract: ‘lack of attachment selectivity’ OR Abstract: ‘disinhibited social engagement’ OR Abstract: ‘indiscriminate social behavior’ OR Abstract: ‘disinhibited social behaviors’ OR Abstract: ‘indiscriminate friendliness’.” The search was run from February to May 2024.
Selection and Data Collection Processes
The study selection process was carried out by three research assistants in three stages. First, the first author identified studies using the keywords in the search engines. Then, after duplicate studies were eliminated, two other research assistants screened studies and read abstracts and titles. Next, the first author reviewed the selected articles and determined their eligibility by reading them in full. When multiple studies were based on the same sample, those with the largest sample size or that assessed RAD and DSED with more than one measure were selected (e.g., Castle et al., 2006). Studies reporting questionnaire-based proportions were excluded as this method is used only to screen for the presence of attachment disorders (e.g., Monette et al., 2022). Moreover, large-scale epidemiological studies with thousands of children were excluded to minimize potential statistical bias arising from heterogeneity in study design and the over-weighting influence of large sample sizes on the meta-analytic pooled proportions. The first author contacted researchers to obtain sociodemographic data when missing from articles, and the requested data were provided.
A coding system was developed to extract the following information from each of the studies: (a) general study characteristics: year of publication, geographical region of study; (b) sample characteristics: child sample’s mean age and sex (% of boys in the sample), sample type (community, at socioeconomic risk, clinical (without placement history), maltreatment/FC, maltreatment/RC, and deprivation/institution/orphanage); (c) methodological characteristics: RAD and DSED measures (interview without observation, interview with observation, diagnosis extracted from clinical files [without information on the assessment method]), nosological system (DSM-5, DSM-IV-TR, ICD-10, DC:0-3R, or RDC). The coding system is presented in Supplemental Table 3. The data collection process was carried out by the first author and two research assistants. Interrater agreement, on 40% of the studies, was excellent (ricc = 1.00, kappa from .88 to 1.00). Differences in the data collected were resolved consensually between coders.
Effects and Synthesis Methods
Comprehensive Meta-Analysis (CMA) version 4.0 was used for all analyses. Event ratios (ERs) were calculated for each diagnostic subgroup within a study and represent the observed proportion of events for that subgroup (e.g., one ER for RAD and one for DSED). There were no overlapping participants between subgroups. When studies included multiple subgroups based on sample type, each subgroup was also treated as an independent unit (e.g., one ER for RAD children in FC and one ER for RAD children in RC). ERs were not derived from comparisons between subgroups within a study. Moreover, a single study could contribute more than one independent ER to the three meta-analyses (#1: DSED-RAD combined, #2: RAD, #3: DSED). Particularly for the first meta-analysis (DSED-RAD combined), only one ER per study was extracted, combining RAD and DSED data unless separate data were available for different sample types. Overall, because ERs were independent, multi-level meta-analyses were not required.
Random-effects models were applied to estimate pooled ERs, reported as proportions (%) in the current study. These models account for variability both within and between studies. For ERs, CMA uses a logit transformation and applies a continuity correction to handle zero or 100% events. Specifically, when a group had zero events, CMA adds 0.5 to each cell to prevent computational issues (Borenstein et al., 2021). All selected studies reported (a) a RAD proportion, (b) a DSED proportion, and/or (c) a RAD-DSED combined proportion. With this data, we conducted three meta-analyses. The first meta-analysis focused on RAD-DSED combined. It included all studies reporting a proportion of children with an attachment disorder, whether the disorder type was unspecified (e.g., Ayaz et al., 2012), explicitly identified as RAD-DSED combined (e.g., Jonkman et al., 2014), or identified as two separate disorders (RAD and DSED) for which we summed the proportions (e.g., Allen & Schuengel, 2020) to avoid double-counting from a single study participant without a disorder. The second and third meta-analyses only included studies reporting proportions of children with RAD only or DSED only, respectively. The Q statistic was used to examine the heterogeneity in effect sizes across studies. The Q’ statistic (Borenstein et al., 2021) was used to compare sets of study effect sizes as a function of categorical moderators: RAD and DSED measure type, nosological system, geographical region of study, and study quality. Comparisons were tested only when two or more of the subsets of studies consisted of at least four studies (Bakermans-Kranenburg et al., 2003). For continuous moderators, such as child age and sex, and year of publication, meta-regressions were performed. These analyses provided b-weighted and z-value statistics for each moderator tested.
Study Risk of Bias Assessments: Individual and Across Studies
The risk of bias in individual studies was assessed by evaluating study quality. The Mixed Method Appraisal Tool (Hong, Pluye, et al., 2018) was used to evaluate five methodological components of quantitative descriptive studies: (a) “Is the sampling strategy relevant for addressing the research question?”; (b) “Is the sample representative of the target population?”; (c) “Are the measurements appropriate?”; (d) “Is the risk of nonresponse bias low?”; and (e) “Is the statistical analysis appropriate for answering the research question?” Coders indicated whether each of these quality criteria was met on a scale ranging from 0% (no criterion was met) to 100% (all criteria were met). Of the final 34 included studies, 4 received a high score (100%), 11 received a very good score (80%), 16 were classified as having a good score (60%), and 3 received a medium score (40%). Study quality scores were examined as a four-category moderator in each of the three meta-analyses. Two coders independently assessed the study quality of 44% of studies (15 of 34 studies). Interrater reliability coefficients for each component ranged from good to excellent (kappa = 1.00 and ricc from .73 to 1.00). Finally, we did not perform publication bias testing (such as with a funnel plot), as it is not recommended for meta-analyses based on proportions, for which symmetry cannot be assumed (Barker et al., 2021).
Results
Study Selection
An initial total of 972 published studies was found, and 116 additional studies were identified through other sources (theses from ProQuest and Thesis Global). Studies were published between 2004 and 2024. After duplicates were removed, 769 abstracts were screened. As a result, 722 studies were excluded, 644 by automation tools and 78 based on study abstracts and titles. Studies were excluded either because they were reviews, theoretical articles, qualitative studies, case reports, they reported attachment classification as secure, insecure, or disorganized, or they did not include any empirical data from which to compute proportions. Finally, 45 full-text studies were assessed for eligibility, of which 11 studies were excluded because (a) RAD or DSED proportions were assessed with a screening questionnaire only (n = 5), (b) proportions were odds ratios or a continuous score (n = 4), or (c) only symptoms of an attachment disorder were reported, with no information on diagnosis/classification (n = 2). Finally, 34 studies with 47 independent ERs and 8,894 participants were included in the current meta-analyses. The flow diagram of the study search and selection is shown in Figure 1.
