
Abstract
Recognizing that intimate partner violence (IPV) negatively affects college students’ health and well-being, colleges offer preventive interventions to address these effects. However, scholarly evidence on this effort has been limited, such that we know little about the risk factors addressed, theoretical approaches, target outcomes, and other essential intervention characteristics. To address this gap, this study reviewed evidence-based IPV preventive interventions conducted in U.S. colleges reported in 25 peer-reviewed articles and dissertations published between 2010 and 2020. Findings showed that IPV preventive interventions for college students were designed to address multilevel risk factors of IPV, typically via bystander interventions and emerging skill-building interventions. Most IPV preventive interventions were theoretically driven primary preventions or a combination of primary and secondary preventions. Most studies of program outcomes focus on awareness of IPV and bystander roles, but 44% of the included articles measured participants’ behavioral outcomes (e.g., actual bystander behavior, reaction to IPV disclosure, IPV screening behavior, social emotional skill use, or decreased rates of IPV perpetration) based on participants’ use of skill-building components (e.g., bystander strategies, healthy relationship skills, conflict resolution, communication skills, empathy, and self-regulation). Student participants in the included studies were predominantly white (>60%) and only two studies included any Latinx students or students at historically Black colleges and universities. This review indicates that future IPV prevention practice, policy, and research must further define and explore how multilevel IPV prevention approaches can address the various systems level of needs among diverse student subpopulations.
Keywords
Intimate partner violence (IPV) is a preventable public health issue. IPV includes diverse forms of abuse or aggression that occur in romantic relationships, including physical, sexual, or psychological abuse and stalking by a current or former intimate partner (Centers for Disease Control and Prevention [CDC], 2022a). A recent American Association of Universities study of college students from a representative sample of 33 universities indicated that 10% of students had experienced IPV victimization since enrolling in college, with prevalence ranging from 6% to 14% across colleges/universities (Cantor et al., 2020). Other studies of multisite samples of college students have shown higher IPV rates, ranging from 32% to nearly 64% (Barrick et al., 2013; Cho et al., 2020; Kaukinen et al., 2015).
Among college students, the risk of experiencing IPV is highest in the typical undergraduate years, ages 18 to 24 (Johnson et al., 2015; Smith et al., 2018). This resembles IPV in other populations, as IPV victimization and perpetration risk begins in adolescence, peaks in prevalence between ages 18 and 24, and decreases in prevalence over subsequent years (Johnson et al., 2015; Smith et al., 2018). Recent studies have shown that IPV places undergraduate college students at a higher risk of numerous adverse physical, psychological, and social outcomes that diminish their well-being and academic success, including physical injuries requiring medical attention, post-traumatic stress disorder, depression, anxiety, suicidality, and problematic substance use (Voth Schrag & Edmond, 2018). Student survivors of IPV have high rates of persistent fear and problems with daily routines after victimization (Cho et al., 2020) as well as poor academic performance, including low grade point average, decreased interest in engagement with the course material, and an inability to follow academic schedules (Banyard et al., 2017; Wood et al., 2020).
Similar to other populations, college students experience IPV in different types, including intimate terrorism and situational couple violence (Johnson, 2008). Intimate terrorism involves coercive controlling, and it is largely understood as gender-based violence perpetrated by men against women to dominate and control one’s partner. Situational couple violence occurs in the context of relationship conflicts based on lack of conflict resolution or communication skills but is not rooted in pervasive patterns of control (Hardesty et al., 2017; Johnson, 2008; Love et al., 2020). College student IPV, like IPV generally, is gendered in that college women experience more sexual abuse and more injuries from IPV than college men (McDermott et al., 2015). However, college student IPV involves bidirectional reports of violence. That is, college students are more likely to be both a survivor and perpetrator of IPV than a perpetrator only or a survivor only (Kaukinen et al., 2015; Varlioglu et al., 2022). This bidirectional pattern of violence is found across all racial/ethnic demographics and gender identities (An et al., 2023; Graham et al., 2019). While a high prevalence of IPV perpetration among college students requires careful interpretation that includes a consideration of gender differences in patterns and harms of IPV and conceptual and measurement issues of IPV victimization and perpetration (Eisner, 2021), efforts to prevent IPV among college students are urgently needed.
Risk factors of IPV among college students may differ by the type of IPV. For example, intimate terrorism (coercive controlling or gender-based violence) is linked to gendered norms (e.g., patriarchal beliefs), power imbalance between intimate partners, especially power and control over women, and peer/social groups that support violence and reinforce toxic masculinity (Capaldi et al., 2012; Elmquist et al., 2016; Hays et al., 2015; Love et al., 2020). By contrast, situational couple violence is linked more to stress-related risk factors, including poor communication and conflict resolution, relationship dissatisfaction, and insecure attachment (Love et al., 2020). Characteristics of the college experience can also serve as risk factors for situational couple violence (Duval et al., 2020), for example, academic stressors (Mason & Smithey, 2012) and access to alcohol (Carey et al., 2015). College students themselves commonly identify communication difficulties as a primary reason they have committed physical violence toward their intimate partner (Elmquist et al., 2016), likely because many college students do not know how “to skillfully communicate their feelings” and “have limited relationships skills” (Kaukinen, 2014, p. 285). Various IPV risk factors that are potentially tied to different types or motives for violence faced by U.S. college undergraduates underline the clear need for understanding how these different IPV risk factors have been addressed in IPV preventive interventions in college contexts.
Many institutions of higher education have established programs under the Campus Sexual Violence Elimination (SaVe) Act of 2013. The SaVe Act requires institutions of higher education to provide programs that prevent sexual assault and other forms of violence, including different forms of IPV. Over the past decade, sexual assault and/or IPV prevention efforts have revealed that bystander programs (i.e., Bringing in the Bystander) are effective tools for preventing sexual assault and/or IPV and have been shown to produce modest short-term increases in IPV awareness and intent to help peer IPV survivors (Banyard et al., 2007; Storer et al., 2016). Other emerging approaches (e.g., the Red Flag Campaign, which combines a social marketing campaign and the bystander approach to IPV; Borsky et al., 2018) have also shown promising results. However, the subject of IPV is often subsumed within programs on sexual assault prevention (Jouriles et al., 2020; Moynihan et al., 2011), and programs for college undergraduates focused solely or predominantly on IPV prevention remain scarce. This is problematic because sexual assault victimization includes violence victimization by perpetrators who are not always an intimate partner (CDC, 2022a, 2022b)—only about 35% of sexual assaults that are reported on college campuses are any of the form of IPV (Bhochhibhoya et al., 2021). Consequently, it is important to understand the evidence-based prevention programs that have explicitly aimed to address IPV.
To date, reviews of IPV interventions for undergraduate college students have primarily focused on approaches for preventing sexual assault (DeGue et al., 2014; Jouriles et al., 2018; Kettrey & Marx, 2019; Katz & Moore, 2013; McMahon et al., 2017). Preventive interventions that focus on other forms of IPV among students have largely been ignored in these reviews. Furthermore, systematic reviews on IPV focus on interventions designed to change bystander attitude regarding IPV and increase bystander intervention behavior (Park et al., 2023; Storer et al., 2016). IPV interventions for college students that address other IPV risk factors have been overlooked in these reviews. Inspired by an ecological systems perspective, Casey and Lindhorst (2009) emphasized the need for multilevel violence prevention programs that address multifaceted risk factors related to individual knowledge, attitudes, or behaviors as well as peer- and community-level risk factors. With this in mind, the current study seeks to review essential characteristics of campus-based IPV prevention programs and address gaps in the literature.
