
Abstract
The aim of this qualitative systematic review was to synthesise best evidence exploring the experiences of identifying and responding to domestic abuse (DA) in the older population from the perspectives of older people and of practitioners. Whilst awareness of DA in the older population is growing, there is still limited awareness and understanding of these experiences. Fifteen databases were searched for studies that included older victims-survivors (aged 60+) and/or practitioners’ experiences of DA with a total of 29 articles selected which met the inclusion criteria. The Critical Appraisal Skills Programme Qualitative Studies Checklist was used to undertake a critical appraisal, and included studies were analysed using thematic synthesis. The studies provide a wide-ranging overview of this phenomenon highlighting unique characteristics of DA in the older population. Key findings included that the identification of abuse in the older population as DA is problematic, as is the nature of agency and organisational responses, such as availability of suitable resources. The findings highlight a range of interconnecting complexities which influence help-seeking and professional responses to DA in the older population, including systemic failures, institutional biases and deeply embedded ageist assumptions which affect older victims-survivors. It is also evident that there is a lack of research which explores this area from an intersectional perspective including, for example, consideration of age alongside gender, disability, ethnicity and sexuality. Several recommendations are suggested to enhance intervention in this area, including the need for policy and practice reform, as well as additional research.
Keywords
Introduction
Domestic abuse (DA) is a well-researched topic, with understanding of the extent and nature of this issue rapidly developing over the last several decades. This includes the definition of DA which has evolved over time to provide greater clarity about its nature and characteristics. The World Health Organization (WHO, 2021) refers to ‘intimate partner violence’ as ‘behaviour by an intimate partner or ex-partner that causes physical, sexual or psychological harm, including physical aggression, sexual coercion, psychological abuse and controlling behaviours’. In the United Kingdom, the definition of DA has been broadened under The Domestic Abuse Act (2021). It states a person’s behaviour is defined as DA if both parties are aged over 16, are personally connected and the behaviour is abusive (which includes violent, threatening, coercive or controlling behaviour, economic, psychological, emotional, physical, sexual or other abuse). This definition broadens perpetrators beyond intimate partners, allowing for the inclusion of DA by other family members which is crucial for older people facing abuse from other relatives (Wydall & Zerk, 2017). We therefore use the UK definition within this systematic review.
Whilst our understanding of DA has developed, research which specifically addresses the experiences and needs of older victims-survivors 1 is more limited leading to a lack of understanding about their experiences and support needs (Bows et al., 2023; Lonbay & Southall, 2024; McGarry & Simpson, 2011). However, it is becoming increasingly well known that the prevalence of DA in the older population is high, underscoring the need for more attention to be paid to this population and their experiences. In 2023, the Office for National Statistics (ONS) in the United Kingdom reported that 3.2% of people between age 60 and 74, and 1.4% over age 75 were subject to DA amounting to an estimated 375,000 cases in a year with concern expressed that this was likely the tip of the iceberg (Bower, 2023). In 2024 these percentages rose to 4% and 2%, respectively (ONS, 2024). Prevalence among older people with dementia may be higher; 11% and 19% for physical and psychological abuse, respectively, with a higher prevalence in relationships with a history of DA (McCausland et al., 2016). Global estimates are harder to ascertain as many studies have considered elder abuse more broadly, to include ‘any relationship where there is an expectation of trust’ (WHO, 2024b) though the WHO estimates that 1 in 6 older people (60+) experience abuse (WHO, 2024b). Previous research has highlighted the physical and mental health impact for victims-survivors of DA, and this is likely to be exacerbated for older people (Knight & Hester, 2016; McGarry & Simpson, 2011). This systematic review is therefore an important contribution to the literature, providing a synthesis of existing research findings with the aim of contributing to our understanding of how best to recognise and respond to DA in the older population. It explores the experiences of older people and practitioners in recognising and responding to DA.
DA in the Older Population
The recognition of DA as a global issue has increased significantly over recent years. This is evident through a range of international research and collection of data across numerous countries which attempts to establish the prevalence and nature of DA (Age UK 2022; García-Moreno et al., 2013; Luoma et al., 2011; ONS, 2024; Stöckl et al., 2012; WHO, 2021). Older people subjected to DA can be a hidden group due to assumptions that it only impacts on younger people (Age UK, 2019, 2020; Henderson et al., 2020) and a historical focus on intimate partner violence (IPV) which excludes the wider range of family members who may perpetrate DA against older people (such as children and grandchildren). This inequity is reflected in data collection, for example, it is only since 2021 that the Crime Survey for England and Wales removed an upper age limit of 75, which had contributed to an invisible status for older victims-survivors and consequent lack of understanding of their specific risks and needs (McGarry & Simpson, 2011; Mohammed, 2018; Straka & Montminy, 2006; Wydall & Zerk, 2017). The WHO (2024a) identified two key problems with existing data (including both research and national data surveys). The first was consistency of age with a range of ages used across studies and jurisdictions to identify ‘older’ people. The second was the lack of age-specific questions within data that related specifically to older women. Benbow et al. (2018) also noted the different ways data is collected and the problematic use of multiple, often overlapping, terms that vary in their meaning. It is suggested a ‘lack of conceptual clarity’ in the distinction between domestic violence/abuse and elder abuse can also create confusion (McGarry et al., 2014, p. 204; Lonbay & Southall, 2024) resulting in the failure of professionals to recognise DA situations with older people and the more general label of elder abuse being applied. Overall, practitioners’ assumptions about abuse and the way they categorise it also impact on prevalence data, and this has contributed to the limited attention paid to DA in the older population in policy and practice (Scott et al., 2004; Wydall & Zerk, 2017). A lack of recognition by practitioners of the gendered forms of violence that impact on women in later life has also been noted, alongside an associated lack of response to this within policy and practice (McGarry et al., 2014; Nägele et al., 2010; Lonbay & Southall, 2024). This is particularly significant as it may lead to older victims-survivor’s needs and necessary interventions being overlooked (Lonbay & Southall, 2024; Wydall & Zerk, 2017).
There is a developing body of research and literature into how older women and other vulnerable groups are at risk from gendered forms of violence, and many researchers have focused on the multiple factors that can contribute to an older woman’s vulnerability to DA (Choi et al., 2017; Sasserville et al., 2022). Economic inequalities, barriers to accessing health and mental health services and traditional gender roles create multiple disadvantages for older women making them more vulnerable to violence from their male counterparts (Allcock, 2018). In addition, it is suggested that professional understanding of DA in the older population is limited (Carthy & Taylor, 2018; Lonbay & Southall, 2024) with little understanding about the perspectives of victims-survivors, particularly those who are not older White, heterosexual women. Connected to this is a lack of understanding of help-seeking (defined as abuse disclosure to obtain support) by older victims-survivors (Lelaurain et al., 2017). Help-seeking behaviour has been widely explored across several fields, including DA, and it is suggested that victims-survivors progress through several stages, each of which is influenced by a range of personal, interpersonal and socio-cultural factors (Liang et al., 2005). The stages, though not required to be linear, are ‘problem recognition and definition, the decision to seek help, and the selection of a help provider’ (Liang et al., 2005). Given the concurrent lack of knowledge regarding how disclosure might be responded to by professionals, the aim of this review was to synthesise the best available evidence exploring the experiences of identifying and responding to DA in the older population from the perspectives of older people and of practitioners. The review therefore aimed to uncover older people’s accounts of DA and help-seeking as well as practitioners’ experiences of identifying and responding to DA in later life. Our review questions were:
What is the experience of older people in accessing and receiving support for DA?
What is the experience of practitioners when they identify and respond to DA in the older population?
As such we hope to better understand what appropriate intervention(s) might be for this population group and to identify barriers and facilitators for disclosing and responding to abuse.
