
Abstract
Intimate partner violence (IPV) is a serious public health challenge with disproportionately high rates among United States (U.S.) Service Members and Veterans. IPV is often conceptualized as a unidirectional phenomenon despite evidence that most IPV is bidirectional, where both members of a couple use and experience IPV. This scoping review examined the current state of the literature on bidirectional IPV among Service Members and Veterans. MEDLINE, Embase, APA PsycInfo, APA PsyArticles, APA PsycExtra, CINAHL, CENTRAL, CDSR, Academic Search Premier, ERIC, Sociological Abstracts, PTSDpubs, ProQuest Dissertations & Abstracts, Scopus, and Web of Science databases were searched. Articles were selected based on the following inclusion criteria: (a) contains data on U.S. Service Members or Veterans over the age of 18; (b) measured IPV use (i.e., perpetration) and experience (i.e., victimization) during an overlapping period, and (c) reported bidirectional IPV at least once in either text, figures, or tables. Overall rates of bidirectional IPV across studies (n = 21) ranged from 25% to 66.9%; rates disaggregated by subtype ranged from 1.5% (bidirectional sexual IPV) to 94% (bidirectional psychological IPV). There was considerable cross-study variation in measurement and operationalization. No studies contained data from both Service Members and Veterans in the same study. Higher rates of overall bidirectional IPV were documented among Veterans (range: 28.4%–66.9%) relative to Service Members (25%). These results highlight the need to collect data on the bidirectional IPV from Service Members and Veterans in the same study and consistent approaches to measuring and operationalizing bidirectional IPV.
Introduction
Intimate partner violence (IPV) encompasses a range of behaviors between current or former spouses and partners that cause physical, sexual, or psychological harm, such as physical aggression, sexual coercion, psychological abuse, and controlling behaviors (World Health Organization, 2025). While often conceptualized as a unidirectional, gendered phenomenon in which men exert power and control over women (Bates, 2016), this perspective has been challenged by evidence that bidirectional IPV, defined as the co-occurrence of IPV experience (i.e., victimization) and IPV use (i.e., perpetration) between partners, as the most common IPV pattern (Langhinrichsen-Rohling et al., 2012; Machado et al., 2024). Further, a recent systematic review identified that bidirectional IPV was consistently the most common pattern regardless of type of sample (i.e., community, forensic, or clinical; Machado et al., 2024). High rates of bidirectional IPV do not necessarily imply gender symmetry with respect to motivation, severity, or impact of IPV, although they underscore the need to examine IPV inclusive of sex, sexual orientation, and within the context of marital and family dynamics (Bates, 2016; Machado et al., 2024).
Service Members and Veterans share challenges that may pose risks for IPV. Service Members and their partners frequently move for military assignments (i.e., permanent change of station moves), posing risks for social isolation by geographically separating people from their social support networks. Individuals who may otherwise leave abusive partners by temporarily moving in with a local friend or relative may therefore be unable to do so, especially when stationed overseas or in remote locations (Kamarck, 2019). Further, difficulties in coping with frequent relocations and other demands of military life (e.g., long work hours, shift work, or unpredictable deployments) may exacerbate relationship conflict and instability, leading to increased risk of IPV (Kamarck, 2019; Le Menestrel & Kizer, 2019). Service Members and their families have access to many supports, services, and resources designed to mitigate the negative impact of stressors that come with military life, although they lose access to most of them upon separation from military service (Castro & Kintzle, 2014; Le Menestrel & Kizer, 2019). Stressors associated with military life and separation from military service have been theorized to contribute to maladaptive responses—including IPV—among families that are highly reactive, overwhelmed, or exhibit deficits in coping skills and resources (Le Menestrel & Kizer, 2019).
Concern relating to high rates of IPV has been documented among military and Veteran populations, relative to their civilian counterparts, leading the Veterans Health Administration (VHA) to implement the IPV assistance program (IPVAP) to promote awareness and enhance approaches to IPV treatment and prevention. Accordingly, terminology used in this study—“IPV use” and “IPV experience,” as opposed to “victimization” and “perpetration,” respectively—adheres to IPVAP’s recommendations for using trauma-informed, person-first language. A recent meta-analysis of population-based surveys identified that 13% of Service Members and Veterans reported recent IPV use and 21% reported recent IPV experience (Cowlishaw et al., 2022), contrasted with past-year IPV use estimates around 6% (Okuda et al., 2015) and 5% for IPV experience the general population (Okuda et al., 2011). There is some indication that Veterans have elevated rates of IPV relative to Service Members. Past-year IPV use prevalence rates have ranged from 5.2% to 36% among Service Members (Coppola et al., 2025; Cowlishaw et al., 2022), compared to 31.8% to 50.8% among Veterans (Coppola et al., 2025; Cowlishaw et al., 2022); meanwhile, past-year IPV experience prevalence rates have ranged from 13.3% to 37.6% among Service Members (Coppola et al., 2025; Gierisch et al., 2013), compared to 24.3% to 47.9% among Veterans (Coppola et al., 2025; Cowlishaw et al., 2022). Elevated rates of IPV, in combination with stressors associated with military life and the military-to-civilian transition, justify the need to examine and understand bidirectional IPV disaggregated by current military affiliation.
Bidirectional IPV has been documented as the most common pattern of IPV (Machado et al., 2024), a finding that has also been replicated in the samples of U.K. Service Members (Langhinrichsen-Rohlinget al., 2012; MacManus et al., 2022) and U.S. Veterans (Portnoy et al., 2023, Portnoy et al., 2024). Bidirectional IPV has been documented as the most prevalent form of IPV regardless of subtype of IPV (physical, sexual, or psychological), global region, sex assigned at birth, sexual orientation, or type of sample (Machado et al., 2024). A recent systematic review documented rates of bidirectional IPV ranging from 2% to 98.4% in clinical samples, in contrast to 3.1% to 89.1% in community samples and 5.3% to 74.4% in forensic samples (Machado et al., 2024). No known evidence synthesis has examined bidirectional IPV in military or Veteran samples, despite their disproportionately high rates of IPV.