Current Study
The current study reviews college-based IPV prevention programs that have attempted to address IPV using a multifaceted definition of IPV (e.g., not only sexual violence). It is based on the CDC’s definition of IPV, which encompasses any aggressions committed against an individual by a current or former intimate partner, including dating violence (DV) and domestic violence, physical, sexual, and psychological violence, and stalking (CDC, 2022a, 2022b).
We conducted this scoping review to address questions about what types of interventions have been designed and evaluated to prevent IPV among college students. Specifically, the current study applies an ecological systems lens to review and analyze the multilevel risk and protective factors, theoretical underpinnings, target intervention outcomes, skill components, delivery methods, and other essential characteristics of IPV preventive interventions (e.g., sample, setting, prevention type, and design). Four research questions guided the present inquiry: (a) What are the characteristics of IPV preventive interventions (e.g., sample, setting, prevention type, and design)? (b) What types of risk and protective factors are these IPV preventive interventions designed to address? (c) What are the major theoretical underpinnings of these interventions? (d) What outcomes were measured for these interventions? (e) What skill-building components do these interventions include? (f) How were these interventions delivered?
Methods
To answer the research questions, we conducted a scoping review of the existing evidence on college-based IPV preventive interventions to identify the types and salient features of college-based IPV prevention programs. Scoping reviews are appropriate for our study as they are defined as “a method of knowledge synthesis that identif[ies] trends and gaps within an existent, emerging knowledge base, or scope of knowledge, for the purpose of informing research, policy, and practice” (Westphaln et al., 2021, p. 2).
Focus Population
Our focus population was undergraduate college students who attend any U.S. university or college. We focused on undergraduates because they are more likely than graduate students to experience IPV victimization (Cantor et al., 2020). Moreover, IPV intervention studies often use “college students” to indicate an undergraduate student sample and rarely to indicate both undergraduate and graduate students.
Study Eligibility Criteria
Studies eligible for inclusion in the present scoping review (a) are in English; (b) include journal articles, dissertations, or theses; (c) test or evaluate a prevention program designed to prevent IPV among undergraduate college students; (d) were implemented in a college setting; (e) used a pre-, quasi-, or randomized controlled experimental design; and (f) reported an effective outcome in at least one outcome indicator (e.g., learning, behavior, and result outcome) based on their hypotheses. This review excluded studies conducted outside the United States, studies that only included graduate students, and those that only focused on interventions in sexual assault but not other types of IPV because such interventions have already been reviewed in multiple systematic and meta-analyses (e.g., Jouriles et al., 2018; Kattrey & Max, 2019; McMahon et al., 2017).
Data Sources and Search Strategies
We searched the literature for all evaluations of IPV prevention interventions for undergraduate college students published between January 2010 and December 2020 in a peer-reviewed journal or as a dissertation/thesis. To identify relevant journal articles, dissertations, and theses across a wide swath of databases and to develop effective search strategies to maximize our search, we consulted our university reference librarian. Databases we systematically searched included Google Site Search, ProQuest Dissertations and Theses, PsycINFO, CINAHL, MEDLINE (PubMed), Academic Search Complete, Social Sciences Citation Index (web of science), Education Research Complete, Criminal Justice Abstract, SocINDEX with full text, ERIC, Psychology and Behavioral Sciences Collection, and Violence and Abuse Abstracts. Keyword searches included the following descriptors entered singularly and in Boolean format with “and” or “or”: kw:(intervention OR education OR training OR prevention OR outcome* OR RCT OR evidence* OR program*) AND kw:(college student* OR undergraduate student* OR young adult*) AND kw:(dating violence OR interpersonal violence OR domestic violence OR intimate partner violence OR healthy relationship OR unhealthy relationship). To exclude studies not conducted in the United States, we included the descriptors “NOT: Europe OR Canada OR China OR South Africa OR Australia OR Turkey OR Brazil” in the advanced search engine because articles from researchers in these countries are the most likely to have studies published in English but not set in the United States.
After retrieving 17,596 initial citations, we screened the titles and abstracts for relevance and conducted full-text review of 217 articles based on our inclusion criteria. After excluding irrelevant and duplicate studies, we reviewed 51 articles and removed additional irrelevant and duplicate articles, including those of interventions that addressed only sexual assault (n = 17). The final study sample consisted of 25 studies. The flowchart in Figure 1 illustrates our screening and study selection process.
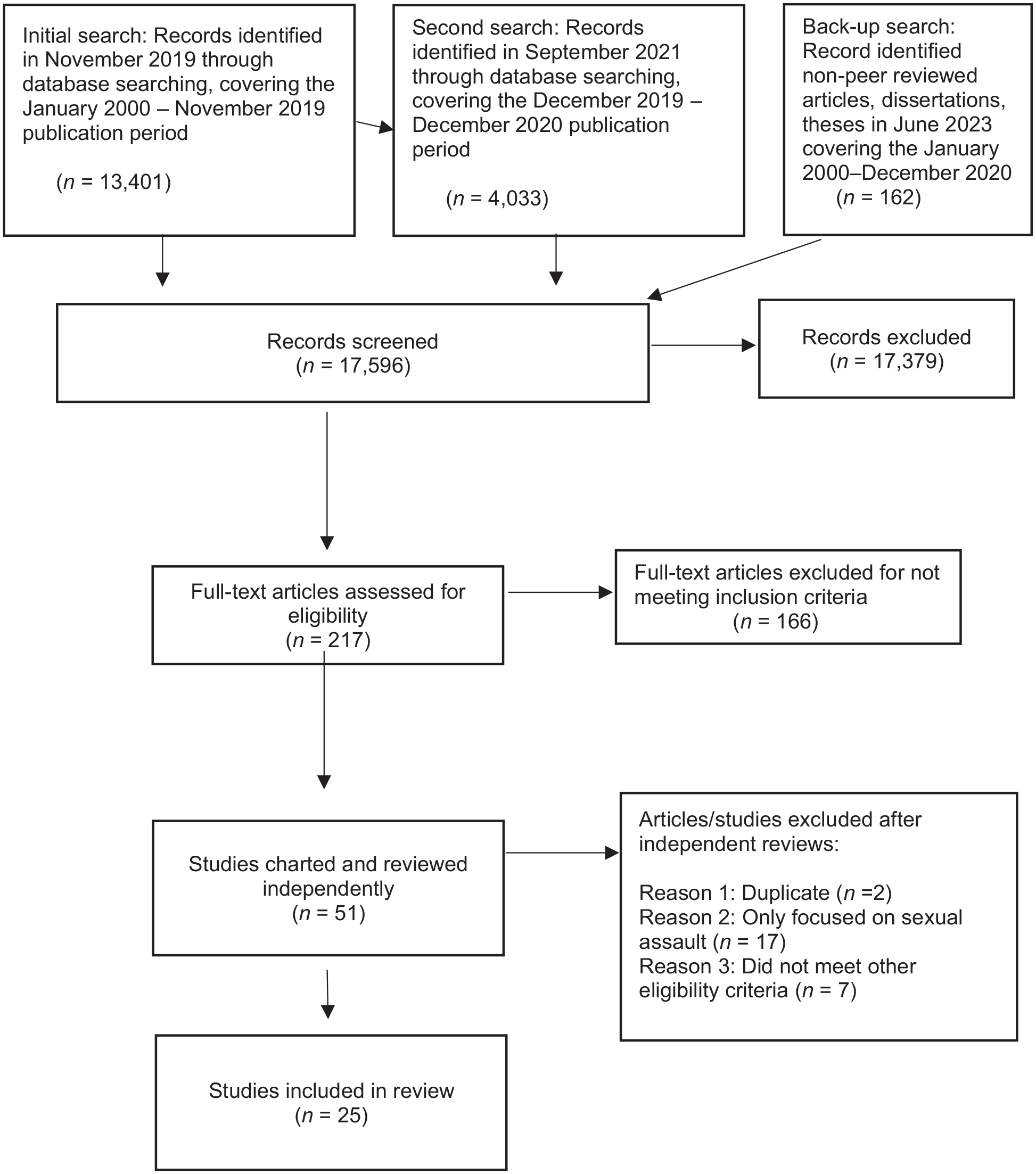
Flowchart for the included studies in the scoping review.