Methodology
Search Strategy
Fifteen databases were searched including: MEDLINE (OVID), PsycINFO (OVID), CINAHL (EBSCO), Scopus, Applied Social Science Index and Abstract, ProQuest, Community Care Inform Adults, Social Care Online, SOC Index, Science Direct, Health Research Premium Collection, Social Policy and Practice, Web of Science, Google Scholar and Cochrane Library. A further search was performed concurrently identifying grey literature (utilising Google and known websites and authors). Database searches were also supplemented by cross referencing the included studies and searching reference lists of relevant articles. These three methods yielded the final articles included. The Sample, Phenomenon of Interest, Design, Evaluation, Research type tool was used to guide the development of our search strategy. The search terms used included older people, DA and experience; domestic violence and experience; elder, domestic violence, interpersonal violence and practitioner. An excel workbook was utilised to keep a record of the search results from the 15 databases and specified searches. The search was first conducted in November 2022 and updated in November 2024 to identify any additional articles that were published in the interim period. While originally developed for quantitative reviews, PRISMA 2020 reporting guidelines were adapted to ensure transparent and structured reporting of this qualitative systematic review, particularly in documenting the search, screening and selection process through a structured search strategy and flow diagram (Page et al., 2021).
Eligibility Criteria
A three-stage process was used to identify articles which met the eligibility criteria (Table 1). In stage one, 371 articles and 44 reports were screened using an abstract screening tool to identify qualitative or mixed method articles published in English within the included date range and which reported on DA from the perspective of older people and/or practitioners. Thresholds for inclusion were kept broad at this point to ensure relevant articles would not be removed. This resulted in 312 records being excluded. Following this, full texts were retrieved resulting in 36 articles and 4 reports being reviewed in stage 2, where a full text screening was undertaken by two reviewers, using the eligibility criteria (Table 1). Nine articles were removed that did not meet the eligibility criteria, for example, studies about DA and older people were excluded where the sample included victims-survivors under age 60.
Inclusion and Exclusion Criteria for Article Selection.
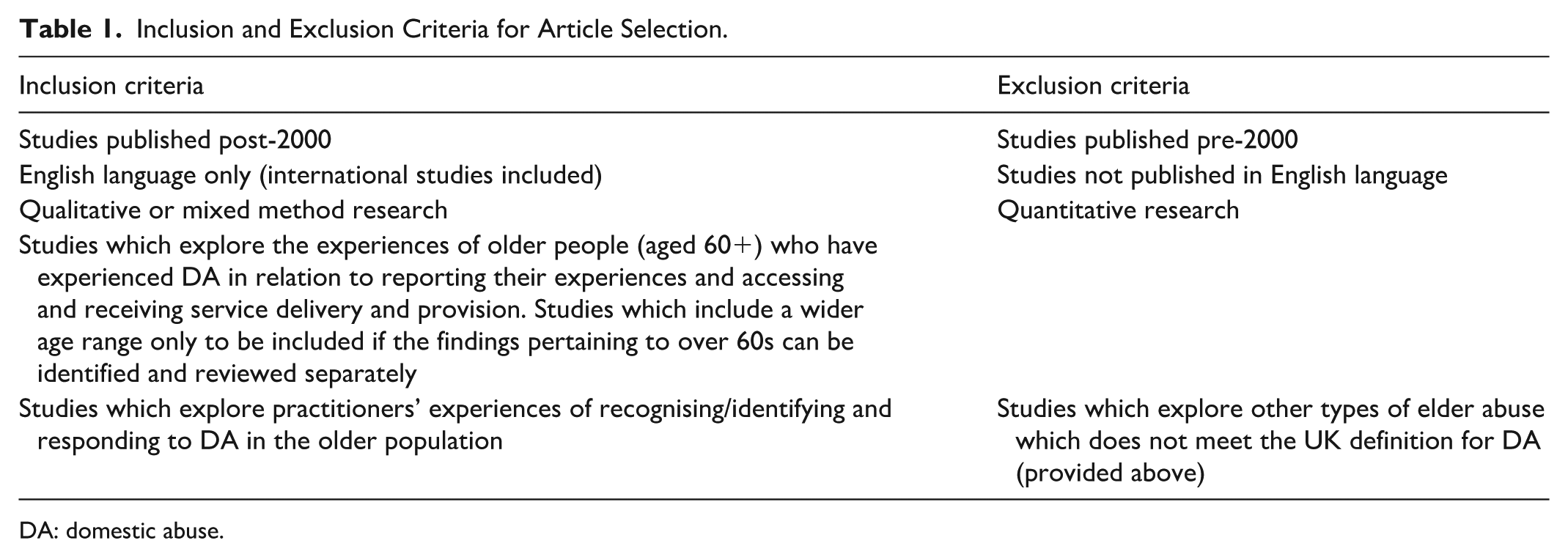
DA: domestic abuse.
In stage 3, two reviewers screened the remaining eligible articles against the Critical Appraisal Skills Programme resulting in a further two removals. In total, there were 25 remaining eligible articles and 4 remaining eligible reports which were included in the review (see Figure 1, for an overview of the process).
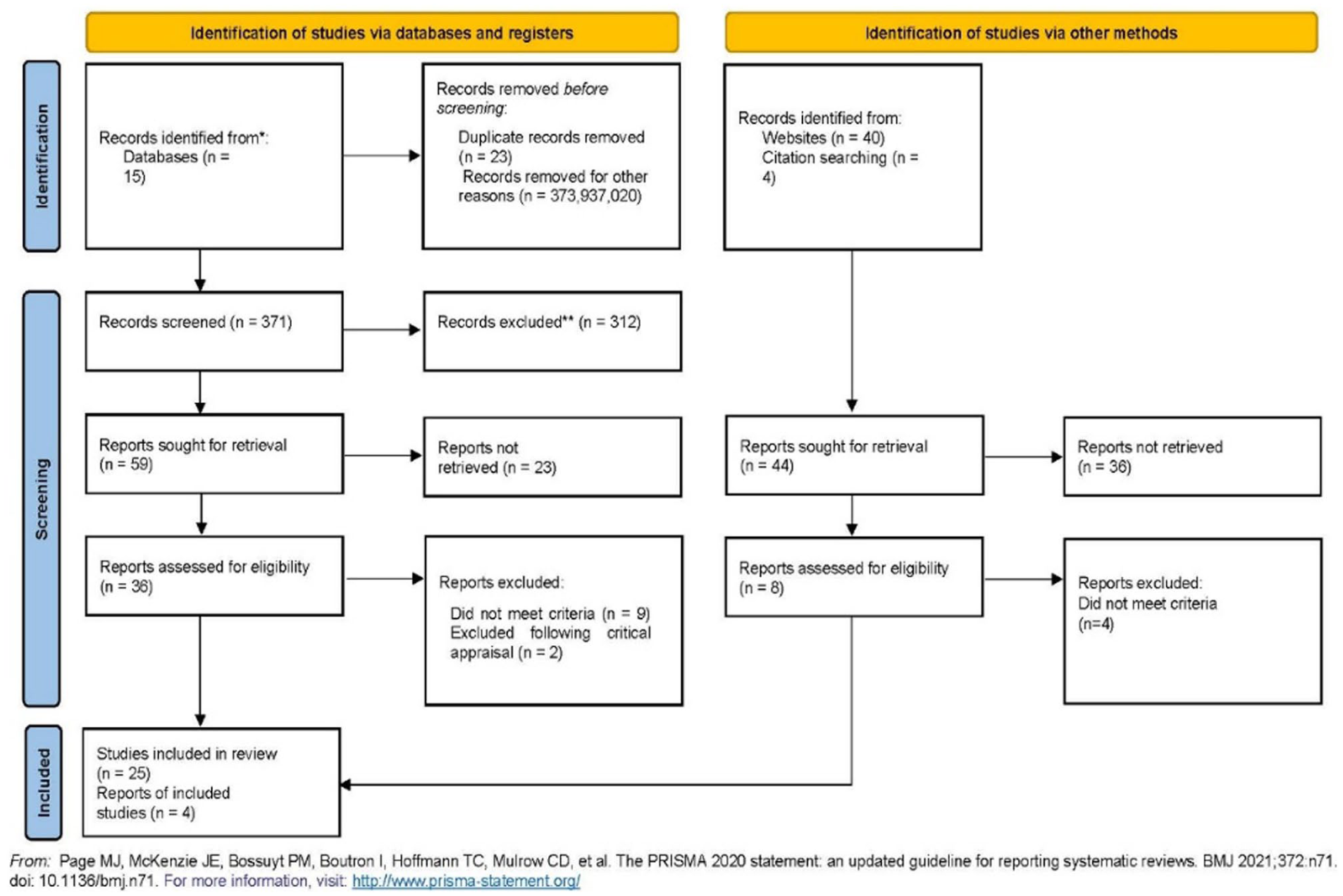
The PRISMA flow diagram.