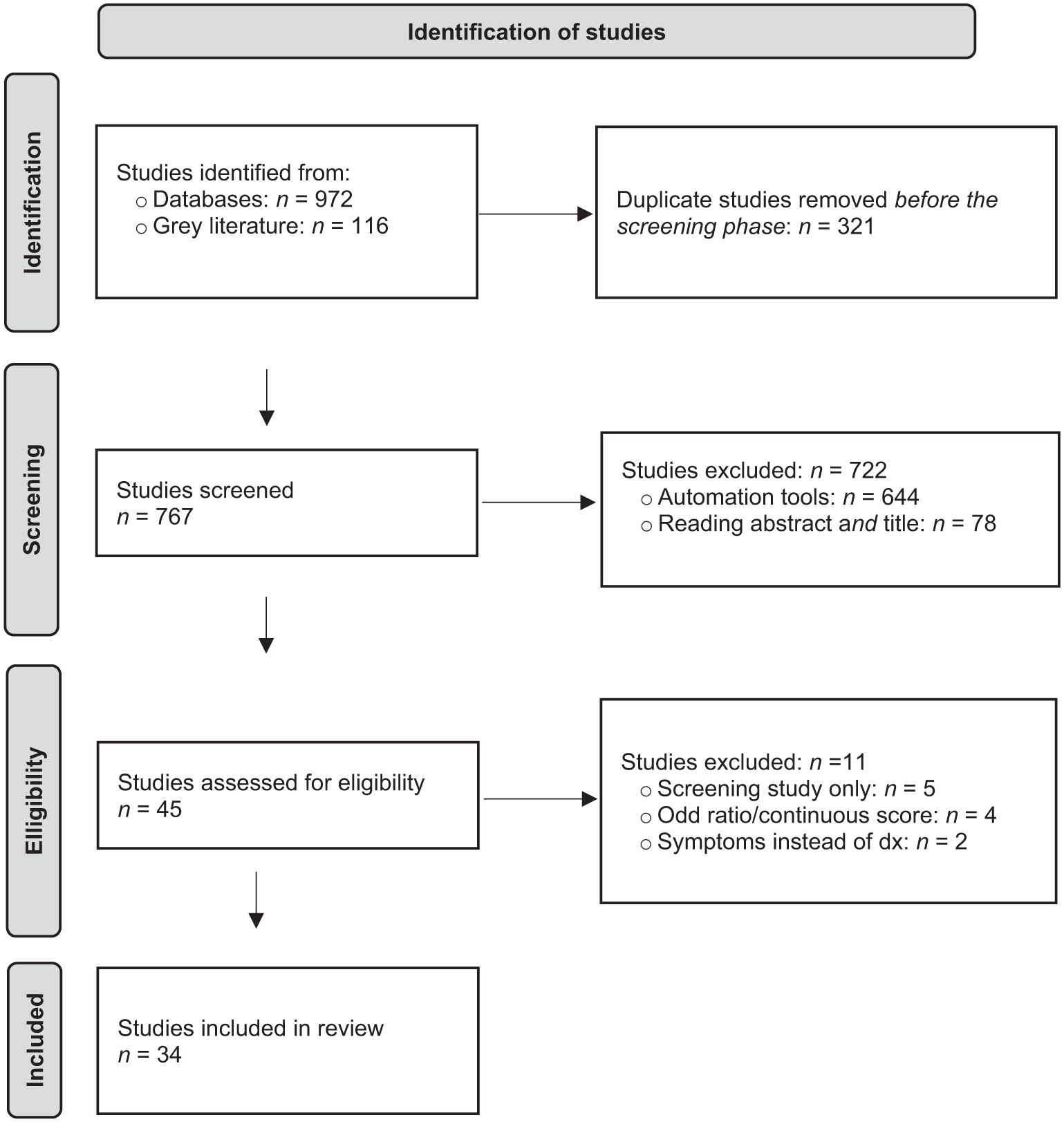
Flow diagram of the study search and selection.
Study Characteristics
The characteristics of each study are presented in Supplemental Table 4. Sample sizes ranged from 20 to 1,646 children, and the studies were conducted in 13 different countries. A large majority of the studies were conducted in Western Europe (k = 25), followed by North America (k = 10), Eastern Europe (k = 3), Africa (k = 2), and the Middle East (k = 1). Fourteen studies assessed preschool-age children, 16 school-age children, and 4 adolescents. On average, 57% of the sampled children were boys. As for sample type, 7 studies included children from the community and 40 from at-risk groups. Of the at-risk samples, 4 included children at socioeconomic risk, 11 from clinical populations (e.g., conduct problems, attention deficit problems) with no placement history, 16 with a maltreatment and FC history, 5 with a maltreatment and RC history, and 4 with a deprivation and institution rearing history. Participant diversity was not assessed due to limited reporting (e.g., on ethnicity) in individual studies.
Results of Meta-Analyses
Forest plots displaying study ERs for each subtype of attachment disorder (RAD-DSED combined, RAD, and DSED) are presented in Figure 2. ERs as a function of moderators, for each attachment disorder, are presented in Tables 1, 2, and 3.
