
Abstract
Parents are their children’s first teachers and there are long-standing calls for their involvement in child sexual abuse prevention. In this rapid systematic review, we asked the following questions: what rationales are used to justify parental involvement in child-focused child sexual abuse (CSA) prevention programs? what approaches are used for parental engagement in child-focused CSA prevention programs? and what are the facilitators and barriers to parental involvement in child-focused CSA prevention programs? We searched CINAHL, Cochrane, ERIC, Medline, PsycInfo, Scopus, and SocINDEX in May 2021. A total of 57 papers met our inclusion criteria, comprised of 50 empirical studies, and 7 program descriptions. Rationales for parental involvement included monitoring and shaping parental attitudes toward CSA program delivery in schools; reinforcing children’s learning at home; promoting parent–child communication about CSA prevention; building parent capacity to respond to child disclosures; and supporting program delivery for preschoolers. Types of parental involvement included the following: communication, learning at home, volunteering, decision-making, and collaboration with the community. Barriers to parent involvement included ineffective program engagement modalities, and parental fears and misconceptions.
Keywords
Introduction
Child sexual abuse (CSA) is a serious ongoing concern for communities globally affecting approximately 20% to 25% of women and 8% to 10% of men worldwide (Barth et al., 2013; Pereda et al., 2009). High prevalence is found in recent research. For example, a synthesis of CSA prevalence in five Nordic countries showed wide rates of 3% to 23% for boys and 11% to 36% for girls (Kloppen et al., 2016). From Japan, a synthesis of eight studies found rates of 1% to 64% for girls and 0% to 44% for boys (Tanaka et al., 2017), and India across 16 studies found rates of 4% to 41% for girls and 4% to 57% of boys (Choudhry et al., 2018). Data from perhaps the most recent prevalence study, conducted in Australia, found rates of 37.3% for women, 18.8% for men, and 52% for people identifying as gender diverse (Higgins et al., 2024; Mathews et al., 2023).
Protecting children from CSA is complex and multifaceted, with solutions typically requiring several interconnected and overlapping approaches. These include adopting a public health approach with coordinated primary, secondary, and tertiary prevention efforts (e.g., Letourneau, Eaton, et al., 2014; Higgins & Russell 2024; Russell & Higgins, 2024), implementing evidence-informed child-safe standards detailing principles and practices for preventing and responding to child sexual abuse and exploitation (e.g., Australian Human Rights Commission, 2018; Keeping Children Safe, 2014; NSPCC, 2017; Saul & Audage, 2007), and utilizing situational crime prevention in which opportunities for harm to children, particularly in institutions, are reduced via deterrence methods (e.g., Firmin, 2020; Higgins & Morley, 2018; Smallbone et al., 2013). These approaches reinforce the need for prevention efforts to recruit, engage, and mobilize multiple members of children’s social ecology. In this review, we address a key group: children’s parents/caregivers.
Parents and Child Sexual Abuse Prevention
Despite barriers regarding the inclusion of parents (Livingston et al., 2020, there is broad consensus on the important role of families and parents/caregivers (henceforth, “parents”) in CSA prevention (Mendelson & Letourneau, 2015; Rudolph & Zimmer-Gembeck, 2018; Trew et al., 2021; Wurtele & Kenny, 2010, 2012; Xie et al., 2016). Parents are typically recruited into CSA prevention via two programmatic routes: (i) via programs in which parents are specifically targeted, also known as parent-led sexual abuse prevention (Rudolph & Zimmer-Gembeck, 2018) or parent-focused prevention (Mendelson & Letourneau, 2015) and (ii) via programs in which children are targeted and parents are engaged as adjuncts, also known as child-focused prevention (Sanderson, 2004).
Regarding the first category―parent-led or parent-focused CSA prevention―in recent research, randomized controlled trials and other rigorous evaluation methodologies have been utilized to investigate the efficacy of parent-focused CSA interventions. For example, in a cluster randomized controlled trial, Guastaferro, Felt, et al. (2020) evaluated the effects of Smart Parents—Safe and Healthy Kids, a single session (~60 minutes) behaviorally based CSA prevention module that was added to an established parenting intervention known as Parents as Teachers. The module, covering topics such as child sexual development, parent–child communication, safety strategies, and parental monitoring techniques, used role-play and other structured experiences designed to increase awareness and shape behaviors. The intervention was successful in increasing parents’ knowledge of and readiness to apply behaviorally specific protective strategies. In another randomized controlled trial, Nickerson et al. (2018) evaluated the effects of a series of four short videos from the Second Step® Child Protection Unit. The videos acknowledge parents’ discomfort, depict parents initiating discussions with their children, and model ways of responding in the event of child disclosures. The intervention was successful in increasing parents’ knowledge, motivation, and frequency of communication with their children about personal safety and CSA prevention.
The theory of change for these parent-led or parent-focused interventions is based on the centrality of protective parenting in CSA prevention embracing the idea that through active and involved parenting enacted via behavioral strategies such as monitoring, supervision, caution around care delegation, checking in with children, and the use of warmth and open communication (Mendelson & Letourneau, 2015; Rudolph et al., 2023b). These interventions are not the subject of this review; however, we will return to this salient point about their theories of change, later in this review.
Regarding the second category―child-focused CSA prevention with parents as adjuncts―the research has a much longer history. By adjuncts, we mean they are added as supplementary rather than essential components. Child-focused CSA prevention interventions are conducted in preschools, schools, and other youth-serving organizations. Interventions are typically delivered by trained facilitators to groups of children (e.g., in classrooms) and comprise a sequence of lessons with content developmentally sequenced for specific age groups (Lu et al., 2023; Walsh et al., 2015). In well-evaluated interventions (i.e., those meeting thresholds for inclusion in high-quality systematic reviews), young children in the early years learn to recognize safe and unsafe situations, name private body parts, begin to understand the concept of body autonomy (i.e., my body belongs to me), and identify adults who can help. As children progress through middle school, they learn about child sexual abuse and grooming, safe and unsafe touching, secret-keeping, that children are not to blame when adults make poor choices, and that offenders may be someone known or unknown. How to seek help and from whom is also a key focus (Walsh et al., 2015). In high school, CSA prevention programs begin to overlap with dating and relationship violence prevention programs or peer victimization prevention programs, and children learn about respectful and healthy relationships, the role of gender norms and bystander behaviors, and making and receiving disclosures (Cohen & Katz, 2021; De La Rue et al., 2017).
The theory of change for these child-focused interventions with parents as adjuncts is that by involving parents through a variety of mechanisms, they may be recruited to support program delivery, reinforce program messages at home, discuss CSA and its prevention with their children, and respond appropriately to disclosures, thereby enhancing prevention effects for children (Babatsikos, 2010; Wurtele & Kenny, 2010).
Previous Reviews
We are aware of a small number of previous narrative reviews on the topic of parents and CSA prevention. Babatsikos (2010) reviewed studies that had collected data on parents’ CSA knowledge, attitudes, and prevention practices. Wurtele and Kenny (2010) reviewed studies in which barriers and facilitators to parents’ participation in CSA prevention programs had been investigated. Hunt and Walsh (2011) reviewed studies of parents’ views about school-based child sexual abuse prevention. These reviews (Babatiskos, 2010; Hunt & Walsh, 2011; Wurtele & Kenny, 2010) differ from our current review in that they reviewed research centered around parent-focused interventions. Our review instead focuses on the inclusion of parents in child-focused interventions or programs.
