
Abstract
This study presents findings from three separate meta-analyses investigating differences between children placed in residential care and in family foster care with regard to three outcomes: internalizing behaviors, externalizing behaviors, and perception of care. Based on publications from the last 20 years, a total of 23 studies were included. The total sample consisted of 13,630 children in care, with 7,469 from foster care and 6,161 from residential care. The results from this study indicated that children in foster care had consistently better experiences and less problems across the three outcomes as compared to children in residential care. Analyses did not reveal evidence of publication bias, and sensitivity analyses also suggested that results were not influenced by individual studies. Additionally, moderation analyses revealed that the differences between foster and residential care could vary depending on certain factors such as the publication year, the gross domestic product of the country, and the length of care. The implications of differences in outcomes between the two placements are discussed.
A great number of children who are unable to live with their families need substitute care each year for reasons such as being abused, neglected, orphaned, or abandoned. It is estimated that 140 million children are orphans worldwide and majority of them are from countries with low Human Development Index (UNAIDS, 2004). Adverse childhood experiences such as these often result in children being taken into the custody of the state, and typically, these children are referred to as children in out-of-home care. The question of how best to provide good living environments for these children to promote positive development in different types of care remains a main concern for many state child welfare agencies.
Rich literature on child placement research has examined the effects of out-of-home care on child development. Residential and family foster care, the two most common forms of substitute care, are usually compared with each other as both conditions require children to be placed under the care of strangers. Residential care is usually referred to as a group home, institutional care, or an orphanage in which professional caregivers are entrusted to look after the daily care and welfare of these children. In contrast, family foster care encompasses parent figures in private families who are entrusted with the care of these children. A small payment to the foster family is usually provided to cover the costs of care.
Residential Care or Family Foster Care
A glance at the child placement literature does not offer a simple solution to the question of how placement decisions are made, due to a number of studies which have demonstrated contradictory results (Bates, English, & Kouidou-giles, 1997; Whetten et al., 2009). On the one hand, research has indicated that there are both short- and long-term benefits in placing children under family foster care as compared to residential care (Dregan & Gulliford, 2012; Smyke et al., 2012). On the other hand, some studies have found no differences in children’s outcomes between foster and residential care (Delfabbro, Barber James, & Betham, 2002; Whetten et al., 2009). Interestingly, in Whetten and colleagues’ subsequent study with the same sample, better physical health and emotional coping were found for children in residential care as compared to those in family foster care (Whetten et al., 2014).
Further examination of these studies suggests that these mixed findings may have arisen from several factors. Firstly, the standards of care differ in different studies, partially attributed to varying societal contexts and change in the sector across time. For example, the residential environment may be far worse in less developed countries (e.g., Romania) than in developed countries (e.g., Germany) whereby there may be better quality resources and more stimulating residential care environments. Similarly, residential care in recent years may have been equipped with better facilities and more skilled staff as compared to residential care 10 years ago. Therefore, it is highly probable that the year a study is conducted in has influence on the comparison results between the two placement types. A previous meta-analysis supported this possible moderating effect in that countries with a high Human Development Index showed smaller delays in residential Children’s IQ (van Ijzendoorn, Luijk, & Juffer, 2008).
Secondly, associations between child outcomes and placement types can vary as a function of the timing and duration of placements and their movement between the types of placement (James, Landsverk, & Slymen, 2004). The age of entry of children in care can be widely varied, and this factor may also be subsequently linked to decisions over placement type and duration. In a sample of 430 children in out-of-home care, James, Landsverk, and Slymen (2004) found that higher levels of externalizing behaviors were associated with experiencing delayed entries into stable placements, late disruptions, and multiple short stays in care. Behavior problems have been demonstrated as both a predictor and an outcome of multiple placement changes (Newton, Litrownik, & Landsverk, 2000). On the other hand, when using a matched sample, Berger, Bruch, Johnson, James, and Rubin (2009) have found that associations between out-of-home placement and child well-being did not vary by the length and stability of placements children experience.
Thirdly, the study quality may also be a contributing factor to mixed findings in the literature. Some studies were cross-sectional whereas others were longitudinal in nature. In some studies, a variety of measures were completed (and also by multiple informants), while others only utilized self-report survey tools. Lastly, some studies applied the same set of measures on both comparison groups while others applied matching techniques to obtain a comparison group from administrative data.
In the context of the above-mentioned differences across studies, a meta-analysis which synthesizes and controls for differences is highly useful for the examination of results from studies comparing foster and residential care. A meta-analysis enables the identification of patterns and disagreements from various findings and/or to discover other interesting relationships that may arise in the context of multiple studies (Greenland & O’Rourke, 2008). It allows for the testing of the consistency of effect size across a body of data. If the effect is consistent, the effect size can be estimated and be reported as robust across the different types of studies. If it varies substantially from study to study, the extent of this variance can be quantified and the dispersion of effects is studied.
Previous Reviews on Outcomes of Children in Care
A number of reviews have examined the outcomes of children in residential care and family foster care, with many focusing on specific treatment programs in residential or family foster care. These reviews generally indicated significant improvement in children’s outcomes after treatment (James, 2011; Knorth, Harder, Zandberg, & Kendrick, 2008; Osei, Gorey, & Jozefowicz, 2016; Reddy & Pfeiffer, 1997; Turner & Macdonald, 2011). For example, James (2011) examined five models of residential treatment model and found four of them promising. There have also been qualitative reviews on residential and foster treatment which did not show obvious differences between the two modalities (Bates et al., 1997; Curtis, Alexander, & Lunghofer, 2001).
