
Abstract
Symptoms and problems that may arise from pediatric condition falsification (PCF) have not yet been systematically documented. The aim of the present study was to create a scoping overview of existing relevant scientific articles related to the physical symptoms and psychosocial problems that victims of PCF can develop. The methodological framework of Arksey and O’Malley was employed for this scoping review, supplemented by methodological insights from Levac et al. We used the PRISMA guidelines for our selection process. The search for physical symptoms was conducted in January 2024 (2013 to 2023). For psychosocial problems, the search was extended (2003–2023) due to the absence of relevant studies between 2013 and 2023. Inclusion criteria were English and Dutch articles, investigating victims of PCF, regardless of age or sex. A total of 29 articles were included; 25 studies on physical complaints and four studies on psychosocial problems. In total, victims of PCF reported 660 physical symptoms as a result of exposure to PCF (N = 82; 23 females, 30 males, 29 unknown). In six cases, exposure to PCF resulted in death of the victim. The victims of PCF reported 176 psychosocial problems in total (N = 225; 40 females, 35 men, 150 unknown). This scoping review indicates that exposure to PCF is accompanied by a wide range of physical symptoms and psychosocial problems among victims of PCF. We recommend including longitudinal research, psychological support, and follow-up protocols of victims after PCF diagnosis (e.g., in the form of questionnaires and interviews) to ensure personalized care.
Keywords
Introduction
Factitious disorder imposed on another (FDIA) is a psychiatric disorder in which an adult repeatedly fakes, induces, simulates, or exaggerates physical and/or mental symptoms in an individual under his or her care (American Psychiatric Association, 2013). Patients who meet criteria for FDIA are deemed perpetrators of medical child abuse (Roesler & Jenny, 2017). The literature on FDIA is plagued by conceptual noise as evidenced by the many alternative terms that have been coined to describe FDIA, including Meadow’s (1977) Munchausen Syndrome by Proxy (MSBP) (Shaw et al., 2008), Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV’s Factitious Disorder by Proxy (FDBP) and the broader term fabricated and/or induced Illness (Butz et al., 2009). Furthermore, more recently, medical professionals have coined the term pediatric condition falsification (PCF) to describe situations where a caregiver provides false information or manipulates the child’s medical history, symptoms, or actual physical condition (Ayoub et al., 2002). These professionals argue that this term is more desirable as it shifts the focus from perpetrators to victims, which, consequently, may guide both research and clinical approaches to help these victims (Meadow, 2002). In line with these developments, the present paper uses the term FDIA to describe the psychiatric disorder and the term PCF to describe the abusive behaviors resulting from this disorder.
PCF may cause a variety of symptoms and complaints. For example, a perpetrator may fabricate symptoms that lead to (medical) examinations and absence from school, lie about witnessing seizures in order to give a victim anti-epileptic medications, or actively induce symptoms that lead to unnecessary surgeries and treatments with potentially life-threatening side effects such as the administration of intravenous immunoglobulin (i.e., severe; Roesler, 2018). Importantly, one presentation of PCF (e.g., exaggeration) can develop into another (e.g., induction) over time (Jenny & Metz, 2020). Estimates from the UK suggest 0.5 to 2.0 per 100,000 children under the age of 16 are victims of PCF each year (Bass & Glaser, 2014; Ehrlich et al., 2008). Nevertheless, the prevalence of PCF is difficult to determine because it often goes unnoticed and unreported (APSAC, 2017). Flaherty and MacMillan (2013) suggest that pediatric healthcare providers only report PCF to child protective services (CPSs) if they have very strong suspicions. Healthcare providers tend to trust that parents know their child best and will provide an accurate account of their child’s medical history and disease progression (Schreier & Libow, 1993). This trust allows perpetrators to push for invasive tests and procedures, which allows PCF to occur (Crumm et al., 2018). An issue that further complicates diagnosis is that 30% of victims have an actual underlying medical condition (Rosenberg, 1987). In these cases, the parent begins to exaggerate, fabricate, or induce symptoms of illness during treatment for the medical problem. Providers are often not trained to question the medical history of children provided by parents (Schreier & Libow, 1993). When they do express doubts about treatments and/or medications requested by parents, parents may approach other healthcare providers. This leads to fragmented care, which allows these parents to continue the deception (APSAC, 2017).
Over the past decades, most research has focused on characteristics of perpetrators. Such efforts have revealed that the majority are women, most often the mother of the victim (Bartsch et al., 2003; McClure et al. 1996). They are often socially capable, manipulative, and friendly to medical personnel. Furthermore, they tend to spend considerable time in the hospital and sometimes have a medical history detailing symptoms comparable to those induced and/or exhibited by the victim (Abdurrachid & Marques, 2020). Yates and Bass (2017) examined the characteristics of 796 perpetrators and found that the majority was married, had a mean age of 27.6 years at the time of detection, and about half of them worked in healthcare, suggesting that a subgroup of perpetrators possesses a considerable degree of medical knowledge (see also Flaherty & MacMillan, 2013). Furthermore, perpetrators in this study often had a history of traumatic experiences, including childhood abuse, and met criteria for a myriad of comorbid psychiatric diagnoses, including somatoform and factitious presentations. Other studies have found perpetrators to have histories of somatoform disorder, factitious disorder imposed on them by their own caretakers, substance use, and other self-destructive behaviors (Bools et al., 1994). Finally, personality disorders, most notably cluster B personality disorder, seem to be common in both female and male perpetrators (Bass & Glaser, 2014; Bass & Jones, 2011; Bools et al., 1994).
Given the hidden nature of PCF, most victims go unnoticed. Those that are known often disappear from the view of care providers because the perpetrator terminates therapy, moves to another place of residence, or disappears shortly after the termination of a supervision order (a child protection measure imposed by the juvenile court) (Libow, 1995). Consequently, little data are available about victims. Nevertheless, existing studies suggest that boys and girls are equally likely to be victims of PCF. Furthermore, oftentimes, multiple children in a family become victim, with all children showing symptoms comparable to those in the detected child (Flaherty et al., 2013). In young children, the age of detection lies between 14 months and 2.7 years (Sheridan, 2003). Older children are less at risk to become victim of PCF. Yet, data suggest 25% of victims are six years or older at the time of detection (Denny et al., 2001; Sheridan, 2003). It can take months, even years, from initial symptom presentation to a diagnosis of PCF (Flaherty et al., 2013). When PCF goes undetected for a long time, the child can take on the sick role and believe that they are truly ill, further complicating detection (Jenny & Metz, 2020).
The extent of harm imposed on the victim seems to depend on the type (e.g., exaggeration and induction) and severity of the PCF presentation as well as on the tests and (medical) procedures that follow (Hornor, 2021). Evidently, victims exposed to induction of symptoms are most at risk for serious harm. For example, unnecessary and invasive medical treatments can lead to complications and mutilations like blindness, organ removal, or hearing loss (APSAC, 2017) and about 6% of these children die because of induced illness causing this additional harm (Bass & Glaser, 2014). Aside from physical complaints, victims may (also) experience psychosocial problems, such as confusion about (psychological) health and relationships, social isolation from peers, an inability to attend school, and psychological symptoms (e.g., excessive compliance or aggressive behavior, low self-image) or develop psychological disorders like post-traumatic stress disorder (PTSD) and eating disorders (APSAC, 2017; Hornor, 2021).