Most recently, in a rigorous systematic review, Rudolph et al. (2024) synthesized the evidence on parental involvement in CSA prevention programs from 24 studies in which parents or primary caregivers were the primary program targets. It differs from this current review in having a narrower precision-oriented remit, focusing squarely on program outcomes and effectiveness (parental knowledge, attitudes, self-efficacy, and behavioral intentions). This review can serve as a companion piece and extension to Rudolph et al.’s (2023a) review by offering a classification of parental involvement using an existing evidence-based typology to shed light on parent participatory practices likely to result in meaningful outcomes.
Aim and Research Questions
Our review aimed to investigate parent involvement in child-focused CSA prevention programs. In this review, “parents” refers to parental figures, caregivers, and guardians who are responsible for the care of a child or children including but not limited to biological relationships. We defined child-focused CSA prevention programs as interventions presented to groups of children and young people aged under 18 years, in which contents and methods had been tailored for specific age groups and cognition levels.
We will summarize how parents have been involved in child-focused CSA prevention education to provide program developers and facilitators with information that might assist them to more purposefully engage parents in CSA prevention education delivered in preschools, schools, and other child and youth-serving organizations.
Research questions that guided our review were as follows:
What rationales are used to justify parental involvement in child-focused CSA prevention programs?
What approaches are used for parental engagement in child-focused CSA prevention programs?
What are the facilitators and barriers to parental involvement in child-focused CSA prevention programs?
Method
To address the research questions, we conducted a rapid systematic review following the rapid review guidelines of Tricco et al. (2017), and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Preferred Reporting (PRISMA) guidelines (Page et al., 2021). 1 To formulate a narrative synthesis of findings, we used the Synthesis without Meta-Analysis reporting guidelines (Campbell et al., 2020) and Popay et al. (2006).
Search Strategy
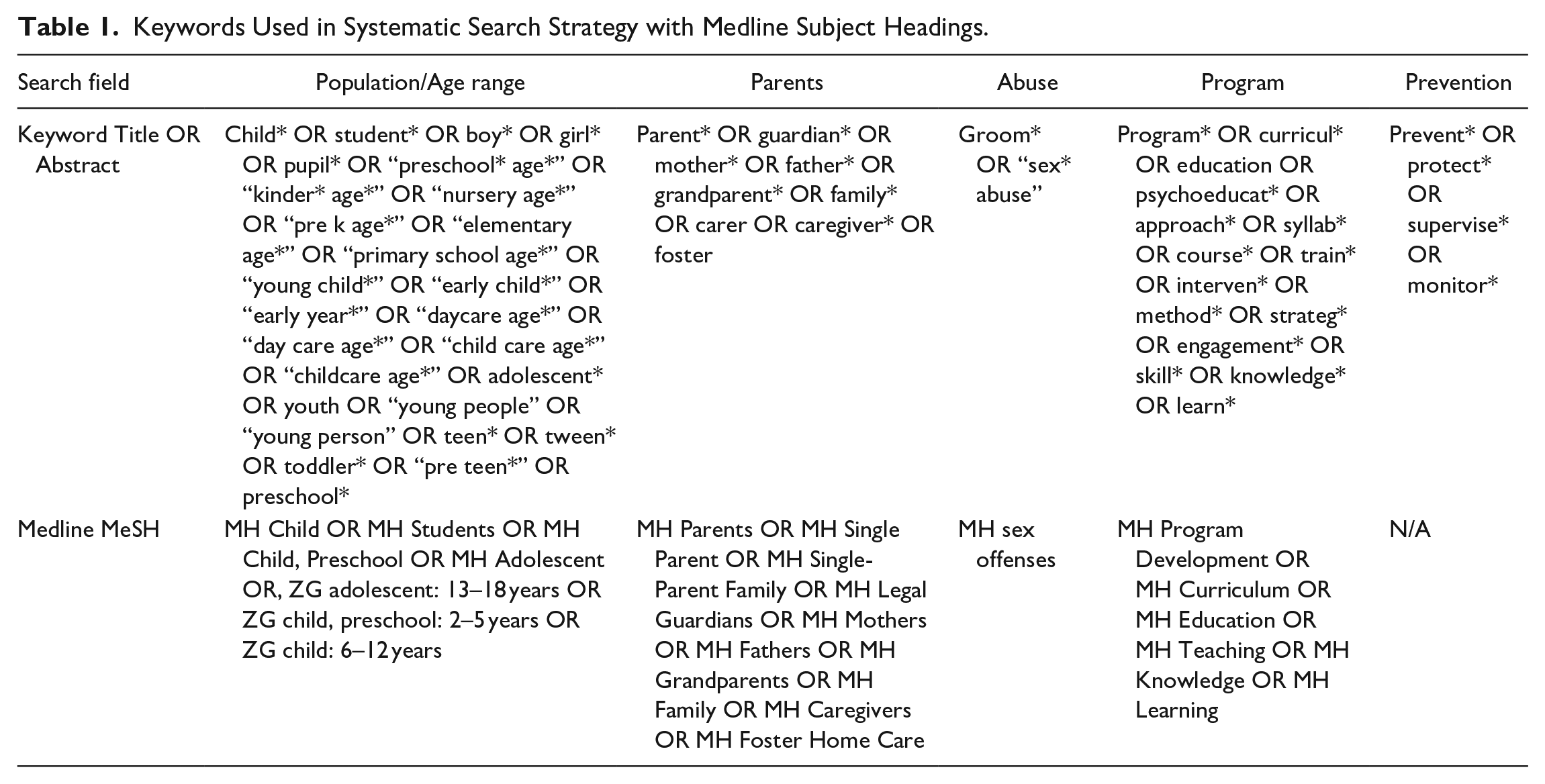
We searched seven databases (CINAHL, Cochrane Library, ERIC [Ebsco], Medline Complete [Ebsco], PsycInfo [Ebsco], Scopus, and SocINDEX) in May 2021 for peer-reviewed papers relating to parent involvement in child-focused CSA prevention programs. We restricted keyword searches to record titles and abstracts and applied relevant subject headings for each database. We did not apply date or language restrictions. The search strategy is shown in Table 1.
Keywords Used in Systematic Search Strategy with Medline Subject Headings.
