
Abstract
This systematic review synthesized evidence from parental child maltreatment (CM) interventions by reviewing intervention evaluation studies on potentially effective intervention components and delivery techniques as well as identifying differences in the presence of these components based on maltreatment type. Quantitative intervention evaluations with an explicit parental CM outcome published in a peer-reviewed journal were considered for inclusion. This resulted in 60 final studies for the systematic review. The quality appraisal did not exclude any studies. Results were narratively synthesized using the Risk and Resilience Ecological framework and the behavior change techniques taxonomy with the help of systems mapping. Findings revealed the prevalence of intervention components among effective interventions, including parental emotional regulation (micro-individual level), managing child misbehavior (micro-family) and home visiting (mezzo). Prevalent behavior change techniques included “social support” and “instruction on how to perform a behavior” across all ecological levels. Physical abuse had the most maltreatment-type-specific intervention components (e.g., cognitive appraisal and parental motivation) and neglect only had one (management of parental risky health behaviors). No unique components targeting emotional and sexual abuse were identified. Findings highlighted potentially effective intervention components and the way they are delivered along with specific components aimed at types of maltreatment. Intervention provision can utilize these findings to tailor and develop effective provisions for parental CM. Researchers can shift attention to areas requiring more evidence such as the inclusion of a cultural perspective and evaluation of intervention provision for fathers, who are currently under-represented.
Keywords
Child maltreatment (CM) is a global issue with a myriad of negative consequences for children, families, and wider society (Levey et al., 2017). Parents are the most common perpetrators of CM and a variety of interventions exist aimed at the prevention of CM for parents at risk and to reduce the recurrence of CM for those parents who have been maltreated (Yoon et al., 2022). While there is extensive research evaluating CM interventions for parents, evidence is fragmented and not established on what works in effective interventions to prevent and reduce CM (Fox et al., 2022). Prior empirical research and syntheses of evidence present a conflicting picture of what works (e.g., Ijzendoorn et al., 2020; Mikton & Butchart, 2009). This may partly be due to CM interventions’ classification as complex with complexity resting on multiple strategies used by interventions, along with variability in the outcomes and samples assessed (Craig et al., 2008). For parents, these interventions often target behaviors that are amenable to change and are mediated by multiple individual, familial, and environmental influences. Petticrew (2005) posits that the complexity of interventions can be addressed by identifying core components of interventions to better understand their utility. To this end, this study aims to examine intervention content, specifically components of parenting interventions aimed at reducing and preventing CM.
Research studies have used interchangeable terms to encapsulate “intervention components” with some studies using the term “core components” (Blasé & Fixsen, 2013) and others using “practice elements” (Chorpita & Daleiden, 2009). For the current study, intervention components refer to the contextual and structural elements of an intervention. More specifically, contextual refers to intervention provision targeting a specific parental goal or using a specific strategy to bring about change (e.g., increasing parental motivation or managing substance use). Structural components refer to the broad organization of the intervention and include settings (e.g., home visiting or online programs) and the overall flexibility of the program (e.g., tailoring to specific needs).
CM research evaluating parental interventions is extensive (e.g., Ijzendoorn et al., 2020; Levey et al., 2017; van der Put et al., 2018), but there are still unanswered questions regarding what intervention components may be effective in preventing and reducing CM. In interventions such as The Incredible Years Programme, parents are taught ways of playing with their children to improve parent–child interactions to ultimately reduce the risk of CM (Eyberg & Bussing, 2010). Melendez-Torres et al. (2019) found intervention components of teaching parents alternate strategies for physical discipline and equipping them with self-regulation skills as optimal for reducing the recurrence of physical abuse. However, the researchers only considered interventions for child physical abuse. Ijzendoorn et al. (2020) umbrella synthesis found interventions focusing on parenting skills to be more effective compared to those emphasizing social support provision. However, effect sizes were low, emphasizing the limiting effect of interventions to reduce CM. Mikton and Butchart (2009) synthesized evidence from 26 systematic reviews of parenting interventions and found several effective components including home visiting and enhancing parenting skills. However, their conclusions were tentative based on the low methodological quality of included systematic reviews. Overall, additional efforts are warranted in research to examine intervention content, extricate evidence of potentially effective intervention components, and provide much-needed insight to help prevent and reduce parent-perpetrated CM.
There is also a dearth of evidence that captures both intervention components (structural and contextual) and how these components are delivered to parents in CM interventions. Interventions may use differing techniques to deliver the same component, and this may impact the effectiveness of the component. For example, an intervention component to enhance parent–child interaction may be delivered through lectures and educational workshops or behavioral practice and rehearsal. Without a shared understanding of what the components are, how they are delivered, and what may be a potentially effective combination of the two, there can be wasted resources and missed opportunities to gain clarity in insight. A structured framework needs to be utilized to systematically code intervention components’ delivery in intervention provision.
Prior syntheses of evidence (systematic reviews and meta-analysis) of parental interventions for CM have attempted to synthesize evidence on the effectiveness of intervention components (e.g., van der Put et al., 2018). However, there is a lack of consensus on the way intervention components are classified and described. Furthermore, commonly used umbrella terms (e.g., parent education) fail to shed light on the nuances within the delivery of components which hinders meaningful comparisons and further obstructs reaching robust conclusions about the evidence. In addition, prior syntheses of evidence have not captured any variations in intervention provision and type of CM. Research in this area generally emphasizes co-occurrence of multiple types of maltreatment (e.g., Jonson-Reid et al., 2004; Kim et al., 2016); however, Higgins and McCabe’s (2001) review concluded that while physical, emotional abuse and neglect have significant co-occurrence, child sexual abuse does not. Similarly, a prior systematic review (Younas & Gutman, 2022a) elucidated risk and protective factors for different types of CM and found unique factors for physical and emotional abuse and neglect. There is no denying that co-occurrence of maltreatment types is common; however, there is value in understanding how intervention components may differ based on the type of maltreatment to further understand what may be optimal in prevention/reduction of each and whether they occur in conjunction or in isolation.
This study addresses these research gaps through systematically reviewing evaluations of parenting interventions for CM and examining intervention provision to explicitly identify core components of interventions that aim to address different forms of CM. The foci of this study are the four types of parental CM: physical, sexual, emotional abuse, and neglect. Intervention provision comprises intervention components which include contextual factors (specific strategies used by interventions, e.g., child development education) and structural factors that encapsulate the intervention setting (e.g., home visiting, community settings, group parenting sessions) and flexibility of the program. This systematic review uses the Risk and Resilience Ecological Framework (Bronfenbrenner, 1979; Fraser et al., 1999) as the theoretical foundation to examine intervention provision for parental CM. This helps provide a comprehensive account of influences on parental CM ranging from the individual and familial (micro) to the wider community (mezzo) and societal or national levels (macro). A prior systematic review utilized this framework to map risk and protective factors for CM on each ecological level providing a comprehensive overview of parental influences (Younas & Gutman, 2022a). This framework enables examination of intervention content within an ecological context while recognizing the complexity of varying influences and helps with a coherent and systematic synthesis of the evidence. While not all interventions will implement strategies on each ecological level, this framework can inform researchers and practitioners about gaps in intervention provision and tailoring provision of support for vulnerable parents.
To capture delivery techniques of intervention components (e.g., instruction on how to perform a behavior, behavioral practice), this study utilizes the behavior change techniques (BCT) and behavior change technique taxonomy (BCTTv1) approach (Michie et al., 2011, 2013). Finally, differences in intervention components based on maltreatment type are explored.
The research questions (RQ) guiding the current study are first, what are the structural and contextual components (including delivery techniques) of parenting interventions that aim to prevent or decrease CM? Second, how does the intervention content differ based on the specific type of CM being addressed?
Methods
The study uses a systematic review method to review evaluations of parenting interventions for CM studies from 1980 to 2022.
Eligibility Criteria
Table 1 displays the eligibility criteria for studies. Only intervention evaluation studies with an explicit CM outcome and those that include biological parents in the intervention were considered for inclusion. Systematic reviews and meta-analyses were only included initially to extract primary studies of CM intervention evaluations and then they were excluded. Outcome evaluations including randomized controlled trials (RCTs) and quasi-experimental studies were included while any process evaluations or those focusing only on cost-benefit analysis or feasibility of interventions were excluded. Quasi-experimental studies were defined as those intervention evaluations that did not include randomization. A key criterion for inclusion focused on the levels of information provided by studies and these should address, in whole or in part, the RQ guiding the review. More specifically, evaluations eligible for inclusion would have some information about specific intervention components.
Inclusion Criteria.
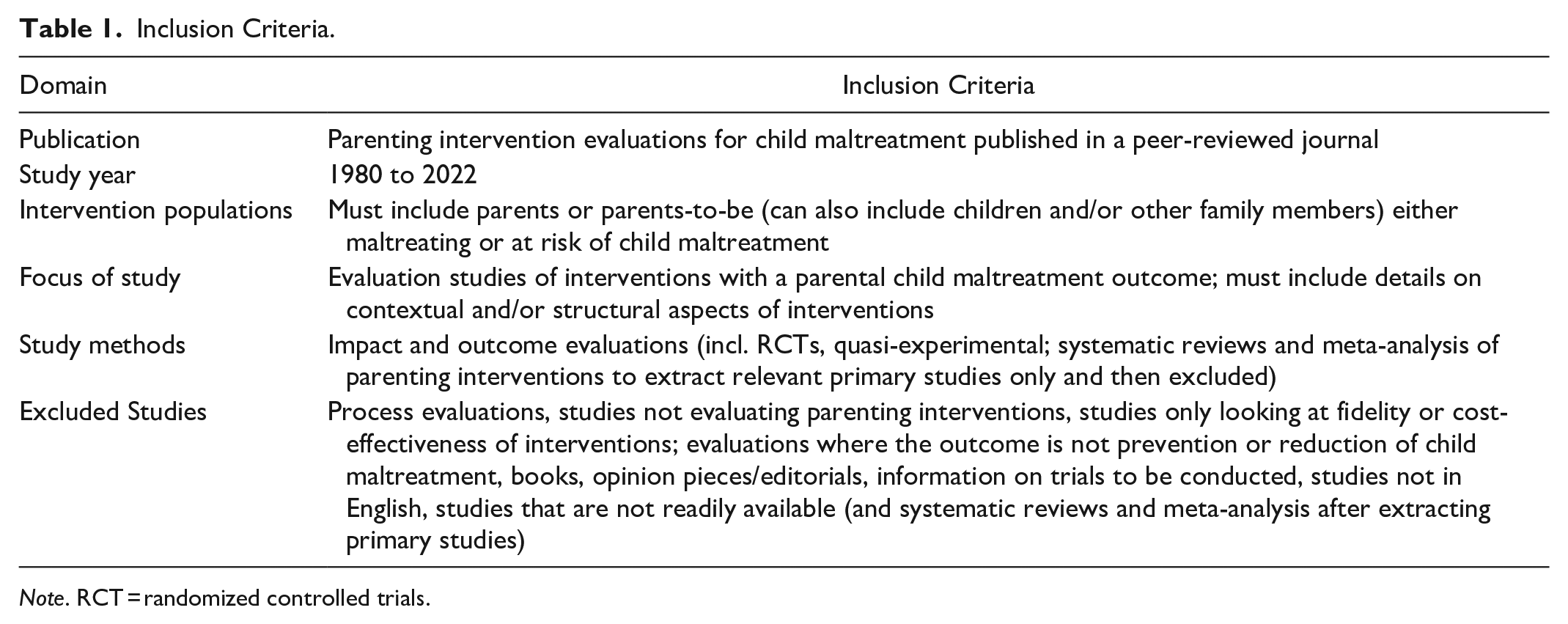
Note. RCT = randomized controlled trials.