Fewer review studies have compared the long-term outcomes for children who live in residential care and family foster care settings. In general, there are consistently negative views on group residential care as a place to raise young children on a long-term basis (Dozier, Zeanah, Wallin, & Shauffer, 2012). However, certain reviews have also found that family foster care has neither positive nor negative effect on children’s developmental trajectories (Goemans, van Geel, & Vedder, 2015). To the best of our knowledge, only two meta-analyses have focused specifically on the comparisons between residential care and family foster care. The first meta-analysis found that children in residential care had substantially lower levels of IQ as compared to those in foster families (van Ijzendoorn, Luijk, & Juffer, 2008). A more recent meta-analysis compared residential care with three other conditions: family foster care, treatment foster care, and no placement. The authors found that the outcomes of residential care were often worse than the other alternate forms of care (Lee, Bright, Svoboda, Fakunmoju, & Barth, 2011). However, this review only included three studies that compared between residential care and family foster care, with two studies demonstrating favorable results for family foster care.
Present Study
The aim of this present meta-analytical study was to examine the differences in outcomes between children who were placed in family foster and residential care. We hypothesized that there would be better outcomes for children in family foster care as compared to those in residential care. We also expected the effects to vary as a function of some study characteristics. Therefore, we examined a list of relevant moderators to account for the variability across studies, including (1) study quality, (2) mean age, (3) time in care, (4) gross domestic product (GDP) per capita for the country where the study was conducted, and (5) year of publication. These variables are explained in detail in the Plan of Analyses subsection.
We performed a series of meta-analyses on three outcomes: internalizing behaviors, externalizing behaviors, and perception of care. These problematic behaviors were usually used as outcome measures among the children-in-care population. Similarly, the perception of care was often used to gauge the subjective well-being of the children in care. However, no meta-analysis has been conducted on these topics among the children-in-care population so far. We thus attempted to synthesize the findings for the first time, and we expected that children in family foster care to have lower levels of problematic behaviors as well as a more positive perception toward their caregiving environment in comparison with children in residential care. The findings of the study can then be used to inform policies and practices in providing care for these disadvantaged children in order to enhance positive developments in the public care system.
Method
Inclusion Criteria
The purpose of the study was to synthesize results from publications that compared the outcomes of children in residential and family foster care in the past 20 years (January 1995 and June 2016). Studies which compared differences between these two particular types of care were included. For residential care, we referred to the care modality where children stayed in group settings with paid staff as the main caretakers (del Valle, 2013). For family foster care, children were placed in a family setting where the foster parents, who were usually not related to the children, were the main caretakers. We focused on the general children-in-care population in the child welfare system. An exclusion criterion was applied such that articles on treatment foster care, such as violence prevention foster care (Bergström & Höjman, 2016), were not included. In other words, children who were in special care or treatment centers, such as youth offenders or children with severe mental health problems, were not the target population of this meta-analysis. Besides, studies which only reported comparisons between children-in-care and the general population (Llosada-Gistau, Montserrat, & Casas, 2015; Monshouwer, Kepper, van den Eijnden, Koning, & Vollebergh, 2015; White, O’Brien, Pecora, & Buher, 2015), as opposed to comparisons between care types, were also excluded.
Among various outcomes, we examined children’s internalizing behaviors, externalizing behaviors, and perception of care. Specifically, internalizing behaviors included symptoms such as being withdrawn, somatic complaints, anxiety, and depression while externalizing behaviors included hyperactivity, delinquent, or aggressive behaviors. Children’s perceptions of care included their perceptions, attitudes, or satisfaction with their experiences in the two different types of placement. Journal articles and dissertations that were published in English and Chinese language were included in the search.
Identification of Studies
The search strategy for this study was to locate all studies comparing residential care with foster family care. First, the first author (D.L.) conducted a cross-database search using English database portals (EBSCOhost, ProQuest, PubMed, Web of Science, Cochrane library, and Google Scholar) and Chinese database portals (China National Knowledge Infrastructure [CNKI] and Airiti library, which covers China’s academic journals, doctoral dissertations, masters’ theses, and conference proceedings).
As different terms may be used to describe family foster care and residential care in various studies, we have included multiple key words for each type of care, including “foster family,” “home* care,” “foster care,” “surrogate family,” “surrogate care,” “group care,” “residential care,” “institut* care,” “congregate care,” and “orphanage.” These key words were connected using Boolean operators such as “OR” and “AND.” We also used a combination of key words such as “type of placement” or “placement type” with “substitute care,” “out-of-home care,” and “children-in-care.” Similarly, the key words used in Chinese databases include “family foster care (Ji Yang Jia Ting)” and “residential care (Fu Li Yuan)” or “orphanage (Gu Er Yuan).”
The search yielded 2,774 studies (2,563 in English and 211 in Chinese). Studies written in any other languages were included only if their English versions were available. We also identified 51 potentially relevant articles by checking through the reference lists of past review studies, and all studies that were included in this current meta-analysis. A flowchart of the literature search process is presented in Figure 1 following Preferred Reporting Items for Systematic Reviews and Meta-analysis recommendations (Moher, Liberati, Tetzlaff, & Altman, 2009). After a review of the abstracts, 152 articles were included for full-text examination, resulting in 23 studies that met the inclusion criteria.