Although victims of PCF are subjected to serious harm, to date, no overview exists of the myriad of physical complaints and psychosocial problems that are encountered in victims of this form of child abuse. The present study aims to fill this void in hopes that an overview paper may aid clinicians in the identification, protection, and treatment of victims. Specifically, we conducted a scoping review to examine what is, at present, known about the physical complaints and psychosocial problems that victims exhibit when exposed to PCF. In this scoping review, we define physical complaints as symptoms or sensations that indicate pain or discomfort in the body. They can vary from mild to severe and may include diseases, injuries, infections, dysfunctions, and physical damage. Such complaints are often the starting point for medical examinations because they suggest that there might be a medical issue that needs assessment and treatment. We define psychosocial problems as an array of complaints that are not strictly medical or somatic in nature and that affect daily functioning (see Vannieuwenborg et al., 2015). Such complaints may include emotional problems, including internalizing problems (e.g., anxiety, inhibition, depressive feelings, and psychosomatic symptoms), externalizing problems (e.g., aggression, restless behavior, and delinquency), and social interaction problems (i.e., making and maintaining contact with others; Wolff et al., 2017).
Method
Research Design
A scoping review was used to answer the above research question. A scoping review is a relatively new research method to gain an overview of the existing literature on a broad topic or a complex research issue (Peterson et al., 2017). A scoping review has no methodological limitations and does not assess the quality of studies (Arksey & O’Malley, 2005). The main goal of a scoping review is to understand the size and diversity of available literature, identify gaps, and clarify a broad research question by means of a systematic approach. Based on the gaps found in the literature, preliminary conclusions can be drawn about the theme in question, which can be used as a basis for empirical follow-up research (Arksey & O’Malley, 2005; Tricco et al., 2016, 2018). The fact that no systematic research has been conducted regarding physical complaints and psychosocial problems of victims of PCF made a scoping review a suitable method for the current study.
The methodological framework of Arksey and O’Malley (2005) was used in the current study, supplemented with methodological comments and remarks from Levac et al., (2010). Using this methodological framework led to a transparent representation of the research process, which enables third parties to replicate the study. In addition, it increased the reliability of the research results (Arksey & O’Malley, 2005). In the methodological framework of Arksey and O’Malley, six steps are described: (a) identifying the research question; (b) searching for relevant studies; (c) selecting studies; (d) mapping the data; (e) collecting, summarizing and reporting the results; and (f) consulting with stakeholders to substantiate or validate the research results. The last step in this framework is optional and was not performed in the current study. To enhance transparency and ensure methodological rigor in the selection process, a PRISMA flow diagram was included (view Figure A1 in the Appendix). Although not originally part of the Arksey and O’Malley (2005) framework, the flow diagram aligns with updated recommendations for scoping review reporting, such as the PRISMA-Scoping Review extension (Tricco et al., 2018).
Search Strategy
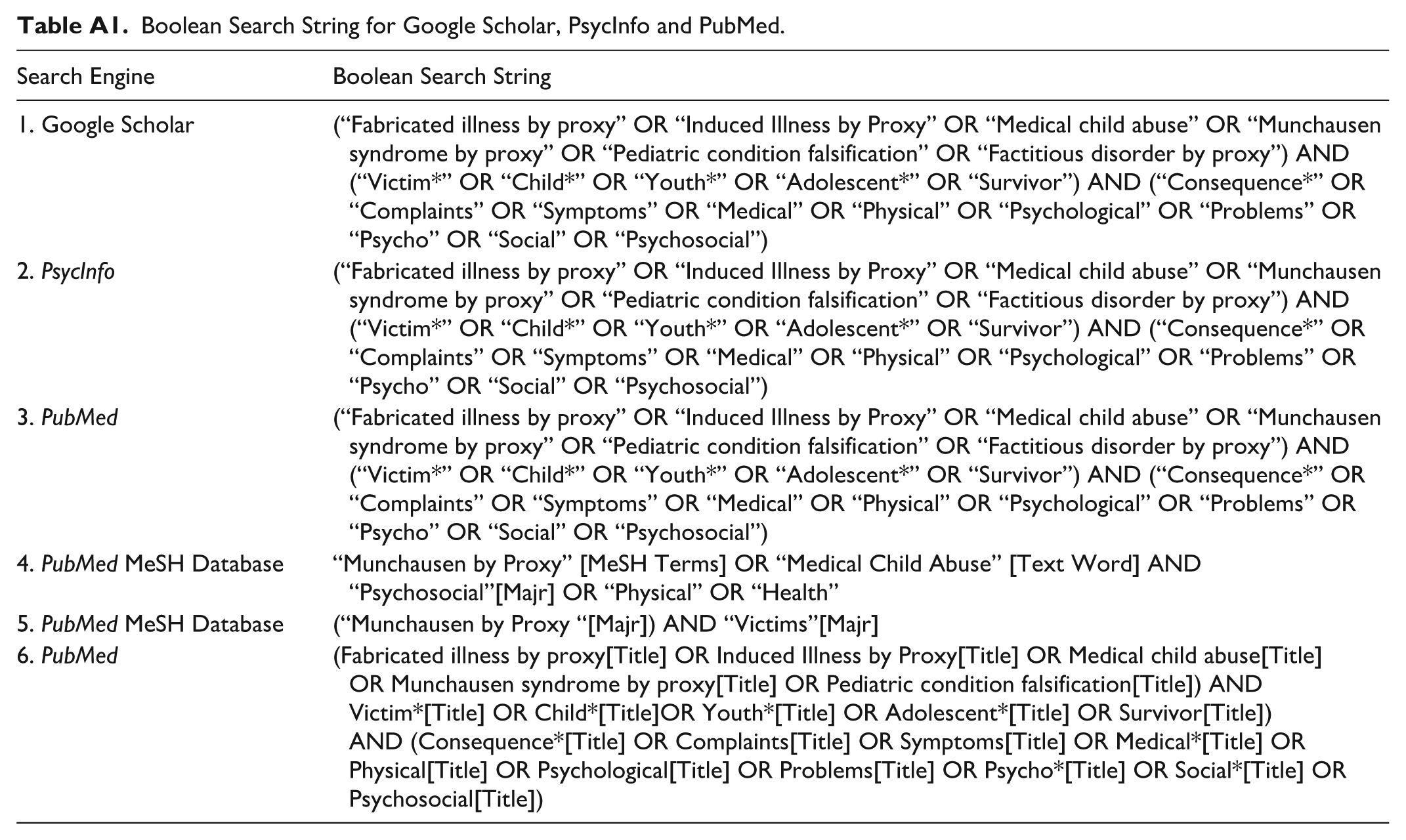
The following constructs were used in this study: PCF, victims, physical complaints, and psychosocial problems. These constructs were operationalized into a list of (Dutch and English) search terms (see the Appendix). The searches were done within the databases of PubMed, Google Scholar and the overarching database EBSCO (PsychINFO, PsycArticles, Psychology, and Behavioral Sciences Collection and Medline). Articles on the relevant constructs were searched as extensively as possible using a Boolean search string. PubMed, EBSCO, and Google Scholar were then searched for relevant articles using a MeSH term. In addition, the references of the included studies were searched for potentially relevant articles that did not emerge from the initial search (backward search). A forward search was also performed, a process in which articles are identified that cite or mention an original article after it has been published. These manually selected articles were included in the study.
