
Abstract
Children of mothers with childhood trauma are at an increased risk for mental health problems, yet the most influential family-related mediators of this intergenerational transmission remain unclear. This systematic review and meta-analysis synthesized effect sizes from 29 studies (n = 352,279 dyads) examining psychosocial family-level mediators between maternal childhood trauma and child mental health. We identified 380 simple and 40 serial mediation paths across four domains: child characteristics, maternal characteristics, parent–child relationship factors, and household characteristics. Maternal characteristics showed the largest pooled effects (proportion median [PM]: 31.2%; ratio median [RM]: 0.21), particularly maternal mental health (PM: 36.0%), maternal attachment style (PM: 27.2%), and maternal social support (PM: 27.2%). Our findings highlight the potential central role of maternal factors in the intergenerational transmission of trauma. Interventions that bolster maternal mental health and social support would be most impactful in disrupting the intergenerational transmission of trauma, though further research is needed.
Keywords
Introduction
Intergenerational trauma is the process by which the psychological impact of a traumatic event may be transmitted from one generation to the next, resulting in subsequent generations experiencing the psychological effects of a traumatic event without direct exposure to it (Bowers & Yehuda, 2016; Yehuda & Lehrner, 2018). The intergenerational transmission of trauma has been examined across various trauma contexts (Bowers & Yehuda, 2016; Morris et al., 2012; van Steenwyk et al., 2018), yielding mixed results (Lindert et al., 2017; Sagi-Schwartz et al., 2008; van IJzendoorn et al., 2003). These mixed findings could be due in part to variation in the timing of parental trauma exposure. Some evidence suggests that, compared to trauma experienced during adulthood, parental trauma experienced in childhood, especially before the onset of puberty, could be associated with more robust transmission across generations (Thompson, 2007; Yehuda & Lehrner, 2018).
In particular, consistent findings of intergenerational transmission from parental childhood exposures have been documented from trauma resulting from adverse childhood experiences (ACEs), including childhood maltreatment (distinct, yet overlapping, concepts; Garrison et al., 2022). ACEs are defined as “potentially traumatic events that occur in childhood … [and] undermine sense of safety, stability, and bonding” (Centers for Disease Control and Prevention, 2024) and includes childhood maltreatment, defined as exposures resulting in “actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust, or power” (World Health Organization, 2022). Two recent meta-analyses reported small, but statistically significant, effects of maternal ACEs on offspring’s externalizing and internalizing behaviors (Loheide-Niesmann et al., 2022; Su et al., 2020).
Given this established association, researchers have called for the development of interventions to prevent the harmful psychological effects of maternal childhood trauma passing to the next generation (Su et al., 2020); however, to best inform intervention development, there is a need to quantify the effect sizes of causal processes underpinning transmission. Although mechanisms remain unclear, literature has identified evidence to support biological factors including genetic or epigenetic mechanisms (Bowers & Yehuda, 2016; Yehuda & Lehrner, 2018) as well as psychosocial mechanisms (Bowers & Yehuda, 2016), which are promising for intervention as they are likely more modifiable than genetic or biological factors. Multiple psychosocial factors within the household likely contribute to the intergenerational transmission of trauma (Cerdeña et al., 2021; Dashorst et al., 2019; Flanagan et al., 2020; Isobel et al., 2019) – for instance, maternal experience of childhood trauma may impact the household environment, such as parenting abilities, parental mental health, or parent-child attachment mechanisms (Cerdeña et al., 2021; Flanagan et al., 2020; Isobel et al., 2019), and, in turn, these family-level factors may impact child development (Su et al., 2020).
To our knowledge, there have been three efforts to synthesize the literature on psychosocial mediators in the intergenerational transmission of maternal childhood trauma. Loheide-Niesmann et al. (2022) and Plant (2016) provided narrative syntheses of mediators from 23 and 10 studies, respectively, examining the impact on child externalizing behaviors; however, the effect estimates were not quantitatively synthesized, leaving the relative contributions of individual mediators unclear. The third review (Ma et al., 2022) included 41 studies on maternal experiences of childhood adversity mediators on child emotional and behavioral problems – the vast majority of which were household factors – but the authors were only able to perform mediation meta-analyses on three constructs (maternal depression, negative parenting practices, and maternal insecure attachment), due to data heterogeneity (Ma et al., 2022). Of these three constructs, maternal depression and maternal insecure attachment identified statistically significant pooled effects (pooled indirect standardized effects of 0.10 and 0.07, respectively), whereas negative parenting practices were not a significant mediator (pooled indirect standardized effect of 0.01; Ma et al., 2022). Collectively, these reviews identified a wide range of mediators for the intergenerational transmission of maternal childhood trauma, and the mediators with the strongest support were those operating within the household (or at the family-level, used interchangeably throughout). This evidence base also suggests that psychosocial factors operating at the family-level would be most influential in mediating the intergenerational transmission of trauma. These included parenting practices, child maltreatment, maternal attachment styles, maternal relationships and social support, among others (Loheide-Niesmann et al., 2022; Ma et al., 2022; Plant et al., 2017).
By synthesizing findings across the literature, these three reviews have provided important insights for intervention development; however, they share five key limitations. First, given that one of these reviews found evidence of publication bias (Loheide-Niesmann et al., 2022), it is possible that the narrative syntheses and meta-analyses are biased (especially given the small number of studies in the meta-analytic sample; Loheide-Niesmann et al., 2022). Second, given the large amount of heterogeneity across mediators, only one review was able to meta-analyze mediation effects and only synthesized three constructs from nine paths (Ma et al., 2022). Third, there are likely multiple, complex pathways involved in the relationship between maternal childhood trauma and child psychopathology, and there is a need to assess complex, multilevel-mediator models (such as serial and other complex paths; Loheide-Niesmann et al., 2022; Ma et al., 2022). Fourth, no review has explored mediators acting through three-generation transmission – which could be another important transmission path (Sagi-Schwartz et al., 2008). Last, the reviews primarily relied on results that were adjusted for covariates. Though in theory adjusted analyses are advantageous by allowing for the adjustment of confounding variables, they would unlikely be uniformly performed and could bias estimates further away from true effects. For example, an adjusted approach might inadvertently adjust for other mediators (blocking effects) or collider variables (i.e., variables on the causal pathway that are common effects of both the exposure and outcome, which would bias estimates; Ananth & Brandt, 2022).
Understanding the role of family psychosocial factors in mediating the intergenerational transmission of maternal childhood trauma is critical to develop household-level psychosocial interventions and disrupt transmission. This systematic review and descriptive meta-analysis aimed to fill knowledge gaps by extracting simple and serial mediation paths that assessed family-level psychosocial mediators in the intergenerational transmission of maternal trauma across two- and three-generations. The primary goal of this review was to quantitatively assess, pool, and rank the effect sizes of a wide variety of family-level mediators in the intergenerational transmission of maternal childhood trauma with the intention to identify which mediators are most influential in transmission to determine which household-level psychosocial factors should be prioritized in intervention development. This review used broad eligibility and search strategies to include a variety of data sources and paths to reduce publication bias. We employed a descriptive meta-analytic strategy of pooled effect measures to include a large sample of paths in our analyses, relying mostly on unadjusted paths to further decrease risk of bias.
Methods
This meta-analysis of pooled effect measures is part of a larger systematic review, for which the protocol and search strategy have been published (Mew et al., 2022). Minor deviations to the protocol were made for feasibility, as summarized in eTable 1. We followed guidelines from the Joanna Briggs Institute (JBI) Manual for Evidence Synthesis (Aromataris & Munn, 2020), the Cochrane Handbook for Systematic Reviews (Higgins et al., 2019), and PRISMA 2020 reporting guidelines (Page et al., 2021; eTable 2), where possible.
Eligibility Criteria
This review had no date restrictions, but was limited to studies published in English, French, Kinyarwanda, and Spanish (selected as team members spoke these languages). We included peer-reviewed literature, doctoral dissertations, and conference abstracts to mitigate publication bias. We included original epidemiological research studies, which includes cross-sectional and cohort studies, and intervention designs if measures were assessed at baseline, to not confound the effect of the intervention on the outcome. Systematic review papers, meta-analyses, case-studies, qualitative studies, and study protocols were excluded.
