
Abstract
This systematic review examines the impact of parental preconception adversity on offspring mental health among African Americans (AAs) and Native Americans (NAs), two populations that have experienced historical trauma and currently experience ethnic/racial mental health disparities in the United States. PsycINFO, PubMed, CINAHL, Scopus, and Web of Science were searched for studies that included at least two generations of AAs or NAs from the same family, measured parental preconception adversity and their offspring’s mental health, and examined the association between these variables. Over 3,200 articles were screened, and 18 articles representing 13 unique studies were included in this review. Among the studies with samples that included AAs (n = 12, 92%), 10 (83%) reported a significant association between parental preconception adversity and adverse offspring mental health. The only study with a sample of NAs (n = 1, 8%) also reported a significant association between these variables. Although the literature suggests that parental preconception adversity is associated with offspring mental health among AAs and NAs, it must be interpreted in the context of the small number of studies on this topic and the less-than-ideal samples utilized—just one study included a sample of NAs and several studies (n = 6, 46%) used multi-ethnic/racial samples without testing for ethnic/racial disparities in their results. A more rigorous body of literature on this topic is needed as it may help explain an important factor underlying ethnic/racial mental health disparities, with important implications for interventions and policy.
Keywords
In the United States, African Americans (AAs) and Native Americans (NAs) experience worse psychological and behavioral health—henceforth referred to as mental health—when compared to White Americans (WAs). The percentage of adults who report depressive symptoms like feelings of sadness and that everything requires effort are 4.2% and 11%, respectively, in AAs compared to 2.6% and 6.6% in WAs (U.S. Department of Health and Human Services Office of Minority Mental Health, 2021). AAs also experience chronic depression at greater rates (56.5% vs. 38.6% in WAs) and are 2.4 times more likely to be diagnosed with schizophrenia compared to WAs (Olbert et al., 2018; Williams et al., 2007). In addition, AA adolescents are two to three times more likely to attempt suicide than WA adolescents (Romanelli et al., 2021). Among NAs, the percentage of adults who report depressive symptoms such as feelings of worthlessness, serious psychological distress, and that everything requires effort are 3.4%, 4.5%, and 10.5%, respectively, relative to 2.3%, 3.8%, and 6.6% among WAs (U.S. Department of Health and Human Services Office of Minority Mental Health, 2021). The prevalence of posttraumatic stress disorder (PTSD) is 23% in NAs compared to 12% in WAs, while 20% of NAs had alcohol use disorder in the past year relative to 14% of WAs (Emerson et al., 2017). Importantly, the suicide rate among NAs has increased recently from 22.3 to 28.1 per 100,000, whereas the suicide rate among WAs has decreased from 18.1 to 17.4 per 100,000 in the same time frame (Stone et al., 2023).
These mental health issues are often compounded because psychological symptoms experienced by AAs and NAs co-occur with other mental illnesses, as sufferers may engage in negative coping mechanisms to manage their symptoms (Brave Heart, 2003; Gaskin et al., 2004). For example, Emerson et al. (2017) found that NAs were 67% more likely to have had alcohol use disorder in the past year if they also experienced PTSD. Similarly, suicide attempts co-occurred with symptoms of depression and substance use among AA adolescents (Romanelli et al., 2021). It may be the case that AAs and NAs use drugs and alcohol to cope with their mental health problems. Because AAs and NAs may engage in maladaptive coping mechanisms to manage their psychological symptoms, effective mental health interventions are often two-pronged. These interventions target both mental health problems and maladaptive coping behaviors (e.g., alcohol use) that further disrupt mental health (Benzies et al., 2011; Brave Heart, 2003). Although maladaptive coping may be a result of mental illness, psychological problems may initially develop in AAs and NAs due to exposure to adversities. Herein, the term adversity refers to all forms of stressful, traumatic, or negative life events experienced from childhood onward that may precipitate a toxic stress (e.g., neurobiological or physiologic) response. That is, adversity includes adverse childhood experiences (ACEs), but comprises a wider array of negative life experiences reported by AAs and NAs. 1 Given that adverse experiences are associated with mental health ailments (Sahle et al., 2021) and that AAs and NAs experience more adversities than WAs (American Psychological Association [APA], 2017), it is important to consider the role that adversity may play in shaping ethnic/racial mental health disparities across generations.
Historical trauma is a form of adversity that presents unique challenges for AAs and NAs that may help explain ethnic/racial mental health disparities (Brave Heart & DeBruyn, 1998; Gaskin et al., 2004; Sotero, 2006). Brave Heart (2003) defines historical trauma as the cumulative emotional and psychological suffering that has been inflicted on a population over generations. AAs have experienced historical trauma in the form of the Atlantic slave trade, slavery, Jim Crow laws, and systemic racism (DeGruy, 2010), and NAs have experienced historical trauma via colonization, forced migration and acculturation, genocidal wars, and systemic ethnic discrimination (Brave Heart & DeBruyn, 1998). Although historical trauma has been linked to negative mental health in individuals who initially experienced the trauma (e.g., slavery, colonization), these outcomes may also be transmitted to their offspring via epigenetic changes passed down through uterine signaling, DNA methylation, or other psychosocial or behavioral pathways (Conching & Thayer, 2019; Sotero, 2006).
Ancestral exposure to historical trauma may also indirectly affect descendants’ mental health by increasing their risk for exposure to adversity. Researchers have theorized that the disproportionate exposure to adversity experienced by AAs and NAs in the United States today can be traced back to the historical trauma experienced by these populations’ ancestors (Brave Heart & DeBruyn, 1998; Gaskin et al., 2004; Sotero, 2006). This idea is reinforced by the fact that AAs and NAs are more likely to experience all adversities, both related and not related to race/ethnicity, compared to WAs (APA, 2017). The literature on ACEs—which disproportionately affect AAs and NAs (Conching & Thayer, 2019)—provides an important framework with which to demonstrate the harms related to adversity exposure. Exposure to ACEs (e.g., child abuse, neglect) is associated with several mental health outcomes, including depression, PTSD, substance abuse, and suicidality (Bucci et al., 2016; Sahle et al., 2021). Specifically, early exposure to adversity can trigger a toxic stress response such that the neuroendocrine immune circuitry becomes dysregulated, producing irregular levels of stress hormones and neurotransmitters that cause lasting damage to brain structure and multiple organ systems. When these responses occur during development, they can become permanently incorporated into future stress regulation and can produce epigenetic modifications that increase the risk for mental illness in adulthood. These maladaptive changes are not only detrimental to AAs’ and NAs’ own mental health, but they may also be passed down to their offspring to affect their mental health too (Bucci et al., 2016; Conching & Thayer, 2019).
The link between exposure to historical trauma and future generations’ mental health has primarily been examined in First Nations Indigenous peoples of Canada and Jewish populations. Studies of Holocaust survivors have found that their descendants are at increased risk for PTSD and psychological distress (Dashorst et al., 2019). The offspring of First Nations parents who attended Indian Residential Schools (IRS) were more likely to experience depressive symptoms and suicidality than the offspring of parents who did not attend the IRS (Bombay et al., 2014). These bodies of literature suggest that victims of historical trauma (e.g., AAs and NAs) may have a higher vulnerability to poor mental health that is passed on to subsequent generations, thereby contributing to contemporary ethnic/racial mental health disparities.