Inclusion and Exclusion Criteria
Only Dutch and English articles were included. The articles were limited to peer-reviewed articles and dissertations. So-called grey literature, such as chapters of books and reports, were included if they appeared to be relevant to this study according to our inclusion criteria. The search for both physical complaints and psychosocial problems was set from 2013 to present. This yielded 25 studies that focused on physical complaints. For psychosocial problems, an additional search was performed from 2003 to 2013, because the initial search resulted in only a few relevant hits. A backward search yielded studies that were conducted before 2003. Finally, articles were included in which both male and/or female victims were mentioned, regardless of their place of residence, origin, and cultural background. With regard to age, children and young people who were between 0 and 18 years old at the time the harm was committed were considered. Any retrospective studies, in which victims look back on their past as victims of PCF, were also included.
Data Screening
Several steps were taken to screen the literature on PCF. First, the Boolean search string (Table A1) was entered into the relevant databases. Articles that were not in Dutch or English were excluded. After this, the literature found was screened for the title and abstract. Duplicates were removed. The literature was then screened for the occurrence of terms that are relevant to this study, including PCF, physical complaints, and psychosocial problems. In the remaining articles, the relevant terms related to the victims were examined, after which the full article was read. Finally, the reference list of the included articles was checked for potentially relevant studies, which were also included. In addition, it was also checked whether the article in question appeared in later studies (forward search). The selection process was recorded in the software program Zotero (Zotero 6.0). An overview of the selection process is shown in a PRISMA flow diagram (see Figure A1 in the Appendix).
Data Extraction and Analysis
For each relevant article in this study, data were collected on the name of the authors, the year of publication, the country in which the data were collected, and the physical complaints and psychosocial problems found in the victims as a result of and as an expression of PCF. The type of (literature) research that was conducted was also noted. For quantitative research, the size of the sample was mentioned. For meta-analyses and (systematic) review articles, attention was paid to the number of articles included, the number of articles within the study, and the number of victims per study. The software program Zotero was used to collect, organize, cite, and share references of literature sources (Zotero 6.0). The extracted data were analyzed using tables and diagrams, using Microsoft Excel software (Microsoft Excel, 2016). A medical specialist (Doctor in a University Hospital, obtaining a PhD) was consulted to review our findings, to remove redundant categories, and for correctly using medical terms.
Results
Search Results and Literature Selection
The search was performed in January 2024 and resulted in 288 articles; 65 articles from Pubmed; 77 from Medline; 36 from PsychInfo; five from Psychology and Behavioral sciences collection; and one from PsychArticles (n = 184). During the initial search period (2013–2023), only a few articles were found on psychosocial problems. For this construct, we performed an additional search for the years 2003 to 2013, including a forward and backward search. This approach yielded 33 articles from Medline; 57 from PsychInfo; five from Psychology and behavioral sciences collection; one from PsychArticles; and eight manually added articles (n = 104). The manually retrieved articles using a backward search concerned studies that were conducted before 2003.
Of the total 288 articles retrieved, 132 articles were excluded based on title and abstract. After removing duplicates, 59 articles remained (n = 97). After careful screening, 21 articles were excluded because they did not address physical complaints or psychosocial problems among victims of PCF. Eight articles were excluded because no full text was available. Finally, one review article was excluded because it was not clear which studies were included and how many victims were involved (view PRISMA flowchart; see Figure A1 in the Appendix). The remaining 29 articles (view Table 1) consisted of 25 studies on physical complaints and four studies on psychosocial problems. In the 25 studies on physical complaints, four studies also described psychosocial problems. These four studies were included in both the analysis of physical complaints and the analysis of psychosocial problems. This resulted in a total of 29 included studies, of which 25 focused on physical complaints and eight on the psychosocial problems.
Overview of Included Studies (N = 29) on Physical Complaints and Psychological Problems of PCF Victims.
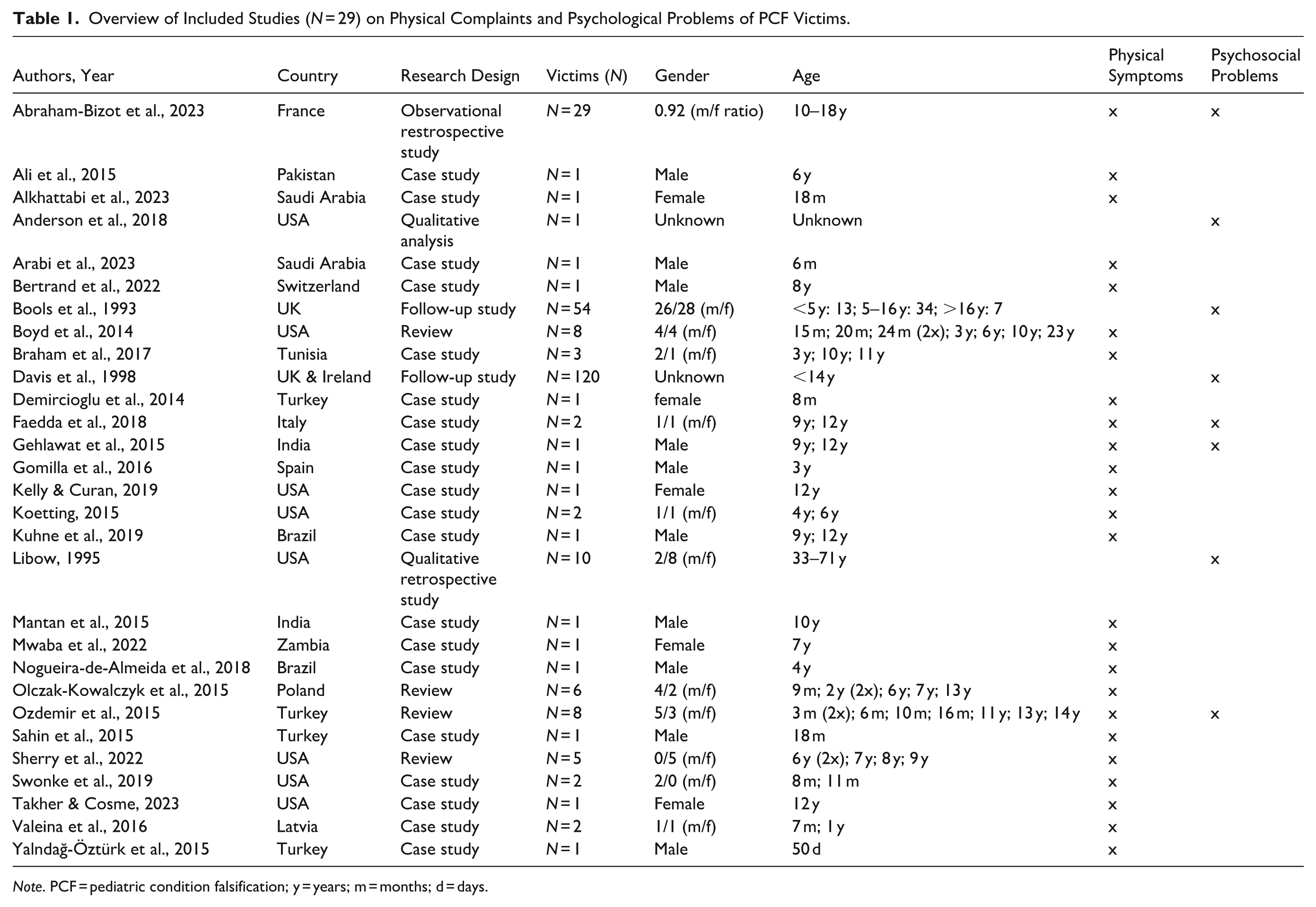
Note. PCF = pediatric condition falsification; y = years; m = months; d = days.
