
Abstract
Trauma-informed care (TIC) is an approach to care emerging in research and in practice that involves addressing the needs of individuals with histories of trauma. The aim of this scoping review was to examine the current literature relating to TIC interventions used in pediatric mental health inpatient and residential settings. We sought to answer the following two research questions: (a) What are the TIC interventions used in pediatric inpatient and residential treatment mental healthcare settings and what are their components? and (b) What are the implementation goals and strategies used with these TIC interventions? We conducted this scoping review according to JBI (formerly Joanna Briggs Institute) methodology for scoping reviews. We included any primary study describing a TIC intervention that was implemented at a specific site which identified and described implementation strategies used. Of 1,571 identified citations and 54 full-text articles located by handsearching, 49 met the eligibility criteria and were included, representing 21 distinct TIC interventions. We present the reported aim, ingredients, mechanism, and delivery (AIMD) of TIC interventions as well as the implementation goals and strategies used, which varied in detail, ranging from very little information to more detailed descriptions. In the context of these findings, we emphasize the complexity of TIC and of TIC interventions, and the importance of identifying and clearly reporting TIC intervention goals, intervention details, and implementation strategies. We suggest applying intervention frameworks or reporting guidelines to support clear and comprehensive reporting, which would better facilitate replication and synthesis of published TIC interventions.
Background
Trauma-Informed Care
“Trauma-informed care” (TIC) is a philosophy that involves addressing the needs of individuals with histories of trauma, whether they are the ones seeking care, or providing care (Fallot & Harris, 2009). Generally agreed upon assumptions of TIC include the four R’s: Realizing the prevalence of trauma, Recognizing manifestations of trauma, Responding appropriately to trauma, and Resisting Re-traumatization. Additionally, many apply the seven principles of TIC: safety (physical and psychological), trustworthiness and transparency, peer support, collaboration and mutuality, empowerment, voice and choice, and cultural, historical, and gender considerations (e.g., Fallot & Harris, 2009; Substance Abuse and Mental Health Services Administration (SAMHSA), 2014). Yatchmenoff et al. (2017) reduce these principles to three common elements: safety, power, and self-worth. For an organization to be trauma-informed, the culture of the organization must reflect the above principles in every interpersonal contact, setting, and relationship, as perceived by both staff and consumers (Fallot & Harris, 2009). Furthermore, it is important that organizations consider every patient and staff member as though they may have trauma histories, an approach known as ‘universal precautions’ (Elliott et al., 2005; Harris & Fallot, 2001).
Trauma-Informed Care in Pediatric Mental Health Settings
Extensive research has linked childhood exposure to trauma and maltreatment with higher rates of physical and mental disorders and healthcare use (e.g., Chu, 2011; Cuijpers et al., 2011; Felitti, 2009; Felitti et al., 1998; Huffhines et al., 2016). A chart review of pediatric psychiatric inpatient hospitalizations was conducted over a 10-month period (Keeshin et al., 2014). The authors found that children and adolescents with a history of maltreatment were more likely to be diagnosed with multiple disorders than youth without a history of trauma (physical abuse adjusted odds ratio = 1.93, p < 0.001; sexual abuse adjusted odds ratio = 2.97; p < 0.001; Keeshin et al., 2014). These authors identified that physical and sexual abuse histories in patients were also independently associated with increased length of stay by 2.3 days (F(3, 1075) = 9.2, p < 0.001; Keeshin et al., 2014), all highlighting the need for trauma-informed services in pediatric mental health settings. Additionally, there may be unique factors to consider in addressing trauma in children and youth within pediatric-specific contexts, such as developmental considerations and relationships between youth and adult caregivers (Lowenthal, 2020).
We identified three recent reviews of TIC interventions (TICI) in pediatric mental health settings (Bailey et al., 2019; Bryson et al., 2017; Lowenthal, 2020). Bailey et al. (2019) systematically reviewed the empirical evidence for organization-wide TICI in out-of-home care published from 2002 to 2017. The authors identified three TICI across seven studies: Attachment Regulation and Competency framework (3 studies), Children and Residential Experiences programme (1 study), and The Sanctuary Model (3 studies) (Bailey et al., 2019).
Bryson et al. (2017) conducted a realist review of implementation strategies of organization-wide TICI in child and adolescent inpatient psychiatric and residential settings including literature from 2000 to 2015. Across 13 articles, they identified five primary factors relating to successful TIC implementation: (a) senior leadership prioritizing TIC, (b) aligning organizational policies and practices, formal and informal, with the principles of TIC, (c) listening to patients’ and families’ experiences, needs, and priorities, (d) supporting staff through training and providing ongoing supervision, coaching, and debriefing, and (e) reviewing data and outcome indicators to foster continuous improvement.
Finally, Lowenthal (2020) performed a scoping review to describe the characteristics of TIC implementation research in child and youth serving sectors. Consistent with the previous reviews, Lowenthal (2020) included only articles that reported results of the TIC implementation initiative. They included 54 articles published between 2004 and 2019, 17 of which were identified as psychiatric inpatient or residential treatment settings. Lowenthal (2020) classified implementation interventions as limited change initiatives (e.g., one-off training with little follow-up), moderate change initiatives (e.g., using a few different types of initiatives over a moderate period of time), and comprehensive change initiatives (e.g., using a multifaceted approach over longer periods of time to support changes in the organizational culture, structure, and policies). This review highlighted the lack of details available in the included studies pertaining to the actual TICI and their implementation strategies.
These three reviews provide preliminary evidence to support organizations wishing to implement TICI in pediatric mental health settings. Yet, the theoretical and practical aspects of TICI remain unclear, particularly as they relate to how TICI are implemented or operationalized in pediatric settings. Authors of these reviews limited their literature searches to articles which reported evaluative results (of the TICI and/or the implementation strategies), and none reported, in detail, the components of each of the TICI nor the implementation strategies used at each site. The most recent review by Lowenthal (2020) provided an overview of the methodological approaches used, geographical locations, and service sectors related to each intervention, however, lacked descriptive details pertaining to the TICI (i.e., what was the actual TIC intervention). The author classified the scope of the TICI implementation initiatives, yet did not clearly describe the criteria, nor the basis for the criteria, for the classification decisions. Furthermore, the article did not include a comprehensive summary of the implementation strategies used within each study.
Research Questions
Within this review, we sought to answer the following research questions: What are the TICI used in pediatric inpatient and residential treatment mental healthcare settings and what are their components? What are the implementation goals and strategies used with these TICI?
Method
Protocol, Registration, and Reporting Methods
This scoping review was conducted according to JBI (formerly Joanna Briggs Institute) methodology for scoping reviews (Peters et al., 2020) guided by an a priori protocol in Open Science Framework (Stokes et al., 2020). We report this review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) (checklist in Appendix A) (Tricco et al., 2018).