Theoretical perspectives propose that different IPV patterns correspond to differences in sampling and relevant sample characteristics (Johnson, 2017). In his theory of IPV typologies, Johnson (2012; 2017) identified three IPV patterns that imply bidirectionality (Bates, 2016): violent resistance (VR), situational couple violence (SCV), and mutual violent control (MVC). VR is typically gendered, characterized by a female partner eventually responding to a male aggressor with violence of her own, meanwhile SCV—violence rising from both partners due to escalating conflict and initially equally across gender—is more common in general samples (Johnson, 2017). Both partners use violence and other tactics in attempting to seize control in MVC. Intimate terrorism (IT), on the other hand, is unidirectional, typically found in help-seeking and law enforcement settings (i.e., courts, probation and parole, domestic violence shelters), and characterizes relationships where primarily men use violence to control their female partners (Johnson, 2012). Although Johnson (2012) does not make specific propositions related to military and Veteran populations, inherent to his typology is the value of examining bidirectional IPV disaggregated by sample characteristics.
An enhanced understanding of bidirectional IPV is critical to meeting the needs of Service Members and Veterans. First, understanding the prevalence of bidirectional IPV yields important implications for practice and policy. Most policies and interventions are tailored to unidirectional IPV (Bates, 2016), although high rates of bidirectional IPV would justify United States (U.S.) Department of Defense (DoD)- and Veterans Affairs (VA)-sponsored programming to address and target co-occurring IPV use and experience. Understanding differences in rates of bidirectional IPV among military and Veteran populations may offer informative cues for risk factors contributing to IPV among these populations. For example, although military and Veteran couples have experienced many “common” stressors that may pose risks for IPV such as deployment, exposure to combat-related trauma, and its sequelae (Le Menestrel & Kizer, 2019), Veteran couples experience an additional set of stressors related to transitioning out of military service and into civilian communities (Castro & Kintzle, 2014). Examining bidirectional IPV disaggregated by current military affiliation may therefore inform the development of treatment modalities and interventions appropriately tailored to each population.
Current Study
As the first known scoping review on bidirectional IPV among Service Members and Veterans, this study included articles published since the review on bidirectional IPV conducted by Langhinrichsen-Rohling et al. (2012). This review aimed to examine the current state of literature on bidirectional IPV among U.S. Service Members and Veterans. By narrowing the scope to U.S. populations, this review reduced heterogeneity related to cross-cultural differences in IPV (Zark & Satyen, 2022) while yielding results that inform programs and practices specific to the U.S. DoD and VA. Secondary goals include comparing rates of bidirectional IPV disaggregated by current military affiliation (i.e., Service Members or Veterans) and identifying understudied groups of Veterans and/or Service Members. Sample characteristics were summarized, with results yielding recommendations for future research, practice, and policy.
Method
Current research on bidirectional IPV among Service Members and Veterans was summarized with a scoping review (Peters et al., 2022), which is a type of systematic review that aims to determine the scope of literature and state of knowledge on a specific topic (Peters et al., 2015). Scoping reviews may be used to examine existing research, clarify definitions and key concepts, and identify knowledge gaps and directions for future research (Peters et al., 2022). Rather than focusing on a narrower research question, we sought to synthesize what is known about bidirectional IPV among Service Members and Veterans, with the goal of guiding future research in this area.
This scoping review was conducted in accordance with Joanna Briggs Institute guidelines for scoping reviews (Peters et al., 2022), adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (Tricco et al., 2018), and pre-registered on Open Science Framework (https://osf.io/). Although the parameters for scoping reviews do not call for critique of methodological rigor or quality assessment (Peters et al., 2022; Tricco et al., 2018), a narrative appraisal (Pluye et al., 2011) was conducted to further contextualize findings.
Search Strategy
An experienced medical librarian (Melissa C. Funaro, MS, MLS) was consulted on methodology and ran a medical subject heading analysis of known key articles provided by the research team. Searches in each database were refined using an iterative process. To maximize sensitivity, the formal search used controlled vocabulary terms and synonymous free-text words to capture the concepts of “Intimate Partner Violence” and “bidirectional” (e.g., “mutual,” “reciprocal,” “common couple violence”). The search strategy was reviewed by a second librarian external to the project, using the PRESS standard (McGowan et al., 2016; see Supplemental Table 1).
On February 5, 2024, the librarian performed a comprehensive search of multiple databases, including MEDLINE, Embase, APA PsycInfo, APA PsyArticles, APA PsycExtra, CINAHL, CENTRAL, CDSR, Academic Search Premier, ERIC, Sociological Abstracts, PTSDpubs, ProQuest Dissertations & Abstracts, Scopus, and Web of Science, which was rerun using the same databases on July 3, 2025. Search results were limited to articles published since 2011, the date of the last comprehensive review on bidirectional IPV (Langhinrichsen-Rohling et al., 2012), and to current. Citation chaser software was used to identify additional articles included for screening based on citing references and references of included studies (Haddaway et al., 2021).
Results were pulled into EndNote, de-duplicated using the using the Yale Reference Duplicator, and uploaded to Covidence [covidence.org] for screening. Four screeners (EC, MR, JY, and LM) independently reviewed titles and abstracts with 50% overlap to ensure that articles met the following inclusion criteria at the title and abstract screening phase: (a) included adults over the age of 18, (b) contained data from Service Members or Veterans, (c) included a U.S. sample, and (d) referenced IPV. Conflicts were resolved through routine meetings to establish consensus. The following exclusion criteria were introduced at the full-text phase: (e) does not measure IPV specifically, (f) does not have data measuring both IPV use and experience during an overlapping time period, (g) does not reference or report results on bidirectional IPV, including associations between IPV use and experience (e.g., correlations), rates of bidirectional IPV, or qualitative results on bidirectional IPV at least once in either text, figures, or tables.
After two rounds of piloting the extraction tool, four independent raters worked in pairs to review full text articles selected for data extraction. Raters entered information into an Excel spreadsheet related to study sample, demographics, measures of and types of IPV assessed, operationalization of bidirectional IPV, rates of bidirectional and unidirectional IPV, and/or correlates or predictions of bidirectional IPV reported in the study. Discrepancies were resolved by meetings in which the articles were reviewed to establish consensus. Final extraction codes were established and entered the final scoping review table. Raters recused themselves from reviewing and extracting articles that they contributed to.