The present review included studies with dyads with at least one primary female caregiver (‘mothers’) who experienced a traumatic event in her childhood (before 18 years) and her child. Though we collected data on fathers in the larger review, we focused on mothers’ childhood trauma to be consistent with prior evidence syntheses, and because of the small number of identified studies that examined father’s childhood trauma. We also included studies of caregiver-grandchild dyads (however, as no studies identified three-generation dyads, we will use the term ‘child’ henceforth). We included broad measures of adverse childhood experiences including experiences of abuse, neglect, and other forms of childhood maltreatment. Studies had to include at least one path that represented a psychosocial factor operating at the family-level (including household- and caregiver-levels). These included factors related to the interpersonal relationship between caregiver and child (e.g., parenting style, attachment) or to the family context more broadly (e.g., family conflict), measured in reference to the time before the child reached 18 years of age.
Studies included quantitatively measured markers of psychological symptoms or functioning (i.e., psychopathology and/or indicators of wellbeing) in the child. We included paths that measured outcomes among children at least four years of age. Though previous reviews did not apply a lower-limit age restriction (Loheide-Niesmann et al., 2022; Ma et al., 2022; Plant et al., 2017), we felt this was appropriate given that the psychological symptoms linked to maternal childhood trauma would most likely, at the earliest, present in children as young as four years (Mar et al., 2023). For example, one meta-analysis showed that the peak age of onset of anxiety/fear-related disorders was 5.5 years (Solmi et al., 2022) and that conduct disorders can be diagnosed in children at four years of age (Mar et al., 2023). We also selected a four year age cut-off to align with the original Child Behavior Checklist (CBCL) instrument developed for children ages four and older (Achenbach, 1991; Mazefsky et al., 2011) as this was often used in seminal studies including the Avon Longitudinal Study of Parents and Children (Chen et al., 2024; O'Donnell et al., 2014; Thompson, 2007). Outcomes were eligible regardless of assessor (for example, child–, caregiver–, clinician– or teacher–reported outcomes were included).
Eligible studies provided sufficient data to evaluate direct and indirect effects from maternal childhood trauma (exposure – or, the independent variable) to child mental health (outcome – or, the dependent variable) via a family-level psychosocial factor (mediator). We included simple or serial mediation paths that explicitly tested for mediation (e.g., via a Sobel test or bootstrapping). We included any statistical method used to evaluate mediation to mitigate publication bias. So, for example, we included studies that assessed mediation using mediation analyses, indirect effects analyses, Baron and Kenny, or structural equation modeling, among others. In addition, we included simple paths that provided mediating path beta estimates from regression models, regardless of whether they tested for mediation or instead reported enough statistical data for our team to back-calculate effect measures, as described below.
Search Strategy and Screening Procedures
The search strategy was developed and reviewed by two medical research librarians. We searched MEDLINE (via Ovid), PsycINFO (via Ovid), PTSDpubs, Scopus (conference papers only), and ProQuest Dissertations and Theses (doctoral dissertations only) in 2021. We used a combination of keywords and controlled vocabulary terms (where available) to identify potentially relevant documents that addressed three concepts: intergenerational relationships, family setting, and intergenerational trauma (eTables 3–7). Title/abstract and full-text screening was performed independently by two reviewers using Covidence software (Covidence software, nd). Our team consisted of eight title/abstract reviewers. We held piloting and training procedures for reviewers before screening. We held two training set rounds of n = 25 records, ultimately yielding a team agreement of 84% (Fleiss Kappa score of 0.76, corresponding to substantial agreement; Hartling et al., 2012; Landis & Koch, 1977). The first author screened every title/abstract record. To accommodate an unexpectedly high yield of papers, our full-text screening team consisted of eleven reviewers. We achieved agreement scores of 80% and 70% (or, Fleiss Kappa scores of 0.71 and 0.78, respectively, corresponding to substantial agreement; Hartling et al., 2012; Landis & Koch, 1977) across two separate training teams to accommodate scheduling conflicts. A more highly trained team member in epidemiology and biostatistics reviewed each full-text record during the full-text screening stage. Senior team members (EM, RH, JB, SL) resolved conflicts when needed.
Data Extraction and Merging of Constructs
We used Research Electronic Data Capture (REDCAP; Vanderbilt University, 2021) software to extract data from included studies. Before extraction, a team of five coauthors piloted eight full-text papers to modify question wording and/or resolve technical issues. A single reviewer performed data extraction for each paper; quality assurance checks were completed on 5% of the articles by either the first or senior authors. Discrepancies were resolved through discussion between the first and senior authors.
Data extraction utilized two REDCAP forms: one applied at the study level, and the other at the path level to accommodate instances where more than one mediation path was reported in a single study. At the study-level, we collected information on study design, authors, statistical analyses, and serial mediation. The majority of information was extracted at the path-level, including details on the exposure, mediator, and outcome variables, and other statistical information. As part of our data extraction process, we assessed the quality of mediation paths using the Lee et al. (2015) tool used in mediation meta-analyses; however, we removed one item (“Did the study control for confounding factors?”) since adjusting for confounding may lead to additional biases when summarizing effect sizes across variables, leaving our quality scores out of six, rather than seven, items.
Before analyses, we combined results of individual “articles” (=a) reporting on the same underlying dataset, or “study” (=s), and used this consolidated information in our analyses. Given that there was often duplicate information between articles corresponding to the same underlying dataset, we developed additional criteria to prioritize which data to extract. We took a case-by-case approach to prioritize paths first from peer-reviewed studies before dissertations. In instances where similar paths came from different articles of the same publication type, we prioritized paths from the largest sample sizes. If the sample size was the same, we prioritized unadjusted standardized betas over other reported statistics (additional criteria in eTable 8). The first and senior authors grouped the mediators into thematic concepts based on high or sufficient conceptual overlap (as reported elsewhere in Domhardt et al., 2021) through discussion.
Data Analysis
We conducted a descriptive meta-analysis of pooled effect measures across simple paths, wherein effect measures were pooled and ranked across paths and studies – aligned with the Glass meta-analytic technique (Glass, 1976). Data analyses were conducted using SAS statistical software version 9.4 (SAS institute inc., 2023). We did not pool effect measures between serial mediation paths. We were unable to conduct traditional meta-analytic methods due to small cell sizes from the heterogeneity in the mediating and outcome constructs. To be included in the pooled analysis, paths needed to report enough statistical information to back-calculate effect size estimates. Specifically, paths needed to report at least two of the three standardized beta estimates for the indirect, direct, and/or total effects, or other information through correlation matrices, means, and standard deviations. We had planned to flip signs for consistent valence; however, this was unnecessary, given that all exposure variables, outcome variables, and mediator variables within the same construct had consistent valences. Using this information, when possible, we back-calculated two measures of effect for each simple path: (1) proportion effect sizes, calculated by dividing the standardized beta estimate for the indirect effect over the standardized beta estimate for the total effect; and (2) the ratio effect sizes, calculated by dividing the beta estimate for the indirect effect over the beta estimate for the direct effect (Miočević et al., 2018). Following guidelines, we did not report proportion effect measures when the direct and indirect effect estimates yielded opposite signs (Miočević et al., 2018) or when the beta for the indirect effect was larger in magnitude than the total effect. This resulted in a higher number of effect measures generated for the ratio effect measures compared to proportion effect measures.
To generate these two effect measures, we included standardized beta estimates, given that they outperform unstandardized estimates in power, type I error rate, and interval width (Miočević et al., 2018). For studies that did not provide unadjusted standardized beta estimates, we used two approaches to back-calculate estimates: (1) through intercorrelations, as the exposure and mediator correlation is equivalent to the unstandardized beta estimate for path a, the mediator and outcome correlation is equivalent to the unstandardized beta estimate for path b, and the exposure and outcome correlation is equivalent to the unstandardized beta estimate for the total effect; or (2) we multiplied the unstandardized beta estimates by SDx/SDy to generate the fully standardized beta estimate (Miočević et al., 2018).
We calculated effect measures using unadjusted beta estimates, when possible, to best allow for comparison purposes, as the goal of the review was to summarize and compare relative magnitudes between paths and studies. Adjusted estimates would be challenging to compare across studies, as different models would be adjusting for different covariates. It is also possible, too, that the adjustment for covariates could bias the validity of the effect estimate if the variables were in fact not confounders (Ananth & Brandt, 2022). Therefore, on statistical grounds, we wanted to interpret standardized coefficients as correlations and not partial correlations, and therefore, we prioritized the unadjusted correlations. However, in instances where unadjusted estimates were not available and could not be back-calculated, we used adjusted beta estimates (or, partial correlations) in our analyses and noted them for potential sensitivity analyses. Given the intention of the study was to compare relative magnitudes, we felt that including some adjusted estimates in this sample would not influence the quality of the study, as we were primarily relying on unadjusted estimates.