Analytic Frameworks for the Review
Risk and Protective Factor Assessment
For studies included in the present review, an ecological systems perspective was used as an analytic framework to identify the risk and protective factors that were addressed in the IPV preventive interventions or mediators or moderators of the impact of IPV on the well-being of IPV survivors (CDC, 2021; Hardesty & Ogolsky, 2020; Heise 1998; Sheng, 2020). The ecological model identifies five concentric levels of systems (individual system, microsystem, exosystems, macrosystems, and chronosystem) for analysis. Individual systems refer to individual characteristics, including intrapersonal characteristics (e.g., cognition, emotion), sociodemographic characteristics (e.g., gender, age), individual socialization factors, and behavior. Examples of individual risk factors of IPV include cognitive distortion and low self-esteem (cognition), emotional recognition and anger (emotion), violent socialization, adverse childhood experiences (ACEs) such as witnessing and experiencing abuse, and problematic alcohol use (individual socialization factors and behavior). The microsystem refers to an individual (system) and their immediate or direct surroundings (e.g., family, peer group, and campus) with which the individual interacts. Microsystem-level risk factors of IPV include relationship conflict, poor communication, and unequal gender power dynamics. Exosystems include social structures that influence the immediate settings in which an individual develops. Examples of exosystem-level risk factors of IPV include unemployment among men, poverty in a community, alcohol abuse in a community, social isolation, and peer group behaviors and attitudes regarding rape. Macrosystems include cultural values and beliefs that influence individual, micro, and exosystem levels and thereby shape an individual’s development of knowledge, customs, or values. Examples of IPV risk factors at the macrosystem level include patriarchy, gender norms (e.g., masculinity), gender inequality, cultural norms that support aggression, and IPV or sexual assault policy. Chronosystems capture the life course impact of time on individual development. Examples of IPV risk factors at the chronosystem level include risk factors at a young age (e.g., poor self-esteem, ACEs, IPV victimization) predicting or explaining IPV (re-)victimization or negative consequences of IPV in later life (CDC, 2021; Heise, 1998; Sheng, 2020).
Target Outcome Assessment
To understand the target outcomes of college-based IPV prevention programs, this study assessed three levels of evaluation outcomes drawn from Kirkpatrick’s levels of evaluation model (1996): (a) learning, (b) behavior, and (c) results. Learning outcomes focused on how the program enhanced the knowledge, attitudes, confidence, commitment, and/or skills of participants. Behavior outcomes indicate how participants apply learning from the program in their behavior (e.g., bystander behavior, communication skills, and IPV perpetration or victimization). Result outcomes measure the impact of the program (e.g., improvement in mental health and academic performance; Smidt et al., 2009).
Prevention Type Assessment
This study also categorized the types of preventions (e.g., primary, secondary, and tertiary prevention) by translating National Institutes of Health and CDC definitions of health prevention into definitions of IPV prevention. Primary prevention of IPV implies working with a general or whole population (e.g., all university college students) to prevent IPV from occurring by alleviating the population’s exposure to risk factors or increasing their awareness of IPV. Secondary prevention of IPV means working with individuals at high risk for IPV (e.g., female college students and college freshmen) by detecting IPV and immediately responding to the detected IPV as early as possible to minimize the impact of IPV. Tertiary prevention includes working with IPV survivors to meet their needs in order to slow or stop the progression IPV victimization (CDC, n.d.; Kisling & Das, 2023). Identifying prevention types can help expose any gaps in addressing the needs of specific groups (e.g., college students generally and student IPV survivors).
Results
Intervention Characteristics of the Included Studies
Table 1 shows intervention topic, sample characteristics and setting, prevention type, and intervention design for all included studies.
Characteristics of Included Studies (N = 25).
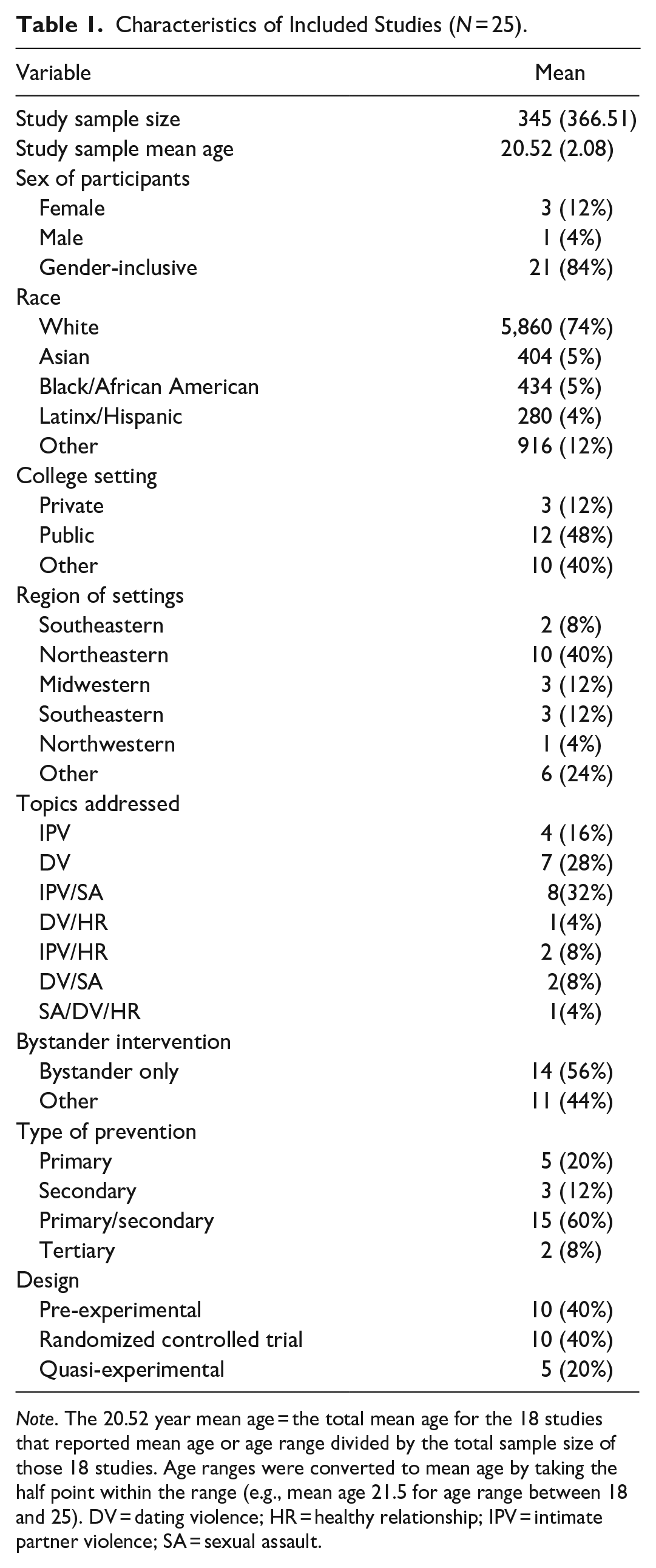
Note. The 20.52 year mean age = the total mean age for the 18 studies that reported mean age or age range divided by the total sample size of those 18 studies. Age ranges were converted to mean age by taking the half point within the range (e.g., mean age 21.5 for age range between 18 and 25). DV = dating violence; HR = healthy relationship; IPV = intimate partner violence; SA = sexual assault.