Much of the work that has explored the transmission of adversity across generations in AAs and NAs has examined the impact of parental prenatal stress (stress during pregnancy) on offspring health and utilized multi-ethnic/racial samples. These studies demonstrate that maternal exposure to prenatal stress is negatively associated with infant mental health (Glover, 2011) through neuroendocrine immune circuitry and epigenetic alterations in the mother (Conching & Thayer, 2019). As populations that have experienced historical trauma, AAs and NAs disproportionately face adversities known to induce these biological changes (APA, 2017). Although there is substantial evidence for the negative effects of parental prenatal stress on offspring mental health, studies that explore the impact of parental preconception (before pregnancy) adversity on offspring mental health need equal attention (i.e., studies that examine parental adversities that occurred any time before conception, starting from the parent’s childhood up to, but before, the child was conceived). It is particularly important to synthesize studies that explore the impact of parental preconception adversity on offspring mental health in AAs or NAs specifically.
The Present Study
Given the known association between historical trauma and offspring mental health in Jewish and First Nations samples (Bombay et al., 2014; Dashorst et al., 2019), the burden of exposure to historical trauma and contemporary adversities for AA and NA populations (APA, 2017; Gaskin et al., 2004; Sotero, 2006), and the ethnic/racial mental health disparities these populations experience (U.S. Department of Health and Human Services Office of Minority Mental Health, 2021), the current study examines the literature to identify what is known about the connection between preconception adversity in AA and NA parents and the mental health of their offspring.
Method
Search Strategy
This review is registered in PROSPERO under protocol CRD42021240281 and was conducted through April 2021. The PICOS (participants, intervention [exposure], comparison group, outcome, study design) tool for systematic reviews was used to develop the search terms, search strategy, and eligibility criteria (Schardt et al., 2007). Participants were AAs and NAs in the United States, exposures were adverse experiences suffered by parents, and outcomes were mental health problems in the offspring. Study designs had to be quantitative. Search terms related to participants (e.g., AA, NA), exposure (e.g., stress, trauma), and outcome (e.g., depression, abnormal behavior) were developed. These were combined with terms related to intergenerationality (e.g., generation, family) for the literature search in online databases (see Supplemental Appendix A).
Inclusion Criteria
Inclusion criteria were developed both to be consistent with those used by similar systematic reviews (Gone et al., 2019; Plant et al., 2018) and to accomplish the aims of the current review. To be included in this review, studies must have met the following criteria:
Empirical, quantitative, and in English.
Include AAs or NAs living in the United States in their samples. If the study includes a multi-ethnic/racial sample AND does not test for ethnic/racial differences in its findings (i.e., compare AAs or NAs vs. other ethnic/racial group[s]), its sample must be ≥70% AA or NA.
Include at least two generations of participants from the same family.
Include measures of parental adversity exposure and offspring mental health, operationalized as psychological and behavioral outcomes, both at the individual level.
Include a measure of parental adversity that occurred any time before pregnancy with the offspring whose mental health is examined in the study.
Examine the association between parental preconception adversity exposure and offspring mental health.
Justification for Inclusion Criteria
This review comprised only studies with samples including AAs and NAs in the United States due to the historical trauma and disproportionate exposure to contemporary adversities that these populations have experienced in the United States. Given that research in Jewish and Canadian First Nations populations suggests historical trauma is associated with poor offspring mental health and that AAs and NAs experience worse mental health compared to WAs, it was essential that included studies empirically examined this link among AAs and NAs. Studies with multi-ethnic/racial samples were required to be ≥70% AA or NA when ethnic/racial differences in findings were not examined to increase the probability that the results for the full sample applied to the AAs or NAs in the sample. Because we were interested in the role of parental preconception adversity in potentially shaping offspring’s health, studies were required to include at least two generations of participants from the same family. In addition, studies were required to measure preconception adversity because much research has already been devoted to examining the link between prenatal adversity and offspring mental health (Glover, 2011). Finally, measuring adversity exposure and mental health at the individual level was essential for included studies to avoid the use of neighborhood or county measures that cannot be accurately designated to any individual or linked between family members.
Screening and Selection
To identify studies that examined the association between parental preconception adversity and offspring mental health among AAs and NAs in the United States, two reviewers (A.A. and A.J.) conducted independent literature searches in PsycINFO, PubMed, CINAHL, Scopus, and Web of Science (WOS) through April 2021 using search terms developed via PICOS (see Supplemental Appendix A). Duplicates were removed from the resulting articles via a citation manager. Each reviewer separately conducted the following processes: screened the articles’ titles; assessed the abstracts of articles whose titles seemed relevant; and read the full text of articles whose abstracts seemed to meet inclusion criteria. Upon reading the full text of the articles, each reviewer separately compiled those that met the inclusion criteria. To comprehensively identify any additional eligible articles, the reviewers then independently conducted forward and backward searches based on the initial set of articles that met the inclusion criteria for the review. This means that they gathered all the studies that their initial set of articles cited in their reference sections; they also gathered all the studies that cited their initial set of articles using WOS. Without removing duplicates from the resulting additional studies, each reviewer separately conducted the aforementioned screening processes of this second set of studies (e.g., by titles, abstracts, and full texts).
Upon separately completing the database search (thereby compiling initial articles for inclusion in the review) as well as the forward and backward searches (thereby identifying additional eligible articles), the two reviewers compared the total articles each believed met inclusion criteria and agreed on 73% of them. Discrepancies were resolved between the reviewers and an advisor (E.A.H.) via a consensual, iterative process until a 100% agreement was reached. Afterward, the first reviewer (A.A.) individually conducted a gray literature search to identify eligible unpublished studies by contacting researchers via the listservs of APA Division 56 (Trauma Psychology), APA Division 38 (Health Psychology), and the International Society for Traumatic Stress Studies special interest group “Intergenerational Transmission of Trauma and Resilience.” Without removing duplicates from the resulting unpublished studies, the studies were screened via the aforementioned screening processes (e.g., by titles, abstracts, and full texts). Some articles produced by the forward, backward, and gray literature searches were duplicates of the articles produced by the original database search.
Data Extraction and Quality Assessment
Descriptive data were extracted from all studies included in the review and a database of study characteristics was created for descriptive analyses. Analytic data were also extracted from all included studies and synthesized in a table of evidence (see Supplemental Appendix B). In addition, a quality assessment of the included studies was conducted using the Newcastle–Ottawa Scale (NOS; Wells et al., 2012). The NOS was chosen for this process because it is widely used and is considered suitable for systematic reviews of observational studies (Zeng et al., 2015). Adapted versions of the NOS for cohort (Kansagara et al., 2017) and cross-sectional (Herzog et al., 2013) studies were used in the current review (see Supplemental Appendix C).
Results
Search Results
Figure 1 presents a modified Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the article screening process (Moher et al., 2009). In total, 2,593 articles were identified through the database search: 612 articles were found in WOS, 274 in PubMed, 509 in CINAHL, 670 in Scopus, and 528 in PsycINFO. After removing duplicates, this initial collection included 1,672 articles. In addition, 1,589 articles were identified via forward, backward, and gray literature searches. Some articles produced by the forward, backward, and gray literature searches were duplicates of the articles produced by the original database search. A total of 3,261 unduplicated articles were screened for inclusion in the review; of these, 76 full-text articles were carefully reviewed after screening.
