
Abstract
Adolescent dating violence (ADV) is associated with short- and long-term physical and psychological adverse health outcomes. Therefore, it is crucial to implement prevention strategies to address ADV in settings that serve adolescents. One natural point of contact is healthcare settings, as adolescents may present to these settings due to general health concerns and concerns related to ADV exposure. However, little is known about the state of the science for how adolescent healthcare providers can participate in ADV prevention and work, as well as the potential barriers healthcare providers may face when incorporating ADV prevention strategies into their practice. To advance understanding, a systematic scoping review was conducted to summarize current evidence on (a) ADV prevention strategies in healthcare settings, and (b) healthcare provider perspectives on implementing ADV prevention strategies. The search was conducted in five relevant databases in September 2023. Peer-reviewed articles published in English before September 2023 were included if they addressed at least one study aim. After screening 5786 articles, 11 articles met the inclusion criteria and were included in this review. Overall, there were only a few studies on ADV prevention strategies designed for implementation in healthcare settings. Common barriers identified to implementing ADV prevention strategies included limited time, training, and resources. Facilitators of implementation included ADV response protocols/guidelines and working in collaborative teams. This systematic scoping review demonstrates that further research is needed to develop and evaluate ADV prevention strategies for different healthcare settings, and to understand effective ways to address barriers to implementing these strategies.
Keywords
Introduction
From a developmental perspective, adolescence is often an important period of seeking and forming first romantic and sexual relationships (Exner-Cortens, 2014; Mercy & Tharp, 2015). Although romantic relationships during this time tend to be brief, they play a crucial role in psychosocial development for many youth (Connolly & McIsaac, 2009). Yet, these relationships can also be a source of conflict, sometimes resulting in adolescent dating violence (ADV; Connolly & McIsaac, 2009). ADV, also known as teen dating violence or adolescent relationship abuse, is a type of intimate partner violence (IPV) that affects millions of young people of all genders and sexualities around the world (Clayton et al., 2023; Exner-Cortens et al., 2021; Sardinha et al., 2022; Tomaszewska & Schuster, 2021). ADV is defined as any physical, sexual, or psychological violence, including stalking, that is experienced in dating, sexual, or romantic relationships before the age of majority (in the United States and Canada, age 18) (Centers for Disease Control and Prevention [CDC], 2025) ADV can occur in person as well as online, using new technologies and media (CDC, 2025; Zweig et al., 2014).
ADV is considered to be an adverse childhood experience that occurs at high rates and affects a substantial minority of youth globally (Clayton et al., 2023). In the United States (U.S.), the latest Youth Risk Behavior Surveillance survey found that among students in grades 9 to 12 who reported dating during the 12 months before the survey, 9.7% and 8.5% of students experienced sexual and physical ADV victimization, respectively (Clayton et al., 2023). This is similar to the prevalence reported in Canada (Exner-Cortens et al., 2021). When considering broader structural factors, youth exposed to social marginalization (e.g., based on socioeconomic status, gender, or sexual identities) are generally at greater risk of ADV victimization (Dank et al., 2014; Exner-Cortens et al., 2023; Mercy & Tharp, 2015).
ADV victimization is also linked with adverse physical and psychological health outcomes. Physical consequences of experiencing or using ADV include an increased risk of sustaining physical injuries, such as bruises, burns, cuts, broken bones, or concussions (Callahan et al., 2003; Exner-Cortens et al., 2024; Reidy et al., 2016; Tharp et al., 2017). Psychologically, a recent systematic review found that ADV is longitudinally associated with several adverse outcomes, including decreased well-being, as well as increased internalizing symptoms (depressive, anxiety, or suicidal ideation), externalizing symptoms (antisocial behaviors), and substance use (alcohol, marijuana, or tobacco) (Campo-Tena et al., 2024). ADV is also robustly associated with increased risk of IPV victimization in adulthood (Campo-Tena et al., 2024).
ADV Prevention
From a public health perspective, the prevention of ADV occurs at three levels: primary, secondary, and tertiary (Lantz, 2022; B. X. Lee, 2017). Although there are different goals for each level of prevention, these approaches are not mutually exclusive. Primary prevention involves providing universal interventions that aim to prevent ADV before it occurs, where programs are offered to all youth regardless of whether they have experienced and/or used ADV (Cornelius & Resseguie, 2007; B. X. Lee, 2017). Secondary prevention offers interventions for early detection among youth at greater risk of experiencing or using ADV, due to lived or living experiences (e.g., child maltreatment; Kameg & Constantino, 2020; B. X. Lee, 2017). Tertiary prevention involves the long-term care and treatment of those who have experienced ADV to promote recovery and reduce the potential of long-term adverse health outcomes (Kameg & Constantino, 2020; Lantz, 2022). It is worth noting that tertiary (and sometimes secondary) prevention approaches may also be referred to as “treatments” or “interventions” (National Research Council (US) and Institute of Medicine (US) Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions, 2009).
To date, most attention has been directed towards implementing primary, and to a lesser extent secondary, ADV prevention approaches within school settings (Camacho Soto et al., 2024; Leviton et al., 2015; McNaughton Reyes et al., 2021). A recent meta-analysis conducted by Farmer et al. (2023) explored the effectiveness of randomized controlled trials (RCT) of school-based ADV interventions and found that these interventions were effective in reducing ADV victimization and perpetration 1-year or longer post-baseline. Although school-based programs show promise in preventing ADV, a holistic prevention strategy requires cross-sector efforts that go beyond the school building to reach as many youth as possible in settings where they naturally may be present. One such setting that has been overlooked to date in ADV research is healthcare.
Healthcare Settings
Healthcare settings that could be part of ADV prevention efforts include primary care clinics (e.g., general practitioner or pediatric clinics), school-based healthcare (e.g., school nurse offices, school-based health centers), and urgent care and hospital settings (e.g., emergency departments; ED). Adolescents may present to these settings for a variety of reasons, from routine check-ups to physical injuries and mental health concerns related to ADV exposure (Kameg & Constantino, 2020). As healthcare access and availability can vary across youth (e.g., Wilson & Klein 2000), it is likely important to engage healthcare providers across different settings to engage in primary, secondary, and tertiary ADV prevention strategies, as relevant to their patient population and practice.
Primary healthcare settings offer the opportunity for routine visits and continuous care across the lifespan (or for pediatricians, until adulthood) (Starfield, 2001). Extending the continuum of primary care, school-based healthcare settings provide accessible primary care services directly in schools, where youth at this age spend the majority of their time (Gibson et al., 2013). Primary care providers are generally tasked with screening for healthy and risky behaviors (e.g., substance use, safe sexual practices), providing counselling, and coordinating referrals to general or specialized services (Starfield, 2001). As such, primary care providers in community clinics, schools, and other settings are well-situated to engage in prevention strategies for ADV, including providing psychoeducation on healthy relationships and ADV or referring youth who disclose ADV to specialized services.
Many adolescents—especially those who are socially and structurally marginalized and, as a result, lack access to primary care services—may also visit the ED as their primary or only source of routine healthcare (Wilson & Klein, 2000). Related to ADV specifically, Singh et al. (2014) found that about one in six adolescents ages 14 to 20 seeking ED care reported recent experiences of ADV and that ADV was associated with alcohol and drug misuse and depression. Therefore, implementing ADV prevention strategies in the ED, and possibly other hospital and secondary or tertiary care settings (e.g., urgent care), may be crucial to ensuring that patient populations who primarily rely on emergency services, do not have access to primary care, or may be at higher risk of ADV due to their lived or living experiences, also have the opportunity to receive tailored, ADV-related intervention.
