
Abstract
Intimate partner violence (IPV) is a public health crisis affecting one in three women and one in ten men in their lifetimes. Rehabilitation professionals are highly likely to encounter survivors of IPV in their practice; yet, there exists no formal review assessing the relationship between IPV and rehabilitation. Our objective was to understand the types and contexts of rehabilitation care currently available for survivors of IPV, opportunities identified in the literature for rehabilitation care, and IPV awareness and education among rehabilitation providers. A search strategy related to IPV and four rehabilitation professionals of interest (occupational therapy, physiotherapy, speech-language pathology/therapy, and physiatry) was developed across 10 databases and complemented by a gray literature search. Two reviewers independently assessed articles for inclusion. In all, 44 articles met inclusion criteria, ranging from primary research articles (48%) to clinical newsletters. Included articles predominantly focused on opportunities for rehabilitation care (68%) and occupational therapists as a profession (68%). A minority of studies examined specific interventions for IPV survivors (18%) or assessed for knowledge and attitudes about IPV (16%) among rehabilitation professionals. To our knowledge, this is the first scoping review exploring the rehabilitation literature for IPV survivors. These findings show an awareness of IPV among rehabilitation professionals, the importance of identifying IPV in clients, and the ways in which rehabilitation professionals are uniquely situated to support survivors of IPV. There remains an opportunity to explore interventions designed specifically for IPV survivors.
Background and Rationale
Intimate partner violence (IPV) is a highly prevalent public health concern that impacts one in three women and nearly one in ten men in their lifetime (Cotter, 2021; Smith et al., 2018; World Health Organization, 2021b). Defined as physical, psychological, sexual, emotional, or financial violence or abuse committed by a current or former spouse or intimate partner (Johnson et al., 2022; King et al., 2017; World Health Organization, 2021b), IPV can have significant impacts on the physical, mental, and emotional well-being of survivors, which may result in longer-term disability (Beydoun et al., 2017; Burczycka, 2018; Kwako et al., 2011; Stubbs & Szoeke, 2022). In addition to IPV increasing the risk of disability, individuals living with disabilities are at higher risk of IPV. Estimates suggest more than half of women living with disabilities experience some form of IPV in their lifetime and women living with disabilities experience almost double the rate of physical violence than women living without disabilities (Chirwa et al., 2020; Savage, 2021).
Due to both the risk of physical injury accompanying IPV and the high rate of IPV among individuals living with disability, IPV survivors are likely to benefit from rehabilitation. Rehabilitation refers to individualized interventions designed to reduce the impact of health conditions and support individuals in being “as independent as possible in everyday activities,” with interventions often including modifying living or working environments, adapting tasks, or implementing assistive supports (World Health Organization, 2021a). As such, rehabilitation professionals—such as physiotherapists, occupational therapists, speech-language pathologists/therapists, physiatrists/physical medicine, and rehabilitation physicians—are highly likely to encounter IPV survivors in their practice. Though related, each of these professions has specific aims. Occupational therapists (OTs), providing occupational therapy (OT), are “regulated health care professionals who promote health, well-being and quality of life by enabling individuals, families, organizations and communities to participate in occupations that give meaning and purpose to their lives” (Canadian Institutes for Health Information, 2022a). Physiotherapists or physical therapists (PTs), providing physiotherapy (PT), are “regulated, evidence-based, primary health care professionals who aim to prevent, assess and treat the impact of injury, disease and/or disorders in movement and function” (Canadian Institutes for Health Information, 2022b). Speech-language pathologists (SLPs), also referred to as speech therapists and providing speech language pathology (SLP), “work to prevent, assess, diagnose, and treat speech, language, social communication, cognitive-communication, and swallowing disorders in children and adults” (American Speech-Language-Hearing Association, n.d.). Physiatry, or physical medicine and rehabilitation, “is a medical specialty that emphasizes the prevention, diagnosis, treatment and rehabilitation of people disabled by disease, disorder or injury” (Association of Academic Physiatrists, n.d.). Due to the physical nature of their work, rehabilitation professionals are ideally positioned to identify signs of IPV that might otherwise be overlooked, and the trust they can develop with their clients over time gives them an opportunity to create a safe space for disclosure (Ballan & Freyer, 2019; Dalton, 2005; Stancliff, 1997). As such, it is imperative that rehabilitation professionals are equipped with the knowledge to identify IPV survivors and support them appropriately.
Among the physical injuries common among IPV survivors, brain injury is both highly prevalent and often overlooked (Campbell et al., 2022; Haag et al., 2022). Within the context of IPV, the substantial physical, cognitive, and mental health impacts of brain injury are exacerbated and can lead to longer-term disability if left unaddressed (Iverson & Pogoda, 2015; Iverson et al., 2017; Ponsford et al., 2014; Roberts & Kim, 2005; St Ivany et al., 2018; Valera & Berenbaum, 2003). Targeted rehabilitation intervention is critical for individuals with brain injury to achieve optimal outcomes and community integration (Sveen et al., 2022), further supporting the role of rehabilitation professionals with IPV survivors.
To our knowledge, no systematic investigation of rehabilitation for survivors of IPV exists in the published literature. To address this gap, this review explores four rehabilitation professions’ ((physiotherapy [PT], speech language pathology [SLP], and physiatry) knowledge and awareness of and interventions for IPV. Based on the literature identified, this review presents findings on three distinct categories of articles: (1) articles describing or evaluating rehabilitation interventions for IPV survivors; (2) articles assessing rehabilitation professionals’ knowledge or awareness of IPV; and (3) articles outlining opportunities for rehabilitation professionals to support IPV survivors. Given the high rate of brain injury among IPV survivors, the high rates of IPV among individuals living with disabilities including brain injury, and the usefulness of rehabilitation in this context, this review additionally reports on if and when brain injury is considered among articles across the three categories.
Methods
This scoping review was guided by Arksey and O’Malley’s 2005 framework, which was expanded by JBI (formerly the Joanna Briggs Institute) (Peters et al., 2015; Peters et al., 2020) and the Preferred Reporting Items for Systematic Review and Meta-Analysis extension for scoping reviews (Tricco et al., 2018). As recommended by the JBI guidelines, a protocol is available via FigShare, an open science platform (Toccalino, Haag, Babineau, et al., 2022).
Search Strategy
In all, 10 databases were identified in collaboration with an information specialist (JB) and searched for relevant articles using a search strategy including text words and subject headings (e.g., MeSH, Emtree) related to IPV and rehabilitation (see Appendix I). Search terms were informed by previous reviews exploring IPV (Toccalino et al., 2023) or the role of rehabilitation professionals (Chan, Estrella, Baddeliyanage, et al., 2022; Chan, Estrella, Syed, et al., 2022). The search strategy was first developed in Medline (see Appendix I) and subsequently translated to the databases. Database searches were last conducted in May 2022 and were not limited by language, year of publication, or geographic location. A manual search of the reference lists of included studies and scoping or systematic review articles identified through the search was conducted to identify additional relevant literature. A gray literature search of relevant IPV, gender-based violence, and rehabilitation organizations was also conducted to identify reports, policy briefs, clinical guidelines, or other unpublished work relevant to rehabilitation for survivors of IPV. The intention of the gray literature search was to capture existing practices being offered on an ad-hoc basis or under unique circumstances that might not be captured in the overall literature.
Eligibility Criteria
Quantitative, qualitative, or mixed-methods research articles or dissertations/theses reporting primary data; commentaries; policy briefs; and clinical guidelines were included in the review if they met the following criteria:
Describe or evaluate: an intervention provided by selected rehabilitation professionals (PTs, OTs, SLPs, and/or physiatrists an opportunity for intervention by selected rehabilitation professionals OR an educational or awareness intervention for selected rehabilitation professionals related to survivors of IPV AND
Focus on interventions for or about adult survivors of IPV (including domestic violence, dating violence, sex work, and sex trafficking).