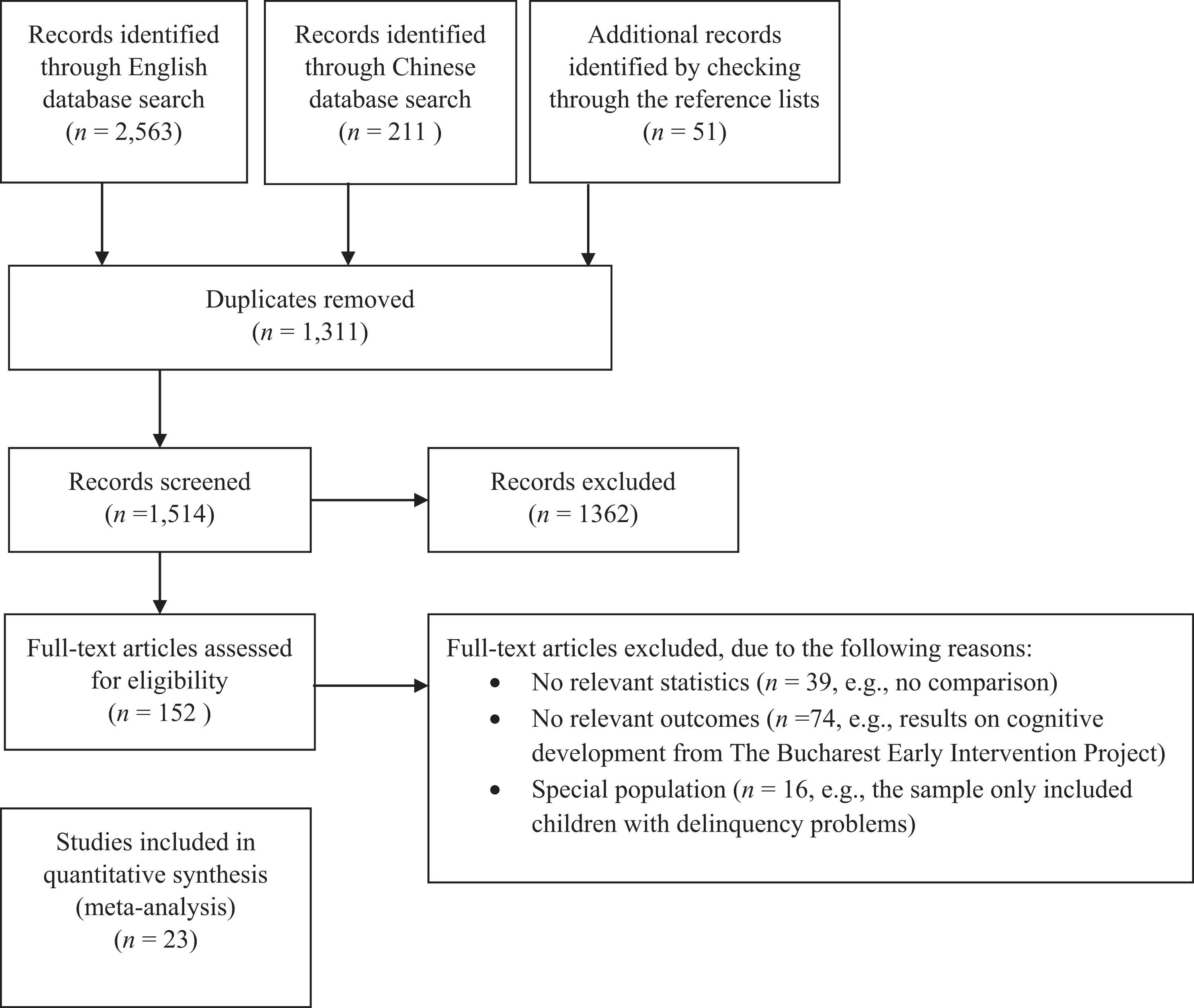
Flowchart of the literature search.
Of all articles, 13 examined both internalizing and externalizing behaviors, with 2 additional articles examining only internalizing behaviors and 5 articles only on externalizing behaviors. Five articles examined perception of care. In total, the final sample that was used in the present study consisted of 23 studies with 38 effect sizes from one doctoral dissertation and 22 journal articles published in English language. None of the articles that were published in the Chinese databases met all inclusion criteria. Table 1 presents the summaries of the study characteristics.
Characteristics of the Included Studies.
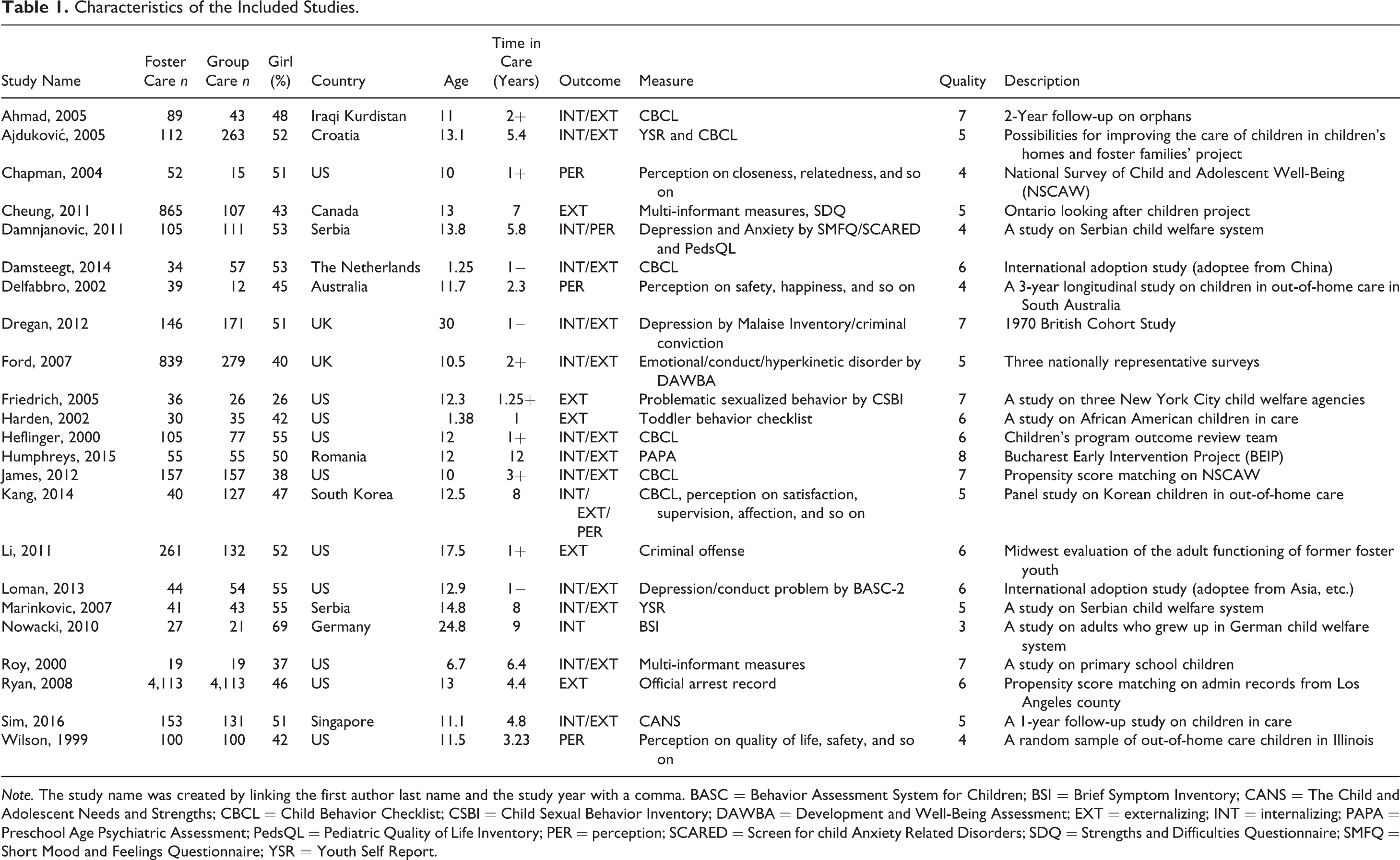
Note. The study name was created by linking the first author last name and the study year with a comma. BASC = Behavior Assessment System for Children; BSI = Brief Symptom Inventory; CANS = The Child and Adolescent Needs and Strengths; CBCL = Child Behavior Checklist; CSBI = Child Sexual Behavior Inventory; DAWBA = Development and Well-Being Assessment; EXT = externalizing; INT = internalizing; PAPA = Preschool Age Psychiatric Assessment; PedsQL = Pediatric Quality of Life Inventory; PER = perception; SCARED = Screen for child Anxiety Related Disorders; SDQ = Strengths and Difficulties Questionnaire; SMFQ = Short Mood and Feelings Questionnaire; YSR = Youth Self Report.
Data Coding
Data coding was conducted for three separate meta-analyses to examine the impact of placement in residential care and family foster care on (1) internalizing problem behaviors, (2) externalizing problem behaviors, and (3) perceptions of care. Each study was coded at three levels: (a) article, (b) sample, and (c) effect size. At article and sample level, we coded for the five variables necessary for moderator analyses (please refer to Plan of Analyses subsection).
For effect size-level coding, Hedges’s g was used as the effect size measure, which is a variation of Cohen’s d that corrects for biases due to small sample sizes (Hedges & Olkin, 1985). When different instruments were used to assess the same construct in one study (or different informants assessed the same construct), a mean effect size was computed for the construct and this mean effect size was used in the final analysis.
When a study reported a relationship without any statistics, we estimated a conservative effect size based on sample size and an arbitrary p value (we used p = 1 if the relationship was nonsignificant and p = .05 if the relationship was significant). If a p value was reported as less than a certain value, we used that value as a conservative estimate. The coding was done independently by two of the authors. All differences were discussed until consensus was reached. With regard to interrater reliability, the two authors achieved 93% identical coding before discussion.
Plan of Analyses
