
Abstract
The immediate aftermath of child sexual assault is a critical yet understudied period where crisis interventions can mitigate or exacerbate trauma. Despite their pivotal role, no systematic review has synthesized qualitative evidence on stakeholder experiences of these services. To aggregate findings from qualitative studies examining children, young people (CYP), parents/carers, and service providers’ (police, medical staff, psychosocial support, and child protection professionals) experiences of crisis responses following child sexual assault. Five databases (MEDLINE, PsycINFO, Embase, CINAHL, ProQuest Social Science) were searched using PICo (Population: Child Sexual Assault survivors/families/providers; Phenomenon: Crisis service experiences; Context: ≤72 hrs post-disclosure). Preferred Reporting Items for Systematic Reviews and Meta-Analyses guided screening ensured transparency. Included studies (n = 22) were synthesized via Joanna Briggs Institute meta-aggregation, deriving actionable themes while preserving meaning. Three stakeholder groups reported systemic challenges:
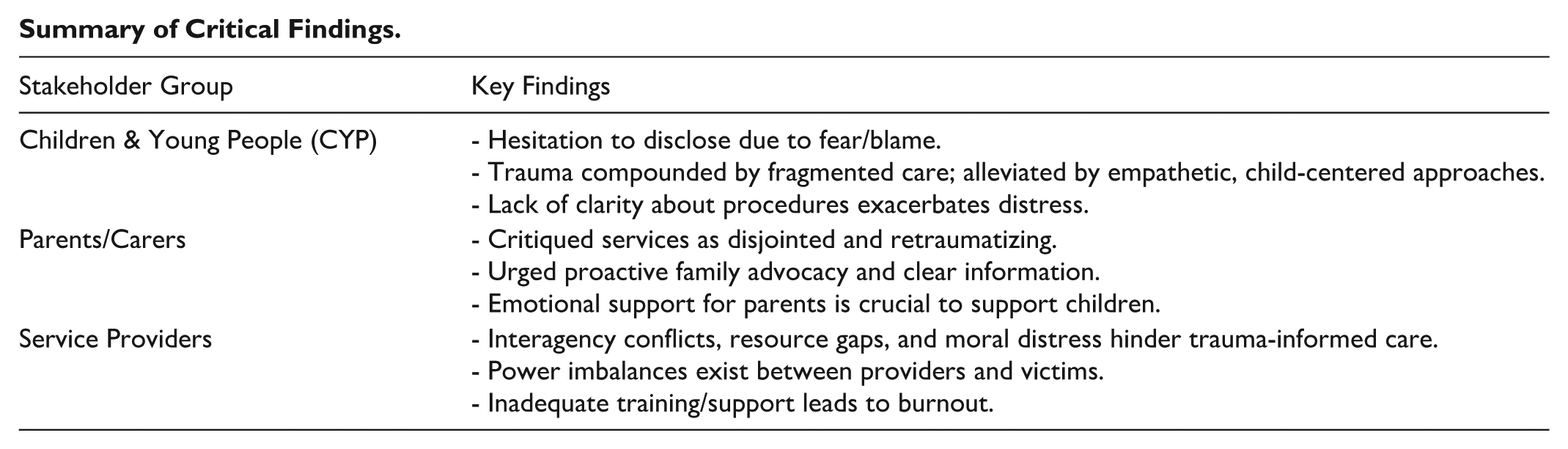
• CYP (16 studies): Hesitated to disclose due to fear/blame; trauma was compounded by fragmented care but alleviated by empathetic, child-centered approaches.
• Parents (6 studies): Critiqued services as disjointed and retraumatizing, urging proactive family advocacy.
• Providers (6 studies): Cited interagency conflicts, resource gaps, and moral distress as barriers to trauma-informed care.
This first meta-aggregation of post-child sexual assault crisis care identifies the need for systemic reforms; standardized multi-disciplinary protocols, dedicated family supports, and provider training as well as clinical and supportive supervision to mitigate secondary trauma. Findings underscore the need for trauma-informed systems to prevent compounding harm during this vulnerable period.
Introduction
Child sexual abuse (CSA) is a pervasive global public health and human rights concern with often profound and long-lasting effects on children, families, and communities (Rahnavardi et al., 2022). It encompasses a wide range of behaviors perpetrated by adults, older or peer-aged adolescents, often in positions of power, authority, or trust, and involving coercion, manipulation, or exploitation (World Health Organization [WHO], 2017). CSA includes acts involving sexual penetration of a child, sexualized touching of intimate body parts, and, in some contexts, non-contact offenses such as exhibitionism or exposure to pornography (Mathews & Collin-Vézina, 2019; Stoltenborgh et al., 2011). Prevalence estimates vary due to definitional and methodological differences as well as under-reporting. However, global meta-analyses indicate that approximately 12 to 18% of girls and 8% of boys experience CSA before the age of 18 (Stoltenborgh et al., 2011). More recent data suggest lifetime prevalence rates of around 9% for contact sexual violence (Piolanti et al., 2025).
Although CSA encompasses a broad range of abusive behaviors, this review focuses specifically on recent child sexual assault. In this context, the term refers to a distinct incident of sexual abuse or sexual violence that is believed to have occurred within the past 72 hrs. This timeframe is significant because it generally represents the window during which forensic evidence can still be collected from the victim (Crawford-Jakubiak et al., 2017). The review, therefore, concentrates on the experience of service system responses triggered by recent disclosures that fall within this forensic window, which differ markedly from the responses to disclosures made outside this timeframe, where legal, forensic, and psychosocial procedures tend to follow a different pathway.
The immediate aftermath of child sexual assault constitutes a critical period, often marked by profound emotional and psychological distress for affected children, their families, and the professionals providing care (Finkelhor & Browne, 1985; Greeson & Campbell, 2013). During these initial hours, children and their caregivers may interact with multiple service providers, including police, child protection workers, mental health professionals, and forensic medical examiners, all while still processing acute psychological and social trauma symptoms. The quality of crisis interventions during this time can influence both short-term outcomes and long-term recovery (Cross et al., 2003). Despite the far-reaching implications of these early interactions, a comprehensive synthesis of stakeholder experiences, encompassing children, young people (CYP), parents, and service providers, remains lacking.
Evidence indicates that the quality and consistency of crisis service provision in this acute period are highly variable. For some children, interventions are experienced as protective and empowering, while others report distressing or retraumatizing encounters (Whitehouse et al., 2025). Caregivers, who may themselves be experiencing shock, anger, or grief, describe gaps in communication, coordination, and support (Van Duin et al., 2022). Professionals face structural and emotional challenges, including resource limitations, procedural constraints, and the psychological toll of working with traumatized children (Middleton & Potter, 2015). Understanding how these perspectives converge and diverge is central to identifying what makes system responses effective in this uniquely sensitive context.
