
Abstract
Health professionals play a significant role in identifying and reporting child physical abuse (CPA). However, several studies have pointed out non-reporting behavior among these professionals, evidencing difficulties identifying and reporting suspected cases. This review aimed to explore the frequency and possible barriers in identifying and reporting CPA by health professionals worldwide and to identify associated factors. This scoping review was conducted in the Pubmed, Web Of Science, Scopus, and SciELO databases between July 2019 and December 2020. Analytical and qualitative observational epidemiological studies were selected and published in English, Portuguese, and Spanish, with data on the identification and/or reporting of CPA by health professionals. Twenty studies fulfilled the criteria of this review. The studies were conducted with dentists, nurses, pediatricians, and general practitioners. The frequency of identification of CPA ranged from 50% to 89%, while the frequency of reporting ranged from 8% to 47%. This review revealed that health professionals had a low frequency of reporting of CPA, especially for dentists. In addition, several associated factors and barriers in the identification and reporting of CPA were identified in the studies. These were discussed in five main themes: training and continuing education in CPA, impact on professional practice, experiences and perceptions about child protection services, the threshold for suspicion of the professional, and the professional category.
Keywords
Introduction
Child physical abuse (CPA) is an important cause of infant morbidity and mortality (Hillis et al., 2016; World Health Organization [WHO], 2020) being associated with significant behavioral, physical, and mental problems in childhood, which can extend into adulthood (Norman et al., 2012). In addition, the CPA generates an economic impact related to financial resources for the support and treatment of affected victims (Fang et al., 2015; Gilbert, Kemp, et al., 2009).
CPA violates the fundamental rights established in the Convention on the Rights of the Child, which guarantee protection and freedom to all children indistinctly (UNICEF, 2004). However, it is still a common occurrence in the intrafamily environment, consolidated in the social, economic, and cultural environment (WHO, 2020).
The identification and reporting of CPA enables measures of intervening actions aimed at prevention, protective or therapeutic intervention, and guarantee of rights. Health professionals occupy the position of protective agents. They are responsible for contacting the competent authorities and the multidisciplinary team care through the surveillance and assistance centers (Malta et al., 2007). In studies conducted through self-reporting of health professionals (Cairns et al., 2005; Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Mogaddam et al., 2016; Silva-Oliveira et al., 2020), the frequency of reporting ranged from 8% to 47% in cases of CPA. However, studies conducted with data from child protection agencies and police services indicate a 1% to 5% variation in records performed by health professionals, suggesting barriers along the way (Gilbert, Widom, et al., 2009).
Scientific literature indicates a high frequency of non-reporting by health professionals of CPA (Silva-Oliveira et al., 2020). Research has been conducted to verify which factors influence this behavior (Cairns et al., 2005; Demirçin et al., 2017; Lazenbatt & Freeman, 2006). The results indicate the existence of difficulties, both to identify and to report child abuse (Silva-Oliveira et al., 2019). The lack of awareness about the reporting process, the relationship of the professionals with the patient or the family, the fear of reprisals, and the failure of communication between the protection agencies (Andrade et al., 2011; Cairns et al., 2005; Flaherty et al., 2006; Silva-Oliveira et al., 2020) are some of the issues already raised as possible barriers to the reporting of CPA cases.
Recently, a scoping review was conducted to map the factors that influence the decision of physicians and nurses when reporting child abuse (Kuruppu et al., 2020). However, there is still a lack of a scoping review aimed to map the literature that permeates the process of identification, reporting, and the associated factor to CPA, as well as the identification of barriers and facilitators for this process of reporting by dentists, doctors, and nurses regarding CPA.
Methodology
A scoping review is a type of literature review valid for the mapping and comprehensive coverage of existing evidence in a given field of research (Arksey & O’Malley, 2005). It has been selected for this study to analyze the extent and variety of existing literature in the identification and reporting of CPA by health professionals and associated factors and barriers. The protocol for the preparation of scoping reviews proposed by members of the Joanna Briggs Institute (Peters et al., 2015) was used, and the Preferred Reporting Items for Systematic reviews and Meta-Analyses—Extension for Scoping Reviews (PRISMA- ScR) checklist (Tricco et al., 2018) was adopted to conduct this review. In addition, the research project was registered in the Open Science Framework platform, available at the osf.io/3e45g.
Research Question
The question that guided the research was: What are the frequencies, associated factors, and possible barriers to the identification and reporting of CPA by health professionals worldwide?
Eligibility Criteria
The inclusion criteria adopted were: Analytical observational epidemiological studies and qualitative studies, published in English, Portuguese, and Spanish, with data on the identification and reporting of CPA by health professionals. Exclusion criteria were: studies that specifically address other types of child abuse, different from physical abuse (sexual abuse, emotional abuse, or neglect) or research on mistreatment in general and intervention studies.
Search Strategy
Three researchers defined the search strategy after elaborating several combinations of words and verifying results. For a less restricted search, the terms “child physical abuse” and “health professionals” separated by the Boolean operator “AND” were used, and with search in all fields, generating the sentence: (“child physical abuse”) AND (“health professionals”). The strategy was implemented in October 2019 in the Pubmed, Web Of Science, Scopus, and Scientific Electronic Library Online (SciELO) databases, with appropriate adaptations for each database. Updates in the search were made on the date of formulation of this article, in June 2021.
Selection of Articles
The search and extraction of the studies were conducted by two researchers independently. The EndNote Web® program was used with a duplicate elimination filter for the organization and reading of the work. In addition to the filter of the program, the manual search of duplicates was performed by the two researchers. The reading of titles and abstracts of 10% (n = 150) of the total sample of retained papers was done by the two researchers independently, selecting the relevant articles according to the eligibility criteria based on the reading of the study summary. The inter-examiner agreement (kappa) was .81, indicating high reliability among the researchers. After this phase, the total number of articles was divided between the two researchers to read titles and abstracts. The articles selected in this stage were again distributed between the two researchers for full-text reading. The divergences in all phases were resolved in consensus between the two researchers and, when necessary, led to a third expert researcher on the subject.