Intervention Topic
Of the 25 studies, 11 (44%) reported that their intervention focused solely on IPV or DV (e.g., Rothman et al., 2018; Terrazas-Carrillo et al., 2020), including well-being among IPV or DV survivors (Draucker et al., 2019; Nguyen-Feng et al., 2015). Another four studies (16%) focused on IPV/DV and healthy relationships (Hays et al., 2015; Khalifian et al., 2019; Webermann et al., 2020) or sexual assault, DV, and/or healthy relationships (Carlyle et al., 2020). The other 10 reported intervening on both sexual assault and IPV/DV and most of these focused more on sexual assault prevention than on holistic IPV prevention (e.g., Peterson et al., 2018; Santacrose et al., 2020).
Fourteen of the 25 studies (56%) solely implemented a bystander intervention approach, and the intervention topic among 10 of these studies was a combination of sexual assault and IPV or DV (e.g., Amar et al., 2012, Hines & Palm Reed, 2015), while the remaining four studies solely addressed DV (Borsky et al., 2018, Lemay et al., 2019; Rothman et al., 2018) or IPV (McKendrick, 2020). An additional five studies incorporated a bystander intervention approach as part of a broader intervention and attempted to enhance bystander awareness or behavior as well as other intervention goals (Fox & Cook, 2011; Hays et al., 2015; Harsey & Freyd, 2020; Jaffe et al., 2017; Kearney, 2018).
Sample Characteristics and Setting
The mean sample size of the 25 included studies was 345 (SD = 366.51). Among the 19 studies reporting participants’ ages, the mean age was 20.52 years (SD = 2.08). Most programs (n = 21) targeted both female and male students; three targeted only college women (Barraza, 2018; Draucker et al., 2019; Moynihan et al., 2010); and one targeted only college men (Kearney, 2018). Data were collected at public (48%), private (12%), and unspecified (40%) schools. The schools were in the Northeast (40%), Midwest (12%), Southwest (12%), Northwest (4%), and elsewhere in the United States (24%).
Intervention Design and Prevention Type
We categorized each study as having one of three evaluation study designs: a randomized controlled trial (40%), quasi-experimental (20%), or pre-experimental (40%). Five of the 25 studies (20%) focused exclusively on primary prevention and attempted to promote healthy relational and/or emotional skills among individual college students (Hays et al., 2015; Jaffe et al., 2017; Khalifian et al., 2019; Terrazas-Carrillo et al., 2020; Webermann et al., 2020). Interventions with both primary and secondary prevention purposes appeared in 15 studies (60%; e.g., Amar et al., 2012; Borsky et al., 2018). These interventions aimed to improve peer bystanders’ attitudes, beliefs, intent to help, efficacy, and/or behaviors regarding IPV prevention and to enhance their ability to identify IPV and sexual assault and respond appropriately to peers at risk. Three studies (12%) had only secondary preventive interventions (Barraza, 2018; Edwards & Ullman, 2018; Edwards et al., 2020). Barraza (2018) studied a program educating service providers at the campus health center in order to improve their ability to screen for IPV based on female students’ reports; all of the other interventions (96%) were implemented with students. Two interventions (8%) sought to promote positive social reactions to disclosures of sexual assault or IPV among peers (Edwards & Ullman, 2018; Edwards et al., 2020). Another two (8%) included tertiary preventive interventions designed to prevent IPV revictimization or the impact of IPV in mental health (Draucker et al., 2019; Nguyen-Feng et al., 2015).
Targeted Risk and Protective Factors and Their Ecological Levels
Table 2, specifically in columns 2 through 4, shows which studies identified risk/protective factors of IPV (or DV), IPV and sexual assault, and/or healthy relationships; what risk/protective factors were targeted in the intervention; and which ecological systems (individual system, microsystem, exosystem, macrosystem, chronosystem) were addressed in the IPV preventive intervention, given our analytic framework of ecological systems perspective (CDC, 2021; Heise 1998; Sheng, 2020).
Risk Factor, Theoretical Underpinnings, Targeted Outcomes, Skill-building Components, and Delivery (N = 25).
