
Abstract
Those who have served in the military are at heightened risk for intimate partner violence (IPV), defined as threatened or actual physical, sexual, or psychological abuse from a current or former romantic partner, relative to the general population. However, no known efforts have compared patterns of IPV use (i.e., perpetration) and IPV experience (i.e., victimization) disaggregated by current military affiliation (i.e., service member or veteran), nor have they compared patterns of unidirectional IPV (either IPV use or experience only) versus bidirectional IPV (i.e., concurrent IPV use and IPV experience) by military affiliation. Using dyadic data from United States service members, veterans, and their spouses who participated in the Millennium Cohort Family Study—the only Department of Defense-wide longitudinal study on military families—we compared rates and frequencies of IPV use, IPV experience, and IPV patterns between service members (n = 2,301) and veterans (n = 1,877). An estimated 37.6% of service members and 47.9% of veterans had any IPV experience; 36.4% of service members and 50.8% of veterans had any IPV use. Veterans had higher rates of IPV experience (adjusted odds ratio [aOR]: 1.43; 95% confidence interval [CI] [1.10, 1.85]) and IPV use (aOR: 1.67; 95% CI [1.29, 2.18]). After adjusting for bidirectionality, veterans had higher rates of bidirectional IPV (aOR: 1.62; 95% CI [1.22, 2.15]) and IPV use (aOR: 2.19; 95% CI [1.29, 3.27]), but not IPV experience. Veterans had an increase in the expected frequency of IPV experience by 47% (adjusted incidence rate ratios [IRR] = 1.47; 95% CI [1.19, 1.81]) and IPV use by 65% (IRR = 1.65, 95% CI [1.35, 2.00]), relative to service members. These findings underscore the value of investment in IPV prevention and treatment upon separation from military service, and the need for targeted programming and resources to address bidirectional IPV among both partners in a dyad.
Keywords
Introduction
Intimate partner violence (IPV) is a pervasive public health challenge defined as threatened or actual physical, sexual, or psychological abuse from a current or former romantic partner. IPV has been linked to adverse physical and mental health outcomes including depression, anxiety, posttraumatic stress disorder (Spencer et al., 2019), severe chronic pain (Walker et al., 2022), and poor physical health (Spencer et al., 2022). Accumulating evidence from predominately United States samples suggests that IPV may be more prevalent and severe among those who have served in the military, relative to civilians (Trevillion et al., 2015), with rates of IPV use and IPV experience 2.17 and 4.2 times higher than civilians, respectively (Cowlishaw et al., 2022). Meta-analyses hint at higher rates of IPV among veterans (Cowlishaw et al., 2022; Gierisch et al., 2013), although no known efforts have directly compared rates of IPV between service members and veterans, nor have they accounted for bidirectional IPV (i.e., the co-occurrence of IPV use [perpetration] and IPV experience [victimization])—the most common pattern of IPV (Machado et al., 2024). To address this gap, we use data from the Millennium Cohort Family Study—the only Department of Defense (DoD)-wide longitudinal study on military families—to examine IPV by current military affiliation (service members vs. veterans), drawing comparisons between IPV rates, frequencies, and patterns (i.e., unidirectional IPV use, unidirectional IPV experience, and bidirectional IPV).
Rates and Patterns of IPV Among Service Members and Veterans
Efforts to disaggregate results from meta-analyses by current military affiliation revealed concerningly high rates of IPV among veterans, relative to service members. Past-year prevalence rates have ranged from 5.2% to 22% among service members (Cowlishaw et al., 2022; Gierisch et al., 2013), compared with 31.8% among veterans (Cowlishaw et al., 2022), for IPV use, whereas past-year IPV experience prevalence rates have ranged from 13.3% to 30% among service members (Cowlishaw et al., 2022; Gierisch et al., 2013), compared with 24.3% to 35% among veterans (Cowlishaw et al., 2022; Gierisch et al., 2013). These findings suggest elevated rates of IPV use and experience among veterans, although there have been no known efforts to directly compare rates or patterns of IPV between service members and veterans using data from the same sample.
Both past and recent evidence demonstrates that bidirectional IPV may be the most common pattern of IPV in civilian (Langhinrichsen-Rohling et al., 2012; Machado et al., 2024), veteran (Portnoy et al., 2023), and military (MacManus et al., 2022) samples. When screening for IPV experience and IPV use concurrently within a sample of treatment-seeking veterans, Portnoy et al. (2023) found that patients were significantly more likely to endorse past-year bidirectional IPV than endorsing unidirectional IPV experience or IPV use. Additionally, McManus et al. (2022) documented high rates of bidirectional IPV among UK service members, identifying 52.7% of service members who reported IPV use also experienced at least one form of IPV. To date, no known efforts have compared rates of bidirectional IPV between service members and veterans, even though high rates of either IPV use or IPV experience within a group or subpopulation may ultimately be driven by bidirectional IPV.