Current Study
Healthcare providers can likely play an important role in ADV prevention strategies due to their frequent contact with a wide range of youth across primary, secondary, and tertiary care settings, including youth who may be experiencing negative health outcomes related to ADV. Yet, little is known about the state and scope of research on implementing such strategies in healthcare settings, including barriers and facilitators that healthcare providers may encounter when engaging in ADV prevention work. Therefore, the purpose of this study was to explore and summarize current evidence on ADV prevention strategies in healthcare settings. For this project, healthcare settings included the many settings that serve adolescents aged 18 and under, including primary care clinics, school-based healthcare services, and hospitals. The primary aim of this study was to understand what types of approaches have been implemented in these settings, and if evaluated, evidence of their effectiveness (Aim 1). The secondary aim of this study was to identify and understand the perspectives of healthcare providers across disciplines (e.g., nurses, physicians), of facilitators, and/or barriers to implementing ADV prevention strategies in their practice (Aim 2). To achieve the study’s purpose, a systematic scoping review methodology was used (Peters et al., 2015). Scoping reviews are appropriate for providing an overview of available evidence (e.g., quantitative, qualitative) on a specific topic when the evidence is heterogeneous in nature. Systematic scoping methodology builds on Arksey and O’Malley (2005)’s work by incorporating a standardized approach (i.e., systematic review methodology) when conducting scoping reviews to improve the robustness of results (Peters et al., 2015).
Methods
Search Strategy
The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews checklist (Tricco et al., 2018). The search protocol for this study was prepared in accordance to Joanna Briggs Institute (JBI) guidelines (Aromataris & Munn, 2020) and uploaded to the Open Science Framework to register the review and increase transparency in research (https://osf.io/b57qu/). To find relevant peer-reviewed literature that addressed the review objectives, five relevant databases were searched: PsycINFO, MEDLINE, CINAHL, SocINDEX, and Scopus. All searches were conducted in the selected databases from September 12–14, 2023. Three search strings were developed: adolescent terms, ADV-related terms, and healthcare setting terms. The search terms were developed for PsycINFO and adapted to all other databases using appropriate keywords and Medical Subject Headings (MeSH) terms (Supplemental Material).
Inclusion and Exclusion Criteria
Searches were restricted to peer-reviewed articles published in English. To be broadly inclusive, no geographical, methodological, or date restrictions were applied. To be included, articles needed to either focus on: (a) ADV victimization and/or perpetration, with primary, secondary, and/or tertiary prevention strategies implemented within a healthcare setting; and/or (b) perceived barriers or facilitators to implementing such strategies as reported by healthcare providers. Healthcare providers were defined as individuals who provided health or medical care or treatment. The target population for these strategies had to be adolescents, with an average age between 10 and 18 years or average grade between grades 6 and 12. The age limit of 18 years was applied because in Canada and the United States, 18 is the age of majority. Prior to this age, then, most youth are considered minors, which impacts their access to healthcare services. Articles were excluded if they did not meet the inclusion criteria or if they were solely focused on ADV screening and detection (i.e., without assessing for benefits or impacts of screening) or immediate medical care for rape or sexual assault (e.g., forensic-related examinations provided by sexual assault nurse examiners). Articles were also excluded if they were non-empirical studies (e.g., commentaries), if the full text was unavailable, or if the article was a duplicate.
Review Procedures
Returns from all databases were exported to Covidence, a systematic review software. Duplicate articles were removed using the Covidence automation tool, as well as manually by the first author (Figure 1). Reference lists of relevant review articles located during the search were screened to identify any additional articles that met the inclusion criteria, but no articles were identified (Figure 1). Screening of all retrieved studies was completed by two independent reviewers (i.e., all studies were double coded). Following independent screening at each step (title/abstract screening and full-text review), the two reviewers met to compare results and reach consensus to resolve any discrepancies in selected or excluded articles. If consensus could not be reached, the second author made the final decision. Interrater agreement for each step was high, with a percent agreement of 99% for title/abstract review and 80% for full-text review.
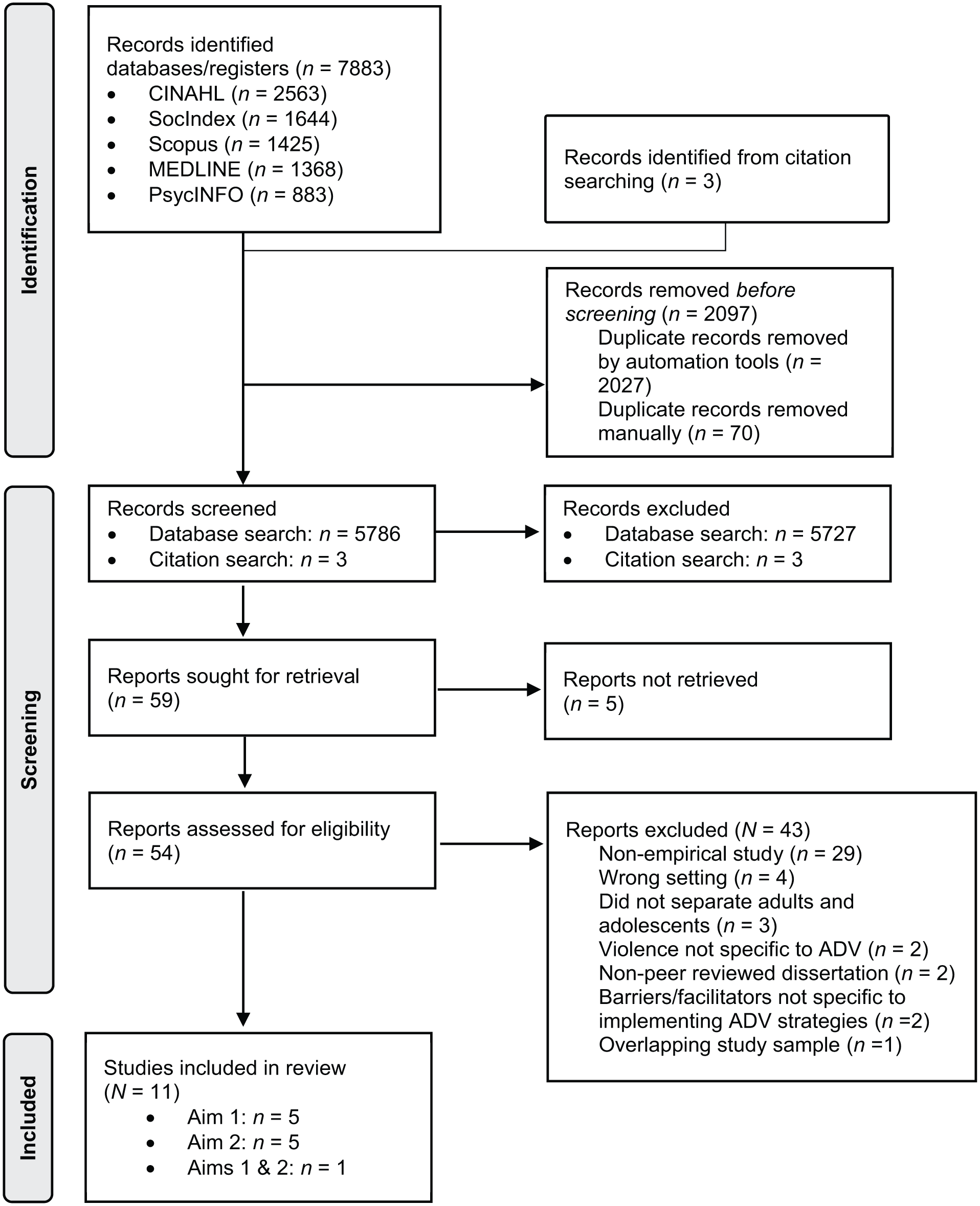
Preferred reporting items for systematic reviews and meta-analyses diagram.