Results
As reported in Figure 1, the final search yielded a total of 1,748 results. Yale Reference Duplicator identified 711 duplications that were removed prior to uploading citations to Covidence [covidence.org] for screening. Covidence detected and removed an additional 15 articles, yielding a total of 1,022 citations for abstract and title review. After removing 972 articles at the abstract and title review stage, 50 articles underwent full-text review, and 22 were included for extraction. Three studies (Portnoy et al., 2024; Stover et al., 2025; Warren et al., 2024) used data from the same parent study; Cigrang et al. (2023) and Snyder et al. (2025) used data from a different parent study. Portnoy et al. (2024) and Stover et al. (2025) yielded redundant information (i.e., estimates of IPV were based on the same sample, measures, and timepoints). Portnoy et al. (2024) and Stover et al. (2025) were therefore treated as a single study and combined into a single row in Table 1 due to substantial overlap, yielding a total sample of 21 studies (see Supplemental Table 2 for studies excluded at the full-text stage). All studies were published in peer-reviewed journals, with the exception of Melvin (2011), which was a dissertation published through a university library (see Supplemental Table 3 for narrative appraisal).
PRISMA 2020 flow diagram for scoping reviews.
Summary of Extraction Results (n = 21).
Note. SM = Service Members; P = partner; V = Veteran; NR = not reported; NS = not specified; N/A = not applicable, AA = African American; NA = Native American; AI/AN = American Indian/Alaska Native; PI = Pacific Islander; * = asked separately; ** = rate calculated from sample. Racial and ethnic categories in the above table reflect language used by authors in their original publication.
CTS = Conflict Tactics Scale; E-HITS = Extended-Hurt/Insult/Threaten/Scream; IJS = intimate justice scale; IPV = Intimate Partner Violence; RVUES = Relationship violence use and experience screener; WEB = Women’s Experience of Battery; OIF/OEF = Operational Iraqi Freedom and Operation Enduring Freedom.
Of the 21 studies included in the review, six included samples of Active Duty Service Members, National Guard Service Members, or spouses of Active Duty Service Members. Fourteen studies were of Veterans only, with the remaining study including both Service Members and Veterans (Melvin, 2011). Sample sizes ranged from 40 (Frey et al., 2011) to 6,063 (Rabenhorst et al., 2012). Most studies (16 of 21; 76.2%) were correlational in design, one was mixed methods and correlational (Melvin, 2011), and one used a quasi-experimental design (Hayes et al., 2015). Among the three studies containing longitudinal data, two contained IPV data from more than one time point (Krauss et al., 2024; Portnoy et al., 2020), and the third study examined temporal ordering of combat deployment in relation to rate ratios of IPV incidents (Rabenhorst et al., 2012). Most studies included convenience (n = 11, 52.4%) or clinical (n = 5, 23.8%) samples. One study was limited to couples with IPV (Rabenhorst et al., 2012), while the remaining 20 studies included participants with and without IPV use and experience. Three studies contained data on IPV-related injury: one classified injuries into mutually exclusive categories based on degree of severity (mild, moderate, or severe; Rabenhorst et al., 2012); another eliminated injury from its analyses due to low prevalence (1.9% in Creech et al., 2017); and the final study identified injury rates of 9.5% to 12.4% among Veterans with substance use disorders (Anderson et al., 2017). No other indicators of IPV severity were used in these studies.
Measurement and Conceptualization
Studies varied in their measurement and conceptualization of bidirectional IPV. Most studies used a version or adaptation of the Conflict Tactics Scale (CTS or CTS-2; Straus et al., 1996; n = 12; 57.1%), with remaining studies using a version or adaptation of the Extended Hurts, Insults, Threatens, Screams (E-HITS; Chan et al., 2010) known as the Relationship Violence Use and Experience Screener (RVUES, Portnoy et al., 2023; n = 2; 9.5%), Abusive Behavior Inventory (Shepard & Campbell, 1992; n = 1; 4.8%), Women’s Experience of Battery (WEB; Smith et al., 1995; n = 1; 4.8%), Intimate Justice Scale (IJS; Jory, 2004; n = 1; 4.8%), a brief researcher-generated screener (Heyman et al., 2013; n = 1; 4.8%), archival data of official reports of IPV (n = 1; 4.8%), or a combination of the items used on the CTS or CTS-2 (Straus et al., 1996) and E-HITS (Chan et al., 2010; n = 2; 9.5%). Regarding timeframe, studies commonly asked about IPV in the past year (n = 8; 38.1%), followed by past 6 months (n = 6; 28.6%), an unspecified period of time (n = 3; 14.3%), past 3 months (n = 1; 4.8%), and multiple timepoints in a longitudinal design (i.e., past 6 months and past 18 months in Portnoy et al., 2020; past 6 months and past 2 months in Krauss et al., 2024; and past year and lifetime in Gerlock et al., 2016). All studies used self-reported IPV data except for Rabenhorst et al. (2012), which used data from a clinical database. Nearly half (n = 9) of studies used dyadic data.
Studies varied in their approaches to reporting on bidirectional IPV. Eight studies used the term bidirectional IPV or bidirectional aggression, three referred to bidirectional IPV as reciprocal violence or reciprocal aggression, and four used the term mutual violence or mutual IPV. Two studies instead described the phenomenon (“two couples were determined to engage in situational couple violence,” [Gerlock et al., 2016, p. 674] “there were robust links between the perpetration of both psychological and physical aggression by Veterans and their loved ones” [Hayes et al., 2015, p. e777]). The remaining four articles displayed either correlations or prevalence rates for bidirectional IPV in tables but did not discuss it anywhere in the manuscript.
Most studies reported on the prevalence of bidirectional IPV or correlated IPV use with IPV experience. Nine studies (42.9%) reported correlations only, six (28.6%) reported only on prevalence rates of bidirectional IPV, five (23.8%) reported both prevalence rates and correlations, and one study had researchers qualitatively determine the number of cases that had mutual IPV. These studies correlated either frequencies of self-reported IPV use with self-reported IPV experience or used dyadic data to correlate frequencies of IPV use and IPV experience across partner dyads.