Data Extraction
After reading the full text, the researchers selected studies that contained information relevant to the study question. Then, tables were constructed in Microsoft Word® to extract the following data: Authors, Year of publication, Country of Origin, Study Design, Audience and Sample, Frequency of identification of CPA and associated factors, Frequency of reporting of CPA, and associated factors and barriers to reporting (Table 1). Implications for practice, policy, and research and critical findings are presented in Tables 2 and 3.
Table Abbreviated With the Main Results of the Articles Included in This Review. June/2021.
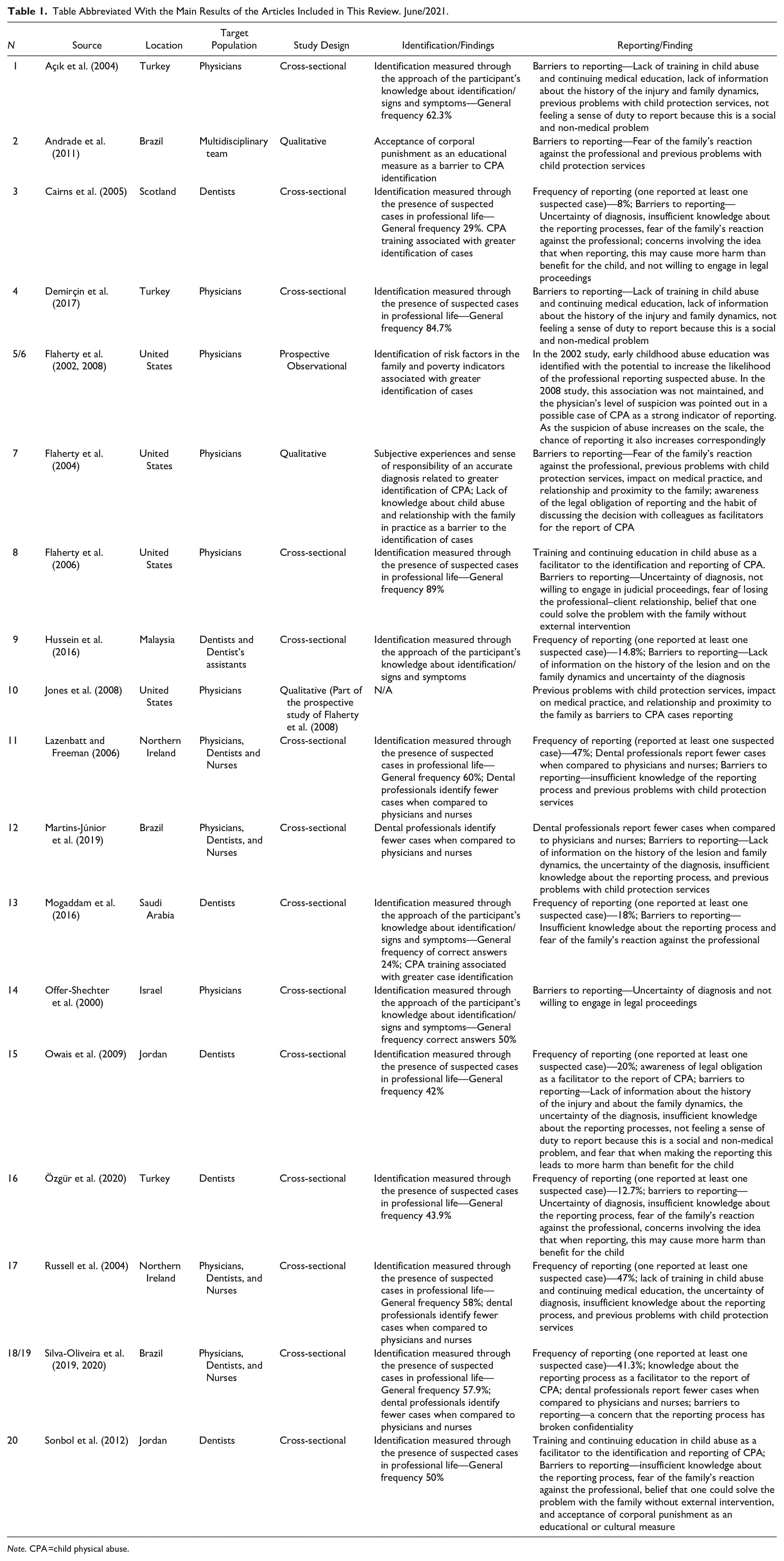
Note. CPA =child physical abuse.
Implications for Practice, Policy, and Research.
