
Abstract
Children of color—especially Black and Indigenous children—are disproportionately overrepresented in foster care and experience barriers in accessing services and receiving physical and behavioral healthcare compared to their White counterparts. Although racial disparities in mental health outcomes of children in foster care have been examined systematically, less is known about racial disparities in their physical health outcomes. This systematic review aimed to examine disparities in physical health outcomes (i.e., general health, developmental delays and disability, chronic illness, health-compromising behaviors, all-cause mortality) of children in foster care by their race and ethnicity (PROSPERO ID: CRD42021272072). Systematic literature searches were conducted in PubMed, EMBASE, PsycINFO, CINAHL, Cochrane Library, and Psychology and Behavioral Sciences Collection. Of the 6,102 unique studies identified, 24 met inclusion criteria: peer-reviewed journal article; published from 1991 to 2021; written in English; involved children in the U.S. foster care system; children were primarily in family-based placements; included health outcomes; included children’s race and ethnicity; conducted quantitative analyses; and had an observational study design. There was limited evidence to suggest racial disparities among physical health domains examined, in part, due to the small number of studies, variability across study measures and designs, how race and ethnicity were categorized, and how related results were reported. Research that disaggregates results by more nuanced race and ethnicity categories, goes beyond including race and ethnicity as control variables, and uses more robust study designs to understand where racial disparities lie is necessary to inform practice and policy efforts to attain race and health equity in child welfare.
Keywords
Approximately 408,000 children were served in the U.S. foster care system in 2020 (U.S. Department of Health and Human Services, 2021a). Children commonly enter foster care following traumatic and violent events such as neglect (64%), parental substance use (35%), physical abuse (13%), and caregiver illness (13%; U.S. Department of Health and Human Services, 2021a). Less common reasons for removal (e.g., housing insecurity, sexual abuse, parental incarceration, parental death) also reflect the trauma, violence, and abuse children entering foster care face (U.S. Department of Health and Human Services, 2021a). Notably, the vast majority of children entering foster care are from families and communities facing poverty (Barth et al., 2006; McGuinness & Schneider, 2007), and in the United States, communities of color have faced systemic policies and practices that have resulted in their disproportionately experiencing poverty over White communities, especially in urban settings (Knott & Donovan, 2010; Yi et al., 2020). As a result of these factors, children entering foster care tend to have poorer mental and physical health compared to those in the general population (Council on Foster Care, Adoption, and Kinship Care et al., 2015; Turney & Wildeman, 2016).
Despite calls to focus on child well-being outcomes (in addition to safety and permanency outcomes in foster care; Font & Gershoff, 2020) and address racial disproportionality and disparities with the goal of race equity in child welfare in mind (Dettlaff, 2020; Kim & Drake, 2018; U.S. Department of Health and Human Services, 2021b), racial and ethnic disparities in children’s health outcomes when they are in foster care, especially physical health outcomes, have been relatively under-examined. Therefore, the current study systematically reviewed the literature on racial and ethnic disparities in the physical health outcomes of children in foster care.
Physical Health of Children in Foster Care
Physical health includes chronic conditions and illnesses (e.g., asthma, obesity), disabilities, general health status and symptoms, health-compromising or health risk behaviors (e.g., smoking, sexually risky behaviors), and mortality (Breslow, 1972; Centers for Disease Control and Prevention [CDC], 2019, 2021a; World Health Organization [WHO], 1948). Research demonstrates that children in foster care are more likely than those in the general population to have fair to poor physical health, learning disabilities, speech problems, and obesity (Turney & Wildeman, 2016). Between 35% and 45% of children entering foster care have at least one chronic physical health condition, and 60% of children under 5 years old have developmental delays (Turney & Wildeman, 2016), along with significant oral health problems compared to children not in foster care (Morón et al., 2019; Sarvas et al., 2021). Youth in foster care are also at increased risk of engaging in health-compromising behaviors (e.g., unprotected sex, alcohol and marijuana use, trading sex for money; Winter et al., 2016) and have an increased likelihood of becoming pregnant (Eastman et al., 2019; Svoboda et al., 2012) and contracting sexually transmitted infections (STIs) and human immunodeficiency virus or acquired immunodeficiency syndrome (HIV/AIDS) (Ahrens et al., 2010; Taylor et al., 2020) compared to their non-foster care peers.