We then ranked the pooled effect measures across domains, sub-domains, and constructs according to pooled median effect sizes – whereby each path was considered equally, even when multiple paths came from the same study. For example, if a single study contributed four paths under the same mediating domain (such as, two different mediators associated with internalizing and externalizing symptoms), all four paths would be considered n = 4 different paths in analyses. We felt it was appropriate to rank effect measures across studies given that we were comparing effect sizes within a pool of estimates already constrained to studies of the same exposure, mediator, and outcome concepts. We placed higher value to rankings of the pooled ratio effects over proportion effects, as these measures include more data and are more statistically robust (Miočević et al., 2018). Proportion effect sizes are reported as percentages throughout. Figures visually demonstrating the distributions of pooled effect measures were generated using R statistical software (R Core Team, 2018). In instances where multiple sample sizes were used to generate the effect measure (e.g., if different sample sizes were used to generate the indirect versus total effects), the smallest sample size was presented in the Figures.
Results
After screening 15,768 titles/abstracts and 1,302 full-text records (Figure 1), we identified 37 articles published from s = 29 larger studies (eTable 9; ranging from 1 to 3 articles per study). 100% (studies [s] = 29) of studies were published in English. Over three-quarters (78%; articles [a] = 29) of articles were peer-reviewed, and the remainder (22%; a = 8) were dissertations. The majority of studies were labeled as prospective cohorts (48%; s = 14) or cross-sectional studies (41%; s = 12); the remainder were retrospective cohort (3%; s = 1) or quasi-experimental (3%; s = 1) studies. Studies were conducted in 11 countries across North America (s = 19; 66%), Europe (s = 6; 21%), Asia (s = 2; 7%), Africa (s = 1; 3%), and Australia (s = 1; 3%). Enrollment start dates ranged from 1990 to 2018. Most studies included both daughters and sons (s = 25; 90%), but some studies were restricted to daughters (s = 2; 7%) or sons (s = 1; 3%) only. No studies assessed paths from grandmother to grandchild; therefore, the entire sample focused on transmission from mother to child. PRISMA 2020 flow diagram (Page et al., 2021). Note. *Based on database searching until Jan 21, 2021 (MEDLINE, PsycINFO, PTSDPubs) and March 10, 2021 (Scopus and ProQuest). See eTables 3–7 for final searches.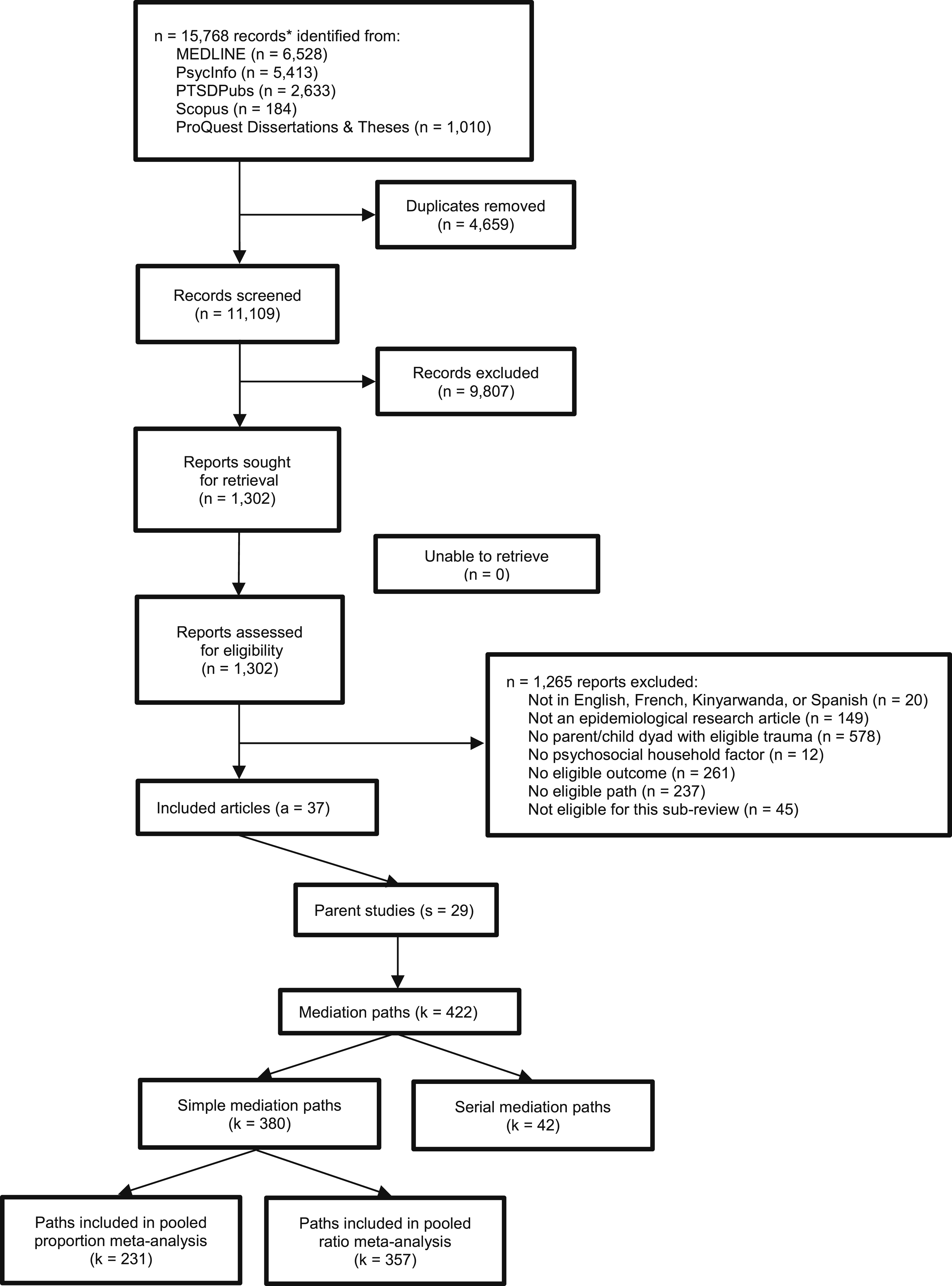
Of the 29 studies, we identified k = 422 paths (k = 380 simple mediation paths and k = 42 serial mediation paths; Figure 1). We identified an average of 15.1 paths in each study (average of k = 1.5 serial mediation paths and k = 13.6 simple mediation paths; ranging from k = 1-124 simple paths and k = 0-16 serial paths). When studies assessed indirect effects for statistical significance, every paper used bootstrapped confidence intervals or structural equation modeling; however, more heterogeneity was reported in the approaches used, including some that used the Baron and Kenny method (k = 24; 5.7%) and/or Sobel test (s = 5; 1.1%). Among the k = 380 simple mediation paths, path quality scores ranged from 1 (lowest quality) to 6 (highest quality), with an average score of 4.52, and drew from a sample of n = 414,627 dyads.
One-quarter of paths (k = 106; 25%) assessed a complete measure of maternal childhood trauma (such as the total scores from the Childhood Trauma Questionnaire [k = 69], Adverse Childhood Experiences screener [k = 29], or the Early Trauma Inventory [k = 5]). The remaining paths assessed a specific sub-area of childhood trauma (e.g., sexual abuse [k = 107; 25%], physical abuse [k = 58; 14%], emotional abuse [k = 41; 10%], physical neglect [k = 20; 5%], or emotional neglect [k = 12; 3%]) or a combination of different sub-areas (k = 78; 19%). Outcome measures were also measured heterogeneously. Only 12% of paths (k = 52) used a broad measure of child psychopathology, including the Child Behavior Checklist (k = 28) and the Strengths and Difficulties Questionnaire (k = 19), among others; however, paths often reported subscales of psychopathology, such as aggregate scales of externalizing (k = 73) versus internalizing symptoms (k = 67), or measures specific to diagnostic conditions including attention-deficit hyperactive disorder symptoms (k = 49), conduct problems (k = 47), dissociative symptoms (k = 34), depressive symptoms (k = 31), or anxiety symptoms (k = 19), among others. Post-traumatic stress symptoms were only measured as an outcome in k = 5 paths.
Distribution and characteristics of simple mediation paths according to mediator domain, sub-domain, and construct.