Information Sources
Searches for relevant studies were conducted using electronic databases, and five were found to be most appropriate; PsycInfo, PsycExtra, Scopus, Web of Science, and Cochrane Library (see Supplemental File 5 for a full search strategy including key terms used for searching in each database). A total of 2,667 results were obtained from five databases. All records were transferred to EPPI Reviewer 4 (Thomas et al., 2010), a software tool for research synthesis. Reliability in screening of studies was undertaken by the second author for 10% of the total studies and 100% reliability was established.
Data Collection Process and Data Items
A data extraction form was devised to capture relevant information from the intervention evaluations (see Supplemental File 1). This form was guided by the template for intervention description and replication (Hoffmann et al., 2014), a checklist that facilitates a detailed description of interventions to facilitate a thorough examination of intervention content.
The data extraction form comprised four sections including extraction of administrative data (e.g., study name, year, reference number), intervention background, aims, structural content of interventions, and type of maltreatment (e.g., target population, length of intervention, and the setting of delivery of intervention). Data were also collected on the contextual factors which included the various activities of interventions (e.g., child development education, enhancement of parental confidence). Lastly, the delivery techniques (BCTs) of intervention components were extracted from the included studies that focused on how the intervention components were delivered (e.g., education, social support).
Figure 1 shows the extraction of data regarding intervention components, illustrating the different types of data extracted from the included studies. Structural elements of the program included both the setting in which they were delivered and the flexibility of the intervention based on parents’ needs.
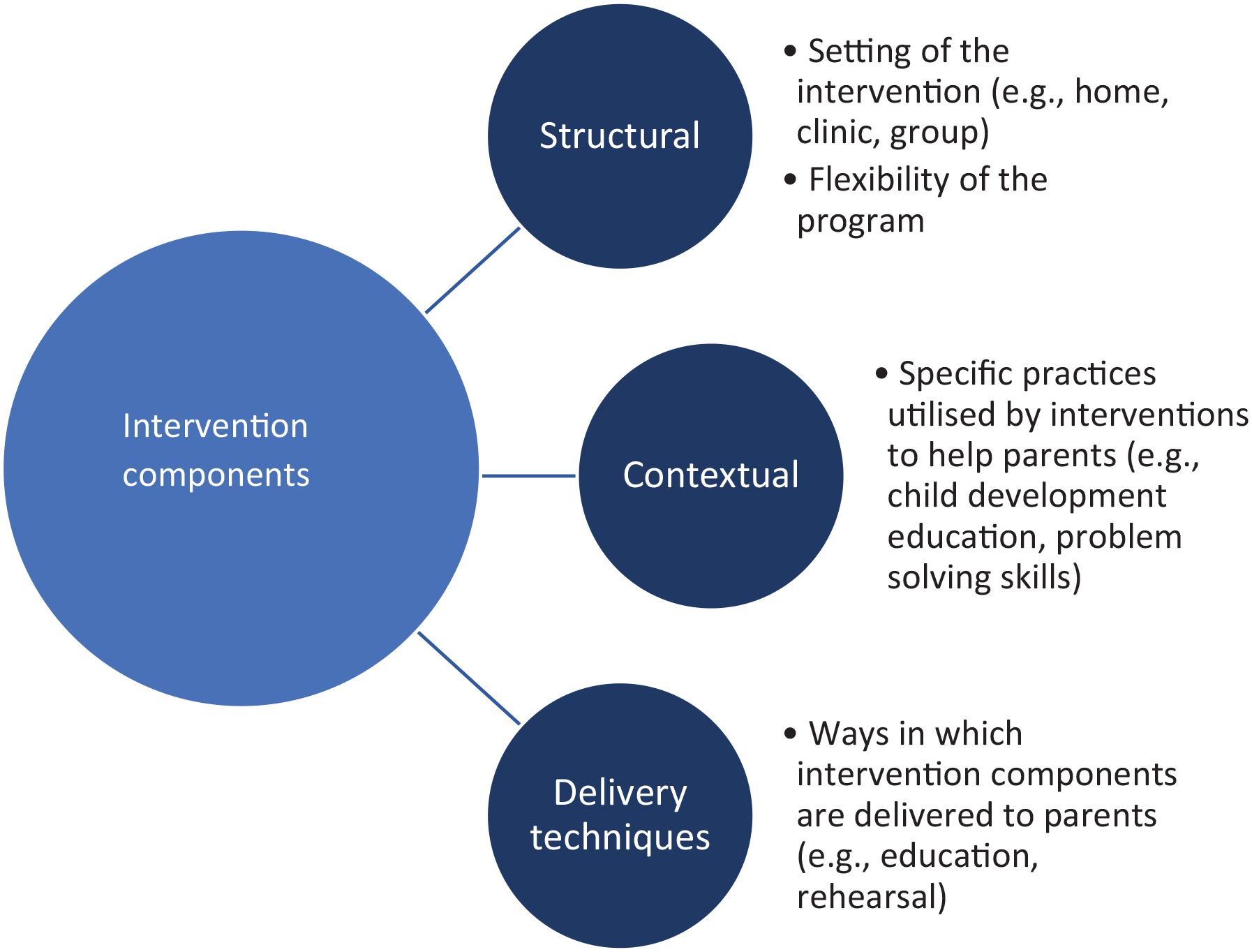
Intervention components: Classification and description.
The contextual elements of the program included specific intervention practices or activities which were taken from intervention descriptions provided by authors of the included studies. An inventory of all intervention practices was recorded in a spreadsheet, and broad domains were created based on the aim of the practice. Broad domains came under three main classifications: activities aimed at the individual parent (physical and psychological support), those aimed at the family (child and family relationship support), and provision of wider and community support (e.g., help with employment or housing). Within each of the broad domains, there were commonalities noted in components across interventions. For instance, managing child misbehavior under the broad domain of family support was identified in 19 interventions. Intervention practices relevant to this classification included teaching parents about alternate child disciplinary methods not involving physical punishment such as time out (Letarte et al., 2010) or training parents in differential reinforcement and positive rewards (Thomas et al., 2011), among others. Similarly, one category under the domain of parental support was “pre-natal health” and this included all practices of interventions targeted at improving or promoting maternal health during pregnancy and was identified in six interventions. Both structural and contextual factors once combined resulted in 40 intervention components. The second author undertook dual data extraction, and 100% reliability was established between the authors.
The intervention components were then mapped onto the ecological framework based on the level of ecology that the intervention component was implemented. Table 2 presents examples of intervention components at each ecological level. For example, parental motivation worked with parents’ motivation and was thus classified under the micro-individual level. Similarly, any intervention component targeting family-level activities such as enhancing the parent–child relationship or strengthening inter-parental relationships was classified under the micro-family level. Mezzo-level components included activities involving the neighborhood or community such as help with housing or referral to other support services. Structural components of interventions were also mapped on the Mezzo level and these indicated overall support from the intervention as nesting in the wider community. No intervention components were identified from the included studies at the macro, societal, and national levels.
Mapping Intervention Components Ecologically.
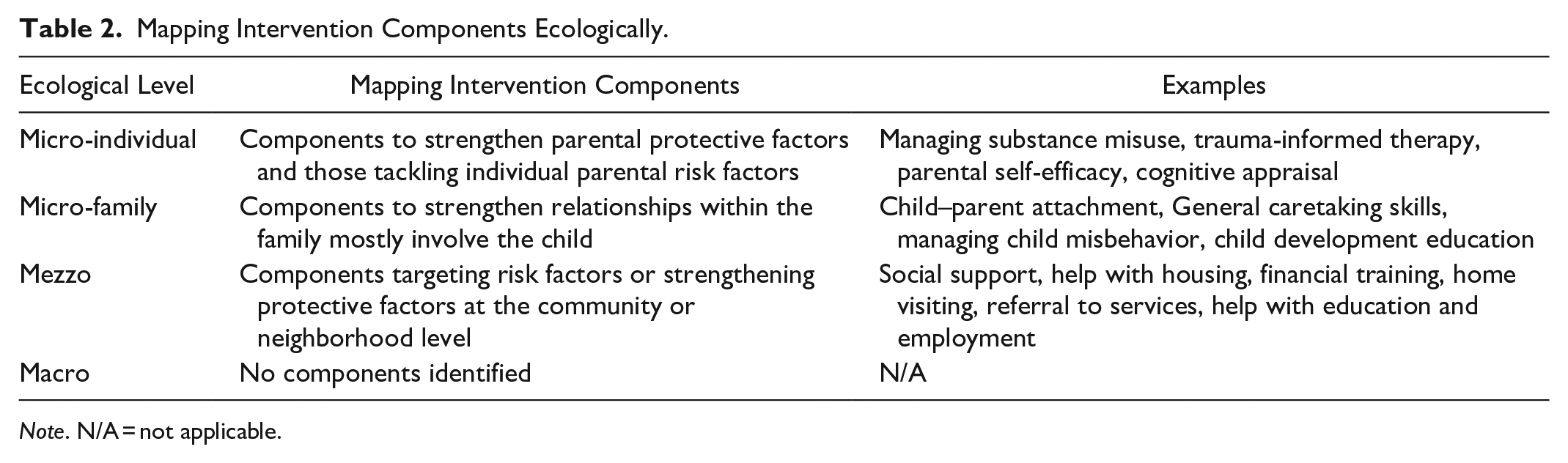
Note. N/A = not applicable.
After extracting relevant details from included studies on how intervention components were delivered to parents, the BCCTv1 taxonomy (Michie et al., 2011; Supplemental File 3) was used to label delivery techniques or BCTs. The BCTTv1 is a 93-item taxonomy of BCTs that are grounded in empirical evidence, and which are “active ingredients” of interventions that can help facilitate a shift in behaviors. The BCT approach has been used in prior systematic reviews (e.g., Miller et al., 2020; Watson et al., 2021) to classify and characterize components used by behavior change interventions. This framework, however, is untested in a systematic review of CM interventions and offers a novel approach to demarcate delivery techniques from intervention components in such interventions. While the BCT framework was initially developed for behavior change interventions particularly in a health context (e.g., hand washing and medication adherence), CM is essentially a parenting behavior and intervention provision targets those behaviors or influences on behavior which are amenable to change. For this reason, the BCT and BCTTv1 (Michie et al., 2011, 2013) can help specify “active ingredients” and provide a systematic way of moving the focus from reviewing only components of interventions to capturing nuances in the way they are delivered. The contextual factors used multiple BCTs across interventions to deliver specific activities to parents. As coding of BCTs requires complex judgments and knowledge of the BCT framework (Wood et al., 2014), a second coder helped to establish inter-rater reliability for all 60 included studies and ensure the taxonomy was adhered to and subjective bias minimized. Initially, inter-rater reliability was established at 78% and discrepancies were discussed, and agreements were made until 100% reliability was achieved in the identification and classification of all BCTs to capture the delivery techniques used across included intervention studies.
Quality Appraisal and Risk of Bias Assessment
Quality appraisal of included RCT studies was completed using the risk of bias tool (Sterne et al., 2019; Supplemental File 2). Determinants of quality included five domains: bias arising from the randomization process, bias from deviations from intended interventions, bias in the measurement of the outcome, bias due to missing outcome data, and bias in the selection of reporting of results.
Quasi-experimental studies were appraised for quality using the Joanna Briggs Institute Critical Appraisal Checklist for Quasi-Experimental Studies (Supplemental File 2). Assessment criteria included clear identification of cause and effect, high level of similarity between treatment and comparison or control groups, complete follow-up, methods for accounting for loss to follow-up, and appropriateness of measures and analyses.