Search Strategy
We applied the three-step search strategy recommended by JBI for scoping reviews (Peters et al., 2020). First, we conducted a pilot search of one of the relevant databases (MEDLINE), designed by the first author (YS) in collaboration with a library scientist (MS). YS subsequently performed an analysis of the text words contained in the titles and abstracts of the identified papers and of the respective descriptive index terms. Second, YS designed a second search, including all the identified keywords and index terms. We performed this search in CINAHL, MEDLINE, and PsycINFO on September 2, 2020. A library scientist (MS) peer reviewed the search strategy in accordance with the Peer Review of Electronic Search Strategies (PRESS) guidelines (Mcgowan et al., 2016). Third, YS screened the reference lists of all included studies for additional studies. The full electronic search strategy for Medline is found in Figure 1 and all search strategies are available through the Open Science Framework (Stokes et al., 2020).
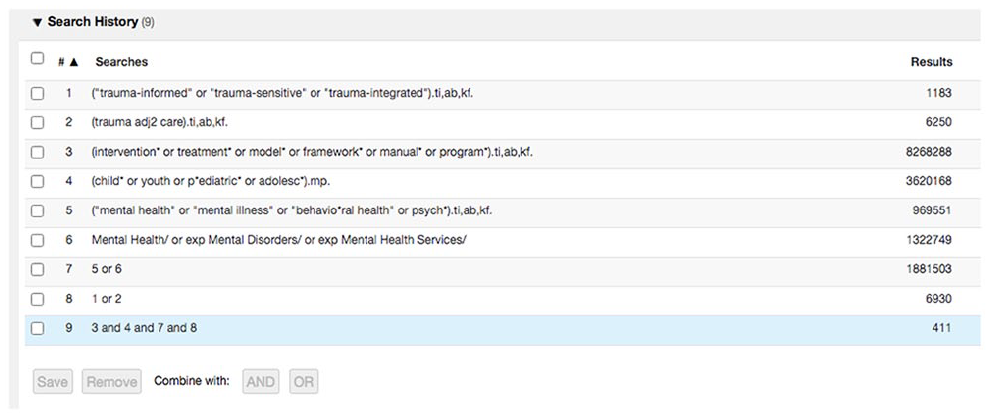
Search strategy in Medline.
Eligibility Criteria
Study Selection
YS uploaded all citations and abstracts to Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia; available at www.covidence.org) and removed duplicates. Two reviewers (YS and MDV) independently screened studies for eligibility using Covidence. We initially conducted a pilot test by screening a random sample of 25 titles/abstracts for inclusion, and then met to discuss discrepancies and to modify the inclusion criteria, if required. Articles were excluded if both reviewers agreed to exclude them, otherwise, they proceeded to the next step of full-text screening. Reviewers met to resolve conflicts, and a third team member (EH or IDG) resolved conflicts as needed. The reviewers then independently screened the remaining full texts in a similar fashion. Articles were excluded if both reviewers agreed to exclude them, and reasons for exclusion were documented. Systematic reviews and scoping reviews meeting first-level screening were retained and YS screened their reference lists for eligible studies.
Data extraction
Two reviewers (YS and JG or MDV or MH) independently extracted study details from the included articles into a template form in REDcap (Research Electronic Data Capture; Harris et al., 2009). We pilot-tested the extraction process as follows: each reviewer independently extracted the data for six articles and then met to compare and reach consensus. At that time, we discussed and revised the forms prior to continuing with the rest of the data extraction. Any disagreements between reviewers’ extractions were resolved through discussion, or with a third reviewer when needed.
We extracted the following data items: study characteristics (first author, study year, year of publication, journal, language, country, corresponding author, study type, study funding, study limitations); study authors’ definition of TIC (verbatim) and reported theoretical underpinnings of TIC; study aims; setting details (type of setting, treatment population of setting, location, urban/ rural location); descriptors of TIC intervention participants, including patients, families, full-time equivalent (FTE) of staff; intervention and implementation strategy details, as described below.
We used the AIMD framework (Aims, Ingredients, Mechanism, Delivery; see Table 1 for definitions) (Bragge et al., 2017) to guide the extraction of information about the TICI and implementation strategies using the following process: Two reviewers (YS and JG) independently extracted the data from each article into Microsoft Word tables and extracted in the same manner any specified goals of the implementation strategies, and any information regarding theory or frameworks used to guide the implementation of the TIC intervention. We resolved discrepancies through consensus.
AIMD Definitions.
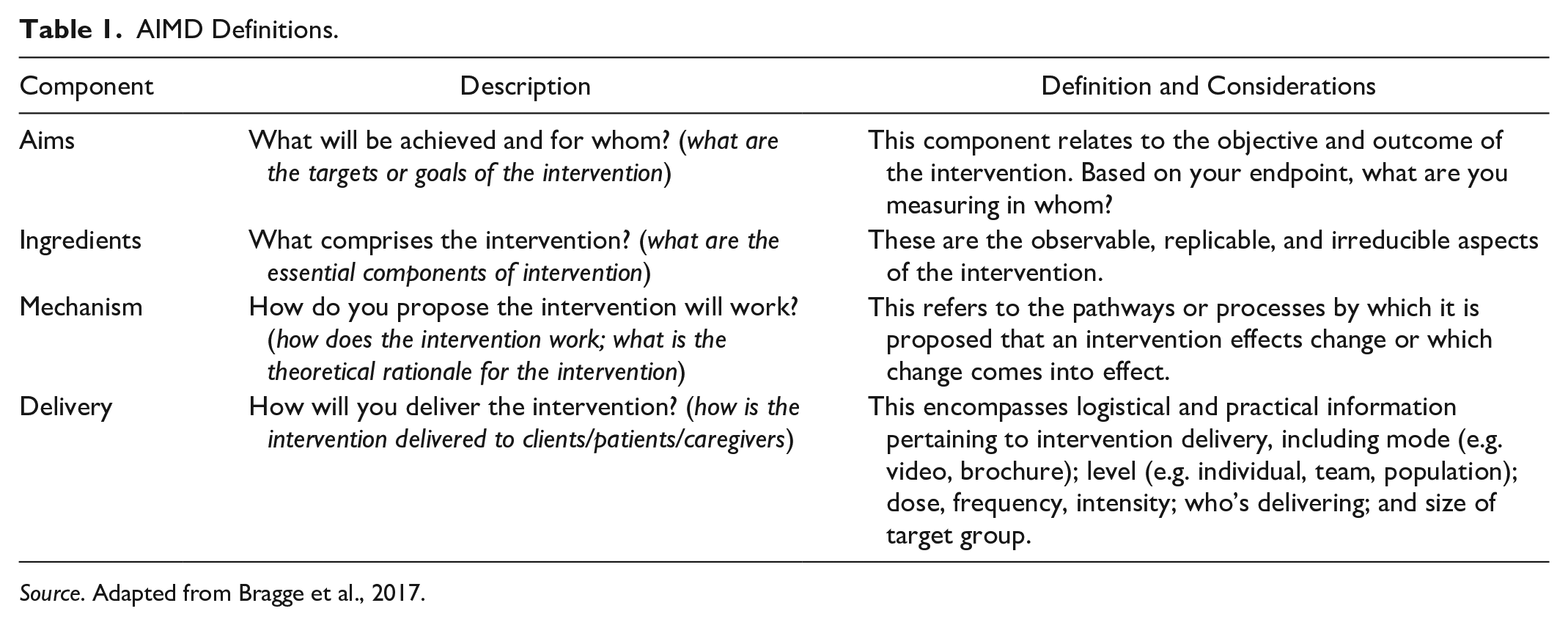
Source. Adapted from Bragge et al., 2017.