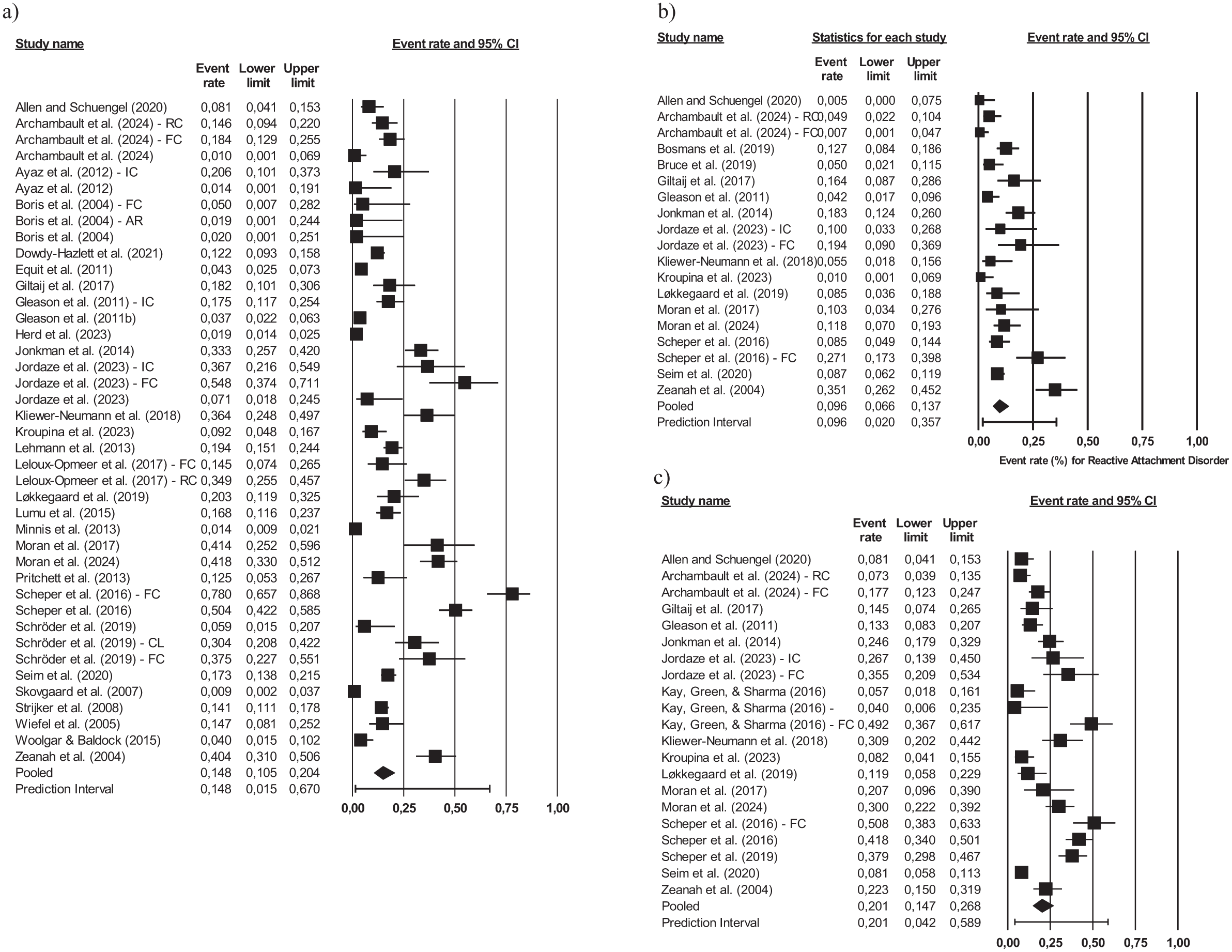
Forest plots for (a) RAD-DSED combined, (b) RAD, and (c) DSED.
Proportions for RAD-DSED Combined and as a Function of Moderators.
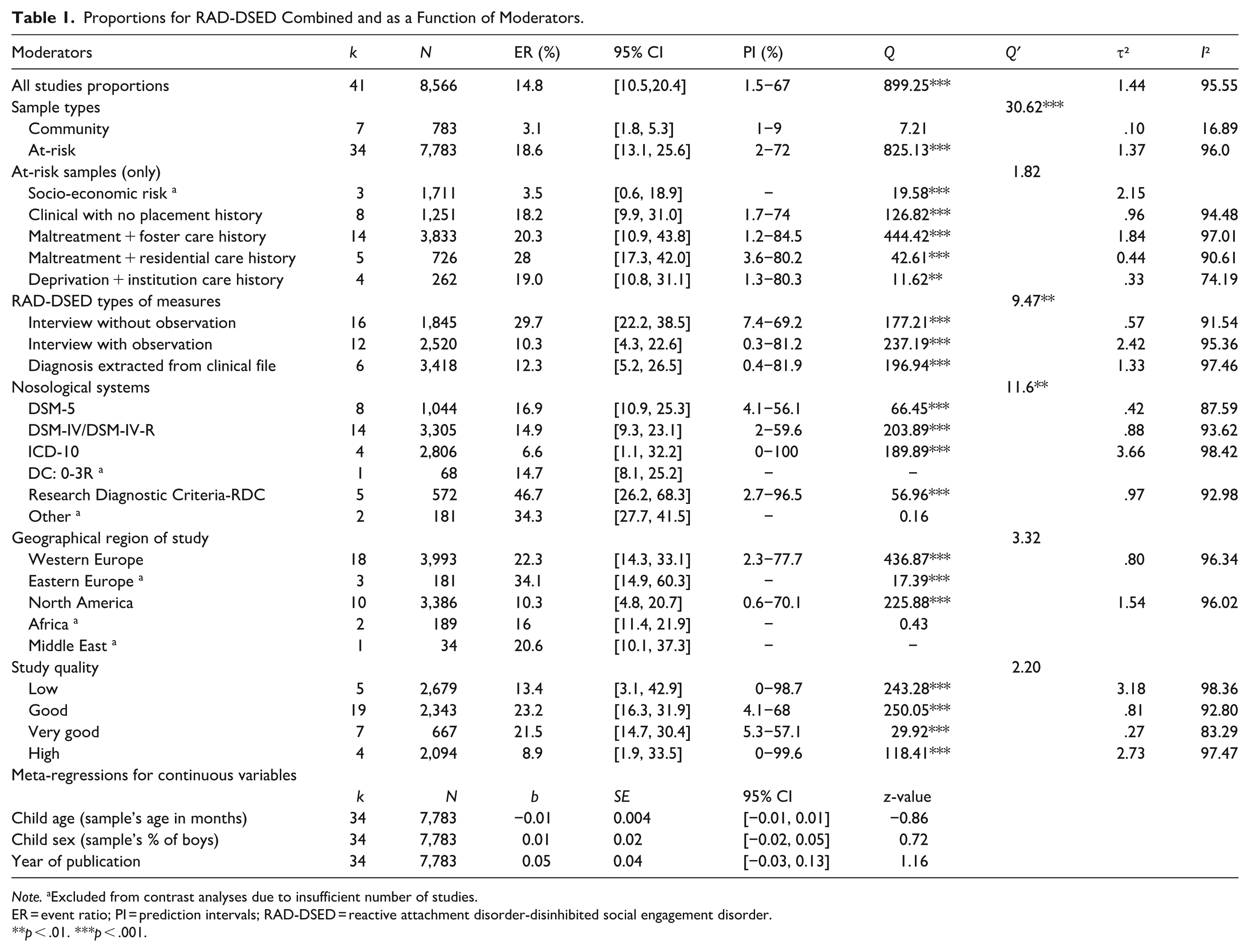
Note. aExcluded from contrast analyses due to insufficient number of studies.