Articles focusing on perpetrators of IPV, children, or youth under the age of 18, violence outside of an intimate partner relationship, or interventions provided by professions other than the four of interest (PT, OT, SLP, and physiatry) were excluded. Protocols, conference abstracts, book reviews, and studies conducted on animals were also excluded. Scoping and systematic reviews exploring relevant content were reviewed for relevant articles but were not included.
Records were managed and duplicates were identified and removed using EndNote referencing software. Covidence Systematic Review Software was used to conduct the screening and monitor agreement between the reviewers’ assessments. Two reviewers independently screened titles and abstracts of all records and the full texts of potentially relevant articles based on the eligibility criteria outlined above. A small subset of articles was reviewed prior to commencing screening at each stage to ensure consistent application of inclusion criteria across reviewers. Differences in screening were resolved through discussion and consensus, or in consultation with a third reviewer if needed. Full texts of articles published in a language other than English were translated using Google Translate or DeepL Translate and the translated texts were reviewed. Articles in languages other than English that could not be translated (e.g., scanned text PDFs) were excluded. The PRISMA flow chart of the study selection process is presented in Figure 1.
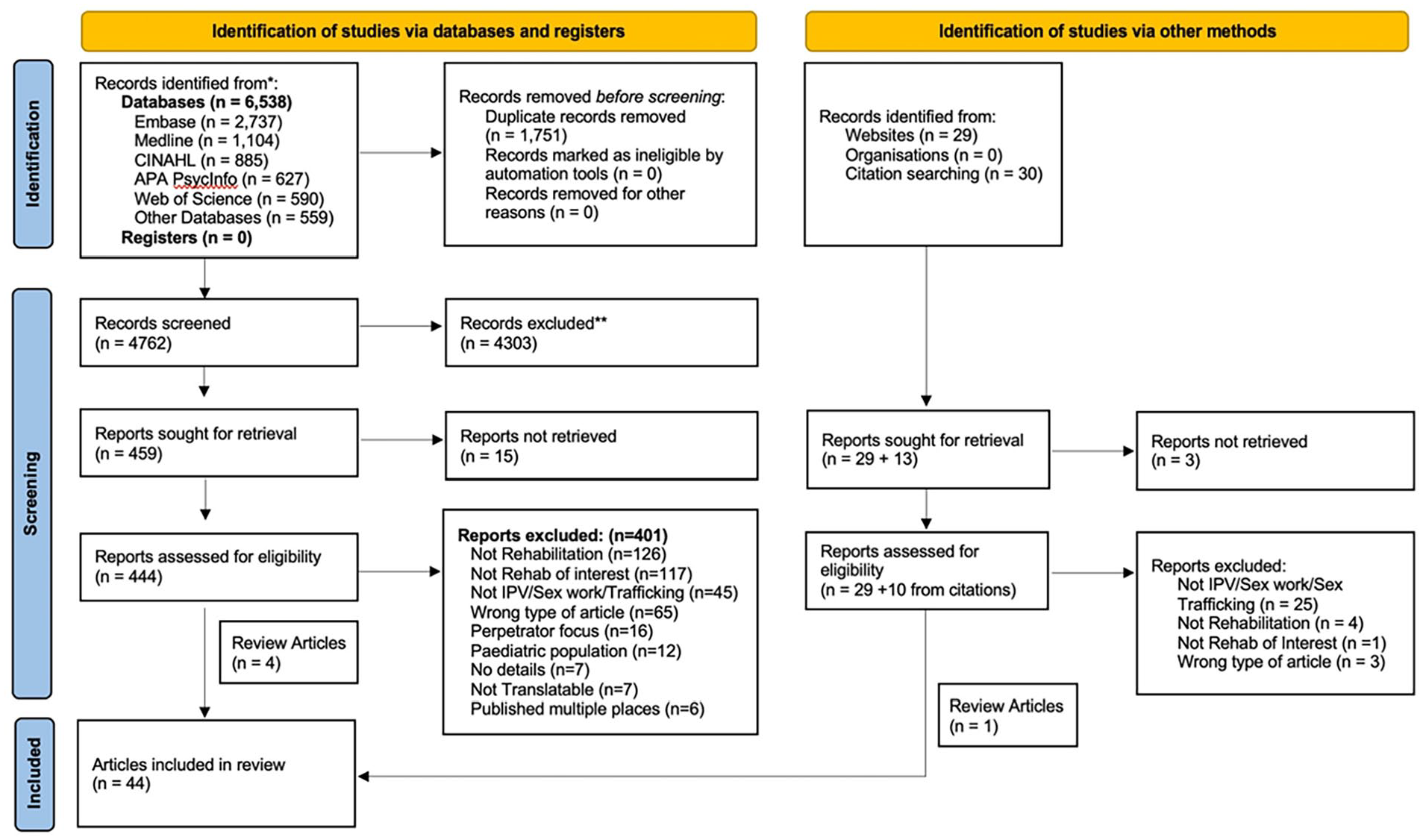
PRISMA flow diagram from Page et al. (2021).
Data Charting and Synthesis
Article characteristics (e.g., year, country, type of article), study characteristics (e.g., setting, population, sample size, participant demographics), and information about the intervention or opportunity (e.g., target population, means of assessment, intervention details, outcomes) were extracted from included studies, with extraction completed by one reviewer and peer reviewed by a second. In addition, we noted if studies considered brain injury, including what assessment tools were used and what proportion of the study population had diagnosed or suspected brain injury. Descriptive statistics were used to convey article characteristics, and narrative synthesis (Popay et al., 2006) was used to synthesize study findings.
Results
The database searches returned 6,538 records, from which the titles and abstracts for 4,762 unique records were reviewed, and 444 full texts were identified for further screening. An additional 29 records were identified through the gray literature search and 30 articles were identified from reference lists. A total of 44 articles met the inclusion criteria and were included in the review (see Figure 1 for a full breakdown). Articles were published between 1996 and 2022, predominantly in peer-reviewed journals (70%, n = 31) and based on data from the United States (86%, n = 38). Approximately half of the articles were primary research articles (48%, n = 21), with the remainder including clinical newsletters (20%, n = 9), commentary or overview-type articles (20%, n = 9), and statements by professional bodies (11%, n = 5), one of which pertained to a legislative bill.
Most included articles discussed opportunities for rehabilitation interventions for survivors of IPV (68%, n = 30). Eight articles (18%) described or evaluated rehabilitation interventions (Cerny et al., 2019; de Oliveira & Ferigato, 2019; Fitzgerald et al., 2017; Gutman et al., 2004; Helfrich & Rivera, 2006; Jones et al., 2021; Mangum et al., 2019; Walton et al., 2017), and seven articles (16%) explored rehabilitation professionals’ knowledge of or attitudes toward IPV (Clark et al., 1996; de Oliveira & Ferigato, 2019; Johnston et al., 2001; Macpherson et al., 2022; Shahgangar, 2004; Sivagurunathan et al., 2019; Williamson et al., 2004). One article touched on both rehabilitation interventions and knowledge and attitudes and is included in both categories (de Oliveira & Ferigato, 2019). Publication of articles discussing opportunities for intervention has been relatively consistent over time, while knowledge articles were more prevalent in the early 2000s and intervention articles have become more prevalent in the last 10 years (Figure 2). Most articles focused on IPV survivors (89%, n = 39), with a small minority focusing on sex trafficking (11%, n = 5 (Cerny, 2016; Cerny et al., 2019; Gorman & Hatkevich, 2016; Mangum et al., 2019; Thompson et al., 2020)). Most of the literature, and all articles focusing on sex trafficking, focused on the role of OTs in supporting survivors. For a summary of article characteristics and participant demographics, see Table 1. None of the included articles explored experiences of gender-diverse or two-spirit individuals, nor did the minority of studies reporting on the race or ethnicity of participants stratify findings or report on implications based on these aspects of identity. In the following sections, findings for each of the three article categories (rehabilitation interventions, knowledge and awareness of rehabilitation professionals, and opportunities for intervention) will be presented, followed by reporting on the recognition of brain injury in this body of literature.