Before starting title/abstract screening, the two reviewers conducted a pilot test to enhance consistency and ensure alignment in screening approaches (Peters et al., 2024). A random sample of 25 titles/abstracts was selected and independently screened by both reviewers using the eligibility criteria. Reviewers met to discuss discrepancies and revised criteria accordingly (e.g., adding the exclusion criterion of sole focus on immediate medical care for sexual violence). Following this pilot test, each reviewer independently screened all titles and abstracts for all 5,786 potential articles (Figure 1). Next, both reviewers independently reviewed 54 full-text articles (Figure 1). From this, 11 articles remained, where five articles addressed Aim 1, five articles addressed Aim 2, and one article addressed both review aims (Figure 1).
Data Extraction and Synthesis
Based on the recommendations of Tricco et al. (2018) and Levac et al. (2010), data relevant to the study aims were extracted from the 11 included articles using a standardized data charting template created in Qualtrics. The first author trialed the extraction form on three articles and then refined and clarified the form with the second reviewer. After the first author completed the data extraction for all included articles, the second reviewer randomly selected and independently reviewed four of the included studies to ensure data extraction was accurate and complete (~1/3 of included articles; Pollock et al., 2023). Since the interrater agreement was adequate on this check (83% agreement), the second reviewer did not extract data for the remaining studies.
Summary tables were used to organize and present the extracted data. For both Aims 1 and 2, the relevant findings were narratively synthesized by healthcare setting type. We chose to organize the results in this way as the services provided and clinical focus across different healthcare settings varies, and so we were interested in exploring if and how interventions or implementation factors were similar within settings. Since scoping reviews are designed to provide an overview of the existing body of literature regardless of quality (Peters et al., 2024), a formal assessment of study quality was not performed. Prevention levels were assigned based on authors’ classification as provided in the article. If an intervention was not classified, the definitions for primary, secondary, and tertiary prevention provided in the Introduction were used to assign the level(s) that the authorship team felt best described the intervention.
Results
Characteristics of Included Articles
Eleven studies met the eligibility criteria and were included in the review (Table 1). Approximately half of these studies were quantitative (n = 6), and the remaining were qualitative (n = 5; Table 1). All articles were published between 2003 and 2023, with the majority published since 2011 (90.9%; Table 1). The majority of studies were conducted in the United States (90.9%), with the remaining one conducted in Spain (Table 1). The youth samples in articles reporting on ADV prevention strategies (Aim 1) ranged between ages 12 and 21 years (Table 1). The youth samples primarily included girls (range 69.9%–85.5%) and Black youth (range 24.0%–68.7% for the 5 of 6 studies that reported on race/ethnicity; Table 1). For Aim 2, of the healthcare provider demographic information provided, the provider samples primarily included women (range 44.0%–98.0% for the 5 of 6 studies that reported on gender) and White providers (range 57.0%–94.1% for the 3 of 6 studies that reported on race/ethnicity; Table 1). For Aim 1, healthcare settings for ADV prevention strategies included school-based healthcare settings (school health centers and nurses’ offices), a university-affiliated adolescent health clinic, and urban hospital settings (pediatric and general EDs, and outpatient care; Table 2). Preventive interventions reported under Aim 1 were at the primary (school-based healthcare settings, n = 2), primary and secondary (primary care setting, n = 1), secondary (ED setting, n =1), and secondary and tertiary (urban hospital setting, n = 2) levels (Table 2). For Aim 2, most articles focused on healthcare providers who worked in primary care clinics and school-based settings (n = 5; Table 3). The remaining article surveyed pediatric medical residents (Table 3). Full details on the described interventions for Aim 1 are in the Supplemental Material.
Description of Included Studies (N = 11).
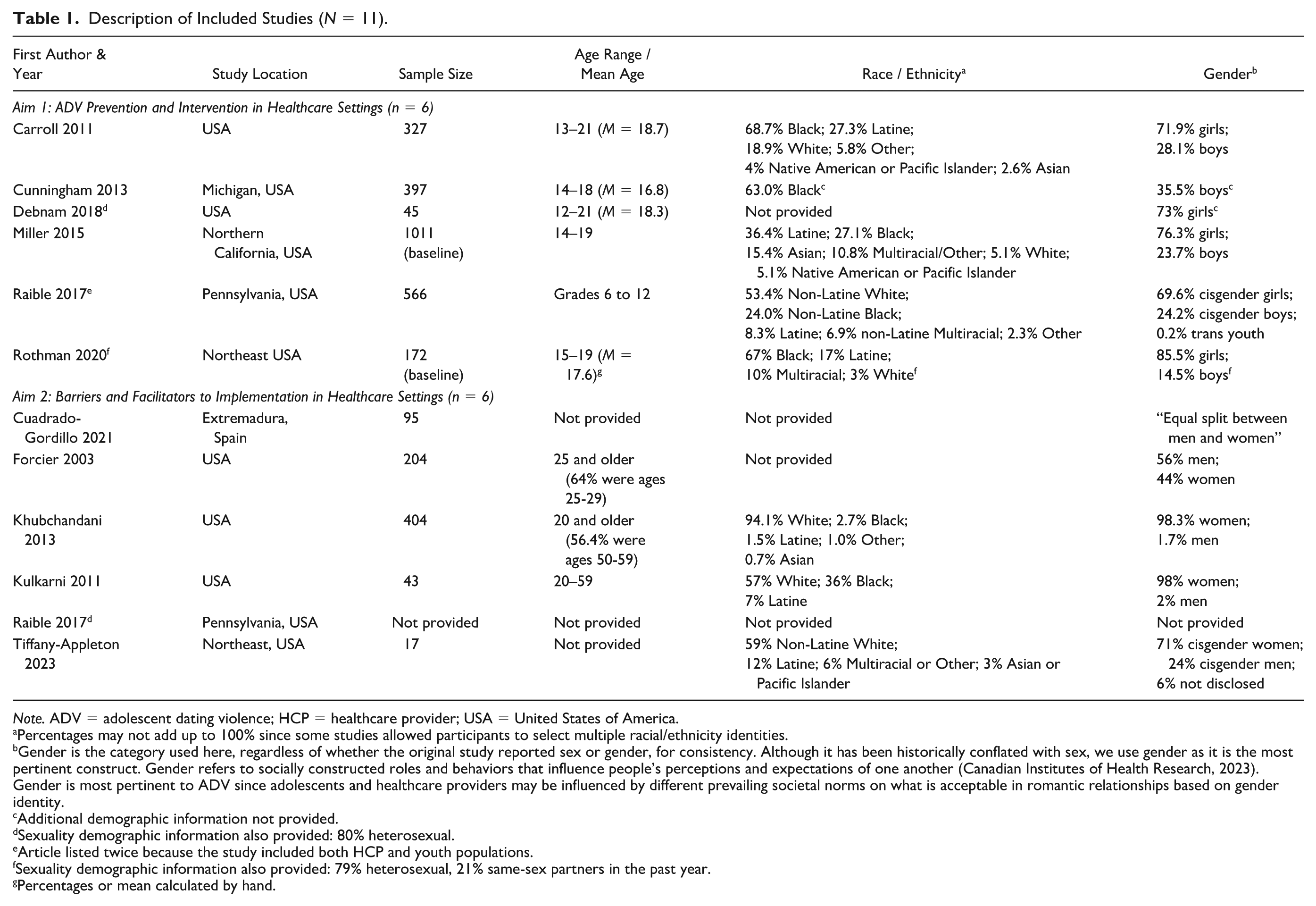
Note. ADV = adolescent dating violence; HCP = healthcare provider; USA = United States of America.