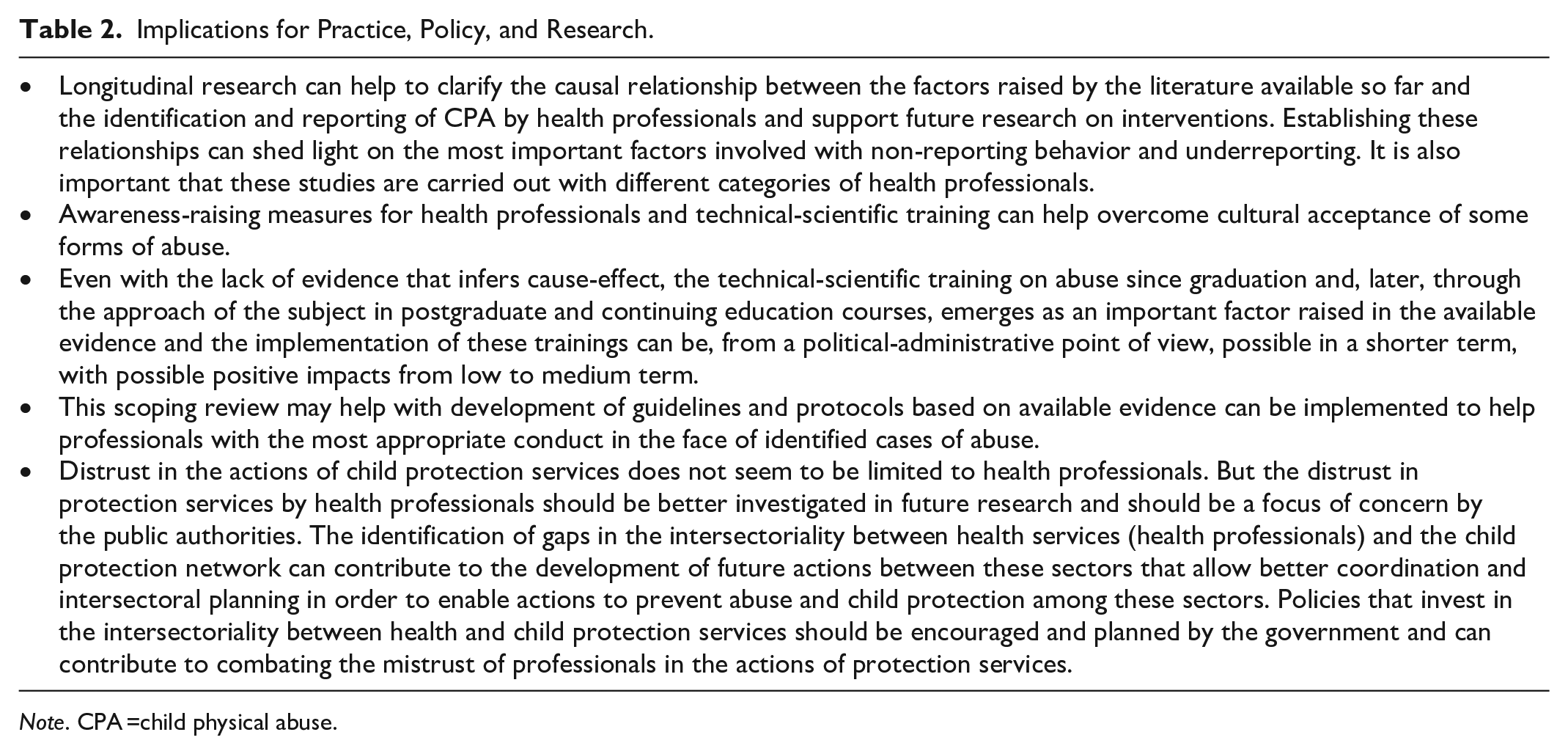
Note. CPA =child physical abuse.
Critical Findings.
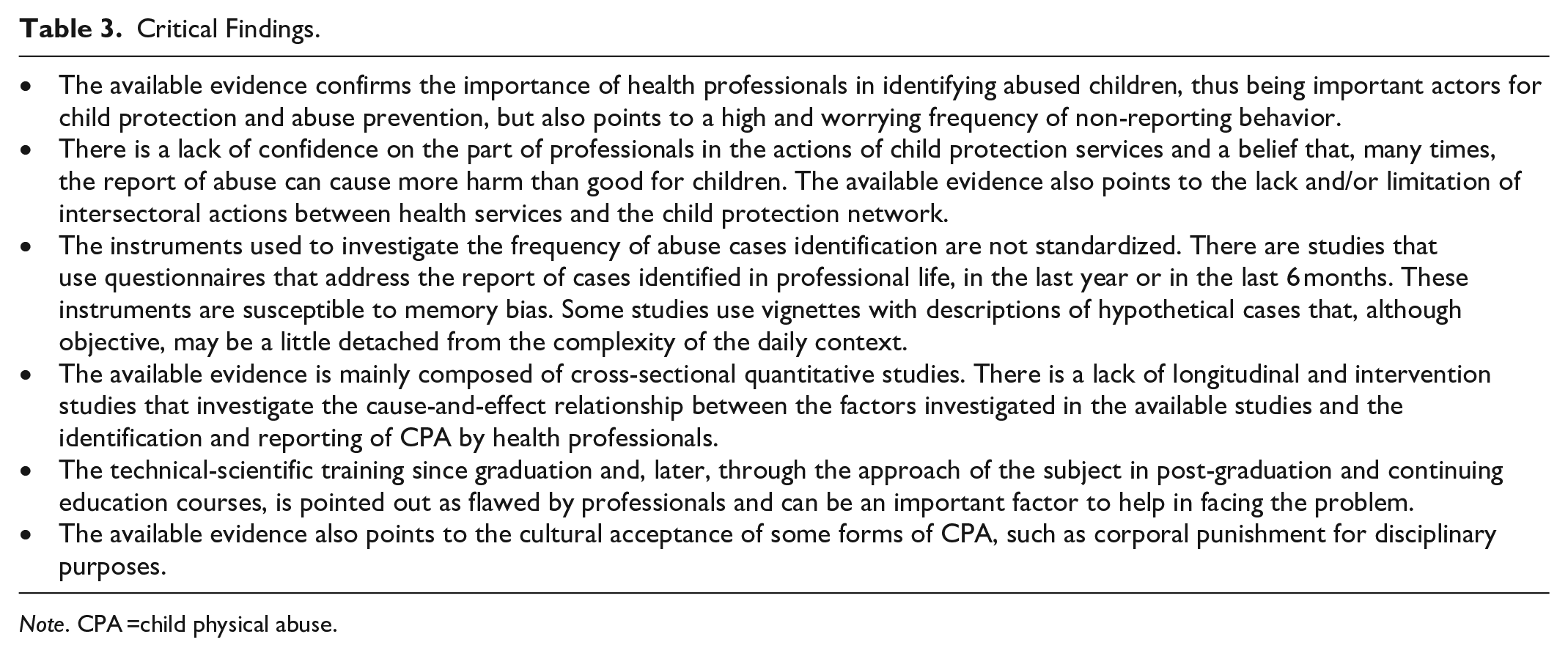
Note. CPA =child physical abuse.