Theoretical Perspectives on Military Life and the Military-to-Civilian Transition
Stressors associated with military life and heightened vulnerability among veterans, particularly during the military-to-veteran transition period (i.e., military transition theory; Castro & Kintzle, 2014; Kintzle & Castro, 2018), have been theorized to contribute to elevated rates of IPV among U.S. service members and veterans (National Academies of Sciences, Engineering, and Medicine [NASEM], 2019). Service members and their families contend with challenges such as deployment-related separation, reintegration stress (Willerton et al., 2010), combat-related mental or physical injuries, frequent relocations, and high levels of work–family–conflict (NASEM, 2019) during military service. These stressors have been theorized to contribute to maladaptive responses such as IPV when families are overwhelmed, highly reactive, or exhibit deficits in coping skills and resources (NASEM, 2019). The DoD provides service members and their families with many benefits and resources designed to buffer the impact of stressors associated with military life, such as employment support, housing, medical care, and childcare (Castro & Kintzle, 2014; NASEM, 2019). However, these benefits are lost upon separation from military service, leading to additional strain and stress during the critical veteran transition period, potentially yielding heightened vulnerability among couples who recently transitioned to veteran status (Castro & Kintzle, 2014; Kintzle & Castro, 2018).
The Present Study
Relatively little is known about differences in rates of IPV use, IPV experience, and bidirectional IPV among military versus veteran families. Whereas results from meta-analyses suggest elevated rates of any IPV use and any IPV experience among veterans relative to service members (Cowlishaw et al., 2022; Gierisch et al., 2013), no known studies have verified this using data collected from both service members and veterans. Further, no known studies have compared rates of bidirectional IPV between service members and veterans in the same sample nor have they examined rates of IPV use and IPV experience after adjusting for bidirectionality. Using self-report data from a large cohort of military and veteran couples, we hypothesized that (H1) veterans would have higher rates of IPV use and (H2) higher rates of IPV experience, relative to service members. We also hypothesized that veterans would have higher frequencies of IPV use and experience (H3) and higher rates of bidirectional IPV (H4), relative to service members.
Method
Data for the present study were drawn from the Millennium Cohort Program (MCP), comprising the Millennium Cohort Study (MCS; service members), the Millennium Cohort Family Study (Family Study; military spouses), and the Millennium Cohort Study of Adolescent Resilience (SOAR; military affiliated adolescents aged 11–17). The MCS is the largest of these program components, with five panels of U.S. service members recruited between 2001 and 2021. MCP recruits new participant panels from Defense Manpower Data Center (DMDC) rosters, randomly sampling currently serving, junior military (2–5 years of service) personnel and their families. Participants in each panel are invited to complete follow-up surveys every 3 to 5 years over their life course (Castañeda et al., 2023).
The present study used data from service members enrolled in MCS Panel 4 (2011–2013) and their spouses who were invited contingently to participate in Panel 1 of the Family Study (N = 9,872). Survey data from the second follow-up (2019–2021) period for these participant panels were primarily utilized, by which time substantial numbers had already transitioned out of service since their enrollment. Participants were excluded from analyses if they did not respond to the follow-up survey (n = 5,694), were divorced or widowed prior to the completion of the second follow-up survey (n = 499), or did not complete the IPV measure (n = 367). The final analytic sample consisted of data from 3,312 couples (veterans, n = 1,381; currently serving, n = 1,931; n = 6,624 individuals).
Data from married service members and their spouses both enrolled respectively into the MCS and into the Family Study were linked for analysis in the present study. Using integrated self-report survey data, as well as archival military personnel and medical records, the Family Study makes it possible to analyze interdependent relational outcomes. Further facilitating the objectives of this study, a self-report measure of IPV use and experience was added to the Family Study surveys at the time of the 2019 to 2021 data collection period (i.e., Panel 1, second follow-up, and Panel 2, baseline).
All data were collected under an approved human subject protection protocol (NHRC.2015.0019), with the informed consent of all volunteering service members and spouses prior to data collection. The Naval Health Research Center Institutional Review Board approved the primary study protocol in accordance with applicable federal regulations governing the protection of human subjects. The VA Connecticut Healthcare System Research Office further reviewed and approved procedures for secondary analyses of these data (VACHS IRB 1791582-1).
Measures
Covariates
We used data from personnel files maintained by the DMDC to determine service members’ sex, age, race and ethnicity, branch, rank, and component. Spouses self-reported their age, race and ethnicity, number of children from current or prior relationships, combined household income, and their military background (veteran, currently serving, civilian). Service members and spouses self-reported their educational attainment and employment status in the second follow-up survey.
Current Military Affiliation
DMDC archival data were used to determine whether participants had separated from military service prior to completing the second follow-up survey.
Intimate Partner Violence
IPV was measured using a modified version of the Relationship Violence Use and Experience Screener (RVUES; Portnoy et al., 2023), which contains four items to measure psychological and physical IPV use, and four items to measure psychological and physical IPV experience, with items presented in pairs (e.g., “you screamed or cursed at your partner” followed by “your partner screamed or cursed at you”). The RVUES includes the Extended Hurt/Insult/Threaten/Scream (E-HITS) tool to screen for IPV experiences (Chan et al., 2010; Iverson et al., 2015; Sherin et al., 1998) and the Modified E-HITS tool to screen for IPV use (Portnoy et al., 2018). Respondents were asked to report on IPV experience and IPV use within the past 6 months on a 5-point scale ranging from 1 (never) to 5 (frequently). For the Family Study, the RVUES wording was modified to refer more specifically to IPV events involving participants’ military or veteran spouses. Responses were coded to identify specific forms of IPV as outlined below.