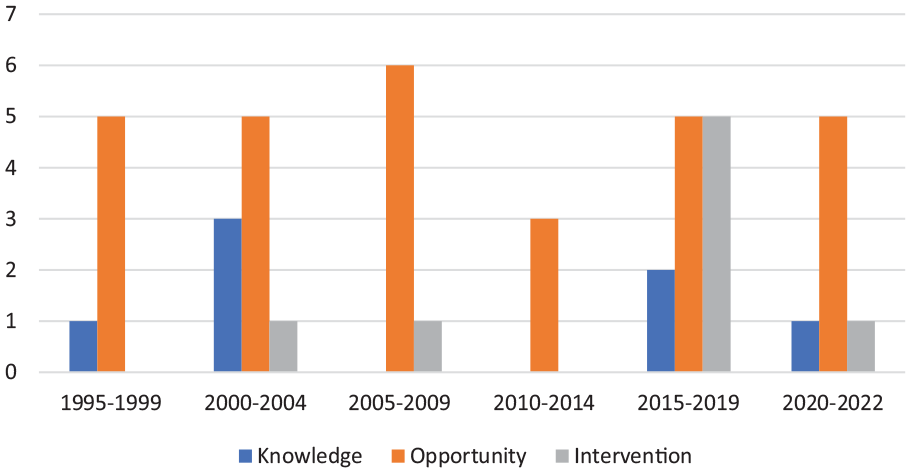
Distribution of articles by year and type.
Summary of Article Characteristics.
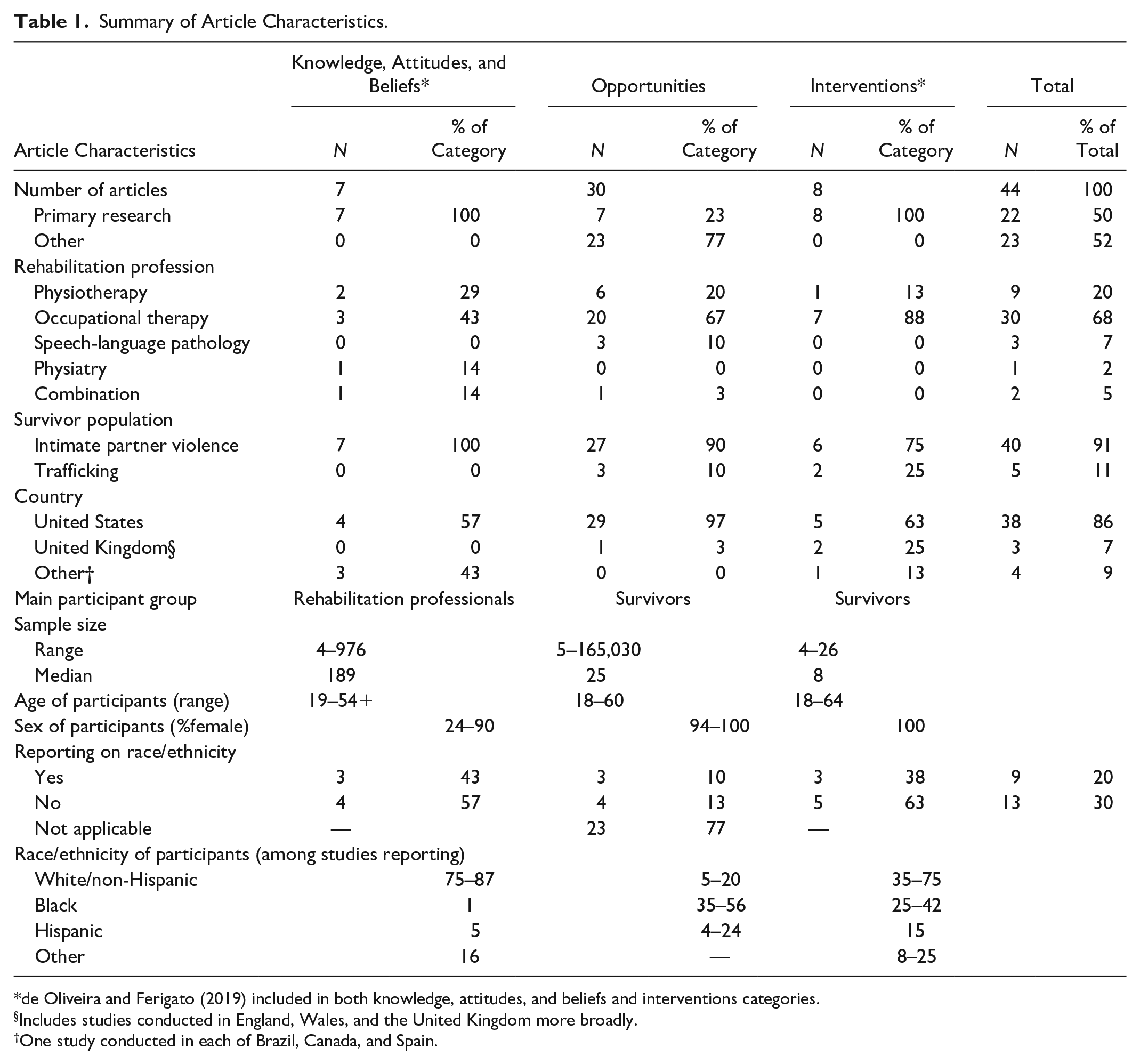
de Oliveira and Ferigato (2019) included in both knowledge, attitudes, and beliefs and interventions categories.
Includes studies conducted in England, Wales, and the United Kingdom more broadly.
One study conducted in each of Brazil, Canada, and Spain.
Rehabilitation Interventions and Outcomes
Eight included studies focused on rehabilitation interventions, predominantly (n = 7, 88%) assessing OT interventions in support settings for survivors of IPV (n = 5) or human trafficking (n = 2). There was a high degree of variability across interventions, consisting of individual and/or group sessions that occurred in frequencies ranging from twice weekly to twice monthly with interventions lasting from several weeks to several months, and sample sizes were relatively low, ranging from 4 to 26. Most of the OT interventions assessed (n = 4, 63%) included individual sessions with intervention objectives highly tailored to the individual needs of participants (Cerny et al., 2019; Gutman et al., 2004; Helfrich & Rivera, 2006; Jones et al., 2021). These tailored interventions covered a variety of topics, but all focused at least in part on life skills such as goal setting, creating routines, communication, and stress or anxiety management. Two studies consisted only of group interventions, one focused on improving executive function (Mangum et al., 2019) and the other on psycho-education to improve self-esteem (Fitzgerald et al., 2017). All studies reporting on outcomes reported significant improvement in the targeted domain and/or high satisfaction among participating survivors; however, participant feedback from one of the shorter interventions suggested a 4-week intervention did not provide enough time to cover topics with the depth survivors wanted (Helfrich & Rivera, 2006). Across studies, there was significant variability in the assessments used and the objectives and delivery of the intervention. A total of 13 assessment tools were used across the nine studies, with the Canadian Occupational Performance Measure (Cerny et al., 2019; Jones et al., 2021; Mangum et al., 2019) and the Occupational Performance History Interview (Fitzgerald et al., 2017; Helfrich & Rivera, 2006) being the only two used more than once. Two additional articles did not discuss specific interventions. One was a broader qualitative exploration of the ways OTs assist survivors of domestic violence within primary care groups, noting the breadth of settings where OTs might support survivors (e.g., community workshops, home visits) and the variety of interventions OTs are equipped to provide (e.g., supporting self-expression related to violence, supporting social participation; de Oliveira & Ferigato, 2019). The final article described the evaluation of an IPV screening assessment for use in a PT clinic, noting strong inter-rater reliability and good construct validity for the tool (Walton et al., 2017). A full summary of rehabilitation intervention articles is shown in Table 2.