Data Analysis
TICI
We aggregated multiple reports on the same TICI, so that each intervention was a unit of interest in the review. We used synthesis tables and descriptive summaries to report on the article characteristics, the TICI characteristics, and the implementation strategies. Two reviewers (YS and JG) independently and (subsequently) collaboratively distilled and summarized the AIMD tables. We compared similarities and differences between the reported interventions and performed a high-level content analysis of TICI objectives.
Goals of implementation strategies
We categorized the goals of the implementation strategies based on the Canadian Institutes of Health Research (CIHR, 2012) categories for knowledge translation (KT) planning goals.
Implementation strategies
We categorized implementation strategies based on the 73 implementation categories defined by the Expert Recommendations for Implementing Change (ERIC; Powell et al., 2015), incorporating the updates recommended for existing category names and definitions as well as three additional categories (Perry et al., 2019), and using Waltz et al. (2015) thematic classification system. YS and JG independently applied the ERIC strategies and implementation goal categories, and discrepancies were resolved with IDG and KBL. We inductively identified an additional category named (77: “Align with organizational or government mandate”) to incorporate a strategy that was not otherwise captured. The four additional categories (three added by C.K. Perry and colleagues, one added by our team) were not included in Waltz and colleagues’ thematic classification system and were therefore labeled as “not categorized.” Throughout this article we will refer to the ERIC implementation categories as the ERIC implementation strategies. We tabulated frequency counts of the ERIC implementation strategies, the ERIC thematic classifications, and the implementation goal strategies and presented summaries in table formats. All categorical synthesis used simple content analysis, in accordance with the JBI guide.
Results
Of 1,571 identified citations and 54 full-text articles located by handsearching, 49 met the eligibility criteria and were included (Figure 2). The earliest article identified was published in 2003 (regarding the Sanctuary Model), with more than one third (n = 19, 39%) published since 2016. In Table 2 we present the characteristics of the 49 included articles. Most articles (n = 41, 84%) were conducted in the USA, while a few were based in Canada (n = 3, 6%) and Australia (n = 4, 8%), and one article (2%) included sites from Canada, Scotland, and USA. Most articles (n = 39; 80%) contained non-experimental study designs, and 20% of articles (n = 10) used experimental or quasi experimental designs. Most intervention sites were residential treatment/congregate care treatment settings (n = 28, 57%), followed by inpatient psychiatric hospital settings (n = 9, 18%). Two articles (4%) reported on both inpatient and residential treatment sites, five articles (10%) were of statewide initiatives, and three articles (6%) were set in child welfare systems that incorporated residential treatment. One article (2%) took place in a mental health treatment unit within a juvenile justice setting, and one (2%) was public health unit intervention which included staff from pediatric psychiatric facilities.
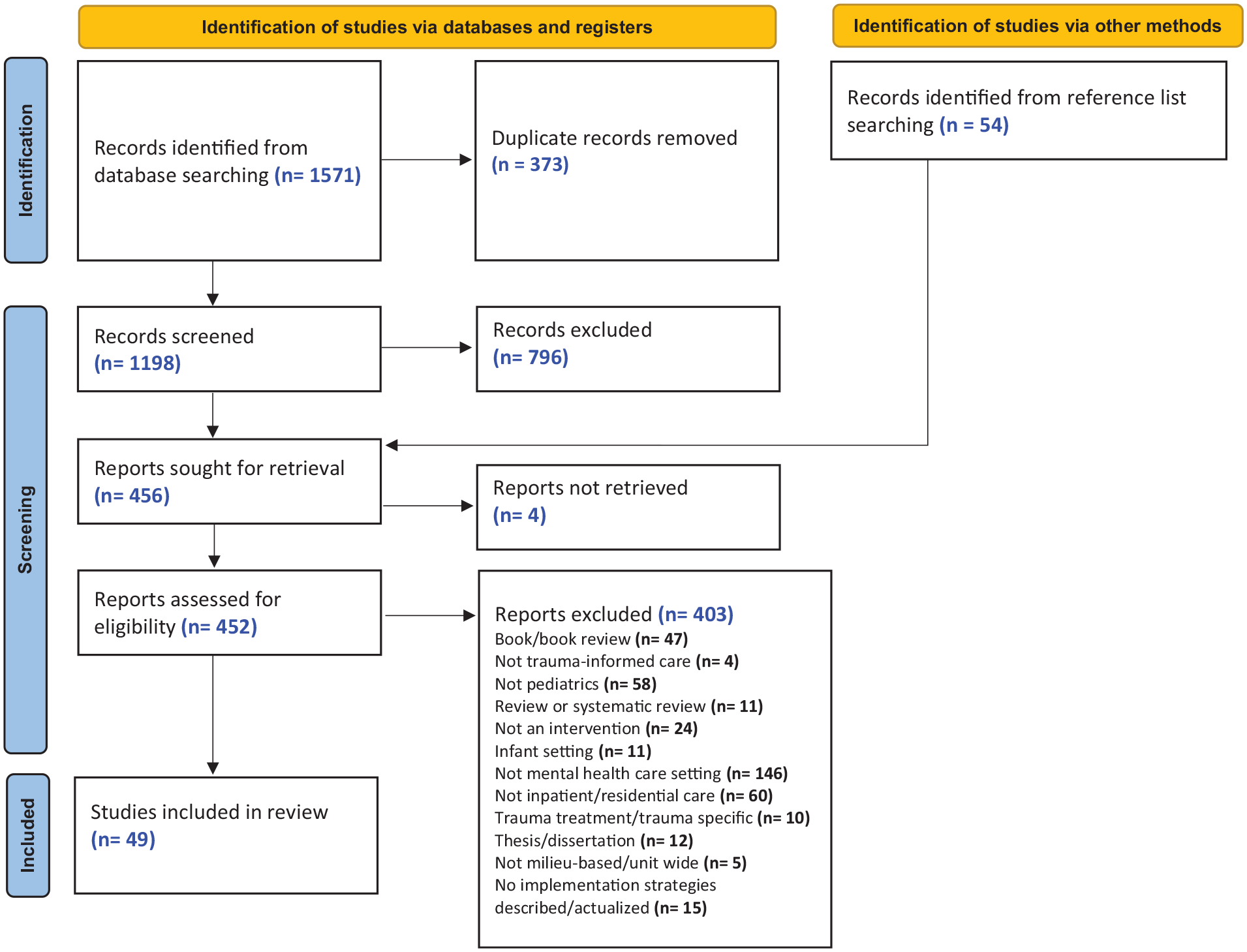
PRISMA flowchart.