Among 11 the studies that measured prevalence of bidirectional IPV, six studies (54.5%) provided an overall rate of bidirectional IPV that included more than one subtype of IPV (see Figure 2). Seven studies reported on the prevalence of at least one specific subtype of bidirectional IPV, including bidirectional psychological IPV (n = 6; 54.5%), bidirectional physical IPV (n = 6; 54.5%), and bidirectional sexual IPV (n = 3, 27.3%). The study that used qualitative raters to assess mutuality of IPV reported on cases where bidirectional IPV appeared to be equal among the partners and did not report on an overall rate of bidirectional IPV (Gerlock et al., 2016). Among the 14 studies that reported correlations, six (42.9%) leveraged dyadic data to examine the correlation of the use of IPV by Service Members or Veterans with the use of IPV by their partner, six (42.9%) measured the correlation between the Service Member or Veteran’s self-reported use and experience of IPV. Two (14.3%) reported on the correlation between the partner’s self-reported use and experience of IPV.
Rates of bidirectional IPV (overall) by study and military affiliation.
In the nine studies in which both members of a couple reported on IPV, four studies (44.4%) used IPV data from the participants’ self-report of their own behavior, two (22.22%) used their partner’s report of participants’ IPV use, two (22.22%) used the highest rating of IPV reported by either partner, and one (11.1%) used a qualitative judgment determined by the researchers. Out of the full sample of 21 studies, 11 (52.3%) used self-reported IPV data from a single reporter, nine studies (42.8%) had IPV data from Veterans or Service Members only, and two studies (9.5%) had IPV data from partners only. Among the nine studies where only Service Members or Veterans (not partners) reported on IPV, authors specified that participants reported on IPV in their current relationship in only one study (Creech et al., 2017). In three studies with military samples, it appeared likely that participants were reporting on their current relationship based on their marital status, length of relationship, and timeframe of the questionnaire (Cigrang et al., 2023; Park et al., 2022; Snyder et al., 2025). Rabenhorst et al. (2012) used archival data from IPV incidents that have been substantiated by the Air Force’s Family Advocacy Program (FAP). In the other studies, the authors did not specify whether participants were reporting on a single relationship, leaving open the possibility that participants were reporting IPV use and experience across multiple relationships or partners.
Nine of the studies included only heterosexual participants (n = 7 were explicitly described as heterosexual and n = 2 appeared to be heterosexual based on other contextual information). Eight studies did not provide information on the sexual orientation of participants. Four studies contained data from nonheterosexual participants; one used data from lesbian, gay, and bisexual Veterans only (Warren et al., 2024), while the remaining three studies included nonheterosexual people as a small portion of their samples (Portnoy et al., 2023; Portnoy et al., 2024; Wolf et al., 2013). All studies detailing data from nonheterosexual participants were collected from Veterans, meaning that data from Service Members came from only heterosexual or unspecified samples. Military samples contained data from almost exclusively married participants, meanwhile Veteran samples tended to contain a variety of types of relationships. Most studies (n = 12) did not report the average length of participants’ relationships. Of those that did, mean relationship lengths ranged from 2.1 years (SD = 1.6) in an active-duty Air Force sample (Snyder et al., 2025) to 21 years (SD = 14.6 years) in a clinical sample of VHA enrollees (Gerlock et al., 2016). No studies explicitly described including data from transgender, nonbinary, or gender-diverse individuals or couples.
Bidirectional IPV Among Service Members
Out of the six samples of Service Members, five studies (83.3%) reported correlations and only one study (n = 1; 16.7%) reported a prevalence rate of bidirectional IPV. The single study reporting on prevalence of bidirectional IPV examined archival records of physical or emotional abuse substantiated by the Air Force FAP (Rabenhorst et al., 2012). This study found that 25% of the incidents involved bidirectional IPV; among the 25% of couples with bidirectional IPV, most (82%) engaged in bidirectional IPV on the same day. Among the five studies that reported on correlations between IPV use and experience or each person’s IPV use (Cigrang et al., 2023; Frey et al., 2011; Park et al., 2022; Reddy et al, 2011; Snyder et al., 2025), correlations ranged from .29 (Frey et al., 2011) to .74 (Park et al., 2022). Three studies examined correlations between IPV use and experience self-reported by the same person, which yielded higher correlations (r = .74 among self-reports of Service Members’ female spouses [Park et al., 2022]; r = .57–.67 among Service Members [Cigrang et al. 2023]; r = .59 among Service Members [Snyder et al., 2025]) than those correlated across partner dyads (i.e., correlated each other’s IPV use across partner dyads; r = .29–.55 in Frey et al., 2011 and Reddy et al., 2011, respectively). Within the study examining correlations among subtypes of IPV, correlations were higher within the same IPV subtype (r = .55 for psychological IPV use and .44 for physical IPV use; Reddy et al., 2011) than between different IPV subtypes (r = .41 between physical and psychological IPV use; r = .37 between psychological and physical IPV use; Reddy et al., 2011). Two studies reported correlations for bidirectional physical IPV (r = .44–.67 [Cigrang et al., 2023; Reddy et al., 2011]) and one reported correlations for bidirectional psychological IPV (r = .55; Reddy et al., 2011). Only one study disaggregated IPV experience and IPV use by gender, reporting slightly higher correlations among men (r = .67) than women (r = .57; Cigrang et al., 2023).
Using data from Air Force personnel who experienced at least one combat-related deployment between 2001 and 2008, Rabenhorst et al. (2012) identified lower rates of bidirectional IPV postdeployment (Rabenhorst et al., 2012). Relative to predeployment, having a husband on active duty, mild abuse, and lack of alcohol consumption at the time of the incident was associated with lower postdeployment bidirectional IPV. Lack of alcohol consumption at the time of the incident was associated with lower rates of bidirectional IPV incidents following a deployment regardless of severity of incident (mild or moderate/severe abuse).