Percentages may not add up to 100% since some studies allowed participants to select multiple racial/ethnicity identities.
Gender is the category used here, regardless of whether the original study reported sex or gender, for consistency. Although it has been historically conflated with sex, we use gender as it is the most pertinent construct. Gender refers to socially constructed roles and behaviors that influence people’s perceptions and expectations of one another (Canadian Institutes of Health Research, 2023). Gender is most pertinent to ADV since adolescents and healthcare providers may be influenced by different prevailing societal norms on what is acceptable in romantic relationships based on gender identity.
Additional demographic information not provided.
Sexuality demographic information also provided: 80% heterosexual.
Article listed twice because the study included both HCP and youth populations.
Sexuality demographic information also provided: 79% heterosexual, 21% same-sex partners in the past year.
Percentages or mean calculated by hand.
Summary of Included Studies with a Youth Population (n = 6).
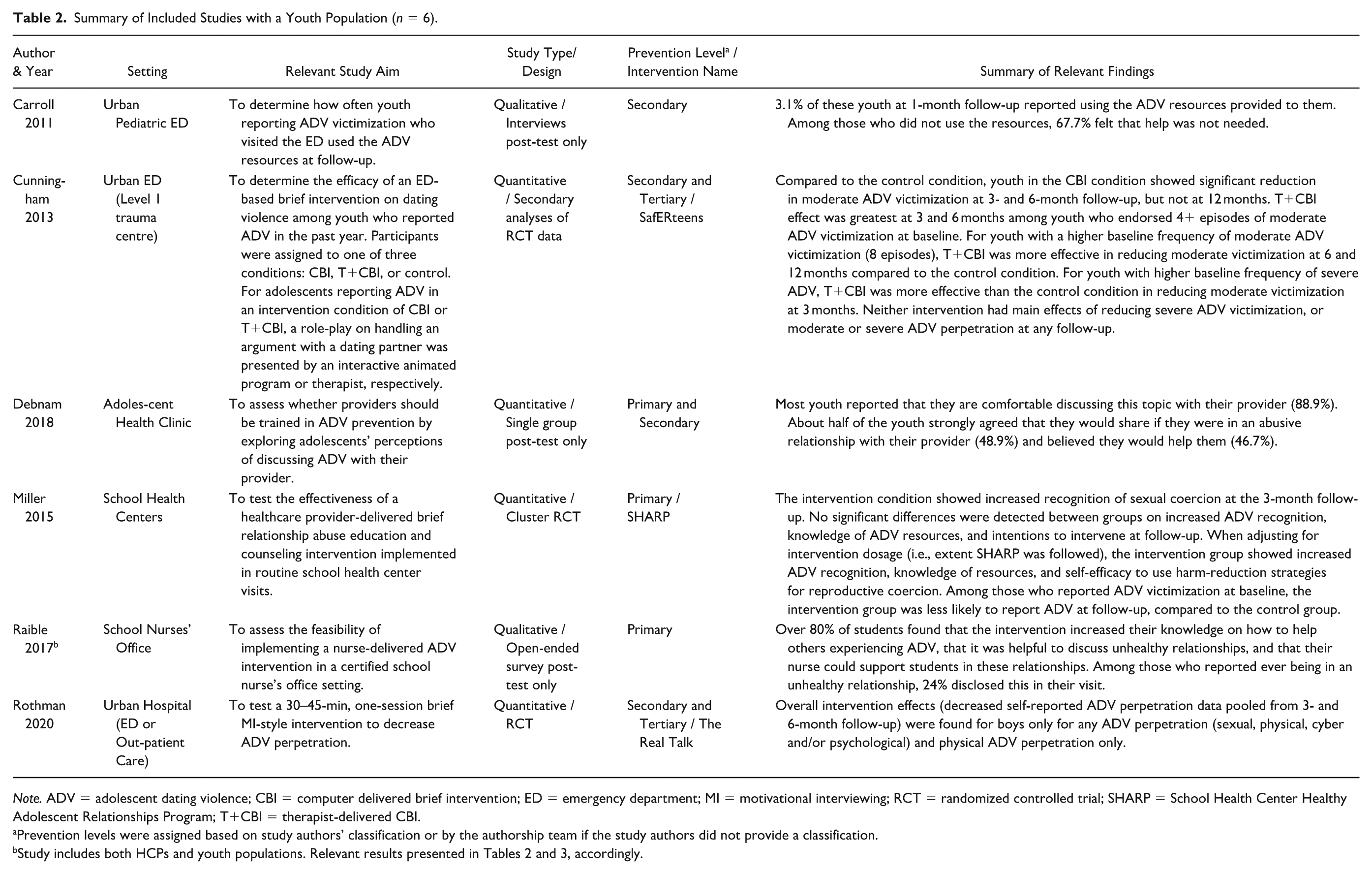
Note. ADV = adolescent dating violence; CBI = computer delivered brief intervention; ED = emergency department; MI = motivational interviewing; RCT = randomized controlled trial; SHARP = School Health Center Healthy Adolescent Relationships Program; T+CBI = therapist-delivered CBI.
Prevention levels were assigned based on study authors’ classification or by the authorship team if the study authors did not provide a classification.
Summary of Included Studies with a Healthcare Provider Population (n = 6).