While quantitative studies offer valuable insights into aspects of service provision such as response timelines, prosecution rates and other measurable outcomes, they may fall short in capturing the lived experiences of victim survivors, their parents/carers, and service providers. Understanding these experiences is essential to evaluating not just what services are delivered, but how they are received, interpreted, and felt. For this reason, qualitative studies were selected for inclusion in this review. They are uniquely suited to exploring the complex, emotionally charged, and context-dependent nature of crisis and forensic systems, allowing participants to express their perspectives in their own words (Van Duin et al., 2022).
To synthesize these qualitative findings, meta-aggregation was chosen as the review methodology. This approach enables a structured and transparent synthesis of qualitative evidence while preserving the integrity of participants’ voices and the meanings conveyed in primary studies (Hannes & Lockwood, 2011). Unlike more interpretive methods such as meta-ethnography, which involve re-conceptualizing findings through theoretical frameworks, meta-aggregation focuses on faithfully representing the original findings and grouping them into actionable categories. The result is a set of synthesized statements that can be directly translated into practice and policy recommendations (Lockwood et al., 2015). Such recommendations are significant in the context of child sexual assault, where ethical imperatives demand that survivors’ experiences, and those of their caregivers and the professionals who support them, are not only documented but meaningfully incorporated into system reform. Meta-aggregation thus provides a rigorous yet respectful way to elevate lived experience into evidence that can inform service design, delivery, and evaluation.
This systematic review and meta-aggregation, therefore, aims to consolidate existing evidence on the experience of service provision in the immediate aftermath of child sexual assault. By examining the experiences of CYP, their parents and carers, and the professionals who support them, the review seeks to identify common themes, unmet needs, and opportunities for improvement. In doing so, it provides an evidence base to inform more effective, coordinated, and trauma-informed crisis interventions that can improve outcomes for those affected by child sexual assault.
Methods
A predefined protocol was registered prospectively in International Prospective Register of Systematic Reviews (PROSPERO; CRD42024553960) to mitigate bias and enhance transparency. Reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses ( PRISMA; Moher et al., 2009) guidelines, with systematic documentation of the search strategy, study screening, and selection processes to ensure reproducibility.
Data synthesis employed the Joanna Briggs Institute (JBI) meta-aggregation approach, a structured methodology that preserves the contextual meaning of primary qualitative findings while enabling their integration into higher-order interpretations (Lockwood et al., 2015). This process systematically consolidated experiential data from children, caregivers, and service providers, generating evidence-based insights with practical implications. Given the diversity of ontological and epistemological positions across the included studies, we followed the JBI meta-aggregation approach, which preserves each study’s findings at face value without re-interpretation through a single paradigm. This allowed us to respect methodological heterogeneity while synthesizing findings into categories and overarching statements in a transparent and reproducible way.
Inclusion Criteria
Participants
Children and young people (aged up to 18 years) who had experiences of crisis services within 72 hrs of their report of sexual assault.
Parents, carers, and guardians of those child victims.
Professionals involved in the crisis/acute response to child sexual assault.
Phenomenon of Interest
The phenomena of interest for this review were experiences with the provision of care provided to children and young people following the disclosure of recent child sexual assault, where that assault was believed to have taken place within the previous 72 hrs. Child sexual assault was defined as any sexual act imposed on a child by an adult, peer-aged or older adolescent that violates the child’s bodily integrity, autonomy, and trust (Mathews & Collin-Vézina, 2019). The experiences and perspectives of their parents/carers as well as service providers (medical, forensic/police and psychosocial) were also sought.
Context
This review will consider any setting where children and adolescents receive a justice, health, or psychosocial support response in the first 72 hrs following the report of sexual assault.
Types of Studies
The review considered qualitative studies including, but not limited to, designs such as phenomenology, grounded theory, and ethnography.
Patient and Public Involvement
No patient participated in the design, planning, and conception of this study.
Search Strategy
To ensure a comprehensive evidence base, our search strategy targeted both published and gray literature. The process consisted of three key steps (Aromataris & Pearson, 2014):
Preliminary Search & Term Identification: An initial limited search in MEDLINE was performed, followed by an analysis of text words in titles/abstracts and relevant index terms (e.g., MeSH).
Systematic Database Search: Using the identified keywords and controlled vocabulary, a full search was conducted across MEDLINE, EMBASE, CINAHL, Social Sciences (ProQuest) and PsycINFO on May 6, 2024. A second search was undertaken on June 5th, 2025. Search terms encompassed child, adolescent, parent/caregiver, and service provider experiences related to crisis responses to child sexual assault.
Gray literature searches: The search for gray literature was sourced through a search of ProQuest Dissertation & Theses, on June 7th, 2024, as well as a customized Google Scholar search in both June 2024 and 2025.
The timeline of inclusion was from database inception to May 6, 2024. A second search of all 5 databases was undertaken on June 5, 2025, to ensure the inclusion of more recent studies. Due to a lack of translation resources, only studies published in English were included. The complete search syntax for all databases and gray literature sources is provided in Supplemental Table 1.
Study Selection
Following the search, all identified citations were collated and uploaded into EndNote (Version X9 [Clarivate Analytics, PA, USA]). Then, into Covidence (Veritas Health Innovation, Melbourne, Australia), where duplicate citations were removed. One independent reviewer (C.W.) screened the title and abstract of each paper against the review’s inclusion criteria. A second and third reviewer assessed a random sample of studies to ensure consistency. Together, three independent reviewers assessed 1,032 items with 91.8% overall agreement (Cohen’s κ = 0.52, moderate). All disagreements were resolved through consensus discussion (Cohen, 1960). Studies identified as potentially eligible or those without an abstract were retrieved for full text review. Full texts were reviewed by C.W. and C.H. Full texts that did not meet the review inclusion criteria were excluded. Any disagreements between the reviewers were again resolved through discussion.
Data Extraction
Two reviewers (C.W. and C.H.) independently extracted data from papers by using a mutually agreed upon, standardized data extraction tool. Findings were extracted primarily from Results/Findings sections of the included studies, with contextual information drawn from Methods and Discussion sections where relevant. The extracted data included Study characteristics, context, geographical location, study methods, and the phenomena of interest relevant to the review question (i.e., experiences of CYP, their parents/carers, and service providers during provision of care). Studies were grouped according to population. Findings and their illustrations were extracted and assigned a level of credibility (Supplemental Table 2; Lockwood et al., 2015).
Data Synthesis
Qualitative research findings from each population (children, parents, service providers) were aggregated using a meta-aggregation approach (Lockwood et al., 2015). The process to synthesize followed a three-step approach. First, individual extracted study findings were rated as either unequivocal (evidence beyond reasonable doubt), credible (contains illustrations that may be challenged), or unsupported (when findings were not supported; Munn et al., 2014). Second, findings of all included studies were extracted and categorized to create a set of categories representing meaningful similarities. Third, similar categories were further synthesized to obtain a comprehensive set of synthesized findings, which were used to develop evidence-based recommendations for practice.
Assessing Certainty in the Findings
The final findings were graded according to the ConQual approach for establishing confidence in the output of research synthesis and presented in a summary of findings (Munn et al., 2014). The ConQual process was used to analyze the level of confidence or trust that exists in the value and level of evidence of each synthesized finding, as shown in Supplemental Table 2.