Of the total number of victims (N = 307, K = 29 studies), 82 were reported in studies on physical complaints and 225 were reported in studies on psychosocial problems. It is noteworthy that these numbers may be inflated because we included case studies, some of which may also have been included in a review (i.e., duplicates). We were unable to fully deduce this via the reference lists of the reviews. With the exception of one study, the perpetrator was the mother in all cases.
Literature Compilation
Table 1 provides an overview detailing characteristics of the articles (e.g., type of study, country of origin, etc.) included in the present review. Table 2 summarizes critical findings of both physical symptoms and psychological problems.
Critical Findings: Physical Symptoms and Psychological Problems of PCF Victims.
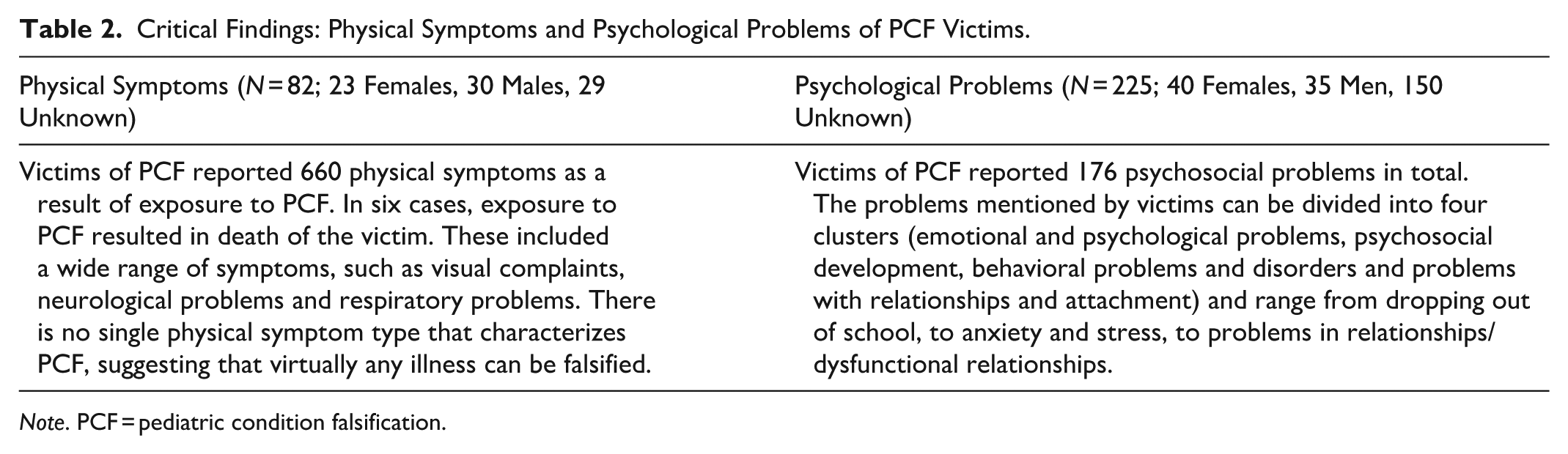
Note. PCF = pediatric condition falsification.
Physical Complaints: Study Characteristics
Of the studies on physical complaints (n = 25), the majority (40%) came from the United States and Turkey. Study designs included single case studies (n = 21), reviews (n = 3), and retrospective observational surveys (n = 1).
Of the 82 victims (i.e., 58.6% of all victims) reported on in these studies, the majority originated from France (n = 29), followed by the United States (n = 19), Turkey (n = 11), and Tunisia (n = 3). Studies from Brazil, Saudi-Arabia, Italy, India, and Latvia each reported two victims, whereas studies from Switzerland, Spain, Pakistan, Zambia, and Poland each reported one victim. Finally, the origin of five victims was not reported.
The age of the victims ranged between 50 days and 18 years old, with a mean age of 5.8 years. In 24 of the 25 studies, the exact age of the victims was mentioned. The average was calculated over these 53 victims. In one study, the exact age was not mentioned, but there was an age group (14–18 years). 41 of the victims (50.1%) were 10 years or older. The group of victims between 4 and 6 years and 7 and 9 years old were almost equal, with a distribution of eight (10.3%) and 10 victims (11.7%). Four victims were between 6 months and 1 year old (7.8%) and 12 victims were in the group of 1 to 3 years. The group up to 6 months involved seven victims (3.9%). Thirty of the victims in the studies focusing on physical problems were male and 23 of the victims were female. The sex of 29 victims could not be determined from the article.
Frequency and Type of Physical Complaints
A total of 660 physical complaints were described (M = 8 per victim) by the victims (n = 82). Complaints that showed similar characteristics, such as similarities in symptoms, were grouped together during the analysis. The same applied to complaints that affected the same body parts, were focused on certain organs, were part of a condition, or were focused on a functional area. Based on this method, the physical complaints mentioned in studies were clustered into groups that logically coincide (for an overview, see Table 3).
Physical Complaints (N = 660) of PCF Victims (n = 82) Clustered by Numbers (n) and Percentages (%).