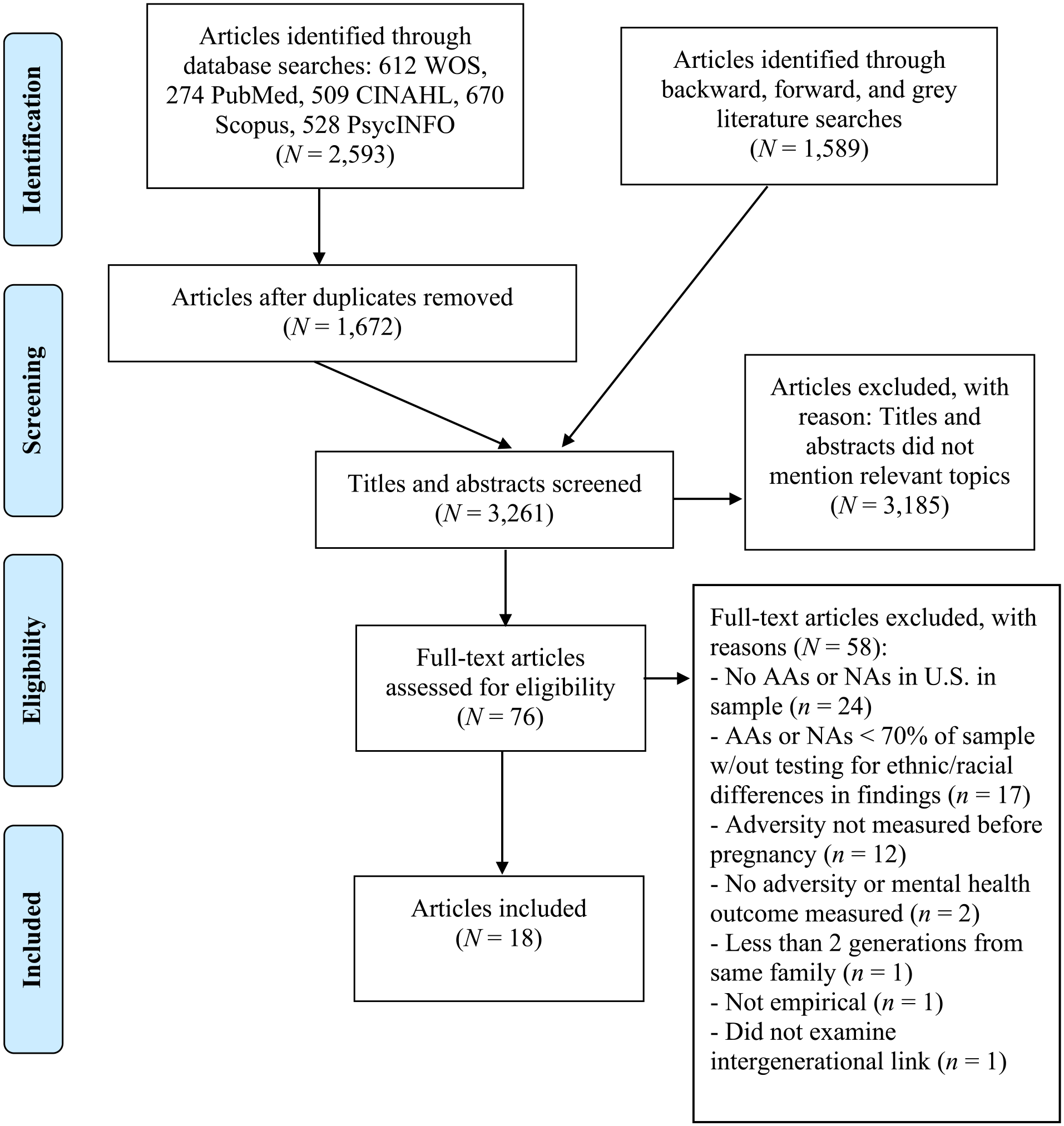
Preferred reporting items for systematic reviews and meta-analyses diagram.
Of these 76 articles, 58 were excluded for the following reasons: 24 articles did not include AAs or NAs living in the United States in their samples, 17 articles used multi-ethnic/racial samples that were <70% AA or NA and did not test for ethnic/racial differences in their findings, 12 articles did not measure parental adversity before pregnancy, two articles did not include individual-level measures of parental adversity or offspring mental health, one article did not include at least two generations of participants from the same family, one article did not examine the association between parental preconception adversity and offspring mental health, and one article was not empirical. The remaining 18 articles representing 13 unique studies were included in this review.
Of the 13 studies reviewed, one study yielded four articles (Esteves et al., 2017; Glackin & Gray 2018; Hatch et al., 2020; Pickett et al., 2018), another study produced two articles (Leifer et al., 1993; Paredes et al., 2001), and a third study published two articles (Russotti et al., 2021; Warmingham et al., 2020). There were 10 other independent studies included in the review. A table of evidence summarizes the key characteristics (e.g., sample size) of the 18 articles produced from the 13 studies (see Supplemental Appendix B). The table is divided into three categories: articles with samples that included exclusively AA or NA respondents (n = 5, 28%), articles with partial AA or NA samples that tested for ethnic/racial differences in their findings (n = 4, 22%), and articles with partial (≥70%) AA or NA samples that did not test for ethnic/racial differences in their findings (n = 9, 50%).
Key findings, including significant and nonsignificant associations, from the 13 independent studies reviewed are presented in Table 1. The table separates the studies into the aforementioned three categories. Four articles produced by one study fell into three different categories. From this study’s sample, Hatch et al. (2020) used a fully AA sample, Esteves et al. (2017) utilized a partial AA sample and tested for ethnic/racial differences in their findings, and Glackin and Gray (2018) and Pickett et al. (2018) used partial (≥70%) AA samples and did not test for ethnic/racial differences in their findings. The single study that produced these four articles was categorized as a study that used a fully AA sample. Both articles that were produced by another study (Leifer et al., 1993; Paredes et al., 2001) utilized exclusively AA samples, so the study was categorized as such. Similarly, both articles produced by a third study (Russotti et al., 2021; Warmingham et al., 2020) utilized partial (≥70%) AA samples and did not test for ethnic/racial differences in their findings, so the study was categorized as such. The rest of the studies in the table were unique and did not produce multiple articles. Because 13 studies produced 18 articles, there may be more than one article cited for each study described in the findings below.
Summary of Significant and Non-significant Findings From 13 Independent Studies.