Any IPV Use and IPV Experience
Two dichotomous indicator variables were developed identifying any IPV use and the other any IPV experience, respectively (1 = yes, 0 = no). Response values above 1 (never) for IPV use and IPV experience on the modified version of RVUES were used to indicate IPV use or IPV experience, respectively.
IPV Frequency
Responses across four types of behaviors considered on the RVUES were summed separately for IPV use and experience to generate two variables, one reflecting frequency of IPV use and another indicating frequency of IPV experience. Summed scores were recoded so that “0” reflected no IPV use or IPV experience and higher values reflected more frequent IPV.
IPV Pattern
Responses from the modified RVUES were used to create four mutually exclusive categories: bidirectional IPV, unidirectional IPV use (i.e., IPV use only), unidirectional IPV experience (i.e., IPV experience only), and no IPV (reference).
Analytic Strategy
We first examined weighted descriptive statistics to assess rates of IPV by military affiliation. Weighted chi-squared tests and regressions were then used to examine significant differences between current military affiliation and IPV use, IPV experience, IPV experience frequency, IPV use frequency, and IPV pattern. Subsequently, we conducted a series of separate weighted multiple logistic regression models—with and without adjustment for other demographic covariates—to further estimate the effect size of associations between military affiliation with any IPV use and any IPV experience.
We used weighted negative binomial regression (NBR) to examine the association of military affiliation both with frequency of IPV use and frequency of IPV experience. Analyses were conducted with and without adjustment for demographic covariates. NBR is a generalization of Poisson regression that accommodates over-dispersion by relaxing the assumption that variance is equal to the mean by modeling over-dispersion and is robust to distributional misspecification (Long & Freese, 2006). NBR was appropriate for modeling count data in the present study because these data were over-dispersed (i.e., the variance of IPV experience frequency and IPV use frequency was greater than its means) and lacked justification for zero inflation in which excess zeros otherwise would have been generated by a process separate from count values (i.e., the RVUES were administered only to spouses who were currently married, meaning that zero values reflected no IPV). Statistically, NBR was further