Study Characteristics (n = 49) Sorted by Intervention (n = 21).
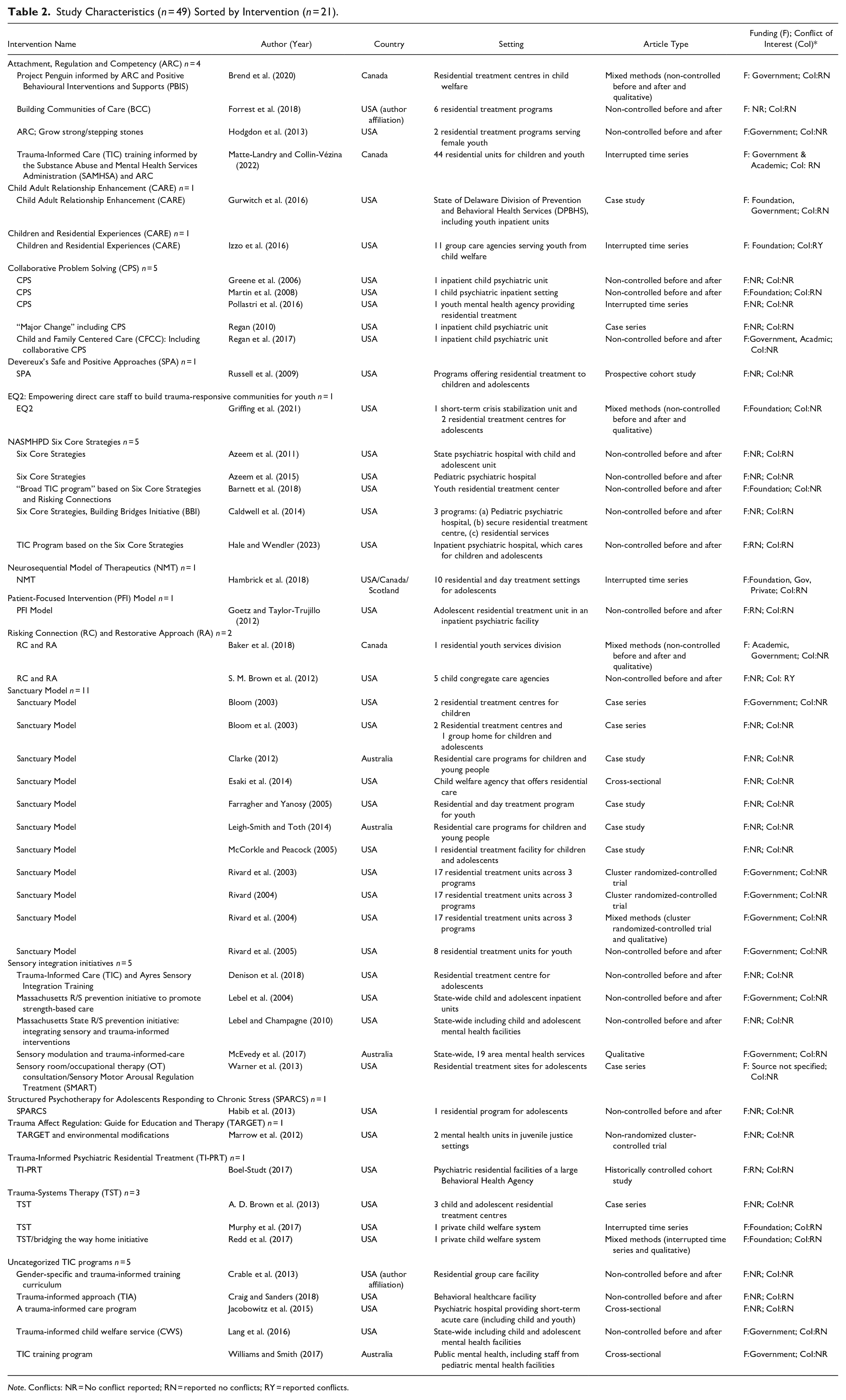
Note. Conflicts: NR = No conflict reported; RN = reported no conflicts; RY = reported conflicts.
TIC Interventions
We grouped together articles reporting on identical sites, and subsequently collapsed all articles reporting on the same intervention, resulting in 21 distinct TICI (Table 2). Some interventions were described by multiple articles, including the Sanctuary Model (11 articles), Collaborative Program Solving (CPS; five articles), the National Association of State Mental Health Program Directors (NASHMHPD) Six Core Strategies (five articles), Attachment, Regulation and Competency (ARC; four articles), Trauma Systems Therapy (TST; three articles), and Risking Connection and Restorative Approach (RC and RA; two articles). Five articles described initiatives that were sensory-integration based. There were five additional TICI that did not fall into the categories above.