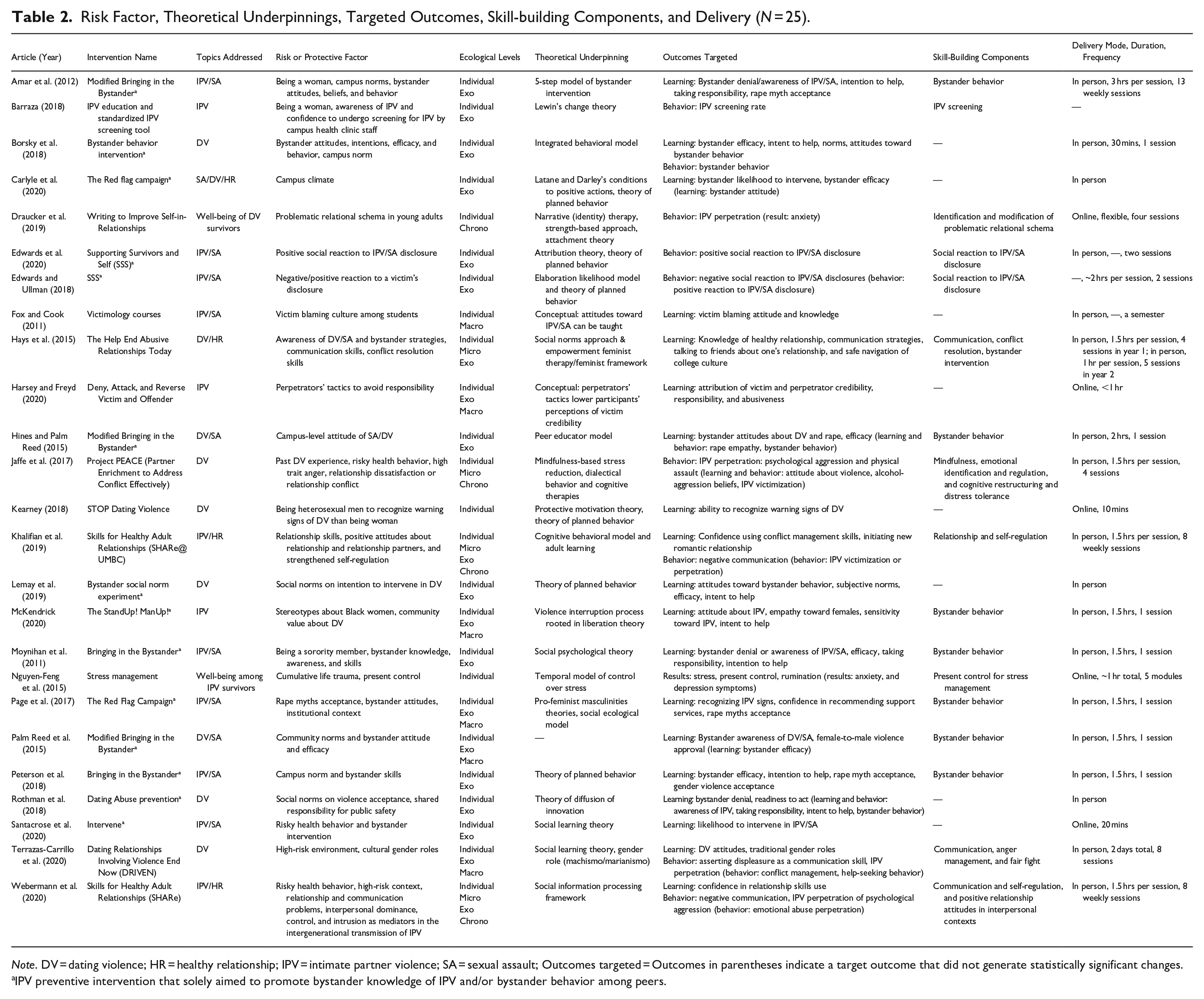
Note. DV = dating violence; HR = healthy relationship; IPV = intimate partner violence; SA = sexual assault; Outcomes targeted = Outcomes in parentheses indicate a target outcome that did not generate statistically significant changes.
IPV preventive intervention that solely aimed to promote bystander knowledge of IPV and/or bystander behavior among peers.
All studies included in our review identified and/or described an attempt to intervene in at least one individual risk or protective factor. Two of the 25 studies (8%) focused only on individual risk factors (Kearney, 2018; Nguyen-Feng et al., 2015). The remaining 23 evaluated IPV prevention programs that implemented multilevel preventive strategies (i.e., strategies to address risk factors of IPV or negative consequences of IPV at multiple system levels; Casey & Lindhorst, 2009). For example, bystander interventions were implemented in order to foster a greater awareness of IPV and cultivate a safe environment by changing campus norms regarding IPV by addressing two-level risk factors at individual and exosystems. However, outcomes measured were individual knowledge, attitudes, and/or behavior, and it was often unclear how the intervention addressed campus norms or culture of IPV. Other studies utilized more comprehensive applications of multilevel preventive strategies. For example, one multilevel prevention program (Hays et al., 2015) that sought to address individual knowledge and awareness of DV and sexual assault as well as bystander strategies also addressed positive communication and conflict resolution skills.
Individual-System-Level Factors
All 25 studies identified at least one risk or protective factor at the individual system level, and 19 (76%) identified knowledge of IPV/sexual assault and intent to intervene, efficacy to intervene, and bystander behavior as individual-system-level risk or protective factors among undergraduate college students (e.g., Borsky et al., 2018; Harsey & Freyd, 2020; Hays et al., 2015; Kearney, 2018). Another study (4%) identified campus health clinic staff’s awareness of IPV and confidence to undergo screening for IPV (Barraza, 2018). The other five studies (20%) identified and/or intervened in other individual risk factors such as emotional and cognitive recognition or regulations (Draucker et al., 2019; Jaffe et al., 2017; Nguyen-Feng et al., 2015; Webermann et al., 2020), previous trauma such as childhood trauma or past DV experience (Jaffe et al., 2017; Nguyen-Feng et al., 2015), and risky behaviors such as problematic alcohol use or substance use (Jaffe et al., 2017; Webermann et al., 2020). A positive attitude based on having intimate relationships was identified as a protective factor at the individual level in one study (Khalifian et al., 2019).
Microsystem- and Exosystem-Level Factors
In four studies (16%), microsystem-level risk or protective factors such as social awareness or interpersonal relationship skills (e.g., empathy), conflict resolution, healthy relationships, and/or communication skills were targeted (Hays et al., 2015; Jaffe et al., 2017; Khalifian et al., 2019; Webermann et al., 2020). Twenty studies (80%) referenced at least one exosystem-level risk or protective factor such as campus norms that support IPV or campus culture against IPV, which was generally measured according to peer attitudes and response/reaction to IPV survivors (e.g., Amar et al., 2012; Peterson et al., 2018; Rothman et al., 2018). Two of the IPV prevention programs that addressed exosystem-level risk factors identified positive social reaction to IPV survivors’ disclosure as a protective factor that mitigated negative IPV health outcomes (Edwards & Ullman, 2018; Edwards et al., 2020).
Macrosystem- and Chronosystem-Level Factors
Six IPV prevention programs (24%) targeted macrolevel risk or protective factors of IPV that included survivor-blaming culture, stereotypes about Black women and community norms on DV, violence-supportive culture, and cultural gender norms (e.g., Page et al., 2017; Palm Reed et al., 2015). Four studies (16%; e.g., Draucker et al., 2019; Jaffe et al., 2017; Khalifian et al., 2019) addressed chronosystem-level risk or protective factors (e.g., intergenerational transmission of trauma, and past trauma in relationships) in prevention programs designed to influence involvement in IPV over the life course or to mitigate its impact on students’ well-being.
Theoretical Underpinnings
All but 3 of the 25 studies (88%) utilized a clear theoretical underpinning to guide their interventions and hypothesize the effect of their interventions on their study outcomes (see Table 2). Two studies (8%) utilized a conceptual framework drawing on existing literature (Fox & Cook, 2011; Harsey & Freyd, 2020) and one (4%) did not explicitly identify their theoretical approach (Palm Reed et al., 2015), although we were able to identify their approach based on previous literature (Moynihan et al., 2010). Social learning theories were the dominant theoretical framework across the studies among IPV interventions that addressed various systems levels of IPV risk factors.