Bidirectional IPV Among Veterans
Among the 14 studies of Veterans, four studies (28.6%) reported on the prevalence of bidirectional IPV only, four (28.6%) reported only correlations, and five (35.7%) reported both prevalence rates and correlations. In total, nine studies (64.3%) reported at least one prevalence rate. Four studies disaggregated bidirectional prevalence rates by IPV subtype, showing that rates varied from 1.0% to 9.8% for bidirectional sexual IPV (Creech et al., 2017; Portnoy et al., 2024; Warren et al., 2024), 3.5% to 26.2% for bidirectional physical IPV (Creech et al., 2017; Dutra et al., 2012; LaMotte et al., 2015; Portnoy et al., 2024; Tharp et al., 2016; Warren et al., 2024), and 28.3% to 94% for bidirectional psychological IPV (Creech et al., 2017; Dutra et al., 2012; LaMotte et al., 2015; Portnoy et al., 2024; Warren et al., 2024). When assessing overall bidirectional IPV during the same timepoint, prevalence rates ranged from 28.4% to 66.9% (Portnoy et al., 2024 and Krauss et al., 2024, respectively). In the one study that assessed prevalence of bidirectional IPV using more than one timepoint, Portnoy et al. (2020) reported that 16% of women who reported IPV use also reported IPV experience either at the same timepoint or the prior timepoint 6 months earlier; among women who used IPV at T3, all but one (96.8%) had IPV experience across timepoints (i.e., had either IPV experience concurrently [i.e., at T3] or in the prior 6 months [i.e., at T2]). One final mixed-methods study divided people into groups based on consensus upon reviewing recorded interviews (Gerlock et al., 2016). Gerlock et al. (2016) identified that 2 out of 441 couples engaged in “situational couple violence,” defined as situations where there was no primary aggressor, although they did not report the overall number or percentage of cases where both members engaged in IPV.
Among the nine studies reporting on correlations, correlations between IPV use and experience ranged from 0.07 to 0.91 (Anderson et al., 2017; Creech et al., 2017; Dutra et al., 2012; Hayes et al., 2015; Kelley et al., 2017; Krauss et al., 2024; LaMotte et al., 2015; Portnoy et al., 2020; Wolf et al., 2013). Similar to findings among Service Members, correlations were higher within the same IPV subtype than between different IPV subtypes (r = .71–.88 for the same IPV subtype and r = .21–.45 across different IPV subtypes [Creech et al., 2017]; r = .74–.76 for the same IPV subtype, r = .35–.40 across different IPV subtypes [LaMotte et al., 2015]; r = .64–.75 for the same IPV subtypes, r = .43–.44 across different IPV subtypes [Dutra et al., 2012]; r = .53–.91 for the same IPV subtypes, r = .34–.55 across different IPV subtypes [Hayes et al., 2015]). One exception to this was Anderson et al., (2017) who reported an overall high correlation (r = .90) for overall IPV experience and use, yet found a lower correlation between physical IPV experience and use (r = .66) than between physical IPV use and injury experience (r = .75). As the only study to report correlations between injury experience and IPV subtype, there was no way to determine if that finding was related to the specific relationship between physical assault and injury experience. Additionally, one study reported low correlations between Veteran and spouse reports of the same IPV subtype (r = .07 and .18 for psychological and physical IPV use, respectively; Wolf et al., 2013), suggesting that that while correlations between the same IPV subtype may generally be higher than correlations among different IPV subtypes, it does not mean the correlations among Veterans’ and partners’ reports of IPV are always high.
Although most studies were cross-sectional, two studies of Veterans reported correlations between IPV use and experience at different time points. Hayes et al. (2015), in a treatment study for IPV, found that magnitude of correlations between use and experience among the same subtype of IPV cross-sectionally were higher (r = .53–.91) than were correlations of the same subtype of IPV across different timepoints (r = .11–.50). In some instances, correlations were negative upon successful completion of a program designed to reduce IPV use (e.g., −.30 between Veteran physical aggression 6 months into treatment and partner physical aggression 3 months after completing treatment). Portnoy et al. (2020) instead found a correlation of .49 between self-reported IPV use at one timepoint (i.e., T2) and self-reported IPV experience in a subsequent wave (i.e., T3, 6 months after T2), which is generally lower than the cross-sectional correlations reported above.
Bidirectional IPV was common among Veterans. Tharp et al. (2016) reported that Veterans with bidirectional IPV also had higher frequencies of IPV than those with unidirectional IPV. Creech et al. (2017) documented bidirectional psychological IPV as the most common pattern among female Veterans. Three studies reported findings that hinted at possible self-defense theories of bidirectional IPV. LaMotte et al. (2015) found that when examining multiple variables in regression analyses, the partners’ IPV use was the only unique predictor of Veterans’ IPV use. Similarly, Dutra et al. (2012) reported that male physical IPV use was the only significant predictor of female physical IPV use, and male psychological IPV use was one of only two predictors of female psychological IPV use. Examining both qualitative and quantitative data, Gerlock et al. (2016) reported that in most instances, women’s physical IPV use was in response to men’s violence toward them.
Bidirectional IPV Among Service Members and Veterans
Melvin (2011) was the only study containing data from Service Members and Veterans, although their results were aggregated by current military affiliation. Melvin (2011) collected self-report data on psychological IPV experience from both partners, identifying bidirectional psychological IPV in 3.75% of couples.
Discussion
This scoping review synthesized 21 articles on bidirectional IPV in military and Veteran populations, reported on the current state of the literature, and examined rates and correlates of bidirectional IPV disaggregated by military affiliation. Findings affirmed the need for continued research on bidirectional IPV in military and Veteran populations, ideally with data from Service Members and Veterans in the same study to reduce heterogeneity attributable to other factors such as differences in sampling, measurement, and conceptualization (see Table 2 for critical findings). Although all Service Members eventually separate from military service and transition into Veteran status, Service Members and Veterans are qualitatively different from each other (Cameron, 2023). Disaggregating rates and patterns of IPV by current military affiliation may provide informative cues for understanding risk factors unique and specific to Service Members and Veterans which, in turn, may inform tailored approaches to treatment and prevention.
Critical Findings.
Most studies in this review documented bidirectional IPV as the most common pattern of IPV. Among studies reporting rates of bidirectional IPV at a single timepoint, overall rates of bidirectional IPV—endorsing at least one type of IPV use and experience among studies measuring more than one subtype of IPV— ranged from 25% (Rabenhorst et al., 2012) to 66.9% (Krauss et al., 2024). When examining bidirectional IPV by subtype, inclusive of studies that either only examined one subtype of bidirectional IPV or disaggregated results by subtype, results ranged from 1.0% for bidirectional sexual IPV (Portnoy et al., 2025) to 94% for bidirectional psychological IPV (LaMotte et al., 2015). Substantial variation in bidirectional IPV has been documented elsewhere in the literature (2%–98.4% as reported by Machado et al., 2024); in the context of the present study, differences in rates of bidirectional IPV may be attributable to factors unrelated to current military affiliation as detailed below, as the only study containing data from both Service Members and Veterans in the same sample (Melvin, 2011) did not disaggregate results by current military affiliation.