Data Extraction and Analysis
Data extraction included the author(s), publication year and country, aims, objectives and research questions, study design, sample details, methods and ethical considerations (key data is reported in Table 2). This was undertaken by one author with checks undertaken. No automaton tools were used to extract data. Findings, themes, quotes, author interpretations and recommendations were also extracted for analysis. Using Thomas and Harden’s (2008) thematic synthesis and managed within NVivo 14 (qualitative data analysis software), two researchers independently coded the data before comparing and refining their descriptive themes collaboratively. Analytical themes were developed through further discussion and refinement. The review has been recorded in Prospero.
Summary of the Included Studies.
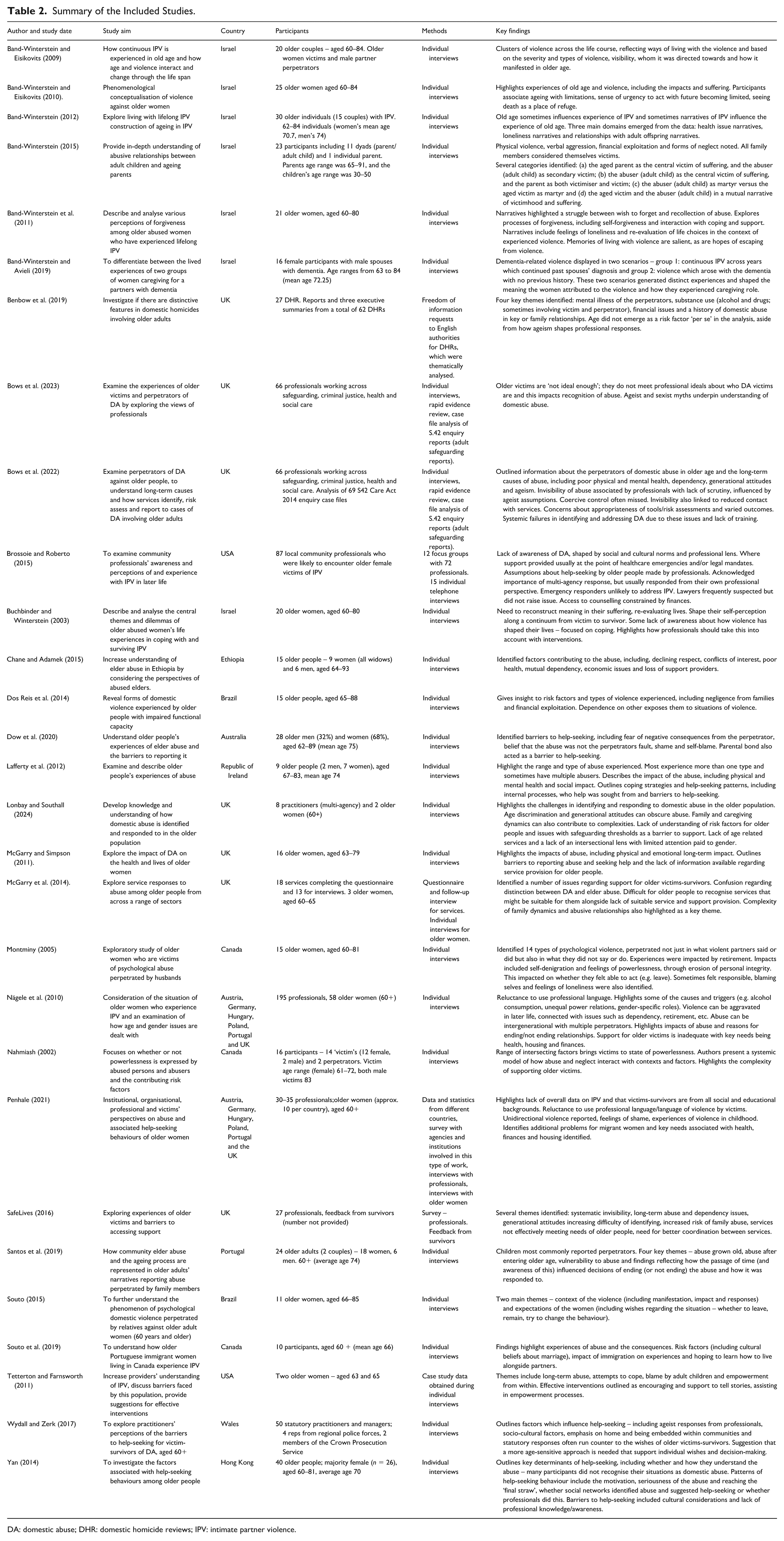
DA: domestic abuse; DHR: domestic homicide reviews; IPV: intimate partner violence.
Results
In total, 29 studies were included, all of which used interviews as the primary method, with some also including surveys or analysis of case files and Domestic Homicide Reviews. Many of the studies which included older victims-survivors as participants focused mainly on the experiences of abuse, including how they coped with and survived their experiences. Within these there was also consideration of disclosure and help-seeking which are explored in the findings below, including some of the key barriers to disclosing and issues which prevent older people from engaging with or maintaining contact with services or other forms of support. Practitioner perspectives are included and add knowledge about how they identify and respond to abuse. It is well established within this body of literature that the experiences and needs of older victims-survivors of DA differ from those of younger victims-survivors. The first section below outlines the forms and characteristics of DA in later life, highlighting some of the unique experiences of older victims-survivors. Following this, key themes from the thematic synthesis are presented.
Forms and Characteristics of Abuse in Later Life
All types of abuse were reported within the studies, including psychological, physical, financial and sexual as well as coercive and controlling behaviour, which was noted as being poorly understood and therefore often overlooked. Women are noted as being at higher risk of abuse with men more likely to perpetrate the abuse, and perpetrators can include grandchildren, children, siblings and partners or spouses, meaning there is also the potential for multiple perpetrators to be abusing an older person and for intergenerational abuse to be occurring, highlighting a key difference and complexity of DA in later life (Band-Winterstein, 2015; Bows et al., 2022, 2023).
For older people who experience abuse, the abuse may be a continuation of ongoing and historical abuse or may have begun in later life, either in new relationships (sometimes following divorce or death of a spouse) or emerging in established relationships. Band-Winterstein and Eiskovits (2009) also identified ‘clusters’ of violence across the life course, including: (a) high or moderate violence directed towards the whole family and maintained across the life course, (b) severe-to-moderate physical and emotional abuse directed overtly towards children and covertly towards ‘wives’ and lessening with age, (c) a shifting of physical violence towards the wife to different types of abuse, or a role reversal or emergence of mutual abuse as the couple ages and (d) violence continuing or worsening even when the male perpetrator becomes ill in later life. This context impacts on the views and perspectives of older victims-survivors. For example, in Santos et al. (2019) study, older victims-survivors who experienced historical abuse expressed regret at having lived a life overshadowed by abuse. A range of complexities are noted, linked to the intersections between age, abuse, gender, disability, sexuality and cultural background which are also poorly understood for older victims-survivors of DA.