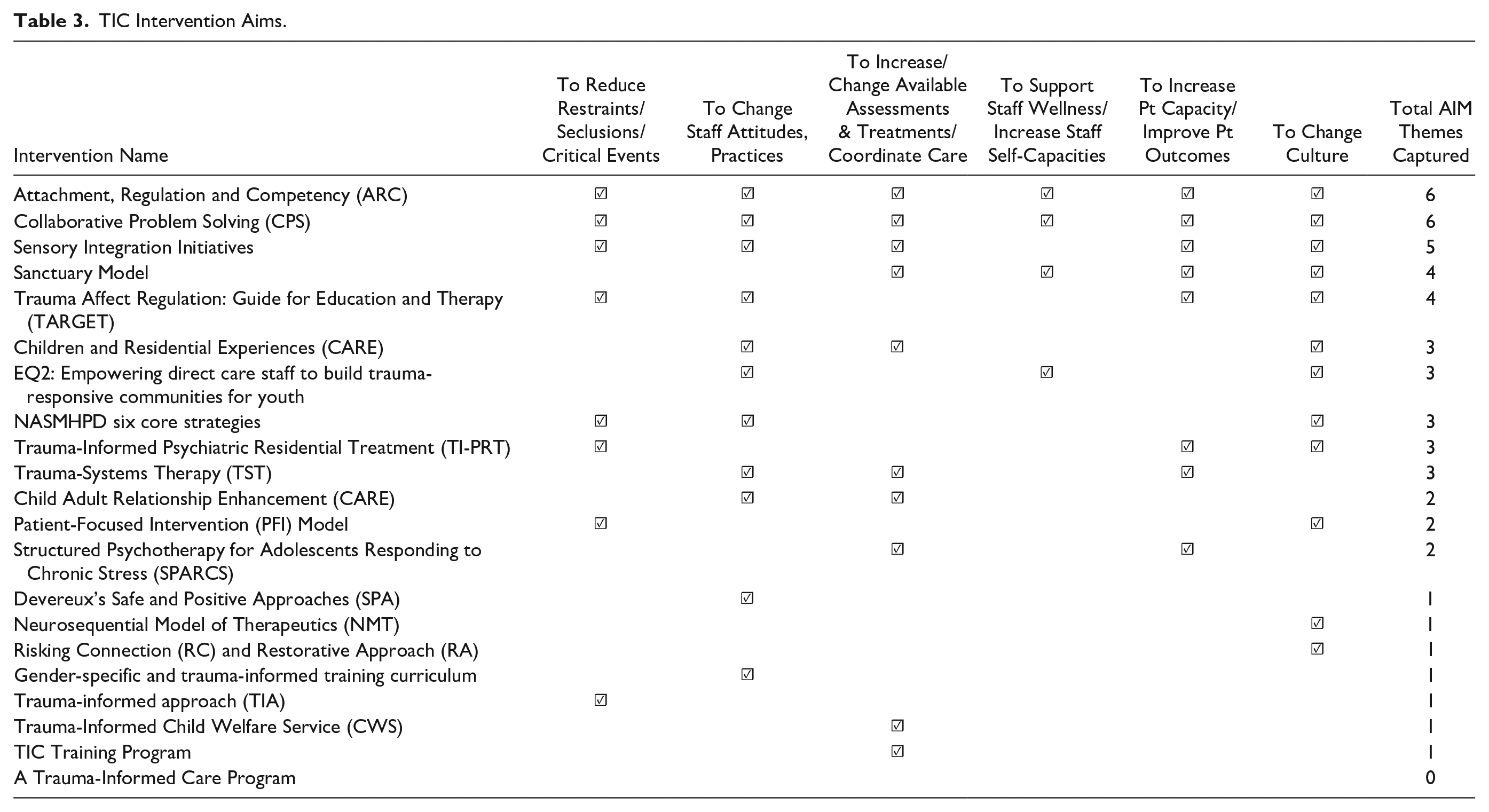
TIC Intervention Aims.
Implementation Strategies
Implementation goals
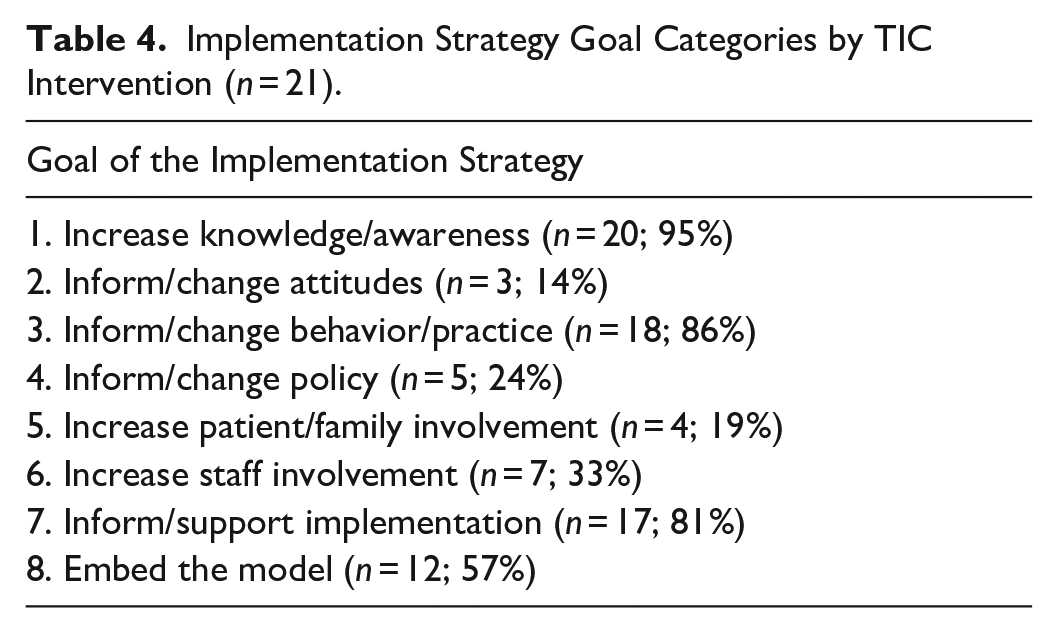
In Table 4 we present the list of implementation strategy goal categories along with a tabulation of the total TICI (n = 21) reporting the respective goals within their implementation strategies. Eleven interventions included five or more different implementation goal categories, while four articles (out of the included 49) reported only one implementation goal, and two articles reported no implementation strategy goals. The most commonly reported implementation goal was to increase knowledge and awareness (20 interventions), followed by changing behavior or practice (18 interventions) and informing or supporting implementation (17 interventions). In Table S2 we present the detailed implementation strategies and implementation goals by TICI (n = 21) including the corresponding ERIC categories and implementation goal categories.
Implementation Strategy Goal Categories by TIC Intervention (n = 21).