Three studies included in the present scoping review documented higher rates of unidirectional IPV, relative to bidirectional IPV. Data from these three studies came from Veteran couples referred to the VA’s Family Mental Health Program for couples’ therapy (Tharp et al., 2016), IPV incidents substantiated by the FAP and documented in the Air Force Family Advocacy System of Records clinical database (Rabenhorst et al., 2012), and couples who self-selected into a study (Melvin, 2011). Johnson (2017) similarly documented higher rates of unidirectional IPV (i.e., IT in his typology) in clinical and legal samples such as those presenting for IPV treatment programs and IPV-related social services. Method factors may alternatively account for higher rates of unidirectional IPV in these three studies, as Melvin (2011) used dyadic data with each partner self-reporting their own IPV experience, Tharp et al. (2016) used dyadic data with each partner self-reporting their own IPV use, and Rabenhorst et al. (2012) used archival data.
Positive correlations between IPV use and experience were consistently documented across studies, except for negative correlations across timepoints in an intervention study designed to decrease IPV use (Hayes et al., 2015). Coefficients ranged from small (i.e., 0.07 in Wolf et al., 2013) to large (i.e., 0.91 in Hayes et al., 2015). Three additional key findings emerged. First, correlations between IPV use and experience were higher in studies using self-report data from the same person, in contrast to studies that correlated partners’ reports of each other’s IPV use, raising the possibility of method effects (Orth, 2013). No studies in this scoping review examined concordance rates or used recommended methods for establishing interpartner agreement such as Kendall’s Tau-b, intraclass correlations, Cohen’s Kappa, or Gwet’s AC1 (Capinha et al., 2024). Nevertheless, using perspectives from both partners and statistical approaches for modeling dyadic data may offer deeper insight into individual perceptions and couple dynamics (Cunha et al., 2025). Second, correlations were generally higher within IPV subtypes than between IPV subtypes. Third, researchers frequently reported zero-order correlations between IPV subtypes, despite substantial overlap (i.e., co-occurrence) between IPV subtypes. For example, Portnoy et al. (2024) identified a latent class of Veterans with bidirectional multiform IPV (i.e., Veterans with high probabilities of psychological IPV abuse or experience in conjunction with either sexual or physical IPV use or experience) that were qualitatively distinct from a latent class of Veterans with bidirectional psychological IPV, underscoring heterogeneity in bidirectional IPV. These findings illustrate the need for future work to model co-occurring forms of bidirectional IPV and to incorporate multimethod designs (i.e., self- and partner reports of IPV) that control for shared method variance in dyadic data (Orth, 2013).
Inconsistencies in measurement, operationalization, and reporting across studies were noted in this scoping review, complicating efforts to draw cross-study comparisons between military and Veteran populations. For example, most studies containing data from Veterans (n = 10; 71.4% of studies on Veterans) measured bidirectional IPV using items from either the CTS or CTS-2, in contrast to 50% (n = 3) of studies on Service Members. Moreover, use of the CTS or CTS-2 were inconsistent, with one study using the CTS (Dutra et al., 2012), others using either select subscales or subsets of items from the CTS-2, and yet another study combining items from CTS and CTS-2 (Tharp et al., 2016). Inconsistencies were also noted with respect to timeframe. Among Service Members, the modal timeframe for measuring IPV was within the past 6 months (n = 3); for Veterans, the modal timeframe (n = 8, 57.1%) was within the past year, presenting Veterans with a larger window of time for self-reporting bidirectional IPV. Rates for bidirectional IPV were only reported in 16.7% of studies (n = 1) containing data from Service Members (Rabenhorst et al., 2012); in contrast, among the 14 studies containing data from Veterans, most (n = 9, 64.3% of studies on Veterans) studies reported on rates of bidirectional IPV. These differences complicate efforts to compare bidirectional IPV rates between Service Members and Veterans as they induce variation in prevalence rates and correlations unrelated to current military affiliation.
Veteran samples included in this review were notably more diverse across several characteristics compared to Service Member samples. As reflected in Table 1, at least 90% of Service Members were married in all but one study (Snyder et al., 2025); among Veterans, only one study contained data from at least 90% of married Veterans (Wolf et al., 2013), and less than 40% of Veterans were married in three samples (Anderson et al., 2017; Portnoy et al., 2023; Warren et al., 2024). Among studies with Service Members that reported on service era, all four indicated that participants served during the post-9/11 era (Cigrang et al., 2023; Rabenhorst et al., 2012; Reddy et al., 2011; Snyder et al., 2025); in contrast, studies containing data from Veterans represented eras spanning from World War II through post-9/11, with seven studies containing data exclusively from Veterans who served during the post-9/11 era (Creech et al., 2017; Kelley et al., 2017; Krauss et al., 2024; LaMotte et al., 2015; Portnoy et al., 2024; Tharp et al., 2016; Warren et al., 2024). All studies containing data on Service Members reported on branch, with each study containing data from a single branch (Air Force: n = 3; Army and/or National Guard: n = 3). Conversely, only 35.7% (n = 5) containing data on Veterans reported branch, all of which contained data from multiple branches (Creech et al., 2017; Gerlock et al., 2016; Hayes et al., 2015; LaMotte et al., 2015; Portnoy et al., 2024).
Among the 21 studies that met criteria for inclusion, the only study containing data from Service Members and Veterans (Melvin, 2011) collapsed all analyses across components (i.e., Active Duty, Reserve, and National Guard) and current military affiliation. This finding highlights a notable gap, as no studies in this review compared bidirectional IPV by current military affiliation with the benefit of data from the same source. As detailed above, factors unrelated to current military affiliation such as cross-study variation in bidirectional IPV conceptualization, bidirectional IPV measurement, and systematic differences in demographics and military characteristics may yield additional heterogeneity when drawing cross-study comparisons between Service Members and Veterans.