justified over other count models based on residual plots, lower Akaike information criteria values, and lower Bayesian information criteria values. Finally, we examined results from unadjusted versus adjusted multinomial logistic regression to estimate associations between military affiliation and IPV pattern, comparing the likelihood of unidirectional IPV experience, unidirectional IPV use, and bidirectional IPV to the reference group of no IPV. We report models with percent change in expected frequency of IPV and incidence rate ratios (IRRs) for the negative binomial portion, the latter of which represents the ratio of incidence (frequency) of IPV among veterans to the incidence (frequency) of IPV among service members, adjusted for covariates. Adjusted odds ratios (aORs) are reported for the logit portion. All descriptive statistics and analytic models were conducted in Stata/MP 18 and weighted to adjust for nonresponse using the methods documented by Corry et al. (2017).
Results
The modal group of service members and veterans were male (86.1%), White non-Hispanic (69.1%), had some college experience (47.4%), and were employed full time (91.6%). Most spouses had no military experience (80.1%), were White non-Hispanic (71.9%), had some college experience (43.4%), and were either employed full time (44.3%) or unemployed (42.4%). Service members and veterans did not differ by race, number of children in the household, or income. Relative to veterans, a significantly larger percentage of service members were male, officers (as opposed to enlisted), and serve on active duty (as opposed to National Guard or Reserve; see Table 1).
Weighted Demographics and Differences by Military Affiliation.
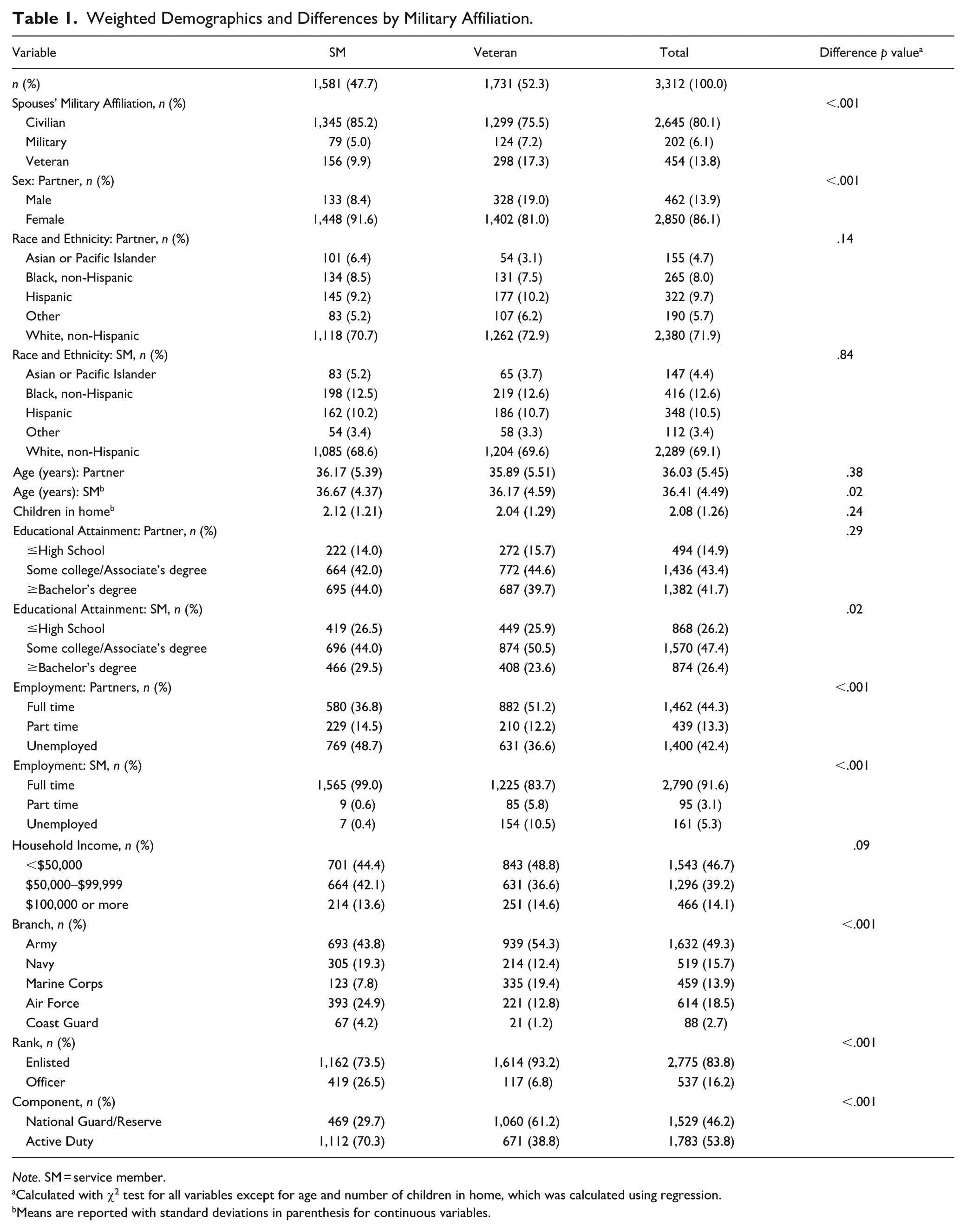
Note. SM = service member.
Calculated with χ2 test for all variables except for age and number of children in home, which was calculated using regression.
Means are reported with standard deviations in parenthesis for continuous variables.
Rates of IPV
As indicated in Table 2, 43.0% of the sample reported any IPV experience (37.6% service members; 47.9% veterans) and 43.9% reported any IPV use (36.4% service members; 50.8% veterans). Whereas more than half (57.9%) of military couples had no IPV, less than half (44.6%) of veteran couples had no IPV. Among veterans with any IPV, bidirectional IPV was the most common pattern across both service member and veterans, representing more than two thirds (77.1%) of participants who reported IPV and over a third of participants in the overall sample (32.0% service members; 43.2% veterans). In contrast, unidirectional IPV experience and unidirectional IPV use represented 5.1% and 6.1% of the overall sample, respectively (see Supplement S-1 for additional information on IPV subtype).