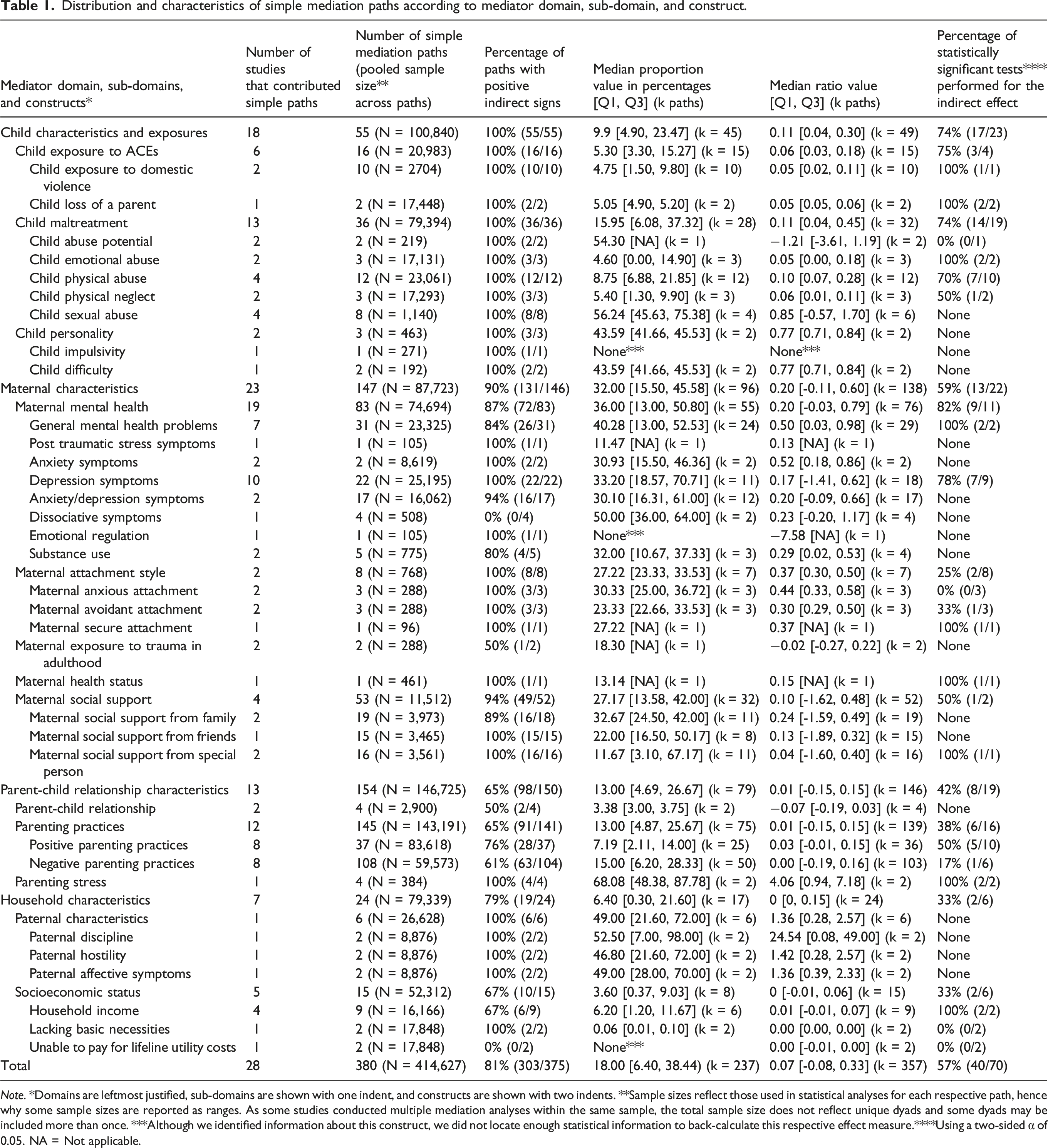
Note. *Domains are leftmost justified, sub-domains are shown with one indent, and constructs are shown with two indents. **Sample sizes reflect those used in statistical analyses for each respective path, hence why some sample sizes are reported as ranges. As some studies conducted multiple mediation analyses within the same sample, the total sample size does not reflect unique dyads and some dyads may be included more than once. ***Although we identified information about this construct, we did not locate enough statistical information to back-calculate this respective effect measure.****Using a two-sided α of 0.05. NA = Not applicable.
Figure 2 and eFigures 2–5 demonstrate our visual descriptive analysis of pooled effect measures from the simple paths across the different domains (Figure 2) and sub-domains within each of the four domains (eFigures 1–5). Among the simple mediation paths, there was a median sample size of n = 196 dyads (range: n = 31−9,397; IQR: 133, 250). k = 70 (18%) of the simple mediation paths reported results from statistical tests of indirect effect with a two-sided α of 0.05 (Table 1). Only k = 40 (57%) paths reported significant results. We were able to calculate the proportion effect measure for k = 231 (61%) of the simple mediation paths, generating effect estimates ranging from 0% to 100% of indirect effect accounting for the proportion of total effect (median: 17.2%; IQR: 6.3%, 38.4%). k = 194 (85%) paths were from unadjusted estimates, and k = 37 (16%) paths were from adjusted estimates. Of the unadjusted beta estimates, k = 185 (95%) were extracted from correlations. We calculated the ratio effect measures for k = 357 simple paths, with effect estimates ranging from −9 to 49 across paths (median: 0.067; IQR: −0.07, 0.33). k = 302 (85%) of these paths were from unadjusted estimates; k = 55 (15%) were from adjusted estimates. Pooled proportion (top panel) and ratio effect (bottom panel) measures for paths across mediating domains. Note. Each line corresponds to one path; the color corresponds to each respective study. Color legend in the right panel (larger scale version in Figure 1) and line width corresponds to the sample size (divided into four categorical bins: n ≤ 150; 150 < n ≤ 200; 200 < n ≤ 250; and n > 250; see eFigures 2–5 for sample size legends). Horizontal red lines indicate the boundaries for +1 and −1 ratio effect measures, which correspond to the thresholds at which the indirect (or mediating) effect is equal in magnitude to the direct effect and changes from being smaller to or larger than the direct effect; zero values correspond to effect sizes where there was no indirect effect compared to direct effect. Values >|±1| correspond to effect sizes where the indirect (or mediating) effect was larger than the direct effect. Due to large variability of values above 1.0 and below −1.0, the pooled ratio effect measures were transformed using the R arctangent transformation (inverse tangent) atan function to aid with data visualization.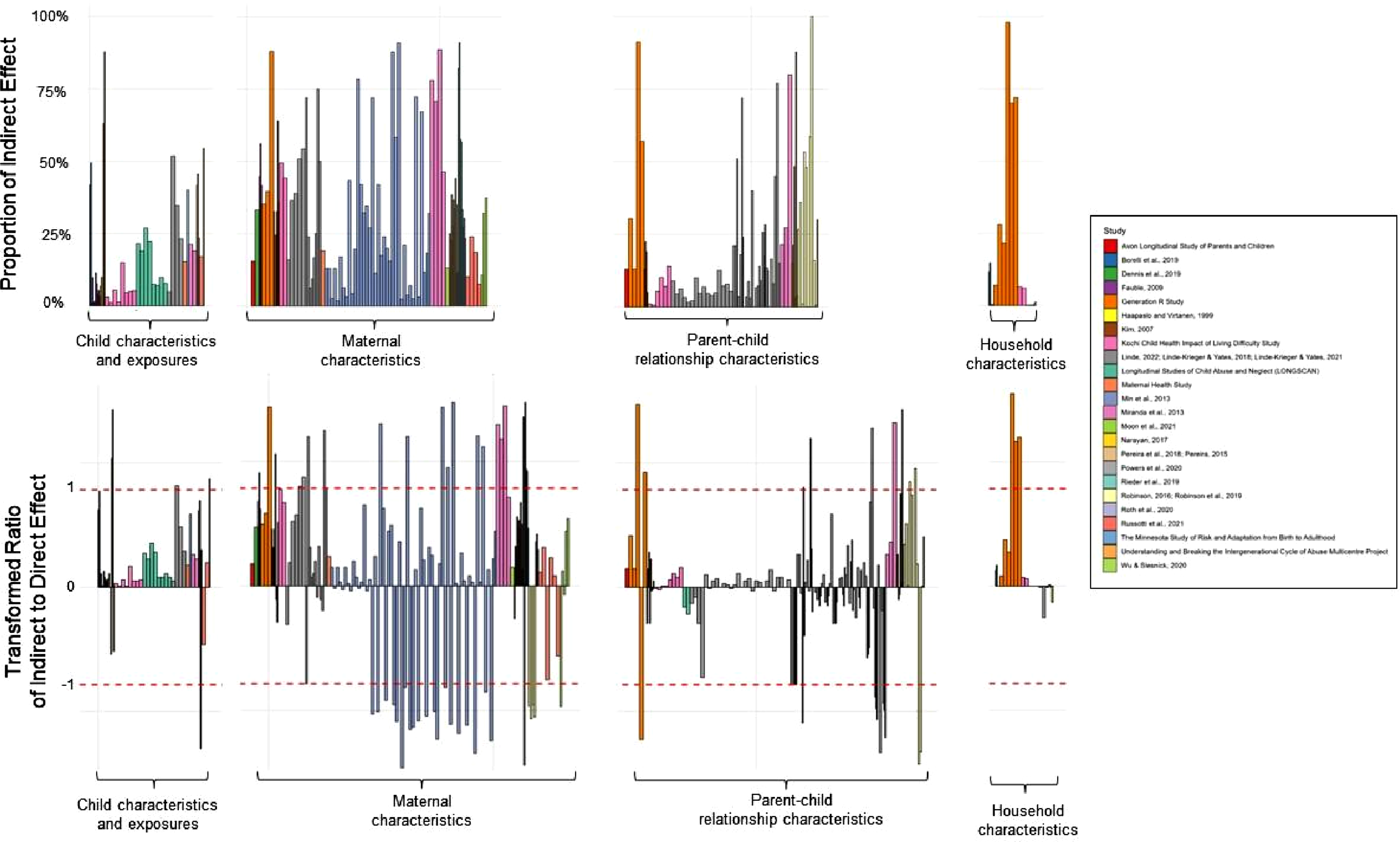
The vast majority of paths provided unadjusted data to calculate effect estimates (84% [k = 194] for proportion effect measures; 85% [k = 302] for ratio effect measures); thus, even though many paths provided data for adjusted estimates, the majority of data used to generate proportion effect measures (k = 185; 80%) and ratio effect measures (k = 293; 82%) came from correlation matrices. This contrasts what authors reported in their studies as majority of studies (s = 25; 86%) adjusted for covariates in their mediation analyses. In fact, k = 29 paths (7%) came from studies that did not explicitly test for mediation, but instead reported statistical data for variables of interest (such as a correlation matrix) that we used to back-calculate effect estimates. Since all papers provided either a standardized estimate or correlation matrix, we did not need to standardize any unstandardized effect estimates.