Within the context of these limitations, higher rates of overall bidirectional IPV were documented among Veterans (range: 28.4% [Portnoy et al., 2024]–66.9% [Krauss et al., 2024]) relative to Service Members (25%; Rabenhorst et al., 2012). According to Johnson’s typology (2012; 2017), elevated rates of bidirectional IPV among Veterans are suggestive of a larger representation of typologies characterized by bidirectional IPV such as VR, SCV, MVC, or a combination of these typologies. Contextual factors and factors that may lead to escalating violence such as substance use (Creech et al., 2017; Kelley et al., 2017; Rabenhorst et al., 2012), frustration (Park et al., 2022), and communication difficulties (Cigrang et al., 2023) were cross-sectionally associated with bidirectional IPV, meanwhile two studies detailed women in their samples using IPV in response to escalating violence (Dutra et al., 2012; Gerlock et al., 2016). These results are suggestive of SCV or VR; however, VR cannot be distinguished from SCV or MVC without more data on motives, context, progression of IPV across time, and gender symmetry with respect to impact and severity.
Perspectives from military transition theory (Castro & Kintzle, 2014), which proposes individuals experience heightened vulnerability during the military-to-civilian transition, yield plausible explanations for differences in rates of bidirectional IPV by military affiliation. Unlike Veteran families, military families have access to many DoD-sponsored resources and supports designed to promote family resilience, positive coping, and adaptation (Le Menestrel & Kizer, 2019). Loss of these benefits upon separation from military service may lead to unemployment, financial strain, and other related stressors (Castro & Kintzle, 2014) which, in turn, may yield heightened conflict and escalating violence leading to SCV. Alternatively, increased rates of bidirectional IPV among Veterans may instead reflect differences in methods, samples, and measurement across studies, or a reluctance for military couples to disclose IPV due to fear of involuntary separation from military service and loss of related benefits (Kamarck et al., 2019). Future research inquiry with longitudinal data is warranted to better understand the extent to which stressors associated with separation from military service are associated with conflict, escalating violence, and subsequent bidirectional IPV.
Consistent with general populations (Machado et al., 2024; Langhinrichsen-Rohling et al., 2012), bidirectional IPV was common among Service Members and Veterans. Importantly, bidirectional IPV prevalence rates represent only one dimension of bidirectional IPV (i.e., whether bidirectional IPV is present or absent), while correlations represent another (i.e., association between IPV use and IPV experience). Nevertheless, high rates of bidirectional IPV in data from predominately heterosexual couples do not imply equivalency across gender with respect to the outcomes and impact of IPV, or the motivation for using IPV. Gender-based differences in the impact and consequences of IPV have been documented in the literature, with women experiencing more severe forms of violence and higher rates of IPV-related lethality risk and intimate partner homicide compared with men (Caldwell et al., 2012; Langhinrichsen-Rohling et al., 2012; Portnoy et al., 2025). It will be important for future research to examine gender-based differences in bidirectional IPV with respect to impact and severity of violence, as well as the broader context and motives for IPV use.
Limitations, Implications, and Future Directions for Research
This scoping review identified several gaps in the literature. Notably, rates of bidirectional IPV were aggregated by relationship characteristics, race or ethnicity, and military service characteristics, few efforts reported on sexual orientation, and no studies included data from gender-diverse participants. All samples contained data from majority-White participants, with exception a study containing data from substantiated instances of domestic violence (Rabenhorst et al., 2012). The few studies with data from participants in same-sex relationships (Wolf et al., 2013) or members of the LGBTQ+ community (Portnoy et al., 2020, 2024; Warren et al., 2024) came exclusively from Veterans, presumably because of DoD restrictions on collecting data on sexual orientation (Watkins, 2022). Future efforts may address these gaps by collecting data from members of the LGBTQ+ community and disaggregating analyses by sexual orientation and gender, which is critical to meeting the needs of a military more diverse than the general U.S. population with a disproportionately large number of LGBTQ+ individuals (Kamarck, 2019).
Despite the relevant contributions of this study, there are inherent limitations. Initially, 1,748 articles were selected for this scoping review. Of these, only 22 studies representing 21 unique data sources met the inclusion criteria for extraction, most of which contained data from convenience samples (Supplemental Table 3). Overall rates of bidirectional IPV—defined as containing more than one subtype of IPV—were reported in only six articles. In total, 11 articles reported at least one rate of bidirectional IPV, inclusive of overall rates or rate(s) for at least one subtype, four of which also reported on correlations between IPV use and experience. This is in itself a limitation, as literature on bidirectional IPV in military and Veteran populations is scarce, raising the potential for limited generalizability and underscoring the need for more research on bidirectional IPV among Service Members and Veterans. In contrast to prior reviews (Langhinrichsen-Rohling et al., 2012; Machado et al., 2024), the present review was restricted to studies containing data from U.S. Service Members and Veterans, therefore yielding policy implications for the DoD and VHA at the expense of applicability to other countries. Further, findings from this study underscore the need for future research to thoroughly examine the context and motives for bidirectional IPV among Service Members and Veterans, as these factors are crucial for understanding bidirectional IPV, developing effective interventions, and making useful policy recommendations (Johnson, 2006).
Implications for research, policy, and practice are summarized in Table 3. These results highlight the need for studies to collect data from Service Members and Veterans participating in the same study to minimize heterogeneity attributable to differences in operationalization, conceptualization, and sampling. Moreover, research on risk markers for bidirectional IPV may guide the identification of risk and protective factors for bidirectional IPV which, in turn, may inform initiatives to prevention. Such efforts are particularly timely, as the DoD recently identified IPV as a priority target in its integrated primary prevention initiative, which has the overarching goal of preventing harmful behaviors by reducing risk factors and bolstering protective factors (Department of Defense, 2022). Finally, guidelines and recommendations for standard approaches to measuring and conceptualizing bidirectional IPV, perhaps through expert consensus processes such as those established by the National Academies of Sciences, Engineering, and Medicine, are essential to ensuring comparable prevalence rates across samples containing data from Service Members and Veterans. Without standardized practices, it remains unclear whether differences in rates of bidirectional IPV reflect true differences across samples.
Implications for Policy, Practice, and Research.