Studies Examining Rehabilitation Interventions for Survivors of IPV and Sex Trafficking.
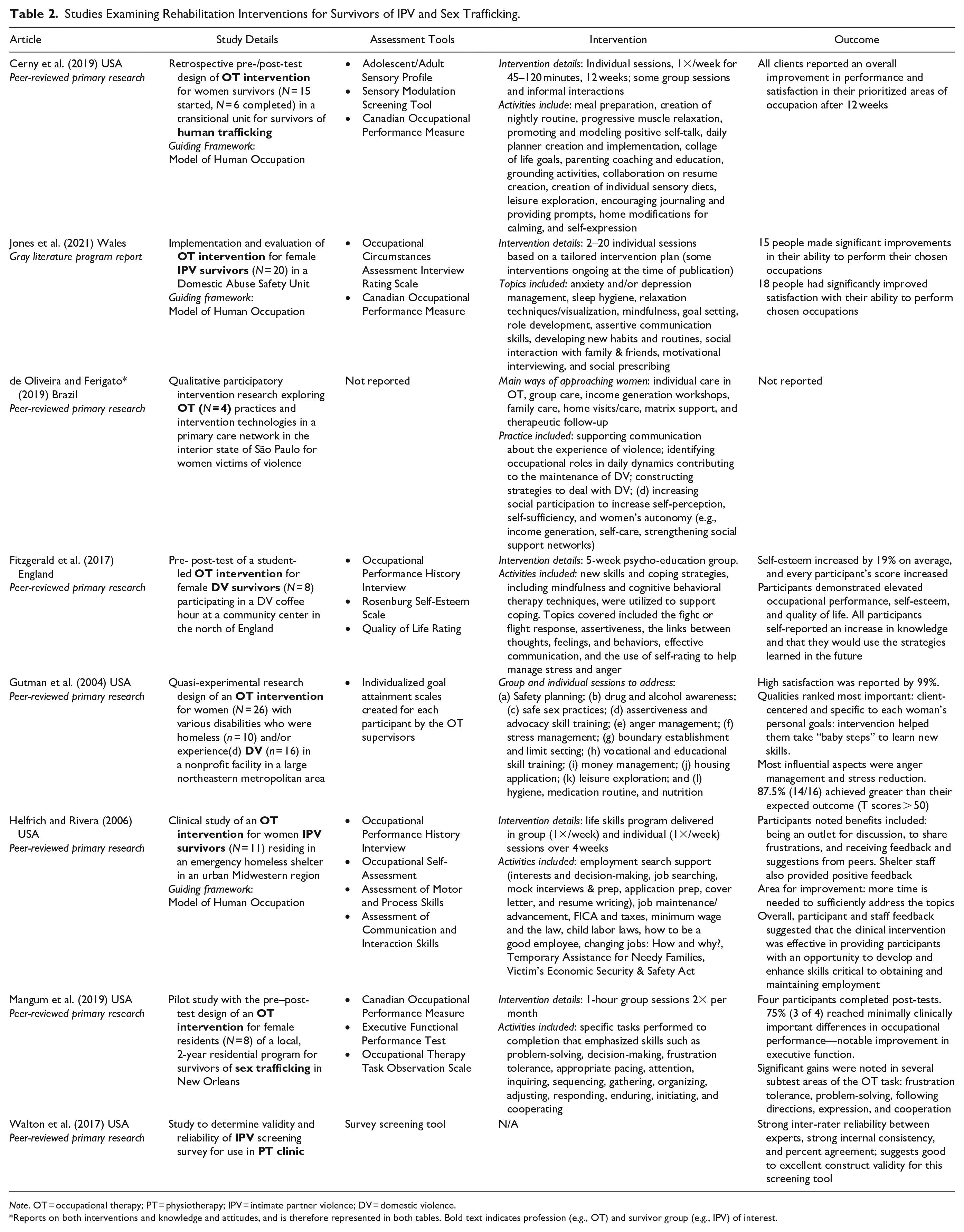
Note. OT = occupational therapy; PT = physiotherapy; IPV = intimate partner violence; DV = domestic violence.
Reports on both interventions and knowledge and attitudes, and is therefore represented in both tables. Bold text indicates profession (e.g., OT) and survivor group (e.g., IPV) of interest.
Assessment of Knowledge and Attitudes of Providers
Seven of the included studies explored knowledge and attitudes about IPV among rehabilitation professionals, with studies predominantly focused on PTs (n = 2), OTs (n = 3), or a combination of the two (n = 1); however, the only study included in this review focusing on physiatrists/physical medicine and rehabilitation physicians was included in this category (Williamson et al., 2004). Most studies (n = 5, 71%) assessed knowledge or attitudes using questionnaires that were adapted from previous studies (Johnston et al., 2001; Shahgangar, 2004; Sivagurunathan et al., 2019; Williamson et al., 2004) and/or developed based on literature reviews (Clark et al., 1996; Johnston et al., 2001). There was minimal overlap in the questionnaires used, though two studies used Tilden et al. (1994) survey on experiences and attitudes toward family violence (Johnston et al., 2001; Williamson et al., 2004). The two remaining studies were a case analysis (Macpherson et al., 2022) and a qualitative exploration using semi-structured interviews (de Oliveira & Ferigato, 2019). Overall, rehabilitation professionals reported being under-prepared to deal with IPV (52-68% of respondents (Johnston et al., 2001; Williamson et al., 2004)) with little to no formal education on the subject (65%–100% of respondents (de Oliveira & Ferigato, 2019; Johnston et al., 2001)). Between 34% and 76% of professionals reported they had not, to their knowledge, encountered IPV survivors or had little experience supporting them within their practice (Johnston et al., 2001; Shahgangar, 2004; Sivagurunathan et al., 2019). When asked, the majority of rehabilitation professionals wanted more information or training about IPV and ways to support survivors (Clark et al., 1996; Shahgangar, 2004), including more knowledge of local laws and services (Williamson et al., 2004). Service providers also preferred practical and team-based approaches to supporting survivors (de Oliveira & Ferigato, 2019; Macpherson et al., 2022). Recommendations across studies focused on the need for more education to be available both through curricula and continuing education opportunities. There was also a noted need for protocols or procedures to help rehabilitation professionals identify IPV among their client base and evaluations of the efficacy of these protocols and the educational programs. A full summary of knowledge and attitudes articles is shown in Table 3.
Studies Examining Knowledge of and Attitudes Toward IPV Among Rehabilitation Professionals.