ER = event ratio; PI = prediction intervals; RAD-DSED = reactive attachment disorder-disinhibited social engagement disorder.
p < .01. ***p < .001.
Proportions for the RAD and as a Function of Moderators.
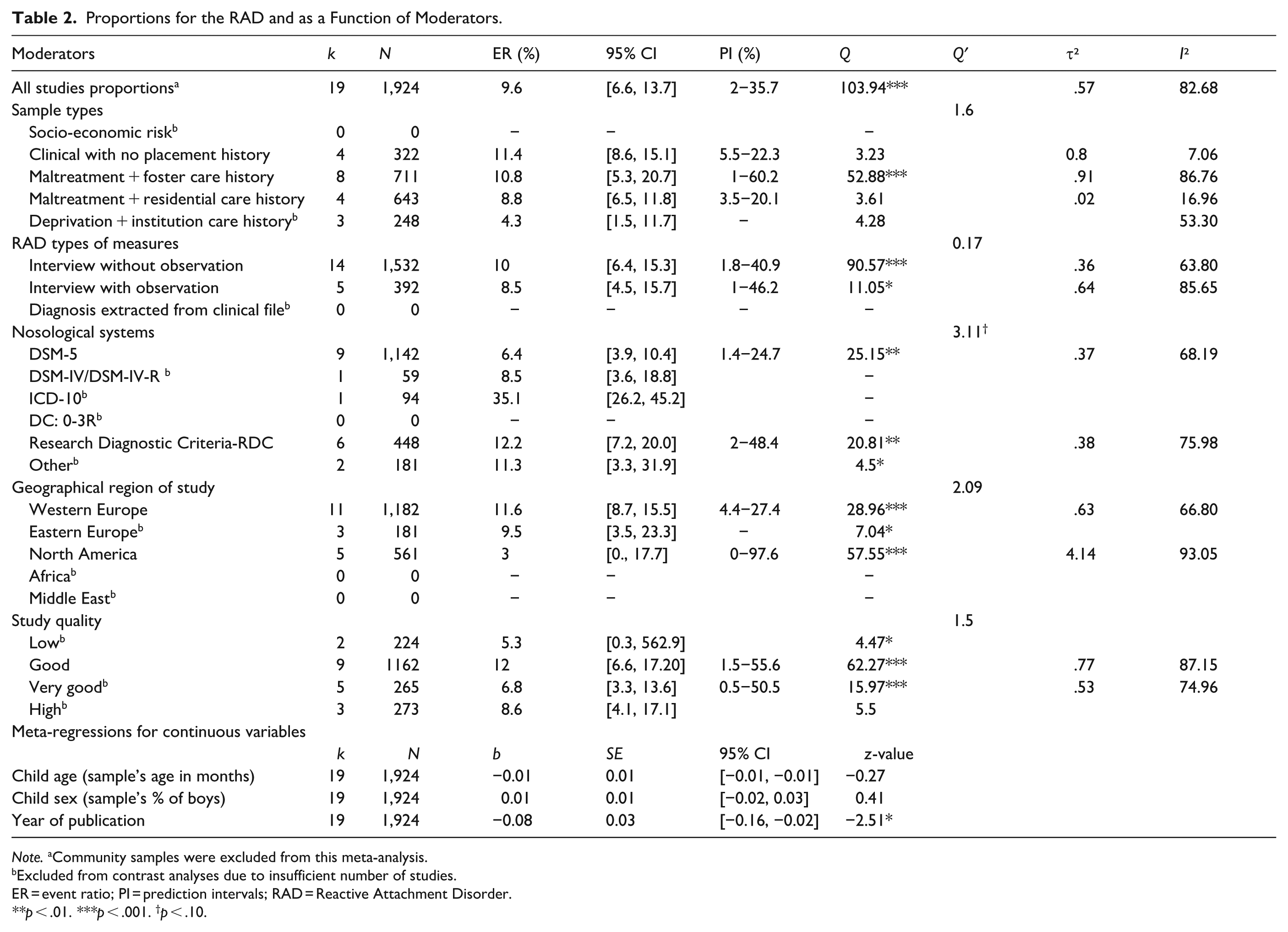
Note. aCommunity samples were excluded from this meta-analysis.
Excluded from contrast analyses due to insufficient number of studies.
ER = event ratio; PI = prediction intervals; RAD = Reactive Attachment Disorder.
p < .01. ***p < .001. †p < .10.
Proportions for the DSED and as a Function of Moderators.