Results
Review results are reported in accordance with the “Enhancing Transparency in Reporting the Synthesis of Qualitative Research” statement, which consists of 21 items and is appropriate for qualitative evidence synthesis (Supplemental Figure 1; Lockwood et al., 2015).
Study Inclusion
The search strategy yielded 16,475 studies from MEDLINE, EMBASE, CINAHL, PsycINFO, Social Sciences (ProQuest), ProQuest Dissertations and Theses and Google Scholar. A total of 4,951 articles were removed as duplicates, which left 11,524 studies that were screened for eligibility by titles and abstracts in Covidence, 10,524 studies were excluded as they were not relevant to the topic. The remaining 100 studies were subject to further detailed assessment by examining the full text, 78 studies were excluded for reasons such as the wrong phenomenon of interest, population, setting and/or study design. Overall, 22 studies were included in the review, as shown in the PRISMA flow chart (Figure 1).
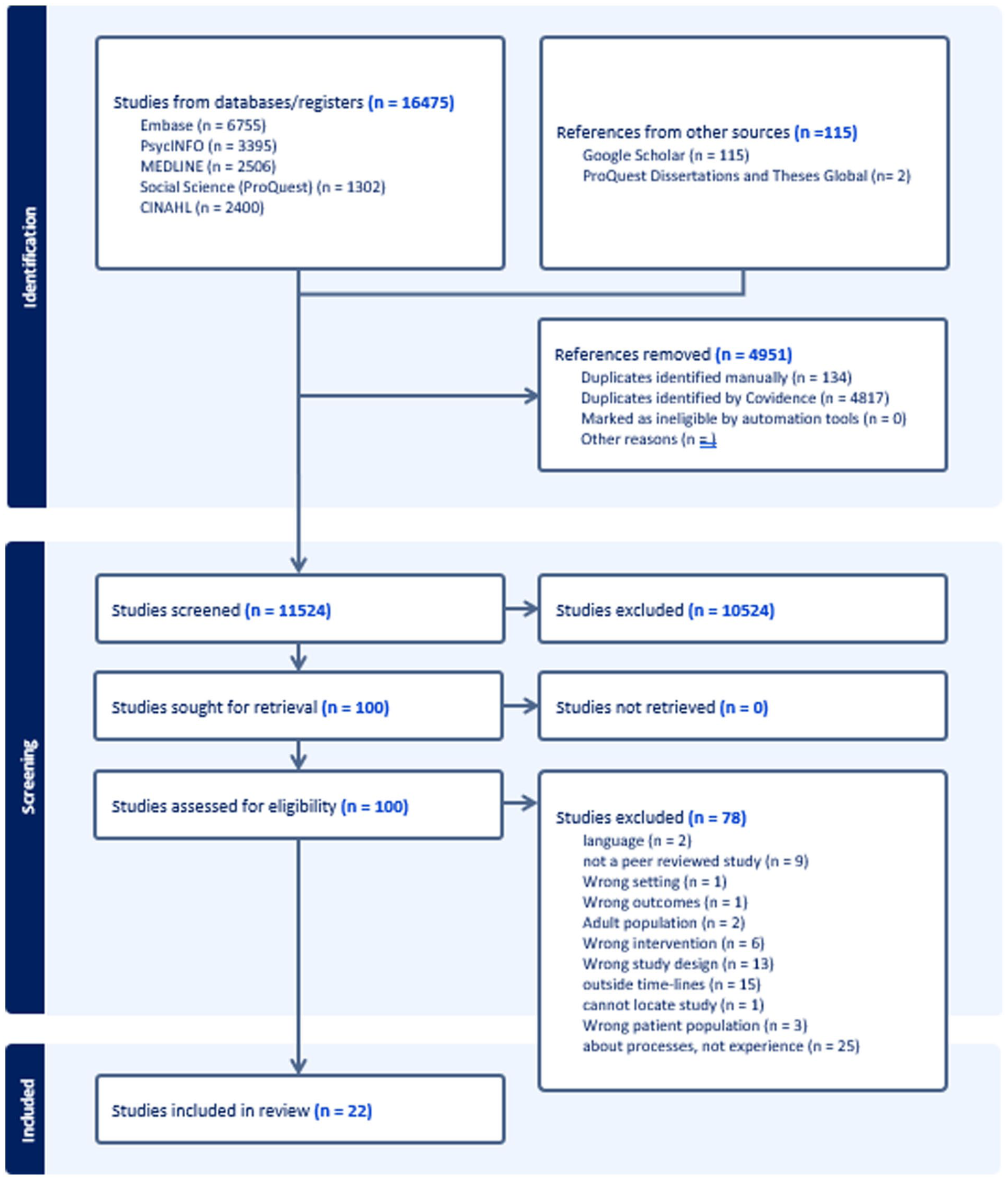
Systematic review of families’ perceptions & experiences of the service system in the hours following child sexual assault.
Methodological Quality
All included studies were critically appraised using the JBI Critical Appraisal Checklist for Qualitative Research (Supplemental Figure 2), a 10-item instrument designed to assess methodological quality and philosophical congruity (Aromataris & Munn, 2017; Hannes et al., 2010). Five criteria (2, 3, 4, 6, and 7) contribute to the ConQual-Dependability rating (Munn et al., 2014), while the remaining criteria assess alignment between philosophical perspective, methodology, and interpretation, as well as ethical and participant representation considerations. All items were scored as “yes,” “no,” or “unclear,” and all studies were included regardless of quality rating (see Table 1).
Qualitative Appraisal.