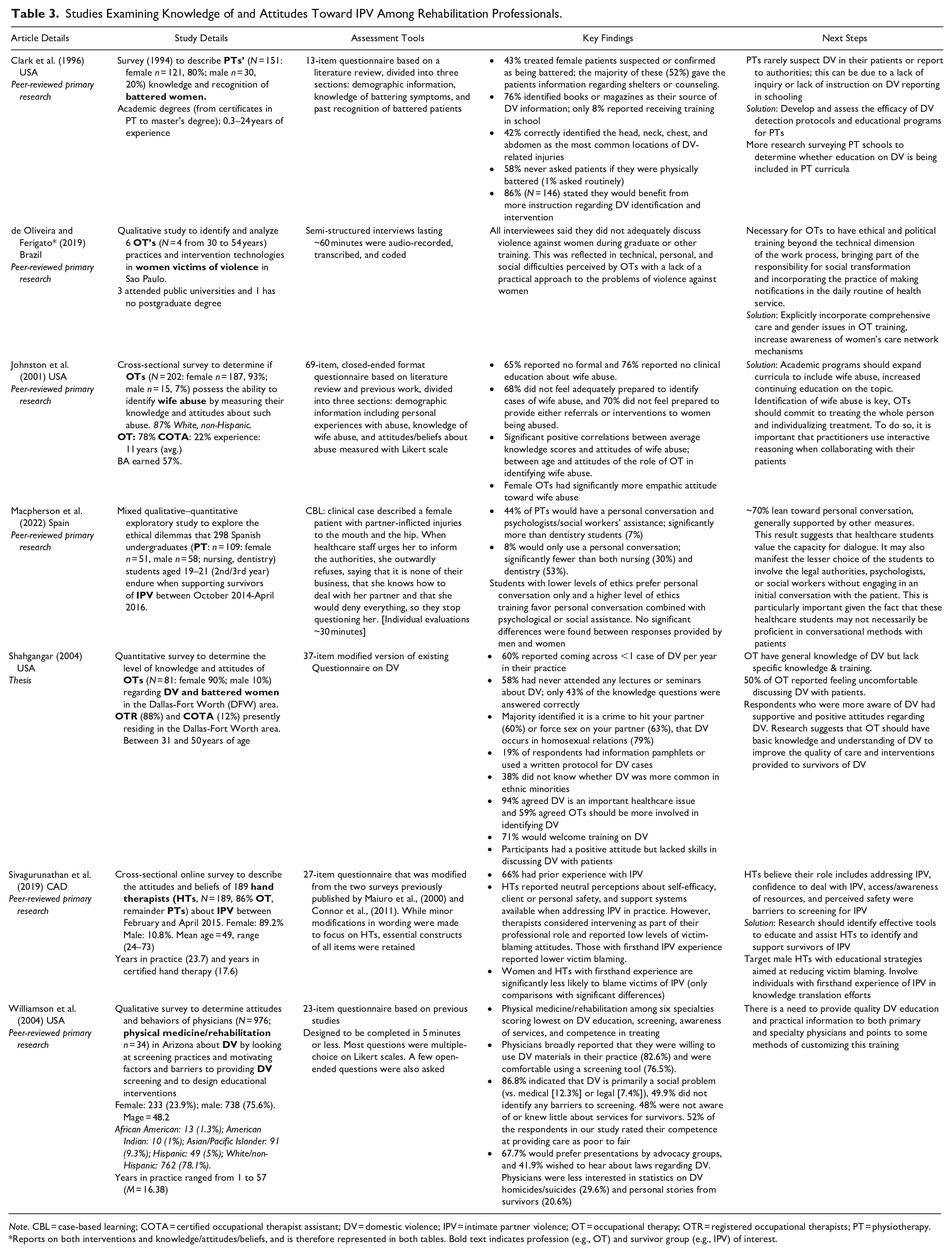
Note. CBL = case-based learning; COTA = certified occupational therapist assistant; DV = domestic violence; IPV = intimate partner violence; OT = occupational therapy; OTR = registered occupational therapists; PT = physiotherapy.
Reports on both interventions and knowledge/attitudes/beliefs, and is therefore represented in both tables. Bold text indicates profession (e.g., OT) and survivor group (e.g., IPV) of interest.
Opportunities for Rehabilitation Interventions
Included articles identified opportunities for rehabilitation professionals to support survivors that broadly grouped into three themes: identification or screening, referral, and support. Identification or screening was discussed in nine of the included articles (Ballan & Freyer, 2021; Dalton, 2005; Foose, 1999; Gaffigan-Bender & Narula, 1998; Gallew, 2004; Helfrich et al., 2001; Johnson, 1997; No Author (APTA Guidelines), 1998; Stancliff, 1997), noting rehabilitation professionals as being in an ideal position to identify survivors because of the nature of the physical assessments they conduct (Ballan & Freyer, 2019; Dalton, 2005; Helfrich et al., 2001; Stancliff, 1997) or the relationship that can be developed between practitioner and client over time (Ballan & Freyer, 2021; Dalton, 2005; Helfrich et al., 2001; Johnson, 1997; Stancliff, 1997). Some authors advocated for embedding screening into routine practice (e.g., Dalton, 2005). Several studies further recommended that individual practitioners or the institutions in which they work should develop and maintain lists of local resources to which they could refer clients when needed (Gallew, 2004; Helfrich et al., 2001; Javaherian, 2006; Javaherian et al., 2007; Javaherian-Dysinger & Underwood, 2011; Javaherian-Dysinger et al., 2017; Johnson, 1997; No Author (APTA guidelines), 1998). In this way, rehabilitation professionals can be prepared to identify and support the survivors who are invariably among their clientele.
Beyond identification and referral, articles discussed many ways in which rehabilitation professionals can support survivors, ranging from relatively small changes within a practice such as having pamphlets on domestic violence available in washrooms or waiting rooms (Helfrich & Aviles, 2001; Javaherian, 2006; Johnson, 1997), to broader institutional changes such as developing procedures or policies regarding IPV or sex trafficking (Ballan & Freyer, 2021; Dalton, 2005; Javaherian, 2006; No Author (APTA Guidelines), 1998). Recommendations for rehabilitation professionals providing care include approaching the conversation in a nonjudgmental way (Gaffigan-Bender & Narula, 1998; Gallew, 2004; Johnson, 1997; Kessler, 2012; Stancliff, 1997), assessing for safety (Helfrich & Aviles, 2001; Koch, 2001; No Author (APTA Guidelines), 1998), and using a trauma-informed approach (Ballan & Freyer, 2019, 2021; Cerny, 2016). At both the individual practitioner level and the institutional level, a collaborative approach to care including rehabilitation professionals, mental healthcare providers, community organizations, and other healthcare providers was encouraged to better support survivors (Ballan & Freyer, 2019, 2021; Foose, 1999; Kessler, 2012). Finally, more education for rehabilitation professionals during their degrees and opportunities for ongoing professional development and training postgraduation were also deemed critical by many authors (Ballan & Freyer, 2021; Cerny, 2016; Dalton, 2005; Gallew, 2004; Javaherian, 2006; Johnson, 1997; No Author (APTA Guidelines), 1998). A full summary of primary research articles and perspective or recommendation articles discussing opportunities for rehabilitation professionals to support survivors is found in Tables 4a and 4b, respectively.
Studies Discussing Opportunities for Rehabilitation Professionals to Support Survivors of IPV and Sex Trafficking (Primary Research Studies).