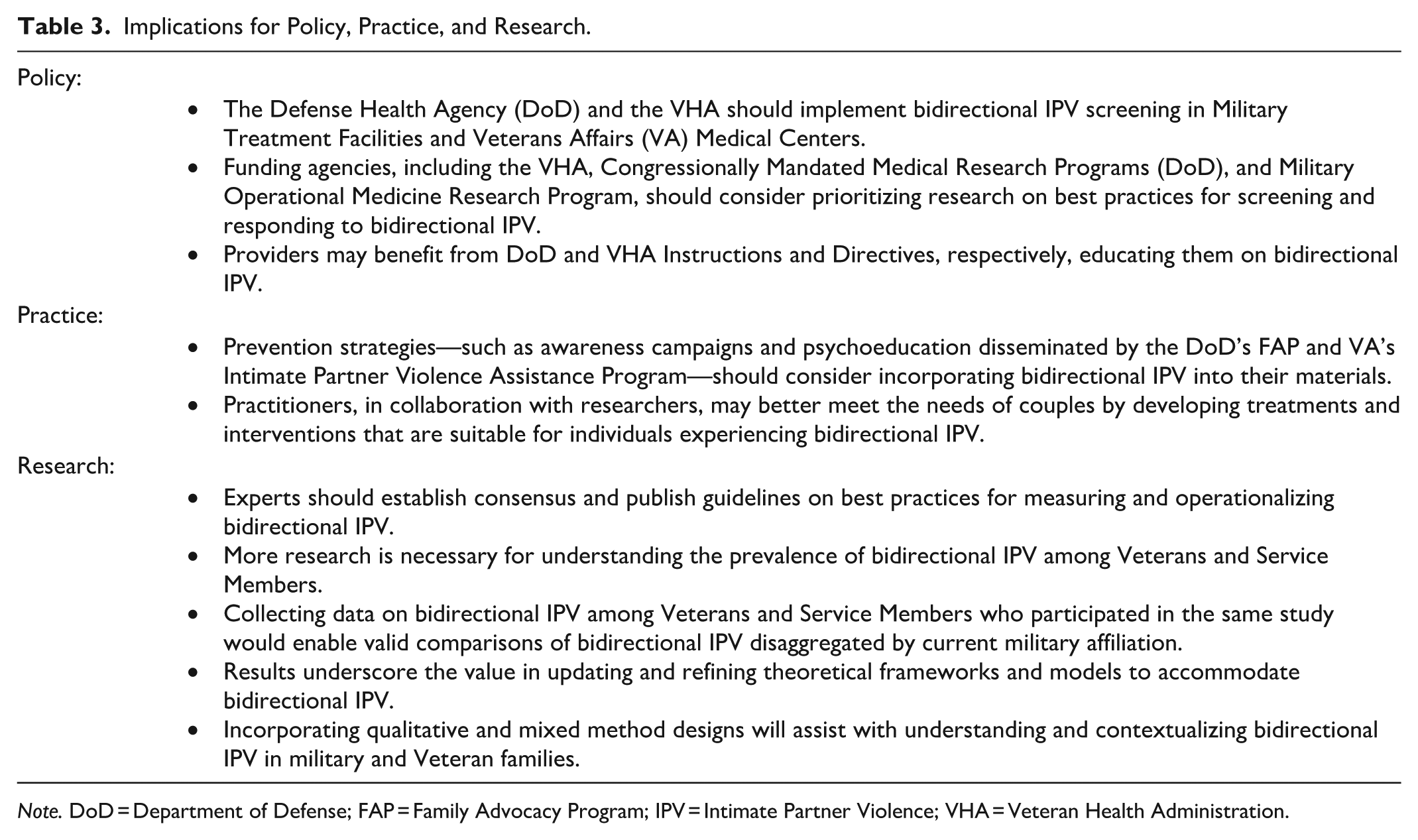
Note. DoD = Department of Defense; FAP = Family Advocacy Program; IPV = Intimate Partner Violence; VHA = Veteran Health Administration.
These findings also support the need to screen for both IPV use and IPV experience in military treatment facilities and VA medical centers. To date, the Department of Veterans Affairs (2024) and DoD (Defense Health Agency, 2025) provide guidance for practitioners to screen for IPV experience only. Formal adoption of bidirectional IPV screening and connection to care via VA directives and DoD instructions, paired with appropriate clinical training and education from the VA’s IPVAP and DoD’s FAP, would assist the VHA and DoD’s clinical workforce with identifying and treating Service Members and Veterans with bidirectional IPV. Awareness campaigns sponsored by the DoD’s Office of Military Community & Family Policy and IPVAP, in collaboration with researchers with expertise in IPV, may serve to challenge misconceptions and stereotypes about IPV. Finally, enhanced coordination across agencies through integrated electronic health records, paired with warm handovers between FAP and IPVAP, may assist with prevention by sooner connecting Veterans with a history of IPV who have recently separated from military service with appropriate support, services, and resources.
In summary, studies from this review contained high rates of bidirectional IPV among Service Members and Veterans, although none of the identified studies disaggregated rates of bidirectional IPV by current military affiliation. Substantial inconsistency in measurement, operationalization, and reporting of bidirectional IPV, in addition to systematic differences between Service Members and Veterans with respect to demographics and military service characteristics, complicated efforts to draw cross-study comparisons. Results highlight the need for standardized approaches to operationalization and measurement and enhanced representation of minorized Service Members and Veterans.
Supplemental Material
sj-docx-1-tva-10.1177_15248380251408371 – Supplemental material for Bidirectional Intimate Partner Violence Among Service Members and Veterans: A Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380251408371 for Bidirectional Intimate Partner Violence Among Service Members and Veterans: A Scoping Review by Elizabeth C. Coppola, Mark R. Relyea, Julie Yeterian, Lauren DeMoss, Galina A. Portnoy, Cynthia Brandt and Carla Smith Stover in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors would like to acknowledge Melissa C. Funaro, MS, MLS, Clinical Research & Educational Librarian of the Cushing/Whitney Medical Library for her support with database searches, Covidence support, and citation chaining.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a VA HSR Career Development Award (CDA 19-234) and by the IPV Center for Implementation, Research, and Evaluation. Dr. Coppola’s time was supported by the Advanced Fellowship in Medical Informatics through the VA Office of Academic Affiliations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The opinions expressed here are those of the authors and do not represent the official policy or position of the U.S. Department of Veterans Affairs nor the U.S. government. The funding sources had no involvement in the study design, analyses, article preparation, or decision to submit.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.