Final judgments of quality were based on the GRADE approach (Ryan & Hill, 2016) where RCTs have an initial consideration of “High” quality, and quasi-experimental studies are initially considered to be of “Moderate” quality. Both study designs were then graded down or up based on the relevant criteria for assessment. Grades include High, Moderate, Low, and Very Low. Any studies assessed as “very low” in quality where the risk of bias is very high and significant errors are identified in reporting, analysis, and presentation of findings, were fit for exclusion. All other judgments of quality (high, moderate, and low) were considered fit for inclusion. Dual quality appraisal was undertaken by the second author for 7% of the studies, and 100% reliability was established between the authors.
Synthesis methods
The first research question guiding the current study focuses on the intervention provision (intervention components and BCTs) that may be effective to prevent or reduce parental CM. This was answered firstly by presenting summary characteristics of all included studies and second, by presenting intervention components on each ecological level using graphs to represent frequency of occurrence as well as a narrative synthesis of the findings. A systems mapping approach was used to visually present the coded BCTs or delivery techniques used by the interventions to deliver the intervention components, and these were also presented based on the individual ecological level. Systems mapping is a systematic and structured way of presenting copious amounts of interlinking information in a manageable way and can show the relationship between the various components and the techniques used to deliver them (Cavill et al., 2020). Systems maps were created using Kumu software (Kumu, 2011).
The second research question on whether intervention content differed based on the type of CM was answered through both a narrative and graphical approach. Venn diagrams, for each ecological level, helped to synthesize evidence on shared intervention components as well as specific ones for the four maltreatment types. These findings were only presented for those intervention evaluation studies that specified a type of maltreatment and not for those where a specific type of maltreatment was not mentioned.
Findings
Figure 2 displays the preferred reporting items for systematic reviews and meta-analysis (Page et al., 2021) flow chart. From the 2,667 studies retrieved, 381 duplicates were found, and 2,124 studies were excluded from abstract screening. A total of 225 studies were considered eligible for full-text screening.
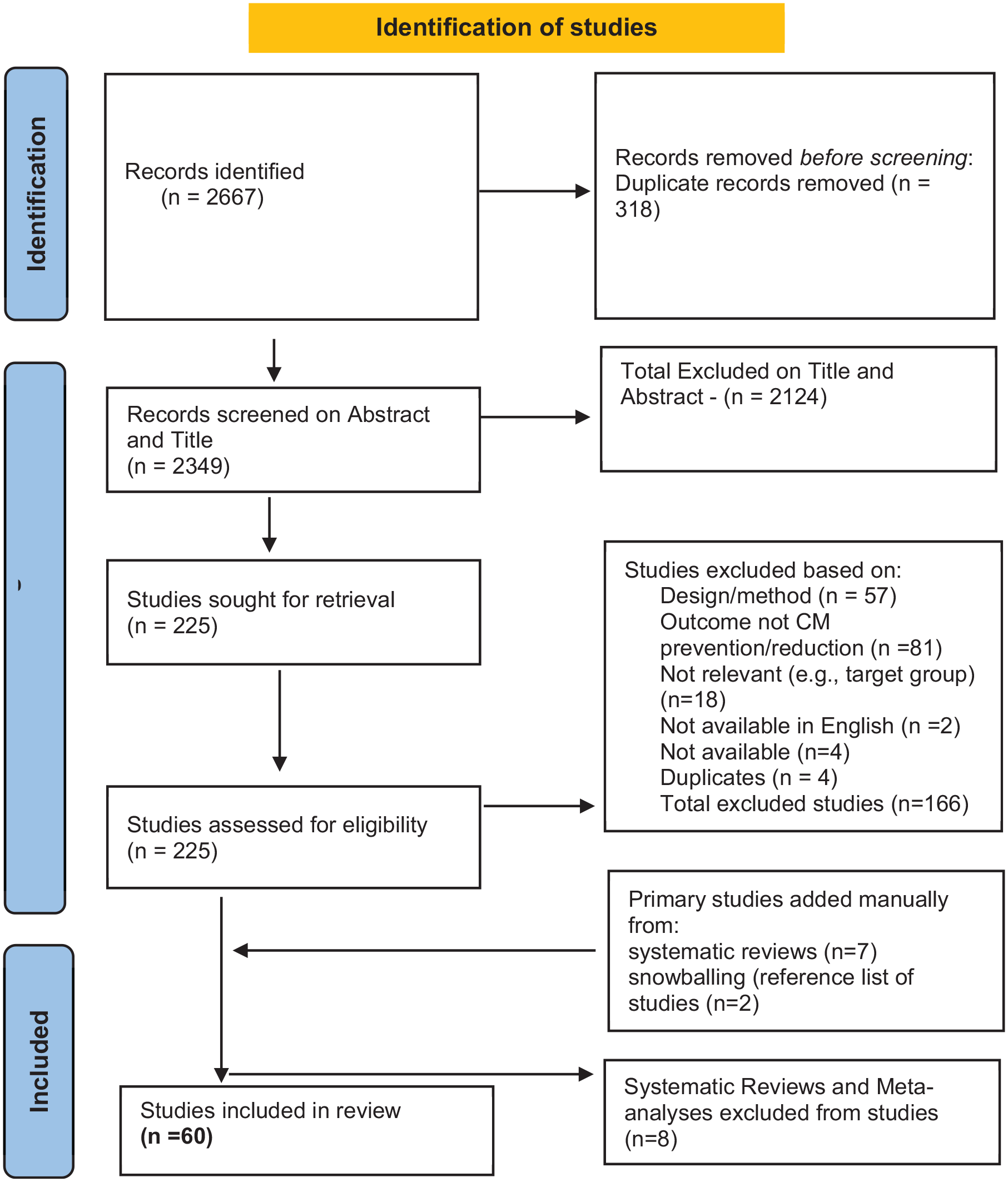
PRISMA flow chart.
Four studies could not be accessed and were unavailable leaving 221 studies. A further 291 primary studies were extracted from systematic reviews and screened and seven met the criteria for inclusion. Two further studies were included using snowballing bringing the number of studies for full-text screening to 230. From these, eight systematic reviews and meta-analyses were excluded and a further 166 studies were excluded for reasons related to outcome, method, target group, duplicates, and language. A final 60 studies were found eligible for inclusion in the systematic review. Forty-six were RCTs and 14 were a quasi-experimental design.
Summary Characteristics of Included Studies
A total of 15 countries were represented in the included evaluations (see Supplemental File 6 for included study characteristics), with the vast majority from the U.S. (61%). Canada and Australia each represented 7% of the studies and 5% were from the U.K. Iran represented 3% of the studies. The remaining 24% included Tanzania, Colombia, Turkey, Jamaica, Burkina Faso (West Africa), Thailand, South Africa, Spain, Netherlands, and New Zealand.
The total sample across all studies was 56,939 with 91.2% comprising parents and families, 5.2% only mothers, 1.5% pregnant females, and 1.3% mother–infant dyads. Parent–child dyads comprised 0.5% of the sample and 0.3% were only fathers. Of the 60 evaluations, 33 samples were classified as “at-risk” while 27 samples were classified as “maltreating.” Parents with unsubstantiated maltreatment records or only referrals to child protective services (CPS) were classified as “at-risk” and only those with substantiated cases of CM were classified as “maltreating.”
From the 60 included evaluation studies 51 reported the intervention name while nine did not. There were some interventions that were evaluated more than once; however, all of them had a different sample and focused on different intervention components. For instance, three studies evaluated the parents under pressure program but Barlow et al.’s (2019) study comprised a sample of high-risk pregnant women, Dawe et al.’s (2007) evaluation included families with substance misuse and Frye & Dawe (2008) sample consisted of mothers in prisons. All interventions aimed to reduce either the risk of CM or its recurrence.
Two intervention evaluations did not report the length or intensity of the intervention. For the remaining 58, the intervention length ranged from three sessions per year (Dishion et al., 2015) to 6 years (Reynolds et al., 2003). Session lengths averaged around 1 hr and for many interventions with the home visiting components, the frequency of home visits decreased with parents making progress in the intervention (e.g., Duggan et al., 2004).
Measurement of CM outcomes comprised a wide variety including self-report measures, observations of the home environment and parent–child interactions, child welfare referrals, and substantiated CM records. Thirty-three of the 60 included evaluations relied on self-report measures alone. The most frequently employed self-report measures included the child abuse potential inventory (Ondersma et al., 2010), the conflict tactics scale (CTS; Straus, 1979) and the parent–child version of the CTS (Straus et al., 1997). Less common among the studies was the adult–adolescent parenting inventory (AAPI; Bavolek, 1984) which aims to capture parents’ abusive attitudes (e.g., belief in corporal punishment) for parents of adolescents. One study (Letarte et al., 2010) utilized the parenting practices interview (Webster-Stratton, 1998) which is like the AAPI but for younger children and aims to capture parents’ potential for physical and psychological abuse. Gulirmak et al. (2021) evaluation of Turkish parents used the recognition of emotional maltreatment scale (Uslu et al., 2010) aiming to evaluate parents’ knowledge of behaviors that may be emotionally abusive. Other measures included mother–child neglect scale (Lounds et al., 2004) and the child discipline scale from the UNICEF multiple indicator cluster survey (UNICEF, 2005).
Measures including child welfare referrals and substantiated records of CM were used by 27 studies and these were acquired from CPS or an equivalent social services or child welfare agency. These were often used alongside observations and/or self-reporting measures. One study (Reynolds et al., 2003) utilized court records and substantiated CM records from CPS.
Observational measures included the home observation and measurement of the environment (Bradley & Caldwell, 1984), which was utilized in one study (Huebner et al., 2002). Another study (Galanter et al., 2012) used the child interaction coding system (Eyberg et al., 2005) to code observations of parent–child interactions.
Of the 60 evaluation studies, 41 reported an effect on CM outcomes. From the 46 RCTs, 16 intervention evaluations showed no effect on parental CM outcomes. From the 14 quasi-experimental studies, only one study showed no effect on parent-related CM outcomes.
Quality assessment results
Of the 60 included studies, 46 were RCTs and 14 employed quasi-experimental methods. After the quality appraisal, none of the studies were ranked very low and thus none were excluded. High-quality ranking was given to 12 RCTs, 33 were ranked as moderate of which eight were quasi-experimental and 25 were RCTs, and a ranking of low was given to nine RCTs and six quasi-experimental studies. Table 3 presents the various study rankings and the broad reasons for each rank given.
Quality Assessment Results.
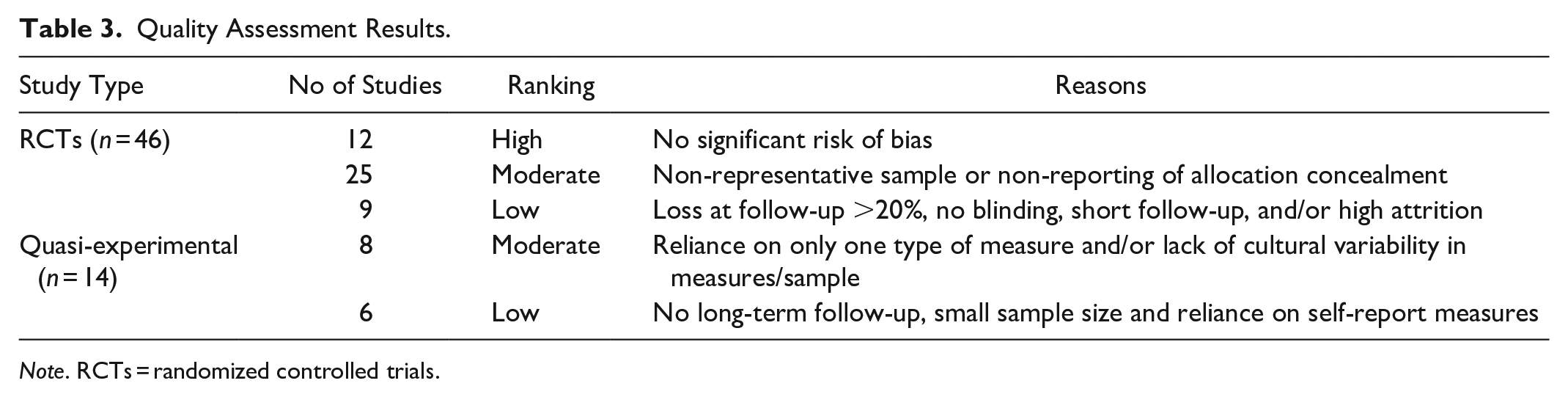
Note. RCTs = randomized controlled trials.