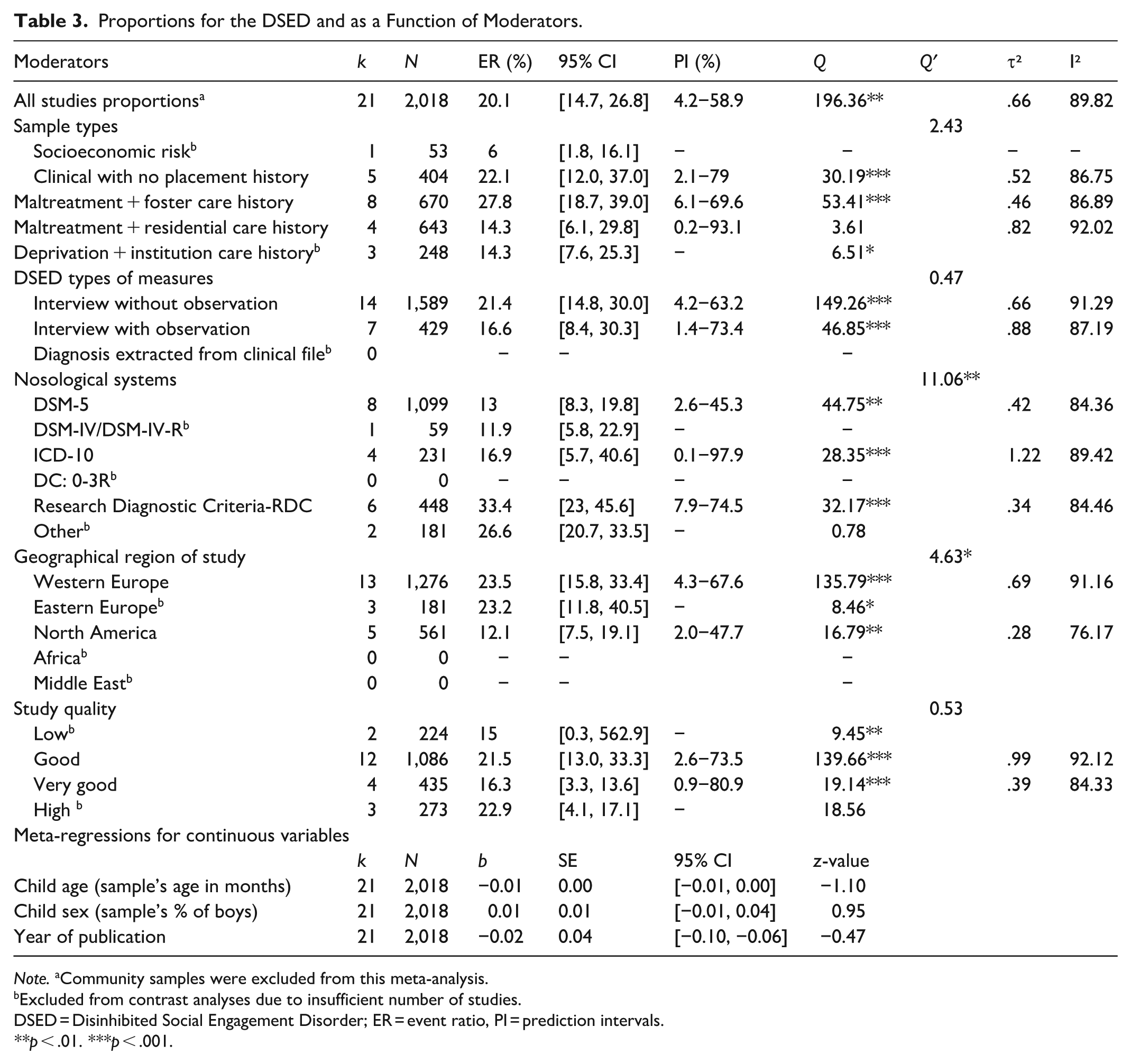
Note. aCommunity samples were excluded from this meta-analysis.
Excluded from contrast analyses due to insufficient number of studies.
DSED = Disinhibited Social Engagement Disorder; ER = event ratio, PI = prediction intervals.
p < .01. ***p < .001.
RAD-DSED Combined
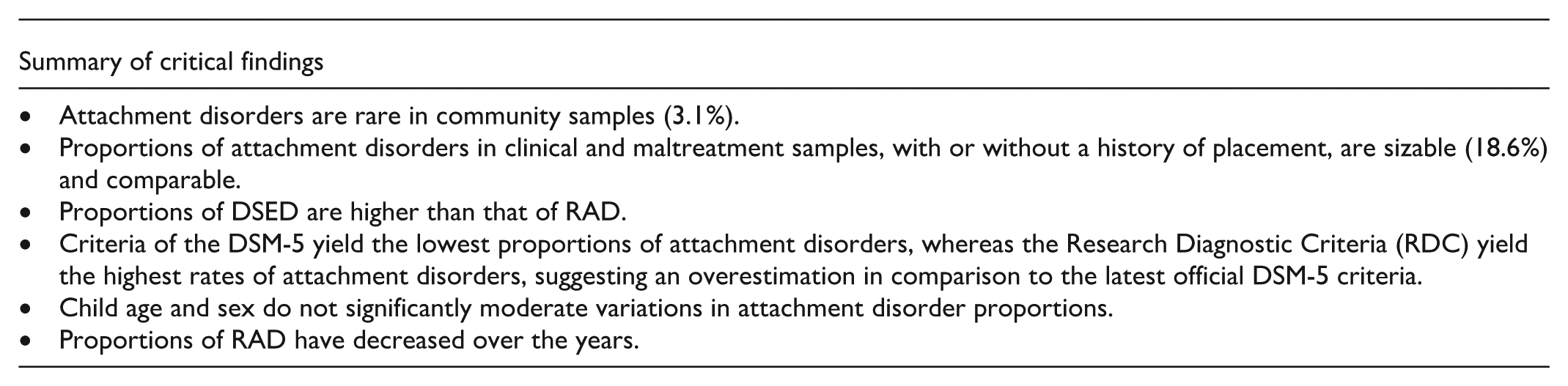
Based on all 41 independent samples (n = 8,566) with a RAD-DSED ER, the pooled estimate for the proportion of children with a RAD-DSED ER was 14.8% (95% CI [10.5, 20.4]). The significant Q statistic indicated heterogeneity across studies (Q = 899.25, p = .001). Moderator analyses revealed that study proportions varied as a function of sample type (Q’ = 30.62, p = .001). Specifically, community samples (3.1% [1.8, 5.3] within a set of homogeneous studies, Q = 7.21, p = .33) included significantly fewer children with an attachment disorder than did at-risk samples (18.6% [13.1, 25.6] within a set of heterogeneous studies, Q = 825.13, p = .001).