Child Characteristics and Exposures
The domain of child characteristics and exposures is composed of three sub-domains and, within them, nine constructs (Table 1); two sub-domains and five constructs obtained data from at least one path that had an indirect effect significant at the α = 0.05 level. n = 18 studies contributed k = 55 simple paths from n = 100,840 dyads; within this, we identified median proportion and ratio values of 9.9 and 0.11 Nearly three-quarters (74%; n = 17) of statistical tests found statistically significant indirect effects at the α = 0.05 level. Across all paths, the pooled indirect effects contributed a median 9.8% (IQR: 4.8%, 26.9%) of the total association between maternal childhood trauma and child psychopathology (below the pooled median of 17.0% in the entire sample) and a pooled median indirect to direct effects ratio of 0.11 (IQR: 0.04, 0.30). Median pooled values did not change considerably when restricted to only statistically significant paths (eTable 10), demonstrating a median pooled proportion of 11.2% and ratio of 0.08. Every path in this domain contributed indirect paths of positive signs. eFigure 2 shows all effect measures, regardless of statistical testing or significance, stratified across sub-domains.
The largest sub-domain was child maltreatment, which included data from n = 79,394 dyads from k = 36 simple paths across s = 13 studies (Table 1). Among paths that were statistically significant at the two-sided α = 0.05 level, the pooled indirect effects contributed a median proportion of 14.9% (IQR: 5.4%, 21.5%) and a pooled median ratio of 0.13 (IQR: 0.05, 0.25; eTable 10). We categorized paths into the following constructs: physical abuse (k = 12; n = 23,061), emotional abuse (k = 3; n = 17,131), physical neglect (k = 3; n = 17,293), sexual abuse (k = 8; n = 869), and child abuse potential (defined as such in the original articles; k = 2; n = 219). For the physical abuse construct, seven of the ten statistical tests of the indirect effect were statistically significant; among significant paths, there was a median pooled indirect effect of 19.0% (IQR: 7.0%, 22.2%) and a pooled median ratio of 0.23 (IQR: 0.08, 0.29) indirect to direct effects. The emotional abuse construct reported two statistically significant tests; among these, the pooled median proportion and ratio measures of effect were modest (9.8% [IQR: 4.6%, 14.9%] and 0.11 [IQR: 0.05, 0.18]; eTable 10). The physical neglect construct yielded modest pooled median effect measures (5.4% [IQR: 1.3%, 9.9%] and 0.06 [IQR: 0.01, 0.11]). Though the remaining two constructs drew from smaller sample sizes, and identified no evidence for statistically significant effects, they yielded moderate measures of effect. The sexual abuse construct yielded pooled median indirect effects of 56.2% (IQR: 45.6%, 75.4%) and pooled median ratio of 0.85 (IQR: −0.57, 1.70), and the child abuse potential construct yielded large measures of effect (pooled median proportions and ratios of 54.3% (drawn from k = 1 path) and −1.21 [IQR: −3.61, 1.19]; Table 1).
The second largest sub-domain was child exposure to adverse childhood experiences. This sub-domain included data from n = 20,983 dyads and k = 16 simple paths across six studies (Table 1). Among the statistically significant paths, the pooled indirect effects contributed a median 5.2% (IQR: 4.9%, 15.3%) of the total association between maternal childhood trauma and child psychopathology and a pooled median indirect to direct effects ratio of 0.06 (IQR: 0.05, 0.18; eTable 10). We categorized paths into two constructs: child loss of a parent (k = 2; n = 17,448) and child exposure to domestic violence (k = 10; n = 2,704). Among statistically significant paths, both constructs yielded modest and similar measures of effect of pooled median proportions of 5.1% and 15.3% and a pooled median ratio of 0.05 and 0.18. The last domain was child personality, but was only comprised of data from two studies and k = 3 paths from n = 192 dyads. We were only able to generate pooled estimates for one construct labeled ‘child difficulty’, which was moderate in size with a pooled median proportion of 43.6% [IQR: 41.7%, 45.5%] and pooled median ratio of 0.77 [IQR: 0.71, 0.84]. No paths within this sub-domain were statistically significant at the two-sided α = 0.05 level.
Maternal Characteristics
The domain of maternal characteristics is composed of five sub-domains and 14 constructs. Three sub-domains and five constructs contained paths that had evidence for a statistically significant indirect effect at the α = 0.05 level (Table 1). s = 23 studies contributed k = 147 simple paths, leading to a pooled analysis drawing on data from n = 87,723 dyads (median proportion = 32.0; median ratio = 0.2). More than half (59%; n = 13) of statistical tests performed on the indirect effects were statistically significant at the 0.05 level. Among statistically significant paths, the pooled indirect effects contributed a median 34.3% (IQR: 27.2%, 44.1%) of the total association between maternal childhood trauma and child psychopathology (which is above the pooled median of 15.1% across significant paths in the entire sample) and a pooled median indirect to direct effects ratio of 0.51 (IQR: 0.24, 0.79; eTable 10). eFigure 3 shows all effect measures, regardless of statistical testing or significance, stratified across sub-domains.
The largest sub-domain was maternal mental health, which included data from n = 74,694 dyads from k = 83 simple paths across 19 studies. Nine tests identified statistically significant indirect effects at the α = 0.05 level. Among statistically significant paths, the pooled median proportion was 41.3% (IQR: 33.2%, 44.2%) and the pooled median ratio was 0.62 (IQR: 0.24, 0.79; eTable 10). We categorized paths into the following eight constructs: general mental health problems (k = 31; n = 23,325), depressive symptoms (k = 22; n = 25,195), anxiety/depressive symptoms (k = 17; n = 16,062), anxiety symptoms (k = 2; n = 8,619), substance use (k = 5; n = 775), dissociative symptoms (k = 4; n = 508), emotional regulation (k = 1; n = 105), and post-traumatic stress symptoms (k = 1; n = 105). Only two constructs included statistically significant paths (eTable 10): the construct of general mental health problems yielded moderate effect measures (pooled median proportion: 46.9% [IQR: 44.2%, 49.5%]; pooled median ratio: 0.89 [IQR: 0.79, 0.98]) and the construct of depressive symptoms yielded moderate effect measures (pooled median proportion: 35.9% [IQR: 26.2%, 41.3%]; pooled median ratio: 0.51 [IQR: 0.24, 0.62]).