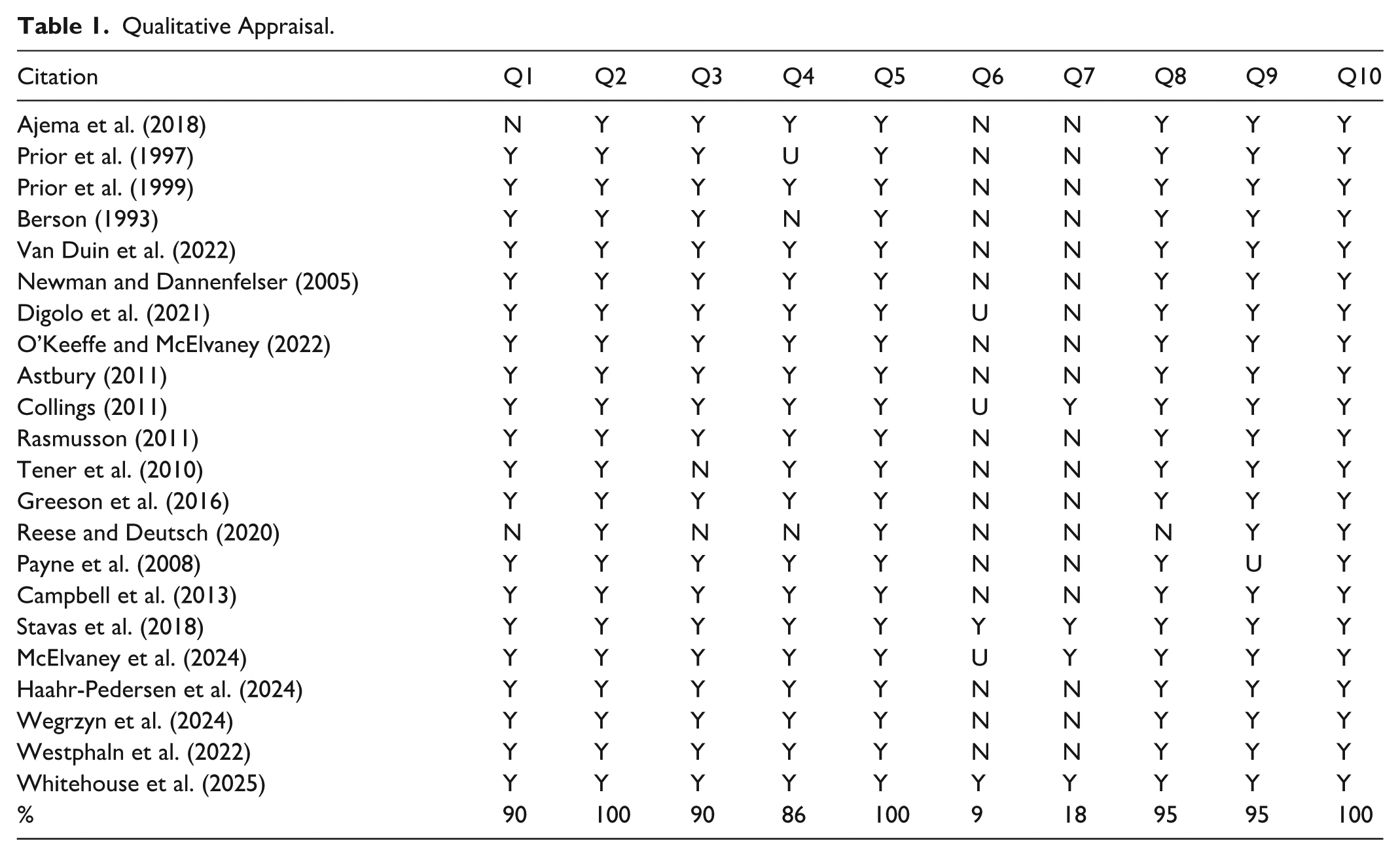
Congruity between methodology and research question (criterion 2) was present in all studies. Criteria 1, 3, 4, and 5—related to philosophical perspective and methodological alignment—were met in 18 of the 22 studies, with exceptions noted for Reese and Deutsch (2020), Tener et al. (2010), Prior et al. (1997), and Berson (1993). Researcher positioning (criterion 6) was absent in 17 studies, unclear in 3 (Collings, 2011; Digolo et al., 2021; McElvaney et al., 2024), and clearly addressed in 2 (Stavas et al., 2018; Whitehouse et al., 2025). Researcher influence (criterion 7) was addressed in 4 studies. Participant voice (criterion 8) was represented in all but one study (Reese & Deutsch, 2020), and ethics approval (criterion 9) was reported in all but one (Payne et al., 2008). Criterion 10, assessing congruity between conclusions and findings, was met in all studies. Any disagreements between reviewers were resolved through discussion.
Characteristics of Included Studies
The studies included in the review were published between 1993 and 2025 and they were from the following countries: Australia (Whitehouse et al.), Canada (McElvaney et al., with Ireland), Denmark (Haahr-Pederson et al.), Ireland (O’Keefe & McIlvaney), Israel (Tener et al.), Kenya (Ajema et al., Diggolo et al.), Malaysia (Nen & Astbury, 2011), South Africa (Collings), Sweden (Rasmusson), The Netherlands (Van Duin et al.), United Kingdom (Prior et al., 1997, 1999), and United States (Berson et al., Campbell et al., Greeson et al., Newman & Dannenfelser, Payne et al., Reece & Deutsch, Stavas et al., Wegrzyn et al., Westphaln et al.). The participants included in the studies were children, youth, parents, or caregivers who had reported their experiences of receiving crisis services in the 72 hrs post-assault. Also, the experiences of professionals who provide these crisis services were included. Children and young people’s ages ranged between 4 and 18 years old. The ages of participants were not noted in the studies of parents/carers or service providers. The sample size of the participants in the individual studies ranged from 1 to 35. A range of qualitative methodologies was used including semi-structured interviews and focus groups. The main phenomenon of interest across the studies were the experiences of children and young people and the way that parents, service providers and systems experience, help, and hinder children during the first 72 hrs following the report of sexual assault. Some studies were specific to the importance of collaboration and proper resourcing of professional groups, but this too was seen as a means to an end; the professionals being concerned for the welfare of their young charges. The settings of all studies were hospitals, Child Advocacy Centers (CACs), police stations, and social service settings (Supplemental Table 3).