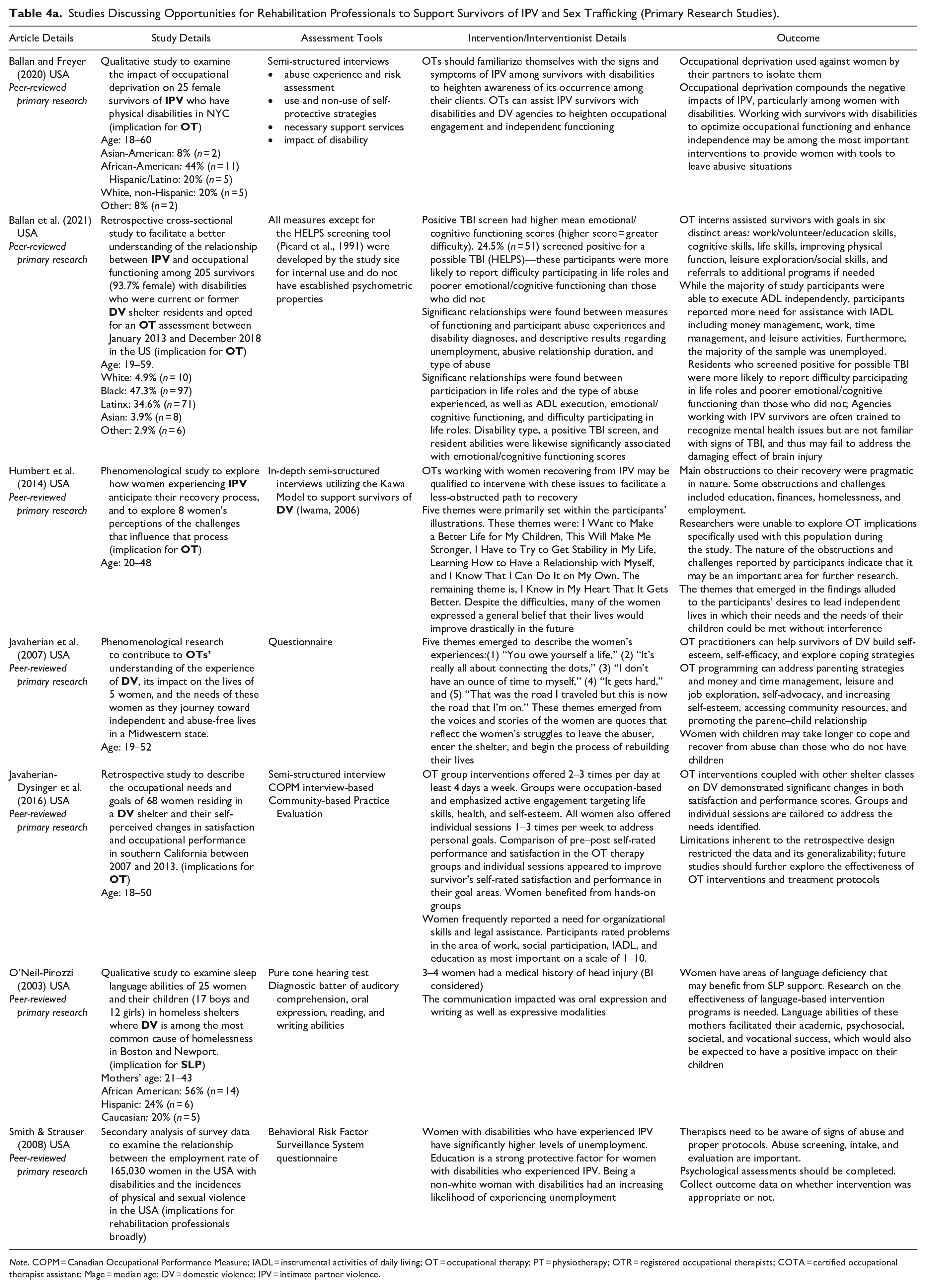
Note. COPM = Canadian Occupational Performance Measure; IADL = instrumental activities of daily living; OT = occupational therapy; PT = physiotherapy; OTR = registered occupational therapists; COTA = certified occupational therapist assistant; Mage = median age; DV = domestic violence; IPV = intimate partner violence.
Studies Discussing Opportunities for Rehabilitation Professionals to Support Survivors of IPV and Sex Trafficking (Perspective Articles).
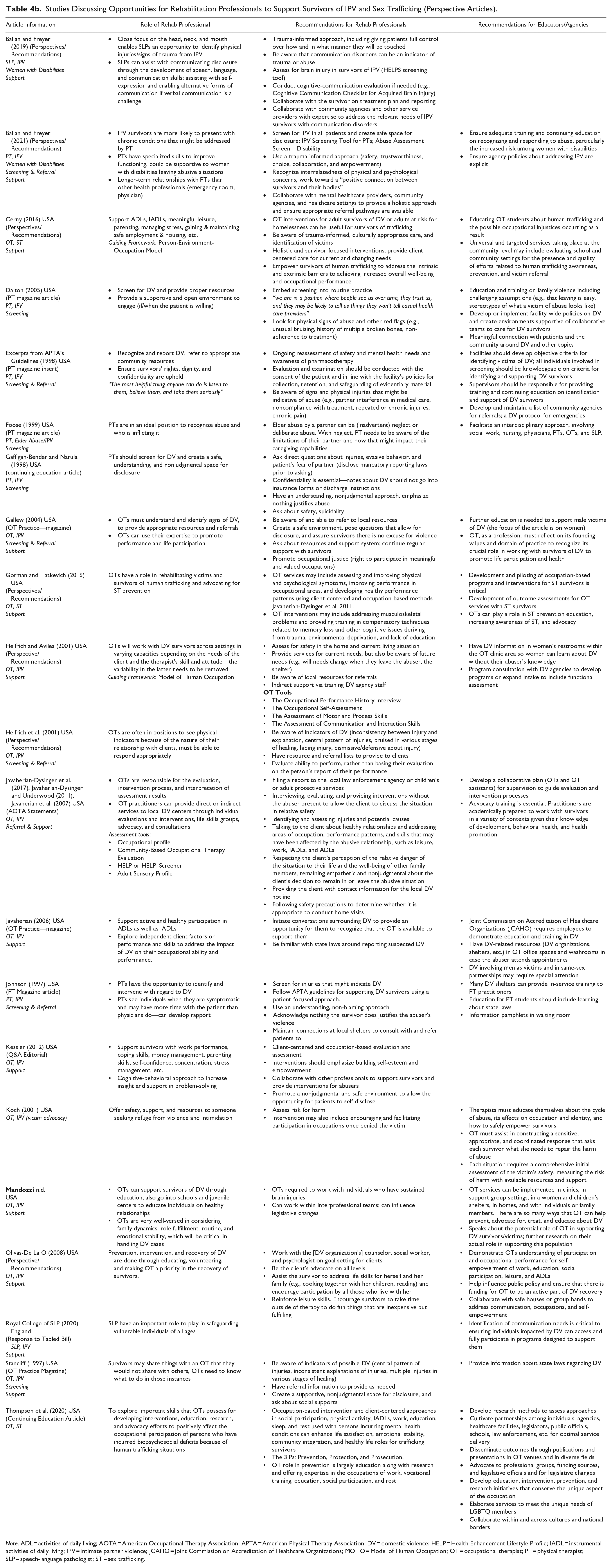
Note. ADL = activities of daily living; AOTA = American Occupational Therapy Association; APTA = American Physical Therapy Association; DV = domestic violence; HELP = Health Enhancement Lifestyle Profile; IADL = instrumental activities of daily living; IPV = intimate partner violence; JCAHO = Joint Commission on Accreditation of Healthcare Organizations; MOHO = Model of Human Occupation; OT = occupational therapist; PT = physical therapist; SLP = speech-language pathologist; ST = sex trafficking.
Identification of Brain Injury
As brain injury, disability, and IPV are highly interrelated and rehabilitation professionals can play a key role in supporting individuals with any or all of these experiences, we additionally reviewed each article to determine whether brain injury was considered. Across categories, there were six studies that focused on women living with disabilities (Ballan & Freyer, 2019, 2020, 2021; Ballan et al., 2021; Gutman et al., 2004; Smith & Strauser, 2008); however, only three specifically discussed brain injury (Ballan & Freyer, 2019; Ballan et al., 2021; Gutman et al., 2004). One additional study, which looked at language functioning among women living in shelters, assessed for brain injury (O’Neil-Pirozzi, 2003). The four articles discussing brain injury are reviewed in the context of their categories below.