Findings
Characteristics of Included Studies
A total of 2,166 studies were retained in search of the databases. After removing the duplicates there remained 1,467 articles for the reading of title and abstract. Of these, 148 were selected for a full reading. After applying the eligibility criteria, 18 articles remained. Subsequently, two additional articles were included that were considered relevant and were published after the initial search period, totaling 20 articles included in this scoping review. All steps are described in flowchart of Figure 1.
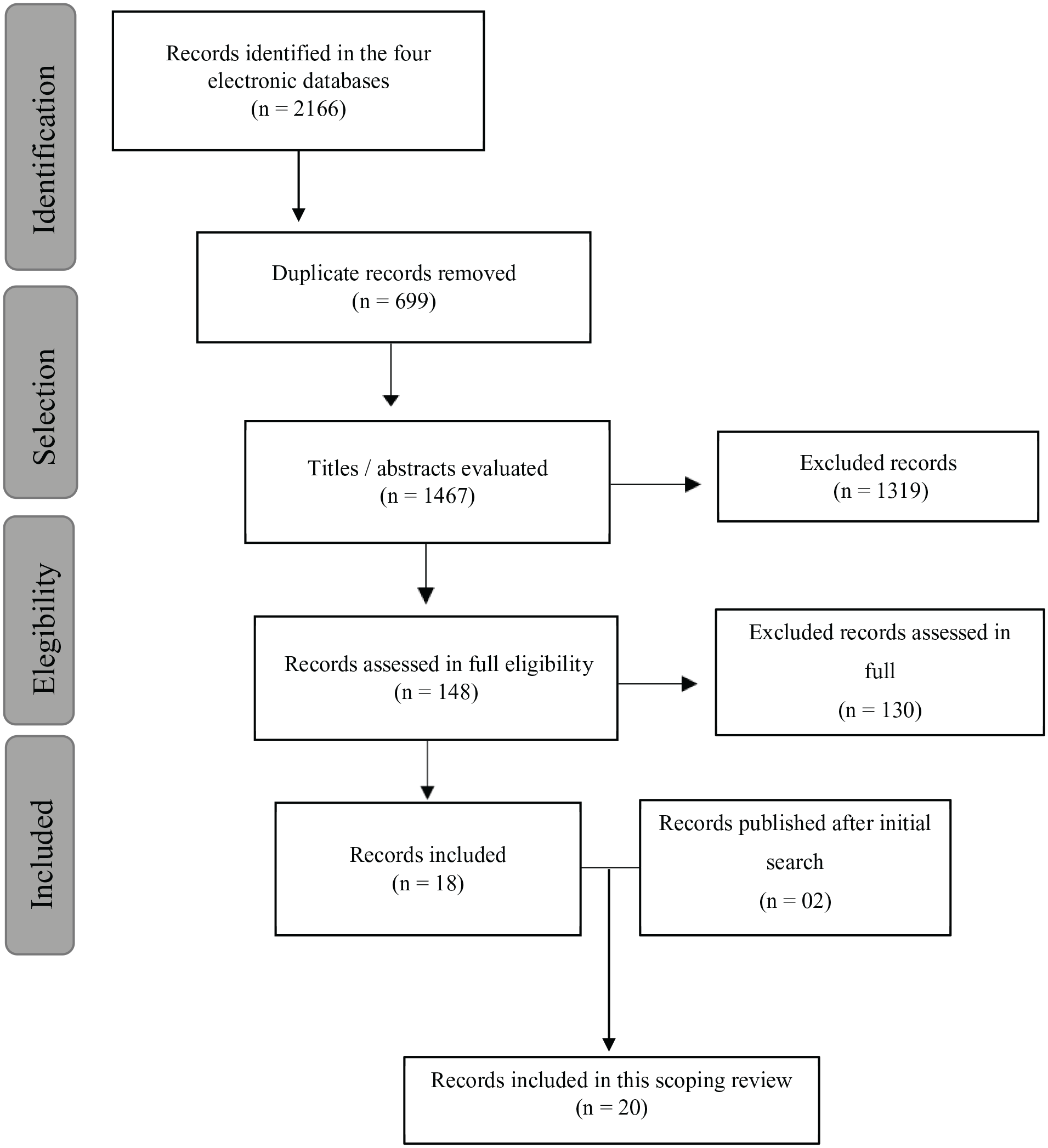
Flowchart.
The selected studies were conducted in nine countries and published between 2000 and 2020. Most articles present a cross-sectional study design, two of them from a prospective cohort (Flaherty et al., 2002, 2008), and three of them are qualitative (Andrade et al., 2011; Flaherty et al., 2004; Jones et al., 2008). The studies were conducted mainly with nurses, dentists, pediatricians, and general practitioners. In one of the studies (Andrade et al., 2011) conducted in Brazil, the interviews were conducted with the entire primary health care unit team, including psychologists, speech therapists, and administrative staff. The questionnaires used for the research or interview script contained questions regarding demographic data and separate sessions that evaluated the identification and reporting of CPA.
Frequency, Associated Factors, Facilitators, and Barriers to the Identification of CPA
Regarding the identification of CPA, 15 articles (Açık et al., 2004; Cairns et al., 2005; Demirçin et al., 2017; Flaherty et al., 2002, 2006;Hussein et al., 2016; Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Mogaddam et al., 2016; Offer-Shechter et al., 2000; Owais et al., 2009; Özgür et al., 2020; Russell et al., 2004; Silva-Oliveira et al., 2019; Sonbol et al., 2012) presented information about the frequency and/or factors related to this variable. The frequency of identification of the CPA ranged from 43.9% to 89% in the studies. It was measured by the number of suspected cases in professional life or a given period before the research or by recognizing signs and symptoms of CPA using vignettes and hypothetical cases. The factor most often mentioned in the studies associated with the identification of cases was training and continuing education in CPA (Cairns et al., 2005; Flaherty et al., 2002; Mogaddam et al., 2016). In addition, the identification of risk factors in the family and poverty indicators were associated with a higher identification of cases of CPA (Flaherty et al., 2002).