Review Findings
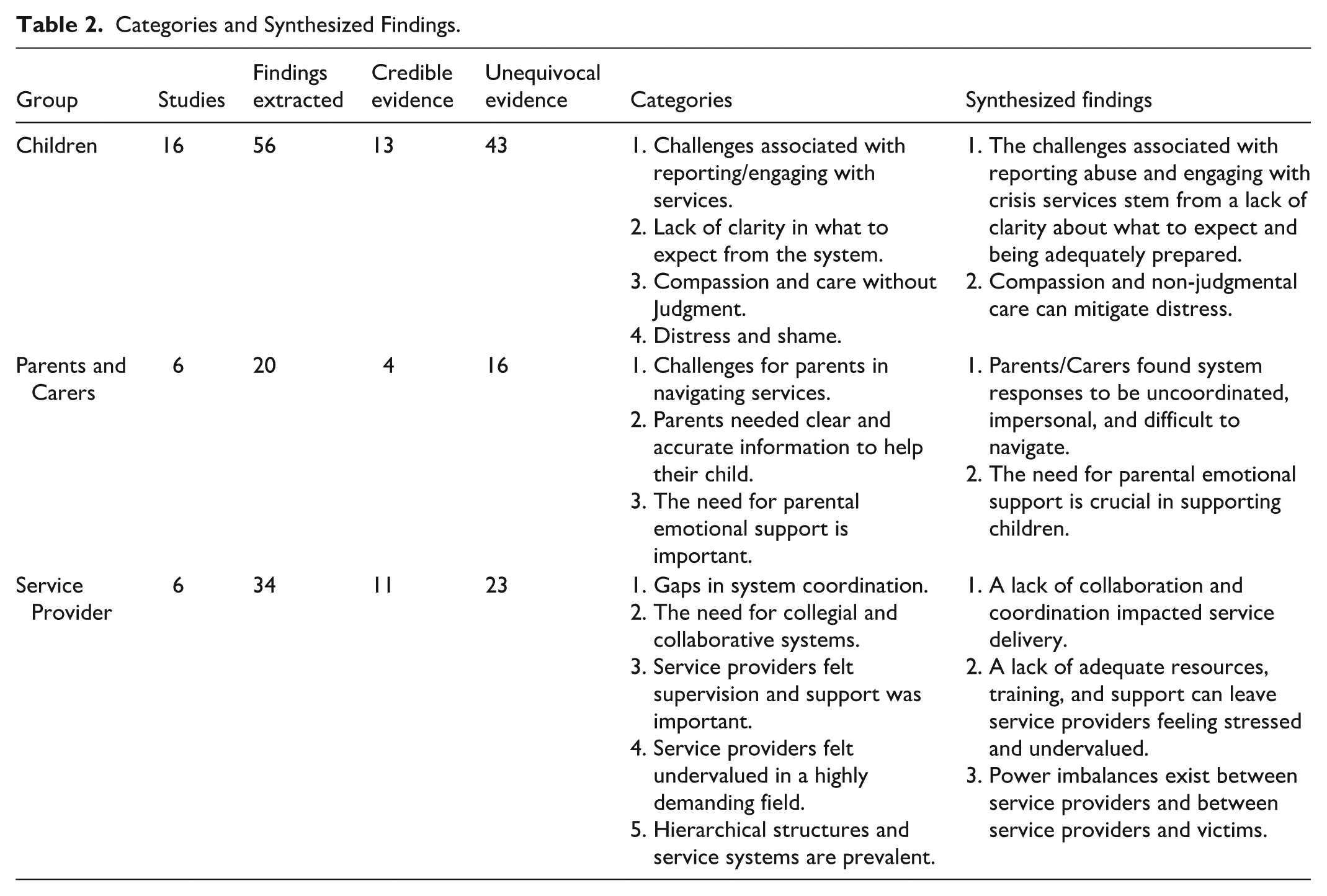
There were 22 studies that met the inclusion criteria. Some of the studies included more than one population of interest. There were 16 studies that examined the experiences of children and young people. Six studies reported on the experiences of parents and carers and six studies reported on the experiences of service providers.
Table 2 summarizes the categories and synthesized findings for each population.
Categories and Synthesized Findings.
Children and Young People. Synthesized Finding 1: The Challenges Associated With Reporting Abuse and Engaging With Crisis Services Stem From a Lack of Clarity About What to Expect From the System
This synthesized finding was generated from the aggregation of two categories, underpinned by 29 extracted findings. The two categories were “Challenges associated with reporting/engaging with services,” and “Lack of clarity in what to expect from the system.”
Children and young people frequently described feeling unprepared and confused when navigating crisis services post-assault, exacerbating their distress. Many reported entering medical and legal processes with little understanding of procedures, leaving them feeling anxious and vulnerable. One participant in Stavas et al. (2018) recalled, “I was a little nervous because I didn’t know what the exam entailed, what the process was or what was gonna take place.” Other studies emphasized how transparent communication could alleviate fear, as one young person noted:
She (the nurse) told me everything else she was doing . . . it was my first gynecologist exam, so I was, it was very, they were very nice about it and told me exactly what they were doing (Campbell et al., 2013).
However, systemic failures often left children and young people without guidance, compounding trauma. A participant in Collings (2011) recounted being turned away without support: “They told us that they could not help us. They told us we needed to report the rape at another police station, and we did not have money to go there.” Others in the Collings study described feeling adrift in bureaucratic processes, with one stating:
At the hospital they told my mother that the social worker was not there . . . they said they would phone her, but they never did. Then they told my mother to phone a free number, but she could not get through (Collings, 2011).
The absence of clear, consistent information intensified feelings of helplessness, as another participant in the same study explained: “I didn’t know what was happening, or what was going to happen next (Collings, 2011).”
For many, the lack of preparation extended to not knowing who was present, how long procedures may take, or whether their privacy would be respected. One young person in the study by O’Keefe et al. (2022) shared:
I did not really have any clue whatsoever before I went in, I find it awkward talking to someone about it, so I did not ask . . . I’m like “how long is it going to take?” or “who is going to be in the room?” or like “would someone else be getting it done at the same time?”, “would I be the only one?” or like if I wasn’t “would other people know that I’m there for that reason as well?” (O’Keefe et al., 2022). Such uncertainty often deterred disclosure, as children feared stigma or retraumatization.
Children and Young People Synthesized Finding 2: Compassion and Non-judgmental Care Can Mitigate Distress
This synthesized finding was generated from the aggregation of two categories, underpinned by 27 extracted findings. The two categories were Compassion & Care without judgment and “Distress and Shame.” When services were delivered with patience, kindness, and respect for autonomy, children reported significantly better experiences.
I like how calm the police were and how they listened to me (. . .) I could tell that when I was saying something they really looked at me and was like “yes, and how did you feel about that.” I think that it was really nice that they were thinking about how I felt (Haahr-Pedersen et al., 2024).
Participants in the reviewed studies emphasized the importance of providers who listened without judgment, explained processes clearly, and empowered them to make decisions. One young person described a positive interaction: “Uh, she took the time to listen to me when I had something to say” (McElvaney et al., 2024), and another; “The main thing was that they were really understanding. Like, if they asked me something and I didn’t understand it, then they’d explain it to me” (Prior et al., 1997). Another appreciated how a nurse “made sure I knew what she was doing and that I was comfortable with it . . . she told me I didn’t have to do anything I wasn’t okay with” (Campbell et al., 2013).
Conversely, perceived indifference or blame from providers deepened shame and sometimes led to a reluctance to engage. One participant in the Greeson et al. (2016) study recounted a dismissive police officer:
He kept saying, “We’ve got people coming in here all the time making stuff up’ . . . It felt like he didn’t believe me.” This young participant went on to say, “So, it just didn’t seem like he really cared to listen.”
Others described interactions that left them feeling stigmatized or powerless, such as a social worker who “used to scare me, the way she looked at you . . . if I said something, she’d start huffing and puffing (Prior et al., 1999).” A recurring theme was the internalization of blame, with one participant reflecting, “I felt ashamed, like I had done something wrong . . . I just wished it wasn’t insinuated that the victim was to blame” (O’Keefe et al., 2022).
In contrast, trauma-informed approaches (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014) such as offering choices, validating emotions, and attempts at genuine connection appeared to foster trust. One participant noted how a provider’s kindness helped alleviate their distress: “It helped a lot for them to be nice . . . to tell my story and not feel uncomfortable or nervous” (Campbell et al., 2013). Another described relief after speaking with police who “listened to everything I had to say . . . and told me I was going to a safe place” (Collings, 2011). Simple gestures, like providers eschewing uniforms to create a less formal atmosphere, also made a difference: “They didn’t have uniforms . . . it was just sitting there talking to someone, and it felt good” (Rasmusson, 2011).