To answer the research questions, three separate meta-analyses were conducted. Random effects models were tested as heterogeneity was assumed due to substantial variations among studies (e.g., cultural differences and age differences). The following covariates were included in the meta-regression analysis: (1) study quality—the overall quality of each study is coded based on the Newcastle-Ottawa Quality Assessment Scale (NOS). NOS is a quality assessment tool for observational studies including case–control and cohort studies. Based on NOS, each study can be assessed in three broad domains: the selection of the study groups (e.g., the representativeness of the exposed cohort), the comparability of the groups (e.g., whether the study controls for any important confounding factor), and the ascertainment of either the exposure or outcome of interest (e.g., whether the assessment of outcome is through independent blind assessment). A score of 5 stars or more out of 9 is considered a good quality study; (2) age—the mean age of the study sample at the time of the outcome assessment; (3) gender—the percentage of girls in the sample; (4) time in care—the average number of years that children had stayed in public care, including both the family foster care and residential care. An arbitrary value of 5 years was used to describe long-term outcomes (5 years or more as compared to less than 5 years); (5) GDP—the GDP per capita (scaled down by 10,000) of the country where the study was conducted. It was assumed that the care quality in higher GDP countries would be better than that in lower GDP countries; (6) year—the year of publication was used as an estimate of the study order, specifically the period when the children stayed in care. It was assumed that the care quality in recent years would be better than that in earlier years. In a few studies, the publication year was more than a decade away from when the children were in care because the outcome data were collected on adults who were formerly under public care. In such cases, the publication year was not a good estimate of the chronological order of the studies; they were thus removed from the meta-regression on publication year as part of the sensitivity analysis.
Due to the small number of studies included, only one of the covariates was tested at each time. Meta-regression was only conducted when the total number of studies included for the particular outcome was larger than six. The Q (the significance test for observed dispersion), I 2 (the ratio of excess dispersion to total dispersion), and τ (the estimated standard deviation of the true effect) were reported as indicators of heterogeneity (Borenstein, Hedges, Higgins, & Rothstein, 2009). Publication bias was tested for all significant relationships by checking the funnel plot. The studies will be distributed symmetrically in the funnel plot around the mean effect size if there is no evidence of publication bias. We also examined the Egger’s regression intercept, which was the statistical test for asymmetry of the funnel plot, to assess the threat of possible bias in the sampling for publications (Orwin, 1983).