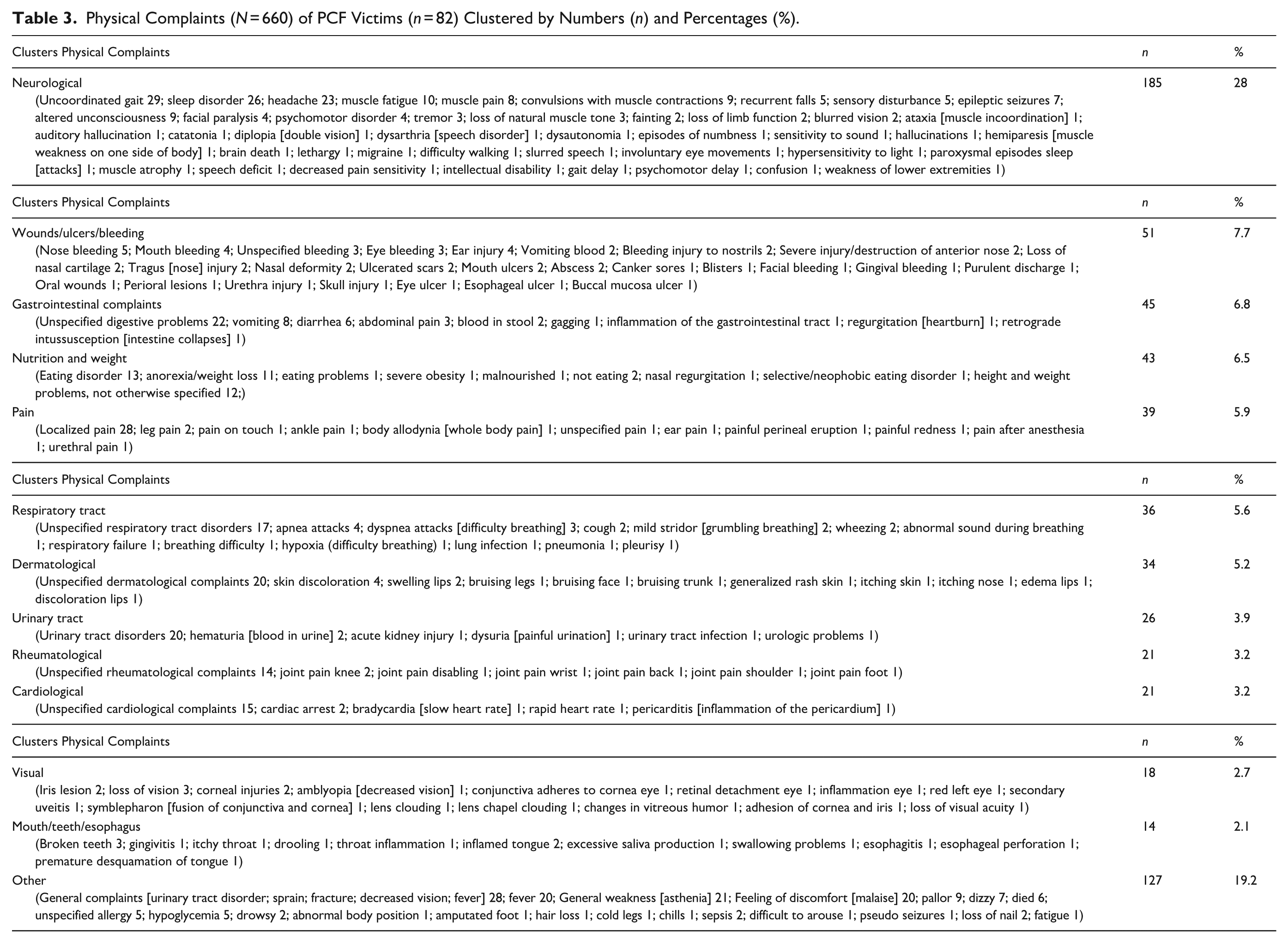
While some complaints were a direct consequence of exposure to PCF, such as a fracture or pain, other complaints were considered long-term consequences of exposure to PCF, including sleep problems and eating problems. In the existing literature, no explicit description of this distinction was found in most cases. The most frequently mentioned physical complaints were an uncoordinated gait pattern (n = 29), localized pain (n = 28), urinary tract disorders (n = 20), and fever (n = 20). The clusters in which most physical complaints fell were neurological (28%), wounds/ulcers/bleeding (7.7%), and gastrointestinal complaints (6.8%). Complaints in the clusters visual (2.7%) and mouth/teeth/esophagus (2.1%) were mentioned the least often by victims (see Table 4). Finally, six victims died as a result of physical complaints caused by exposure to PCF.
Psychosocial Problems (N = 176) of PCF Victims (n = 225) Clustered in Numbers (n) and Percentages (%).
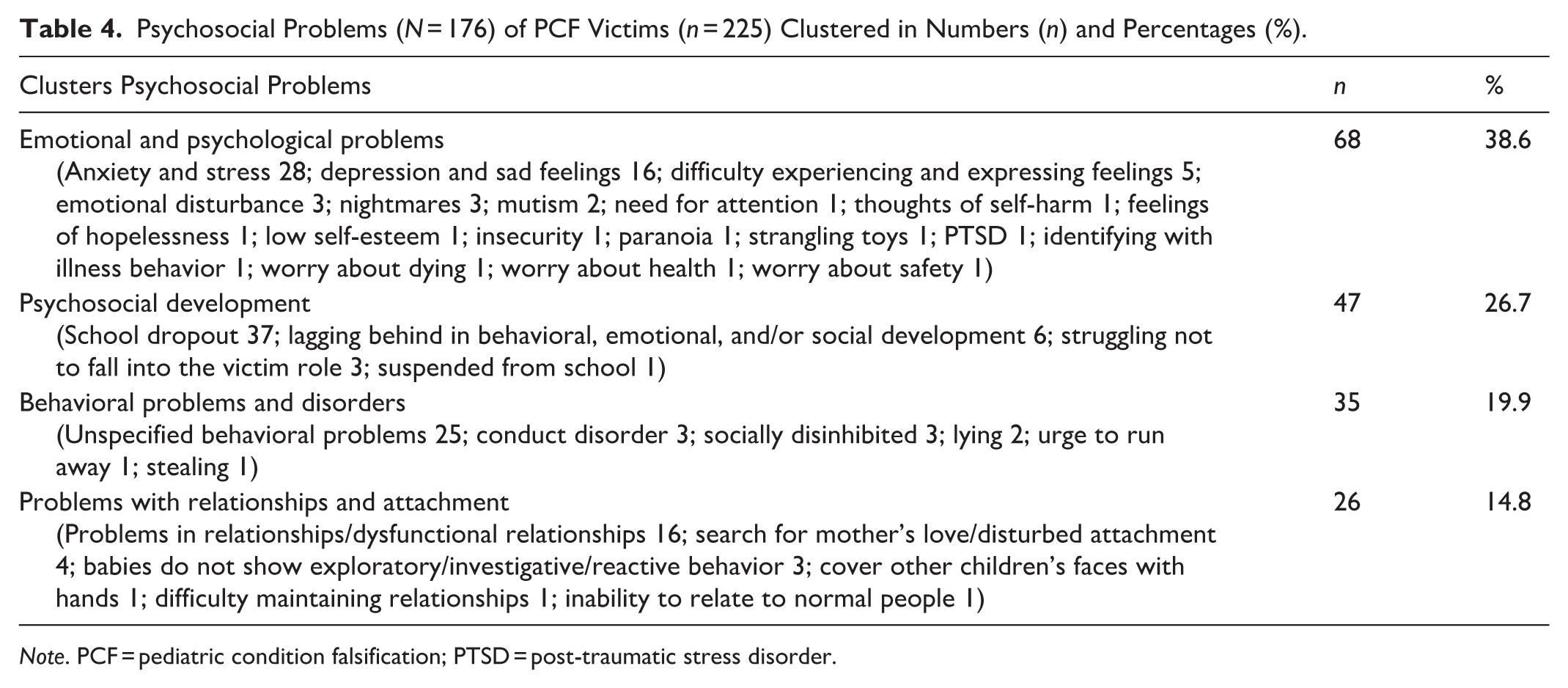
Note. PCF = pediatric condition falsification; PTSD = post-traumatic stress disorder.