Parents and Carer’s Synthesized Finding 1: Parents and Carers Found System Responses to be Uncoordinated, Impersonal, and Difficult to Navigate
This synthesized finding was generated from the aggregation of two categories, underpinned by 13 extracted findings. The two categories were: Challenges for parents to navigate services’ and “Parents needed clear and accurate information in order to help their child.” Parents and carers frequently describe fragmented, bureaucratic, and emotionally draining experiences when seeking help for their child. Many reported poor communications between agencies, leaving them to manage crises without support. One parent recounted a devastating lapse in coordination:
After we reported to police, I took my child to our doctor’s clinic, and I text the police saying, “I’m just here at the clinic, because I want her seen” and she said, “Look don’t worry about it, go home . . . we’ll call you about taking her to hospital.” But I wanted something there and then because to me . . . I was just . . . The time was ticking, and I just didn’t want to leave it any longer . . . So then I thought, well okay, I’ll just have to go home and wait . . . And then we didn’t get in (to hospital) until the following day, which left it I think closer to 40 hours or something like that. And it was just too much time to have to wait, to have to let children wait. And I got told I was going to get a call first thing in the morning. And so, I waited, waited, waited, and I didn’t get that call. So, I then had to follow up. (Whitehouse et al., 2025)
Others highlighted how systemic inefficiencies eroded trust, with one carer noting:
They were there to enforce the rules, and that was it. You weren’t even people to them—they didn’t take time to know your name. It’s not their fault; it’s the workload. But it’s impossible to form a relationship with someone that overwhelmed (Prior et al., 1998).
Long wait times and logistical barriers further compounded distress. A participant described, “You have to wait more than an hour at every point” (Ajema et al., 2018), while another emphasized the physical and financial strain of accessing care: “The distance between facilities was unbearable. We were referred to a hospital 34 km away before receiving emergency help” (Ajema et al., 2018). Parents also expressed frustration over the lack of transparency about processes, leaving them unprepared to advocate for their child. One explained: “It wasn’t automatically clear what had to happen—legal steps, police reports, medical and psychological care for the child, support for us. If we’d known, we could’ve said, ‘This is what we want, and this is what we don’t’ (Van Duin et al., 2022).”
Parents and Carers Synthesized Finding 2: The Need for Parental Emotional Support Is Crucial in Supporting Children
This synthesized finding was generated from one category, underpinned by 7 extracted findings. The category was: “The need for parental support is crucial to support children.” Parents and carers emphasized that their own emotional well-being directly impacted their ability to support their child. Those who received empathic and consistent care described markedly better coping. One parent praised a provider who “showed huge understanding, was always there . . . when they were needed. I can very well imagine, if they hadn’t been there, it would have been so much more difficult . . . We were given every opportunity to ask questions (Van Duin et al., 2022).”
Another highlighted the value of feeling “heard”: “I found her (the social worker) very sincere and a very good listener . . . I felt she really cared about us (Prior et al., 1999).”
Conversely, the absence of support left parents feeling isolated and destabilized. One recounted the moment of crisis: “All at once . . . at that very moment, somebody pulls a rug out from under you. And you start falling, and that doesn’t stop for the next 2 days (Van Duin et al., 2022).”
Another felt abandoned by professionals and processes:
What am I going to read off there? It’s not going to tell me how to deal with it. What do I do now when I get her home? I have never dealt with anyone that’s been . . . Had anything like that happen so I’m at a loss. All I can think of is, put her to bed, see how she’s in the morning. And then what? (Whitehouse et al., 2025)
Without adequate emotional scaffolding, parents struggled to manage their own trauma while guiding their child through systems that often retraumatized both.
Service Providers Synthesized Finding 1: A Lack of Collaboration and Coordination Impacts Service Delivery
This synthesized finding was generated from two categories, underpinned by 20 extracted findings. The categories were: “Gaps in system coordination” and “The need for collegial and collaborative systems.” Service providers across disciplines, including law enforcement, child protective services (CPS), medical personnel, and social workers, described professional and service silos as a major barrier to effective care. Competing protocols, territorialism, and poor interagency communication often undermined investigations and victim support. One law enforcement officer noted, “CPS workers will interview the perpetrator before law enforcement does, and that can mess up the criminal case. If the perpetrator knows they’re a suspect, they can leave or change their story.” Another highlighted jurisdictional conflicts: “Everyone wants to control the investigations. There can be a tug-of-war regarding who is in charge” (Newman & Dannenfelser, 2005).
Providers also emphasized how bureaucratic inefficiencies delayed or derailed interventions. A social worker explained:
The hospitals and the medical systems require so many steps . . . it becomes a disservice. It’s just been trying to work through those structural barriers. And it is, immense. I mean, it is not a one prong situation. Each health institution has at least 20 to 50 prongs (Westphaln et al., 2022).
Others lamented the toll on victims: “At the end, the victim suffers most. She needs to repeat the story from one person to another (Nen & Astbury, 2011).”
Conversely, interdisciplinary collaboration improved outcomes. A provider described the value of trust-building: “I’ve gotten to know colleagues who I never knew before . . . Now I know who these people are. I know what resources are out there . . . So I think that’s very helpful (Westphaln et al., 2022).”
Service Providers Synthesized Finding 2: Inadequate Resources, Training, and Support Leave Providers Feeling Stressed and Undervalued
This synthesized finding was generated from two categories, underpinned by 10 extracted findings. The categories were: “Service providers felt supervision and support was important’ and Service providers felt undervalued in a highly demanding field.” Providers universally cited resource shortages as a critical challenge, with underfunding exacerbating caseloads and burnout. One bluntly stated, “Funding. Funding. Funding” (Payne et al., 2008), while another noted, “We have many cases but can only help a few . . . Even now, we have our hands full (Nen & Astbury, 2011).”
Lack of institutional support compounded stress. A provider described punitive leadership:
“Superior officers tend to be harsh whenever you make mistakes . . . They treated you as if you didn’t work hard on the case . . . They never tried to hear our problems” (Nen & Astbury, 2011). Others highlighted inadequate staffing: “because an urgent response is needed, you have to neglect other cases” (Nen & Astbury, 2011).
However, well-resourced, trauma-informed environments fostered better care. One provider praised a facility with dedicated interview rooms:
Kids seem to make themselves at home here. They love writing on the whiteboard tables . . . The medical is fine; everything looks so nice in the exam room . . . The therapy room is a great private place to talk to families after the interview (Westphaln et al., 2022).
Another credited grants for “really good interview equipment, really good teleconferencing equipment, video viewing equipment, furniture for live, in-person meetings . . . All of those things bring the agencies together . . . (Westphaln et al., 2022).”
Service Providers Synthesized Finding 3: Power Imbalances Existed Between Providers and Between Providers and Victims
This synthesized finding was generated from one category, underpinned by four extracted findings. The category was: “Hierarchical structures and service systems are prevalent.” Providers identified hierarchies that marginalized certain roles, particularly social workers. One noted,
“. . . it is not uncommon for the (social worker) in a hospital to be the first person to receive a case, who know the whole thing . . . but she/her has no power over the case. She/he may participate in a group discussion, but she/he is not recognized as a protector (Nen & Astbury, 2011).” Others described territorialism within teams: “Some of the team kind of get territorial . . . It’s like, this is the way we’ve been doing it . . . Sometimes it can be very frustrating (Westphaln et al., 2022).”