Most of the included studies addressed two-level risk factors (e.g., individual and exosystem levels, individual and microsystem levels). Studies of interventions that were designed to address individual and exosystem levels of IPV risk factors facilitated changes in campus norms against IPV/sexual assault and ultimately among peer bystanders. These utilized (a) social psychology theory and social learning theories that promote learning and prosocial attitudes toward IPV/sexual assault among peer bystanders (Amar et al., 2012; Moynihan et al., 2010; Santacrose et al., 2020), (b) health behavior promotion theories such as the theory of planned behavior (Lemay et al., 2019; Peterson et al., 2018) and the integrated behavioral model (Borsky et al., 2018), or (c) a combination of social learning theory and health behavior promotion theory (Carlyle et al., 2020). By applying social psychology theory, which is a social learning theory, Moynihan et al. (2011) hypothesized that prosocial behavior toward an IPV survivor as a peer bystander (a third party) can be taught through a bystander skill building approach and attempted to increase peer bystanders’ intention to help a peer survivor. Using a health behavior promotion approach, Rothman et al. (2018) applied a theory of diffusion of innovation that explains how knowledge diffuses over peers in a certain system so that they adopt the knowledge into an initial action. Their intervention aimed to foster awareness of IPV and actual bystander behavior among students on one campus.
To address individual and microsystem levels of IPV risk factors, studies also employed theoretical frameworks centering on social learning theory. However, they also applied a cognitive behavioral model and involved a skill-building approach or skill-building components to promote students’ social emotional skills, such as emotional recognition and regulation (Khalifian et al., 2019; Jaffe et al., 2017; Webermann et al., 2020) or social awareness or relationship skills such as empathy, conflict resolution, communication, and/or healthy relationships (Hays et al., 2015; Khalifian et al., 2017; Webermann et al., 2020). For example, Khalifian et al. (2019) utilized both social learning theory and a cognitive behavioral model in order to facilitate confidence using conflict management skills in intimate relationships and skills for initiating new romantic relationships and communication.
At the macrosystem level, IPV prevention programs was designed to promote changes in social norms, values, and culture, and these programs also often used social learning theories to inform interventions to reduce survivor-blaming culture (Fox & Cook, 2011), to make it harder for perpetrators to lower survivors’ credibility (Harsey & Freyd, 2020), and, in an intervention focusing on Hispanic students, to address the impact of traditional gender norms such as machismo and marianismo (Terrazas-Carrillo et al., 2020). Two programs (8%) used critical theories (i.e., empowerment theory and feminist theory). Among these, McKendrick (2020) applied liberation theory, which is based on the understanding that social institutional oppression perpetuates violence and the related issues of inequality and poverty in their intervention at a historically Black college or university (HBCU). The aim was to challenge stereotypes about Black women survivors of IPV and cultural norms that tolerate DV against Black women. Page et al. (2017) applied feminist theory, which implicates masculinity in shaping a culture that supports violence and sexual assault against women and emphasizes perpetrators as the target of intervention, not the survivors.
At the chronosystem level, studies employed clinical theories, including cognitive, behavioral, attachment, and narrative therapeutic theories as well as a mindfulness approach. These approaches attempted to lessen the impact of ACEs and related trauma on student survivors’ well-being. For example, cognitive behavioral theories were applied to lessen intergenerational transmission of IPV (Webermann et al., 2020) and buffer the impact of past DV exposure on IPV revictimization (Jaffe et al., 2017). Social learning theory was also applied in tandem with cognitive behavioral models to prevent IPV revictimization among a general student sample by fostering positive attitudes about relationships and romantic partners (Khalifian et al., 2019).
Types of Outcomes Measured
Outcomes mostly aligned with the risk factors targeted by each study and their theoretical/conceptual underpinnings. The measured outcomes were related to learning only in 13 studies (52%), behavior only in three studies (12%), results only in two studies (8%), and both learning and behavior in seven studies (28%; e.g., Carlyle et al., 2020; Terrazas-Carrillo et al., 2020; see Table 2). The learning outcomes assessed in 20 studies (80%) included knowledge of and attitudes toward IPV, sexual assault, and/or bystander efficacy and intent to intervene among peers (e.g., Amar et al., 2012; Fox & Cook, 2011; Hines & Palm Reed, 2015). The behavioral outcomes assessed in 11 studies (44%) was (a) bystander behavior (Borsky et al., 2018; Hines & Palm Reed, 2015; Rothman et al., 2018), (b) IPV screening behavior (Barraza, 2018), (c) reaction to IPV disclosure (Edwards & Ullman, 2018; Edwards et al., 2020), (d) social emotional skill use (Khalifian et al., 2019; McKendrick, 2020; Terrazas-Carrillo et al., 2020; Webermann et al., 2020), and (e) IPV victimization or perpetration (Draucker et al., 2019; Jaffe et al., 2017; Khalifian et al., 2019; Terrazas-Carrillo et al., 2020; Webermann et al., 2020). Two studies (8%) focused on result outcomes measured IPV survivors’ well-being (e.g., stress level, anxiety, depressive symptoms; Draucker et al., 2019; Nguyen-Feng et al., 2015).
Skill-Building Component
Seventeen studies (68%) examined interventions with a skill-building component designed to prevent IPV, sometimes in tandem with sexual assault (see Table 2). Ten of these examined interventions designed to teach bystander skills (e.g., bystander behavior, social reaction to IPV disclosure) through group discussion of bystander skills or role play exercises (e.g., Hays et al., 2015; McKendrick, 2020). Program facilitators were peer(s) (e.g., Page et al., 2017; Peterson et al., 2018), a professional (e.g., Amar et al., 2012; Hays et al., 2015; Palm Reed et al., 2015), or a combination of peers and professionals (e.g., Hines & Palm Reed, 2015; McKendrick, 2020), or were unspecified (e.g., Moynihan et al., 2010). Bystander skill-building tended to be briefly addressed along with other learning components such as psychoeducation lectures and group discussions (e.g., Borsky et al., 2018; Hines & Palm Reed, 2015).
The remaining seven studies taught a variety of skills. Specifically, two interventions (Edwards & Ullman, 2018; Edwards et al., 2020) encouraged participants to provide supportive reactions to a peer survivor’s disclosure of sexual assault or IPV through experiential role play exercises and scenarios led by peer facilitator(s). Barraza (2018) presented on how to administer an IPV screening measure (HITS) to clinical staff members in a college health center. Jaffe et al. (2017) incorporated mindfulness skill-building components administered by trained facilitators in four 90-minute sessions that addressed emotional identification and regulation, distress tolerance, cognitive restructuring, and effective communication skills. A trained and supervised master’s student in clinical psychology facilitated a series of in-session activities (e.g., breathing exercise, discussions, and games) and homework (e.g., mindfulness log, emotion identification log, review rules of fair fighting with partner, and cognitive attribution log) to build relevant skills. Three studies (12%) examined interventions that promoted healthy interpersonal skills and other positive self and social awareness and management skills (Khalifian et al., 2019; Terrazas-Carrillo et al., 2020; Webermann et al., 2020). Khalifian et al. (2019) developed a program called Skills for Healthy Adult Relationships (SHARe) and Webermann et al. (2020) updated it. Khalifian et al. (2019) developed and piloted SHARe to teach communication skills (e.g., different strategies for approaching problem solving with peers and romantic partners) and to help increase participants’ confidence in utilizing conflict management strategies (e.g., self-regulation) and initiating a romantic relationship. Webermann et al. (2020) utilized skill-building role plays and practice assignments across their eight sessions, facilitated by one or two clinically trained professionals.