Types of IPV by Military Affiliation (Weighted).
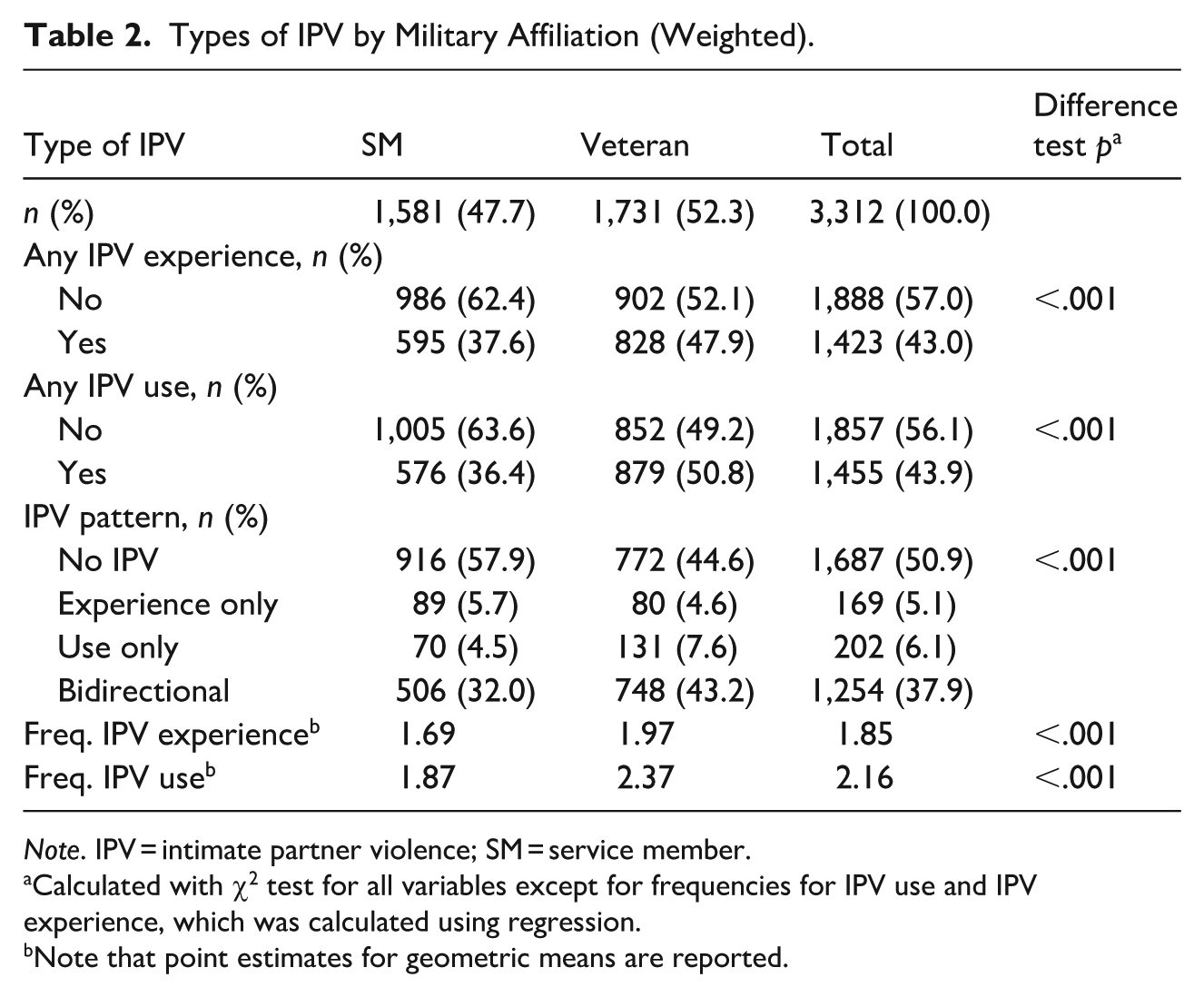
Note. IPV = intimate partner violence; SM = service member.
Calculated with χ2 test for all variables except for frequencies for IPV use and IPV experience, which was calculated using regression.
Note that point estimates for geometric means are reported.
Associations Between Veteran Status and Any IPV Use and Any IPV Experience
Initial bivariate tests confirmed that a larger percentage of veterans had reported IPV experiences, χ2 (1, N = 3,306) = 14.83, p < .001), and IPV use, χ2 (1, N = 3,308) = 28.74, p < .001), relative to service members. Unadjusted logistic models again showed that veterans were more likely to report IPV experience (OR = 1.52, 95% confidence interval [CI] [1.22, 1.88], p < .001) and IPV use (OR = 1.80, 95% CI [1.45, 2.23], p < .001), relative to service members. After adjusting for covariates, veterans still had elevated rates of any IPV experience (aOR: 1.43; 95% CI [1.10, 1.85]; Table 3, Model 1) and any IPV use (aOR: 1.67; 95% CI [1.29, 2.18]; Table 3, Model 2; Supplement S-1) relative to service members.
Results by IPV Pattern (Weighted).
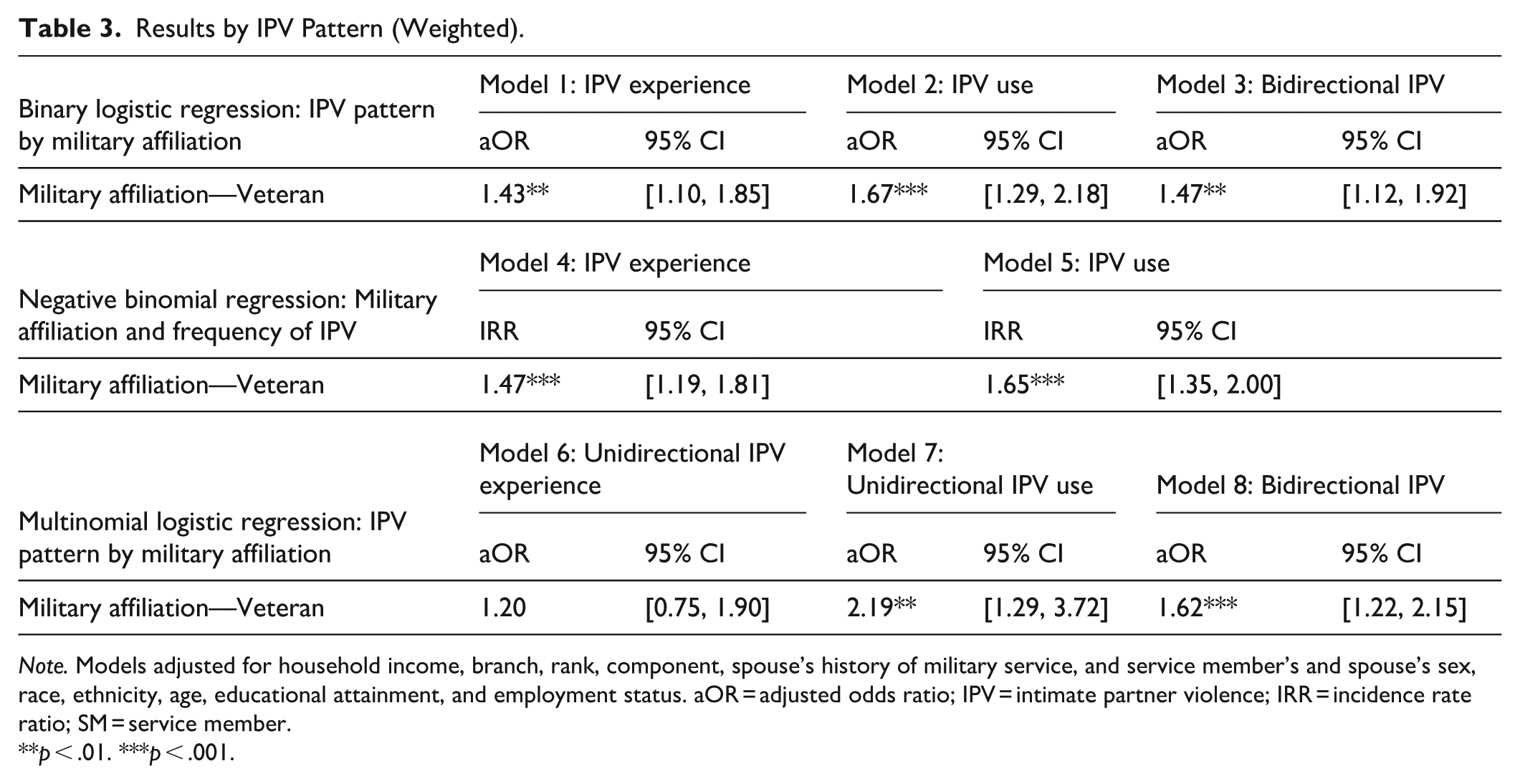
Note. Models adjusted for household income, branch, rank, component, spouse’s history of military service, and service member’s and spouse’s sex, race, ethnicity, age, educational attainment, and employment status. aOR = adjusted odds ratio; IPV = intimate partner violence; IRR = incidence rate ratio; SM = service member.
p < .01. ***p < .001.
IPV Use and Experience Frequency
As reported in Table 2, veterans had higher mean overall frequencies of IPV use and IPV experience, relative to their service member counterparts. Results from unadjusted NBR further estimated that veteran status was associated with a 55% increase in the expected frequency of IPV experience (IRR = 1.55; 95% CI [1.31, 1.83], p < .001) and an 81% increase in the expected frequency of IPV use (IRR = 1.88, 95% CI [1.52, 2.15], p < .001). After adjusting for covariates, veterans had an increase in the expected frequency of IPV experience and use by 47% (IRR = 1.47; 95% CI [1.19, 1.81], p < .001; Table 3, Model 4) and 65% (IRR = 1.65, 95% CI [1.35, 2.00], p < .001; Table 3, Model 5; Supplement S-3), respectively, relative to service members.