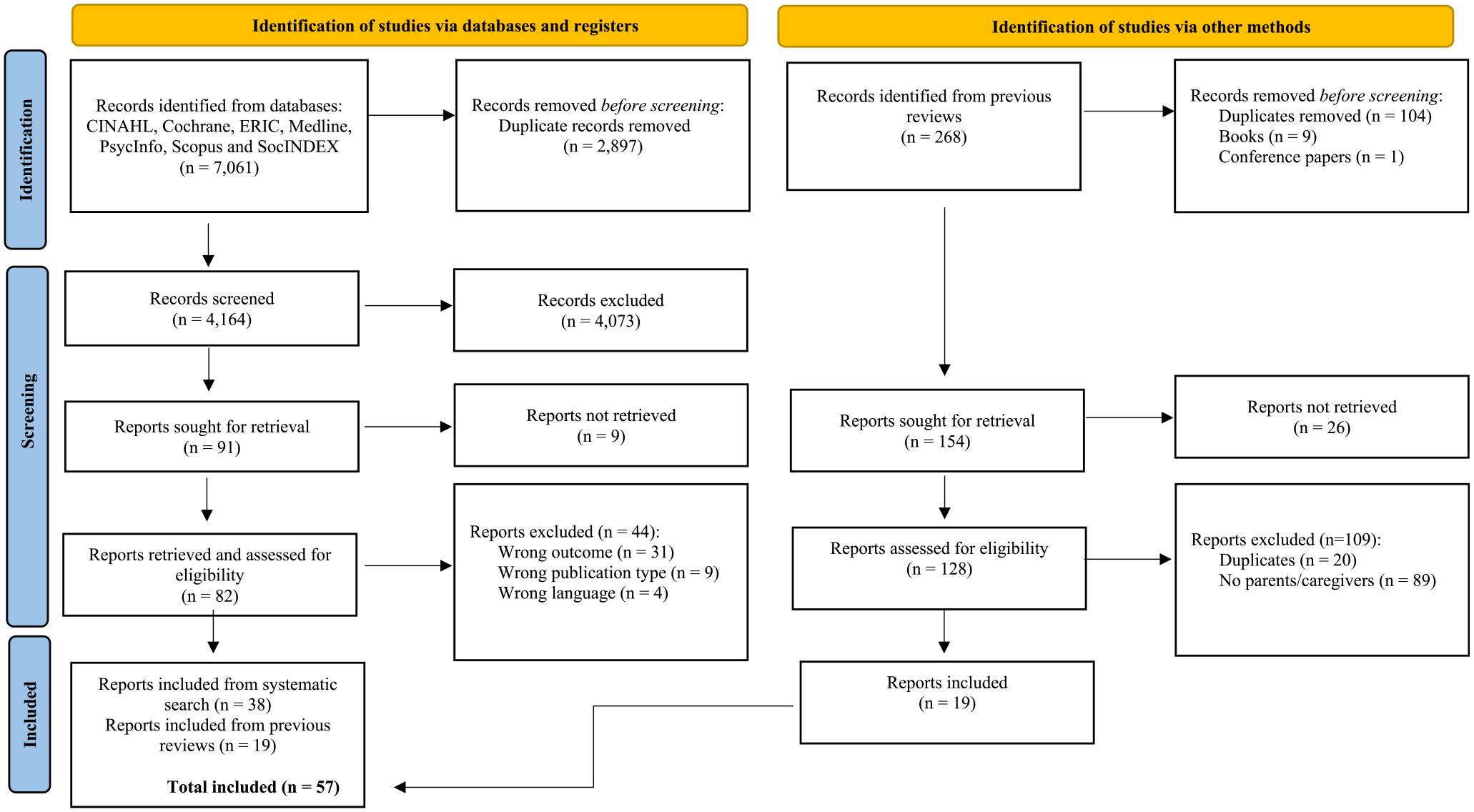
We supplemented this systematic search with additional targeted searches. Having previously conducted a review of effective delivery methods in CSA prevention programs (Trew et al., 2021), we were aware of several reviews on the efficacy of CSA prevention programs (Brassard & Fiorvaanti, 2015; Davis & Gidycz, 2000; Del Campo & Fávero, 2019; Fryda & Hulme, 2015; Kenny et al., 2008; Lynas & Hawkins, 2017; Rispens et al., 1997; Topping & Barron, 2009; Walsh et al., 2015). Together, these reviews included 268 studies. After removing duplicates (n = 104), we retrieved a total of 128 studies. We searched the text of each study (using Ctrl + F) for the following terms: parent, carer, guardian, mother, and father. If any one of these terms were found, we screened the full text of the paper against our review’s inclusion and exclusion criteria. Using this process, we identified 19 further papers (as shown in Figure 1).
PRISMA flowchart.
Eligibility Criteria
After removing duplicates, we used Rayyan (Qatar Computing Research Institute; QCRI) (Ouzzani et al., 2016) to screen records from the systematic search against inclusion and exclusion criteria. Authors 1 and 2 double-blind screened all articles and worked together to resolve conflicts. Unresolved conflicts were referred to Author 5. We included articles if they met the following three criteria:
Focus: A child-focused CSA prevention program or intervention in which children or young people (i.e., aged under 18 years) were the target audience and parents were adjuncts.
Intervention: Primary prevention program (i.e., aiming to prevent CSA before it occurs rather than provide treatment or address effects after CSA has occurred).
Participants: the intervention involved parents in a meaningful way (i.e., more than simply providing consent for their child to take part in a study).
We excluded papers in which the participants in the intervention were not children (i.e., were aged 18 or above) and where data were not disaggregated (i.e., so that those aged under 18 could be clearly distinguished). We excluded papers in which interventions targeted at-risk groups (i.e., secondary prevention initiatives), children and young people engaged in harmful sexual behavior, and programs for victims/survivors (i.e., tertiary prevention initiatives). We excluded papers in which the sole reason for parent involvement was to provide consent for their children’s participation in research.
Screening and Selection
Figure 1 shows the PRISMA flow diagram. Our systematic searches yielded 7,061 records of which 2,897 were duplicates. After screening, 38 papers remained. An additional targeted search strategy identified a further 19 papers. Together, we had a total of 57 papers from which to extract data.
Data Extraction and Analysis
Data were extracted in a standardized format, using a MS Excel spreadsheet. Rationales for parent involvement were thematically coded in an inductive or “data-driven” process (Braun & Clarke, 2019) in which we coded text in each paper according to the way(s) in which authors had represented reasons for parent involvement. Themes were developed from codes. A similar process was used to analyze barriers and facilitators to parent involvement. Types of parental involvement were coded in a deductive or “theory-driven” approach against Epstein’s (2018) framework of six types of involvement, also known as the “school-family-community partnership model.” The most recent version of the typology was described by Epstein et al. (2018, pp. 19–21). It is a well-established model that has been incorporated into the USA’s No Child Left Behind—Public Law 107-110, 2002, SEC. 1118—and is based on decades of empirical research on parent educational engagement initiatives in schools.
Critical Appraisal
We used the Joanna Briggs Institute (JBI, 2020) critical appraisal tools to conduct a methodological quality assessment of the studies included. The JBI tools provide the convenience of a single location in which to source critical appraisal tools. However, the instruments required adaptation to suit a rapid systematic review of the type we were conducting which captured a wide range of included study designs.
In the absence of a JBI critical appraisal tool specifically for randomized controlled trials, these studies were appraised using the quasi-experimental tool. We noted the absence of criteria to assess blinding of outcome assessors, study attrition, and selective reporting. The JBI critical appraisal tool for analytical cross-sectional studies was used for cross-sectional studies. The JBI critical appraisal tool for qualitative studies focused heavily on the philosophical basis for theory–methodology–methods congruence; however many of the included qualitative studies in our sample did not proclaim a theoretical standpoint (e.g., interpretivism, constructivism) as they were rather more agnostic about the nature of reality and knowledge in data and truth claims. As Williams et al. (2020) pointed out, within the range of tools available for appraising the methodological quality of qualitative studies, there is confusion about what should be assessed. For example, is it adherence to hallmarks of qualitative research like credibility, transferability, dependability, and confirmability; or adherence to reporting guidelines with indicators about the extent and transparency of reported study information? These points will be addressed in the review limitations.