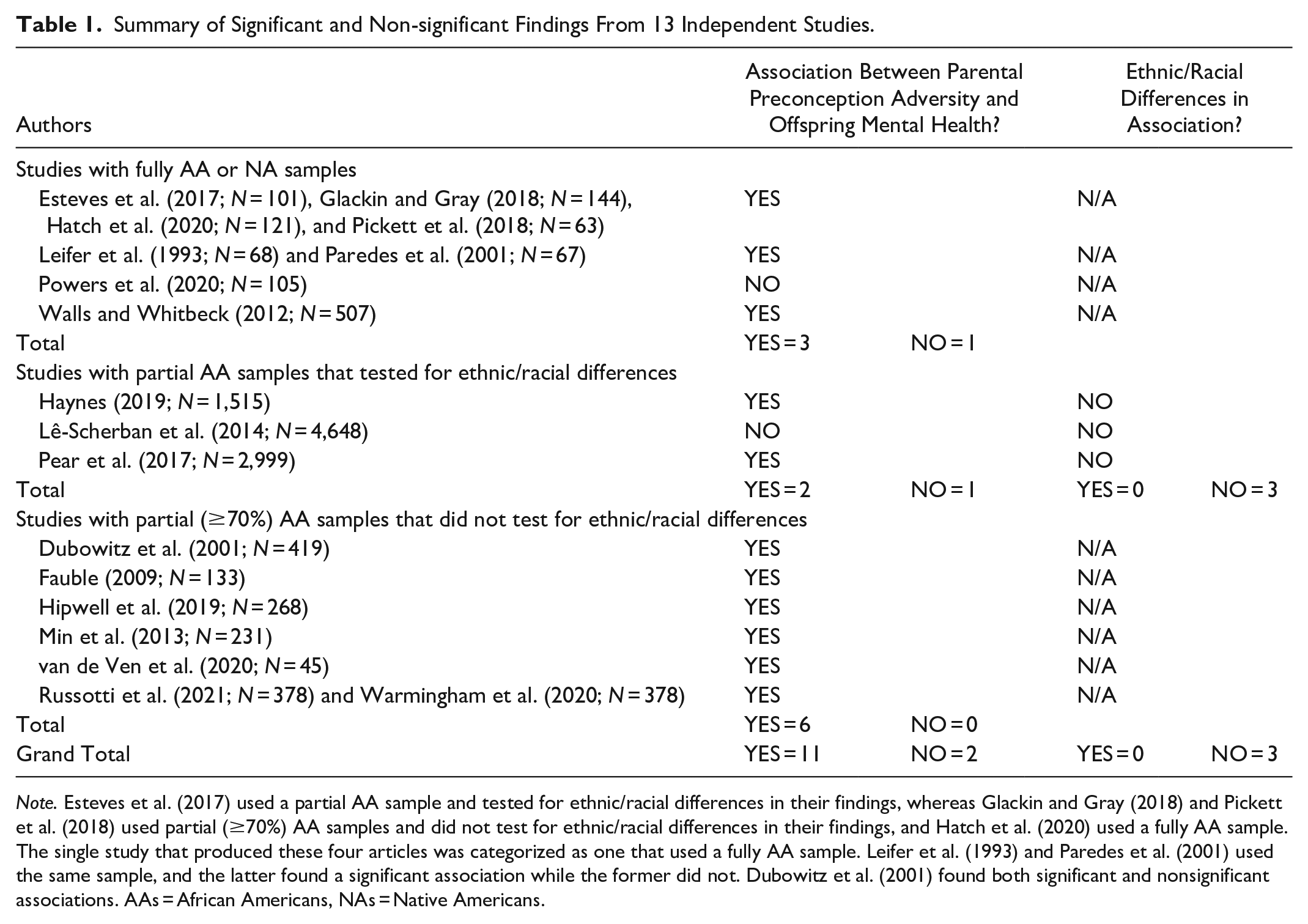
Note. Esteves et al. (2017) used a partial AA sample and tested for ethnic/racial differences in their findings, whereas Glackin and Gray (2018) and Pickett et al. (2018) used partial (≥70%) AA samples and did not test for ethnic/racial differences in their findings, and Hatch et al. (2020) used a fully AA sample. The single study that produced these four articles was categorized as one that used a fully AA sample. Leifer et al. (1993) and Paredes et al. (2001) used the same sample, and the latter found a significant association while the former did not. Dubowitz et al. (2001) found both significant and nonsignificant associations. AAs = African Americans, NAs = Native Americans.
Study Characteristics
Of the 13 included studies, four (31%) used fully AA or NA samples, three (23%) used partial AA samples and tested for ethnic/racial differences, and six (46%) used partial (≥70%) AA samples without testing for ethnic/racial differences (see Table 1). Studies with samples including AAs (n = 12, 92%) were published between 1993 and 2021, with the majority published after 2012 (n = 9, 75%). Of these 12 studies, seven (58%) used a prospective cohort design (Dubowitz et al., 2001; Fauble, 2009; Hipwell et al., 2019; Lê-Scherban et al., 2014; Min et al., 2013; Pear et al., 2017; van de Ven et al., 2020), and the remaining five studies (42%) were cross-sectional (Esteves et al., 2017; Glackin & Gray 2018; Hatch et al., 2020; Haynes, 2019; Leifer et al., 1993; Paredes et al., 2001; Pickett et al., 2018; Powers et al., 2020; Russotti et al., 2021; Warmingham et al., 2021). A single study of NAs (8%) was published in 2012 and utilized a cross-sectional design (Walls & Whitbeck, 2012).
Sample Characteristics
Sample sizes of the 12 studies that included AAs ranged from 90 to 9595 participants with a mean of 2,125, a median of 499, and a standard deviation of 3,509 (See Supplemental Appendix B for details). In addition, eight of these studies (67%) used a convenience sample of participants (Dubowitz et al., 2001; Esteves et al., 2017; Fauble, 2009; Glackin & Gray 2018; Hatch et al., 2020; Leifer et al., 1993; Min et al., 2013; Paredes et al., 2001; Pickett et al., 2018; Powers et al., 2020; Russotti et al., 2021; van de Ven et al., 2020; Warmingham et al., 2020). The remaining four studies (33%) used a subsample of participants who were recruited via probability sampling (Haynes, 2019; Hipwell et al., 2019; Lê-Scherban et al., 2014; Pear et al., 2017). In the single study that included NAs, 507 offspring were recruited from American Indian reservations in the United States (n = 439, 87%) and Canada (n = 68, 13%) via convenience sampling (Walls & Whitbeck, 2012).
Parental Adversity Measures
Of the 12 studies that included AAs, 11 (92%) utilized a maternal measure of adversity, while one (8%; Lê-Scherban et al., 2014) used a grandparental measure. Most of these studies examined maternal childhood adversity (n = 11, 92%) except one (8%; Lê-Scherban et al., 2014) that measured educational attainment, an indicator of socioeconomic status. Of the 11 studies that assessed childhood adversity, five (45%) utilized the Childhood Trauma Questionnaire (Fauble, 2009; Min et al., 2013; Powers et al., 2020; Russotti et al., 2021; van de Ven et al., 2020; Warmingham et al., 2020), and three (27%) used the ACEs survey (Esteves et al., 2017; Glackin & Gray 2018; Hatch et al., 2020; Haynes, 2019; Pear et al., 2017; Pickett et al., 2018). One study (9%) examined maternal childhood loss (e.g., death of a family member), negative relationships with parents (e.g., abusive), family problems (e.g., domestic violence), sexual abuse, and instability of care (Leifer et al., 1993; Paredes et al., 2001). The remaining two studies (18%) that measured childhood adversity examined maternal history of sexual or physical abuse and childhood stress (e.g., poverty), respectively (Dubowitz et al., 2001; Hipwell et al., 2019). In the only study that included NAs, a grandparental measure of relocation experience (an indicator of historical trauma) was utilized (Walls & Whitbeck, 2012).