Psychosocial Problems: Description of the Study Population
Of the eight studies reporting on psychosocial problems, half originated from England and the United States. The studies included two qualitative retrospective studies, two reviews, two single case studies, one follow-up study, and one qualitative analysis. In one study, victims were given a checklist containing 27 symptoms of PTSD. The majority of the 225 victims originated from England and Ireland (n = 174), followed by (France (n = 29; 12.9%), United States (n = 11; 4.9%), Turkey (n = 8), Italy (n = 2), and India (n = 1).The age of the victims ranged between 3 months and 71 years. The studies used different age groups, which meant that a distinction could only be made between victims up to 18 years old and victims 18 years and older. A total of 214 victims were 18 and 10 victims were over 18 years old. The age of one victim was unknown. A total of 40 of the victims were female and 35 were male. The sex of the remaining 150 victims was not reported.
Frequency and Type of Psychosocial Problems
A total of 176 psychosocial problems were mentioned. We divided psychosocial problems into four clusters: emotional and psychological problems (38.6%); social development (26.7%); behavioral problems and disorders (19.9%); and relationship problems and attachment (14.8%). School dropout was mentioned by 37 victims and anxiety and stress by 28 victims. Difficulty experiencing and expressing feelings and delays in behavioral, social, or emotional development were mentioned five and six times, respectively. A search for motherly love/disturbed attachment occurred four times and socially disinhibited behavior and struggling not to fall into the victim role were both mentioned three times. Mutism and lying were both mentioned twice. Craving for attention, the urge to run away, thoughts of self-harm, feelings of hopelessness, low self-esteem, difficulty distinguishing between fantasy and reality, insecurity, PTSD, strangling toys, and identifying with illness behavior were all mentioned once (see Table 5 for a full overview).
Implications for Research and Practice.
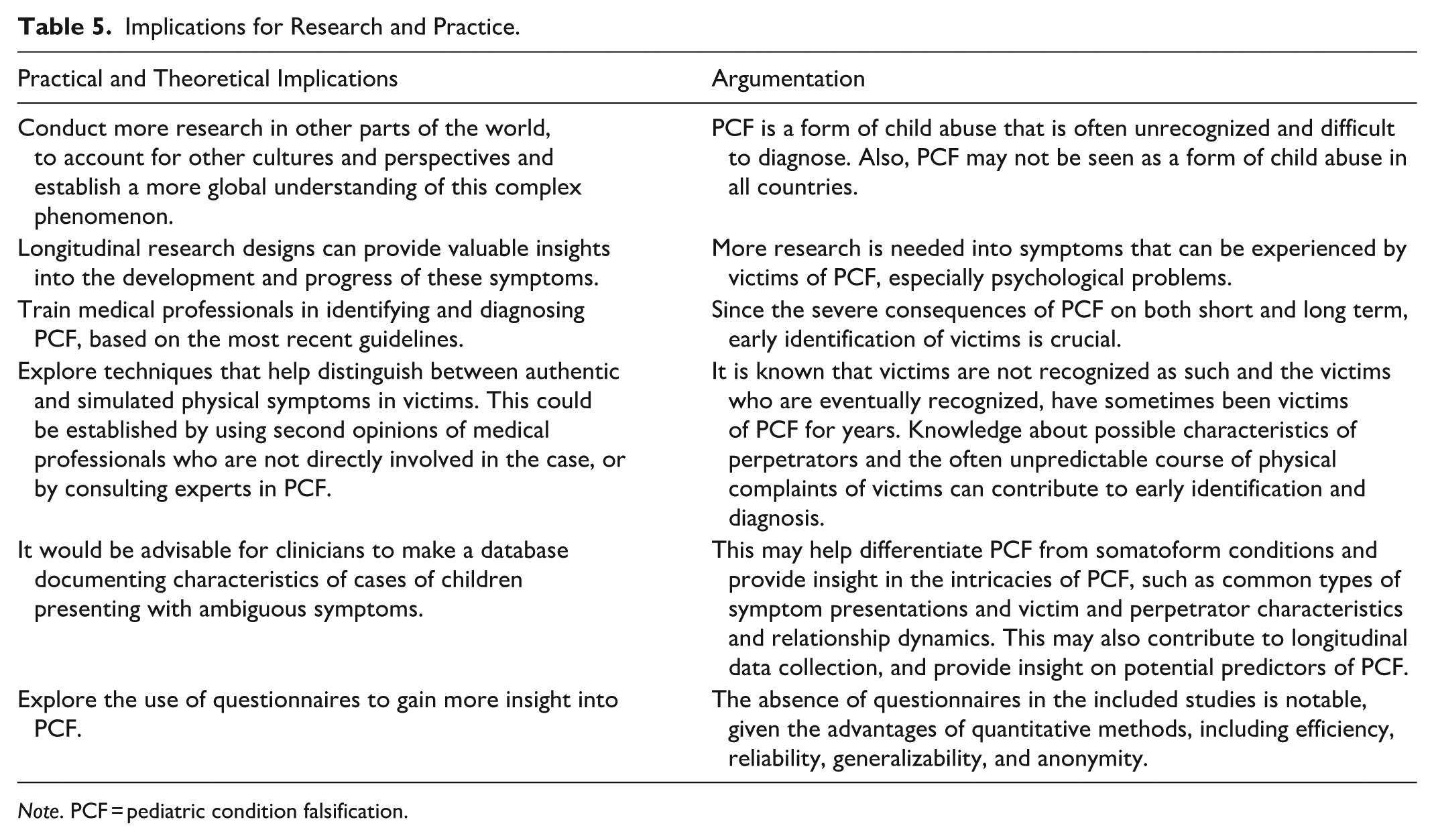
Note. PCF = pediatric condition falsification.
Discussion
The aim of the current scoping review was to present an overview of the physical complaints and psychosocial problems that victims experience due to PCF exposure. Our main findings are catalogued below. A summary of implications for practice and research can be found in Table 5.