IPV Patterns
When coded dichotomously, veterans had a 62% increase in the odds of reporting bidirectional IPV at the bivariate level (OR = 1.62, 95% CI [1.30, 2.01], p < .001), relative to service members. After adjusting for covariates, veterans had a 47% increase in the odds of reporting bidirectional IPV than service members (OR = 1.47, 95% CI [1.12, 1.92], p = .004; see Table 3, Model 3). Furthermore, in unadjusted multinomial models using a four category classification (no IPV, unidirectional IPV use, unidirectional IPV experience, and bidirectional IPV), veterans had a 121% increase in the odds of IPV use (OR = 2.21, 95% CI [1.32, 3.69], p = .002) and 75% increase in the odds of bidirectional IPV (OR = 1.75, 95% CI [1.39, 2.20], p = .001), relative to service members. In covariate-adjusted multinomial models, veterans had a 119% increase in the odds of IPV use (OR = 2.19, 95% CI [1.29, 3.72], p = .001; Table 3, Model 7) and 62% increase in the odds of reporting bidirectional IPV (OR = 1.62, 95% CI [1.22, 2.15], p < .001; see Table 3, Model 8). IPV experience did not vary by military affiliation in multinomial models (see Supplement S-4).
Discussion
Using data from military and veteran couples participating in a cohort study, we documented higher rates and frequencies of IPV use and IPV experience among veterans, even after adjusting for demographic and military characteristics. Veterans also had higher rates of bidirectional IPV, with two out of five veteran couples reporting both IPV experience and use compared with 3 out of 10 service members. After modeling the overlap between concurrent IPV use and experience (i.e., bidirectional IPV) vis-à-vis other forms of IPV (i.e., unidirectional IPV use and unidirectional IPV experience), veterans were more likely to have bidirectional IPV and IPV use relative to service members. These findings suggest that although veterans in the present study had elevated rates of any IPV use and any IPV experience, relative to their service member counterparts, such differences are partially attributed to elevated rates of bidirectional IPV—as in, IPV experience no longer differed after accounting for bidirectional IPV. These findings set the foundation for future investigation into risk factors for bidirectional IPV among veterans. Consistent with military transition theory, maladaptive coping among both partners may play a role in response to the stress of separation from military service (Castro & Kintzle, 2014; Kintzle & Castro, 2018).