For sensitivity analysis, the jack knife method was used to assess the impact of the inclusion of transformed and estimated effect sizes using arbitrary p values as well as studies with extreme effect sizes. Through this procedure, one study was removed each time to determine whether the overall effect size is biased by the influence of any one study (Borenstein et al., 2009). Cohen’s (1992) guidelines for interpreting mean effect sizes were employed, whereby Hedges’s g of at least .10, .30, and .50 were considered as small, moderate, and large, respectively. All data analyses were conducted using Comprehensive Meta-Analysis Version 3.
Results
Internalizing Behaviors
The first meta-analysis included 15 studies with a total of 3,574 children in care. As shown in Figure 2, children from residential care (n = 1,608) reported higher levels of internalizing behaviors, with a Hedges’s g of −.30 (95% confidence interval (CI) [−.41, −.20]), p < .001. There was no evidence of substantial heterogeneity (Q = 20.42, p = .12, I 2 = 31.44%, τ = .11). An examination of the funnel plot showed symmetrical distribution of studies. Egger’s regression intercept was 1.02 (p = .96, two-tailed), indicating no evidence of publication bias. A sensitivity analysis showed that the result was not influenced by any individual study.
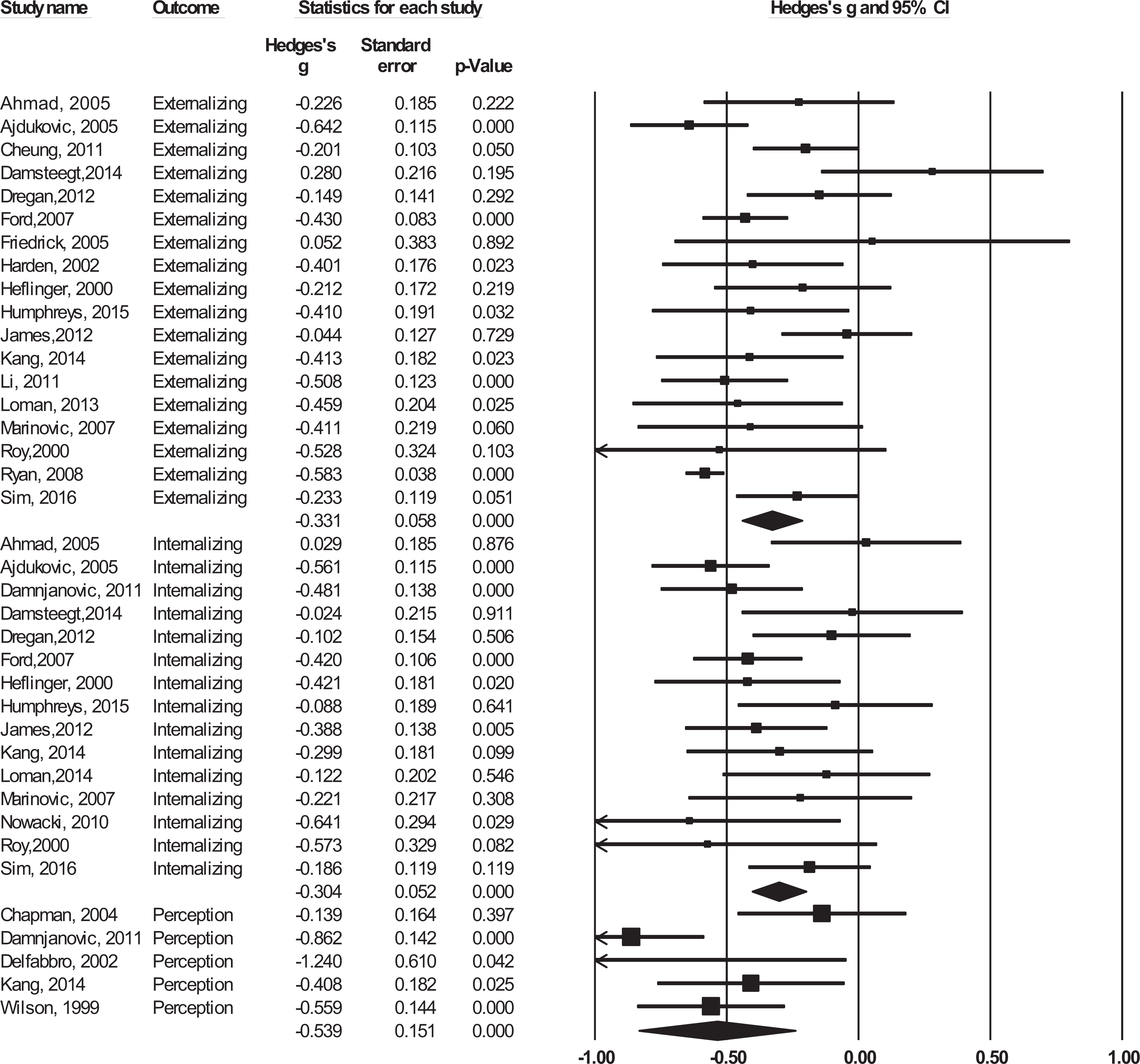
Forest plots by study names and outcomes.
The results of the meta-regression analyses are presented in Table 2. The difference in internalizing behaviors between family foster care and residential care was found to not be significantly influenced by the age of the sample, percentage of girls in the sample, and GDP per capita of the country where the study was conducted. There was a significant moderating effect for publication year and study quality, in that studies in recent years and with higher quality ratings reported smaller differences between residential and family foster care. A sensitivity analysis on publication year showed no changes to the meta-regression result, by removing the studies using adult participants (Dregan & Gulliford, 2012; Li, 2011; Nowacki & Schoelmerich, 2010, where the children were placed in care as early as in 1970s). There was also a significant effect with time in care: Studies where children stayed for more than 5 years on average have a larger pooled effect size as compared to studies where children stayed less than 5 years.