Furthermore, children in foster care are 42% more likely to die than children in the general population, and mortality gaps between the two groups widened across time from 2003 to 2016 such that mortality rates of the general child population decreased while those of the foster care population remained the same (Chaiyachati et al., 2020). End-of-life trends and all-cause mortality of children in foster care indicate that decedents are younger (e.g., on average, 6 years old), with infants experiencing the highest proportion of deaths in foster care (Lindley & Slayter, 2019). Children who die in foster care also experience significant trauma (e.g., maltreatment, parental substance use; Lindley & Slayter, 2019). In sum, children in foster care experience a host of negative physical health outcomes—in the domains of general health, health-compromising behaviors, disability or developmental delay, chronic illnesses, and all-cause mortality—that require consistent access to quality healthcare, treatment, and support to promote their well-being.
Racial Disparities in the Health Outcomes of Children and Foster Care
When considering racial disparities in health outcomes of children in foster care, the broader experience of racial disparities for children, and particularly children whose families are enduring poverty, provides important context. Multiple social and contextual factors contribute to disparities in pediatric health by race and ethnicity (Slopen & Heard-Garris, 2022). As a result, children of color are less likely to access primary care, experience continuity of care, or report positive experiences with their primary care providers (Stevens & Shi, 2003). Children of color are at significantly higher risk for morbidity and mortality when they have asthma (Hill et al., 2011) and other chronic conditions (e.g., renal disease; Patzer et al., 2012). Together, these findings illustrate the challenges that families of color face in accessing healthcare services for their children, contributing to worse overall health.
Compared to the literature on racial and ethnic disparities in foster care outcomes (e.g., permanency, placement stability), less is known about the health outcomes of children in foster care by their race and ethnicity. Barth et al. (2020) conducted a scoping review to examine differences in outcomes between child welfare and non-child welfare samples, as well as Black children with child welfare involvement experiences compared to other race children. Two studies were identified, which focused on emergency care episodes (Doyle, 2013) and early adolescent pregnancy (Font et al., 2019). However the main results were not reported by children’s race and ethnicity. Kennedy et al. (2022) conducted a meta-regression to examine racial disparities in several well-being domains of children during and after foster care. Across the 70 studies they reviewed, the child well-being domains examined included education, employment, mental health, and behavioral outcomes, but not physical health. The authors concluded that the current evidence base has substantial limitations that prevented the evaluation of racial disparities in well-being outcomes. Questions about whether children and youth currently in foster care differ in their physical health outcomes—both morbidity (e.g., chronic illness, disability) and mortality—by their race and ethnicity remain still. Because children of color—especially Black and Indigenous children—are disproportionately represented and possibly more negatively impacted by their experiences in foster care and, simultaneously, are less well-served by healthcare systems and face greater inequities when it comes to healthcare access and health-promoting services even when they are not in foster care, there is a need to better understand where disparities in health outcomes lie. Highlighting such disparities is a necessary first step to remedy them and thus promote race and health equity in child welfare (National Conference of State Legislatures, 2021).
The Current Study
This systematic review aimed to examine racial and ethnic disparities in the physical health of children in the U.S. foster care system to understand differences in multiple physical health domains—general health status, health-compromising behaviors, chronic or serious illness, developmental delay or disability, and all-cause mortality—by race and ethnicity. A secondary goal was to understand the rigor of the evidence base as indicated by study design and methodology. Responding to recent calls to address racial disparities in outcomes of children and youth in foster care and for children served by healthcare systems (U.S. Department of Health and Human Services, 2021b), this study provides key insights into the strengths and limitations of the evidence concerning racial and ethnic disparities in physical health outcomes across different domains, informing research, practice, and policy.
Methods
We employed PRISMA’s updated guidelines for reporting systematic reviews (Page et al., 2021). Before starting the project, we pre-registered our systematic review protocol at PROSPERO (www.crd.york.ac.uk) (PROSPERO ID: CRD42021272072).
Eligibility Criteria
To meet inclusion criteria, an article needed to: (1) be from a peer-reviewed journal; (2) be published between 1991 and 2021 (relevant studies appeared as early as 1991); (3) be written in English; (4) involve children and youth in the U.S. foster care system; (5) involve majority foster children and youth in family-based placements (including kinship and non-kinship foster care); (5) focus on the health of foster children and youth as main outcomes; (6) include race and ethnicity information of foster children and youth; (7) be quantitative in its analyses; and (8) be observational in study design. An article was excluded from the study if it was: (1) not from a peer-reviewed journal (e.g., report, dissertation); (2) outside the range of the publication date of 1991 and 2021; (3) not written in English; (4) not focused on the U.S. foster care population; (5) focused primarily on foster children and youth in non-family-based placements (e.g., group homes, institutions); (6) focused only on children and youth no longer in foster care (e.g., former foster youth, individuals who aged out after 21 years old); (7) did not examine the health of foster children and youth as main outcomes; (8) did not include the race and ethnicity information of foster children and youth; (9) was not a quantitative study (e.g., qualitative interview); and (10) focused primarily on evaluating an intervention and its effects (e.g., program evaluation).