Estimates of any IPV experience (43.0%) and any IPV use (43.9%) within the past 6 months among service members and veterans in the present study were higher than the 12-month prevalence rates reported by Cowlishaw et al. (2022; 13% and 21% for IPV use and IPV experience, respectively). Data on IPV behaviors from the present study were collected from partners in contrast to self-reported data from service members and veterans, raising the risk of methodological variation, although high rates of inter-partner agreement on IPV have been documented elsewhere in the literature (Walsh & Stephenson, 2022). Other potential explanations include differences in operationalization or measurement, particularly as validated instruments are rarely used in the literature (Cowlishaw et al., 2022).
Rates of any IPV experience (47.9%) and any IPV use (50.8%) among veterans in the present study were comparable to past-year rates from veterans who completed the RVUES during a mental healthcare visit at Veterans Health Administration (VHA) facilities (49% and 46.5% for experience and use, respectively; Portnoy et al., 2023), with a high degree of consistency across studies even after adjusting for bidirectionality (bidirectional IPV: 43.2% in both the present study and in Portnoy et al., 2023; 4.6% and 7.6% for unidirectional experience and unidirectional use, respectively, vs. 5.8% [unidirectional experience] and 3.2% [unidirectional use] in Portnoy et al., 2023). Whereas Portnoy et al. (2023) used data from a subset of veterans eligible for, enrolled in, and using VHA healthcare (Cameron, 2023), potentially conferring heightened vulnerability relative to the broader veteran population (e.g., VHA enrollees have poorer health and more socioeconomic disadvantage relative to non-VHA enrollees; Eibner et al., 2016), the present study instead used data from veterans regardless of their VHA enrollment or engagement. However, veterans in the present study had separated from military service and reintegrated into civilian life relatively recently (i.e., between the enrollment period [April of 2011 to April of 2013] and the second follow-up survey [2019–2021]), raising the possibility that differences in IPV rates may reflect heightened vulnerability due to the stress of reintegrating into civilian life (Castro & Kintzle, 2014; Kintzle & Castro, 2018).
When examining IPV patterns after adjusting for the overlap between IPV use and experience, bidirectional IPV was the dominant form of IPV in the present study, representing more than three quarters of service members and veterans who had either IPV use or IPV experience. This finding challenges the notion that IPV use and IPV experience are mutually exclusive behaviors among members of a couple. Future research is necessary for understanding the context, motivations, severity of injuries inflicted, and consequences of bidirectional IPV (Langhinrichsen-Rohling et al., 2012; Machado et al., 2024). Although high rates of bidirectional IPV and low rates of unidirectional IPV have been documented in general samples (Machado et al., 2024), UK military personnel (MacManus et al., 2022), and veterans seeking mental healthcare at the VHA (Portnoy et al., 2023), the present study is the first known effort to examine bidirectional IPV disaggregated by current military affiliation.
Veterans in the present study had significantly higher rates of bidirectional IPV and unidirectional IPV use than their service member counterparts, even after accounting for their unidirectional IPV experiences. High rates of bidirectional IPV yield potential implications for resource allocation and programming, as bidirectional IPV tends to result in more serious injuries (Palmetto et al., 2013) and has been linked to an elevated risk of mental health challenges (Hellmuth et al., 2014), relative to unidirectional IPV. Moreover, most IPV interventions assume unidirectional IPV and therefore unsuitable for those with bidirectional IPV (Bates, 2016), warranting the need for more research to inform programming for couples with bidirectional IPV.
Although assessing bidirectional IPV separately from unidirectional is an important distinction, it still does not reveal important contextual factors related to the relationship violence, such as impact (e.g., resulting injury) or function. Notably, prior research shows that although women may report higher rates of IPV use, men’s use of IPV against women is more likely to inflict injury, posttraumatic stress, and relationship dissatisfaction (Archer, 2000; Caldwell et al., 2012). Future work should investigate the context, motives (e.g., self-defense or retaliation), and dynamics underpinning the use of violence among partners (Machado et al., 2024), particularly as in some instances partners may use violence only in self-defense (Babcock et al., 2019). Ideally, future research honing on marital and family dynamics, paired with qualitative and mixed method investigations aiming to contextualize bidirectional IPV (Machado et al., 2024), can enhance the understanding of bidirectional IPV and inform the development of evidence-based programming and interventions for couples with bidirectional IPV.
By leveraging data from military and veteran couples in the same study, findings from the present study strengthen the evidence base for understanding differences in rates of IPV by military affiliation. Theoretical propositions from military transition theory (Castro & Kintzle, 2014; Kintzle & Castro, 2018) may offer explanations for differences in rates of IPV among veterans. According to military transition theory, service members and their families contend with a range of stressors throughout the military-to-veteran transition including those related to healthcare, employment, finances (Derefinko et al., 2019), housing, and social support (Markowitz et al., 2023), that have been theorized to lead to poorer outcomes and maladaptive behaviors (Castro & Kintzle, 2014; Kintzle & Castro, 2018). Elevated rates of other forms of risky behavior (e.g., looking to start fights, substance use, reckless driving; Markowitz et al., 2023) and self-directed violence (Sokol et al., 2021) have been documented among veterans who recently separated from military service; thus, it is reasonable to expect heightened vulnerability to other violent behaviors such as IPV during the military-to-veteran transition. Additionally, the decision to continue to serve presumably reflects perceived relative costs and benefits of military life versus the civilian sector or other factors (e.g., problematic behaviors) that may lead to separation, which therefore may bias comparisons between veterans and nonveterans (Wolf et al., 2013).