Physical Complaints
Victims of PCF reported a total of 660 physical complaints as a result of exposure to PCF. In six cases, exposure to PCF led to the death of the victim. These findings are in line with previous research (Ozdemir et al., 2015; Swonke et al., 2019; Valeina et al., 2016), which found that exposure to PCF causes physical complaints in victims and can even lead to death. In all included studies, the physical symptoms were diagnosed by medical professionals, which increases reliability of the reported symptoms. The reported physical complaints by both victims and medical professionals in the included studies varied widely in severity and nature. They included a wide range of symptoms, such as visual complaints, neurological problems, and respiratory problems. Exposure to PCF can also lead to permanent physical complaints, such as amputation and blindness, and in extreme cases even to the death of the victims. Neurological complaints in particular were frequently reported, which is consistent with previous research (Doughty et al., 2016) and can be explained by the subjective nature of neurological symptoms, such as pain, weakness, and sensory abnormalities (Stone, 2013). This subjective nature makes it difficult to objectively measure or refute neurological symptoms (Stone, 2013). Furthermore, neurological disorders are often complex and variable in nature, which creates opportunities for neurological symptoms to be faked and falsified (Bass & Wade, 2019). The included studies showed that there is no single physical symptom type that characterizes PCF, suggesting that virtually any illness can be falsified. The fact that any illness can be targeted for falsification emphasizes the need for healthcare providers to be alert to a wide range of potential deceptions. This requires thorough evaluation and the ability to recognize patterns of irregularities in medical reports and symptoms. Medical professionals, therefore, need to follow current guidelines and use a multidisciplinary approach when assessing suspected cases suggestive of PCF, in order to minimize potential physical harm to victims (Lazenbatt, 2012). Interestingly, certain symptoms frequently described in clinical practice as being fabricated in PCF cases such as apnea and cyanosis were rarely reported in the included studies. This may reflect underreporting, diagnostic ambiguity, or the transient nature of these symptoms, which can make them difficult to document in clinical records or case studies (Roesler & Jenny, 2017). Most of the included studies were single case studies. Given the complexity and limited recognition of PCF (Abraham-Bizot et al., 2023), this design may be preferred and contributes to the field’s slow development. Case studies offer detailed documentation of victims’ physical complaints, aiding in diagnosis (Olczak-Kowalczyk et al., 2015). However, their limited generalizability hampers broader applicability (Thomas, 2011), highlighting the need for follow-up research. The absence of follow-up in these studies makes it impossible to differentiate between short-term, long-term, and permanent physical complaints. This distinction is crucial for understanding the full impact on victims.
The heterogeneity of cases illustrates the diverse manifestations of PCF (Braham et al., 2017), complicating diagnosis and limiting the reliability of conclusions. Compared to research on other forms of child abuse, studies on PCF-related physical complaints remain scarce (Fry et al., 2012; MacGinley et al., 2019). This may be due to the underrecognition of PCF, diagnostic challenges, and cultural variation in interpreting medical child abuse.
Psychosocial Problems
Research into psychosocial problems experienced by victims after exposure to PCF resulted in only five studies in the past 20 years and three studies that were found through a backward search. The victims of PCF reported a total of 176 psychosocial problems as a result of exposure to PCF. These findings are consistent with several previous studies that indicate a variety of complaints victims can experience (Abraham-Bizot et al., 2023; Bools et al., 1993; Libow, 1995). The psychosocial problems mentioned by victims can be divided into four clusters (emotional and psychological problems, psychosocial development, behavioral problems, and disorders and problems with relationships and attachment) and range from dropping out of school, to anxiety and stress, to problems in relationships/dysfunctional relationships. Ten of the victims in previous research (Libow, 1995) mentioned psychosocial problems that persisted into adulthood and affected their psychosocial well-being, suggesting that exposure to PCF does not only cause short, but also long-term psychosocial problems. The lack of studies on psychosocial problems in combination with the number of psychosocial problems mentioned by victims is remarkable. In the included studies, reference was consistently made to research by Libow (1995) when discussing the psychosocial problems that victims experience as a result of exposure to PCF, a study that was conducted 30 years ago. One explanation for the lack of studies into psychological problems is that more emphasis is placed on the importance of recognizing and diagnosing PCF by the physical complaints that victims experience. This might be due to the fact that a complete clinical picture is more difficult to identify and objectify when it concerns more ambiguous complaints or problems (Awadallah et al., 2015; Koetting, 2015). Therefore, professionals might not think of a PCF diagnosis when confronted with ambiguous, psychological problems. Also, it might be the case that psychosocial problems develop later on (as opposed to direct physical complaints), which makes them more difficult to investigate.
It is also noteworthy that in studies of physical complaints, little to no attention has been paid to the psychosocial problems that these victims can develop. The lack of research into psychosocial problems is a gap in the existing literature, especially since the serious consequences of other forms of child abuse have been extensively mapped (Fry et al., 2012; MacGinley et al., 2019). The medical context in which PCF is often a topic of interest might play a role in this. The fragmentation of different disciplines, such as the medical and psychological sectors, can further complicate this, which means that research into psychosocial problems remains fragmented. Of the studies that investigated psychosocial problems, nearly half employed a qualitative retrospective design, which may introduce bias. Retrospective reports often rely on reconstructed memories influenced by current beliefs and perceptions, rather than accurate recall of past emotions, thoughts, or behaviors (Matt et al., 1992; Robinson & Clore, 2002b). Memory distortion and selective recall are common, particularly when recalling events from the distant past. Furthermore, findings from retrospective qualitative studies may be context-specific and shaped by individual victim characteristics, limiting their generalizability (Tenny et al., 2022).