RQ1
What are the Structural and Contextual Components (Including Delivery Techniques) of Parenting Interventions That Aim to Prevent or Decrease CM?
Intervention components were extracted and mapped onto the various ecological levels and the delivery techniques were mapped to corresponding BCTs (see Supplemental File 4 for BCT definitions). There were eleven intervention components identified on the micro-individual level and mapped to 25 BCTs, 15 intervention components on the micro-family level and mapped to 17 BCTs, and 14 intervention components were identified on the Mezzo level and mapped to 20 BCTs. No macro-level components were identified from the included studies.
Figure 3 shows a graph depicting all the BCTs across three ecological levels and the number of corresponding intervention components.
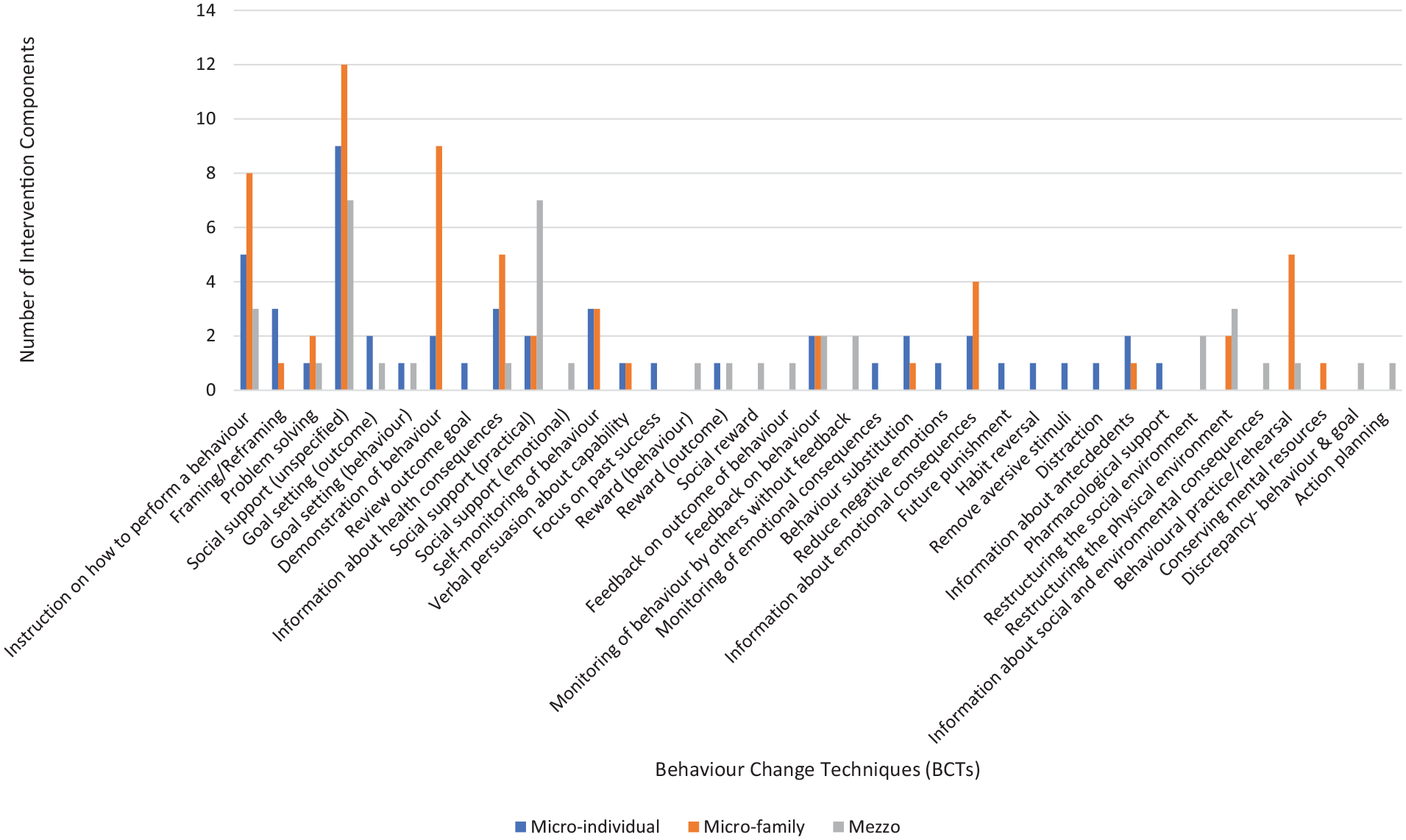
BCTs and the number of intervention components.
Micro-Individual Intervention Components and BCTs
Setting and achieving goals was the most prevalent intervention component at the micro-individual level and was identified in 17 interventions of which 10 showed significant effects for CM outcomes (see Supplemental File 7). Interventions used goal setting as a means of enhancing parents’ confidence (Barth, 1988; Gessner et al., 2008), changing abusive behaviors (Scott et al., 2021), improving parenting (Siolvsky et al., 2011), and as a means of assessing how parents were progressing in the intervention (MacMillan et al., 2005). This component was mapped to six BCTs showing the varying nature of delivery techniques used across interventions to deliver the same component. For instance, Duggan et al.’s (2004) evaluation used the BCT of “Goal setting (behavior)” and mothers were asked to set goals for their mental health. Luthar et al. (2007) intervention used role play exercises and this was mapped to the BCT of “demonstration of behavior.” Interventions also assessed parents’ progress by reviewing goals and this was mapped to the BCT of “review behavior goal” (e.g., MacMillan et al., 2005) and reviewing goal attainment mapped to the BCT of “review outcome goal” (e.g., Scott et al., 2021).
Parental emotional regulation was the second most prevalent intervention component at the micro-individual level and was found in 15 interventions, of which 14 had a significant effect on CM outcomes. Ten BCTs were mapped to the delivery of this component across the 15 interventions. The BCT of “demonstration of a behavior” was used by Fennell & Fishel (1998) evaluation in which practitioners showed parents how to regulate their emotions through modeling. Dawe et al.’s (2007) evaluation of an intervention practiced mindfulness techniques with parents to manage their anger and this was mapped to the BCT of “reduce negative emotions.” The BCT of “feedback on a behavior” was mapped to an evaluation where parents were first listened to and then their feelings were reflected back and clarified to them as a way of enhancing their emotional self-regulation (Fennel & Fishel, 1998). The BCT of “social support (practical)” was used in one intervention which helped pregnant women find housing to reduce their stress levels (Mejdoubi et al., 2015). “Social support (unspecified)” was another BCT used by an intervention that provided anger management counseling to parents (Schaeffer et al., 2021). Dawe et al. (2007) evaluated an intervention that taught parents techniques for managing difficult emotions and this was mapped to the BCT of “instruction on how to perform a behavior.”
Problem-solving skills were another prevalent micro-individual level component that was identified in 12 interventions and mapped to three BCTs. Luthar et al.’s (2007) intervention evaluation described the provision of therapy to enhance problem-solving skills and this was mapped to the BCT of “social support (unspecified)” while another intervention (Ismayilova et al., 2020) coached parents to develop skills to effectively solve daily parenting problems and this was mapped to the BCT of “problem-solving.” Finally, the BCT of “instruction on how to perform a behavior” was used in one intervention which taught parents various skills to identify and find solutions to problems (Huebner et al., 2002)
There were eight other intervention components and these were identified in less than 10 interventions and there were several variations in their corresponding BCTs. For example, the intervention component management of substance abuse was found in nine interventions and mapped to nine BCTs including “pharmacological support” (Schaeffer et al., 2021), “instruction on how to perform a behavior” (Frye & Dawe, 2008) and “remove aversive stimuli” (Donohue et al., 2004), among others.
Figure 4 displays a systems mapping approach showing the links between various intervention components and BCTs, highlighting the variety and overlapping nature of BCTs to deliver components across interventions. The most common BCT at the micro-individual level was “social support (unspecified),” which was linked to nine different intervention components. Following this, the BCT of “instruction on how to perform a behavior” was linked to five components, and the BCT of “self-monitoring of behavior” was mapped to three components.
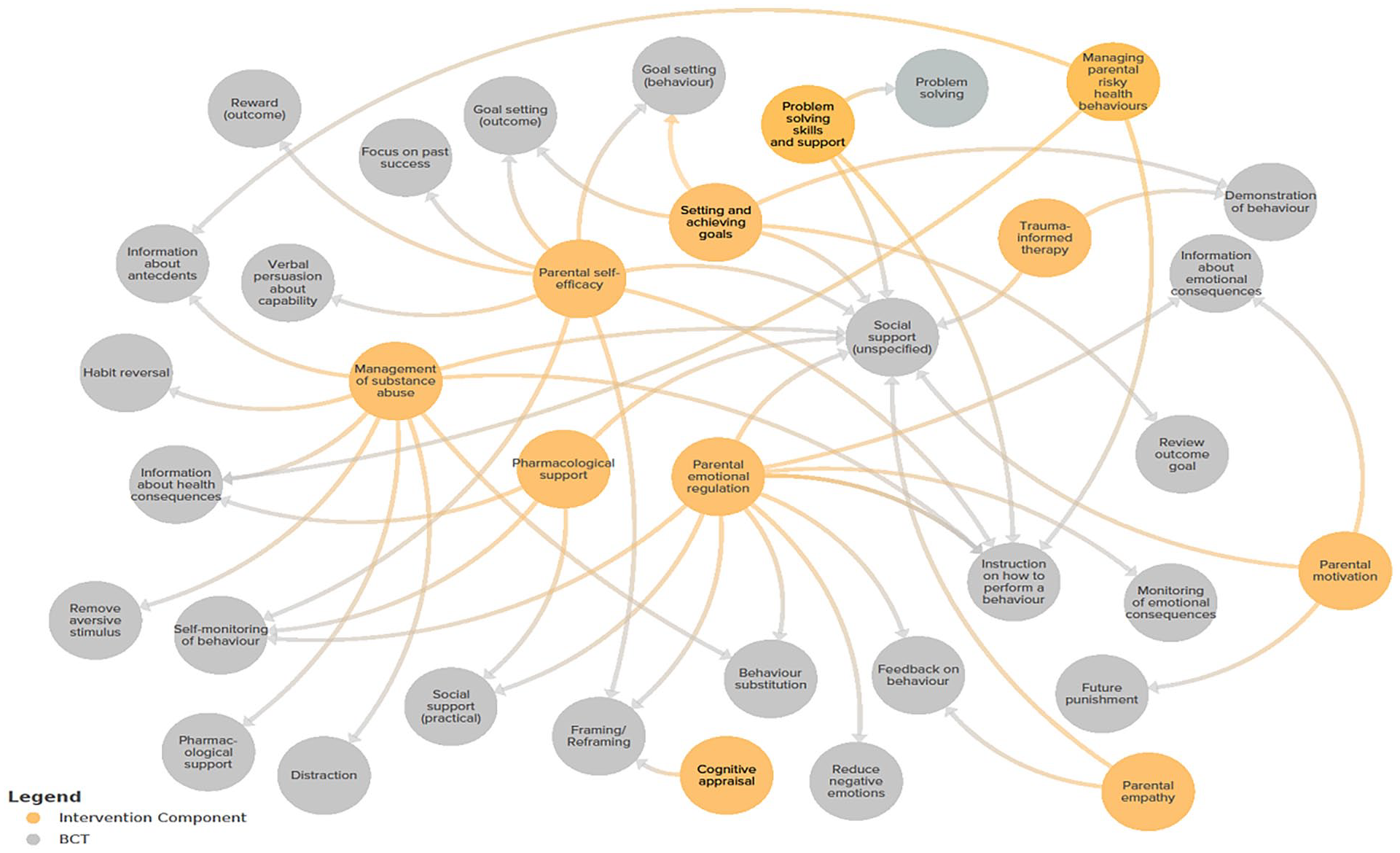
Micro-individual intervention components and BCTs.