Thematic Synthesis
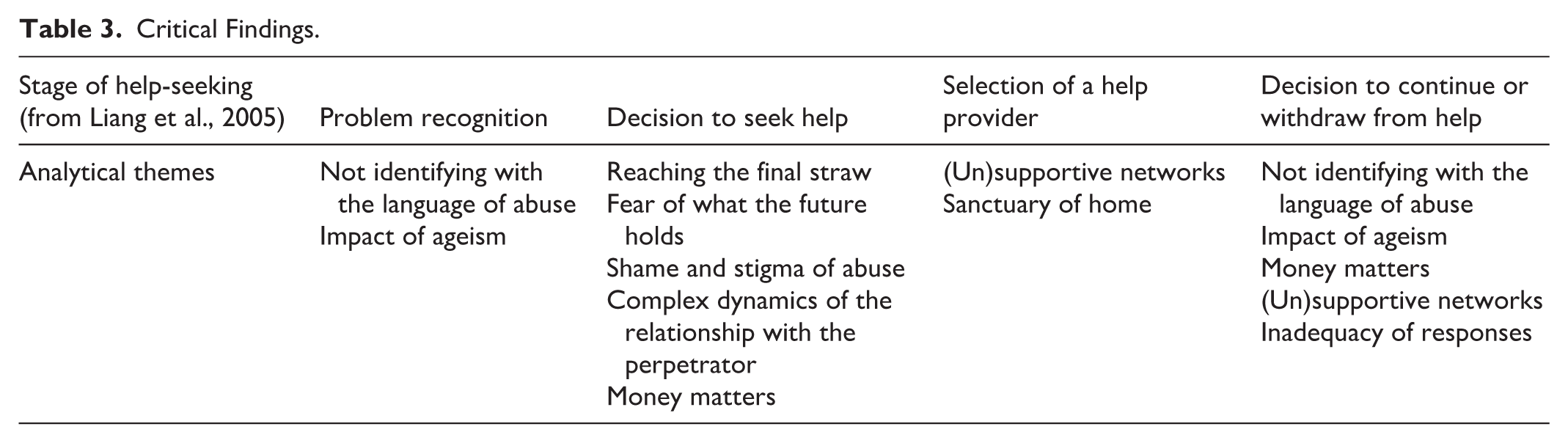
We identified nine analytical themes which reflect older people’s and practitioners’ experiences and perspectives on identification of and responses to DA. An overview of critical findings is presented within Table 3. Although presented separately for clarity, the nine analytical themes are interrelated, and Table 3 shows how they connect with Liang et al.’s (2005) help-seeking theory. Further interpretation of the themes through this theoretical lens is undertaken within the discussion. The themes illustrate the complex circumstances that older victims-survivors can find themselves in, caught between a ‘painful past and a trap like future’ (Buchbinder & Winterstein, 2003, p. 37).
Critical Findings.
Not Identifying with the Language of Abuse
Not identifying with the language of abuse operated as a significant issue in two ways. Firstly, it impacted on problem recognition, and secondly it impacted on how older people responded to professionals. It was noted across the studies that the person not recognising themselves as a ‘victim’ of DA was a barrier to problem recognition and thus to disclosure (Lonbay & Southall, 2024), for example, in Yan’s sample, only about half of their participants (men and women) labelled what they had experienced as abuse (Yan, 2014). The language used to discuss and share experiences also operated as a barrier for some older victims-survivors. In Nägele et al.’s (2010) study, this was noted as a reluctance to use the term ‘domestic violence’ or ‘partner violence’. Many authors also noted that conceptual confusion between ‘elder abuse’ and ‘DA’ can also impact on how it is identified and responded to, with use of terms such as elder abuse potentially leading to responses that do not fully recognise the complexities and dynamics of DA in later life or ignore the often gendered dynamics of the abuse impacting on the suitability of responses for older people (Bows et al., 2023; Lonbay & Southall, 2024; McGarry et al., 2014; Penhale, 2021; Wydall & Zerk, 2017). Wydall and Zerk (2017) highlighted that professionals in their study raised issues with the use of terms such as ‘perpetrator’ and ‘abuser’ which could isolate older victims-survivors further, impacting on whether they chose to continue with seeking help.
The Impact of Ageism
Ageism influenced help-seeking by firstly masking abuse in later life and by influencing responses to older victims-survivors; thus, ageism impacted both problem recognition and decisions to continue or withdraw from support. The social construction of a ‘victim’ and ‘perpetrator’ of DA and contrast of this with the reality of older victims-survivors/perpetrators was discussed in some studies. Bows et al. (2023), for example, discussed the ‘ideal victim’, assumed to be young and female, and how this means that older people are less likely to be viewed as victims-survivors of DA. The lack of recognition of DA in later life was attributed to ageism, with an assumption that people grow too old to engage in violent relationships (Brossoie & Roberto, 2015). This has had a knock on impact of reducing the number of age appropriate services and support systems that have developed for older victims-survivors; many studies noted a lack of suitable options for responding to DA in this population (Bows et al., 2022; Lonbay & Southall, 2024; McGarry and Simpson, 2011; McGarry et al., 2014; Nägele et al., 2010; Penhale, 2021; SafeLives, 2016; Santos et al., 2019; Souto, 2015). Homogenisation of the older population was also noted, with assumptions made about what older people might want and the sorts of activities they might enjoy (Band-Winterstein & Eiskovits, 2010; McGarry & Simpson, 2011; Wydall & Zerk, 2017). Chane and Adamek (2015) identified ‘declining respect for elders’ as a contributor to abuse and others noted ageism as influencing responses, including ‘risk assessment and management of potentially abusive situations’ (Benbow et al., 2019, p. 1114). This was echoed by others, for example, Wydall and Zerk (2017, p. 7) who commented that ‘little consideration was given to ensuring that the older person was central to the decision-making process and thus, ageism hindered a person centered-approach’. However, it was noted that ‘older people are willing and able to talk about their abusive experiences, including its impact on them’ and that ‘older people placed a high value on having someone to talk to about their abusive experiences’ (Lafferty et al., 2012, p. 52). Whilst the impact of ageism is a unique analytical theme, it is a systemic issue that impacts all stages of help-seeking.
Reaching the Final Straw
The literature suggests that older victims-survivors rarely seek help, and the decision to seek help may typically happen via third parties who notice signs of abuse (including health and social care professionals, friends or family members; Lafferty et al., 2012; SafeLives, 2016; Yan, 2014). Many of the articles also noted that when older victims-survivors do seek help, it is often preceded by a critical moment, described as a breaking point when they ‘couldn’t bear it anymore’ (Santos et al., 2019, p. 62). Lafferty et al. (2012) noted that older women ended abusive relationships when they ‘reached an all-time low’ (p. 11) with deteriorating physical and mental health. Their participants indicated that they felt that the only way to end the abuse was to die by suicide and reported the abuse for their own safety, highlighting the severe emotional distress experienced by victims-survivors. Acknowledging the impact the abuse had on them was also part of this, including the ‘irredeemable price’ they had ‘to pay in physical and psychological health’ (Buchbinder & Winterstein, 2003, p. 28). Santos et al. (2019) noted that some older victims-survivors decided to seek help if their health declined and they become more fearful of the consequences of remaining in the abusive relationship, thus linking help-seeking with growing older and ‘the perception of increasing physical vulnerabilities’ (p. 62). Souto (2015, p. 5) also noted this, stating that ‘calling the police was a last resort’ for participants in their study, quoting a participant who said, ‘I called the police because I was afraid that the situation was getting worse!’. For some older people, the desire to escape violence was coupled with a longing for a more peaceful life, linked by some articles as connected to participants’ perceptions that they had a ‘limited time to live’ (Santos et al., 2019, p. 62) and wanting to live ‘peacefully and happily’ (Nägele et al., 2010, p. 68).