Given the limited number of children with an attachment disorder in the community samples, the homogeneity of this sample set, and the heterogeneity observed within at-risk studies, moderator analyses were run only on at-risk samples (k = 34). These analyses indicated that study proportions varied significantly as a function of attachment disorder measure (Q’ = 9.47, p = .009). Specifically, studies that used an interview with an observational measure (10.3%) included significantly fewer children with an attachment disorder than studies that relied only on an interview (29.7%). Also, proportions varied as a function of nosological system (Q’ = 11.60, p = .02), such that studies that relied on the RDC system yielded significantly higher proportions of children (46.7%) with an attachment disorder than studies that relied on ICD-10 (6.6%), DSM-IV/IV-TR (14.9%), or DSM-5 (16.9%) diagnostic criteria. There were no significant differences in the proportions of children across at-risk sample types (Q’ = 1.82, p = .61; 18.2% for clinical with no placement history, 20.3% for maltreatment with FC history, 28% for maltreatment with RC history, and 19% for deprivation with institution care history). Proportions did not vary significantly as a function of the geographical region of study, child age and sex, year of publication, and study quality (Q’ from 2.20 to 3.32, and b from −0.01 to 0.05).
Reactive Attachment Disorder
Based on 19 independent samples (excluding community samples; n = 1,924), the pooled estimate for the proportion of children with RAD was 9.6% (95% CI [6.6, 13.7]). The significant Q statistic indicated heterogeneity across studies (Q = 103.94, p = .001). Moderator analyses revealed that proportions were significantly lower in more recently published studies (b = −0.08, p = .01), indicating a decrease in the diagnosis of RAD over the years. Moreover, RAD proportions varied marginally as a function of nosological system (Q’ = 3.11, p = .08), as fewer children tended to be classified as RAD in studies that used the DSM-5 (6.4%), compared with those that relied on the RDC (12.2%). Study proportions of children did not vary significantly as a function of sample at-risk type, RAD measure, geographical region of study, study quality, or child age and sex (Q’ from 0.17 to 2.09, and b from −0.01 to 0.01).
Disinhibited Social Engagement Disorder
Based on 21 independent samples (excluding community samples; n = 2,018), the pooled estimate for the proportion of DSED was 20.1% (95% CI [14.7, 26.8]). The significant Q statistic indicated heterogeneity across studies (Q = 196.36, p < .001). Moderator analyses revealed that proportions varied as a function of nosological system (Q’ = 11.06, p = .004): Significantly fewer children were classified as DSED in studies that used the DSM-5 (13%), compared with studies that relied on the RDC (33.4%). Also, proportions varied according to geographical region of study (Q’ = 4.63, p = .03), with North American studies reporting significantly lower DSED proportions (12.1%) than Western European studies (23.5%). Proportions did not vary significantly as a function of sample type, DSED measure, study quality, year of publication, or child age and sex (Q from 0.47 to 2.43, and b from −0.02 to 0.01).
DSED and RAD proportions were also compared. Results revealed that DSED proportions were significantly greater than RAD proportions (Q’ = 9.34, p = .002).
Discussion
The aim of this study was to estimate the overall proportions of children diagnosed with RAD-DSED combined, RAD, or DSED. Based on data from 47 independent samples, our results indicate that the overall proportion of children with RAD-DSED combined was 14.8%. This proportion is based on studies that involved community and at-risk samples. While heterogeneity was not observed in community studies, it was relatively substantial in the set of at-risk studies for each of the three pooled estimates of RAD-DSED combined, RAD, and DSED. To more fully understand this heterogeneity, moderator analyses on at-risk studies only examined whether proportions varied by sample, methodological, and general study characteristics.
Sample Characteristics
As expected, a higher proportion of children from at-risk samples (18.6%) presented an attachment disorder (RAD-DSED combined) compared to those in community samples (3.1%), where such disorders were clearly uncommon. This aligns with findings of epidemiological studies (5/100,000 annually in Hong, Moon, et al., 2018; 0.006% in Upadhyaya et al., 2019). Lower rates in community samples are probably due to the diagnostic requirement of exposure to extreme forms of inadequate care (criterion C). Parental care deprivation, maltreatment, and out-of-home placement are considerably more common among at-risk populations.
We hypothesized that the proportions of attachment disorders would be higher in samples comprising children with deprivation, institutional care, maltreatment, placement, and mental health problems (clinical group), compared to those from socioeconomic risk. However, this comparison could not be conducted due to the limited number of studies in the socioeconomic risk group. We were able to compare other at-risk groups (with at least four studies) according to sample types (Maltreatment and FC; Maltreatment and RC, Deprivation and institutional care, and Clinical group without placement), though findings revealed no significant differences in the proportions of RAD-DSED combined, RAD, and DSED. This lack of finding suggests that these four at-risk groups share sufficiently common underlying characteristics to outweigh their differences. Adverse experiences are clearly prevalent among children who have been institutionalized, deprived of parental care or maltreated, and it is a required criterion for RAD and DSED (criterion C). In examining the composition of the clinical samples, some studies reported the presence of maltreatment or traumatic experiences among these children, which may help explain why rates of RAD and DSED, for children with mental health problems, do not differ from those with maltreatment and institutional care experiences. For example, Schlensog-Schuster et al. (2024) observed that 50% of the children and adolescents with mental health diagnoses who sought care for mental health problems had experienced maltreatment. In the study by Løkkegaard et al. (2019), 53% of the sample comprised trauma-exposed children receiving care for mental health problems. In the study by Scheper et al. (2016), 54% of home-reared children not exposed to out-of-home placement and referred for emotional or behavioral problems had a history of maltreatment. Future research is needed to more fully understand the differential impact of children’s adversity, such as the nature, severity, and timing of maltreatment experiences, on the rates of attachment disorders among those living with their biological parents versus those in out-of-home care.