Among the intervention articles, only one of eight (13%) mentioned diagnosed or suspected brain injury, noting 19% of the women experiencing domestic violence had sustained a traumatic brain injury substantial enough to receive a diagnosis and medical treatment (Gutman et al., 2004). The authors noted an additional group of women who experienced cognitive impairment with no known cause, which the authors suggest might be a result of the impacts of domestic abuse over time (Gutman et al., 2004). None of the seven articles discussing knowledge or attitudes referred to brain injury or its possible intersections with IPV. Three of the 30 opportunities articles (10%) mentioned brain injury in some way. Two of the primary research articles assessed for brain injury. One identified 25% of their participants screened positive for a possible brain injury using the HELPS screening tool. Participants who screened positive for brain injury were more likely to report difficulty participating in life roles and poorer emotional or cognitive functioning than those who did not (Ballan et al., 2021). In the other primary research article assessing brain injury, authors identified 16% of their sample had experienced at least one head injury, noting that some of the language deficits seen in these individuals may be due to the head injury (O’Neil-Pirozzi, 2003). Finally, one study recommended SLPs assess for brain injury using the HELPS screening tool (Ballan & Freyer, 2019).
Discussion
This systematic scoping review identified 44 articles across peer-reviewed and gray literature addressing knowledge and awareness of and interventions for IPV among rehabilitation professionals. Articles broadly grouped into three categories: rehabilitation interventions for IPV survivors, assessment of rehabilitation professionals’ knowledge of and attitudes toward IPV survivors, and identified opportunities for rehabilitation professionals to support IPV survivors. The eight studies exploring rehabilitation interventions assessed a highly heterogeneous group of predominantly OT interventions that were highly individualized and designed to support life skills and meaningful engagement. Despite the wide range of intervention approaches, each reported high satisfaction among survivors, functional improvements, or both, indicating a highly tailored approach is beneficial and integral to appropriate IPV support. Assessments of knowledge and attitudes explored a broader range of rehabilitation professionals, with three of the four groups of interest (OT, PT, and physiatry) included. Across professions, there was a noted lack of education about IPV, with rehabilitation professionals often reporting feeling underprepared to support survivors. Rehabilitation professionals expressed a desire for more information and training about IPV as well as protocols for identification. The need for education was further emphasized across the articles discussing opportunities, both within training programs and in continuing education initiatives. This included education on adequately identifying survivors of IPV, developing in-depth safety planning, and ensuring that survivors are referred to necessary supports within the community. Several recommendations for practice change were presented in opportunities articles. First, the importance of a nonjudgmental and trauma-informed approach to supporting survivors was emphasized. Articles further suggested that practitioners or the institutions in which they work should be aware of local resources to which they can refer survivors and, whenever possible, strive for collaboration with other disciplines to support holistic care for survivors. Critically, articles emphasized a client-centered approach to service delivery, involving survivors in all aspects of their care planning (Ballan & Freyer, 2019).
Despite increased IPV among individuals living with disability and heightened risk for disability, particularly brain injury, among IPV survivors, only a small minority of studies addressed disability (n = 6, 14%) and/or brain injury (n = 4, 9%), all but one of which focused on opportunities for intervention. Notably, none of the articles assessing knowledge and attitudes of providers considered brain injury or disability, preventing an assessment of how the intersecting stigma may impact the way survivors living with a disability may be perceived. Women living with disabilities experience increased rates of all forms of abuse compared to women living without disabilities and can experience “disability-specific abuse” such as neglecting to provide personal care or tampering with assistive devices (Austin et al., 2014). This disability-specific abuse and other challenges such as the abuser being a primary caregiver can hinder the identification of IPV among individuals living with disabilities (Plummer & Findley, 2012). The use of tailored screening tools, such as the Abuse Assessment Screen for disability, can be incorporated to better support IPV identification among individuals living with a disability. Physical abuse sustained during IPV often targets the head and neck region, increasing the likelihood that survivors may sustain a brain injury, which can lead to disability (Gutman, 2021; Sheridan & Nash, 2007). Rehabilitation professionals must be aware of possible brain injuries in IPV survivors to provide appropriate and tailored support. Therefore, education should also include how and when brain injury screening tools should be used (Ballan & Freyer, 2019).
In many instances, rehabilitation professionals are the first point of contact for survivors of IPV and were identified as well positioned to screen for and identify survivors (Dalton, 2005). Providing adequate screening and intervention is crucial to ensure survivors are receiving the support that they need. Furthermore, it is imperative that education and training among rehabilitation professionals and within organizations reflect the complex nature of IPV and includes awareness and specified screening tools for survivors of IPV, including survivors with disabilities and/or brain injury, to ensure that widespread and inclusive support is provided. Several promising practices were identified to assist rehabilitation professionals in supporting IPV survivors including building flexible programs that can be tailored to a survivor’s specific needs, building IPV education into rehabilitation training for professionals, and developing local networks of resources to which they can refer survivors. This review affirmed the dearth of brain injury-sensitive rehabilitation services available to IPV survivors with very few rehabilitation professionals screening or otherwise accounting for brain injury in the included studies. This is especially noteworthy, as many psychological and physiological issues found in IPV survivors have been traditionally associated with the severity of abuse or posttraumatic stress disorder when these challenges may instead be a result of sustaining one or multiple brain injuries (Banks, 2007; Kwako et al., 2011). There is a pressing need for further education, training, and awareness on brain injury considerations in IPV as well as survivors of IPV with disabilities among rehabilitation professionals.
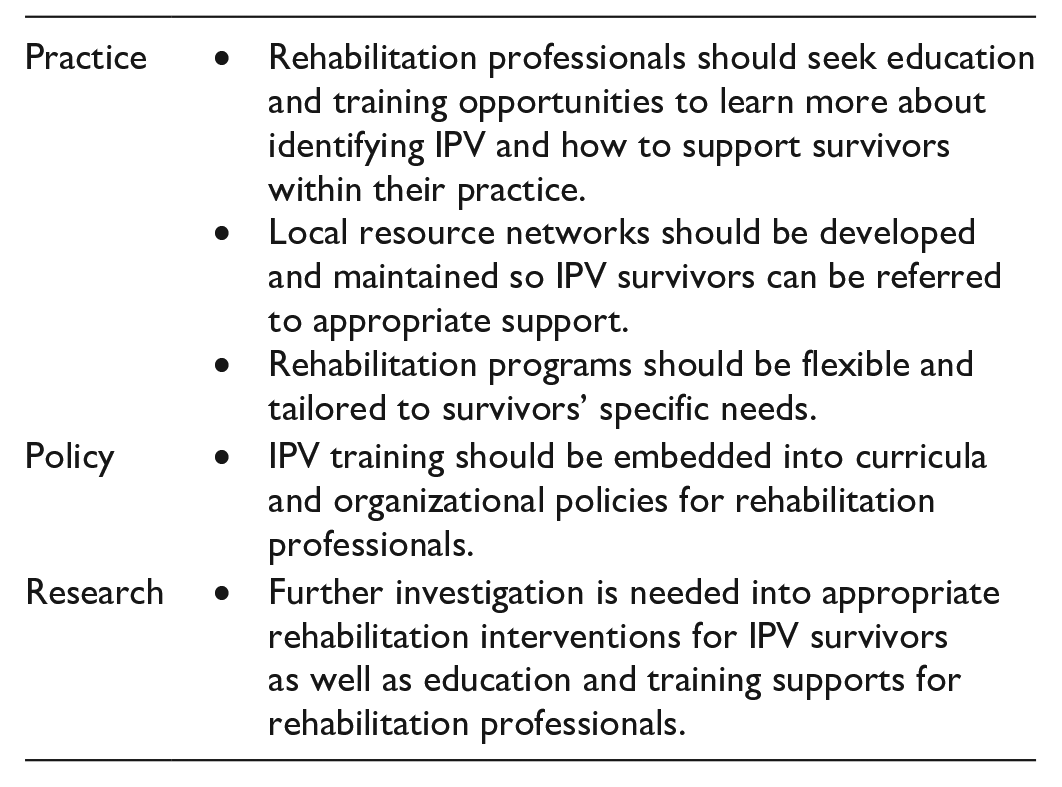
Recommendations
The need for increased awareness and opportunities for education is a well-documented recommendation for service providers supporting IPV survivors (e.g., Goicolea et al., 2015; Haag et al., 2019; Monahan & O’Leary, 1999; St Ivany & Schminkey, 2016; Toccalino, Haag, Estrella, Cowle, Fuselli, Ellis, Colantonio, 2022). While this need is echoed in this review, we recognize putting this burden on individual providers, on top of the demand of their existing duties, is unlikely to affect systemic change. We therefore propose three system-level changes to better support rehabilitation professionals throughout their training and careers. First, we call on educational institutions to review and revise their curricula to ensure all rehabilitation professionals graduate with at least some awareness of IPV and its connection with brain injury. While we recognize training programs already cover a large volume of content, IPV can be woven into existing aspects of curricula, for example, when learning about disability. Second, we encourage accreditation bodies responsible for continuing education credits to include and promote offerings covering IPV. Most accreditation bodies require a minimum number of continuing education credits on an annual or bi-annual basis. Promoting content that includes or focuses on IPV is one way to support professionals in the workforce gain awareness and skills to support survivors. Finally, we call for cross-sectoral collaboration both within healthcare and between healthcare and IPV services. For organizations such as hospitals or community health clinics who already work in multidisciplinary teams, we encourage engagement with local women’s shelters and IPV services both to support rehabilitation professionals in better supporting IPV survivors and to provide IPV service providers places to refer survivors for rehabilitation-related support. This type of engagement can also be pursued at the individual level, with rehabilitation professionals developing their own networks of other healthcare and IPV service providers. Critical to this collaboration is adequate funding to support the time necessary to develop and maintain these relationships (Toccalino, Haag, Estrella, Cowle, Fuselli, Ellis, Gargaro, et al., 2022).