Santos et al. (2019) also noted that age influenced help-seeking with their participants’ awareness of the ageing process also limiting their willingness to disclose abuse and seek help. Nägele et al. (2010) reported that the desire to leave the situation and live a life free from abuse and violence was strong from their participants, echoed in other articles (Dow et al., 2020; McGarry & Simpson, 2011; Santos et al., 2019) and in contrast to some practitioners’ perspectives where assumptions were made about older people’s likelihood of leaving abusive relationships, again highlighting the impact of ageism in professional responses (Lonbay & Southall, 2024; SafeLives, 2016; Bows et al., 2022; Wydall & Zerk, 2017). It is important to intervene before people reach a breaking point; however, risk factors for this population are poorly understood, though poor physical and mental health, dependency, generational attitudes, ageism, poverty, isolation and alcohol and substance abuse are noted by several studies as creating complex situations of vulnerability for older people (Benbow et al., 2019; Bows et al., 2022; Lafferty et al., 2012; Lonbay & Southall, 2024; Penhale, 2021; Dos Reis et al., 2014). While some practitioners across studies were aware and understood DA as an issue for older people, they expressed concern that many professionals lacked this awareness. This leads to services not being effectively targeted at older victims-survivors and therefore not responding as effectively as they would if they had a better understanding of the issues. Practitioners’ views overall were that guidance and training is required to improve knowledge and responses, particularly around key risks for older people (Penhale et al., 2021; Nägele et al., 2010; Lonbay & Southall, 2024; SafeLives, 2016).
Fear of What the Future Holds
‘Fear of what the future holds’ was also noted in the studies as influencing the decision to seek help, for example, Buchbinder and Winterstein (2003, p. 37) commented on how participants were caught between a ‘painful past and a trap like future’, linked to perceived limited prospects of choice, happiness, work, independence and alternative intimate relationships due to increasing age. This fear extended to concerns about not being listened to or believed, that choice and control could be removed by professionals following disclosure alongside other potential unwanted consequences and fear of institutionalisation (Bows et al., 2023; Dow et al., 2020; Lafferty et al., 2012; Lonbay & Southall, 2024; SafeLives, 2016; Souto, 2015; Yan, 2014).
Older people in these studies frequently feared that disclosing abuse and seeking help would result in a loss of choice and control, a fear that is not without basis, for example, SafeLives (2016, p. 17) reported participants being pressured into leaving by professionals and not being free to make their own decisions. Wydall and Zerk (2017, p. 8) noted that ‘older victim-survivors anticipated a lack of informed choice regarding statutory involvement’ with practitioners noting that it was not uncommon for them to ‘encounter alarmist, negative stereotypes about the statutory sector’ (p. 8). Fear of institutionalisation by older victims-survivors was noted, with participants citing this as a barrier to disclosure and help-seeking and in some cases it being used as a threat by perpetrators (Dow et al., 2020; Lafferty et al., 2012; SafeLives, 2016; Wydall & Zerk, 2017). SafeLives (2016, p. 19) reported that the ‘lack of specialised services for victims with disability’ can force ‘them to stay in abusive relationships’ and practitioners in Lonbay and Southall (2024) and Wydall and Zerk’s (2017, p. 7) studies noted inappropriate use of care home placements as ‘often all we can offer’ and this being ‘everyone’s worst nightmare’. Some studies noted that older people ‘make active, rational and logical decisions within the context of their own abusive situation and their family network’ and their financial and health status (Santos et al., 2019; Wydall & Zerk, 2017, p. 7), but that ageist and paternalistic attitudes could sometimes influence how practitioners responded (SafeLives, 2016). However, the studies emphasise that the outcomes sought by older people include the desire for interventions that support their independence and help them to manage their circumstances without feeling pressured to make decisions that will significantly alter their lives, highlighting the importance of their views and perspectives being respected.
The Shame and Stigma of Abuse
Shame and stigma were also frequently reported barriers to help-seeking across the studies (Brossoie & Roberto, 2015; Dow et al., 2020; Lafferty et al., 2012; Penhale, 2021; Souto et al., 2019), with generational norms and ‘strong cultural values and expectations’ sometimes preventing older people from disclosing abuse and seeking help (Brossoie & Roberto, 2015, p. 6). Nägele et al. (2010, p. 65) stated that disclosing and seeking help may be seen as a ‘sort of betrayal/violation of the intimate sphere and the partnership’. For many victims-survivors, marriage was seen as a lifelong commitment ‘for better or worse’ (Nägele et al., 2010, p. 65) with the perspective of ‘you’ve made your bed, now lie in it’ (Brossoie & Roberto, 2015, p. 4). These generational norms are problematic for help-seeking, increasing the shame and embarrassment that older victims-survivors can therefore feel when disclosing their experiences (Brossoie & Roberto, 2015; McGarry & Simpson, 2011). These difficulties were recognised by practitioners as well as being articulated by victims-survivors. The role of cultural norms in perpetuating silence and shame connected to abuse was also noted (Band-Winterstein & Eiskovits, 2009; Wydall & Zerk, 2017; Yan, 2014) and religion, though sometimes a support (Lafferty et al., 2012), could also compound feelings of shame and silence victims-survivors (Brossoie & Roberto, 2015).
The evidence from across the studies makes it clear that older victims-survivors value emotional support and someone to talk to about what is happening with this person providing a point of contact for disclosure. Key sources of support were adult children, friends, police, general practitioner (GP) and other medics, clergy, social work and other relatives. However, how this is received can have a clear impact on ongoing help-seeking. Both victims and those practitioners that had awareness of DA in the older population emphasised the need for professionals to be persistent, professionally curious and to keep offering opportunities for disclosure and engagement (SafeLives, 2016; Tetterton & Farnsworth, 2011).
Complex Dynamics of the Relationship with the Perpetrator
DA in later life can be linked to a range of perpetrators creating a level of complexity that is not found in DA situations with younger people. Two subthemes reflect the complex dynamics of the relationship with the perpetrator which influences decisions to seek help: ‘fear for the perpetrator’ and ‘fear of the perpetrator’.
Fear of the Perpetrator
Participants feared the perpetrator and potential consequences of seeking help, or attempting to leave, which could be compounded by other factors such as isolation (Santos et al., 2019). Both practitioners and victims-survivors identified behaviour used by perpetrators to control their victims and reduce their likelihood of seeking help. Perpetrators were noted as making a range of threats to control the victim. These included threatening to kill or harm them or their children with or without use of weapons, threatening to harm themselves (including suicide), destroy cherished belongings, cut off financial support or resources, prevent access to other family members, destroy homes, harm livestock and pets, remove the victim from the homes or to place victims in institutions (Band-Winterstein & Avieli, 2019; Band-Winterstein & Eisokovits, 2009; Brossoie & Roberto,2015; Dow et al., 2020; Lafferty et al.,2012; Montminy, 2005; Nägele et al., 2010; Souto, 2015; Tetterton & Farnsworth, 2011). Nägele et al. (2010) also commented on how the impact of trauma can cause offenders to seem even more powerful, increasing levels of fear. Health conditions may also increase fearfulness as well as be exacerbated by fear which can negatively impact on health (Souto, 2015). The long-term exposure to abuse that many older victims may have experienced can also serve to intensify this fear and may be compounded by issues such as a lack of appropriate services and fear of institutionalisation (Souto, 2015), further preventing help-seeking. The concept of forgiveness may also influence behaviour with Band-Winterstein et al. (2011) finding that forgiveness was an important tool for older victims-survivors in relation to their self-preservation and empowerment.