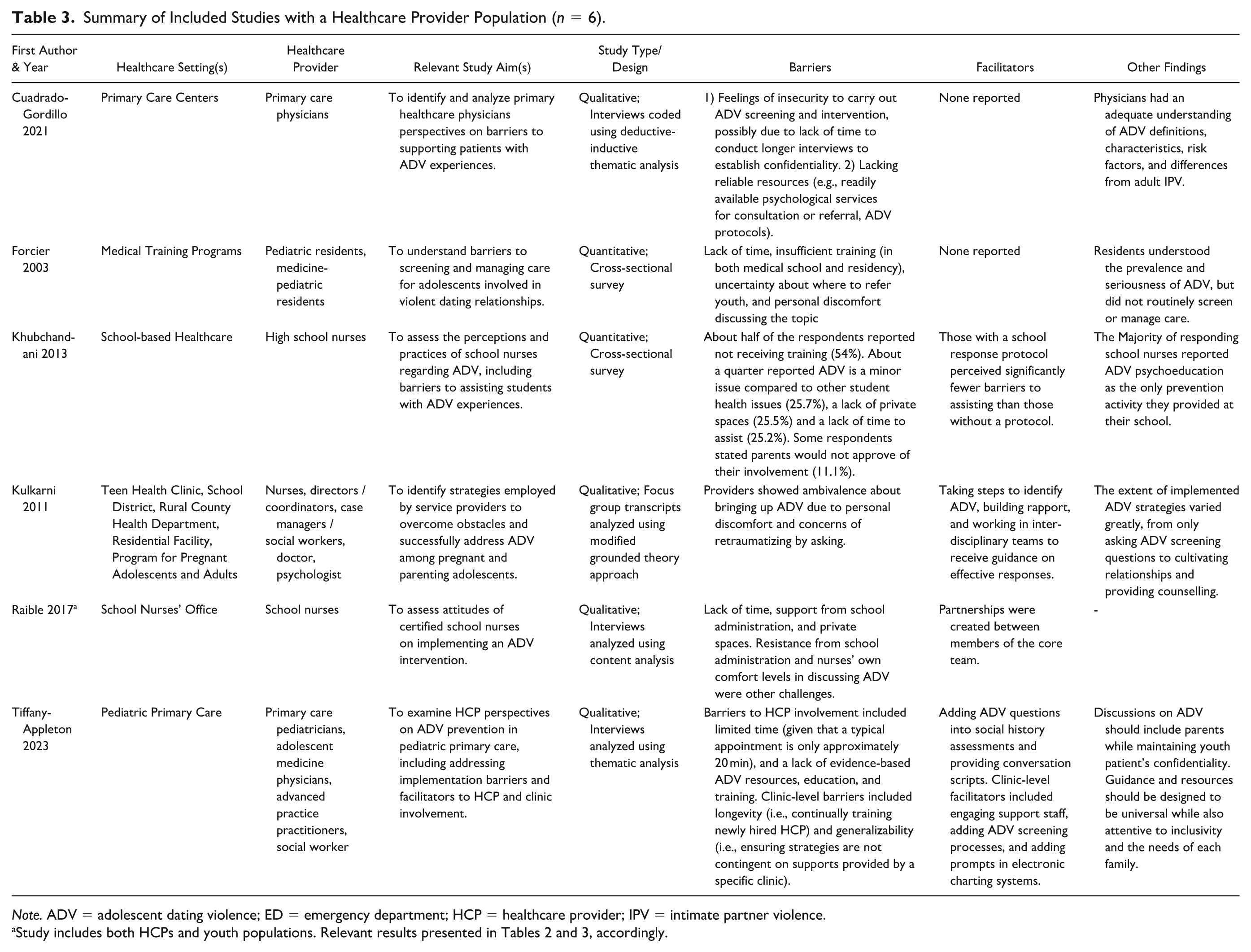
Note. ADV = adolescent dating violence; ED = emergency department; HCP = healthcare provider; IPV = intimate partner violence.
Aim 1: Adolescent Dating Violence Interventions in Healthcare Settings
School-based Healthcare Settings
Two articles reported on primary prevention strategies used in school-based healthcare settings (Table 2). Both of these interventions used a single-session, universal education and brief counselling approach (i.e., provided to all students who sought out healthcare services). E. Miller et al. (2015) conducted a cluster RCT to test the effectiveness of the School Health Center Healthy Adolescent Relationships Program intervention within school health centers. Clinicians served as facilitators and received training on the intervention, which involves discussing healthy and unhealthy relationships, introducing and providing a brochure on ADV, conducting an ADV assessment, and making a warm referral to a victim service if needed (Supplemental Material). At the 3-month follow-up, significant differences were detected between groups of youth for increased recognition of sexual coercion only (Table 2). Among participants who reported ADV victimization at baseline, intervention participants were less likely to report ADV victimization at follow-up as compared to control participants (Table 2). Based on these findings, three of the same researchers conducted a qualitative study to assess the feasibility of implementing a nurse-delivered ADV intervention in school nurses’ office settings (Raible et al., 2017; Table 2). School nurses received training similar to the one provided in E. Miller et al. (2015)’s study (Supplemental Material). Student feedback was generally positive, where a majority of students found that the information provided by nurses increased their knowledge on how to help peers experiencing ADV (Table 2).
Primary Care Settings
Only one study was conducted in a primary care clinic and reported on a primary/secondary intervention (Table 2). Debnam et al. (2018) surveyed adolescents after their visits with providers who had received ADV training. The training provided clinicians with ADV psychoeducation, screening questions, methods to build trust with youth and respond to disclosures, and information on confidentiality laws and the importance of referral lists. Most youth participants reported feeling comfortable discussing healthy relationships with their provider post-intervention, and almost half of youth participants strongly agreed that they would tell their provider if they were in an abusive relationship and believed their provider would help (Table 2).
Hospital Settings
Three studies reported on secondary and/or tertiary prevention strategies used in hospital-based settings (Table 2). Carrol et al. (2011) provided local resources to adolescents with ADV experiences who visited a pediatric ED. Of the youth who participated in follow-up interviews 1 month later, a majority of them had not used any of the resources provided, with many reporting that help was not needed (Table 2). The other two articles evaluated brief, single-session, motivational interviewing interventions targeted at reducing occurrences of ADV victimization and/or perpetration. Cunningham et al. (2013) completed secondary analyses of RCT data to assess the efficacy of a 30-minute, ED- and computer-based intervention (SafERteens) in reducing moderate and severe physical ADV victimization and perpetration (Table 2). The intervention groups included a computer-delivered brief intervention (CBI) condition, or a therapist-delivered CBI condition, where the therapists were research social workers trained on motivational interviewing techniques and the SafERteens intervention (Supplemental Material). Moderate ADV behaviors included pushing, shoving, grabbing, or slapping, twisting an arm or hair, or throwing something that could hurt. Severe ADV behaviors included punching, hitting with something that could hurt, choking, slamming against a wall, beating up, burning or scalding on purpose, kicking, or using a knife or gun. Reduction in moderate ADV victimization was found for the CBI condition only, as compared to the control condition at the 3- and 6-month follow-up (Table 2). No significant differences were found by intervention condition for severe ADV victimization or any ADV perpetration (Table 2), however, the authors reported that analyses for ADV perpetration may have been underpowered.
To address this identified need for an effective intervention for ADV perpetration, Rothman et al. (2020) designed The Real Talk, a 30–45-minute, hospital-based intervention specifically aimed at decreasing ADV perpetration (Table 2). Interventionists were non-clinicians (community members with ADV education experience or Master of Public Health students) who underwent a standardized 20-hour training on motivational interviewing. Modest intervention effects for decreased ADV perpetration (any physical, sexual, psychological, and/or cyber perpetration) were found at the 3- and 6-month follow-up among boys only (Table 2).
Aim 2: Barriers and Facilitators to Implementation in Healthcare Settings
School-Based Healthcare Settings
Two articles reported on school nurses’ perceptions of barriers and facilitators to implementing ADV prevention strategies in school-based healthcare settings (Table 3). Khubchandani et al. (2013) identified the following barriers to supporting students with ADV experiences in this setting: insufficient training on assisting students; lack of time to assist students; lack of private spaces to have sensitive conversations; and nurse perspectives that ADV is a minor issue compared to other student health issues (Table 3). Those with a standard ADV school response protocol or procedure perceived significantly fewer barriers to providing ADV assistance, suggesting that a school protocol served as a prevention facilitator (Table 3). Raible et al. (2017) also reported on several barriers related to implementing their ADV intervention in a school nurse office setting, including lack of time, issues with support from school administration, and a lack of private spaces, as well as nurses’ personal discomfort in discussing ADV with students (Table 3). An identified facilitator was the close partnership formed between intervention team members (Table 3).