Victim blaming and racial bias further eroded trust. A participant criticized training curricula: “Local curriculum includes victim blaming,” suggesting that law enforcement officers are learning to blame victims “before they even encounter these cases (Payne et al., 2008).” Another shared an example of racial inequity:
I’ve had clients that were . . . frustrated their child was sexually assaulted and they felt as though the entire child welfare system wasn’t taking them seriously . . . They felt they were given the run around because they were African American (Westphaln et al., 2022).
Discussion
The experiences of CYP, and their parents and caregivers navigating service systems after reporting acute sexual assault reveal a dissonance between the intentions of institutions and lived realities of receiving their care. Participants in the studies included in the review sometimes encountered processes that may have inadvertently perpetuated their trauma rather than facilitate their healing, with forensic and medical procedures often perceived as objectifying or dismissive of developmental needs (Berson, 1993; Collings, 2011). Young people described feeling reduced to sites of evidence collection within systems that appear to prioritize procedural efficiency over psychological safety (Campbell et al., 2013; O’Keeffe et al., 2022; Whitehouse et al., 2025). Such accounts align with broader conceptualizations wherein systems designed to protect instead perpetuate harm through inflexible protocols and inadequate trauma responsiveness (Greeson et al., 2016). For marginalized youth, these challenges may be compounded by misinterpretations of trauma responses and systemic biases that further alienate those already distrustful of institutional interventions (Reece & Deutsch, 2020).
A recurring theme across studies is the absence of developmentally appropriate communication, leaving children unprepared for invasive examinations or abrupt separations from caregivers (Rasmusson, 2011; Van Duin et al., 2022). Younger children, whose developmental capacities may limit their ability to process directions from professionals, are especially vulnerable to distress when procedures lack transparency or agency (Stavas et al., 2018). Yet research also highlights promising alternatives, such as trauma-informed modifications that incorporate visual aids, child-led pacing, or narrative techniques to restore a sense of control (Tener et al., 2010; Westphaln et al., 2022). Models like Barnahus, which integrate forensic, medical, and therapeutic services under one child-centered framework, demonstrate that objectives for justice need not come at the expense of psychological well-being (Rasmusson, 2011).
Caregivers face parallel challenges as they navigate systems that often neglect their dual roles as advocates for their children and as secondary victim survivors in their own right. Many report inconsistent or absent guidance on legal and medical processes, leaving them ill-equipped to mitigate their child’s distress or navigate complex bureaucratic landscapes (Digolo et al., 2021; Van Duin et al., 2022; Whitehouse et al., 2025). This lack of support can exacerbate anxiety and, in some cases, lead to disengagement from essential services (Ajema et al., 2018). However, relational approaches such as trauma-informed psychoeducation, designated case liaisons, and the inclusion and validation of caregivers’ expertise, have been shown to enhance resilience and improve outcomes for both children and families (Reece et al., 2020; Westphaln et al., 2022). These findings highlight the necessity of integrating caregiver support into systemic responses rather than treating it as ancillary to child-focused interventions.
Frontline providers, meanwhile, articulate the ethical and operational tensions inherent in systems that demand trauma-informed care but fail to supply the necessary resources or structural support. Underfunding, interagency fragmentation, and competing professional priorities can hinder effective collaboration, leaving professionals navigating conflicting mandates (Newman & Dannenfelser, 2005). Racial and disability-related disparities appear to, at times, further complicate service delivery, with marginalized populations frequently encountering additional barriers to care (Payne et al., 2008; Reece & Deutsch, 2020). Such systemic shortcomings not only undermine intervention efficacy but also contribute to secondary traumatic stress among providers, who report moral injury when forced to prioritize bureaucratic requirements over a child’s emotional needs (Campbell et al., 2013; O’Keeffe et al., 2022).
Collectively, these findings challenge systems to move beyond fragmented, reactive approaches and toward models that honor the interdependence of children, families, and providers. Trauma-informed frameworks, though widely endorsed, must be operationalized in ways that address power imbalances, resource inequities, and the unique needs of marginalized populations (Greeson et al., 2016; Payne et al., 2008). Evidence from successful models like Barnahus and CAC’s suggest that systemic change is achievable when child-centered principles are structurally embedded rather than superficially adopted (Digolo et al., 2021; Rasmusson, 2011). The immediacy of post-assault care demands systems that prioritize coordination over bureaucracy, yet the implementation of centralized models remains uneven (Herbert & Bromfield, 2015). Similarly, the pervasive lack of trauma-informed practices calls for training and collaboration tied to measurable competencies. The emotional labor of providers, often rendered invisible, must also be formally acknowledged through operational, clinical, and supportive supervision, workload protections, and mental health support.
These gaps and alignments between current practices and established international guidelines are striking. The emphasis on coordinated, trauma-informed care resonates with the Lanzarote Convention (Council of Europe, 2007), which mandates integrated, child-centered responses to sexual violence. Yet persistent service fragmentation, despite evidence supporting centralized models, reveals a dissonance between policy intent and implementation, particularly in resource-limited contexts (National Children’s Alliance, 2020). This, in turn, aligns with the WHO’s (2017) advocacy for trauma-informed, multi-sectoral care, which nonetheless acknowledges systemic barriers to equity in low-income settings. The review’s critique of training standards further reflects gaps in the WHO’s framework, which prioritizes competency-based protocols but lacks enforcement mechanisms. Finally, the invisibility of providers’ emotional labor contrasts sharply with the International Labour Organization’s (2022) guidelines on workplace mental health, underscoring the need for institutional accountability.
In summary, this review maps the lived realities of crisis service engagement during a period of profound vulnerability, offering not just a critique but a pathway for transforming post-sexual assault care for CYP, and their families. The findings challenge systems to reconcile procedural demands with developmental sensitivity, interdisciplinary collaboration, and the integration of lived experience into policy design.