Fear for the Perpetrator
Victims-survivors’ decisions to seek help were also influenced by fear for the perpetrator, for example, worrying about what might happen to them (Nahmiash, 2002). Where perpetrators were a partner, feelings of emotional dependency could influence help-seeking, as well as concern about being alone in later life (McGarry et al., 2014; Nägele et al., 2010; Wydall & Zerk, 2017). Caregiving dynamics between the perpetrator and the victim-survivor are more likely in the older population (SafeLives, 2016) and can create multiple complexities and challenges, including masking the abuse and its historical nature (Lonbay & Southall, 2024). Practitioners in some studies noted that the caring dynamic and/or dependency on the abuser (including emotional, economic and immigration status dependency) could prevent the victims-survivors from seeking help and make it difficult for professionals to make contact and access them (Band-Winterstein & Eisikovits, 2010; Lonbay & Southall, 2024; Montminy, 2005; SafeLives, 2016; Souto et al., 2019). If the perpetrator was the cared for person, this can create feelings of guilt, particularly if the abuse has arisen alongside worsening health conditions or due to medical issues such as dementia, as noted by a participant in the SafeLives (2016, p. 15) study who said ‘and I still kept thinking, this man is ill and I can’t leave him’. Band-Winterstein and Avieli (2019, p. 375) noted that the presence of dementia in the perpetrator shaped older female victims-survivors’ narratives, including their willingness to care for the abusing partner; where the abuse was historical the women reported the care as a burden and expressed exhaustion and intolerance, whereas when the abuse had arisen with the dementia the women were more likely to ‘feel devoted to the welfare of their spouses’. This is an important finding lending emphasis to Lonbay and Southall’s (2024) assertion that establishing whether the abuse is historical is crucial in directing appropriate responses and avoiding ongoing DA being categorised as a symptom of the perpetrator’s illness or age-related conditions.
Help-seeking was also noted as less likely to occur in cases where the perpetrator was a child or grandchild (Dow et al., 2020; Nahmiash, 2002). Parents may prioritise maintaining family relationships and protecting children, creating additional barriers to help-seeking as they fear negative consequences such as imprisonment for their family member (Dow et al., 2020; Wydall & Zerk, 2017). In one study, a participant said ‘I can’t take him to court, I just can’t do that’, demonstrating the emotional conflict they felt between protecting themselves and protecting their child (Dow et al., 2020, p. 5). A reluctance to disclose abuse perpetrated by children can also arise through a sense of responsibility for the abuse through their own parenting or through justification of the abuse due to the circumstances, for example, substance use, unemployment or mental health problems (Bows et al., 2022; Dow et al., 2020; Wydall & Zerk, 2017). Older victims-survivors may perceive reporting abuse as a betrayal of the family unit. This perception, coupled with societal norms that prioritise family loyalty, can make it difficult for them to disclose the abuse or seek external support (Lafferty et al., 2012; Dow et al., 2020; Nahmiash, 2002). These findings highlight the complexity of parent–child or grandparent–grandchild relationships, the victim-survivor’s sense of responsibility and the emotional and practical difficulties in addressing the abuse. Older victims can fear that ‘by seeking help they may lose contact with, or in some way cause harm to’ their children or grandchildren (Dow et al., 2020). In such instances, Dow et al. (2020, p.7) noted that family mediation may be effective as it is ‘not perceived as being adversarial and suggests resolution of conflict’; however, such approaches may also be problematic as they can lead to normalisation of the behaviours and a perception that the victim-survivor should stay and try to work through issues with the perpetrator. Some practitioners across the studies demonstrated understanding of these dynamics and the additional complexities that may be impacting on the victim-survivor’s decision to leave the abusive relationship or pursue prosecution in the courts (Lonbay & Southall, 2024; Nägele et al., 2010; Santos et al., 2019).
Money Matters
Both practitioners and victims-survivors highlighted practical issues as important barriers to help-seeking. The impact of retirement was raised, linked to reduced income and to increased conflict and tension in the abusive relationship (Santos et al., 2019). Some felt that the choice to be made was stay in the abusive situation or gain ‘a level of independence from a violent husband, but only at the price of poverty’ (Buchbinder & Winterstein, 2003). As older victims-survivors are often financially dependent on the perpetrator this creates an additional barrier to help-seeking, highlighting the importance of financial support for older victims-survivors (Santos et al., 2019). This problem is exacerbated by limited opportunities for seeking employment and raising additional funds in later life, as noted by a primary care doctor in Brossoie and Robertos’(2015, p. 6) study who said ‘They can’t get a job. They can’t take care of themselves. They don’t feel confident being on their own and they don’t have anywhere to go’. Brossoie and Roberto (2015) also noted that ‘fewer older adults sought counselling because of financial reasons’ highlighting that access to financial resources limits help-seeking in multiple ways, including decisions to seek help in the first instance and whether to contribute or withdraw from support. Nägele et al. (2010, p. 65) also drew attention to the situation of older immigrant women who are noted as often being economically dependent due to not having ‘their own income or pensions or if they do’ having ‘only modest ones’. Ongoing financial and practical support is therefore crucial.
(Un)supportive Networks
Selection of a help provider can be problematic for older victims-survivors, depending on their networks. Wider social networks, connections and the church were often a supportive factor for older victims-survivors and friends and other relatives were noted as people from whom older victims-survivors would seek help, for example, Band-Winterstein (2012, p. 510) noted that children’s role in DA could be through intervention, negotiating and ‘policing’ and helping the parents to cope, with others noting similar support from children (Nägele et al., 2010). However, family could also be a negative influence, including by supporting historical patriarchal structures, refusing to believe that the abuse was taking place, preventing victims-survivors from seeking help or hindering practitioner interventions and support (Dow et al., 2020, SafeLives, 2016). SafeLives (2016, p. 13) also noted that ‘adult children may put pressures on their parent to stay’. Such pressure could influence decisions to seek help or leave, as victims-survivors may not want to lose contact with their children thus linking with decisions to withdraw from support. This is likely compounded by the finding from across the studies that these older victims-survivors are also likely to have a lack of informal and formal support networks (McGarry & Simpson, 2011; Souto et al., 2019; Wydall & Zerk, 2017). Retirement may also reduce older people’s social networks, and Montminy (2005) noted that entering retirement appeared to increase the risks and impact of psychological abuse. Whilst isolation is a significant issue for many older people, in the context of DA, it is often a deliberate strategy of coercive control.
The Sanctuary of Home
The importance of home and it roles in influencing whether older victims-survivors continued with or withdrew from support was highlighted in the studies, with practitioners in Wydall and Zerk’s (2017) study commenting on how older victims-survivors placed much greater emphasis on the importance of home than younger people. Wydall and Zerk (2017, p. 9) described the home as a ‘site of ontological security’ creating a paradoxical situation whereby the home is the place of unsafety and abuse, alongside being a space of sanctuary. Furthermore, practitioners in Wydall and Zerk’s (2017) study spoke about how severing links with the home could lead to increased isolation for older victims-survivors. Other studies also noted emotional attachments to the home as a barrier to help-seeking and decisions to leave (Brossoie & Roberto, 2015; Nägele et al., 2010; SafeLives, 2016). The importance of not ‘pushing’ older people to leave was also highlighted (SafeLives, 2016), and many studies identified that where older people connect with services the provision of information, emotional and practical support is crucial with the importance of listening to and respecting the older victim-survivor’s views and decisions highlighted (Lafferty et al., 2012; Lonbay & Southall, 2024; SafeLives, 2016).