Offspring Mental Health
Half of the 12 studies that included AAs (50%) measured mental health when offspring were aged between 3 and 17 years (Dubowitz et al., 2001; Esteves et al., 2017; Glackin & Gray 2018; Hatch et al., 2020; Haynes, 2019; Leifer et al., 1993; Min et al., 2013; Paredes et al., 2001; Pickett et al., 2018; Russotti et al., 2021; Warmingham et al., 2020). Four studies (33%) did not provide offspring ages or merely provided an average age for the sample (Fauble, 2009; Pear et al., 2017; Powers et al., 2020; van de Ven et al., 2020). One study (8%) measured outcomes when offspring were between 3 and 9 months old (Hipwell et al., 2019), and in another study (8%), offspring age ranged from 25 to 59 years (Lê-Scherban et al., 2014). The single study of NAs assessed mental health when offspring were aged between 10 and 12 years. For clarity, we describe below the specific mental health outcomes reported in each study in greater detail. Note that a few studies assessed several different outcomes (Dubowitz et al., 2001; Leifer et al., 1993; Paredes et al., 2001; Powers et al., 2020).
Of the 12 studies that included AAs, seven (58%) assessed offspring behavior problems using the Child Behavior Checklist (Dubowitz et al., 2001; Esteves et al., 2017; Fauble, 2009; Glackin & Gray 2018; Hatch et al., 2020; Leifer et al., 1993; Min et al., 2013; Paredes et al., 2001; Pickett et al., 2018; Russotti et al., 2021; van de Ven et al., 2020; Warmingham et al., 2020). Three studies (25%) measured emotional reactivity/regulation (Hipwell et al., 2019; Powers et al., 2020; Russotti et al., 2021; Warmingham et al., 2020), two (17%) measured cognitive/ego functioning (Dubowitz et al., 2001; Leifer et al., 1993; Paredes et al., 2001), and two (17%) measured cigarette smoking (i.e., substance abuse; Lê-Scherban et al., 2014; Pear et al., 2017).
In addition, one study (8%) assessed offspring feelings related to school and friends, fears and worries, and age-inappropriate sexual behaviors (Leifer et al., 1993; Paredes et al., 2001), one (8%) assessed PTSD (Powers et al., 2020), and one study (8%) assessed depression and/or anxiety (Haynes, 2019). In the single study including NAs, offspring depression and delinquency were assessed using the Center for Epidemiological Studies Depression Scale and items from the conduct disorder module of the Diagnostic Interview Schedule for Children—Revised, respectively (Walls & Whitbeck, 2012).
Parental Adversity and Offspring Mental Health
Studies With Fully AA or NA Samples
Four (31%) of the 13 studies reviewed used fully AA or NA samples. Three studies demonstrated a significant association between parental preconception adversity and offspring mental health. Specifically, the first study found that maternal ACEs were related to more overall offspring behavior problems among AAs, controlling for offspring exposure to adversity (Esteves et al., 2017; Glackin & Gray, 2018). This study also showed that offspring had more total behavior problems when their mothers experienced more ACEs in the context of low family social support (Hatch et al., 2020) or when their mothers experienced fewer ACEs but valued aggression (Pickett et al., 2018). Maternal psychopathology also mediated the maternal ACEs-offspring behavior problem association in this study (Glackin & Gray, 2018). The second study found that maternal childhood adversities were associated with fewer positive experiences at school/with friends and more overall offspring behavior problems among AAs (Leifer et al., 1993; Paredes et al., 2001). The third study demonstrated a positive association between forced grandparental relocation and grandchildren’s delinquency and depression among NAs through increased grandparental alcohol problems, increased maternal substance use and depression, and decreased maternal warmth and supportiveness toward their offspring (87% resided in the United States, Walls & Whitbeck, 2012).
Two studies also reported a nonsignificant association between parental preconception adversity and different offspring mental health indices. Specifically, Powers et al. (2020) reported that maternal childhood adversities were not associated with offspring emotional regulation and PTSD, while Leifer et al. (1993) reported that maternal childhood adversities were not associated with offspring cognitive/ego functioning and age-inappropriate sexual behaviors. To summarize, three studies reported a significant association between parental preconception adversity and offspring mental health (two studies used a fully AA sample and one study used a fully NA sample) and two studies reported a nonsignificant association among AAs. Note that one of the four studies reported significant links with some offspring outcomes and nonsignificant links with different offspring outcomes in a fully AA sample.
Studies With Partial AA Samples That Tested for Ethnic/Racial Differences
Three (23%) of the 13 studies tested for ethnic/racial differences using multi-ethnic/racial samples. In two studies, there was a significant link between parental preconception adversity and offspring mental health. Particularly, Haynes (2019) found that maternal ACEs were associated with significantly increased odds of offspring depression and/or anxiety, and Pear et al. (2017) reported that maternal childhood adversities were positively associated with offspring risk of cigarette smoking before age 18. However, neither study found ethnic/racial differences in these findings. Another study reported that grandparental educational attainment was not associated with grandchildren’s current cigarette smoking for AAs and WAs, controlling for grandchildren’s own educational attainment (Lê-Scherban et al., 2014). In summary, two studies reported that parental preconception adversity was associated with offspring mental health in multi-ethnic/racial samples including AAs, while the third did not. However, none of the studies documented ethnic/racial differences in their findings.
Studies With Partial (≥70%) AA Samples That Did Not Test for Ethnic/Racial Differences
Six (46%) of the 13 studies examined the parental preconception adversity and offspring mental health association in multi-ethnic/racial samples that were ≥70% AA without testing for racial/ethnic differences. All six of these studies found that parental preconception adversity was significantly related to offspring mental health. One study reported that maternal childhood maltreatment significantly predicted more overall offspring behavior problems and emotion dysregulation through increased maternal depressive symptoms and offspring experiences of maltreatment (Russotti et al., 2021; Warmingham et al., 2020). Three of the six studies reported a significant link between maternal childhood adversities and overall offspring behavior problems (Fauble, 2009; Min et al., 2013; van de Ven et al., 2020). Min et al. (2013) also found that maternal psychological distress and perceived social support mediated this association, while van de Ven et al. (2020) discovered that offspring frontal alpha symmetry moderated the association such that the association between maternal childhood adversity and child behavior problems was significantly stronger among children with more right frontal activity (vs. children with more left frontal activity).
One study reported that maternal exposure to emotional neglect predicted more negative emotional reactivity in offspring, while maternal exposure to emotional abuse predicted less negative emotional reactivity in offspring (Hipwell et al., 2019). The final study reported a significant association between maternal childhood adversities and total offspring behavior problems and a nonsignificant association between maternal childhood adversities and offspring cognitive functioning (Dubowitz et al., 2001). Thus, all six studies that used multi-ethnic/racial samples (≥70% AA) without testing for racial/ethnic differences found a significant association between parental preconception adversity and offspring mental health. Note that one of these six studies reported a significant association with one offspring outcome and a nonsignificant association with a different offspring outcome.