Few studies have evaluated the barriers related to the identification of CPA (Andrade et al., 2011; Lazenbatt & Freeman, 2006; Russell et al., 2004; Silva-Oliveira et al., 2019), but in general, most authors concluded that identification failures were associated with a lack of training in child abuse. In addition, the professional category was an important variable related to the identification of CPA. For example, all studies that researched physicians, dentists, and nurses showed that dental professionals are the ones who least recognized cases of CPA (Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Russell et al., 2004; Silva-Oliveira et al., 2019).
Specifically, in qualitative method studies, two of them (Andrade et al., 2011; Flaherty et al., 2004) evaluated factors related to the identification of CPA by health professionals. Flaherty et al. (2004) identified that past subjective experiences and the sense of responsibility of a correct diagnosis are related to the identification of the CPA, while Andrade et al. (2011) detected that the acceptance of corporal punishment as an educational measure is a barrier to the identification of CPA.
Frequency, Associated Factors, Facilitators, and Barriers to the Reporting of CPA
Twelve studies showed data on the frequency of reporting of CPA and its associated factors (Cairns et al., 2005; Flaherty et al., 2002, 2006;Hussein et al., 2016; Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Mogaddam et al., 2016; Owais et al., 2009; Özgür et al., 2020; Russell et al., 2004; Silva-Oliveira et al., 2020; Sonbol et al., 2012). The frequency of reporting ranged from 8% to 47%, and the main facilitating factors were: Training and continuing education in child abuse (Flaherty et al., 2002, 2006; Sonbol et al., 2012), with information on mandatory reporting laws (Owais et al., 2009) and the professional category. Medical and nursing staff reported more cases of CPA to the authorities when compared to the oral health team (Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Silva-Oliveira et al., 2020).
Almost all studies evaluated the barriers to the reporting of CPA. The main barriers found were: lack of training in child abuse and continuing medical education (Açık et al., 2004; Demirçin et al., 2017; Russell et al., 2004), lack of information on the history of the lesion and on family dynamics (Açık et al., 2004; Demirçin et al., 2017; Hussein et al., 2016; Martins-Júnior et al., 2019; Owais et al., 2009), diagnostic uncertainty (Cairns et al., 2005; Flaherty et al., 2006; Hussein et al., 2016; Martins-Júnior et al., 2019; Offer-Shechter et al., 2000; Owais et al., 2009; Özgür et al., 2020; Russell et al., 2004), insufficient knowledge about reporting processes (Cairns et al., 2005; Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Mogaddam et al., 2016; Owais et al., 2009; Özgür et al., 2020; Russell et al., 2004; Sonbol et al., 2012), previous problems with child protection services (Açık et al., 2004; Flaherty et al., 2002; Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Russell et al., 2004), not feeling the duty to report because this is a social and non-medical problem (Açık et al., 2004; Demirçin et al., 2017; Owais et al., 2009), fear of the reaction of the family against the professional (Cairns et al., 2005; Mogaddam et al., 2016; Özgür et al., 2020; Sonbol et al., 2012), fear that by making the reporting this will lead to more harm than benefits for the child (Cairns et al., 2005; Owais et al., 2009; Özgür et al., 2020), desire not to be involved in legal proceedings (Cairns et al., 2005; Flaherty et al., 2006; Offer-Shechter et al., 2000), fear of losing the professional–client relationship (Flaherty et al., 2006), a belief that the problem could be solved with the family without external intervention (Flaherty et al., 2006; Sonbol et al., 2012), the acceptance of corporal punishment as an educational or cultural measure (Sonbol et al., 2012), and the fear regarding the breach of confidentiality of the reporting process (Silva-Oliveira et al., 2020).
Regarding the reporting of CPA, the main barriers identified in the qualitative studies were: fear of the reaction of the family against the professional (Andrade et al., 2011; Flaherty et al., 2004), previous problems with child protection services (Andrade et al., 2011; Flaherty et al., 2004; Jones et al., 2008), impact on medical practice (Flaherty et al., 2004; Jones et al., 2008), and the relationship and closeness to the family (Flaherty et al., 2004; Jones et al., 2008). In addition, awareness of mandatory reporting legislation and discussing the decision with colleagues are pointed out as factors associated with the decision to report cases of CPA (Flaherty et al., 2004).
Discussion
Regarding the frequency of identification and reporting of CPA, it was difficult to accurately analyze the data due to the differences in the research instruments used in the studies. To assess the identification and recognition of cases of CPA, some studies used vignettes with hypothetical cases to which professionals should respond to their level of suspicion of CPA. In other studies, the frequency of identification was measured by the number of times that the professional suspected CPA in their practice, in a certain period before the research. For example, in the last 6 months or the last year. Regarding the frequency of reporting and identification, the articles used different time measurements for analysis, making inferences difficult through an average frequency. However, the non-reporting behavior of CPA cases, evidenced by the discrepancy between identification and reporting rates, is a finding common to all studies included in this review. These data suggest a worldwide trend towards underreporting of cases of CPA by health professionals. Many children who experience child abuse go unnoticed by the sector.
Regarding the factors associated with identification and reporting of child abuse that health professionals have, and its barriers, from our results, we identified five themes that permeate the evidence pointed out in the articles. They are Training and continuing education in CPA, Impact on professional practice, Experiences and perceptions about child protection services, personal threshold of suspicion of abuse, according to Kuruppu et al. (2020) classification, and Professional Category.