(In)adequacy of Responses
Overall, there was consensus in the studies across both victims-survivors of abuse and practitioners that responses were not adequate to meet the needs of older people. Policies, guidance and common DA tools were noted as inadequate or unsuitable for use with an older population. Statutory responses were criticised with authors noting that contact with the Criminal Justice System was often unhelpful or even contributed to the violence. Wydall and Zerk (2017, p. 6) also commented on how ‘statutory responses often ran counter to the expressed wishes of the older person’. Where services did intervene to offer support, there were other issues encountered such as the lack of resources to offer suitable help, including legal support, support for mental health and a lack of suitable housing options for older victims-survivors (Lafferty et al., 2012; Lonbay & Southall, 2024; McGarry & Simpson, 2011; McGarry et al., 2014; Nägele et al., 2010; Wydall & Zerk, 2017). Many of the studies highlight the need for increased awareness and understanding of DA in the older population, particularly for practitioners, so that it can be more readily recognised and the complexities of abuse in this population better understood (Bows et al., 2022; Brossoie & Roberto, 2015; Buchbinder & Winterstein, 2003; Chane & Adamek, 2015; Dos Reis et al., 2014; Lonbay & Southall, 2024). Additionally, some authors noted that multi-agency working required significant improvement in order to effectively respond to DA in the older population, for example, practitioners in Brossoie and Roberto’s (2015) study stated that they ‘often’ responded from the ‘vantage point of their own professional domain’ and noted challenges in coordinating services with SafeLives (2016) describing an ‘ideological gulf’ between DA services and older people’s services.
Discussion
This review has synthesised the evidence on older people’s help-seeking behaviour for DA as well as practitioners’ experiences in identifying and responding to abuse. The findings highlight a range of complex, intersecting factors which influence the identification of and responses to DA and perpetuate a cycle of invisibility for older people within the DA landscape. Whilst there is some crossover in relation to the experiences of younger victims-survivors, the findings from this review clearly highlight that there are also critical and significant challenges that are unique to older victims-survivors and which require a tailored response. To best explicate these, we have drawn on the help-seeking theory introduced above (Liang et al., 2005) to interpret the findings. Liang et al. (2005) noted that their model is primary described in cognitive terms, but that interpersonal and socio-cultural factors will also influence help-seeking. This is clear within the review findings which highlight interpersonal and systemic influences on the older person and on practitioners. The theory of help-seeking has been used within DA studies with younger victims-survivors and includes three stages: problem recognition, decision to seek help and selection of a help provider (Liang et al., 2005). Although Liang et al. (2005) noted that ‘the helper she [the victim-survivor] chooses will influence how she defines the problem and whether she seeks help again’, the importance of the help providers’ reaction in influencing older victims-survivors decisions was so evident within this review that it was deemed necessary to add an additional stage in our help-seeking by older victim-survivors framework, which is the decision to continue or withdraw from help. Understanding of help-seeking following DA experiences has largely been developed from the perspectives of younger victims-survivors and does not account for age-specific factors. This review has therefore addressed an important gap in knowledge by both extending Liang et al.’s (2005) theory and applying it within the context of older victims-survivors of DA.
Recognition of the Problem
Recognition of the problem was raised by practitioners and by older people in this review as being highly problematic, both for themselves and for others to whom they might turn for help. Recognition of the problem may be particularly difficult when the abuse is nonphysical, which has also been found with younger victims-survivors (Lelaurain et al., 2017). Friends, family or faith communities may also minimise or normalise the abuse, making recognition harder (Dow et al., 2020; McGarry & Simpson, 2011; SafeLives, 2016). Although not raised specifically within this review, the wider literature on DA also highlights the issue of ‘gaslighting’ whereby perpetrators manipulate victims-survivors into doubting their own perceptions, making it hard for them to recognise their abuse (Sweet, 2019). Psychological abuse was, however, apparent within these studies including manipulation and blaming which overlap with gaslighting behaviour (Montminy, 2005; Santos et al., 2019). DA is also obscured through issues such as DA materials not featuring older people and a lack of training addressing older victims-survivors (McGarry & Simpson, 2011). Public discourse and policy framing DA as a young woman’s issue alongside generational and patriarchal norms make it difficult for older victims-survivors to identify and name their abuse. These generational norms, shaped by historical discourses of family privacy and gender roles, intersect with shifts in DA policy, which only recently began to recognise other forms of nonphysical violence, including for example, coercion and control. This historical lag creates an awareness gap for older people who may remain unaware of current legal protections or support systems available.
Decisions to Seek Help
Older victims-survivors’ decisions to seek help may be precipitated by a critical moment, supported by the wider DA literature which suggests that the more severe the violence and abuse the more likely the person will seek help (Ansara & Hindin, 2010; Lelaurain et al., 2017; Rohn & Tenkorang, 2024). Fear of shame and stigma can prevent help-seeking for all victims-survivors of DA (Ansara & Hindin, 2010; Rohn & Tenkorang, 2024); however, uniquely for older people internalised generational norms may also present an additional and significant barrier in the decision to seek help. For example, these may impact on attitudes towards authority and institutional care which can exacerbate fears around seeking help, especially if older victims-survivors associate this with loss of autonomy or forced institutionalisation. Such fears may be compounded for groups who have historically faced discriminatory responses from service providers, for example, older LGBTQ+ people and people from Black and Minority Ethnic communities. Decisions to seek help are also influenced by the dynamics of the abuse and the relationship with the perpetrator, with systemic barriers (such as lack of access to personal funds) further complicating help-seeking decisions. Ageism plays a pervasive role, influencing whether older victims-survivors recognise services as available for them, as well as practitioners’ recognition of DA. This is also impacted by life course experiences and societal shifts.
Selection of a Help Provider
The literature reviewed did not cover extensively how selections were made about whom to turn to for support. However, it does identify that older people turn to a range of trusted others for help and support following DA. Evidence from the wider literature on violence and abuse demonstrates that most victims-survivors disclose to informal services, though disclosure to formal support services is also common (Ansara & Hindin, 2010; Dworkin et al., 2019). Furthermore, there is evidence in the wider literature that help from a formal service is more likely to be sought the more severe the level of violence faced (Ansara & Hindin, 2010; Lelaurain et al., 2017; Rohn & Tenkorang, 2024). People within informal networks may lack the knowledge or understanding to respond appropriately or may minimise abuse due to generational norms (McGarry & Simpson, 2011). This highlights a significant gap in the literature regarding how informal networks can be better equipped to help older victims-survivors. Further work is also needed to understand why older people may be more likely to turn to these networks.
Selection of a help provider is also influenced by fears about how the person might react as well as awareness of who is available to offer help and support. The literature reviewed did not cover aspects which allow for an intersectional analysis; however, the wider literature (pertaining to younger victims-survivors) indicates that people from Black and Minority Ethnic communities may face additional barriers rooted in both ageism and racism, which may lead to mistrust of institutions that have historically marginalised their communities (Mendoza & Rochford, 2024; Waller et al., 2023). For example, there is evidence that ethnicity is a barrier to help-seeking, potentially due to immigration status or perceptions of organisations as inaccessible (Lelaurain et al., 2017; Mendoza & Rochford, 2024). Generational and patriarchal norms also influence whether and how people select who to turn to and older victims-survivors may have limited knowledge of who is available for support, influenced by how services have developed over time, as well as more limited support networks overall.
Decision to Continue or Withdraw From Help
Although not part of the original help-seeking theory, this stage is included to highlight the importance of help provider reactions to the older victim-survivor. The importance of a ‘first positive contact’ from services has been highlighted in the wider literature (Lelaurain et al., 2017), and this review demonstrates that help provider responses influence whether older victims-survivors continue to engage with support following disclosure. Family and friends play a core role (Lafferty et al., 2012) and the way that initial disclosures and requests for support are received can impact on the person making the disclosure. For example, receiving a negative reaction to the disclosure can increase the severity of PTSD, depression and general distress across different forms of violence, and the victim-survivor’s own perception of reactions is an important factor within this (Dworkin et al., 2019). Healthcare practitioners, especially GPs, are often able to identify abuse and facilitate help-seeking so it is crucial for them to react appropriately (Nägele et al., 2015). There is a need for additional training so that they can recognise physical and nonphysical signs of abuse and to help address embedded ageist assumptions.