Two authors independently assessed each study against the relevant study design checklist. Studies were rated against 8 or 9 appraisal criteria, depending on the checklist used with rate response options for each criterion recorded as yes, no, or unclear. A final score of between 0 (indicating low quality) and 1 (indicating high quality) was agreed only when two assessors rated 100% agreement on each item. A third author adjudicated on discrepancies.
Findings
Characteristics of Included Papers
A total of 57 papers met our inclusion criteria. These comprised 50 empirical studies, and 7 program descriptions. We included program descriptions because these provided detailed information on parent program involvement, oftentimes more detailed than could be provided in study reports. The 57 papers were published from 1984 to 2021, with most falling in the 1980s and 1990s (n = 41, 72%), indicating growth and then a decline in the volume of scholarship on CSA prevention programs involving parents. The majority of papers originated from the United States of America (USA) (n = 38, 65.5%), followed by Canada (n = 7, 12.1%), Ireland (n = 2, 3.4%), and New Zealand (n = 2, 3.4%). One paper was included from each of Argentina, China, Germany, Malaysia, the Netherlands, England, Iran, Israel, and Scotland (n = 1, 2%). In the presentation of findings that follow, we report analyses variously using papers (n = 57), studies (n = 50), and program descriptions (n = 7).
Of the 50 included studies, 27 (54%) used a pre- and post-test design with a control group and another 9 (18%) used a pre- and post-test design without a control group. Other study designs included six feasibility studies one of which was purely qualitative (12%), three cross-sectional studies (4%), and four other qualitative studies (6%). One paper was a study protocol (2%). Supplemental Table 1 shows study characteristics.
Study Quality
The quality of the 50 studies included in our review was highly varied. For the quasi-experimental tool, scores ranged between 0.2 and 1.0. For the cross-sectional tool, scores ranged from 0.25 to 1.0. For the qualitative tool, scores ranged between 0 and 0.6. We noted that studies with lower scores tended to have been published earlier (in the 1980s or 1990s), prior to the introduction of ever more stringent reporting guidelines. We did not perform quality appraisals on program descriptions or study protocols because program evaluations had not yet been completed. Quality appraisal scores are shown in Supplemental Table 1.
Programs
A wide range of programs were the subject of empirical studies or program descriptions involving parents including Body Safety Training program (n = 5) (e.g., Wurtele et al., 1992a), Red Flag/Green Flag (n = 4) (e.g., Kolko et al., 1987), Stay Safe program (n = 3) (e.g., MacIntyre & Carr, 1999), Talking About Touching (n = 2) (e.g., Madak & Berg, 1992), Keeping Ourselves Safe (n = 2) (e.g., Briggs & Hawkins, 1994), Kids Learning About Safety (n = 2) (e.g., Kenny, 2009b), Who do you Tell (n = 2) (e.g., Tutty, 1997), and others. Several programs were not named (n = 8). Program names are recorded in Supplemental Tables 1 and 2.
Parents
Of the included 50 studies, all provided for optional parent involvement. However, only 27 studies reported on any data collected from parents. Parent sample sizes ranged from 4 (Ruzicka et al., 2021) to 355 (Kolko et al., 1987); however, in many studies, precise parent participation numbers were not given. Small studies predominated. No study provided corresponding child and parent participation rates; therefore, it was not possible to establish the extent to which both child and parent(s) had been exposed to a program. Consistent with previous research, female rather than male caregivers were the predominant participants. The proportion of female caregivers, compared to any other caregiver, involved in CSA programs ranged between 62% and 100%, as shown in Supplemental Table 1. In three studies, participants were described as 100% mothers (Khoori et al., 2020; Ruzicka et al, 2021; Tremblay & Bégin, 2000). We identified no studies in which male caregivers comprised the larger proportion of participants. No studies reported any data on parents from diverse sexual orientations or gender identities.
The racial/ethnic backgrounds of participating parents were inconsistently reported. From the information given, 14 studies reported a majority White/Caucasian parents (Binder & McNeil, 1987; Briggs & Hawkins, 1996; Ko & Cosden, 2001; Liddell & Young, 1986; Poche et al., 1988; Pohl & Hazzard, 1990; Ratto & Bogat, 1990; Tutty, 1997, 2000, Wilson & Golub, 1993; Wurtele et al., 1992a, 1992b; Wurtele, 1993a, 1993b). Kenny’s (2009a, 2009b, 2010) studies conducted in Florida reported a majority Hispanic parents (71%–90%); Briggs and Hawkins (1994) New Zealand study reported one-third combined Maori and Pacifica parents; Kimberly’s (2020) study reported a majority African American parents (68%); and Weatherley et al.’s (2012) Malaysian study reported a majority Malay parents (74%). Two studies reported parent faith backgrounds as Jewish (Gesser-Edelsburg et al., 2017) and Catholic (Swan et al., 1985).
The timing of parent involvement in CSA prevention programs varied. Of the 57 included papers, parents were involved: at the same time as their child’s engagement (in 31 programs, 54.4%), before their child’s engagement (in 26, 45.6% of the programs), and after their child’s engagement (n = 10, 17.5%). 2 CSA prevention programs were delivered to children in narrow age range groups typically in single classes (e.g., preschoolers; Tutty, 1992), though some programs appeared to be offered in increments spanning multiple school year levels (e.g., Grades 1–5, Jin et al., 2017), and others where programs were offered to several but not all grades (e.g., Grades 1 and 3, Hébert et al., 2001). Of the 50 evaluation studies, 34 (68%) targeted primary (elementary) school children (aged ~5–12 years); 26 (45.6%) targeted preschool children (aged 0–4 years), and 6 (10.5%) targeted secondary (high) school young people (aged ~12–17 years). As will be described below, the timing of parent involvement, in some programs, was related to child age, with greater involvement expected and offered to parents with younger children.
Rationales for Parental Involvement
In the entire corpus of 57 papers (inclusive of empirical studies and program descriptions), we identified five main rationales used to justify parental involvement in child-focused CSA prevention programs: (i) monitoring and shaping parental attitudes toward CSA program delivery in schools; (ii) reinforcing children’s learning at home; (iii) promoting parent–child communication about CSA prevention; (iv) building parent capacity to respond to child disclosures, and (v) supporting program delivery for preschoolers. These rationales provide clues to aspects of underlying program theories.
The first rationale for parent/caregiver involvement was to monitor and shape their attitudes toward the provision of CSA prevention programs. In this rationale, parent/caregiver attitudes were thought to exert an influence on schools’ CSA prevention program uptake. It followed, therefore, that to create a positive attitudinal climate among parents/caregivers, they should be involved early in the program implementation process. This typically entailed providing information to parents/caregivers and inviting them to information sessions to meet program facilitators, share their views, and have questions answered (e.g., Hébert et al., 2001; MacIntyre et al., 2000; Madak & Berg, 1992; Kolko et al., 1987; Taal & Edelaar, 1997), and obtaining parental consent for their child’s participation prior to program implementation (e.g., Pohl & Hazzard, 1990; Swan et al., 1985; Wurtele et al., 1986). In 36 of the 57 papers (63.2%) programs sought parental consent for children to take part in a child-focused CSA prevention program.