Implications and Recommendations
The results of this scoping review provide several theoretical and practical implications. PCF is a form of child abuse that is often unrecognized and difficult to diagnose (Abraham-Bizot et al., 2023; Ozdemir et al., 2015). Additionally, PCF may not be seen as a form of child abuse in all countries (e.g., view Cheung et al., 2005). The current scoping review resulted in studies from Western countries (Europe and the USA) only, and studies from other continents are currently lacking. One general recommendation is, therefore, to conduct more research in other parts of the world, account for other cultures and perspectives, and establish a more global understanding of this complex phenomenon. The results of the current scoping review also indicate that more research is needed into symptoms that can be experienced by victims of PCF, especially psychological problems. Although challenging to establish, longitudinal research designs can provide valuable insights into the development and progress of these symptoms. Research on PCF dominantly stems from retrospective case reviews. Identification of cases remains very difficult because of the hidden nature of actions that accompany PCF. Since there are severe consequences of PCF on both short and long term, early identification of victims is crucial. One recommendation, therefore, is to train medical professionals in identifying and diagnosing PCF, based on the most recent guidelines. It is recommended to repeat training periodically so that medical professionals remain informed of the most recent developments. It is known that victims are not recognized as such, and the victims who are eventually recognized have sometimes been victims of PCF for years (Libow, 1995). Knowledge about possible characteristics of perpetrators and the often unpredictable course of physical complaints of victims can contribute to early identification and diagnosis (Teeuw & Schoonenberg, 2024). Furthermore, it is recommended to explore techniques that help distinguish between authentic and simulated physical symptoms in victims. This could be established by using second opinions of medical professionals who are not directly involved in the case, or by consulting experts in PCF. Currently, the DSM-5 does not describe PCF but only FDIA, which solely focuses on the perpetrator side. This seems to have contributed to a strong focus on perpetrator characteristics. It would be advisable for clinicians to make a database documenting characteristics of cases of children presenting with ambiguous symptoms. Such databases may help differentiate PCF from somatoform conditions and provide insight in the intricacies of PCF, such as common types of symptom presentations and victim and perpetrator characteristics and relationship dynamics. This may also contribute to longitudinal data collection and provide insight on potential predictors of PCF. For future studies, it is recommended to explore the use of questionnaires to gain more insight into PCF. The absence of questionnaires in the included studies is notable, given the advantages of quantitative methods, including efficiency, reliability, generalizability, and anonymity (Watson, 2015). Only one included study (Libow, 1995) employed a questionnaire, consisting of 33 demographic and open-ended items, along with a 27-item PTSD symptom checklist. Considering that mothers are typically the perpetrators in PCF cases (Awadallah et al., 2005), it is important to assess whether fathers or other caregivers can provide accurate responses to gain insight into the victim’s psychosocial functioning. Instruments such as the Child Behavior Checklist, Strengths and Difficulties Questionnaire, and Pediatric Symptom Checklist have been used for this purpose (Vogels et al., 2009). Finally, a significant challenge in interpreting the findings of this scoping review was the lack of detailed reporting on the differentiation between pre-existing medical conditions and symptoms attributable to PCF. In many of the included studies, the data did not clearly distinguish between these two factors. This lack of differentiation complicates both the diagnosis of PCF and the treatment of affected children, as it remains unclear whether some of the physical and psychological symptoms may be genuine medical issues rather than the result of caregiver-induced symptoms. Earlier research suggests that approximately 30-60% of PCF victims have underlying medical conditions, further highlighting the complexity of distinguishing between genuine illness and falsified symptoms (Hall et al., 2000; Lau et al., 2006). However, the absence of systematic reporting on this issue in the included studies makes it difficult to establish a clear understanding of the extent to which pre-existing conditions contribute to the clinical presentation of PCF victims. Future studies could address this issue by incorporating more rigorous diagnostic criteria and reporting standards, which clearly distinguish between medical conditions and symptoms induced or fabricated by caregiver.
Limitations
Several limitations of the current review are worth mentioning. In the included studies, insufficient attention has been paid to the long-term consequences that victims can develop. Although some studies addressed the direct consequences of exposure to PCF, it remains unclear which physical complaints and psychosocial problems are considered permanent or secondary to the abuse. For example, a victim can be given laxatives to fake bowel problems, experiences permanent bowel problems (gastrointestinal problems), and then develops depressive symptoms as a result of these physical problems. This distinction was not made in the included articles, which is why it is also missing from this scoping review. Another shortcoming is that it is difficult to determine which physical complaints are a direct result of PCF and which ones are fabricated, which can confuse the assessment of the physical complaints. Moreover, the physical complaints mentioned by perpetrators do not necessarily have to be experienced as such by the victim. The existing literature lacks thorough research into the authenticity of these complaints, which makes it challenging to distinguish actual physical complaints from manipulated or exaggerated complaints. In addition, victims are exposed to unnecessary medical treatments and examinations, ranging from blood tests to laparoscopy. The physical complaints that can result from these interventions are not explicitly mentioned in the included studies. Finally, a limitation of our study was that the search, screening, and selection were largely done by one researcher. Although this researcher consulted the other researchers regarding during the search, screening, and selection process, this approach does not fully mitigate the risk of selection bias. To diminish such bias as much as possible, we used predefined inclusion and exclusion criteria.
Conclusion
The importance of more future research into physical complaints and psychosocial problems that PCF victims experience are highlighted in this review. The current overview can contribute to a better understanding of the complexity, diversity, and severity of the physical complaints and psychosocial problems that victims can experience. In addition, the results showed that there is a lack of recent research into the psychosocial problems and that more attention is paid to the physical complaints that may develop. The recommendations in the current study can contribute to a greater awareness and understanding of PCF with the ultimate goal of protecting vulnerable children from this complex form of child abuse.
Footnotes
Appendix
Boolean Search String for Google Scholar, PsycInfo and PubMed.
| Search Engine | Boolean Search String |
|---|---|
| 1. Google Scholar | (“Fabricated illness by proxy” OR “Induced Illness by Proxy” OR “Medical child abuse” OR “Munchausen syndrome by proxy” OR “Pediatric condition falsification” OR “Factitious disorder by proxy”) AND (“Victim*” OR “Child*” OR “Youth*” OR “Adolescent*” OR “Survivor”) AND (“Consequence*” OR “Complaints” OR “Symptoms” OR “Medical” OR “Physical” OR “Psychological” OR “Problems” OR “Psycho” OR “Social” OR “Psychosocial”) |
| 2. PsycInfo | (“Fabricated illness by proxy” OR “Induced Illness by Proxy” OR “Medical child abuse” OR “Munchausen syndrome by proxy” OR “Pediatric condition falsification” OR “Factitious disorder by proxy”) AND (“Victim*” OR “Child*” OR “Youth*” OR “Adolescent*” OR “Survivor”) AND (“Consequence*” OR “Complaints” OR “Symptoms” OR “Medical” OR “Physical” OR “Psychological” OR “Problems” OR “Psycho” OR “Social” OR “Psychosocial”) |
| 3. PubMed | (“Fabricated illness by proxy” OR “Induced Illness by Proxy” OR “Medical child abuse” OR “Munchausen syndrome by proxy” OR “Pediatric condition falsification” OR “Factitious disorder by proxy”) AND (“Victim*” OR “Child*” OR “Youth*” OR “Adolescent*” OR “Survivor”) AND (“Consequence*” OR “Complaints” OR “Symptoms” OR “Medical” OR “Physical” OR “Psychological” OR “Problems” OR “Psycho” OR “Social” OR “Psychosocial”) |
| 4. PubMed MeSH Database | “Munchausen by Proxy” [MeSH Terms] OR “Medical Child Abuse” [Text Word] AND “Psychosocial”[Majr] OR “Physical” OR “Health” |
| 5. PubMed MeSH Database | (“Munchausen by Proxy “[Majr]) AND “Victims”[Majr] |
| 6. PubMed | (Fabricated illness by proxy[Title] OR Induced Illness by Proxy[Title] OR Medical child abuse[Title] OR Munchausen syndrome by proxy[Title] OR Pediatric condition falsification[Title]) AND Victim*[Title] OR Child*[Title]OR Youth*[Title] OR Adolescent*[Title] OR Survivor[Title]) AND (Consequence*[Title] OR Complaints[Title] OR Symptoms[Title] OR Medical*[Title] OR Physical[Title] OR Psychological[Title] OR Problems[Title] OR Psycho*[Title] OR Social*[Title] OR Psychosocial[Title]) |
Acknowledgements
We would like to thank Dr. Kim Claessen, MD, PhD at the Leiden University Medical Center (LUMC) the Netherlands, for her valuable input and expert review of the medical terminology used in our categorization of symptoms. Her clinical insights contributed to refining the structure and accuracy of the presented data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.