Methodological Characteristics (Measures and Nosological Systems) and Publication Year
We postulated that the proportion of attachment disorders would vary according to attachment disorder types of measures, with studies relying on interviews and observational measures reporting lower rates than those not relying on observational measures. Our findings support this hypothesis, but only for RAD-DSED combined. Specifically, studies that used an interview alongside an observational measure (10.3%) and those reporting diagnoses extracted from clinical files (12.3%) reported lower proportions of RAD-DSED combined, compared to studies using only an interview without observational measures (29.7%). These findings may be explained by the fact that observation-based assessments evaluate both the child’s and the caregiver’s behavior, providing information from multiple sources rather than relying on a single source. Observational assessments also offer an independent perspective that goes beyond caregiver perceptions. Furthermore, because observation-based assessments are generally conducted by trained evaluators, such as professional clinicians, and our data indicate that diagnoses documented in clinical files (reflecting clinician assessment) were likewise associated with lower rates, our findings suggest that exclusive reliance on caregiver reports may produce higher, and potentially inflated, estimates of problematic behaviors. This reinforces the need of conducting multi-method assessments that include observation by a clinician or qualified professional. However, it should be noted that some individual studies (Archambault et al., 2024; Jonkman et al., 2014; Kliewer-Neumann et al., 2018) based on the recent DSM-5 interviews without observation have yielded low rates of RAD.
The studies reporting the highest rates of attachment disorders were mostly those using the DAI, which applies RDC criteria (Gleason, Fox et al., 2011). A possible explanation is that RDC criteria have relatively low threshold for symptom identification, meaning that symptoms are considered present on the DAI as soon as there is some evidence of a symptom (a score of 1: “some evidence”), not necessarily a definitive confirmation (a score of 2: “definitely present”; (Scheper et al., 2016, p. 547). As for RAD and DSED, their rates did not significantly vary according to the types of measures. This may be because more studies reporting RAD and DSED rates separately relied on the DSM-5 nosological system. None of the studies reporting only RAD-DSED combined used the DSM-5. Consequently, when the more restrictive DSM-5 algorithm is used, adding an observational measure may offer little incremental validity to the evaluation procedure, though this hypothesis remains to be tested.
We also hypothesized that the proportion of RAD-DSED combined, RAD, and DSED would be lower when evaluated using the DSM-5 diagnostic criteria. Due to the limited number of studies relying on some nosological systems (e.g. DC:0-3R), we were unable to compare study rates across all systems. However, comparisons were made on studies using the DSM-5, DSM-IV, RDC criteria, and ICD-10. Across all three meta-analyses, studies using RDC criteria reported significantly higher proportions of RAD-DSED combined (46.7%) than those using other systems (DSM-5: 16.9%; DSM-IV-TR: 14.9%). Studies with RDC criteria also reported higher proportions of DSED (33.4%) and RAD (12.2%, marginally significant) than studies using the DSM-5 (13% and 6.4%, respectively). These findings suggest that the RDC stands out from other nosological systems, likely due to its less restrictive criteria.
The year of publication also emerged as a significant predictor of RAD proportions. Specifically, the more recent the studies, the lower the RAD proportions reported in the studies. This result was not found for either RAD-DSED combined or DSED. The decline in RAD rates is likely due to the introduction of the more restrictive DSM-5 criteria in 2013. It may also reflect greater methodological rigor and caution among researchers and clinicians in recent years following concerns that community-based clinical assessments may have overestimated RAD proportion and that research practices have not consistently used the best evaluation methods (Allen, 2011, 2018; Allen & Schuengel, 2020).
Country of Study and Child Age and Sex
Findings of this study also show that DSED proportions varied according to the geographical region of study. This was not found for either RAD-DSED combined or RAD. The studies conducted with North American samples reported lower proportions (12.1%) than those conducted with Western European samples (23.5%). The former group of studies primarily relied on the DSM-5, whereas the latter relied on the ICD-10 or the RDC. Measurement invariance across countries and assessment methods might account for this finding. The use of DSM-5 criteria and DSM-based measures in North America contrasts with the nosological systems and measures commonly used in Western Europe, raising the possibility that the construct of DSED was not assessed equivalently across regions. Moreover, the absence of clear behavioral thresholds, combined with variations in clinical interpretation and sampling contexts, could contribute to systematic differences in reported proportions of DSED. Therefore, the observed differences in this study may reflect measurement discrepancies rather than genuine variations in proportion. Child age and sex were not significant moderators in none of the three meta-analyses. This is not surprising given that most studies did not find sex differences, and there was little age variability across studies. It may be that age and sex do not influence RAD and DSED proportions, given that these problematic behaviors seem highly influenced by proximal factors of the environment such as adverse living conditions in early childhood.
Differences in DSED and RAD Rates
Findings also reveal that, within at-risk samples, the proportion of DSED (20.1%) was significantly higher than that of RAD (9.6%). According to attachment theory, infants are expected to develop a selective attachment with a caregiver, toward whom they intentionally direct attachment behaviors to meet their needs – a developmental process considered adaptive for survival (Bowlby, 1969/1982). Under the DSM-5 (APA, 2013, 2022), children with RAD are exposed to adverse conditions that may hinder the formation of such selective attachments. These conditions (e.g., repeated placements and separations, instability in caregiving, caregiver disengagement. If children with DSED, unlike children with RAD, show little hesitation in approaching strangers, this may reflect greater exposure to relational interactions where their needs are met, even if caregiving responses are inconsistent or suboptimal. From a developmental perspective, seeking behaviors toward a caregiver can support adaptation to the environment, potentially explaining the higher likelihood of DSED behaviors compared to RAD. Children with RAD struggle both to seek and accept comfort from caregivers, which may indicate an absence of selective attachment and a reduced capacity of adaption. Moreover, from a nosological perspective, DSED requires only two symptoms (out of four), making its diagnostic criteria less restrictive than those for RAD, which require both reticence in seeking (A1) and accepting (A2) comfort from a significant caregiver, along with at least two additional criteria (B1, B2, B3). In sum, the marked difference in RAD and DSED proportions supports the conceptual distinction between these two disorders (APA, 2013; Zeanah & Gleason, 2015). However, more research is needed to better understand the high frequency of DSED in at-risk populations.