The second rationale for parent involvement was to reinforce children’s learning at home. In this rationale, it was proposed that parents played a significant role in the reinforcement of program knowledge and skills (e.g., Borkin & Frank, 1986; MacIntyre & Carr, 1999; Tutty, 1997; Wilson & Golub,1993). Parental support for their children’s learning was encouraged in various ways such as via the provision of guided resources, role-play scenarios, topics for open discussion, and direct instruction on concepts. The intention was for parents to enhance classroom learning via repetition, a proven effective learning strategy, and to supplement classroom learning by contextualizing prevention messages to suit their child’s developmental stage, cognitions, and family experiences.
The third rationale for parent involvement was to promote parent–child communication about CSA and its prevention. In this rationale, congruent with ideas promoted in the provision of positive parenting programs (e.g., Sanders et al., 2014) and comprehensive sexuality education (e.g., Goldfarb & Lieberman, 2021), parents can be encouraged to begin conversations with their children about CSA and its prevention and to sustain these conversations over time. It was thought that when parents become actively involved in the CSA prevention programs, their willingness and ability to talk with their children about personal safety-related topics will increase. In turn, this was thought to further reinforce and contextualize program messages to suit family needs (e.g., Kenny, 2010; Tremblay & Bégin, 2000).
The fourth rationale for parent involvement was to build parents’ capacity to respond appropriately to CSA disclosures. This was evident in a small number of papers (e.g., Hébert et al., 2001; Kenny, 2009a; Tremblay & Bégin, 2000; Weatherley et al., 2012). In this rationale, it was proposed that parents may need to be prepared to be recipients of children’s disclosures and to be able to handle these effectively.
The fifth rationale for parental involvement was evident in papers addressing CSA prevention education for preschoolers. In this rationale, parental involvement was deemed necessary by children’s young age and perceived vulnerability (e.g., Miltenberger et al., 1991: Tutty, 1992).
Types of Parental Involvement
We coded the strategies and methods used for parental engagement in child sexual abuse prevention programs into six categories using Epstein et al.’s (2018) framework for parent–school–community partnership. These were as follows: (i) parenting, (ii) communication, (iii) learning at home, (iv) volunteering, (v) decision-making, and (vi) collaboration with community as shown in Table 2. In the corpus of 57 papers (inclusive of empirical studies and program descriptions), we identified 83 instances in which parental engagement could be classified into one of these six engagement types. This is shown in Supplemental Table 1.
Epstein’s (2018) Framework of Six Types of Involvement.
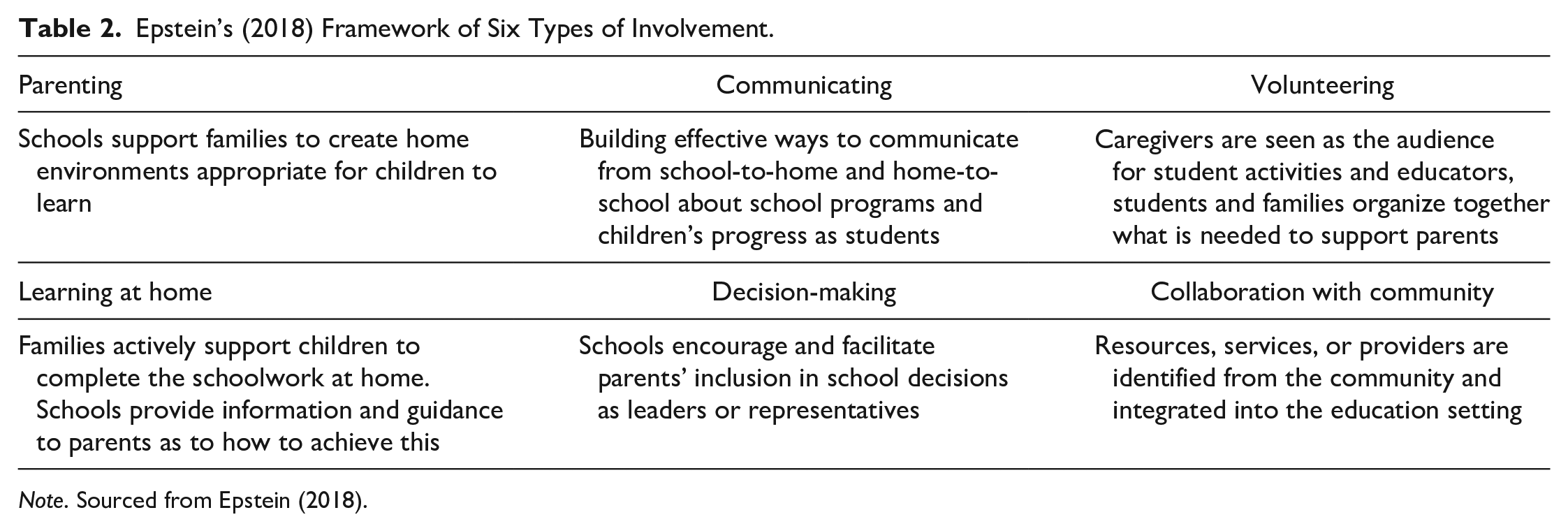
Note. Sourced from Epstein (2018).
The most used parental engagement strategy was communication. The communication category involved stakeholders designing effective forms of communication between preschool/school and home (Epstein et al., 2018). Two forms of school-to-home communication strategies were observed: program-specific communications and awareness-raising communications. In the program-specific communication strategy, parents were invited to attend workshops or information evenings held at the preschool or school. These sessions could be led by school staff or by program facilitators who would introduce the CSA prevention program content and methods. This communication strategy was used by the largest proportion of programs (n = 23, 42.1%) and occurred either before the program had been delivered or while the program was underway. At these information-sharing events, parents were provided an opportunity to ask questions about the content and delivery method of the programs, with the understanding that parents would benefit from understanding how program providers taught sensitive topics to their children. The awareness-raising communication strategy identified in one-third of programs (n = 19, 33.3%) was to provide general CSA education sessions to parents about CSA. These sessions, either workshops or events, did not discuss specific program content but were designed to raise awareness and impart factual knowledge on CSA warning signs and indicators, risk and protective factors, ways of keeping children safe, and managing disclosures. Like the workshops or information evenings, these education sessions tended to be offered to parents before or during program delivery with children. In these communication sessions, materials such as videos, lectures, group discussions, and anonymous question times were used as engagement tools. In 10 (17.5%) of the programs, parents were provided with materials to take home with them and these included an overview of the proposed curriculum (Fisher, 1985; MacIntyre & Carr, 1999; MacIntyre et al., 2000; Meiksin et al., 2019; Tobin, 1985), practical resources to use with children at home via which to spark discussion such as posters or storybooks (Liddell & Young, 1986; Spungen et al., 1989) or booklet and pamphlets on child sexual safety (Johnson, 1987).
The second most used parental engagement strategy was learning at home. Over one-third of programs (n = 21, 36.8%) used a learning-from-home approach which could be further subdivided into two parental engagement sub-categories. The first learning from home sub-category delegated parents as teachers, to deliver the CSA prevention program with their child(ren) at home, with the preschool or school venue serving only as a conduit. This approach was utilized by 11 programs (19.3%). In this approach, parents were provided with preparation in the form of training and issued with a curriculum to guide program delivery. Parents were the sole program facilitators. Practical resources were offered to parents to support program delivery including workbooks with scripted scenarios or vignettes to prompt discussions with children. The second learning-from-home sub-category engaged parents only in homework support. This was evidenced in 10 programs (17.5%) in which parents provided supplementary support to complement a program delivered in preschool or school by teachers or program facilitators. In this approach, children completed the CSA prevention program at school and were encouraged to complete homework with parents to repeat and reinforce program concepts and messages. Homework tasks could be workbooks, story books, coloring books, sticker book activities, topic discussions, and guided role-plays.