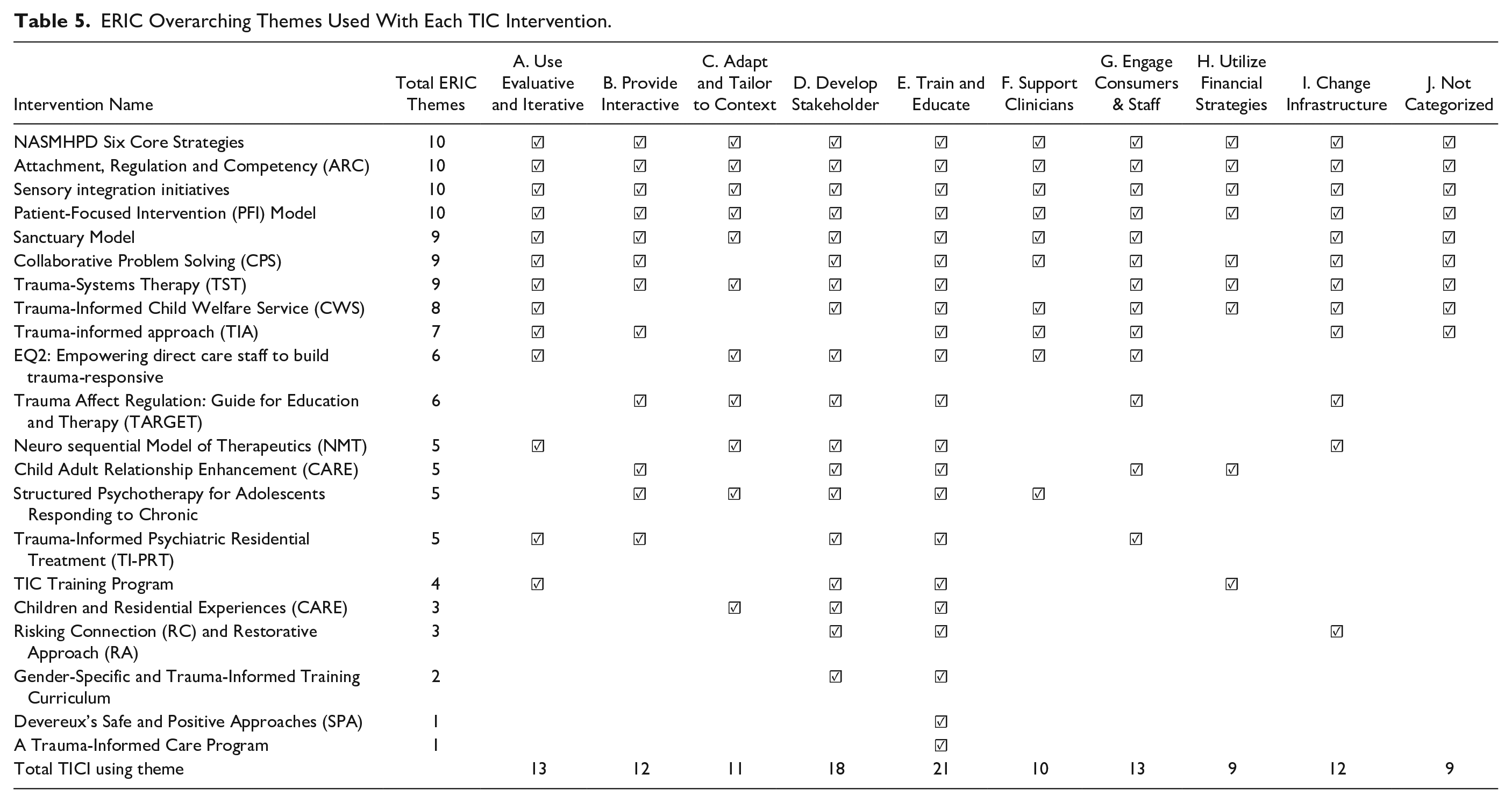
ERIC Overarching Themes Used With Each TIC Intervention.
Discussion
Recent Proliferation of TICI
In this scoping review, we identified 21 TICI in pediatric mental health inpatient and residential settings across 49 articles. While our database search spanned from 1995 onwards, the earliest article we identified was published in 2003 and most articles (n = 35) were published since 2010. The reasons for the recent proliferation of different TICI and approaches may be numerous. First, settings and populations are diverse and complex and require specialized adaptations according to the context in which the interventions are to be implemented. Second, and perhaps more importantly, TICI that are better known and more established are not widely accessible to the public; they tend to be quite expensive to purchase and implement and require a substantial commitment of time, effort, and resources (Hanson & Lang, 2016). For example, in addition to the cost of purchasing the Sanctuary Model, there may be further internal resources required, as the model is designed to be implemented over three years (Andrus, 2022). To obtain the certification, organizations must demonstrate that they have met all 28 of the Sanctuary Institute Standards for Certification (Sanctuary Institute, 2021). Organizations may therefore opt to design and develop their own less expensive and comprehensive approaches. Third, as demonstrated in this review, the reporting of TICI and their implementation is often limited and lacks detail, making them difficult to replicate. Fourth, various definitions of TIC exist (e.g., Bath, 2008; Becker-Blease, 2017; Hanson & Lang, 2016; SAMHSA, 2014; The National Child Traumatic Stress Institute, n.d.). We have yet to achieve a consensus on what TIC actually represents, and the elements and mechanisms needed to achieve it (Hanson & Lang, 2016; Perry, 2020). Hence, it logically follows that depending on the TIC definition adopted by organizations aiming to implement TIC, various TICI could be developed to achieve their desired goals.
Complexity of TIC: TICI Aims, Targets, and Implementation
In this scoping review we identified TICI that endeavour to operationalize the complexity of TIC through various intervention aims, target audiences, and multifaceted interventions. In many cases, it was difficult to identify the TICI aims (distinct from the study aims). When explicitly reported, they varied, potentially indicating that the TICI were designed for different purposes, or possibly representing a continuum of the multiple levels along the complexity of TIC. Aims ranged from abstract to narrower and more specific. TICI specifically targeted patients (e.g., Clarke, 2012; Forrest et al., 2018; Habib, et al., 2013; Marrow et al., 2012), staff (e.g., Crable et al., 2013; Hale & Wendler, 2023; Russell et al., 2009), and caregivers (e.g., Hodgdon et al., 2013; Regan et al., 2017), or a combination thereof. While it may seem evident to target patients with TICI, some authors posit the importance of also including direct care staff (e.g., Wolf et al., 2014) and caregivers (e.g., Lotty et al., 2020; Sullivan et al., 2016) in the cultivation of trauma-informed organizations that engender safety, trustworthiness, support, collaboration, and empowerment. Moreover, perhaps we need to consider not only multiple target audiences but also the complexity of how these audiences interact dynamically within TICI. This may be especially true within the pediatric context, where caregivers play an essential role in supporting and bridging the youth to the community. Eight of the twenty-one TICI aimed to reduce seclusion and restraint events. Yet all those TICI also encompassed aims that went beyond and targeted other areas such as increasing patient capacities, changing staff attitudes, and bringing about a broader culture change, seeming to indicate a general consensus that TIC aims go well beyond simply reducing restraints and seclusions. The most common aim, stated by 12 of the 21 of TICI included in this review, was to promote a form of organizational culture change. While the higher-level aim of culture change is congruent with the complexity of TIC, we also need to consider how this can be operationalized in practice (Hanson & Lang, 2016). A recent example of a TICI (not included in this review, as it is not published in the peer-reviewed literature) that considers the larger cultural context and operationalization of TIC, is a tool developed by the National Children Traumatic Stress Network (NSTCN) called the Trauma-Informed Organizational Assessment (TIOA; Halladay Goldman et al., 2019). The TIOA assesses nine broad aspects of TIC within the organization (covering youth, caregiver, and staff domains) and includes a detailed implementation guide exhibiting the complexity of TIC and the complexity of implementing a TICI.