Primary Care Settings
Two articles reported on barriers that emerged in primary care practice (Table 3). Cuadrado-Gordillo and Parra (2021) interviewed primary care physicians in Extremadura, Spain, and they reported barriers to ADV prevention (including detection, screening, and intervention) included lack of time and reliable resources or sources of information (Table 3). Implementation facilitators were not discussed in this article. Tiffany-Appleton et al. (2023) interviewed primary healthcare providers and found that limited time was a key barrier to employing ADV prevention strategies (Table 3). Facilitators to address identified barriers included explicitly incorporating ADV questions into confidential social histories and providing ADV conversation scripts, and adding prompts in electronic charting systems to remind providers to ask about ADV (Table 3).
In their study, Kulkarni et al. (2011) interviewed a variety of healthcare service providers from five different healthcare settings, including primary care settings and one school-based healthcare setting (Table 3). These settings provided healthcare services for pregnant and parenting adolescents. Barriers to addressing ADV experiences with youth included personal discomfort in discussing ADV and concerns about retraumatizing adolescents when asking about ADV experiences (Table 3). Facilitators included asking more behavioral or descriptive screening questions, as opposed to explicitly asking if the youth had experienced abuse (since a patient’s personal definition of abuse may differ), building a trusting relationship with youth, and working in interdisciplinary teams that included social workers or counsellors to seek consultation on next steps (Table 3).
Other Setting
Forcier et al. (2003) surveyed pediatric and medicine-pediatric residents on major barriers to discussing ADV during adolescent health visits and they reported lack of time, insufficient training during medical school and residency training, not knowing where to refer patients, and discomfort in discussing ADV (Table 3). Facilitators of implementation were not discussed.
Discussion
To our knowledge, this systematic scoping review is the first to explore the state of the science on conducting ADV prevention work in healthcare settings, including healthcare providers’ perspectives on barriers and facilitators they encounter when engaging in this work. To capture all relevant research, we included any peer-reviewed article using any type of study design (i.e., quantitative, qualitative, and/or mixed-methods). Using these criteria, we identified 11 studies that addressed the study aim(s). Critical findings of the review are summarized in Table 4.
Critical Findings.
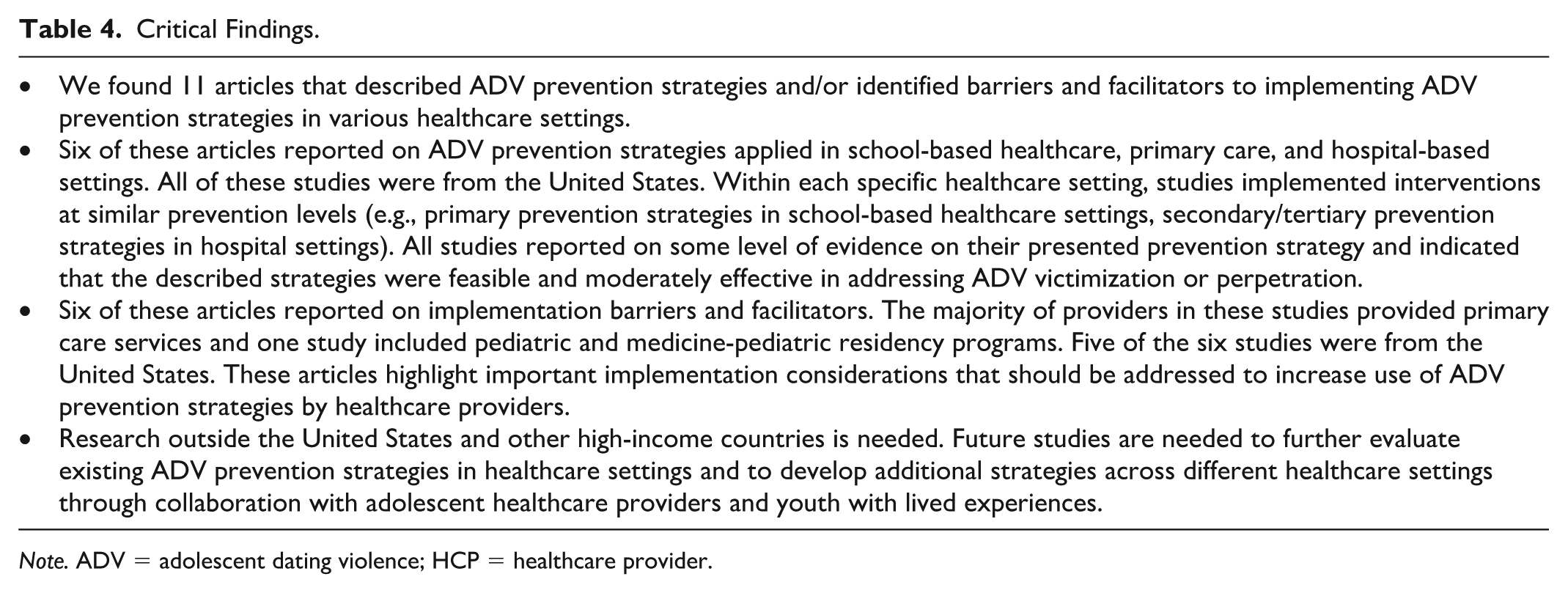
Note. ADV = adolescent dating violence; HCP = healthcare provider.
Aim 1: ADV Prevention in Healthcare Settings
Two articles focused on primary ADV prevention strategies for use in school-based settings. Both studies employed the same ADV preventive intervention, which included providing education about healthy relationships and ADV to all youth visiting the clinic, and counselling and referrals for those who disclosed ADV experiences. These studies found that post-intervention, youth reported greater ADV recognition (although one study did not conduct tests of statistical significance; Raible et al., 2017). Thus, like many primary ADV prevention programs delivered in school-based settings, school-based healthcare programs may also increase knowledge of and attitudes towards ADV (e.g., De La Rue et al., 2017; C. Lee & Wong, 2022). However, as knowledge and attitudes are only moderately correlated with behavior (at best), future studies should further examine the long-term impact of preventive interventions in school healthcare settings on ADV victimization and/or perpetration.
Only one article focused on the feasibility of a primary/secondary prevention strategy for use in primary care settings (Debnam et al., 2018). This study found that most youth were open to discussing ADV with their clinician, and that many would disclose ADV experiences to them. However, it is unclear why these youth were more open to discussing ADV and whether any of them had ever experienced ADV themselves. This finding is in line with previous studies, which have found that youth perceive discussing ADV with their healthcare provider as important (E. Miller et al., 2010; Sieving et al., 2021). Given that primary healthcare providers are well-positioned to engage in ADV prevention strategies, and these settings offer opportunities for routine visits (Starfield, 2001), further research should be conducted to better understand the feasibility and effectiveness of implementing ADV prevention strategies in this setting.