One of the seven studies that taught a variety of skills addressed the cultural relevance to students of color of an IPV prevention intervention, the Dating Relationships Involving Violence End Now (DRIVEN) program, which was tailored for this study and to Latino students (Terrazas-Carrillo et al., 2020). This intensive eight-session program utilizes experiential exercise tools (e.g., role plays, mock presentations of topics) and materials on healthy relationships, gender stereotypes in Latino culture, DV, relationship equality, effective communication, managing anger, and fighting fair.
Overall, interventions with mindfulness or relationship skill-building components that also embraced self-awareness and self-regulation components tended to incorporate more extensive activities and modules and facilitators with specific (educational) training and/or supervision. By contrast, interventions with bystander behavior skills training and those that promoted supportive peer reactions to IPV/sexual assault disclosure exhibited the most flexibility regarding peer and/or professional facilitators.
Delivery Mode, Duration, and Frequency
We observed some patterns in delivery mode, duration, and frequency (see Table 2), but many studies did not report key information regarding the intervention’s delivery, making it difficult to critically assess patterns across all of the studies. Nonetheless, 20 studies (80%) examined interventions that were administered in person. For example, interventions with extensive skills training components were delivered in person (Jaffe et al., 2017; Khalifian et al., 2019; Terrazas-Carrillo et al., 2020; Webermann et al., 2020). In contrast, three bystander interventions (Harsey & Freyd, 2020; Kearney, 2018; Santacrose et al., 2020) and two tertiary prevention programs that addressed the impact of IPV on student survivors’ well-being were delivered online. Among these, one built stress management skills (Nguyen Feng et al., 2015) and the other was designed to revise students’ relationship schema (Draucker et al, 2019). While both tertiary prevention programs consisted of multiple modules, the administration of their online trainings was different. The stress management skill-building program took about an hour (Nguyen Feng et al., 2015), while the relationship schema modification program was flexibly administered by each participant (Draucker et al., 2019).
Extensive skills training prevention programs (Jaffe et al., 2017; Khalifian et al., 2019; Terrazas-Carrillo et al., 2020; Webermann et al., 2020) tended to be longer in duration and to have sessions that occurred more frequently than bystander behavior skill training interventions. In general, in-person interventions took participants more time to complete than online interventions.
Discussion
This scoping review identified and assessed the characteristics of college-based IPV preventive interventions across 25 studies, including target risk and protective factors, theoretical underpinnings, target outcomes measured, skill-building components, and delivery methods. Informed by an ecological systems perspective, this study found that most of the IPV prevention programs reviewed were theoretically driven, multilevel health preventive interventions (Casey & Lindhorst, 2009). Consistent with findings of previous systematic reviews on college-based sexual assault prevention programs (e.g., Storer et al., 2016), our review showed that a substantial number of IPV prevention programs addressed individual and exosystem level risk factors (e.g., campus norms related to IPV and sexual assault) and were guided by social learning and health behavior promotion theories. We found that these IPV prevention programs utilized bystander intervention approaches that aimed to educate peer behaviors for primary and secondary IPV prevention purposes. These bystander interventions targeted participants’ individual learning and behavior outcomes. Specific outcomes of the interventions included raising bystander awareness of IPV (Rothman et al., 2018), increasing intention to help as bystanders (Santacrose et al., 2020) and improving bystander intervention behavior (Borsky et al., 2018) as part of a larger goal to transform campus norms regarding IPV.
Fewer programs offered interventions that provided relationship education (e.g., Webermann et al., 2020) and/or social emotional learning education (e.g., Jaffe et al., 2017). These interventions aimed to address risk factors at a more diverse systems level (e.g., individual, micro, and/or chrono) and to change outcomes such as the use of social emotional skills (e.g., emotional regulation and healthy relationship skills) and IPV victimization or perpetration. IPV prevention programs using relationship and/or social emotional learning approaches tended to utilize clinical theoretical frameworks such as cognitive behavioral theory, the mindfulness-based stress reduction model, and attachment theory, and they often incorporate clinical theories along with social learning theories. Most college-based IPV prevention programs targeted changes in IPV awareness and behavior among general student populations rather than long-term impacts on mental well-being. Thus, social learning theories seemed to be widely accepted as appropriate for addressing IPV risk factors at multiple systems levels. Conversely, feminist perspectives on IPV seemed to be lacking except in a study addressing macrosystem level risk factors, such as stereotypes about IPV survivors (McKendrick, 2020).
Overall, the studies in the corpus suggest that college-based IPV prevention programs are not being intentional enough about aligning their theoretical underpinnings with the type of violence (e.g., gender-based violence or situational couple violence) they aimed to prevent. For instance, college-based IPV prevention programs (n = 19) that were designed to address campus norms that were supportive of IPV or lack of awareness of IPV rarely applied a feminist perspective. Indeed, only two studies examined exceptions (Hays et al., 2015; Page et al., 2017). Without using feminist or other critical perspectives, programs may not adequately address elements such as patriarchal gender norms or masculinity associated with gender-based violence. The absence of such theoretical underpinnings of college-based IPV prevention programs may indicate that (a) interventions are not designed consistently with their assumptions about the types of IPV (e.g., gender based violence, situational couple violence, or both) or (b) assumptions about IPV types are not clearly positioned. While mutual violence is referenced in college IPV literature (Kaukinen et al., 2015; Varlioglu et al., 2022), most college-based IPV prevention programs in the studies reviewed here did not aim to address risk factors for situational couple violence. This finding underlines a gap in existing interventions, and program evaluations are needed to address situational couple violence in college campuses. The same risk factors may explain both gender-based violence and situational couple violence or risk factors of either violence type may moderate/mediate another type among college students. Future research should assess whether this is the case and if college-based IPV prevention programs need to modify their theoretical frameworks and/or their target risk/protective factors.
We observed inconsistencies between some studies’ identified risk factors and measured target outcomes. For example, studies commonly identified IPV risk factors as social and cultural norms related to IPV but measured outcomes at the individual level (e.g., Peterson et al., 2018; Santacrose et al., 2020). In other instances, studies only measured learning outcomes although the interventions included skill-building components (e.g., Hays et al., 2015). Such inconsistencies appeared to reflect the practical and methodological limitations of operationalizing and measuring risk factors as well as participant retention issues. Indeed, some studies acknowledged that the practical difficulties of measuring behavior outcomes drove a focus on measuring learning outcomes (e.g., Kearney, 2018; Lemay et al., 2019). Future research needs to assess long-term behavioral outcomes.
This scoping review highlighted the potential benefits of integrating skill-building components into IPV prevention programs. First, IPV prevention programs that solely implement individual skill-building components (e.g., healthy relationship skills, conflict resolution, use of empathy, and/or communication skills; Draucker et al., 2019; Webermann et al., 2020) or integrating the components into other multilevel IPV prevention approaches (e.g., bystander intervention; Jaffe et al., 2017; Terrazas-Carrillo et al., 2020) appear to lessen IPV incidence among participating college students. Our scoping review also identified pioneering IPV prevention programs that teach college students relationship skills (Khalifian et al., 2019; Webermann et al., 2020). Such individual-oriented healthy relationship skill-building approaches may be more feasible than an at-risk couple-oriented IPV primary prevention strategy, given potential challenges in recruiting college student couples for a similar relationship education program. The authors of this review found in a study that college students themselves perceived that promoting students’ acquisition of healthy relationship skills could serve as a protective factor against IPV in relationships ([Author blinded], under review). To be sure, this type of intervention may be more relevant to preventing situational couple violence than coercive controlling violence.