Quality Assessment
Risk of bias (ROB) was moderate or high in 11 (92%) of the 12 studies that included AAs see Supplemental Appendix D). This was because these studies included non-representative samples (n = 8, 67%), no information about or inadequate participant response/follow-up rate (n = 10, 83%), retrospective measures of parental preconception adversity (n = 11, 92%), no adjustment for important potential confounders (n = 3, 25%), small samples (n = 3, 25%), and/or non-validated outcome measures (n = 2, 17%). The lone study that included NAs had a moderate ROB due to its non-representative sample and use of a retrospective measure of parental preconception adversity. To summarize, most (n = 12, 92%) of the 13 included studies are limited by their moderate or high ROB.
Discussion
This review examined whether parental preconception adversity was significantly associated with offspring mental health in AAs and NAs in the United States. Of the 13 independent studies included, nine studies (69%) reported that AA or NA parents with more adversity exposure were significantly more likely to have offspring with mental health problems compared to AA or NA parents with less adversity exposure (Fauble, 2009; Hatch et al., 2020; Haynes, 2019; Esteves et al., 2017; Glackin & Gray, 2018; Hipwell et al., 2019; Min et al., 2013; Pear et al., 2017; Pickett et al., 2018; Russotti et al., 2021; van de Ven et al., 2020; Walls & Whitbeck, 2012; Warmingham et al., 2020), two studies (15%) reported that AA parents with more adversity exposure were no more likely than AA parents with less adversity exposure to have offspring with mental health problems (Lê-Scherban et al., 2014; Powers et al., 2020), and two studies (15%) reported both significant and non-significant associations between these variables among AAs (Dubowitz et al., 2001; Leifer et al., 1993; Paredes et al., 2001; see Table 1). Importantly, none of the three studies (23%) that tested for ethnic/racial disparities in their results found a stronger association between parental adversity and offspring mental health for AAs relative to WAs (Haynes, 2019; Lê-Scherban et al., 2014; Pear et al., 2017).
This review provided no evidence that intergenerational transmission of adversity may help explain contemporary ethnic/racial mental health disparities among AAs or NAs when compared to WAs. However, the number of studies addressing these findings directly is quite small (n = 3, 23%) and the studies are significantly limited (e.g., single-item, non-validated measures, Haynes, 2019; Lê-Scherban et al., 2014; Pear et al., 2017). In addition, only one of 13 studies (8%) assessed an ethnicity/race-related adversity (historical/racial trauma; Walls & Whitbeck, 2012). This is an important oversight because AAs and NAs disproportionately experience these adversities and this type of parental adversity may have a stronger link to offspring mental health, contributing to contemporary mental health disparities (Conching & Thayer, 2019; Sotero, 2006). Similarly, few studies (n = 5, 38%) examined offspring mental health outcomes known to disproportionately affect AAs or NAs, including depression, substance abuse, and PTSD (Haynes, 2019; Lê-Scherban et al., 2014; Pear et al., 2017; Powers et al., 2020; Walls & Whitbeck, 2012). These outcomes may be more likely to show stronger associations with parental preconception adversity among AAs and NAs. Nonetheless, this review implies that there is an equally strong link between parental adversity and offspring mental health across ethnic/racial groups.
That said, our findings suggest that parental preconception adversity may negatively affect offspring mental health among AAs and NAs in the United States. This is consistent with prior literature examining the relationship between parental exposure to historical trauma and offspring mental health among Canadian First Nations and Jewish populations (Bombay et al., 2014; Dashorst et al., 2019). The results are also consistent with studies investigating the link between parental childhood adversities and offspring mental health using multi-ethnic/racial samples that included fewer than 70% AA or NA (Condon et al., 2019; Cooke et al., 2021; Esteves et al., 2020; Gissandaner et al., 2021; Jones, 2019; Plant et al., 2018; Saunders, 2019; Thompson, 2007; Wurster et al., 2020). These studies did not test for ethnic/racial differences in their results and thus were not eligible for inclusion in this review. That several relevant studies have discovered similar trends in the relationship between parental preconception adversity and offspring mental health lends credibility to the results of the current review and suggests that intergenerational transmission of adversity is common across ethnic/racial groups. However, the studies reviewed possessed some important limitations.
Limitations of the Literature
The generalizability of these findings is limited as just four studies (31%) used representative samples (Haynes, 2019; Hipwell et al., 2019; Lê-Scherban et al., 2014; Pear et al., 2017). Convenience samples are not representative of the population to which authors seek to generalize and the inherent selection bias in these samples vastly increases the likelihood that unmeasured characteristics will confound studies’ results. Furthermore, only three studies (23%) provided adequate participant response/follow-up rates (Hipwell et al., 2019; Lê-Scherban et al., 2014; Walls & Whitbeck, 2012). Attrition, particularly selective attrition, can render samples less representative as research respondents may differ from non-respondents in ways that are confounded with the variables of interest. Thus, not reporting response/follow-up rates or obtaining inadequate follow-up rates makes it impossible to determine the validity of a study’s findings, thereby lowering our confidence in the accuracy of the findings and their generalizability.
Twelve of the 13 studies reviewed (92%) employed a retrospective report of parental preconception adversity. Retrospective reports rely on participants’ fallible memories that may bias results through under- or overreporting of adversities (Widom, 2019). Results may also be biased by the measures through which parental preconception adversities were sometimes examined. For example, the ACEs survey, which was used in three studies (23%) does not assess the frequency, intensity, timing, or chronicity of exposure to the limited number of adversities specified (McLennan et al., 2020). This could cause under- or overestimation of the relation between ACEs and mental health outcomes because the ACEs reported are not necessarily equivalent. In all, 11 studies (85%) assessed preconception adversity only in the mother, potentially introducing a gender bias that highlights maternal preconception adversities but ignores those of the father and other parental figures. That is, studies provided no reliable information about the potential intergenerational impact of paternal, grandparental, or nonbiological parental (e.g., stepparents, adopted parents) preconception adversity.
Four studies (31%) used parental reports of offspring mental health, introducing another source of bias (Esteves et al., 2017; Fauble, 2009; Glackin & Gray, 2018; Hatch et al., 2020; Haynes, 2019; Pickett et al., 2018; van de Ven et al., 2020), as parental reports may be imprecise due to social desirability biases and overestimation or lack of knowledge about offspring mental well-being. These reports also methodologically confound the parental adversity assessment with the offspring’s health outcome. Parental reports of offspring mental health were likely common in this literature because offspring were under 18 years of age in all but one study (Lê-Scherban et al., 2014). The studies’ almost exclusive inclusion of non-adult offspring also limits our knowledge of the long-term mental health impact of parental preconception adversity on offspring among AAs and NAs.