Implications for Research, Policy, and Practice
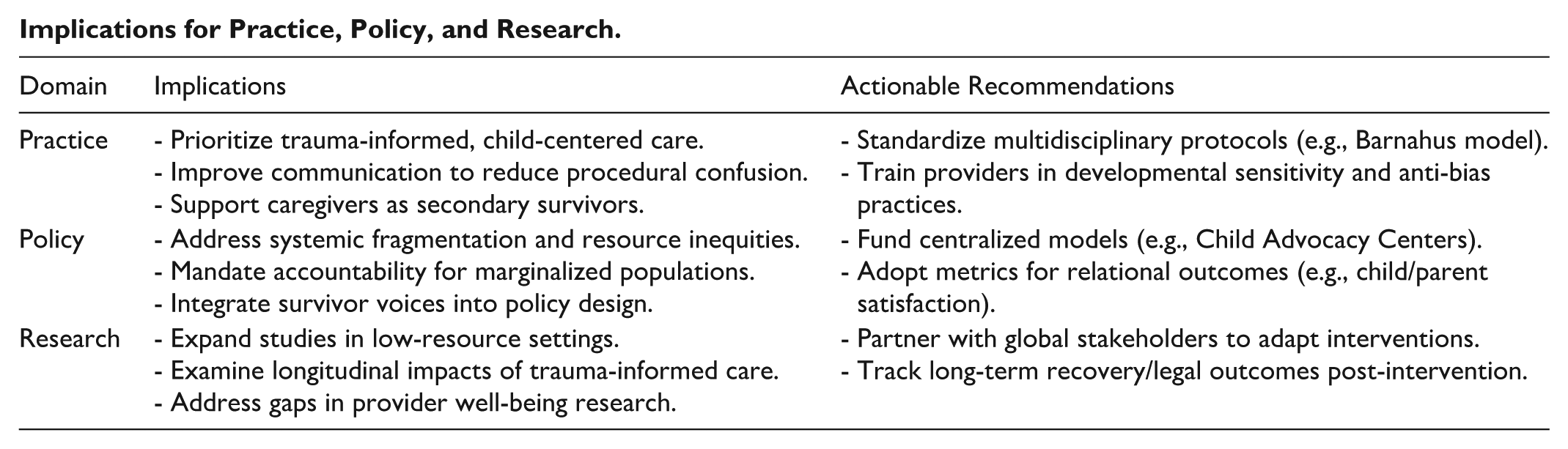
The synthesis of evidence presented in this review calls for a reimagining of how systems conceptualize and respond to acute child sexual assault. While the Discussion highlighted what is often a dissonance between institutional structures and lived experiences, the path forward requires a paradigm shift toward restorative (trauma transformative) systems (Tucci et al., 2024). Central to this shift is the recognition that trauma responsiveness cannot be achieved through isolated interventions but must be woven into the fabric of institutional design, from frontline interactions to policy governance (Haahr-Pederson et al., 2024).
For practice, this means not only the adoption of trauma-informed principles but a confrontation with the structural barriers that can render them ineffective. Children’s experiences of procedural confusion and caregivers’ struggle with opaque systems reveal a critical need for operational transparency; that is, protocols that are not only standardized but also demystified through developmentally appropriate communication and shared decision-making. Of course, consistency should not come at the cost of flexibility. Systems must balance uniformity with the capacity to adapt to individual needs, particularly for vulnerable children and young people whose trauma responses can be misunderstood (SAMHSA, 2014). The relational dimensions of care, at all stages of the response, must be prioritized alongside procedural rigor, ensuring that children and families are engaged as active participants rather than passive subjects of intervention.
At the policy level, accountability mechanisms must evolve to address not just service delivery but systemic equity. The persistent gaps in access and quality for marginalized communities, seemingly rooted in racialized disparities, geographic inequities, or institutional bias, must be addressed. Policy frameworks should mandate anti-oppressive practices, to identify and rectify disparities in attrition, referral, and engagement. Equally vital is the redistribution of power in policy design itself. Survivor-led organizations and community advocates could have formal roles in shaping interventions, ensuring systems are answerable to those they serve. The Barnahus and CAC models demonstrate that structural integration is achievable, but their principles must be adapted (and resourced) to address localized contexts and cultures.
Underpinning these changes is the need to redefine institutional success. Metrics focused on throughput, or rates of prosecution must be supplemented by measures of relational outcomes: Do children feel heard? Do caregivers feel equipped? Do providers feel ethically supported? This reorientation acknowledges that the path after trauma is not a linear process but a relational one, requiring systems to place a high value on dignity.
Strengths and Limitations
This systematic review provides a comprehensive synthesis of qualitative evidence on the experiences of CYP, parents/carers, and service providers in the immediate aftermath of child sexual assault. A key strength is its inclusion of diverse stakeholder perspectives, which illuminates the complex interplay between individual trauma and systemic responses. By integrating accounts from survivors, caregivers, and professionals, the review highlights how structural inefficiencies, relational dynamics, and resource disparities shape outcomes during this critical period. The findings are further strengthened by their alignment with trauma-informed care principles (SAMHSA, 2014), reinforcing the empirical basis for policy and practice reforms. Additionally, the review’s focus on the immediate post-assault phase, a pivotal yet often neglected dimension of child abuse research, fills an important gap in the literature, offering actionable insights for improving crisis response systems.
However, several limitations must be acknowledged. While the review includes studies from both high-income and developing countries, the majority of evidence derives from well-resourced settings, potentially limiting the transferability of findings to low- and middle-income contexts. The studies from developing nations highlighted particluar challenges, such as severe resource constraints and insufficient provider training, which may exacerbate systemic fragmentation in ways not fully captured by data from higher-resourced systems. This disparity suggests that while trauma-informed interventions may be broadly relevant, their implementation must be adapted to local realities, including infrastructure limitations and cultural norms around disclosure and support.
Selection bias within primary studies is another concern, as participants who engage with research may not fully represent those who disengage from services due to distrust or the chaotic aftermath of sexual assault.
Finally, while the review identifies trauma-informed care as a key mitigator of distress, the absence of longitudinal data in the literature limits conclusions about its sustained impact on recovery or legal outcomes. These limitations highlight the need for further research, particularly in underrepresented regions, to explore how structural inequities and cultural contexts shape post-assault care. Nevertheless, the review’s findings offer a critical foundation for rethinking crisis responses, emphasizing the necessity of adaptable, context-sensitive approaches that prioritize survivor needs amid varying resource constraints.
Summary of Critical Findings.
Implications for Practice, Policy, and Research.
Supplemental Material
sj-docx-1-tva-10.1177_15248380251397418 – Supplemental material for Fractured Systems, Compounded Trauma: A Systematic Review and Meta-Aggregation of Crisis Service Experiences After Child Sexual Assault
Supplemental material, sj-docx-1-tva-10.1177_15248380251397418 for Fractured Systems, Compounded Trauma: A Systematic Review and Meta-Aggregation of Crisis Service Experiences After Child Sexual Assault by Caroline Whitehouse, Peter McKenzie, Carmel Hobbs, Angela Johns-Hayden, Jessica Opie and Hanan Khalil in Trauma, Violence, & Abuse
Footnotes
Ethical Considerations
As this was a systematic review, ethics approval was not required.
Author Contributions
Conceptualization: C.W., J.O.; Methodology: C.W., H.K. and J.O. contributed equally, A.J.H.; Software: EndNote, Covidence; Formal analysis: C.W., C.H., H.K.; Data curation, C.W., A.J.H., C.H.; Writing-original draft preparation, C.W.; Writing-review and editing, C.W., H.K., P.M.; Visualization: C.W.; Supervision, H.K. and J.O., P.M.; Project Administration, C.W.
All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Institutional Review Board Statement
Not relevant to this work.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.