Micro-Family Intervention Components and BCTs
The most prevalent component on the micro-family level was “child development education and health information” found in 20 interventions and linked to five BCTs (see Supplemental File 8). For example, the BCT of “instruction on how to perform a behavior” was identified in an intervention that enhanced parents’ knowledge through teaching modules and lectures (Britner et al., 1997). The BCT of “information about health consequences” was linked to the provision of information regarding children’s health and nutrition (Gulirmak et al., 2021). Interventions that used video feedback (BCT of “demonstration of a behavior”) highlighted how their parenting affected children’s emotions and mental health (BCT: “information about emotional consequences”; Gulirmak et al., 2021; Knox et al., 2013).
The second most frequent component was “managing child misbehavior” found in 19 interventions and linked to 11 BCTs. Interventions used the BCT of “instruction on how to perform a behavior” by teaching parents appropriate ways of disciplining their child (Siolvsky et al., 2011). The BCT of “behavioral practice/rehearsal” allowed parents to practice their disciplinary techniques (Jouriles et al., 2010) and the BCT of “behavior substitution” enabled the substitution of abusive practices of discipline with alternative behavior (e.g., time-out; Dawe et al., 2007). The BCTs of “information about antecedents” and “framing/reframing” were mapped to interventions that taught parents to reason with their children and explain the consequences of their behaviors and to help parents identify triggers that may account for children’s misbehaviors and not attribute negative intentions to children (e.g., Donohue et al., 2004). Some interventions helped and enabled parents to deal with parenting challenges such as managing tantrums (the BCT “problem-solving”; Siolvsky et al., 2011). Interventions also showed parents how to alter the environment to prevent hazards (BCT: “restructuring the physical environment”; Huebner et al., 2002) and gave information to parents on how their discipline practices influence children’s physical and psychological development (BCT: “information about health consequences”; Huebner et al., 2002).
The third most prevalent intervention component on the micro-family level was “strengthening relationships,” which focused on creating and maintaining healthy relationships with children, family, friends, and intervention practitioners. This component was found in 17 interventions and linked to five BCTs. Interventions provided information to parents on what comprised a healthy relationship and the consequences of such on parents’ mental and emotional health (BCT: “information about emotional consequences”; Barlow et al., 2019). Interventions provided counseling to parents to improve communication (BCT: “social support [unspecified]”) and taught ways of remaining calm in hostile situations (BCT: “instruction on how to perform a behavior”; Stevens-Simon et al., 2011). Parents were also helped to identify prior toxic relationships and harmful patterns to prevent their reoccurrence (BCT: “feedback on behavior”; Frye et al., 2008).
Figure 5 shows the links between micro-family level components and BCTs. The most frequent delivery techniques or BCTs were those of “social support (unspecified)” which linked to 12 intervention components and “instruction on how to perform a behavior” and “demonstration of the behavior,” which each linked to nine intervention components.
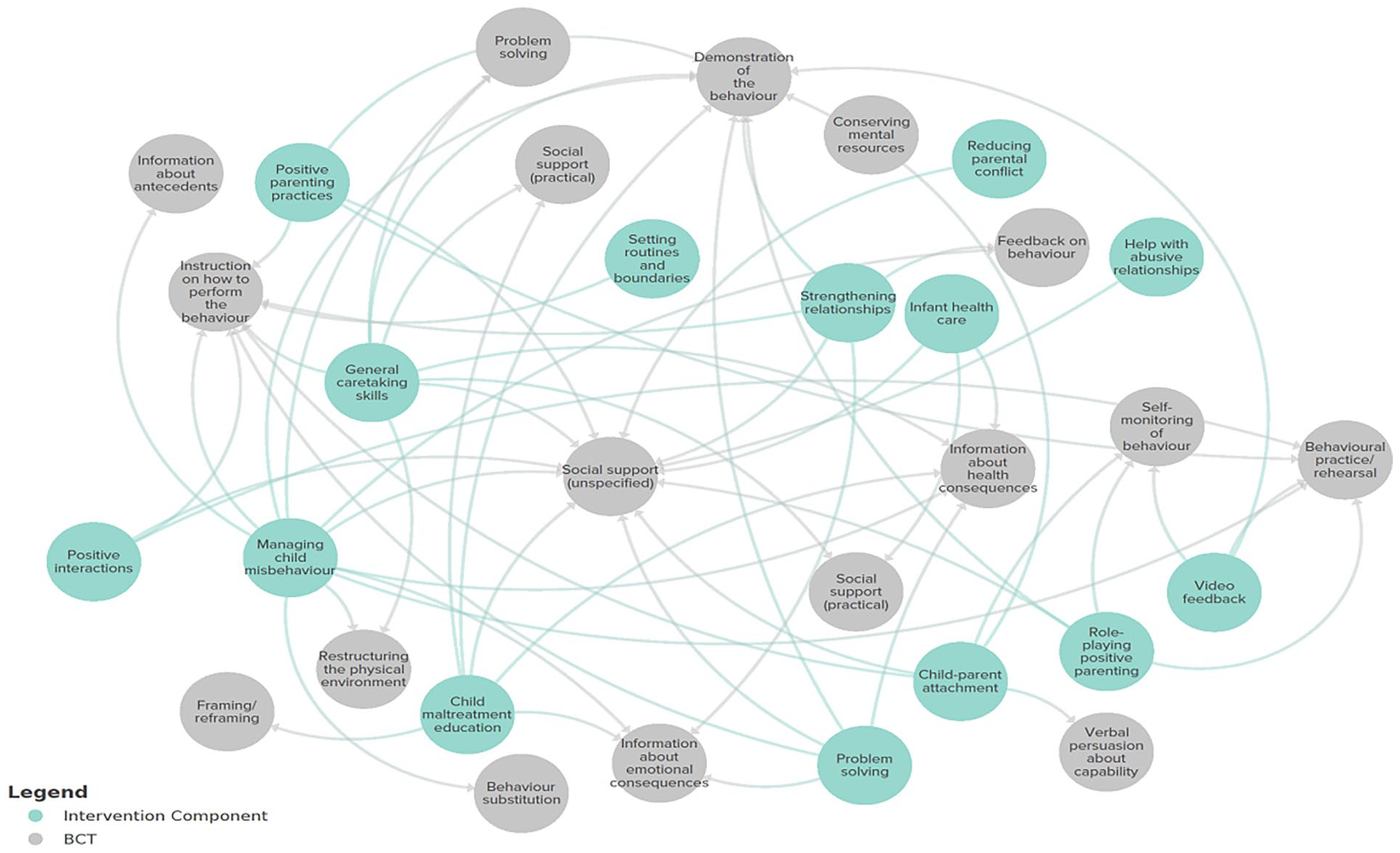
Micro-family intervention components and corresponding BCTs.
Mezzo Level Intervention Components and BCTs
At the mezzo-ecological level, 14 intervention components were identified and linked to 20 BCTs (see Supplemental File 9). The most prevalent intervention component at the Mezzo level was “home visiting” in 40 interventions and linked to the BCT of “monitoring of behavior by others without feedback.” Frye & Dawe (2008) intervention evaluation reported prison visitation for mothers in custody and Eddy et al.’s (2020) evaluation examined home visiting aimed at all family members in the home.
“Social support” was the second most prevalent intervention component and was found in 20 interventions and linked to eight BCTs. This component focused on enhancing parents’ access and use of services as well as creating and maintaining support networks (e.g., with other parents; Dawe et al., 2007; Olds et al., 1986), and this was linked to the BCT of “restructuring the social environment.” In one intervention (Dakof et al., 2010), practitioners helped mothers become independent and set plans in place to balance work and family life. This was linked to the BCT of “goal setting (behavior and outcome).” The same intervention also supported mothers in resolving family crises and dealing with parenting issues (BCT: “problem-solving”). The BCT of “social support (practical)” was linked to interventions that provided practical help such as budgeting and finance (e.g., Gessner et al., 2008), and the BCT of “social support (emotional)” corresponded to the use of therapists and coaches in interventions to help parents better utilize their social networks for support (e.g., Jouriles et al., 2010).
The third most prevalent intervention component was “parenting group sessions” located in 19 interventions and linked to two BCTs, “restructuring the physical environment” and “social support (unspecified).” The former BCT was identified when interventions provided parenting sessions in the community (e.g., Letarte et al., 2010), and the latter was associated with coaching sessions to enable the building of trust between the practitioner and parent in group sessions (e.g., Lachman et al., 2017).
Figure 6 illustrates the intervention components and the corresponding BCTs at the mezzo-level. The most common BCTs were “social support (unspecified)” and “social support (practical),” each linked to seven intervention components. Following this, the BCTs of “instruction on how to perform a behavior” and “restructuring the physical environment” were each linked to three intervention components.