The second largest sub-domain was maternal social support, which drew from n = 11,512 dyads in k = 53 paths across four studies, though only one test identified evidence for statistically significant indirect effects at the α = 0.05 level (Table 1). The pooled indirect effects contributed a median 27.2% (IQR: 13.6%, 42.0%) of the total association between maternal childhood trauma and child psychopathology and a pooled median indirect to direct effects ratio of 0.10 (IQR: −1.62, 0.48). We categorized paths into the following three constructs: support from family (k = 19; n = 3,973), support from a ‘special person’ (language used in the original study instrument meaning an individual considered significant to the respondent, such as a significant other; k = 16; n = 3,561), and support from friends (k = 15; n = 3,465). Only the construct social support from a special person reported evidence for statistical significance, and its pooled median proportion was 35.0% (from k = 1 path) and the pooled median ratio was 0.54 (from k = 1 path; eTable 10).
The third largest sub-domain was maternal attachment style, drawing from n = 768 dyads in k = 8 paths from two studies (Table 1). Among statistically significant paths, the pooled indirect effects contributed a median pooled proportion of 30.4% (IQR: 27.2%, 33.5%) and a pooled median ratio of 0.44 (IQR: 0.37, 0.50; eTable 10). This sub-domain had three constructs: anxious attachment (k = 3; n = 288), avoidant attachment (k = 3; k = 288), and secure attachment (k = 1; n = 96) (Table 1). The avoidant and secure attachment styles yielded at least one statistically significant path (eTable 10). Of these, both avoidant and secure attachment styles had moderate effect sizes, though avoidant attachment produced larger estimates compared to secure attachment (pooled median proportions of 33.5% [from k = 1 path] compared to 27.2% [from k = 1 path]; pooled median ratios of 0.50 and 0.37; eTable 10). The last sub-domains were maternal exposure to trauma in adulthood, which showed a pooled median proportion of 18.3% and a pooled median ratio of −0.02, and maternal health status, which generated a pooled median proportion of 13.1% and a pooled median ratio of 0.15.
Parent-Child Relationship Characteristics
The domain of parent-child relationship characteristics was composed of three sub-domains and two constructs (Table 1). Only two sub-domains and two constructs contained paths that identified a statistically significant indirect effect at the two-sided α = 0.05 level (eTable 10). Thirteen studies contributed k = 154 simple paths, leading to a pooled analysis drawing on data from n = 146,725 dyads (median proportion [MP] = 13.0; median ratio [MR] = 0.01). Less than half (42%; n = 8) of statistical tests performed on the indirect effects were statistically significant. Across statistically significant paths, the pooled indirect effects contributed a median 8.6% (IQR: 6.2%, 12.1%) of the total association between maternal childhood trauma and child psychopathology (which is slightly below the pooled median of 15.1% across significant paths in the entire sample) and a pooled median indirect to direct effects ratio of 0.07 (IQR: −0.10, 0.11; eTable 10). eFigure 4 shows all effect measures, regardless of statistical testing or significance, stratified across sub-domains.
The largest sub-domain was parenting practices, which included data from n = 143,191 dyads from k = 154 simple paths across 13 studies (Table 1). Six tests identified evidence for statistically significant indirect effects at the α = 0.05 level within this sub-domain. Among statistically significant paths, the pooled indirect effects contributed a median 8.6% (IQR: 6.2%, 12.05%) of the total association between maternal childhood trauma and child psychopathology and a pooled median indirect to direct effects ratio of 0.07 (IQR: −0.10, 0.11; eTable 10). We categorized paths into the two constructs: positive parenting practices (k = 37; n = 83,618) and negative parenting practices (k = 108; k = 59,573; Table 1). The negative parenting practices construct included: maternal hostility/aggression, harshness, shouting, slapping, insensitivity, undifferentiated rejection, indifference/neglect, low support, authoritarian control, intrusiveness, boundary dissolution, overprotection, role-confusion, and negative maternal perception of the child. The positive parenting practices construct included: appropriate maternal perceptions of the child, parenting enjoyment and confidence, appropriate and consistent levels of discipline, warmth/sensitivity and understanding, use of positive reinforcement, and meeting the child’s nutritional needs. Both constructs showed modest measures of effect, though negative parenting practices showed slightly higher values (pooled MPs of 14.5% [IQR: 5.7%, 29.4%] and 7.2% [IQR: 2.1%, 14.0%]; pooled MRs of 0.00 [IQR: −0.19, 0.16] and 0.03 [-0.01, 0.15]). Only five paths showed statistically significant associations for positive parenting practices (50% of tests performed); however, only one of the six tests performed was significant for negative parenting practices (eTable 10).
The second largest sub-domain was the parent-child relationship, which included data from n = 2,900 dyads from k = 4 simple paths across two studies (Table 1). The effect measures were modest, as the pooled indirect effects contributed a median 3.4% (IQR: 3.0%, 3.8%) of the total association between maternal childhood trauma and child psychopathology and a pooled median indirect to direct effects ratio of −0.07 (IQR: −0.19, 0.03). No statistically significant paths were found among this sub-domain. The last sub-domain was parenting stress, which included data from n = 384 dyads from k = 4 simple paths from just one study; despite this, this study generated two tests of statistical significance for two of these paths. Among the two paths without tests for statistical significance, the effect measures were very large, as the pooled indirect effects contributed a median 68.1% (IQR: 48.4%, 87.8%) of the total association between maternal childhood trauma and child psychopathology and a pooled median indirect to direct effects ratio of 4.06 (IQR: 0.94, 7.18).
Household Characteristics
The domain of household characteristics was composed of two sub-domains and six constructs; only one sub-domain and one construct included statistically significant paths (Table 1). Seven studies contributed k = 24 simple paths, leading to a pooled analysis drawing on data from n = 79,339 dyads (MP = 6.4; MR = 0.0). One third (33%; n = 2) of statistical tests performed on the indirect effects were found statistically significant at the α = 0.05 level. Across statistically significant paths, the pooled indirect effects contributed a median 6.2% (IQR: 6.0%, 6.4%) of the total association between maternal childhood trauma and child psychopathology (which is below the pooled median of 15.1% among significant paths in the entire sample) and a pooled median indirect to direct effects ratio of 0.07 (IQR: 0.06, 0.07; eTable 10). eFigure 5 presents all effect measures, regardless of statistical testing or significance, stratified across sub-domains.
The largest sub-domain was socioeconomic status, which included data from n = 52,312 dyads from k = 15 simple paths across five studies (Table 1). Two tests identified evidence for statistically significant indirect effects at the α = 0.05 level. Among the statistically significant paths, the pooled indirect effects contributed a median 6.2% (IQR: 6.0%, 6.4%) of the total association between maternal childhood trauma and child psychopathology and a pooled median indirect to direct effects ratio of 0.7 (IQR: 0.06, 0.07). We categorized paths into three constructs: household income (k = 9; n = 16,166), lack of basic necessities (k = 2; n = 17,848), and inability to pay for lifeline utility costs such as electricity or gas (k = 2; n = 17,848). Household income generated two tests of statistical significance. Among statistically significant paths, this construct generated modest measures of effect (pooled median proportion: 6.2% [IQR: 6.0%, 6.4%]; pooled median ratio: 0.07 [IQR: 0.06, 0.07]).
The second sub-domain was paternal characteristics, which included data from k = 6 simple paths, but within just one study that included n = 8,876 dyads (Table 1). The included paper did not test for statistically significant indirect effects for any paths within this sub-domain; however, the measures of effect were very large. The pooled indirect effects contributed a median 49.0% (IQR: 21.6%, 72.0%) of the total association between maternal childhood trauma and child psychopathology and a pooled median indirect to direct effects ratio of 1.36 (IQR: 0.28, 2.57). We categorized paths into three constructs: paternal discipline (k = 2), paternal hostility (k = 2), and paternal affective symptoms (k = 2).
Serial Mediation Paths
We identified k = 42 serial mediation paths, most of which transcended multiple domains. The majority of serial mediation paths (k = 41; 98%) included two variables; only one serial mediation path included three variables (k = 1; 2%). Twenty serial mediation paths from s = 4 studies assessed the impact of maternal trauma onto the maternal mental health or another psychological factor. Nine serial mediation paths from s = 2 studies assessed the impact of maternal trauma on maternal social support, and how it then impacted maternal enjoyment of parenting or authoritarian control. Eight serial mediation paths assessed the impact of maternal trauma on the impact of child ACEs (including experiences of maltreatment, stress exposure, and intimate partner violence in the household) and then its downstream impact on further ACEs, maternal depression, or maternal use of physical punishment. One path assessed the impact of maternal trauma on paternal hostility through paternal discipline on child mental health. Several other paths assessed the impact of the same variable but were administered at different timepoints.