We also found a large degree of variability in the nature, scope, and number of implementation strategies used to implement each TICI, which is consistent with findings of other reviews of TICI (e.g., Bryson et al., 2017; Lowenthal, 2020). Some TICI used more than half of the 77 ERIC implementation strategies, while others used very few, but the majority did use a multipronged implementation plan. All the included TICI used educational meetings as an implementation strategy with two using educational meetings as the sole implementation strategy. Yet, educational meetings as an exclusive strategy are likely to fall short in achieving the commonly targeted culture change. This was illustrated by authors of two TICI included in this review. Williams and Smith (2017) reported that while training was effective in increasing knowledge and altering attitudes, training had less effect on changing individual practice and an even lower level of influence on changing workplace practice. Lang et al. (2016) also flagged the shortcomings of educational meetings in producing practice changes and warned that “as interest in trauma-informed care grows, there is a risk that ‘receiving some trauma-related training’ becomes equivalent to ‘being trauma-informed’” (Lang et al., 2016, pp 121-122).
Lowenthal (2020), in their review of TIC implementation in the child- and youth-serving sectors, created a three-category post-hoc analytic framework called the TIC Implementation Scope Continuum to classify the nature, scope, and number of implementation strategies of the range of TIC implementation initiatives. Limited Change Initiatives (LCI) consisted generally of one-off trainings with little to no follow up, while Comprehensive Change Initiatives (CCI) used numerous strategies over longer periods of time to create lasting changes in organizational culture, structure, and policies. While this framework offers potential to classify the nature and scope of TIC implementation initiatives, the framework needs to be studied to establish reliability and validity. Further, an important direction for future focus would be to investigate the association between their comprehensiveness and intensity and the effectiveness of the TICI and its implementation.
Reporting of TICI and Implementation Strategies
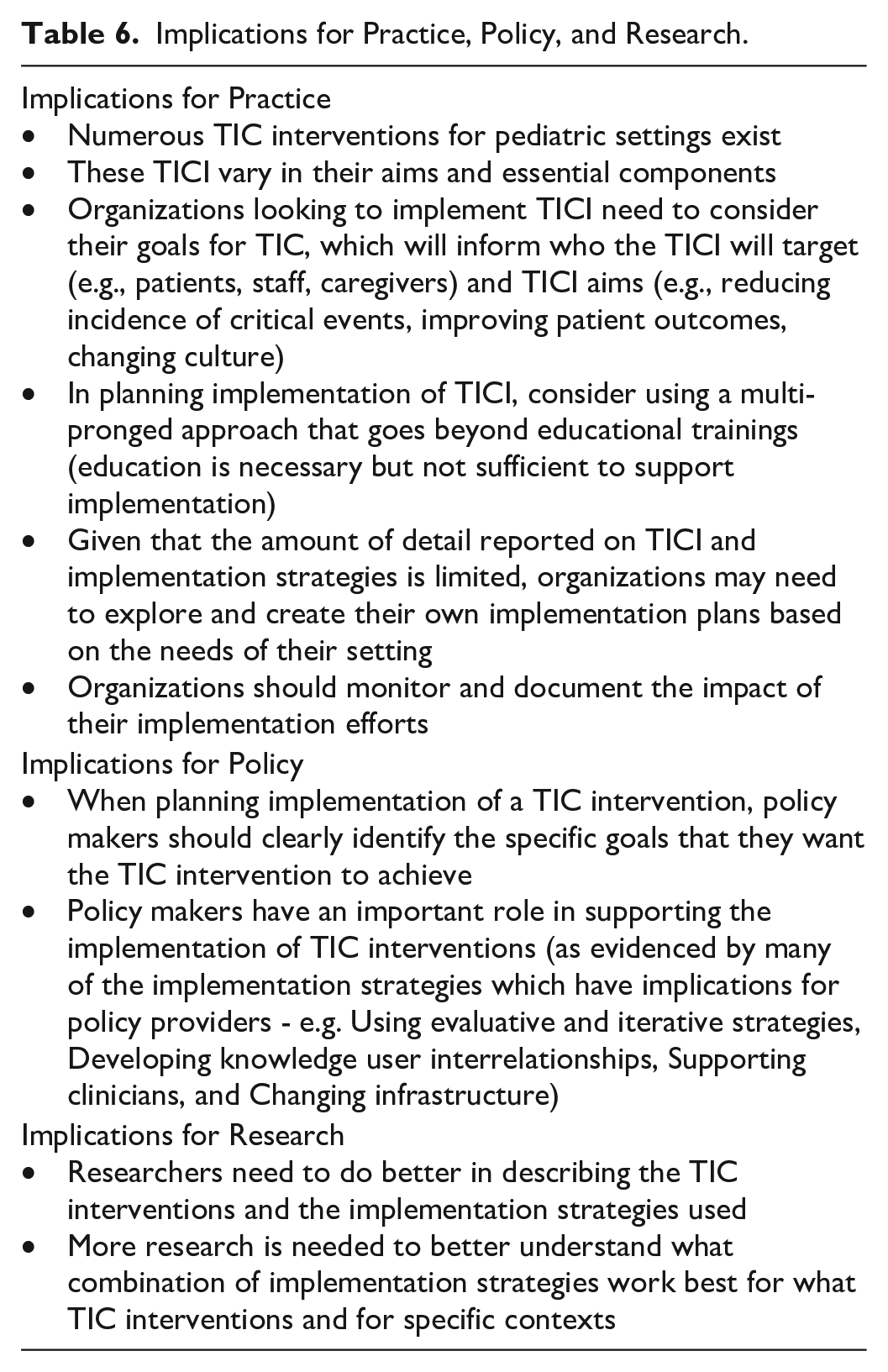
In conducting this scoping review, we found the reporting of both the TICI and of the implementation strategies to be varied and limited. Some articles did not describe or described very minimally the intervention and/or the implementation strategies, so we suggest caution when reviewing and interpreting what was actually done. We note from these articles that there is confusion or lack of clarity around the TICI in contrast to strategies used to implement it. Some articles reported primarily the implementation strategies (such as describing the TICI as a “training”) rather than what the TICI was in practice. From an implementation perspective, a training would be an implementation strategy to facilitate the adoption of the core clinical intervention, whatever that may be (Eldh et al., 2017). To achieve greater clarity and consistency in the reporting of TICI will necessitate further elucidation and agreement around each of these concepts: TIC definitions, TICI, and TIC implementation strategies. Moreover, intervention frameworks or reporting guidelines should be adopted to aid in consistent reporting of and to distinguish between clinical and implementation interventions or strategies (Eldh et al., 2017). None of the included articles in this review incorporated intervention frameworks or reporting guidelines, which made the TICI difficult to synthesize. There are a number of intervention reporting guidelines in the EQUATOR (Enhancing the Quality and Transparency of Health Research network; Simera et al., 2010) database that may be useful to consider in identifying the most useful guidelines for the reporting of TICI, such as the Template for Intervention Description and Replication (TIDieR) checklist (Hoffmann et al., 2014), and the Standards for Reporting Implementation Studies (StaRI) checklist (Pinnock et al., 2017). In our scoping review protocol, we initially selected the (TIDieR) Checklist to guide our data extraction of the TICI and of the implementation strategies. After commencing data extraction, we realized TIDieR Checklist incorporated detailed elements that for the most part were not relevant to the reported TICI that we had identified. After reviewing other available frameworks, we opted to use the AIMD framework (Bragge et al., 2017) as a structure for breaking down and discussing the TICI. Furthermore, the Expert Recommendations for Implementing Change (ERIC; Powell et al., 2015) as a taxonomy for classifying the implementation strategies proved useful for classifying/categorizing strategies used to implement TICI. While intervention frameworks and reporting guidelines can structure and facilitate reporting, the onus remains on the authors to report completely and transparently what took place, otherwise we are still left with incomplete and inconsistent reporting. We encourage authors to enhance the descriptive clarity of the TICI and implementation strategies used with the support of available intervention frameworks and reporting guidelines. See Table 6 for a summary of the implications from this review findings for practice, policy, and research.