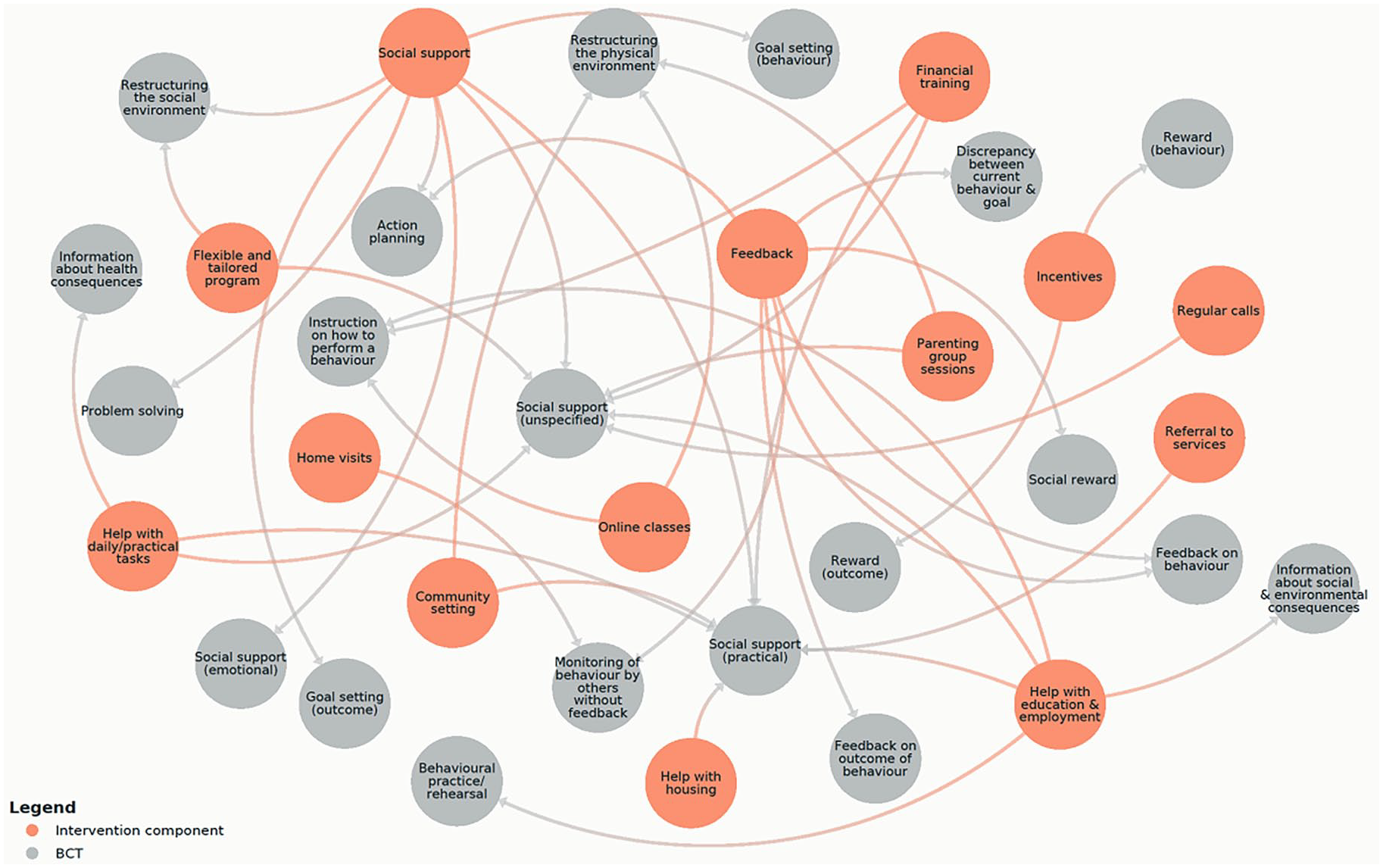
Mezzo interventions components and associated BCT.
Interventions Showing No Effect
Nineteen out of the 60 evaluations did not show an impact on CM outcomes (e.g., Siegel et al., 1980; Siolvsky et al., 2011). There were a few intervention components that were found to be absent in interventions without effect. These included the “cognitive appraisal” and “parental motivation” components at the micro-individual level and “setting routines and boundaries” and “reducing parental conflict” at the micro-family level. Intervention components of “financial training” and “incentives” were lacking at the mezzo level.
With respect to BCTs, only two BCTs were not found in interventions without effect while these were present in interventions that showed an effect on CM outcomes. These included “reward (outcome)” and “reward (behavior).” Of note, two BCTs were prevalent in effective interventions but only identified in one non-effective intervention (Skar et al., 2021). These BCTs were “monitoring of emotional consequences” and “reduce negative emotions.” Both were linked to the intervention components of “parental emotional regulation” found in 14 effective interventions (e.g., Barlow et al., 2019; Frye & Dawe, 2008).
RQ2. How Does the Intervention Content Differ Based on the Specific Type of CM Being Addressed?
From the 41 interventions that showed a significant effect on CM outcomes, only 27 specified a maltreatment type. Table 4 shows the type of maltreatment specified across the 27 effective interventions.
Effective Interventions and Maltreatment Types.
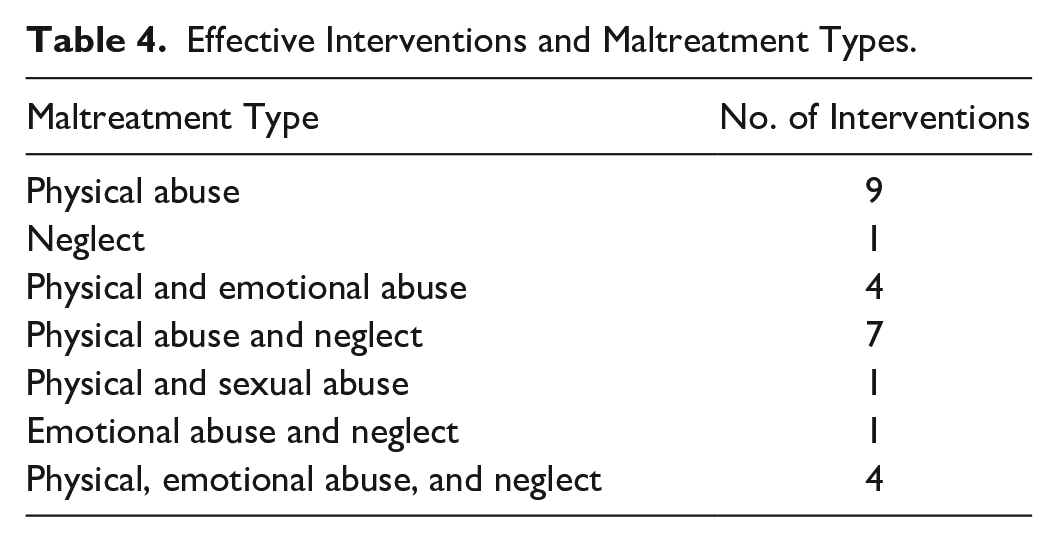
Figure 7 displays the maltreatment-type-specific intervention components across the 27 effective interventions.
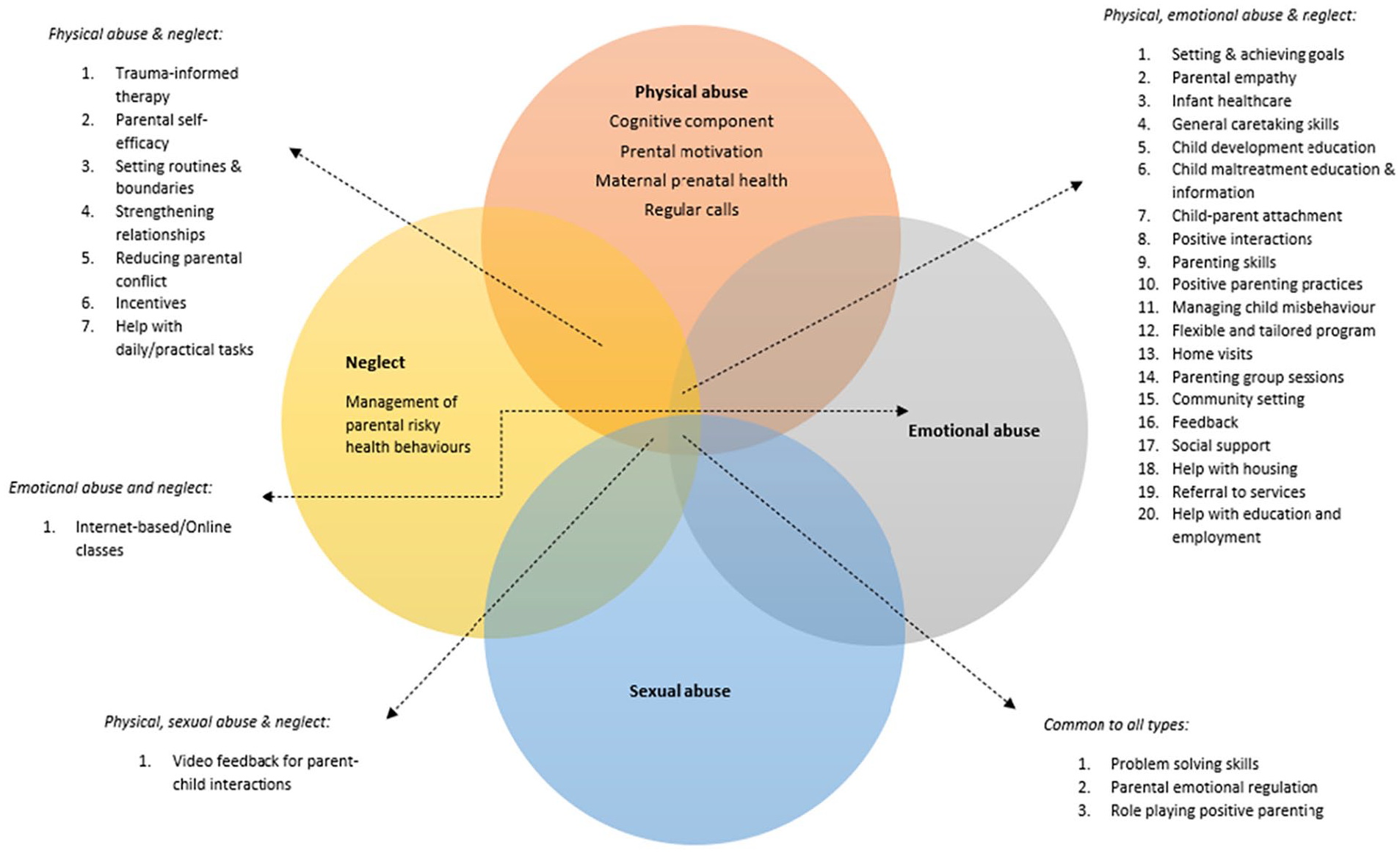
Maltreatment-type-specific intervention components.
Four intervention components were unique to physical abuse. These included the cognitive component (Bugental et al., 2010), parental motivation (Dakof et al., 2010), maternal prenatal health care (Fulton et al., 1991), and regular calls from intervention practitioners (Arruabarrena et al., 2022). For neglect, the management of parental risky health behaviors (Donohue et al., 2004) was the only unique intervention component. No unique components were found for parental sexual and emotional abuse.
The most shared components (20) were between physical, emotional abuse and neglect and included setting and achieving goals (LeCroy et al., 2020), enhancing parental empathy (Guterman et al., 2013), managing child misbehavior (Huebner et al., 2002) and social support (Ismayilova et al., 2020), among others. Physical abuse and neglect shared seven intervention components including trauma-informed therapy (Schaeffer et al., 2021), strengthening relationships (Fergusson et al., 2005), and reducing parental conflict (John et al., 1984). The only shared component between physical, sexual abuse, and neglect was video feedback for parent–child interactions (Fennell & Fishel, 1998). There was one shared intervention component between neglect and emotional abuse which was internet-based online classes (Gulirmak et al., 2021). Common intervention components of problem-solving skills, parental emotional regulation, and role-playing positive parenting were found for all four maltreatment types (e.g., Fergusson et al., 2005; Schaeffer et al., 2021).
Discussion
This systematic review was guided by two RQ; what are the structural and contextual components (including delivery techniques) of parenting interventions that aim to prevent or decrease CM? Second, how does the intervention content differ based on the specific type of CM being addressed? The review examined intervention components across 60 intervention evaluation studies for parental CM. It explored the varying delivery techniques used to implement the components through BCTs and finally, explored maltreatment-type-specific variation among intervention components. The review found that at the micro-ecological level, potentially effective intervention components such as goal setting and achievement, parental emotional regulation, managing child misbehavior, relationship strengthening, and problem-solving skills were included. At the mezzo level, home visits, parenting group sessions, and social support were frequently utilized. No macro-level intervention components were identified in the review. The BCT framework (Michie et al., 2013) enabled identification of delivery of components. The most prevalent BCTs across all ecological levels were social support (unspecified) and instruction on how to perform a behavior. Further, on the micro level, self-monitoring of behavior and demonstrations of the behavior were prevalent BCTs while at the mezzo level, social support (practical) was commonly utilized.