Domain and Sub-domain Rankings
Rankings of domains and sub-domains are visually represented in Figure 2 and eFigures 2–5. The maternal characteristics domain yielded the highest ranking of median pooled effect measures for both proportion (31.2%) and ratio (0.21) methods (Table 1). This ranking remained unchanged even when the sample was restricted to statistically significant paths (MP: 34.3%; MR: 0.51; eTable 10). The child characteristics domain had the second-highest median pooled ratio effect measure (0.11), and the third-highest median pooled proportion effect measure (9.9%). The parent-child characteristics domain had the third-highest median pooled ratio effect measure with a near-zero value (0.01), and the second-highest median pooled proportion effect measure (13.0%).
Among sub-domains that gathered data from multiple studies (three or more), the following sub-domains contributed the highest median pooled effect sizes: maternal attachment style (MP: 27.2%; MR: 0.37), maternal mental health (MP: 36.0%; MR: 0.22), maternal social support (MP: 27.2%; MR: 0.10), and child maltreatment (MP: 16.0%; MR: 0.11). Despite large sample sizes, parenting practices (MP: 13.0%; MR: 0.01) and socioeconomic status (MP: 3.6%; MR: 0.0) produced lower effects. Among sub-domains that gathered paths that reported statistically significant indirect effects, the following sub-domains contributed the highest median pooled effect sizes: maternal mental health (MP: 41.3%; MR: 0.62), maternal social support (MP: 35.0%; MR: 0.54), and maternal attachment style (MP: 30.4%; MR: 0.44).
Discussion
To our knowledge, this systematic review provided the first attempt to quantitatively rank the effect sizes of a wide variety of family-level mediators of the intergenerational transmission of maternal childhood trauma. We included data gathered from 40 serial and 380 simple mediation paths drawn from n = 352,279 dyads and identified sufficient literature to evaluate four psychosocial family-related mediating domains, organized into 13 sub-domains and 32 constructs. Although several paths were significant across domains, there was considerable heterogeneity in effect measure sizes and significance tests, suggesting that trauma is likely transmitted through the interplay of several risk and protective factors. The maternal characteristics domain yielded the highest ranking of pooled effect measures (MP = 32.0%), followed by the child characteristics (MP = 9.9%) and parent-child characteristics (MP = 13.0%) domains. Among sub-domains, maternal attachment style (MP = 27.2%), maternal mental health (MP = 36.0%), maternal social support (MP = 27.2%), and child maltreatment (MP = 16.0%) yielded the highest pooled effect measures. These maternal factors seem to play a larger role than other family-related influences, such as parent-child relationship (MP = 13.0%) or household (MP = 6.4%) characteristics, suggesting the potential important role of supporting mothers to help break the cycle of trauma across generations. These findings suggest that factors stemming from the mother could play the largest role in mediating the intergenerational transmission of maternal childhood trauma, and that a mother’s own mental health, her personal attachment style, and the support she receives are potentially some of the most influential ways her early trauma can affect her child’s mental health. We did not identify any studies that assessed mediators between the first and third generations, which suggests a research gap in this broader field.
Our findings support results from similar prior reviews (Loheide-Niesmann et al., 2022; Ma et al., 2022; Plant et al., 2017). Other reviews have consistently reported that factors stemming from the mother (e.g., mental health, stress levels, and social support) are more associated with trauma transmission than other family-level factors from other sources (e.g. maternal depressive symptoms), and to our knowledge, this review is the first to provide quantitative evidence of this phenomenon. We also found a consistent indirect path from maternal childhood trauma to child outcomes via child maltreatment, though the effects were modest. A novel contribution was that we identified some evidence that factors related to the father might also influence transmission of maternal childhood trauma (Rijlaarsdam et al., 2014). The authors of the work that identified this relationship suggest that women who have experienced childhood maltreatment are more likely to have partners who engage in hostile or aggressive behavior, and this behavior is associated with harsh parenting and offspring adjustment problems (Rijlaarsdam et al., 2014).
Maternal anxiety and stress might be a common factor in the transmission of trauma across generations. Though there were low sample sizes for each, maternal anxiety (MP = 30.9), maternal anxious attachment (MP = 30.3), and parenting stress (MP = 68.1) appeared to have particularly high effect measures. This aligns with the broader literature, which shows that maternal stress – especially during the pre- and post-natal period – can increase risk of offspring psychopathology (Clayborne et al., 2023; Kinsella & Monk, 2009; Rees et al., 2019). Literature suggests that this mechanism likely operates through biological pathways; these findings align with the developmental origins of health and disease hypothesis, which states that maternal stress during critical developmental windows can lead to sustained alterations in the fetal nervous system and have long-term impacts on child psychopathology (Clayborne et al., 2023). Other research demonstrates similar impacts from parental anxiety throughout the child’s developmental lifespan spanning from infancy, childhood, and adolescence (Sweeney & Wilson, 2023). One review identified 18 studies assessing parental anxiety on child mental health outcomes and identified significant negative associations with very small, small, and moderate effects (Sweeney & Wilson, 2023). More research studies with larger sample sizes are needed to evaluate the impact of maternal stress and anxiety as a mediator for intergenerational trauma transmission. There is also a need for future studies to investigate how different forms of anxiety and stress, as well as the timing of maternal trauma, impact the degree and mechanism of trauma transmission.
It was notable that effect measures from parent-child relationships characteristics (MP = 13.0%) were small in magnitude. Nearly half (45%) of studies and half (40%) of simple paths included at least one path within this domain, but the pooled MR was only 0.01, indicating a near-zero indirect effect. The small effects are in contrast with the emphasis the wider intergenerational trauma field has placed on parenting behaviors in transmission (Flanagan et al., 2020). Further research could explore more factors related to the parents themselves, rather than the interaction between parent and child, and explore these interrelationships through further serial mediation models. For example, parent-child factors might not mediate the relationship between maternal childhood trauma and child psychological outcomes, but could mediate variables downstream, such as mediating the path from parental post-traumatic stress symptoms to child psychopathology. Additionally, it is notable that maternal attachment was only evaluated in two studies. The dearth of empirical mediation paths measured within the maternal childhood trauma research area contrasts with the attention given to attachment theory in the broader intergenerational trauma literature across other trauma types (Isobel et al., 2019). In a similar vein, it was striking that only one study measured the mediating impact of parental post-traumatic stress symptoms, given the strong effects of maternal mental health symptoms more generally, and that the exposure of interest is trauma.
The family-related mediating concepts identified in this review overlap with those presented in previous narrative reviews, including maternal mental health, parenting practices, maternal social support, child maltreatment, maternal physical health, among other factors (Loheide-Niesmann et al., 2022; Plant et al., 2017). Our findings also validate another mediation meta-analysis which demonstrated that maternal depression and maternal insecure attachment generated a significant pooled indirect effect (pooled standardized effects: 0.10 and 0.07, respectively; pooled proportion effects: 47% and 25%, respectively; Ma et al., 2022). Our review expands upon prior research due to its sheer size. The largest existing review gathered n = 82 effect sizes for analyses — less than one quarter of those identified in our study. Further, it was limited to externalizing symptoms, whereas our review delved into the broader psychological effects of intergenerational trauma across a broad spectrum of mental health measures (Loheide-Niesmann et al., 2022). Our review identified socioeconomic status as a mediator and gathered a sufficiently large number of paths such that we were able to sub-categorize domains more granularly compared to other reviews. This included different subtypes of child maltreatment and maternal mental health, which allow for deeper understandings of mediators and their underlying mechanisms.
Our results support other research that has identified mixed evidence to support the role of parenting practices in the intergenerational transmission of trauma. Though Plant (2017) concluded that parenting practices would be a key mediator for intervention, our results did not strongly support this finding and rather align with findings from other reviews suggesting that parenting practices are less impactful in the intergenerational transmission of trauma compared to other mediators (Loheide-Niesmann et al., 2022; Ma et al., 2022). This is surprising, given that many family-based skills interventions to improve child socio-emotional development (such as the Strengthening Families Program; Kumpfer et al., 2015) have a parent skill-building component. However, one potential explanation is that, given 90% of the papers included in this review were drawn from North America, Europe, and Australia, further research conducted in more expansive non-Western racial or ethnic groups might identify different associations.
Furthermore, fathers might play a larger role in intergenerational trauma transmission. Though this review focused on maternal childhood trauma and did not explore paternal trauma, we identified one study that assessed this and found large effect measures of father-related factors mediating transmission from mother to child (MP = 49.0%), suggesting potential to integrate the role of fathers into family-based interventions. In a similar vein, one meta-analysis demonstrated that parental gender was a statistically significant moderator of intergenerational transmission of trauma from parent to child, such that transmission was more pronounced among trauma exposed mothers compared to trauma exposed fathers (maternal mean weighted Pearson product-moment correlation = 0.29 [95% CI: 0.24, 0.33]; paternal mean weighted Pearson product-moment correlation = 0.13 [95% CI: 0.04, 0.22]; Morris et al., 2012). Studies have assessed mediators in the relationship between paternal childhood trauma specifically on child mental health (Seteanu & Giosan, 2021), with several more assessing the impact of mediators in mixed parental gender studies (Charak et al., 2021; Ochoa et al., 2022).