Meta-Regression on Internalizing Behaviors.
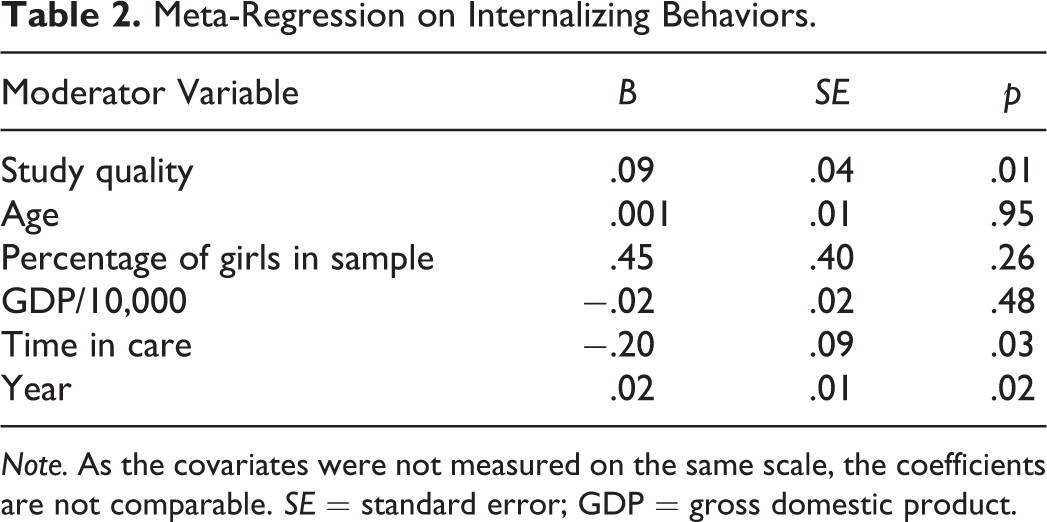
Note. As the covariates were not measured on the same scale, the coefficients are not comparable. SE = standard error; GDP = gross domestic product.
Externalizing Behaviors
The meta-analysis on externalizing behaviors included 18 studies with a total of 13,048 children in care. As shown in Figure 2, children from residential care (n = 5,902) reported higher levels of externalizing behaviors than family foster care children (n = 7,146), with a Hedges’s g of −.33 (95% CI [−.44, −.22]), p < .001, and substantial heterogeneity (Q = 55.74, p < .01, I 2 = 69.50%, τ = .19). A sensitivity analysis showed that the result was not significantly influenced by any individual study.
The distribution of studies is asymmetrical in the funnel plot, and the Egger’s regression intercept was 1.98 (p < .01, two-tailed). A detailed examination of the funnel plot showed that the asymmetry was not due to small study effect. Instead, there were more small-scale studies with trivial results. Using a trim and fill method with nine additional studies, the adjusted effect size would be a higher Hedges’s g of −.55 (95% CI [−.65, −.41]). A sensitivity analysis was conducted by separating studies that appeared to be outliers in terms of the outcomes or moderators. Out of the 18 studies, 2 used a specific outcome (conviction or arrest) rather than a more generalized externalizing behavior (Dregan & Gulliford, 2012; Ryan, Marshall, Herz, & Hernandez, 2008). Another three studies used young children (such as 1-year-old) as study samples (Damsteegt, van IJzendoorn, Out, & Bakermans-Kranenburg, 2014; Harden, 2002; Roy, Rutter, & Pickles, 2000) while majority of the other studies used adolescent samples. After removing the five studies, the funnel plot became symmetrical with a nonsignificant Egger’s intercept of .67. The pooled effect size is still significant for the remaining 13 studies, with a Hedges’s g of −.34 (95% CI [−.45, −.24]), p < .001, and reduced heterogeneity (Q = 20.65, p = .06, I 2 = 41.88%, τ = .12).
Meta-regression results using the 13 studies are presented in Table 3. The results showed that the difference in externalizing behaviors between family foster care and residential care was not significantly influenced by the quality of the study, year of publication, and time in care. A sensitivity analysis on publication year showed no changes to the meta-regression result, by removing the studies using adult participants (Dregan & Gulliford, 2012; Li, 2011). The moderating effect for GDP was significant, indicating that studies conducted in high GDP countries had a smaller pooled effect size. In fact, the Hedges’s g was only −.27 (95% CI [−.41, −.14]) among the countries with high GDP as compared to −.48 (95% CI [−.61, −.34]) among countries with relatively lower GDP based on median split. There was also a significant moderating effect for age and percentage of girls in the sample, in that studies with older participants and studies with more girls had larger pooled effect sizes.
Meta-Regression on Externalizing Behaviors.
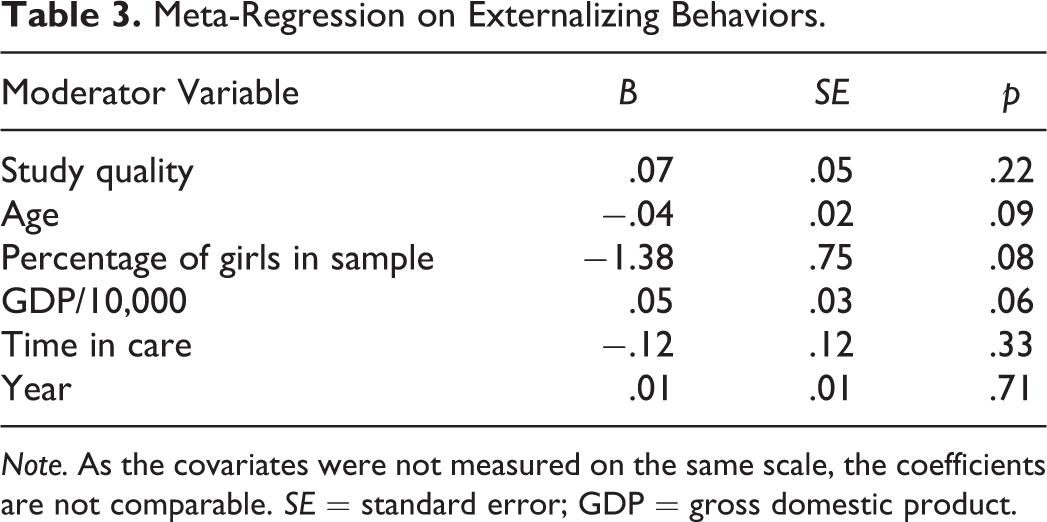
Note. As the covariates were not measured on the same scale, the coefficients are not comparable. SE = standard error; GDP = gross domestic product.