From the included studies in the review, only 41 interventions were effective and from these, 27 identified a specific type of maltreatment. With respect to maltreatment type variance, interventions targeting physical abuse featured the most unique components such as cognitive appraisal, enhancing parental motivation, and promoting maternal prenatal healthcare. Those interventions focusing on neglect had a single unique intervention component of managing parental risky health behaviors. No unique intervention components were identified for emotional or sexual abuse. Components common across all maltreatment types included problem-solving skills, parental emotional regulation, and role-playing positive parenting.
Study Characteristics
From the included studies, there were 41 effective interventions and the majority of these reported a small effect on CM outcomes. Prior meta-analytic evidence of interventions is supportive of this finding with effect sizes generally small for preventing or reducing CM (Euser et al., 2015; Ijzendoorn et al., 2020).
A mix of self-report and objective measures were used in the included evaluations and from the 41 interventions showing an effect, 20 evaluations used self-report measures only, and 21 used objective measures either on their own or with a self-report measure. Prior evidence consistently points to the superiority of objective measures to lower the risk of bias (Hawes & Dadds, 2006). It may be difficult to assess whether parents’ self-reports are accurate, and there may be under-reporting of abusive behavior and over-reporting of changed behavior (Oliver & Washington, 2009). Researchers need to adapt measures that reduce the risk of bias to present an accurate assessment of intervention effectiveness.
Fifteen countries were represented in the included evaluations but 86% of the studies were from high-income countries including the U.S., Australia, U.K., and other European countries while only 14% included low- and middle-income countries (LMIC) including Iran, Tanzania, Thailand, and Burkina Faso (West Africa). As most of the evidence on CM evaluations comes from HIC, evidence tilts toward the Global North (McCloskey, 2011). However, since CM is a global concern, gaining insight into effective intervention components in LMIC can provide needed insight and promote uniformity in the global prevention of CM.
Intervention Components
The most prevalent intervention components from effective interventions on the micro level (individual and family) included setting and achieving goals. Ward et al. (2014) conducted a narrative systematic review of child protection cases highlighting goal attainment as a reflection of parental motivation to change behaviors. This component has also been included in interventions for institutionally maltreated children (Finch et al., 2021). However, evidence on the effectiveness of this component is limited and this is generally not highlighted as prevalent or significant in prior syntheses (e.g., van der Put et al., 2018; Melendez-Torres et al., 2019). Researchers need to shift attention to examining the efficacy of this component given its found in majority of the effective CM interventions.
Parental emotional regulation, another prevalent intervention component, is supported by prior evidence. Branco et al.’s (2021) systematic review of universal parenting programs highlighted the role of this component in reducing CM risk. Similarly, evidence suggests that enabling parents to manage their anger and stress can be particularly significant for reducing physical abuse (Lavi et al., 2021; Stith et al., 2009).
There is some conflicting evidence for the third most prevalent intervention component of problem-solving. A meta-analysis by Gubbels et al. (2019) found that this component did not contribute to the efficacy of interventions. However, another meta-analysis (van der Put et al., 2018) found that programs focusing on enhancing parenting skills, including problem-solving, have a larger effect size compared to those who don’t engage parents. More research on the effectiveness of this component can inform interventions about its potential inclusion to avoid wasting resources on ineffective components. Similarly, Mikton and Butchart’s (2009) review of reviews found some evidence of the effectiveness of the parental problem-solving component in reducing the overall risk of CM but not actual CM.
Parent education was also a prevalent intervention component found in our review. Scott et al.’s (2022) meta-analysis did not find parent education as effective for preventing abusive head trauma in infants. Given this evidence, it is possible that parent education is more effective in universal programs or those targeting a specific sub-group of parents (e.g., adolescent mothers) who may lack knowledge about parenting and child development (Cullen et al., 2017). Also, educational interventions target the enhancement of parenting rather than direct CM reduction or prevention (Holzer et al., 2006) suggesting that this component may be redundant in directly affecting CM outcomes. A closer examination of this intervention component and its utility in CM interventions is further warranted.
Managing child misbehavior was another prevalent component. A prior review of interventions to prevent the recurrence of child physical abuse found that this component was effective in reducing physical abuse by teaching parents strategies and appropriate methods of managing their children’s behavior and providing alternatives to abusive discipline (Melendez-Torres et al., 2019). A link was also noted between this component and parental emotional regulation. Studies reveal that parental dysregulation of emotions is linked to harsh physical punishment and inappropriate attributions of intent to child misbehavior (Mammen et al., 2002). Given that both these components are linked, it makes sense for interventions to have a collective strategy in which parental emotional regulation and management of child misbehavior are combined. Further research can establish the link between these two components and whether their absence or presence affects CM prevention and reduction.
The component of strengthening relationships, identified in our review as prevalent on the micro-family level, is supported by prior research. Previous longitudinal studies have established the protective nature of safety, nurturing, and supportive relationships for CM (Jaffee et al., 2013; Schofield et al., 2013). There is also evidence that a trusting relationship between practitioner and parent can help reduce the risk of CM (Vseteckova et al., 2021).
Mezzo-level prevalent components included home visiting identified in 26 effective interventions. Han and Oh (2022) systematically reviewed the evidence and found home visiting to be effective in CM prevention and reduction and Peacock et al. (2013) found effectiveness for this component especially when it begins in the prenatal period. There is some conflicting evidence with respect to the length and intensity of home visits with prior meta-analytic evidence (Nievar et al., 2010) finding that the effectiveness of this component rests on longer length and higher frequency of delivery. However, systematic reviews (e.g., Aslam & Kemp, 2005; Kendrick et al., 2000) find that duration of home visits aligns with the co-occurrence of risk factors, with more vulnerable families requiring more intense and longer home visits. More research to explore the intensity of home visiting and its association with mitigating various risks can illuminate its pathway to effectiveness.
A majority of the reviewed effective interventions had social support as a common intervention component and this is supported by prior evidence (e.g., Cutrona, 2000). Parental stress and isolation can elevate the risk of CM; hence, the provision of social support can buffer this risk (Thompson, 2015). What is not evident from prior research is the distinction between different types of social support (e.g., counseling, help with housing, referral to services) and their contribution to CM prevention.
There is also some overlap noted between the component of home visiting and that of social support. Prior literature reveals that social support without “social monitoring” is not as effective and in fact, informal social support can be harmful especially when there is an acceptance of abusive parenting (Thompson, 1995). A collective strategy of both formal social support and a monitoring element (e.g., home visiting) may be optimal for CM interventions.
Finally, the third most prevalent intervention component on the mezzo level was parenting group sessions. Previous literature reveals that parenting groups can be effective in reducing mental health difficulties and enhancing social connections (Lyu et al., 2022). However, conflicting meta-analytic evidence suggests that individual settings are more effective than group ones, especially in reducing child physical abuse risk. Researchers need to establish evidence for the efficacy of this component and its association with parenting risk.
No macro-level intervention components were identified from the included evaluations. It is arguable that interventions may not have the remit to provide national or policy-level intervention components. Government policy and legislation may be best suited for the provision of national-level campaigns, education, service availability, and promotion of service utilization to reduce and prevent parental CM (Austin et al., 2020; Klevens et al., 2016).
Behavior Change Techniques
The most common delivery techniques used to implement intervention components were the BCTs of “social support (unspecified)” and “instruction on how to perform a behavior” across micro and mezzo ecological levels. “Self-monitoring of behavior” was prevalent on the micro-individual level, “demonstration of the behavior” at the micro-family level, and “restructuring the physical environment” and “social support (practical)” at the mezzo level.
The use of the BCTT (Michie et al., 2011) to explore delivery techniques of CM interventions is a novel approach. While prior literature supporting this review’s findings is scarce, there is some evidence from research that substantiates the use of certain BCTs in interventions. For instance, a prior study found that BCTs of “instruction on how to perform a behavior” and “restructuring the physical environment” are prevalent in interventions targeting intergenerational CM (Younas & Gutman, 2022b). Howlett et al.’s (2022) systematic review of substance abuse interventions also found BCTs of “instruction on how to perform a behavior” and “social support (unspecified)” to be common among effective interventions.
In prior syntheses of evidence for CM, specific techniques of delivery for intervention components have not been explored in much detail. Kaminski et al.’s (2008) meta-analysis did find that teaching parents and demonstrating effective parenting skills result in positive outcomes for CM lending support to the BCTs prevalent in our findings. The majority of prior reviews focused on intervention components (e.g., Temcheff et al., 2018) and more research to delineate specific delivery techniques for components can provide insight into whether they are optimal.
Interventions Without Effect
Cognitive appraisal and enhancing parental motivation were two components missing from interventions without effect. Melendez-Torres et al.’s (2019) systematic review of the prevention of child physical abuse did not find either of these components as effective. However, with respect to cognitive appraisal, a prior RCT found that this is effective in reducing parental stress (Preuss et al., 2021). As high levels of parental stress are associated with CM (e.g., Geprägs et al., 2023), it is possible that not including this component contributed to the lack of effect in the interventions. Similarly, components of reducing parental conflict and setting routines and boundaries were also missing from ineffective interventions. There is contradictory evidence regarding these components with some evidence that improvement of specific parenting skills does not directly impact CM outcomes (Gubbels et al., 2019) while other evidence suggests that parenting skills can impact outcomes for maltreating parents (van der Put et al., 2018). However, based on the “spill-over hypothesis” (Nelson et al., 2009), frequent conflict between parents can spill over onto the parent-child relationship. One explanation for the lack of effect in these interventions could be attributed to these missing intervention components. For instance, coupled with high parental stress and parental conflict, there may be an increase in negative parenting behaviors (e.g., hostility towards child, harsh discipline), ultimately increasing the risk of CM (Sturge-Apple et al., 2006). For parenting interventions targeting the reduction and prevention of CMs, the integration of components that focus on cognitive appraisal and reduction of parental conflict may be necessary for the intervention to be successful. Further research examining these specific intervention components and their links with intervention effectiveness is needed to establish their significance.
For BCTs, two were missing in interventions without effect; BCTs of “reward (behavior)” and “reward (outcome).” These were linked to components of incentives and enhancing parental self-efficacy. Schoeppe et al. (2014) suggest that incentives can enhance parental program engagement. However, an evaluation of an intervention providing incentives to parents did not lead to lower attrition (Quetsch et al., 2020). More research on these delivery techniques can provide insight into whether they are optimal or redundant for CM outcomes.
Comparisons of components and delivery techniques between effective and non-effective interventions are outside the scope of this systematic review; however, to implement best practices in CM interventions, future research is needed to fill this gap.
Maltreatment-Type-Specific Variation in Intervention Components
Prior evidence supports the efficacy of managing child misbehavior and parental emotional regulation as effective for reducing and preventing physical abuse (Barlow et al., 2006; Melendez-Torres et al., 2019). Our review found that neglect and emotional abuse shared online provision of the program in effective interventions. Nieuwboer et al. (2013) meta-analysis found online classes enhanced parenting outcomes. There is, however, a sparsity of evidence of the effectiveness of online interventions for CM outcomes. As CM interventions can be limited in engaging the parents who require these services the most (Rostad et al., 2018), online alternatives may be promising, particularly considering the COVID-19 pandemic and the consequential surge in CM (Park & Walsh, 2022). Implementation and evaluation of online programs need more focus from research, especially for neglect and emotional abuse.
Video feedback for parent–child interactions, as shown in Figure 7, was a shared component among child physical, sexual abuse, and neglect. Fukkink (2008) meta-analysis revealed video feedback can enhance parent–child interactions and general parenting competency for parents at risk of CM. Similarly, Cassiba et al. (2015) found video feedback to be effective in reducing aggressive and frightening caregiving behavior and promoting appropriate ways of disciplining children, resulting in a lower risk for physical abuse. Evidence suggests that this component can help enhance mother–child attachment by recording interactions between the parent and child and emphasizing strengths of the relationship (de Graaf et al., 2009). There is limited evidence on how this component can help prevent child sexual abuse and more research to establish an association between the two is required.