One of the subjects that most emerged in the studies was the need for training and continuing education in child abuse. The results suggest that training and qualification in child abuse are related to greater identification and reporting of CPA by health professionals. The lack of these can act as a barrier for professionals to identifying and reporting cases (Cairns et al., 2005; Flaherty et al., 2002, 2006; Mogaddam et al., 2016; Sonbol et al., 2012). Studies have questioned the self-perception of physicians regarding their training in child abuse, and a significant number of professionals reported having received insufficient information about child abuse in undergraduate courses and willingness for training in the subject. In one of the studies (Flaherty et al., 2004), participants reported that education in child abuse was sporadic in their professional life and pointed out the lack of knowledge on the subject as a barrier to identify possible cases of CPA. Kuruppu et al. (2020), in recent research on child abuse, pointed out that all studies in their systematic review recommend continuing education on the subject, which is identified as an important facilitator for the reporting of child abuse in the research.
Information is lacking and there is a dearth of published data on the state of development of clinical practice, professional education at undergraduate and postgraduate level, level of specialization, and on training in relation to child abuse for professionals designated for compulsory reporting. In Brazil, for example, the recognition and conducts regarding child abuse does not seem to be part of the mandatory curriculum of undergraduate courses in nursing, medicine, and dentistry. However, it is known that the training of health professionals to identify and report child abuse varies between countries (Fluke et al., 2021).
In the United States, for example, child abuse pediatrics is a pediatric subspecialty. Becoming a certified child abuse pediatrician requires 3 years of post-residency in an accredited program and then passing an American Board of Pediatrics subspecialty certification exam (Fluke et al., 2021). However, child abuse pediatrics is not recognized as a subspecialty in any European or South American country, including Brazil (Fluke et al., 2021).
Some of the factors identified in this study as barriers to reporting, such as insufficient knowledge about reporting processes (Cairns et al., 2005; Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Özgür et al., 2020) and the belief that this is a social and non-medical problem (Açık et al., 2004; Demirçin et al., 2017; Owais et al., 2009) are problems that can be solved through child abuse education. Some of the factors identified as facilitators of the recognition and reporting of CPA, such as the identification of risk factors in the family (Flaherty et al., 2002) and the awareness of the legal obligation of reporting (Flaherty et al., 2004; Owais et al., 2009) are perceptions that can be acquired through training in child abuse. In the prospective cohort study by Flaherty et al. (2002, 2008), continuing medical education was not associated with CPA reporting. However, the history of the case, such as the incompatibility of the lesion with the report of the guardians or with the level of development of the child, was significantly associated with a greater chance of reporting. The authors suggest that this is related to successful physician training in CPA. In a study conducted only with dental professionals, Özgür et al. (2020) found that about 67% of the participants had not received education in child abuse during graduation.
In this sense, it is necessary to emphasize the importance of the undergraduate course for the technical-scientific training of the individual. Child abuse is not a widespread topic among the curricular matrices of health courses, especially dentistry (Özgür et al., 2020; Silva-Oliveira et al., 2020). Health professionals must receive scientific, technical training on child abuse from the undergraduate course. According to Demirçin et al. (2017), training and continuing education on child abuse should be supported by employers and professional associations to have greater involvement of the professional categories.
The Impact of Reporting on Professional Practice
The impact on professional practice was addressed in the studies from two perspectives. One of them was concerning the bureaucracy of getting involved in a reporting for mistreatment. The unwillingness to get involved in legal proceedings was deemed to be a barrier to the reporting of cases (Cairns et al., 2005; Flaherty et al., 2006; Offer-Shechter et al., 2000) as also workload pressures constituting another barrier (Flaherty et al., 2004; Lazenbatt & Freeman, 2006). In a study conducted with public health service professionals in Brazil (Andrade et al., 2011), participants reported an exhausting workload due to the amount of work for few active professionals, limiting their productivity. Russell et al. (2004), in a study conducted in the United Kingdom, found among health professionals the conception of not finding relevant evidence for CPA and believing that reporting would be another burden added to their already stressful work. This condition can discourage the professional from getting involved in the reporting process.
Another discussion was conducted from the point of view of the professional’s relationship with the family. Fear of consequences for the professional was pointed out as a barrier to case reporting (Flaherty et al., 2004; Mogaddam et al., 2016; Özgür et al., 2020), as well as the fear of losing a family as a client (Andrade et al., 2011; Flaherty et al., 2006; Jones et al., 2008). In the same study, conducted in Brazil (Andrade et al., 2011), the professionals also reported the fear of retaliation by the family because it is a community of high social vulnerability and high rates of violence. In this sense, it is important to consider the precarious social structure and culture of violence that disfavor the reporting of cases.
Perhaps, the physician’s close relationship with the family may trigger emotional factors in the decision-making of the report. In the study by Jones et al. (2008) the professionals examined appeared to project that closeness to the family and knowledge of the background of the family both facilitated and prevented reporting. For some professionals, the good relationship with patients led to a greater reluctance to consider and report CPA. Other professionals, however, considered closeness to the family as a chance to assess risk factors, which could increase the chances of reporting.
Experiences With Child Protection Services and the Association With Reporting
Many studies have pointed out that the previous experiences of professionals with child protection services can influence their non-reporting behavior (Açık et al., 2004; Jones et al., 2008; Martins-Júnior et al., 2019; Russell et al., 2004). As Kuruppu et al. (2020), point out this distrust in child protection services leads the professional to form an opinion that solving the problem in the office without reporting would be more beneficial to the child. Fear of adverse consequences for the child (Cairns et al., 2005; Owais et al., 2009; Özgür et al., 2020) and the belief of being able to solve the problem directly with the family (Flaherty et al., 2006; Sonbol et al., 2012) were identified in this study as barriers to reporting CPA. It is noteworthy that the reporting of child abuse cases is important not only for the intervention of the system in the cycle of violence of the specific case, but also for collecting data on the subject. The establishment of more reliable statistics allows broader reflections on the subject and can support the development of studies aimed at future interventions (Gilbert, Widom, et al., 2009).