Perception of Care
The third meta-analysis was on five studies examining the children’s perception of care. It included 848 children, with 450 from family foster care and 398 from residential care. Similarly, it was shown that children from family foster care had more positive perceptions about care, Hedges’s g = −.54 (95% CI [−.84, −.24]), p < .001, with considerable heterogeneity (Q = 13.00, p = .01, I 2 = 69.22%).
An examination of the funnel plot showed symmetrical distribution of studies. Egger’s regression intercept was −.67 (p = .82, two-tailed), indicating no evidence of publication bias. A sensitivity analysis showed that the result was not influenced by any of the studies. No moderating analyses were conducted due to the small number of studies included.
Discussion
Overview of Key Findings
This study examined differences between family foster care and residential care in terms of children’s perceptions and outcomes. Three separate meta-analyses were conducted using a total of 23 studies involving 13,630 children in care, with 7,469 from family foster care and 6,161 from residential care. The results indicated that children in family foster care had consistently better experiences and fewer problems across the three outcome indicators (i.e., perceptions of care, internalizing, and externalizing problems) as compared to children in residential care. The analyses revealed no evidence of publication bias, indicating that the result is not biased toward small studies with larger effect sizes.
Internalizing and externalizing behaviors
Compared to studies on internalizing behaviors, the studies on externalizing behaviors had more heterogeneity. Moderating factors were found to differ between the two types of problematic behaviors. For internalizing behaviors, studies in more recent years with higher quality ratings and with children who had shorter length of time in care reported smaller differences between residential and family foster care. For externalizing behaviors, the results showed that studies conducted in higher GDP countries with younger participants and more boys had smaller pooled effect size. In other words, the gap in internalizing behaviors between foster and residential care became larger when children stayed in care for a longer period of time. In contrast, the effect on externalizing behaviors is more influenced by age and gender of the sample rather than time in care. The result is consistent with gender and developmental studies in that males usually have higher levels of externalizing behaviors, and such behaviors may continue from childhood and peak at adolescence with some acute symptoms such as offending (Bongers, Koot, Van Der Ende, & Verhulst, 2004; Broidy et al., 2003; Moffitt, 1993).
With regard to the contributing factors of the year of publication and the GDP of the country, the differences between foster and residential care were smaller for more recent studies on internalizing behavior and for those conducted in more developed countries on externalizing behavior. An explanation may lie in the recent development and implementation of changes toward improving the quality of out-of-home care in some countries. For example, it was found that in recent years that residential care in both Germany and the Netherlands has been more focused toward the development and funding of small-scale group homes with increasing professionalization of staff (Hardera, Zeller, López, Köngeter, & Knorth, 2013).
Additionally, it may be inferred from published statistic reports that developed countries with higher GDP have a more fine-grained understanding of the characteristics of their out-of-home care population: Statistics on out-of-home care in Australia, United Kingdom, and United States are more detailed, thematically organized, and publicly accessible as compared to less developed countries. This may enable them to be more targeted in their reforms for the out-of-home care sector. A better quality of care may mitigate some of the negative effects that could arise due to care type, hence reducing the differences between residential and family foster care. Another explanation for these differences may lie in that the rationale for placement type is different across time and countries. For example, it was found that more children aged 3 years and below were placed into residential care in countries with lower GDP, who then subsequently developed more serious attachment and behavioral problems (Browne, 2005).
Perceptions of care
The analysis on children’s perceptions about care showed that children in family foster care had more favorable perceptions about their placement, with a large effect size being observed. In other words, children in foster families reported higher levels of satisfaction with care settings and caregivers, higher levels of feelings of safety, and so forth (Delfabbro et al., 2002). Children’s opinions toward care are important as it may be related to their development and well-being. Increased feelings of safety have been postulated to allow children to focus more on school tasks and thus lead to increased scores on academic outcomes (Ratner et al., 2006). Similarly, children who were more satisfied with their placement were reported to display fewer problematic behaviors (Cheung, Goodman, Leckie, & Jenkins, 2011). However, children in care usually have no say in the decision-making process with regard to their placement (Unrau, 2007). In particular, the rationale for placement is usually based on adult assessment of children’s risk factors and needs, and these reasons may not be adequately explained to the children (Khoo, Skoog, & Dalin, 2012; Scholte, 1998). Therefore, efforts should be made in the child welfare system to include the voices of children in order to enable appropriate placements and support in order to improve their quality of life (Fox & Berrick, 2007).
Comparisons With Previous Reviews
To the best of our knowledge, no previous meta-analysis has compared children with long-term placement in foster and residential care. A similar analysis was found in a recent review by Lee, Bright, Svoboda, Fakunmoju, and Barth (2011), who compared residential care with family foster care and treatment foster care and concluded that outcomes of residential (group) care were generally worse than family foster care. However, the analysis on family foster care in Lee’s review was made up of only three studies with varying stay length and treatment.