Our review found the most maltreatment-type-specific components for physical abuse. Evidence of the effectiveness of the cognitive appraisal component exists in prior research (e.g., Lawson et al., 2020). Azar and Weinzierl (2005) suggest that maltreating parents have maladjustments in their cognitive schemas resulting in misattribution of intent to children’s misbehavior and enhancing the risk of physical abuse. Cognitive reframing to shift this schema can reduce the risk of CM.
For parental motivation, prior evidence syntheses (Barlow et al., 2006) support its efficacy for reducing child physical abuse. Regular calls from intervention practitioners were another intervention component specific to physical abuse but there is a sparsity of evidence on its effectiveness. It is possible that regular calls from the intervention provide an additional monitoring aspect (akin to home visiting) which may be helpful in reducing physical abuse risk.
Our review identified only one neglect-specific intervention component which was the management of parental risky health behavior, and this was found in one intervention examining neglecting mothers who had used substances during their pregnancy. Prior evidence suggests that the provision of advice and information on safe sexual behaviors, contraception, and antecedents to sexually transmitted diseases can be effective in reducing neglect. There is also some empirical evidence of parental history of childhood physical and sexual abuse and its association with promiscuity and unsafe sex practices in adulthood (Hillis et al., 2001; Widom & Kuhns, 1996). Research on mothers who are sex workers and those who also misuse substances have a higher risk of child neglect (McClelland & Newell, 2008). More research can establish the effectiveness of this component, especially for child neglect and for specific parenting subgroups.
No maltreatment-type-specific components were identified for child emotional and sexual abuse. In CM literature, the focus on these two maltreatment types is relatively less compared to physical abuse and neglect, calling for a shift in focus by researchers to consider effective intervention provisions for emotional and sexual abuse.
Limitations
In the first instance, the narrow inclusion criteria restricted study inclusion to only published research in peer-reviewed journals that may have led to the exclusion of relevant and valuable evidence falling outside this criterion. While this was done to ensure high-quality evidence was included, especially given the copious published research on the subject, unpublished evidence could have reduced bias and provided further insight.
Further to this, a second reviewer was not included to check reliability in the systematic review processes, especially for searching and screening of studies that may have enhanced selection bias. This was done due to a lack of resources and the large number of studies included in the systematic review. However, steps were taken to ensure risk is minimized through multiple searches in databases, snowballing, and including primary studies from relevant systematic reviews.
Thirdly, all the data synthesized in our review was based on researchers’ description of interventions and while one criterion for inclusion was sufficient information about components, researchers may have failed to report all intervention components and the way in which they were delivered. Similarly, included studies were RCTs and quasi-experimental studies, and no relevant qualitative study or other study designs emanated from the database searches signifying evidence that may have been missed. Furthermore, nearly half of the included evaluations relied only on self-report measures; thus, the validity of responses and links to effectiveness can be questionable. There may be bias in reporting in such measures (Schaeffer, 2000) so care should be taken to interpret these findings in light of this limitation.
Another potential limitation is the use of the BCTT framework (Michie et al., 2013) to extract delivery techniques of intervention components, as this is a novel approach and findings are exploratory in nature. It is unknown to what extent the delivery of components was implemented as described and whether all techniques were reported in the evaluations. There were also no significant findings in relation to differences in BCTs between effective and non-effective interventions. More research is needed to elucidate the applicability of this framework for CM interventions, particularly for delineating delivery techniques from intervention components.
Furthermore, researchers of included evaluations used several umbrella terms (e.g., parent education, social support) which represented multiple individual components, and this was a challenge when synthesizing findings. Efforts, however, were made to ensure intervention components were narrow and specific. For instance, positive interactions and positive parenting practices were categorized as separate with each representing different aims and strategies in our review despite the majority of included evaluations categorizing these under parent training. A uniform approach is needed by researchers to describe intervention components and ensure that singular strands are categorized separately as they each target unique skills and behaviors rather than falling under one umbrella term. Expert consensus in the classifications and uniformity in the description of intervention components can reduce heterogeneity across CM evaluations and improve their reporting and replication.
Finally, a significant evidence gap in maltreatment-type-specific intervention components for emotional and sexual abuse limits the conclusions. Further research can increase knowledge and highlight intervention efforts to reduce and prevent parent perpetration of child emotional and sexual abuse.
Diversity
Representation of intervention evaluations of CM from LMIC was low, and the majority of evidence was from the Western hemisphere. Researchers stress the need for culture-based and region-specific CM interventions from around the globe (Badrfam & Zandifar, 2021), which can enhance the applicability of findings. It can also show the transferability of effective interventions in HIC to LMIC and any associated issues.
A lack of fathers’ representation was also of note. Many evaluations either focused solely on mothers or both parents and only one intervention targeted fathers (Scott et al., 2021). This indicates a significant gap in knowledge of optimal ways of supporting fathers to prevent and reduce CM (Dolan, 2013). Efforts are needed from both intervention developers and researchers to target and engage fathers and help bridge this evidence gap.
Key Findings and Implications
Table 5 presents a summary of the key findings of this systematic review and its implications for research and practice.
Summary of Critical Findings and Implications.
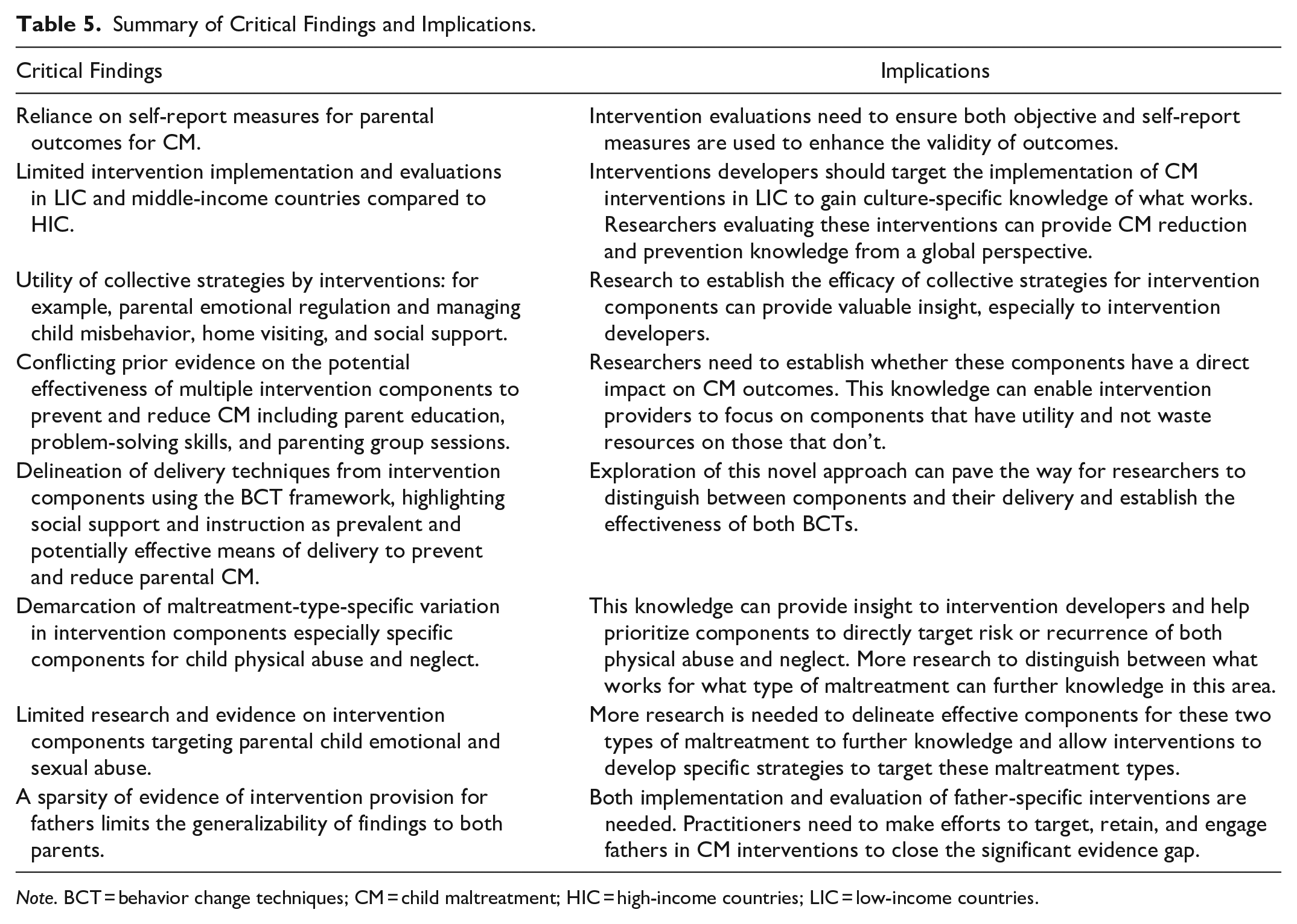
Note. BCT = behavior change techniques; CM = child maltreatment; HIC = high-income countries; LIC = low-income countries.
Conclusion
This systematic review synthesized evidence on intervention provision from 60 CM intervention evaluation studies. An examination of intervention content revealed prevalent and potentially effective intervention components and delivery techniques (BCTs). On the micro levels (individual and family), setting and achieving goals, parental emotional regulation, problem-solving skills, managing child misbehavior, child development education, and strengthening relationships were the most common intervention components in effective interventions for CM. On the mezzo level, home visiting, parenting group sessions, and social support were prevalent intervention components.
The BCT framework (Michie et al., 2013) helped to distinguish between intervention components and the way they were delivered. The most prevalent BCTs were “social support (unspecified)” and “instruction on how to perform a behavior” across all ecological levels. “Self-monitoring of behavior” on the micro-individual level, “demonstration of the behavior” on the micro-family level, and “social support (practical)” on the mezzo level were most common. No macro-level intervention components were identified from the studies.
Of the 41 effective interventions, only 27 specified a maltreatment type. Intervention components common to all maltreatment types included problem-solving skills, parental emotional regulation, and role-playing positive parenting. Physical abuse had the most unique components (e.g., cognitive appraisal, enhancing parental motivation, and maternal prenatal healthcare) followed by neglect which only had one unique component of management of parental risky health behaviors. No maltreatment-type-specific intervention components were identified for emotional and sexual abuse.
Collective strategies in intervention provision (e.g., home visiting and social support) merit additional research to establish the efficacy of these combined components. The use of the BCTT can pave the way for further examination of CM interventions using a behavior change perspective. More research on specific intervention components targeting emotional and sexual abuse is needed. Researchers need to shift attention to delineating specific strands of components rather than using umbrella terms (e.g., parent education or social support) in order to specify the various strategies used within these components enabling a more thorough assessment of their effectiveness as well as comparison with other components. Further, a cross-cultural perspective is needed, especially intervention implementation and evaluation in LMIC, to inform global reduction and prevention of CM. Finally, efforts to target fathers in interventions and to promote their engagement and retention are needed to fill a significant gap in the evidence about what works for fathers and how intervention provision can support them.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-1-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-2-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-3-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-3-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-4-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-4-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-5-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-5-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-6-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-6-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-7-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-7-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-8-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-8-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-9-tva-10.1177_15248380241305572 – Supplemental material for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components
Supplemental material, sj-docx-9-tva-10.1177_15248380241305572 for Unpacking Parenting Intervention Content for Child Maltreatment: A Systematic Review Examining Core Components by Fatima Younas and Leslie Morrison Gutman in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.