The third most used parental engagement strategy was volunteering, where parents were offered an opportunity for program participation mirroring the way students were engaged. Participation was always optional (hence, “volunteering”). Ten programs (17.5%) included an element of parental volunteering. Of these, volunteering parents were taught the program side-by-side together with their children (n = 4, 7.0%), or in parallel separately without their children (n = 6, 10.5%). A side-by-side example is where a group of parent–child dyads watched a puppet show together (e.g., Borkin & Frank, 1986: Gesser-Edelsburg et al., 2017; Johnson, 1987). An in-parallel example is where a program was delivered to parents with adaptations for an adult audience (e.g., Currier & Wurtele, 1996; Kenny, 2010; Tremblay & Bégin, 2000).
The fourth most used parental engagement strategy was decision-making in which parents were co-opted, indirectly, to CSA program decisions. This approach was broadly evident in several programs (n = 9, 15.8%). Program providers sought parental input before program deployment, typically within information-sharing sessions. Parents were offered the chance to preview program content and methods in videos or plays designed for children and provided views on program feasibility and acceptability, thereby enabling program facilitators to tailor programs for specific audiences. After program completion, parents provided feedback on their children’s responses. For example, they commented on whether they noticed changes in the child’s demeanor or behavior. They provided their perceptions on changes in their child’s use of self-protective behaviors, and their willingness to discuss CSA and its prevention with their child.
The fifth and least used parental engagement strategy was collaboration with the community. This approach involves mobilizing and coordinating other agencies and referral services within the community to wrap support around program delivery. We observed a version of this in only one program that introduced parents to members of the community who could be contacted later for referral to CSA-related services (MacIntyre et al., 2000).
None of the studies directly addressed Epstein’s sixth involvement strategy, parenting. To be coded into this category, a CSA prevention program would need to assist families by equipping them with knowledge and skills for CSA prevention in the context of understanding child and adolescent development (particularly sexual development), and the program would partner with parents to create conditions for CSA prevention at home and in day-to-day family life. Therefore, to be coded into this category, CSA prevention programs would need to evidence at least some of the characteristics of parent-led or parent-focused interventions as noted in the literature review above (e.g., Mendelson & Letourneau, 2015; Rudolph et al., 2022) with explicit teaching (of parents) how these strategies could also be used in other contexts to keep children safe. The absence of such papers in our corpus of 57 papers may signal a lack of connection or cross-over between the two programmatic routes by which parents are recruited into CSA prevention (i.e., parent-led programs, and child-focused programs), and this may represent lost opportunities to fully mobilize parents in prevention efforts.
Barriers to and Facilitators of Parental Involvement
In the corpus of 57 papers (inclusive of empirical studies and program descriptions), we identified several barriers and facilitators for parental involvement in CSA prevention programs.
Of the 57 papers, 26 papers mentioned barriers. The most frequently reported barrier was ineffective program engagement modalities that were incongruent with family routines, schedules, and time constraints within busy families (Kenny, 2009a; Kolko et al., 1989; Ruzicka et al., 2021; Shumow, 1988; Charlesworth & Rodwell, 1997; Wurtele et al., 1992b). One paper acknowledged that modalities for program involvement requiring attendance at meetings assumed that parents could devote significant time and energy to be involved in CSA prevention education. This made it inaccessible to some families, particularly isolated families and lower socioeconomic status families who could not afford to allocate time away from work or easily organize others to take over parenting duties (Briggs & Hawkins, 1994). One paper specifically nominated the absence of suitable childcare as a barrier to parental participation in evening information sessions (Kenny, 2009a). One paper reported extensive outreach that gained momentum over a 2-year period to engage parents of preschool-aged children in a social worker-delivered child personal safety program. Parental engagement efforts grew to involve parents in a planning committee, posting letters to each parent accompanied by program brochures, having posters displayed in daycare centers, scheduling evening parent sessions, sending reminder notices, offering complementary dinner and childcare for families attending, and having daycare staff present to demonstrate their support (Spungen et al., 1989).
A cluster of barriers related to fears and misconceptions appeared related to both child participation and parental involvement in programs. These included the taboo nature of the topic (Khoori et al., 2020), the belief that their children were not at risk (Wurtele et al., 1991), worry that programs would frighten children (Ratto & Bogat, 1990; Tutty, 2000; Wurtele et al., 1986), discomfort about children’s sexuality (Liddell & Young, 1986; Sprungen et al., 1989); concern that the program would trigger parents’ own painful memories (Wurtele et al., 1992a), parental distress about the topic (Spungen et al., 1989), and spousal opposition (Khoori et al., 2020). These fears and misconceptions were interpreted by researchers to explain reasons for and define different levels that may prevent parents from engaging comfortably in CSA prevention programs, and this seems particularly relevant to parents of preschool-aged children who may believe children are too young for this topic to be introduced.
Of the 57 papers, 22 papers mentioned one or more facilitators of parental involvement. Prior awareness of knowledge of CSA and its prevention potentially acted as a facilitator of parental engagement in programs. In evaluated programs in which baseline information was collected from children’s parents, it was hypothesized that parents with fair knowledge of the subject matter and/or were more informed on the topic prior to participating were more highly motivated toward program involvement (Briggs & Hawkins, 1994; Tremblay & Bégin, 2000; Tutty, 1997). Although programs were able to capitalize upon this motivation, there was never a description of how parents could be supported to further increase their knowledge and become involved in more meaningful ways.
A cluster of facilitators related to programs’ use of outreach, communications, and information provision. Most papers described providing parents with some kind of learning materials. With many of the papers reporting on programs evaluated in the 1980s and 1990s proceeding the ubiquity of electronic communications, materials were typically provided in hard copies. These materials explained program content and methods, reinforced program themes and messages, and provided suggested ways to approach conversations about CSA with children. Three papers emphasized the crucial nature of sensitive program adaptation, including outreach, for culturally and linguistically diverse parent groups (Kenny, 2009b, 2010; Tobin, 1985). Two studies, as described above, provided a suite of outreach activities, as a method for supporting and enabling parents’ program involvement (Jin et al., 2017; Spungen et al., 1989). Another included a follow-up phone call with parents to check in and monitor program compliance (Ratto & Bogat, 1990).
Discussion
Given the continuing high prevalence rates for CSA (e.g., Mathews et al., 2023), its serious effects (Hailes et al., 2019), and the associated economic burden (Letourneau, Brown, et al., 2018), there is a pressing need for effective prevention efforts to which all members of children’s social ecology are contributors. Parents are their children’s first educators (Walsh & Brandon, 2012) and there are long-standing calls for their involvement in CSA prevention efforts (Wurtele & Kenny, 2010). Decades of international research in a multitude of disciplinary fields, not least in education, has demonstrated that parental involvement matters: it translates to benefits for children (Kim, 2022).