Generalizability of Conclusions
The studies included in this review covered a great variation of children with regard to age, country, and time in care. However, majority of these studies examined children’s outcomes of both genders in their adolescence and the majority of these children stayed in care for more than 1 year. More than half of the studies were conducted in Western countries such as United States and United Kingdom. For problematic behaviors, majority of the studies used the Child Behavior Checklist (CBCL) or the Youth Self Report (YSR) as the outcome measure. In studies not using CBCL/YSR, the outcome measure for internalizing behavior is usually an established scale of depression or anxiety. Sensitivity analysis on the outcome measure showed that results did not differ significantly. In contrast, the measurement of externalizing behaviors varied greatly for some of the studies, such as the use of criminal convictions in two studies. Further analysis showed that studies that utilized a very young sample or criminal convictions as the outcome measure for externalizing behavior appeared to be outliers as compared to other studies. Therefore, the findings on problematic behaviors can be considered generalizable to studies with adolescent children in care where outcomes are measured on a general internalizing/externalizing framework. More evidence is needed to support the usage of outcomes for young children and administrative official data (e.g., criminal convictions) as proxies for externalizing outcomes.
As for perception of care, although the results of the analysis on perception were based on five studies, four of these studies used a representative sample of teenage children. The sensitivity analysis also revealed a stable estimated effect size even with the removal of any one study from the analysis. To some extent, the pooled finding is representative of adolescent children’s perceptions of residential care and family foster care.
Potential Bias and Limitations
The major limitation of this meta-analysis lies in the methodological differences between included studies. Specifically, the placement of children into different types of care was not random. Based on past studies, children in residential care usually entered the system at an older age and with higher psychological and behavioral needs. Therefore, meta-analysis conducted using studies with a convenient or representative sample may mistakenly reinforce differences in children’s profiles in care, although these differences may have existed from entry into care and are not resultant from care. Similarly, the included studies usually did not differentiate children who were admitted primarily for treatment and those admitted primarily for care. Although we excluded studies on treatment efficacies to focus solely on the comparisons between different types of care, it is unclear to what extent treatments were still provided to these children in different settings. At present, the diverse methodologies contribute to great difficulties in comparing the results across studies—this situation needs to be improved and more clarity is needed in terms of the criteria and efficacy of placement modes in order to help policy makers and practitioners to make better decisions.
The second concern with regard to drawing conclusions concerning residential care is the lack of data on the differences between types of residential care. Some studies distinguished between group home and institutions, where the latter referred to institutes with more than 20 beds (Vogel, 1999). Some studies compared different types of group homes, where in certain SOS Children’s Villages, they lived in group homes together with caregivers in a family-like setting (Ajduković & Franz, 2005). Originally, there were plans to code the size of residential care (e.g., number of beds), but majority of the studies did not report such information. This information could contribute to within-subject variations and thus should be reported in future studies.
Another limitation lies in the fact that the moderators (publication year and GDP) that were used to infer the quality of care were measured with some imprecision. For example, there is always a lapse of time between data collection and publication, and the length may vary among studies. Similarly, the quality of care may differ between cities or between urban and rural areas within the same country. Using a country’s GDP to estimate the quality of care was thus also a source of potential bias. Nevertheless, the present meta-analyses results showed a promising effect of professionalization of care. Future studies should report the quality of care on a standardized format, so that a more accurate measure can be used in the synthesis and comparison of results.
Implications and Conclusion
Taken together, the findings in this study suggest that it might be beneficial to invest in the development of family foster care services, despite the reduction of supposed advantages of family foster care over residential care pertaining to outcomes that were likely to have been brought about with improvements in care conditions, the rising affluence of various societies, as well as more advanced research methods. The results demonstrate considerable robust effects of poorer behavioral and psychosocial outcomes for children placed in residential homes as compared to those in family foster care. These results imply that family foster care offers better caring environment, possibly due to the provision of more individualized, stable, and responsive caregiving and the provision of a safer, more home-like environment as compared to residential homes.
Furthermore, preliminary research on the interaction effects between resilience and placement type indicated that family foster care might facilitate much better outcomes for children with resilience as compared with residential care (Sim, Li, & Chu, 2016)—such results provide food for thought about the social capital that we invest in our children in care and whether placement options can augment these. Hence, policy efforts should be made to promote the placement of children removed from families into family foster care as compared to placing them in residential homes. More resources should also be allocated to increase the pool of foster caregivers and to provide the necessary support and training.
However, not all children, because of their experiences, may be able to cope with close relationships in a substitute family, and there has to be a consideration of particular circumstances of institutions and social structures in different communities (see Nowacki & Schoelmerich, 2010); hence, it would be prudent to continually have some residential care facilities that are made available for children who are in severe, acute distress and those who are not coping well in family foster care for various reasons. It is worthy to note that in the current study, the gap between outcomes in residential and family foster care was reduced in studies published in more recent time and by the GDP of the country. This finding may indicate that there is space for the substantial improvement of the quality of care and environment offered in residential homes. More research has to be done to identify which aspects of residential care carry the benefits and which carry the risks. Some suggestions from past studies have indicated that smaller child-to-caregiver ratios and increased training and professionalization of caregiving staff will be helpful directions to pursue. The physical living conditions such as the provision of facilities and the structural building layouts of residential homes should also be looked into to provide a feeling of safety and warmth for the child. In addition to training and upgrading, adequate resources have to be allocated for the proper monitoring of these care institutions in order to ensure optimal functioning.
Furthermore, more integrated and professionalized assessment at the point of entry into the out-of-home care system is needed, including the need to take into account the opinion of the child. The provision of an age-appropriate explanation for the child to understand the placement decision can be considered, so as to facilitate better adjustment of the child to the new environment.
Negative effects of childhood maltreatment can be enduring and these effects may be cumulative in leading to greater inequality in later years of life. The current meta-analytic study shows that care placement types do play a role in mitigating some negative consequences of childhood maltreatment, although the extent of this mitigation on other outcomes not included in this study remains to be determined.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.