Importantly, few studies (n = 3, 23%) accounted for the offspring’s own exposure to adversity (Esteves et al., 2017; Glackin & Gray, 2018; Hatch et al., 2020; Lê-Scherban et al., 2014; Pickett et al., 2018; Russotti et al., 2021; Warmingham et al., 2020), and only six studies (46%) tested mechanisms of transmission in the association between parental preconception adversity and offspring mental health (Esteves et al., 2017; Fauble, 2009; Glackin & Gray, 2018; Hatch et al., 2020; Min et al., 2013; Pickett et al., 2018; Russotti et al., 2021; van de Ven et al., 2020; Walls & Whitbeck, 2012; Warmingham et al., 2020). Given that children’s own experiences of adversity may affect their mental health (Kerker et al., 2015), and that parental adversity may increase the risk of offspring adversity exposure (Negriff et al., 2020), it is vital that studies of the intergenerational transmission of adversity account for these factors. Moreover, merely examining the direct relation between parental preconception adversity and offspring mental health does not tell us how these associations occur, making it harder to identify appropriate intervention targets.
A final critical limitation of the current review is the small number of independent studies included (n = 13), many of which used multi-ethnic/racial samples without testing for ethnic/racial differences (n = 6, 46%). Also, just one study used a sample of NAs. The fact that only seven studies reported results specific to AAs or NAs (54%) separate from other ethnic/racial groups makes it more difficult to draw robust conclusions about the link between parental preconception adversity and offspring mental health in AAs and NAs (see Table 1). However, the six studies (46%) with multi-ethnic/racial samples that did not test for ethnic/racial differences included samples that were ≥70% AA (see Table 1), improving our confidence that the results of these studies apply to the AAs in the samples. However, without testing for racial/ethnic differences we cannot know if these findings are unique to the AA population and a potential explanation for the mental health disparities between AAs and WAs. Stronger conclusions about the impact of parental preconception adversity on offspring mental health among AAs and NAs and its contribution to health disparities in the United States will require much more rigorous research.
Future Directions
Future research should be devoted to investigating the relation between parental preconception adversity and offspring mental health outcomes using fully AA and NA samples to examine the mechanisms by which parental adversity may affect offspring outcomes. Researchers should endeavor to recruit these samples via probability sampling (noting response rates) and obtain enough participants to afford their studies adequate power. When multi-ethnic/racial samples are used, researchers should test for ethnic/racial disparities in their findings to examine whether the findings reflect health disparities between WAs and AAs or NAs in the sample. The challenge of relying on retrospective recall of parental preconception adversities may also be addressed if participants are identified early in life before conception (e.g., childhood) and followed longitudinally for multiple generations (while mitigating high attrition). These longitudinal studies should follow participants’ offspring into adulthood to ensure that they will be able to report on their own mental health and to document the potential long-term consequences of parental preconception adversity on subsequent generations’ mental health. This ability to self-report would also be possible in correlational studies that recruit parent–child dyads with adult offspring. However, if researchers must use retrospective measures of parental preconception adversities, they should utilize psychometrically validated measures that assess frequency, intensity, timing, or chronicity of exposure to a representative, systematically derived list of adversities. These could be newly developed measures or an expanded version of longstanding measures like the ACEs survey (McLennan et al., 2020).
Scholars should assess a broader range of parental preconception adversities (e.g., father, grandparent) in future research. Paternal adversity may have a unique impact on the offspring mental health different from that of the mother’s adversity and it may interact with maternal adversity to affect offspring’s well-being (Lee et al., 2013). Similarly, exploring dyads separated by two or more generations could demonstrate the scale of the impact that adversities suffered by one’s ancestors may have on one’s mental health many generations later (Brave Heart, 2003; Sotero, 2006). Investigating the link between parental preconception adversity and offspring mental health in non-biological dyads (e.g., step and adopted families) may also suggest socio-environmental pathways of trauma transmission such as parental perceived social support and offspring’s own exposure to adversities (Min et al., 2013; Sotero, 2006). The latter is an especially important factor that must be accounted for in future research, given that one’s own experiences of adversity may impact one’s mental health in addition to or beyond parental adversity exposure and may partially or fully explain the association between parental preconception adversity and offspring mental health (Kerker et al., 2015; Negriff et al., 2020; Russotti et al., 2021; Warmingham et al., 2020). Other mechanisms of transmission, especially biological pathways such as epigenetics, should also be explored in future studies (Conching & Thayer, 2019).
Future research should assess ethnicity/race-related adversities (e.g., ethnic/racial discrimination) among AAs, NAs, and WAs and compare the strength of the association between these adversities and offspring mental health across ethnic/racial groups. Researchers should also assess offspring mental health outcomes known to disproportionately affect AAs and NAs (e.g., depression, PTSD, Emerson et al., 2017; Williams et al., 2007) and compare the strength of the link between various parental adversities and these outcomes across ethnic/racial groups (AAs and NAs vs. WAs). These methodological practices may help reveal disparities in the strength of the link between parental preconception adversities and offspring mental health that may be specific to different racial/ethnic groups (Conching & Thayer, 2019; Sotero, 2006). Subsequent research that addresses these issues will facilitate the production of a more cohesive and rigorous body of literature on the link between parental preconception adversity and offspring mental health among AAs and NAs in the United States and provide a clearer picture of its contribution to health disparities.
Implications
Our findings indicate a need for the future development of a more unified body of literature on this topic that could have important implications for intervention and policy (see Table 2). We have shown that parental preconception adversity may place offspring at risk for mental health challenges among AAs and NAs (as well as other ethnic/racial groups), suggesting that providing treatment and instrumental support to multiple generations may prove beneficial for AA and NA families (Benzies et al., 2011). Moreover, the identification of pathways linking parental preconception adversity with offspring mental health could elucidate important factors (e.g., social support, Hatch et al., 2020; Min et al., 2013) on which to intervene for AAs and NAs. As exposure to adversity may have mental health effects across generations in AAs and NAs, policies are needed to address these populations’ disproportionate risk for such exposures by targeting structural inequalities such as poverty, residential segregation, unemployment, low-quality schools, etc. (Thoits, 2010). Moreover, given the association between mental and physical health (Wang et al., 2020), addressing the mental health impacts of these exposures may also help reduce stress-related physical health ailments. Decreasing AAs’ and NAs’ risk for preconception adversity exposure may thus curtail excessive healthcare costs in the United States, improve these populations’ quality of life, and in so doing, promote their many contributions to society, both for the contemporary generation and potentially for generations to come.
Review’s Implications for Research, Practice, and Policy.