Our aim with this review was to identify rationales, approaches, and barriers and facilitators to parental involvement in child-focused CSA prevention programs. In addressing these aims, we classified parental involvement using an existing evidence-based typology (Epstein et al., 2018). We uncovered parent-participatory practices that have been used (so far) in child-focused CSA prevention programs. We have also uncovered practices that appear to be missing.
The inductive classification of five rationales for parents’ involvement provides clues for a more detailed, albeit untested, underlying theory of change for child-focused CSA prevention programs with parents as adjuncts. For example, beginning early in the preschool years, if parents have baseline CSA knowledge, hold positive attitudes toward CSA program delivery, and can reinforce children’s learning at home, this may result in better, more frequent, and earlier parent–child communication about CSA prevention, and supportive responses to child disclosures.
Missing from this discourse was parental gender equity. Aligning with previous research, we found that female, rather than male, caregivers were most often involved (or assumed to be involved) in programs and their involvement was more strongly observed (and expected) in CSA prevention programs with younger children of preschool age. This means that the burden of CSA prevention disproportionately falls on females. Although some previous studies have shown that CSA disclosures are most likely to be made to children’s mothers (e.g., Russell & Higgins, 2021; 2023), recent research synthesis on CSA disclosure pathways suggests that children, particularly girls, may first test the waters by disclosing to same-age peers before then disclosing to a parent, most likely their mother (rate range 24%–77%); however, a meaningful minority disclose to fathers (rate range 1.7%–20%) (Manay & Collin-Vezina, 2021). Given that disclosure is a “relational process” (Manay & Collin-Vezina, 2021, p. 16), involving considerations of trust, reliability, and help-seeking capability, more can be done to mobilize fathers’ involvement including in building their base-level knowledge of CSA, its characteristics, and prevention, and later shaping their attitudes positively toward program delivery. The complexity and sensitivity of fathers’ involvement should also be recognized since males, including but not limited to fathers, are the predominant CSA offenders (e.g., Mathews et al., 2023) and little is known about the outcomes of broad-based educational and awareness-raising interventions for CSA prevention with men. For example, secondary influences on offending trajectories and help seeking have not thoroughly been studied.
Deductive classification of parental involvement against Epstein’s (2018) six categories revealed that communication, learning at home, and volunteering were the most used approaches. Our findings show that parental involvement in CSA prevention programs was most often due to program provider efforts in communicating with parents. This was typically done via workshops or information sessions where prescribed information about CSA generally and/or program-specific information was given to parents. However, parents’ actual information needs did not seem to be considered and, arguably, should be. For example, if parents within a community are hesitant for children to learn about CSA, then it may be important to share program-specific information to alleviate concerns about what will be taught and how. However, if the goal of parental involvement is to support a whole-of-community response to CSA, then general CSA knowledge and behavioral skills training might be more important.
We found parent involvement in program decision-making and collaboration with the community were seldom used strategies. These findings are important for program developers and implementers as there appear to be many lost opportunities to mobilize parents in prevention efforts. For example, via parent representation on school boards and governing bodies who make decisions on resource allocation, or via parent councils, committees, and associations working collaboratively with school staff to select and schedule interventions. Our study did not uncover any programs that were specifically co-designed with parents; however, we are aware that at least one is underway (e.g., Malamsha et al., 2021) and program co-design with stakeholders and end-users is increasing in health research broadly (e.g., Slattery et al., 2020). However, guidance on program co-design with parents in the complex field of CSA prevention is lacking.
Epstein’s (2018) category of “parenting” was completely absent or, at the very least, invisible in study reports, highlighting the gap between child-focused and parent-focused prevention. To address this and create more opportunities to support parents in their parental roles, child-focused CSA prevention programs with parents as adjuncts can look toward excellent examples in parent-led and parent-focused CSA prevention programs, especially for behavioral skills training. This would involve incorporating direct teaching of protective parenting approaches such as monitoring, supervision, caution around care delegation, checking in with children, and warm and open communication (Guastaferro, Felt, et al., 2020; Mendelson & Letourneau, 2015; Rudolph et al., 2022).
We identified a dominant barrier to parent involvement in CSA prevention programs: ineffective program engagement modalities. Our findings showed that school-based programs engaged parents through a range of modes and materials along an involvement spectrum. From learning about and agreeing to their child’s participation in a program, through attending information sessions and receiving handouts, to completing homework activities alongside their child/ren. However, we found that programs stopped short without capturing opportunities to reach the very far end of the involvement spectrum in which, in the future, we might find dual-focused CSA prevention programs, aiming to increase the knowledge and skills of children and young people together with their parents and caregivers. These programs would incorporate the best of child-focused programs AND the best of parent-led or parent-focused programs. An important next step down this integrated prevention program route would be to evaluate the effect of these approaches on both child and parent outcomes. Future studies could also investigate whether the involvement of one or both parents differentially affects the program outcomes. Disclosure data must be collected as this can provide one indicator that a prevention program might actually result in children’s application of new knowledge and skills to threat situations (Guastaferro, Shipe, et al., 2023). Disclosure data may there provide insight into the effectiveness of different types of parental involvement.
We identified a dominant facilitator of parent involvement in CSA prevention: prior awareness of knowledge of CSA and its prevention. Our findings show that parents’ knowledge of CSA prevention was a facilitator of their involvement in child-focused CSA prevention programs. However, it is unclear due to the limitations in study designs whether parent prior knowledge improves prevention program outcomes for children. Therefore, to ensure parents are on a level playing field, parental involvement (e.g., in information sessions or education and training) should occur before a child-focused program is implemented. Alternatively, parent-led or parent-focused programs could be fully implemented prior to children engaging in a program. Involving parents in a parent-focused program prior to the implementation of a child-focused program provides opportunities to build baseline knowledge, increase their self-efficacy for CSA prevention discussions with their children, and monitor and shape parents ’attitudes toward program delivery. In a best-case scenario, informed parents can leverage social networks to create a groundswell of support for program delivery. Involving parents in CSA prevention education before their child’s program participation can also address further barriers identified in this review, those relating to fears and misconceptions which were more evident for parents of younger children and should be addressed considering the known age of onset of child sexual abuse in pre-adolescence and adolescence (Abd el Rahman et al., 2017; Aydin et al., 2015; Ferragut et al., 2021; Finkelhor, 1995; McKillop et al., 2015). A final benefit to parent involvement before child participation is that parents themselves will receive CSA prevention education. Many will not have received this, themselves, while at school. Critical findings are summarized in Table 3.
Critical Findings.