Personal Threshold of Suspicion of Abuse Impacting on Reporting
In their research, Kuruppu et al. (2020) point out that each individual has a threshold for suspicion. When reached, it activates the responsibility to report; it classifies this topic found in their research as “Personal threshold of suspicion of abuse.” In our study, factors such as diagnostic uncertainty (Cairns et al., 2005; Flaherty et al., 2006; Hussein et al., 2016; Martins-Júnior et al., 2019; Offer-Shechter et al., 2000; Özgür et al., 2020), the lack of information about the lesion and family dynamics (Açık et al., 2004; Demirçin et al., 2017; Hussein et al., 2016; Martins-Júnior et al., 2019; Owais et al., 2009) and “Not feeling an obligation to report” (Açık et al., 2004; Demirçin et al., 2017; Owais et al., 2009) were found in many articles as barriers to the reporting of CPA. Kuruppu et al. (2020) discuss that the amount of information the professional has about a given case can influence the personal threshold for suspicion, which can be enhanced when you have credible information about the case.
Apparently, despite the medical decision-making based on the objective evaluation of the patient, concerning the diagnosis of CPA, decision-making is strongly influenced by the professional’s personal experiences and beliefs (Flaherty et al., 2006). According to this idea, other factors found in this study that could influence the individual level of suspicion of the professional were the sense of responsibility, past experiences, and the act of discussing the decision with colleagues, who were appointed as facilitators for the reporting of CPA (Flaherty et al., 2004).
In the prospective cohort study by Flaherty et al. (2002, 2008), it was evidenced that the level of suspicion of the doctor in an alleged situation of CPA was a strong indicator of whether he would report the case to the authorities. According to their results, as suspicion increases on a scale, the greater are the chances of reporting. It is important to consider that the main international regulatory agencies guide the reporting even when it comes to suspected cases of child abuse because, in the protection systems of countries such as the United States of America, Australia, and Brazil, the protection agencies are assigned to investigate and confirm whether the suspicion was true or not, in addition to monitoring the child in whose case the suspicion was confirmed.
But we need to consider that the studies raised in this review deal with the identification and reporting of child abuse by health professionals from nine countries. All these countries contain regulations or laws that deal with the obligation of reporting even suspected cases of abuse by professionals who deal with children in their daily work (Fluke et al., 2021). However, these laws vary in scope and specification across countries. These laws require designated persons to report suspected abuse and neglect. Countries such as Brazil, Denmark, Finland, France, Hungary, Mexico, Norway, South Africa, and Sweden have very general legislative duties (Fluke et al., 2021). Australia, Canada, and the United States, on the other hand, have robust legislation and pay detailed attention to the development of these laws over several decades, and legislation in these countries continues to evolve through experiences of success and failure and new phenomena (Matheus & Kenny, 2008). But even in these countries there is variability regarding legislation in different provinces and states. These laws are complex, can often contain loopholes and cause certain legal uncertainties, but which, in addition, coexist with political, economic, social, and cultural forces in each society.
With regard to physical abuse, for example, many legal devices associate it with physical injuries, such as bruises or fractures. But physical abuse is the event in which the child is subjected to physical punishment, spanking or beating, which, even, many times, may not lead to physical consequences, but can lead to psychological consequences, which do not leave visual marks. These definitions of child abuse and physical abuse also vary across countries based on cultural characteristics. In Brazil, where compulsory reporting is established by law, but a general law, and where physical punishment for disciplinary purposes is also prohibited by law, there is still a strong cultural acceptance of physical punishment for disciplinary purposes. A survey carried out with primary care health professionals in a large urban center pointed out that almost 70% of these professionals have already identified at least one case of physical abuse among their patients (Silva-Oliveira et al., 2019). However, qualitative research has pointed to the cultural acceptance of spanking for disciplinary purposes by these professionals (Andrade et al., 2011), which leads them not to see it as physical abuse, impacting the identification and reporting of these cases.
The acceptance of physical punishment as an educational or disciplinary measure, identified in this study as a barrier to the recognition of cases of CPA, can also be a factor that can influence threshold for suspicion of the professional. The results of Andrade et al. (2011) suggested that although there was the identification of signs of physical violence by professionals, some tended to differentiate between physical punishment and ill-treatment, pointing to a conceptual divergence among professionals, possibly supported by cultural values. Other studies have suggested that the perception of professionals regarding corporal punishment influences the reporting behavior of child abuse (Morris et al., 1985; Tirosh et al., 2003). Thus, social norms that tolerate physical punishment can influence the concept of physical abuse by professionals. According to Owais et al. (2009), it should be remembered that corporal punishment is incompatible with international human rights standards.
It is also worth noting the importance of legislation always being accompanied by actions and public policies, such as training and continuing education, institutional support, intersectionality, among other measures, so that it is not just punitive measures, in order to seek comprehensive health care and guarantee children’s rights. This reflection is important because there is already evidence that the legislation that stipulates compulsory notification is effective in increasing the contact of children who suffer abuse, especially severe and frequent abuse, with child protection systems. (Tonmyr et al., 2018). However, there is still a lack of studies that assess whether these laws are successful in preventing the recurrence of child abuse and in effectively assisting victims and their families, since their effectiveness as a public health strategy is unknown.
Professional Category in Identifying and Reporting Physical Abuse
A subject that emerged in the studies conducted with nurses, physicians, and dental professionals is the significant difference in reporting behavior between professional categories. All studies concluded that dentists identify and report fewer cases of CPA when compared to medical and nursing professionals (Andrade et al., 2011; Lazenbatt & Freeman, 2006; Martins-Júnior et al., 2019; Russell et al., 2004; Silva-Oliveira et al., 2019, 2020). The study by Russell et al. (2004) detected those nursing professionals who were more willing to get involved and report cases of CPA. According to the study, they possibly had contact with patients for more extended periods and on a more personal level. In another study (Silva-Oliveira et al., 2020), pediatricians were identified as the category that most reported cases of CPA.