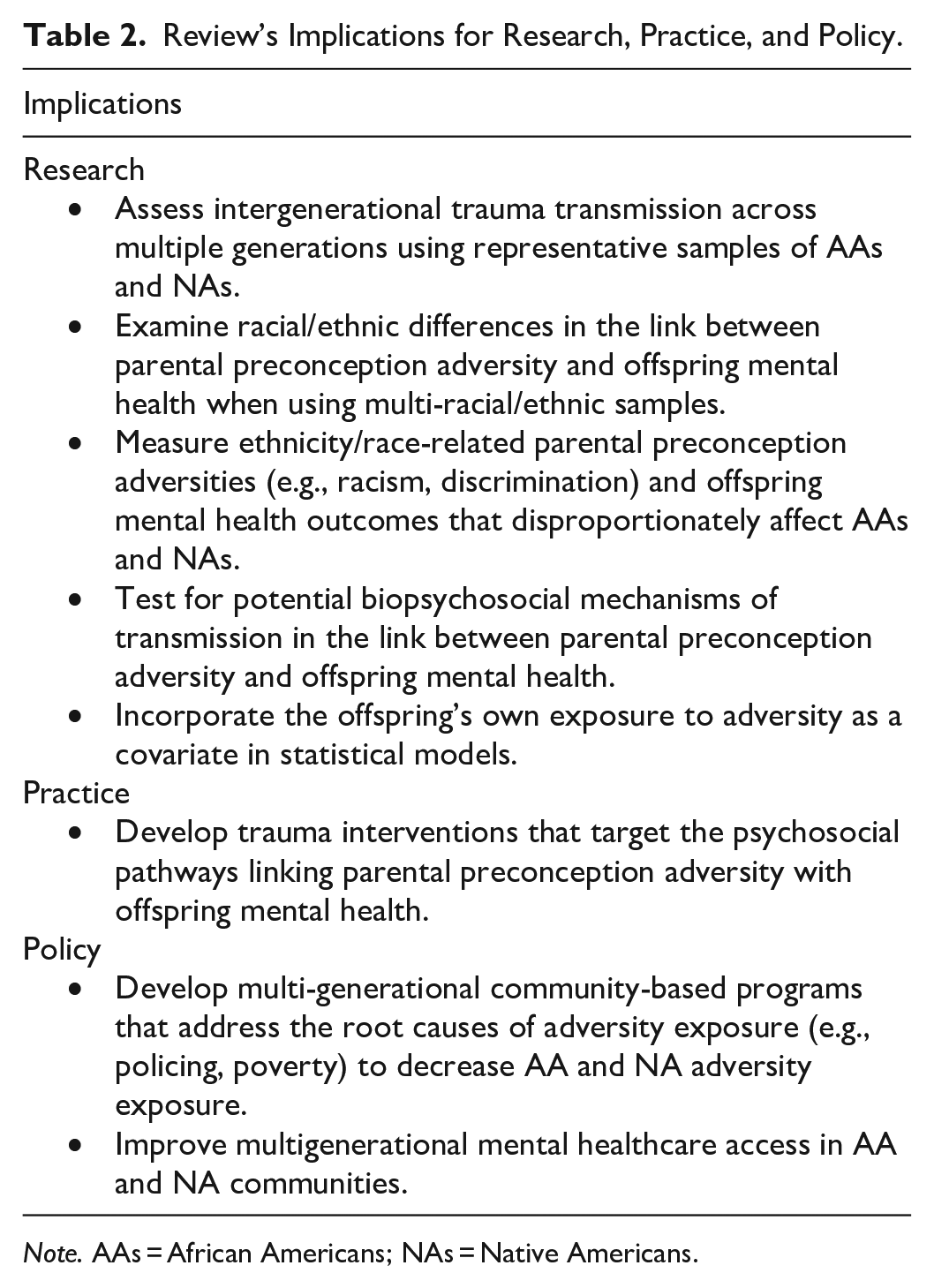
Note. AAs = African Americans; NAs = Native Americans.
Conclusion
The current review suggests that parental preconception adversity is associated with worse offspring mental health among AAs and NAs in the United States, but that this association is not unique to AAs or NAs (see Table 3). Several mechanisms of transmission were implicated in this association. Nonetheless, additional rigorous research is required to confidently verify whether the association between parental preconception adversity and offspring mental health is stronger in AAs and NAs and elucidate how this association may contribute to contemporary ethnic/racial mental health disparities in the United States. Such a body of knowledge would advance the development of novel targeted interventions, such as multi-generational mental health interventions as well as social policies to improve AAs’ and NAs’ quality of life.
Summary of Review’s Critical Findings.
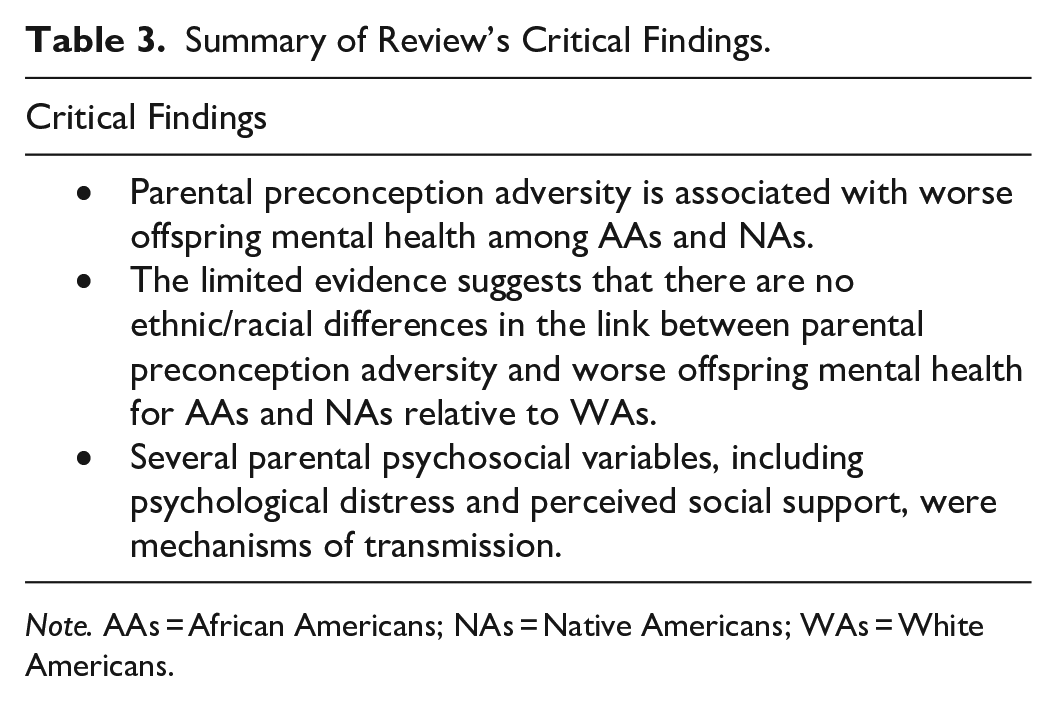
Note. AAs = African Americans; NAs = Native Americans; WAs = White Americans.
Supplemental Material
sj-docx-1-tva-10.1177_15248380231200464 – Supplemental material for Parental Preconception Adversity and Offspring Mental Health in African Americans and Native Americans in the United States: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380231200464 for Parental Preconception Adversity and Offspring Mental Health in African Americans and Native Americans in the United States: A Systematic Review by Adebisi A. Akinyemi, Adrianna Jones, Josiah A. Sweeting and E. Alison Holman in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We thank UCI research librarians Nicole Carpenter, Steve Clancy, and Linda Suk-Ling Murphy as well as Dr. Joss Brosschot and Dr. Julian Thayer for guidance in systematic search practices. Dr. Sweeting now works for Asha ABA, LLC and the State Bar of California.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded in part by the National Science Foundation Graduate Research Fellowship Program under Grant DGE-1839285 to Ms. Adebisi Akinyemi, and the University of California, Irvine Graduate Division Eugene Cota Robles Fellowship to Mr. Josiah Sweeting. Any opinions, findings, and conclusions or recommendations are those of the authors and do not necessarily reflect the views of the National Science Foundation.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.