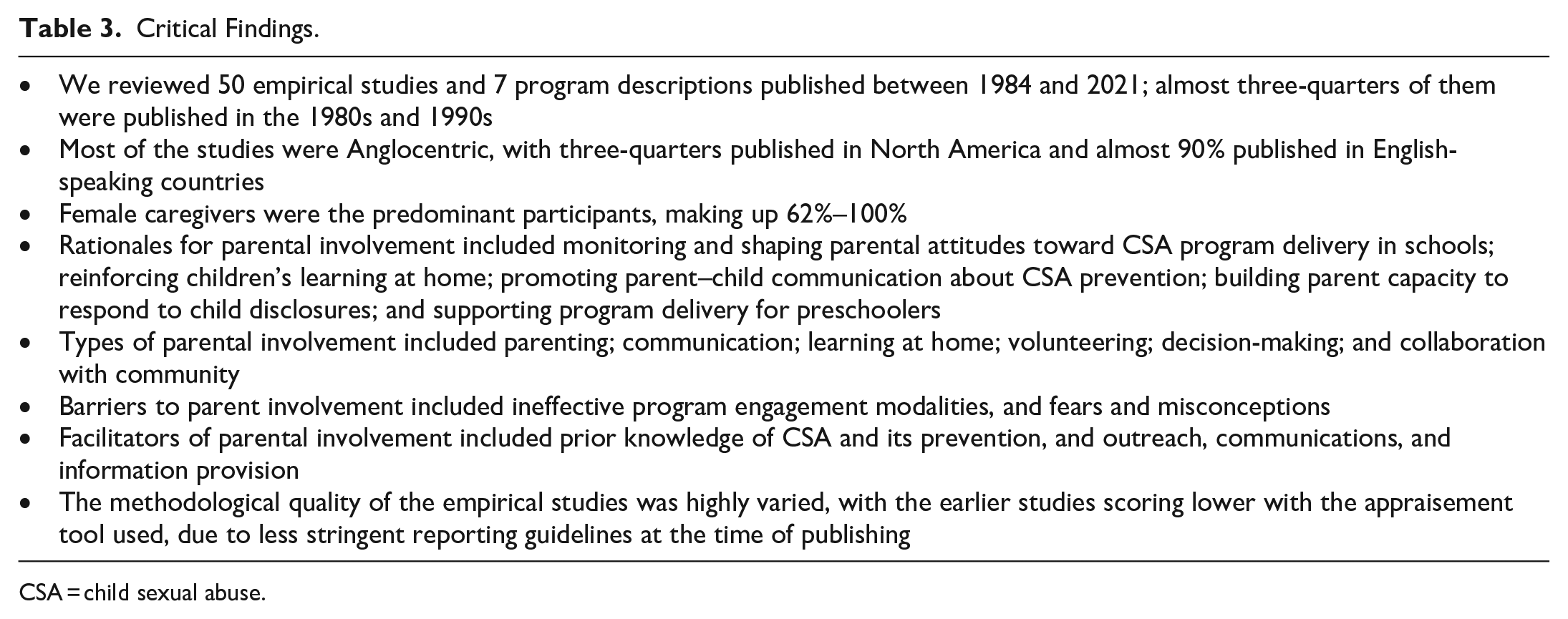
CSA = child sexual abuse.
Diversity
The generalizability of findings from this review should be interpreted with several diversity limitations in mind. The empirical studies and program descriptions included in this review were conducted in high- and middle-income countries. Reporting on the plurality of parental demographic characteristics, including cultural and linguistic diversity, sexual orientations and gender identities, and (dis)ability status was poor, and should be improved in future study reports. As noted above, many studies (and the interventions they were evaluating) focused on mothers.
Limitations
This review was limited to an analysis of parent involvement in child-focused CSA prevention education. We did not inquire into the outcomes or effectiveness of parent involvement; this has been studied in detail by Rudolph et al. (2024). In addition to the above-mentioned diversity limitations, the body of research is aging with only six studies reported in the past 10 years. The studies had methodological weaknesses associated with variability in study designs and selective reporting of program features, sample characteristics, and study procedures.
Implications for Practice and Future Research
From our review, there are several key implications for practitioners, policymakers, and researchers to consider in their work (see Table 4).
Implications for Practice, Policy, and Research.
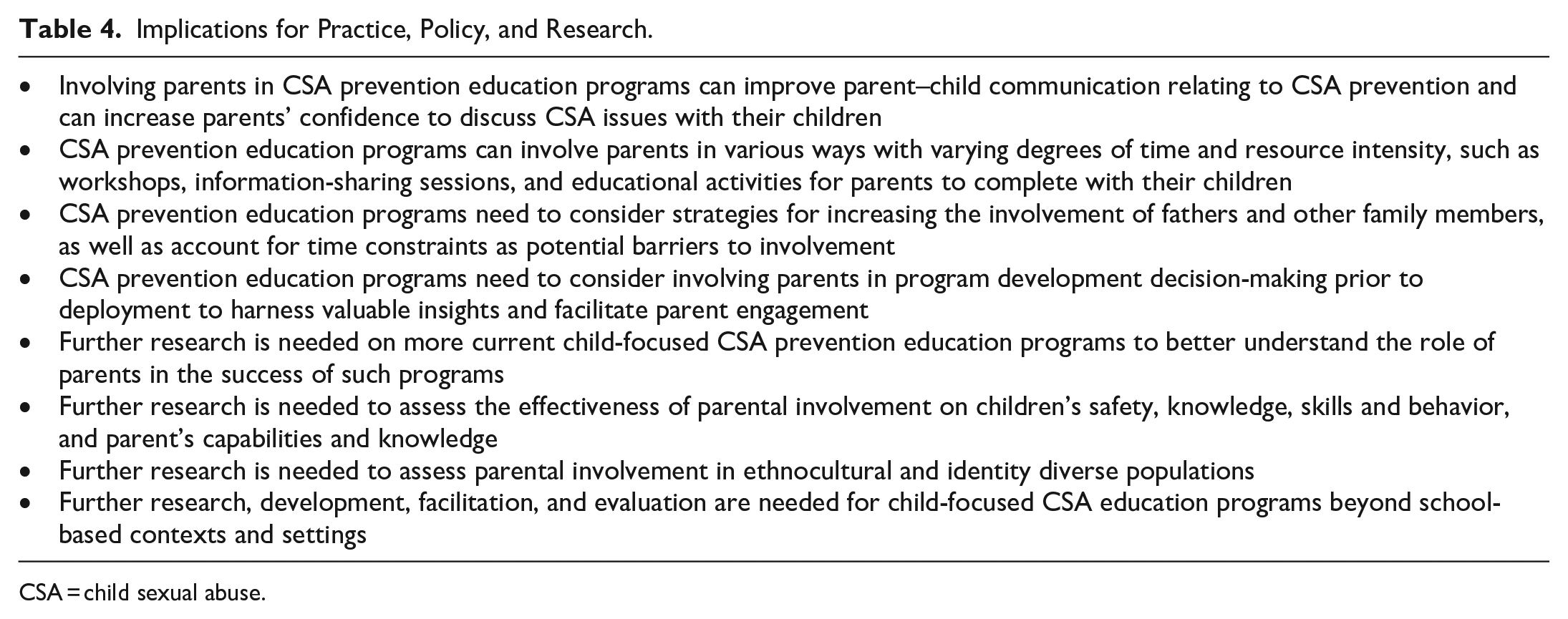
CSA = child sexual abuse.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241235895 – Supplemental material for Engaging Parents in Child-Focused Child Sexual Abuse Prevention Education Strategies: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380241235895 for Engaging Parents in Child-Focused Child Sexual Abuse Prevention Education Strategies: A Systematic Review by Douglas Hugh Russell, Sebastian Trew, Lottie Harris, Jessica Dickson, Kerryann Walsh, Daryl John Higgins and Rhiannon Smith in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review is based in part on work that was funded by Bravehearts Foundation—an Australian child protection organization dedicated to the prevention and treatment of child sexual abuse through funds provided by the Westpac Safe Children, Safe Communities grant scheme.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.