Our review identified a service gap in current IPV prevention programming: namely, that these programs rarely addressed ACEs or intergenerational transmission of trauma as risk factors of IPV. Numerous studies show that cumulative trauma increases the risk of IPV perpetration and victimization (e.g., Zhu et al., 2023) and mental health service needs among college students (e.g., Seon et al., 2022). Given findings that self-control over emotions can be a protective factor for IPV and a mediating factor of intergenerational transmission of IPV (Nguyen-Feng et al., 2015; Webermann et al., 2020), future IPV prevention programs should promote college students’ control over their emotions and thoughts to mitigate stress or their likelihood of IPV perpetration. Examples of trauma-informed practice include elements of recognizing the existence of trauma and its signs among college students, addressing their social emotional needs, and preventing revictimization of trauma as part of health prevention programs in higher education (Conley et al., 2015; Joss et al., 2019; Rahimi & Liston, 2023) and their target outcomes centered on fostering positive coping skills such as relaxation, mindfulness, and social skills. Incorporating trauma-informed components into IPV prevention programs and evaluating their effect would be a foundational step to preventing and/or addressing IPV.
Our findings also foreground disproportional representation of some college student groups in and across settings. Some of these findings corroborate Barlow and Cromer’s (2006) observation that undergraduate research pools tend to overrepresent female students, freshmen, and psychology majors. Further, very few of the reviewed studies examined behavioral changes among students at minority-serving institutions. HBCUs and Hispanic-serving institutions comprise, respectively, 3% and 16% of the institutions of higher education in the United States, yet only two intervention studies in the current review were implemented in such settings. Our findings thus call for intentional efforts in future studies to examine IPV programming in minority-serving institutions in order to tailor effective programming for diverse student populations.
This review’s promising findings should be interpreted in light of several limitations. Search terms or keywords used to identify articles for this review might have excluded relevant literature (e.g., for evidence-based relationship education for young adults, see Simpson et al., 2018), despite our thorough examination of previous systematic reviews on IPV and/or sexual assault and our consultation with a reference librarian. Also, relevant publications published after December 2020 were not included in this review; thus, future analyses should include the latest findings. This review categorized interventions as focusing on IPV, sexual assault, and/or healthy relationships based on how each included article defined their topic area. Yet conceptualization and/or operationalization can still vary across studies. For instance, some studies define IPV as physical abuse only, while others include both physical and emotional abuse in their definitions, which potentially limits our ability to compare findings across studies. Our findings also may not be applicable to young adults outside higher education settings, although IPV may be even more common among young adults not in college.
Conclusion
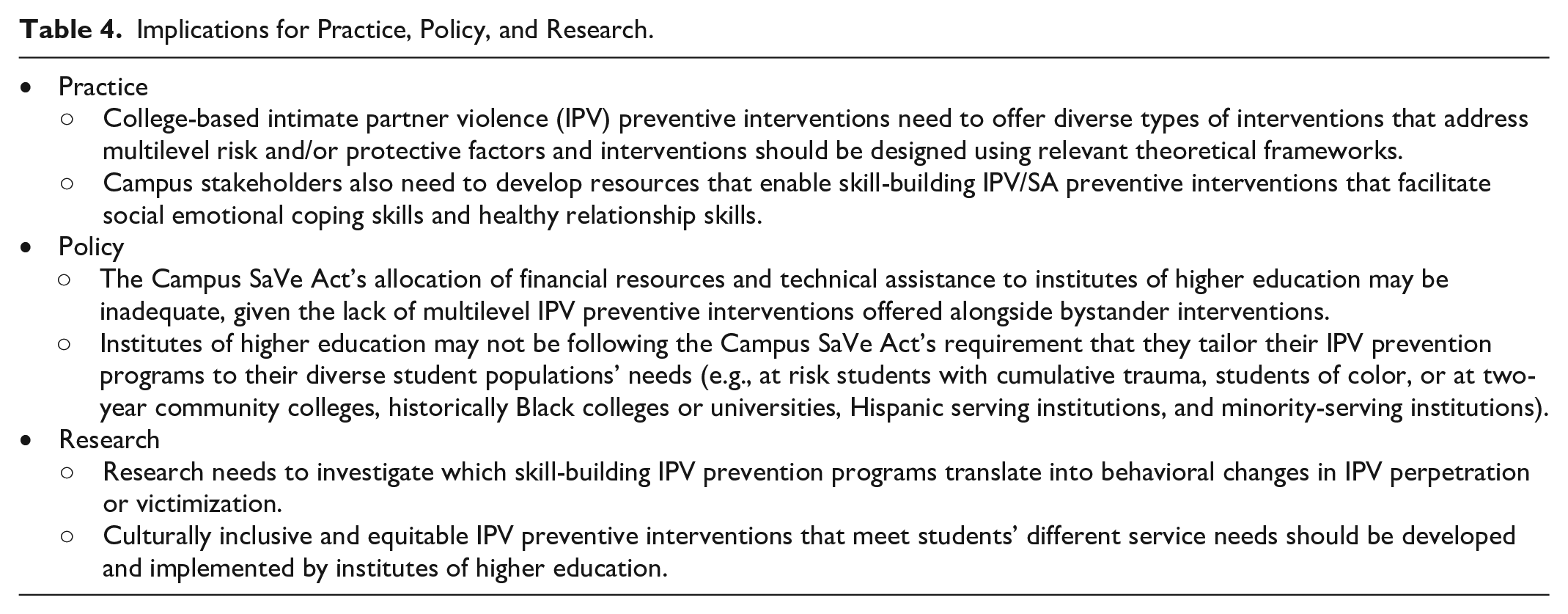
Key points of the research review and implications for practice, policy, and research are available in Table 3 and Table 4, respectively. Our review highlights that various college-based IPV preventive interventions exist and address multilevel IPV risk factors at individual system, microsystem, exosystem, macrosystem, and chronosystem levels. Although bystander interventions are useful for raising students’ awareness of IPV and/or sexual assault, skill-building intervention approaches appear to be a means of enhancing college-based IPV prevention programs. Skill-building IPV prevention approaches seem to be a good addition to the current emphasis on building campus norms against IPV in that they address individual- and micro (relationship) system-level protective/risk factors of IPV. From a mental health prevention perspective, campus-based IPV prevention may also benefit from addressing cumulative life course trauma to prevent IPV and other mental health issues among students and from securing funding to support skill-based trainings. Combining preventive interventions that promote healthy relationship skills, social emotional learning, and peer norms against IPV would capitalize on the respective strengths and address the limitations of each approach alone, as well as increasing the capacity of existing IPV interventions to tailor strategies for diverse students’ needs.
Key Points of the Research Review.

Implications for Practice, Policy, and Research.
Footnotes
Acknowledgements
We would like to express our deepest appreciation to professor Jennifer Hardesty for her constructive feedback during the revision process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by New York Community Trust’s Fahs-Beck Fund for Research and Experimentation (Grant number 234430).