Finally, three studies reported on secondary and/or tertiary preventive interventions occurring in hospital-based settings. Carroll et al. (2011) found that when youth with ADV experiences were provided with local resources, most did not use them. Although the follow-up period was relatively short (1 month), this finding highlights the need to understand alternative ways to connect youth with relevant resources, such as reviewing possible resource options with patients. The remaining two studies reported on brief, single-session interventions that used principles of motivational interviewing, a directive method to enhance an individual’s intrinsic motivation to change (W. R. Miller & Rollnick, 2012). The SafERteens intervention demonstrated some effectiveness in reducing ADV victimization (but not ADV perpetration) among adolescents with a higher frequency of moderate ADV episodes. The Real Talk intervention solely focused on reducing ADV perpetration and found a small, but positive, short-term effect any ADV perpetration reduction, but only for boys. Notably, there were relatively fewer boys in this sample, possibly suggesting that this intervention was particularly impactful for this population. Overall, given that a substantial minority of youth who use ED services have recently experienced ADV (Carroll et al., 2011; Singh et al., 2014), such brief preventive interventions highlight the opportunity to implement targeted ADV interventions in hospital-based settings.
In terms of implementation, it is important to note that both SafERteens and The Real Talk were conducted by trained facilitators, and not clinicians working in these settings. Although this reduces the burden on hospital staff to administer ADV interventions, additional costs associated with implementing these interventions can limit their sustainability, such as ongoing training of facilitators and monitoring intervention delivery. As such, it is also important to conduct implementation studies in the future, including cost-effectiveness studies by type of provider trained to deliver the intervention, and studies focused on strategies to support intervention sustainability (Fernandez et al., 2019). It is also worth noting that these preventive interventions were developed to be implemented in hospitals that serve ethnically and racially diverse populations, particularly Black youth. A recent systematic review of help-seeking intentions and behaviors for ADV among Black and Latine youth found that they may be less likely to seek formal help, due to feelings of fear and mistrust and lack of access to basic and culturally appropriate healthcare services (Padilla-Medina et al., 2022). Therefore, along with implementing preventive interventions in settings that serve minoritized communities, it is critical that future research actively engage youth with lived experiences of ADV in the co-creation of these interventions to ensure that they are appropriate and center their voices, needs, and strengths.
Of the three studies that evaluated the effectiveness of ADV preventive interventions, only one study found differences in intervention effects by gender (Rothman et al., 2020). Since help-seeking among boys may disrupt adherence to patriarchal masculine norms (hooks, 2004), boys may experience greater stigma when seeking help for ADV behaviors (Bundock et al., 2020). Therefore, it is possible that the opportunity to discuss ADV perpetration with a nonjudgmental adult in The Real Talk intervention was more impactful for boys than girls (Rothman et al., 2020). E. Miller et al. (2015)’s study did not find gender differences and Cunningham et al. (2013)’s study was not powered to evaluate intervention effects by gender. As such, further research is needed to better understand the gendered nature of ADV reporting and help-seeking by youth (White, 2009).
Aim 2: Barriers and Facilitators to Implementation in Healthcare Settings
Several common barriers were identified, highlighting that ADV is likely not regularly or consistently addressed within primary care settings. For example, almost all articles cited limited time, training, and resources as substantial barriers. Time constraints limited providers’ ability to conduct ADV assessments, provide adequate assistance, develop rapport and establish a trusting relationship, and prioritize discussing ADV over other health concerns. Furthermore, although providers identified the need for evidence-based training and resources, guidance on assessing for and responding to ADV are not widely standardized (Tiffany-Appleton et al., 2023). These barriers reflect common challenges in program implementation across settings. Thus, established implementation strategies could be used to design tools to address these barriers, and ultimately improve the adoption and implementation of ADV strategies in healthcare settings (Powell et al., 2015). Providers may also hesitate to discuss ADV with patients due to a lack of resources, such as reliable referral sources to psychological services (Cuadrado-Gordillo and Parra, 2021). This issue of identifying ADV experiences but being unable to provide appropriate support and resources is similar to reports from healthcare providers supporting women experiencing IPV (Tower, 2006).
Aim 2 studies also identified a few facilitators to implementing ADV strategies in healthcare settings that provide primary care services, including receiving guidance on identifying and responding to ADV (e.g., conversation scripts; working in collaborative, interdisciplinary teams). These strategies can be beneficial to healthcare providers as they can reduce the cognitive load and pressure of asking appropriate questions on ADV and increase confidence in responding to ADV (Kulkarni et al., 2011; Tiffany-Appleton et al., 2023). Moreover, receiving support from the clinic (e.g., prompts from electronic charting systems) can further facilitate the implementation of ADV strategies. These facilitators tap into standard implementation strategies for healthcare settings, such as “Organize Clinical Implementation Team Meetings” and “Remind Clinicians” (Powell et al., 2015). Overall, addressing the identified barriers and facilitators using existing implementation strategies may increase the use of ADV prevention strategies by healthcare providers.
Limitations
This systematic scoping review has several limitations that should be noted. First, articles that solely focused on screening were excluded, as the focus of screening articles (e.g., providing clinical guidance, assessing the effectiveness of various screening questions in detecting ADV, identifying risk factors for ADV victimization or perpetration) differs from the primary aim of the current review, which was to summarize the outcomes of defined ADV prevention strategies. However, screening is another potential prevention strategy that should be the focus of a future review, given that routine screening for IPV for adults is not always recommended (MacMillan et al., 2009; Wathen et al., 2008), and thus further information and evidence on the effectiveness of ADV screening is needed. Second, all studies but one included in this review were conducted in the United States, including all Aim 1 studies on specific prevention strategies. This may be a result of only including peer-reviewed articles in the English language.
Furthermore, all studies were conducted in high-income countries, limiting our understanding of ADV prevention strategies implemented in differently resourced healthcare systems and structures. Conducting future work in low- and middle-income countries, as well as high-income countries outside the United States, is critical as several structural-level barriers could differentially impact youth’s access to healthcare services globally, which can thus serve as barriers to healthcare setting-based ADV prevention programs. For instance, living in rural areas with a limited number of clinics, hospitals, or healthcare providers may impact youth’s access to primary, urgent, or specialty care services. Additionally, minimal or no healthcare cost (e.g., insurance) coverage may restrict youth to only access healthcare services from certain settings (e.g., school health centers). Although a few studies in the current review developed and implemented ADV interventions in healthcare settings that serve all patients regardless of insurance coverage, other structural-level barriers to accessing healthcare services likely still limit youth participation in ADV interventions and should be explored in future research. Only one article focused solely on ADV perpetration, highlighting a phenomenon found in the broader ADV literature of focusing on prevention strategies for ADV victimization. Finally, diversity considerations of patients were minimally discussed by providers when reporting implementation barriers and facilitators. Only one article focused on services for pregnant and parenting adolescents, despite being a population at greater risk for experiencing ADV (Silverman et al., 2004). More broadly, given that a number of studies have found that those who experience structural marginalization are at greater risk of experiencing ADV and are less likely to access formal help (Exner-Cortens et al., 2023; Mercy & Tharp, 2015; Padilla-Medina et al., 2022), experiences of marginalization and how they shape access to healthcare services, also need to be considered when investigating how to improve ADV-related care.