Limitations and Future Directions
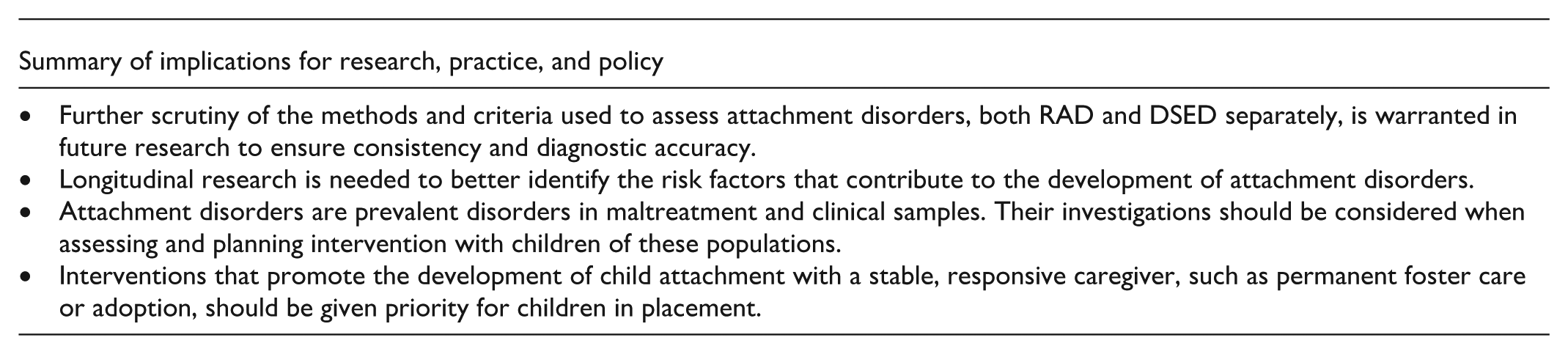
This study has limitations. First, excluding studies that relied solely on screening questionnaires helped prevent inflated pooled proportions, as such questionnaires are typically designed to prioritize sensitivity over specificity. However, this criterion may have introduced selection bias by disproportionately retaining studies with clinically recruited or clinically characterized samples. Second, although the included studies originated from 14 countries, most were conducted in North America (25%) and Europe (60%), with few or none from Africa, Asia, Australia, or South America. As a result, populations from these regions were significantly underrepresented, limiting the generalizability of the findings. Another limitation is that measurement invariance across countries was not examined in the present meta-analyses. The difference in DSED proportions between North America and Western Europe may partly reflect limited measurement equivalence. Additionally, due to study heterogeneity, future research should consider examining other important moderators, such as age at first placement, number and duration of placements, permanent adoption vs. temporary FC placement, and type of maltreatment. Given the limited information on these moderators in individual studies, we were unable to examine them in our analyses. Therefore, additional longitudinal research is needed on the risk factors associated with the development of RAD and DSED. Randomized controlled intervention studies could also offer valuable insights, as changes in RAD and DSED following interventions may reveal salient causal developmental mechanisms of RAD and DSED. Also, further scrutiny of RAD and DSED assessment methods and diagnostic criteria is warranted to ensure consistency and diagnostic accuracy in future research.
Clinical Applications
Currently, three validated tools based on DSM-5 criteria comprehensively cover all behavioral diagnostic indicators of RAD and DSED: The ETRAD-Q (Monette et al., 2022, 2024), the RAD and DSED Assessment semi-structured interview (RADA; Archambault et al., 2024; Lehmann et al., 2018), and the DAI (Smyke & Zeanah, 1999). Given current rates of RAD and DSED in maltreatment and clinical samples, these disorders should be considered in assessments and intervention planning. Moreover, although few interventions have been validated to address RAD and DSED (Zeanah et al., 2016), fostering stable attachment relationships between caregivers and children who have experienced maltreatment, out-of-home placement, and have a low likelihood of family reunification remains essential. To this end, permanent FC or adoption should be prioritized. Research shows that early placement in FC significantly increases the likelihood of forming an attachment with a caregiver (Kliewer-Neumann et al., 2023; Zimmermann et al., 2024), and establishing such a relationship is considered a key mechanism for reducing RAD symptoms (Guyon-Harris et al., 2018; Zeanah & Gleason, 2015, 2021). For children in FC who maintain contact with biological parents, one study found that such contact in cases of RAD/DSED was associated with the persistence of RAD symptoms (Zimmermann et al., 2024). Attachment-based interventions with maltreating parents can enhance parental sensitivity (Cyr et al., 2022), yet further studies are needed to test whether these interventions reduce symptoms of RAD and DSED. It also remains to be seen whether these interventions are beneficial during supervised visits with biological parents, without disrupting the attachment relationship with the foster parent or causing confusion and distress for the biological parent and child.
Conclusion
The current series of meta-analyses indicated that in community samples, RAD and DSED are rare phenomena. However, in at-risk samples, rates are prevalent, ranging from 8.8% to 11.4% for RAD and from 14.3% to 27.8% for DSED. DSED proportions were found significantly higher than that of RAD. RAD and DSED proportions, assessed separately, were not associated with type of measures, but higher rates of RAD-DSED combined were observed when assessments relied solely on interviews without observational measures. Moreover, results indicated that the DSM-5 diagnostic criteria, which are more restrictive and precise, yielded lower RAD and DSED proportions (6.4% and 13%, respectively), particularly when compared to the Research Diagnostic Criteria (RDC) measure. Official nosological systems (i.e., DSM-5, ICD-10, DC:0-3) yielded comparable RAD and DSED rates when measured separately. Harmonizing diagnostic criteria across nosological systems and encouraging both clinicians and researchers to adopt these systems and validated measures may enhance the rigor, comparability of future studies, and consistency in clinical practice. An important next step for the field is the need to standardize the conceptualization, understanding, and assessment of RAD and DSED.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261433023 – Supplemental material for Reactive Attachment Disorder and Disinhibited Social Engagement Disorder: Meta-Analyses of Proportions
Supplemental material, sj-docx-1-tva-10.1177_15248380261433023 for Reactive Attachment Disorder and Disinhibited Social Engagement Disorder: Meta-Analyses of Proportions by Maude Archambault, Sébastien Monette and Chantal Cyr in Trauma, Violence, & Abuse
Footnotes
Ethical Considerations
No ethical approval was required for this study
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A scholarship was provided to the first author from the Fonds de recherche du Québec – Société et culture (FRQSC) and the Social Sciences and Humanities Research Council of Canada. Financial support was provided to Chantal Cyr from the Canada’s Research Chair program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available upon request
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.