Importantly, this review highlights several meta-scientific issues in this field of research. As expected based on prior reviews, we identified a high degree of heterogeneity among the constructs of exposures, mediators, and outcomes (along with their measurement instruments). There was substantial heterogeneity in terms of how the indirect effect was analyzed and reported – for example, differences in adjustment approaches and analytic methods across the different studies. Many studies did not test for statistically significant indirect effects, yet provided beta estimates for the exposure on mediator (path a) and mediator on outcome (path b) paths in structural equation models. It was not uncommon that the total effects reported in the retrieved studies were larger than the sum of the direct and indirect effects – suggesting potential errors in reporting in the original studies. This is especially relevant given that we were often relying on data presented in correlation matrices, sometimes only included in Supplemental Materials, which might have been more subject to reporting errors compared to data reported in the main manuscript.
Our meta-analysis was restricted to simple paths, and thus, we did not account for multiple, interrelated mediators; therefore, this review likely oversimplifies the many interrelated and complex relationships impacting trauma transmission. This review only identified k = 42 serial mediation paths, spanning across multiple domains, but the majority evaluated the downstream impacts of maternal mental health measures, which aligns well with our findings that maternal mental health is likely most impactful in transmitting trauma intergenerationally. These serial mediation paths were generally well-reported and were conducted under conditions with a theoretical basis (meaning, the authors justified relationships underlined with prior research and theory). However, we were sometimes unable to extrapolate content from serial mediation paths into simple paths. We therefore recommend that authors in serial mediation papers also report the unadjusted and adjusted simple path models in their Supplemental Material, if possible, to allow for these results to be integrated into evidence synthesis efforts.
Our review has multiple noteworthy limitations. First, it is possible that some mediators found not to be influential in this review could be influential when tested in combination with other mediators (impacting through other mechanisms not explored). For example, though socioeconomic status did not yield large pooled effect estimates, it is possible that this construct is still influential in how it operates through other mediators (e.g., maternal mental health). Second, though most included paths were gathered from unadjusted estimates, for instances where unadjusted estimates were unavailable, we used adjusted estimates (n = 55; 14%). If these paths were adjusted appropriately, for example, informed by a causal diagram with empirical justification a priori, then it is possible that these adjusted estimates would be minimally biased. However, we rarely observed the presentation of such causal diagrams in the articles we reviewed, so it is possible that these adjustments could have reduced or further biased the mediating effects. Third, some mediators were challenging to classify into one specific, mutually exclusive domain. For example, the mediator “hostility towards the child” overlapped with elements of child maltreatment but was classified under the negative parenting practices construct under the parenting practices sub-domain for the purpose of analyses. Fourth, we conducted a descriptive meta-analysis that did not aim to be inferential, or pool tests of statistical inference, but rather aimed to compare the relative magnitude of effects across domains, sub-domains, and constructs (Glass, 1976). Using this approach, we did not weight paths by sample size, study quality, or precision; thus, it is possible that a low-quality cross-sectional study with a modest sample size would influence the median just as much as a large high-quality prospective cohort study. Fifth, given that some larger studies would have contributed multiple paths across different mediators and outcomes within the same constructs, it is possible that these studies could have disproportionate influence on the domain-level medians and should be interpreted with caution and alongside the visual depictions across Figures. Last, it is also possible that other relevant studies have been published since this review, given that the search strategy was conducted in 2021.
We also report limitations related to the quality of included studies themselves. We included study designs that measured the exposure (maternal trauma) and outcomes (childhood mental health outcomes) at the same timepoint. Though we have labeled these studies as cross-sectional, as defined in the literature, methodologically we would consider these retrospective cohort designs with a cross-sectional assessment; however, it should still be noted that the measurement of both variables at the same timepoint could be subject to recall and other biases (Baldwin et al., 2019). Similarly, oftentimes the mother would report on all variables (exposure, mediators, and outcomes) which could bias estimates. For example, mothers could amplify maternal characteristics, or underreport negative practices, due to recall or social desirability biases. We recommend more prospective studies be conducted with external assessments to prevent bias in future research.
Ratio effect measures should also be interpreted with caution. The sign itself does not correspond to the direction of the indirect effect, but rather demonstrates a difference in direction between the indirect and direct effects. This is referred to as inconsistent mediation, where the mediator acts like a variable that suppresses the correlation between the exposure and outcome variables (Kenny, 2024). The sign of the ratio effect measure depends on the combination of signs of the indirect and the direct effect. For example, a positive sign could mean that either all paths are positive or that both the indirect and direct effects are negative (both work in the same direction). The signs of this metric thus proved less useful in our descriptive meta-analysis.
Despite its limitations, this review prompts several new avenues of research. Though not formally tested, our results appear to show larger effect measures among child externalizing behaviors, which align with findings identified in other reviews (Plant et al., 2017) and could be further explored; however, it should also be interpreted with caution, given that parents are more likely to report externalizing over internalising problems. More research assessing complex mediation paths among these highly ranked constructs is needed to understand the interplay between variables to further inform intervention development. It would also be of use to continue to understand whether the type of exposure variable (i.e. composite measures, such as ACEs versus a more focused measure of a specific traumatic experience) would impact the significance and degree of moderation to inform intervention development. This review also only identified a small handful of studies outside of North America and Europe, suggesting a need for more work on this subject in more geographically diverse contexts. Given that this work focused on maternal trauma, there is also a need for further research on paternal trauma and intergenerational trauma transmission. Finally, there is a need for future work to promote standardization in measurement and reporting across studies involving mediation analyses, especially with respect to statistical information and analyses to aid in future evidence synthesis.
Implications for Practice
Our findings underscore the potential central role of maternal factors in the intergenerational transmission of trauma. Interventions that bolster maternal mental health and social support would be most impactful in disrupting the intergenerational transmission of trauma, though further research is needed to validate these results. We recommend that programs that interface with families with maternal childhood trauma histories provide additional mental health and social support resources and that programmers conceptualize that these supports should also strengthen child mental health.
Conclusion
This systematic review provided the first attempt to quantitatively rank the importance of a wide variety of family-level mediators in the intergenerational transmission of maternal childhood trauma. Our review identified four major domains of mediating concepts: child characteristics and exposures, maternal characteristics, mother-child relationship characteristics, and household characteristics. Factors stemming from the mother directly – including mental health, attachment, and social support – appeared to play the largest role in the intergenerational transmission of maternal childhood trauma. In contrast, parenting practices and socioeconomic status were not mediators with substantial effect sizes. These findings suggest that interventions supporting maternal mental health, social support, and stress-management could be most impactful in disrupting intergenerational trauma transmission for future generations, though future work is needed to validate our results and evaluate a more diverse sample of mediating concepts.
Supplemental Material
Supplemental Material - Family-Level Mediators in the Intergenerational Transmission of Maternal Childhood Trauma: Systematic Review and Meta-Analysis of Pooled Effect Measures
Supplemental Material for Family-Level Mediators in the Intergenerational Transmission of Maternal Childhood Trauma: Systematic Review and Meta-Analysis of Pooled Effect Measures by Emma J. Mew, Rhayna Poulin, Veronika Shabanova, Hannah Gorman, Marie-Claire Meadows, Jessica L. Bonumwezi, Victoria Chung, Rachel Hennein, Audrey Huang, Kevin Quach, Vanessa Blas, Ashlin Ondrusek, Karly Weinreb, Kate Nyhan, Si’itia Soliai-Lemusu, Jueta McCutchan-Tofaeono, Nicola L. Hawley, Sarah R. Lowe in Child Maltreatment
Footnotes
Acknowledgments
We would like to thank Vermetha Polite for assistance with downloading full text articles. We would also like to thank Julia Stover for helping build the REDCap data extraction form and thank Xintong Lu for figure generation.
Ethical Considerations
This systematic review did not require ethical approval as all data was drawn from publicly available literature.
Funding
The primary source of funding was a Canadian Institutes of Health Research Doctoral Foreign Study Award (#DFD-175791; PI: EJM). EJM was also supported by the Michael B. Bracken Doctoral Fellowship at the Yale School of Public Health, a P.E.O Scholar Award, and by the Duke Center for Global Mental Health. No funders were involved in the study design, collection, analysis, interpretation of data, or the decision to submit this work for publication.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original dataset is available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.