Ageist responses and pressure from informal networks can reinforce stigma and pressure victims-survivors to either stay in abusive situations or leave against their will (Dow et al., 2020; Femi-Ajao et al., 2020; SafeLives, 2016). Ageist assumptions also shape responses and frame tensions between protection and autonomy. Ludvigsson et al. (2022, p. 5) noted that reduced autonomy was sometimes a ‘consequence of dependence on help’, which included decisions about where victims-survivors lived. The idea that older victims-survivors should be placed in care homes as a default ‘solution’ reflects deep-seated ageist assumptions around institutionalisation as inevitable in later life, as well as highlighting the lack of resources which further compounds the issues. Growing awareness has led to increased recognition of the need for specialist services and responses (Penhale, 2021).
Limitations
While the findings of this systematic review are relevant to advance our understanding of DA in the older population, limitations must be acknowledged. There is a strong reliance in the studies on self-report data which may have been influenced by context such as cultural norms and gender expectations as to what behaviour was considered abusive (Ricoy-Cano et al., 2024). In addition, we recognise the challenges in defining DA highlighted by Zhang et al. (2022). Findings therefore need to be taken cautiously bearing in mind cultural, geographical and definitional variations. Despite these variations, it is important to recognise the focus of the review is on qualitative data and the consistency of the emergent themes. While not specifically excluded, there was little reference to the intersectional nature of abuse which affects older victims-survivors differently depending on gender, race, sexuality, disability and socio-economic status. This is an area where further research is required.
Conclusion
This systematic review included 29 articles that met the inclusion criteria and highlighted that there is a need for more research in this area to provide further evidence about what interventions are wanted and needed by older victims-survivors. The review addresses an important gap by synthesising existing evidence about DA in the older population. By mapping analytical themes against Liang et al.’s (2005) help-seeking theory, the review has highlighted age-specific factors that influence each stage of help-seeking and extended the theory in regards to the importance of a fourth stage, the decision to continue or withdraw from help.
Future research should focus on the intersection of age, race, gender and other identities to understand how these factors shape help-seeking among older people and responses from practitioners. Additionally, longitudinal studies could explore how generational shifts in policy and awareness impact older victims-survivors engagement with services over time. More work is needed to clarify differences in help-seeking and support needed for older people where the abuse is historical (e.g. abuse grown old in the relationship) or where it has begun later in life, particularly where caregiving dynamics also intersect.
Key areas for support include the need for emotional support to reduce feelings of isolation and access to practical support and information. Services need to be age-appropriate and culturally sensitive and ensure that they support older victims-survivors to address feelings of shame and stigma. Older victims-survivors may also need additional support to manage complex family dynamics and to address health needs which may be exacerbated by age or by being in an abusive situation over a long period of time. Addressing DA in the older population therefore requires multi-level interventions, including training professionals to recognise abuse, improving financial, housing and other practical support, challenging ageism and creating age-sensitive DA services. An overview of our key recommendations is included in Table 4.
Implications for Practice, Policy and Research.
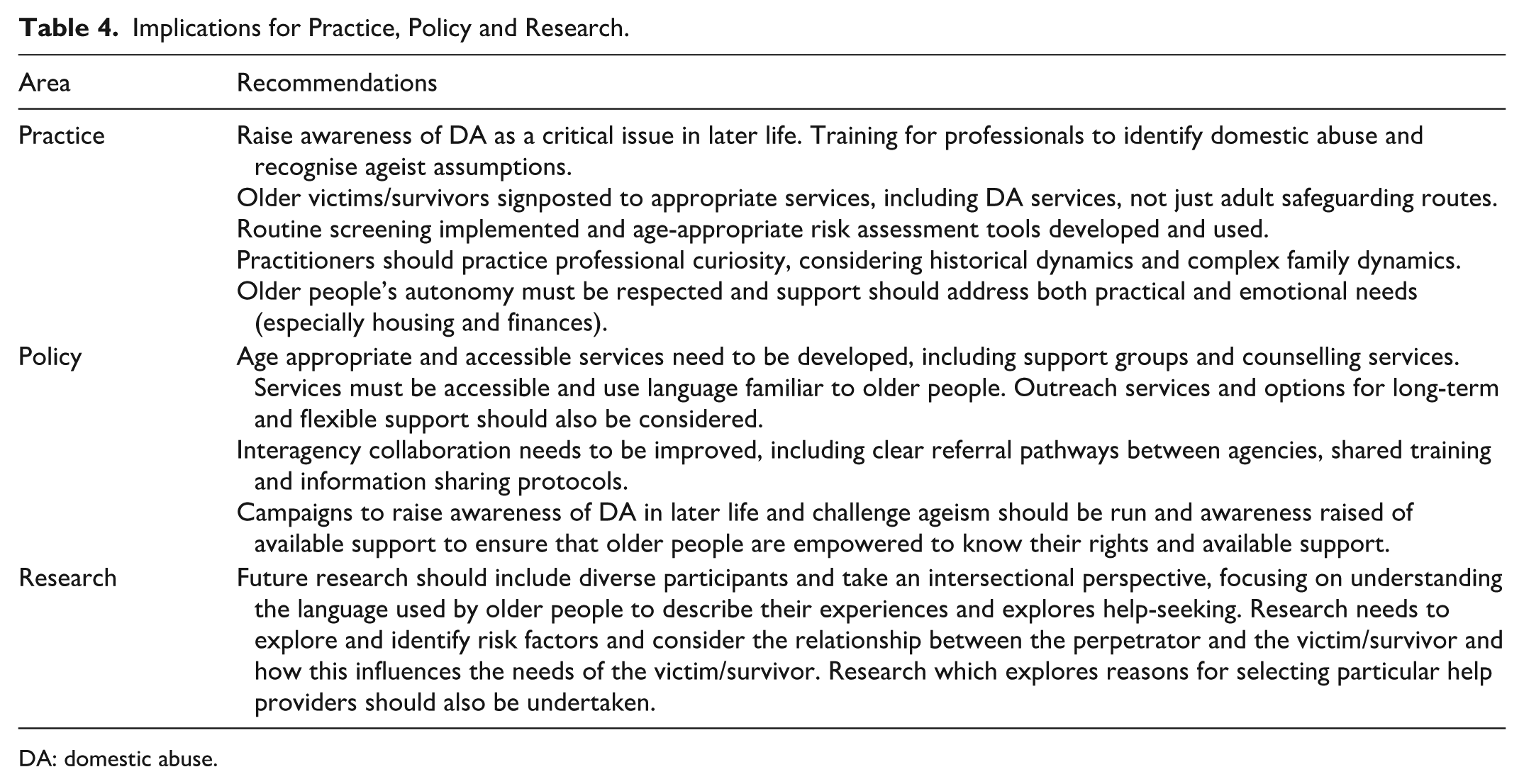
DA: domestic abuse.
Using help-seeking theory has helped to reveal several challenges, including systemic failures, institutional biases and embedded ageist assumptions which affect older victims-survivors. The focus must shift from helping older victims-survivors navigate systems that were not designed for them and do not work for them to developing these systems so that they fully meet the needs of the older population. This requires not only more research and training, but also policy reform, accountability and a shift in how we conceptualise DA across the lifespan.
Footnotes
Acknowledgements
We would like to thank the authors of the original studies included in this review, as well as the participants who contributed to those studies, without whom this synthesis would not have been possible.
Ethical Considerations
Ethical approval was obtained via the University of Sunderland (reference number 016572).
Consent to Participate
Informed consent was not applicable as no new data were collected from participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by University of Sunderland. Sarah Lonbay is also partly funded by the NIHR ARC NENC (NIHR200173). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Citations for all studies used in this review have been provided.