Implications for Practice, Policy, and Research.
Study Limitations
Our search strategy included the terms of “trauma-informed”, “trauma-sensitive”, “trauma-integrated”, and “trauma * care” which are commonly used to describe this phenomenon (e.g., Hanson & Lang, 2016), but it is possible additional relevant articles exist that were not indexed with these terms. Due to feasibility concerns, we excluded non-peer reviewed articles, including theses, as well as articles published in languages outsides of English or French; in doing so, we may have missed relevant TICI. It is also possible that others may have coded data differently (e.g., when applying the ERIC implementation strategies as categories). However, our citation screening, data extraction, and data coding processes involved two independent team members and reviewed with the larger team when consensus or clarification was needed leading us to believe that the chance of miscoding was small. We did not assess the quality of the included studies, however this is consistent with guidance related to conducting scoping reviews (Peters et al., 2020). This review focused on pediatric settings and therefore we could not compare how TICI within adult and pediatric settings differ, however this may be a valuable area for future research.
Most articles identified in this scoping review were based in the USA, with a few based in Canada and Australia, and one article including sites from Canada, Scotland, and USA. Given that the healthcare system in the USA differs from other systems in the world, there may be limitations to the transferability of these interventions to other locations. Furthermore, the lack of published interventions implemented elsewhere in the world, including in from countries in the Global South, limits our ability to conceptualize TIC and TIC implementation within diverse settings and contexts. Finally, our analysis was limited to what was reported in articles (both in terms of the TICI and the implementation strategies). Authors may not have fully reported what was done in either the clinical intervention or the implementation.
Conclusions
In conducting this scoping review, we identified numerous admirable efforts to implement TICI in pediatric inpatient and residential mental health settings, demonstrating a broad interest in TIC. The included TICI encompassed some common aims and elements, however, there were also many differences. In selecting, implementing, or reporting on a TIC intervention, it will be important for organizations to consider their goals for TIC and to describe the aims and core components of the TIC intervention separate from the implementation strategies to be used. This specificity will better allow for synthesis and transferability of TICI. We suggest that a tailored implementation plan should multi-pronged approach that goes well beyond educational trainings. We also recommend that further research focuses on developing a better understanding of what combination of implementation strategies work best for what TICI under specific contexts.
Supplemental Material
sj-docx-1-tva-10.1177_15248380231193444 – Supplemental material for Trauma-Informed Care Interventions Used in Pediatric Inpatient or Residential Treatment Mental Health Settings and Strategies to Implement Them: A Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380231193444 for Trauma-Informed Care Interventions Used in Pediatric Inpatient or Residential Treatment Mental Health Settings and Strategies to Implement Them: A Scoping Review by Yehudis Stokes, Krystina B. Lewis, Andrea C. Tricco, Erin Hambrick, Jean Daniel Jacob, Melissa Demery Varin, Justine Gould, Dhiraj Aggarwal, Paula Cloutier, Catherine Landriault, Stephanie Greenham, Michelle Ward, Allison Kennedy, Jennifer Boggett, Roxanna Sheppard, David Murphy, Marjorie Robb, Hazen Gandy, Sonia Lavergne and Ian D. Graham in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380231193444 – Supplemental material for Trauma-Informed Care Interventions Used in Pediatric Inpatient or Residential Treatment Mental Health Settings and Strategies to Implement Them: A Scoping Review
Supplemental material, sj-docx-2-tva-10.1177_15248380231193444 for Trauma-Informed Care Interventions Used in Pediatric Inpatient or Residential Treatment Mental Health Settings and Strategies to Implement Them: A Scoping Review by Yehudis Stokes, Krystina B. Lewis, Andrea C. Tricco, Erin Hambrick, Jean Daniel Jacob, Melissa Demery Varin, Justine Gould, Dhiraj Aggarwal, Paula Cloutier, Catherine Landriault, Stephanie Greenham, Michelle Ward, Allison Kennedy, Jennifer Boggett, Roxanna Sheppard, David Murphy, Marjorie Robb, Hazen Gandy, Sonia Lavergne and Ian D. Graham in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-3-tva-10.1177_15248380231193444 – Supplemental material for Trauma-Informed Care Interventions Used in Pediatric Inpatient or Residential Treatment Mental Health Settings and Strategies to Implement Them: A Scoping Review
Supplemental material, sj-docx-3-tva-10.1177_15248380231193444 for Trauma-Informed Care Interventions Used in Pediatric Inpatient or Residential Treatment Mental Health Settings and Strategies to Implement Them: A Scoping Review by Yehudis Stokes, Krystina B. Lewis, Andrea C. Tricco, Erin Hambrick, Jean Daniel Jacob, Melissa Demery Varin, Justine Gould, Dhiraj Aggarwal, Paula Cloutier, Catherine Landriault, Stephanie Greenham, Michelle Ward, Allison Kennedy, Jennifer Boggett, Roxanna Sheppard, David Murphy, Marjorie Robb, Hazen Gandy, Sonia Lavergne and Ian D. Graham in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors wish to thank Margaret Sampson, MLIS, AHIP, PhD (Library Services, CHEO RI) for peer review of the MEDLINE search strategy. We also thank Murshida Haider and Sophie Lightfoot for assistance with data screening and extraction and additional members of the CHEO TIC Advisory Committee, Shannon Watson and Sarah Bissex for their input.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received funding from the CHEO Psychiatry Associates Research Fund for research assistants to aid with screening and data extraction.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.