Limitations
Findings from the present study should be considered with respect to its limitations. We cannot exclude the possibility that partners of service members may be more reluctant to disclose IPV than partners who are married to veterans. Additionally, only marital partners in heterosexual relationships with U.S. service members at the time of enrollment were eligible for participation in Family Study Panel 1, limiting the generalizability of findings in the present study. It will be important for researchers to examine IPV among service members and veterans characterized by nontraditional family structures, and for future surveys to collect data from nonmarital partners, given the growth in nontraditional family structures in the United States within recent decades (Smock & Schwartz, 2020). Another limitation involved reliance on self-report data from spouses to assess IPV. While an improvement over using data from official tracking systems in which service members and their partners may perceive barriers to reporting (Kamarck, 2019), we did not capture the perspectives of service members and veterans in assessing IPV. Forthcoming MCP follow-up surveys will include self-report data on IPV behaviors from service members, veterans, and their partners, enabling a more comprehensive understanding of behaviors, attitudes, beliefs, and processes that lead to IPV.
Implications and Future Directions
These findings yield many implications for research, policy, and practice. These findings lay the foundation for future research into factors that may contribute to elevated rates of IPV among veterans, such as the circumstances surrounding selective early attrition from military service (e.g., combat exposure, medical discharge, legal issues) or stress associated with separation from military service. Importantly, these results underscore the need to develop and administer IPV interventions that are tailored to the specific context, as interventions designed for unidirectional violence are unsuitable for bidirectional IPV and vice versa (Bates, 2016). The DoD and VHA also should consider updating protocols, procedures, and training manuals to better reflect the true nature of IPV. Finally, these findings underscore the value of detecting IPV as a first step for connection to IPV-related healthcare and social service resources (NASEM, 2024). The VHA recently expanded directives to screen all veterans for IPV experience at least once a year, regardless of age or sex, providing a model for other agencies and departments such as the DoD.
High rates of IPV use, IPV experience, and bidirectional IPV documented in the present study support calls for enhanced screening and detection of IPV in military communities, throughout the military-to-veteran transition, and after transitioning into veteran status. Such efforts are critical for understanding risk and protective factors for IPV among service members and veterans, evaluating the impact of intervention and prevention activities, and resource allocation. Risk and protective factors among service members and veterans may differ from civilian populations (NASEM, 2019) and throughout the military family life cycle, underscoring the need for longitudinal research on IPV throughout transitions such as the military-to-veteran transition (Castro & Kintzle, 2014). Moreover, high rates of bidirectional IPV underscore the value of examining IPV through a family science lens in which IPV rises from patterns of family or marital dynamics (Machado et al., 2024) or stressors experienced by all family members, as opposed to examining IPV as an individual phenomenon. Continued investment in IPV research is critical to optimizing DoD initiatives to reduce harmful behaviors among service members (Department of Defense, 2022) and VA initiatives to help veterans impacted by IPV (U.S. Department of Veterans Affairs, 2025).
Supplemental Material
sj-docx-1-jiv-10.1177_08862605251370402 – Supplemental material for Rates and Patterns of Intimate Partner Violence Among Service Members and Veterans
Supplemental material, sj-docx-1-jiv-10.1177_08862605251370402 for Rates and Patterns of Intimate Partner Violence Among Service Members and Veterans by Elizabeth C. Coppola, Travis N. Ray, Mark Relyea, Valerie A. Stander, Cynthia Brandt and Galina A. Portnoy in Journal of Interpersonal Violence
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: Report number 24-95 was jointly supported by the Department of Veterans Affairs (VA), Veterans Health Administration, and by the Defense Health Agency. The Millennium Cohort Family Study is conducted at the Naval Health Research Center, a U.S. Navy Bureau of Medicine and Surgery command, under work unit no. N1240. This research was supported by a VA HSR Career Development Award (CDA 19-234) and by the IPV Center for Implementation, Research, and Evaluation (IPV-CIRE), an IPVAP Innovation Hub that receives funding from VHA’s Care Management and Social Work Service. Dr. Coppola’s time was supported by the Advanced Fellowship in Medical Informatics through the VA Office of Academic Affiliations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Disclaimer
V.S. is an employee of the U.S. government. This work was prepared as part of her official duties. Title 17, U.S.C. §105 provides that copyright protection under this title is not available for any work of the U.S. government. Title 17, U.S.C. §101 defines a U.S. government work as work prepared by a military service member or employee of the U.S. government as part of that person’s official duties. The opinions expressed here are those of the authors and do not represent the official policy or position of the Department of the Navy, Department of Defense, U.S. Department of Veterans Affairs, nor the U.S. government. The funding sources had no involvement in the study design, analyses, article preparation, or decision to submit. The study protocol was approved by the Naval Health Research Center Institutional Review Board in compliance with all applicable federal regulations governing the protection of human subjects. Research data were derived from approved Naval Health Research Center Institutional Review Board protocol number NHRC.2015.0019.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.