We further would encourage individual rehabilitation professionals to consider the possibility of IPV among the individuals they support who are living with disability and/or who have experienced brain injury. For rehabilitation professionals already working with IPV survivors, we would encourage them to consider the possibility of brain injury. Finally, we challenge rehabilitation professionals to put aside any assumptions they might have about who experiences IPV—individuals across genders, ethnicities, and economic or social statuses experience IPV.
Future Directions
Through this review, we identified several promising directions for future research. Very few of the included studies reported on race or ethnicity among study participants and none of the included articles discussed the potential impacts of racism, racialization, or culture, either among survivors or rehabilitation professionals. A recent scoping review investigating integrated care pathways for Black persons reported differential access to and lower quality rehabilitation care for Black people than white people in several included studies (Omar et al., 2023). The authors of studies included in the review discussed systemic inequalities, racial prejudices, and biases as contributors to this differential access, factors that Omar et al. (2023) note describe anti-Black racism. Recognizing, naming, and understanding the impacts of anti-Black, anti-Indigenous, and other forms of racism on IPV survivors seeking rehabilitation are critical to dismantling systems of oppression and providing equitable care.
All articles identified in this review focused exclusively or predominantly on women or female survivors, in most cases with men or males as perpetrators of the abuse. Though some studies noted that men and gender-diverse individuals experience IPV and that IPV can occur outside of heterosexual relationships, none specifically explored rehabilitation among these groups, indicating an opportunity for future research.
While the volume of articles discussing opportunities for rehabilitation professionals to support survivors indicates an awareness of IPV, only a small subset of the articles in this review discussed specific interventions for IPV survivors with very little overlap in assessment tools or approaches, suggesting more research is required to determine what works for survivors and under what circumstances. Furthermore, only a small subset of articles explored the knowledge and attitudes of rehabilitation professionals, most of which were published more than 15 years ago, before the acknowledgment of IPV as a public health crisis. More investigation into what rehabilitation professionals know and believe about IPV and how training programs can better support them in supporting survivors is warranted, both broadly and in the more specific contexts of disability and brain injury.
Finally, the overwhelming majority of literature included in this review centered on OTs as a profession. Future work to support PTs, SLPs, and physiatrists in their care of IPV survivors, as well as more work on how these professions can work together in supporting survivors would be beneficial. Encouragingly, we are aware of a forthcoming resource for SLPs on supporting IPV survivors, suggesting that awareness is growing (Wiseman-Hakes et al., In Press).
Strengths and Limitations
To our knowledge, this review is the first systematically conducted, peer-reviewed synthesis of the literature exploring the role of rehabilitation professionals for survivors of IPV and sex trafficking. Our search strategy spanned 10 databases and included a search of gray literature, increasing the breadth of article types identified. Furthermore, there were no date, language, or geographic restrictions placed on the search. Translation services were used to ensure articles published in languages other than English were not automatically excluded and to broaden the scope of included articles.
As with any review, the findings presented here are limited by the literature included. Most of the primary research articles had small or convenience samples and there was little overlap in the assessments used across studies, limiting the ability of this review to compare findings or identify best or promising practices. Furthermore, many of the included articles were published more than 15 years ago, before the acknowledgment of IPV as a public health crisis. Finally, 86% of the articles included were conducted in the United States, and 68% were centered on OTs, which may limit the generalizability of findings to other health systems, professions, or settings.
Conclusions
PTs, OTs, SLPs, and physiatrists are highly likely to encounter survivors of IPV and sex trafficking in their practice and are in a prime position to provide support and care. Given this opportunity, it is imperative that in addition to being well-placed, these professionals are well equipped to aid in IPV survivor rehabilitation. Despite the identifiable gaps in the literature, in research, and practice concerning IPV survivors, vital information was gathered on roles that rehabilitation professionals presently engage in when supporting IPV. This review suggests numerous recommendations that rehabilitation professionals can utilize to ensure that IPV-specified programs or supports are incorporated within their practices.
Critical Findings
There is both an opportunity and a need for rehabilitation professionals to support IPV survivors.
Generally, rehabilitation professionals report being underprepared to support IPV survivors; they require more education and training to confront biases and be better able to identify and support survivors.
Interventions for IPV survivors to support life skills, activities of daily living, and meaningful engagement are positively received and result in improvements in the areas being addressed.
Implications for Practice, Policy, and Research
Supplemental Material
sj-docx-1-tva-10.1177_15248380231196807 – Supplemental material for Exploring the Relationships Between Rehabilitation and Survivors of Intimate Partner Violence: A Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380231196807 for Exploring the Relationships Between Rehabilitation and Survivors of Intimate Partner Violence: A Scoping Review by Danielle Toccalino, Gifty Asare, Jenna Fleming, Joyce Yin, Amy Kieftenburg, Amy Moore, Halina (Lin) Haag, Vincy Chan, Jessica Babineau, Nneka MacGregor and Angela Colantonio in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380231196807 – Supplemental material for Exploring the Relationships Between Rehabilitation and Survivors of Intimate Partner Violence: A Scoping Review
Supplemental material, sj-docx-2-tva-10.1177_15248380231196807 for Exploring the Relationships Between Rehabilitation and Survivors of Intimate Partner Violence: A Scoping Review by Danielle Toccalino, Gifty Asare, Jenna Fleming, Joyce Yin, Amy Kieftenburg, Amy Moore, Halina (Lin) Haag, Vincy Chan, Jessica Babineau, Nneka MacGregor and Angela Colantonio in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We would like to acknowledge the support of Nicole Fontyn-Taylor for providing feedback on drafts of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is currently being supported through the Public Health Agency of Canada’s investment Preventing and Addressing Family Violence—The Health Perspective. The views expressed herein do not necessarily represent the views of the Public Health Agency of Canada. This research was supported, in part, by the Canada Research Chairs Program funding (CRC-2019-00019).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.