Research, Practice, and Policy Recommendations
Research, practice, and policy recommendations are provided in Table 5. For research, additional studies are needed to test the effectiveness of ADV prevention strategies for healthcare settings in different regions and contexts, including how provider and youth needs may differ across differently resourced settings (e.g., low- and middle-income countries). Future studies should also be conducted in other geographical locations outside of the United States to understand whether healthcare settings are generally suitable for implementing ADV prevention strategies. Included studies also demonstrated that healthcare providers can be engaged in ADV prevention efforts, but that they may face substantial barriers. Future studies should focus on investigating which supports could aid providers to engage in this work using existing healthcare-focused implementation strategies as a guide (Powell et al., 2015). Moreover, none of the included studies focused on perspectives of healthcare providers who work in EDs or other hospital-based settings. Given that youth visiting an ED may have recent ADV experiences that are associated with other health conditions (Singh et al., 2014), the unique implementation barriers and facilitators that these providers may encounter should be studied. The perspectives of healthcare providers who work in mental health settings were also missing. This could be a valuable research area given that these providers provide tertiary-level treatments to address mental health conditions related to ADV experiences.
Recommendations for Future Research, Practice, and Policy.
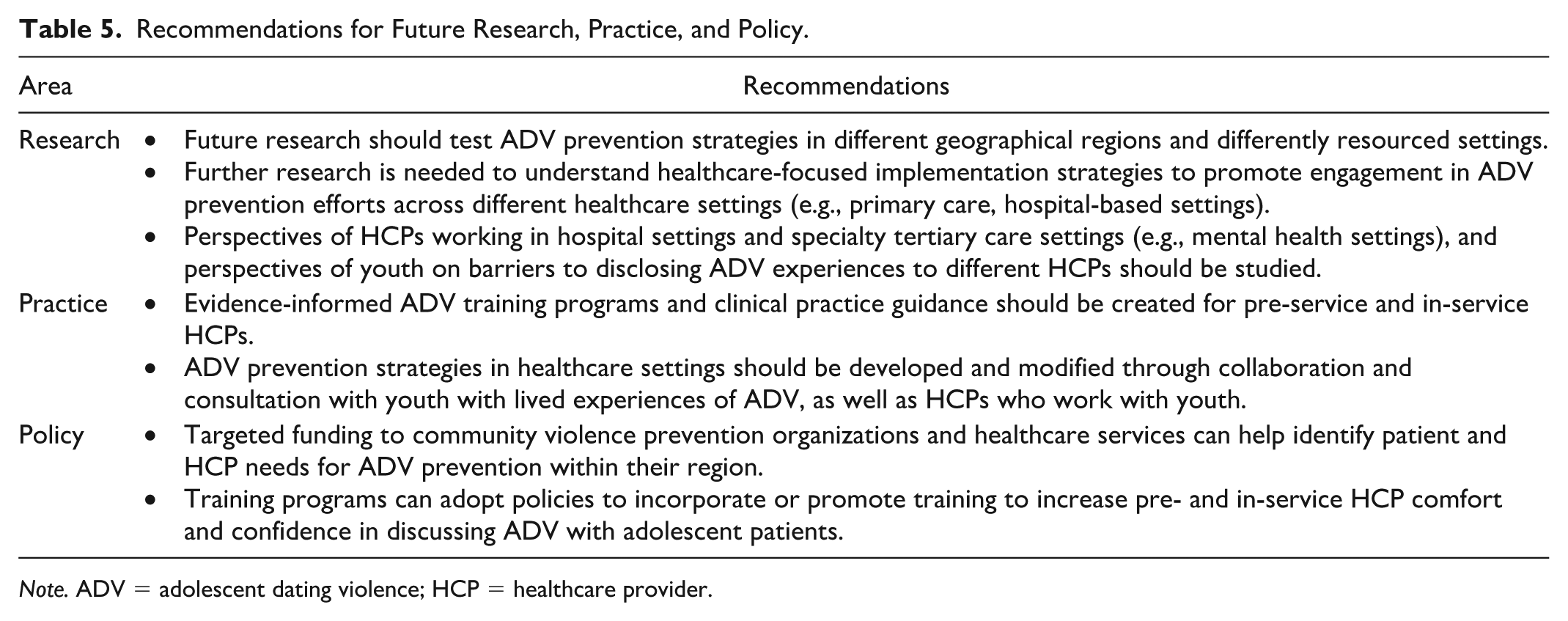
Note. ADV = adolescent dating violence; HCP = healthcare provider.
Further research is also needed to understand the perspectives of youth who have previously experienced ADV on disclosing to healthcare providers. A recent systematic review found that youth report several barriers to ADV help-seeking behaviors and intentions from formal sources of support, including concerns around confidentiality, feelings of embarrassment, lack of trust in professionals, and viewing help-seeking as a sign of weakness (Bundock et al., 2020). These identified barriers can guide research on youth perspectives on healthcare provider involvement in ADV prevention efforts. These barriers should also be addressed in the design of future ADV preventive interventions (e.g., developing training for providers on how to discuss limits to confidentiality and build trusting relationships with patients).
Although only one article looked at pre-service professionals, healthcare professional training programs can provide students with direct ADV training before they are in the field. This can include identifying different types of ADV (i.e., beyond physical or sexual violence), discussing healthy and unhealthy romantic relationships, and responding appropriately to disclosures of ADV. For in-service providers, the development of evidence-informed practice guidelines that are readily accessible to healthcare providers appears to be a valuable tool. In both cases, it is crucial that trainings and guidelines be developed through consultation with youth who have lived experiences and with healthcare providers who work with youth.
For policy, recommendations include increased funding to violence prevention organizations or health services to comprehensively outline areas of need and address identified gaps within their geographical regions. Healthcare professional training programs can also adopt policies that promote training to increase pre-service providers’ confidence and comfort in discussing ADV. Clinical guidance on addressing ADV could be developed and made readily accessible on professional healthcare organization websites for providers working with youth.
Conclusion
Experiencing ADV can lead to adverse short- and long-term health outcomes. Given that healthcare providers are in frequent contact with youth and that youth may present to these settings due to ADV-related health concerns, there is growing interest in implementing ADV prevention strategies in healthcare settings. The present review identified several promising ADV prevention strategies that have been developed and evaluated in school-based healthcare and hospital settings. Although healthcare settings appear well-situated to conduct ADV prevention work, we also found that substantial barriers exist, including limited time, training, and resources, and provider discomfort. Future research should focus on developing, evaluating, and improving ADV prevention programs offered in healthcare settings that address these identified barriers.
Supplemental Material
sj-docx-1-tva-10.1177_15248380251381811 – Supplemental material for Adolescent Dating Violence Prevention in Healthcare Settings: Systematic Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380251381811 for Adolescent Dating Violence Prevention in Healthcare Settings: Systematic Scoping Review by Ruchi Vijh, Deinera Exner-Cortens, Sheri Madigan and Melanie Noel in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
Thank you to Jenna Himer for her support on this project during the article screening process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ms. Vijh’s work was supported in part by funding from a Canadian Institutes of Health Research (CIHR) Canadian Graduate Scholarship—Master’s (CGS M) Award. Dr. Exner-Cortens’ work was supported in part by funding from the Alberta Children’s Hospital Research Institute (ACHRI) and the Canada Research Chairs program (CRCP). The funders had no role in the study design; collection, analysis or interpretation of data; writing of the report; or the decision to submit the manuscript for publication.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.