Dentists seem to be the category of health professionals with lower opportunities for education and training in the fight against child abuse, when compared to the other categories (Özgür et al., 2020). Cairns et al. (2005) point out that greater training in maltreatment was associated with a higher rate of identification of CPA among Scottish dentists, as well as a greater belief that the dental team is in a favorable position for the detection of cases. In this sense, it is worth mentioning the evidence that 50% to 75% of cases of child abuse present signs and symptoms in the head and neck region (Cairns et al., 2005; Cavalcanti, 2010; Martins-Júnior et al., 2019), evidencing an important possibility of contribution by dentists.
The results suggest that education and training in child abuse can influence the behavior of dentists on the subject and, therefore, the training of these professionals should be discussed by educational institutions and dental professionals. In addition, Silva-Oliveira et al. (2019) discuss that this discrepancy in the behavior of identification and reporting by dentists can happen due to the limitations of the class regarding the holistic view of the patient. Professional training in dentistry still has a more pronounced focus on the technical-scientific model of care, which focuses on treating and preventing diseases and oral conditions. Therefore, the teaching model of dentists should be debated and reviewed, emphasizing the integrality of care as fundamental from the perspective of health care.
Limitations and Final Considerations
Since it is a scoping review, this study presents some limitations regarding the methodological design itself. The most relevant information related to the subject was more addressed in its extension, not in-depth. Specific studies on each theme identified may be interesting to support the planning of strategies that enable the increase of identification rates and reporting of CPA. Furthermore, the methodological quality of the articles included in this review was not performed.
Only one study in our sample discussed socioeconomic and racial issues in the decision-making of physicians to report CPA (Flaherty et al., 2008). The results of this study indicate that among children with private health insurance in the United States, black children were more likely to be reported to child protection services. In contrast, the race did not influence decision-making among children of lower socioeconomic status. A previous study (Lane et al., 2002) showed racial disparities in evaluating and reporting fractures for possible child abuse. Black children were more evaluated and notified more to child protection services than white children. Data that assess the relationship of race and socioeconomic status of the child in the process of identification and reporting of CPA are necessary. This may be a topic addressed in education and training in CPA to combat racial disparities in health care delivery. The study results by Kuruppu et al. (2020) regarding the factors that influence the decision of primary care physicians and nurses to report child abuse, respecting compliance with compulsory reporting, support much of the evidence found in this study. We reiterate that our review focused on a specific form of abuse, CPA, and therefore our findings are discussed with a focus on this type of abuse. In addition, we also discussed the facilitators and barriers to the identification of CPA, and articles published in Portuguese and Spanish were included, and articles conducted with dental professionals, which allowed us to discuss the differences between the three professional categories.
Although our study has identified themes that were common to most studies, it is important to highlight that cultural, social, and economic differences ensure that the impact of each variable is different for each country. For example, the process of referral of cases, the structure of child protection services, and the very mandatory or optional nature of the reporting are some of the factors that may be different between countries and may influence the decision of the professionals.
The findings presented in this study indicated a significant variability of associated factors, facilitators, and barriers, which reveal the complexity that involves the identification and reporting of CPA by health professionals. These factors need to be considered given their multiplicity in the face of the planning and elaboration of future interventions. These results may guide strategies to increase the involvement of health professionals in the reporting of CPA. It may also corroborate discussions about the specific nuances of this type of child abuse.
Critical Findings
The available evidence confirms the importance of health professionals in identifying abused children, thus being important actors for child protection and abuse prevention, but also points to a high and worrying frequency of non-reporting behavior.
There is a lack of confidence on the part of professionals in the actions of child protection services and a belief that, many times, the report of abuse can cause more harm than good for children. The available evidence also points to the lack and/or limitation of intersectoral actions between health services and the child protection network.
The instruments used to investigate the frequency of abuse cases identification are not standardized. There are studies that use questionnaires that address the report of cases identified in professional life, in the last year or in the last 6 months. These instruments are susceptible to memory bias. Some studies use vignettes with descriptions of hypothetical cases that, although objective, may be a little detached from the complexity of the daily context.
The available evidence is mainly composed of cross-sectional quantitative studies. There is a lack of longitudinal and intervention studies that investigate the cause-and-effect relationship between the factors investigated in the available studies and the identification and reporting of CPA by health professionals.
The technical-scientific training since graduation and later through the approach of the subject in post-graduation and continuing education courses, is pointed out as flawed by professionals and can be an important factor to help in facing the problem
The available evidence also points to the cultural acceptance of some forms of CPA, such as corporal punishment for disciplinary purposes.
Implications for Practice, Policy, and Research
Longitudinal research can help to clarify the causal relationship between the factors raised by the literature available so far and the identification and reporting of CPA by health professionals and support future research on interventions. Establishing these relationships can shed light on the most important factors involved with non-reporting behavior and underreporting. It is also important that these studies are carried out with different categories of health professionals.
Awareness-raising measures for health professionals and technical-scientific training can help overcome cultural acceptance of some forms of abuse.
Even with the lack of evidence that infers cause-effect, the technical-scientific training on abuse since graduation and later through the approach of the subject in postgraduate and continuing education courses, emerges as an important factor raised in the available evidence and the implementation of these trainings can be, from a political-administrative point of view, possible in a shorter term with possible positive impacts from low to medium term.
This scoping review may help with development of guidelines and protocols based on available evidence can be implemented to help professionals with the most appropriate conduct in the face of identified cases of abuse.
Distrust in the actions of child protection services does not seem to be limited to health professionals. But the distrust in protection services by health professionals should be better investigated in future research and should be a focus of concern by the public authorities. The identification of gaps in the intersectionality between health services (health professionals) and the child protection network can contribute to the development of future actions between these sectors that allow better coordination and intersectoral planning in order to enable actions to prevent abuse and child protection among these sectors. Policies that invest in the intersectionality between health and child protection services should be encouraged and planned by the government and can contribute to combating the mistrust of professionals in the actions of protection services.
Conclusions
This review showed that health professionals, especially dentists, underreport CPA. The associated factors and barriers to identification and reporting cases of CPA presents great variability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordination for the Improvement of Higher Education (CAPES) and National Council for Scientific and Technological Development (CNPq).