Information Sources
The databases used for searching were PubMed, Excerpta Medica dataBASE (EMBASE), PsycINFO, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, Psychology and Behavioral Sciences Collection. All databases were searched for relevant articles in September 2021.
Search Strategy
The search strategy involved producing relevant search terms and combinations that would help identify pertinent articles. The current systematic review was part of a larger systematic review and meta-analysis project that, in addition to physical health outcomes, explored mental health and behavioral health outcomes of foster children, and thus used a comprehensive set of search terms that would capture articles focusing on all outcomes of interests (i.e., physical health, mental health, behavioral health) to the larger project. Two different search strategies were used. Specifically for PubMed, Medical Subject Headings (MeSH) terms were used, which is the National Library of Medicine controlled vocabulary thesaurus employed for indexing articles within PubMed (National Center for Biotechnology Information, n.d.), and their combinations. As such, the following search strategy was used: (“Child, Foster”[Mesh] OR “Foster Home Care”[Mesh]) AND (“Health”[Mesh] OR “Disabled Children”[Mesh] OR “Chronic Disease”[Mesh] OR “Mental Health”[Mesh] OR “Anxiety”[Mesh] OR “Depression”[Mesh] OR “Attention Deficit and Disruptive Behavior Disorders”[Mesh] OR “Conduct Disorder”[Mesh] OR “Tourette Syndrome”[Mesh] OR “Obsessive-Compulsive Disorder”[Mesh] OR “Stress Disorders, Post-Traumatic”[Mesh] OR “Autistic Disorder”[Mesh] OR “Substance-Related Disorders”[Mesh] OR “Self-Injurious Behavior”[Mesh])
For all other databases including EMBASE, PsycINFO, CINAHL, Cochrane Library, and Psychology and Behavioral Sciences Collection, we used the following search strategy: (“foster children” or “foster youth” or “foster adolescents” or “child welfare involved children” or “child welfare involved youth” or “child welfare involved adolescents” or “kinship foster children” or “non-kinship foster children” or “foster care” or “non-kin foster care” or “foster homes” or “non-kin foster homes”) AND (“health” or “physical health” or “disability” or “disabilities” or “chronic illness” or “mental health” or “psychological health” or “behavioral health” or “internalizing problems” or “externalizing problems” or “child behavior problems” or “anxiety” or “depression” or “oppositional defiant disorder” or “conduct disorder” or “attention-deficit hyperactivity disorder” or “Tourette syndrome” or “obsessive-compulsive disorder” or “post-traumatic stress disorder” or “autism” or “substance use” or “self-harm”)
Selection and Data Collection Process
All search results were imported into Covidence (Veritas Health Innovation, n.d.), where we engaged in the screening of the collected title, abstracts, and full texts. As shown in Figure 1 (PRISMA flowchart), an initial 7,926 articles were identified in our search. Covidence automatically removed 1,824 duplicate citations. The remaining 6,102 articles were first reviewed for their eligibility by two independent reviewers (second and third authors). Any discrepancies between the two were resolved by an additional reviewer (first author) either independently or within a group consultation of all three reviewers during weekly meetings held for the purpose of continuous assessment of inclusion and exclusion of articles. After this initial review, 246 articles were found. Due to the substantial number of articles found, the research team made the decision to focus the current systematic review on examining racial and ethnic disparities in foster children’s physical health outcomes only. Specifically, physical health was distinguished from mental and behavioral health by using definitions from authority sites (i.e., CDC, WHO, National Institutes of Health [NIH]). For example, according to the CDC and NIH, mental health refers to one’s emotional, psychological, and social well-being, with examples including depression, anxiety, attention-deficit hyperactivity disorder, autism, post-traumatic-stress disorder, and self-harm (CDC, 2021b; NIH, n.d.). On the contrary, physical health primarily concerns the state of the physical body (e.g., brain, weight, bones, muscles, organs) and how well it functions, with dimensions of physical health often focused on morbidity and mortality (i.e., general health status and symptoms, chronic conditions, disabilities, health-compromising and health risk behaviors, death; Breslow, 1972; CDC, 2019, 2021a; WHO, 1948)
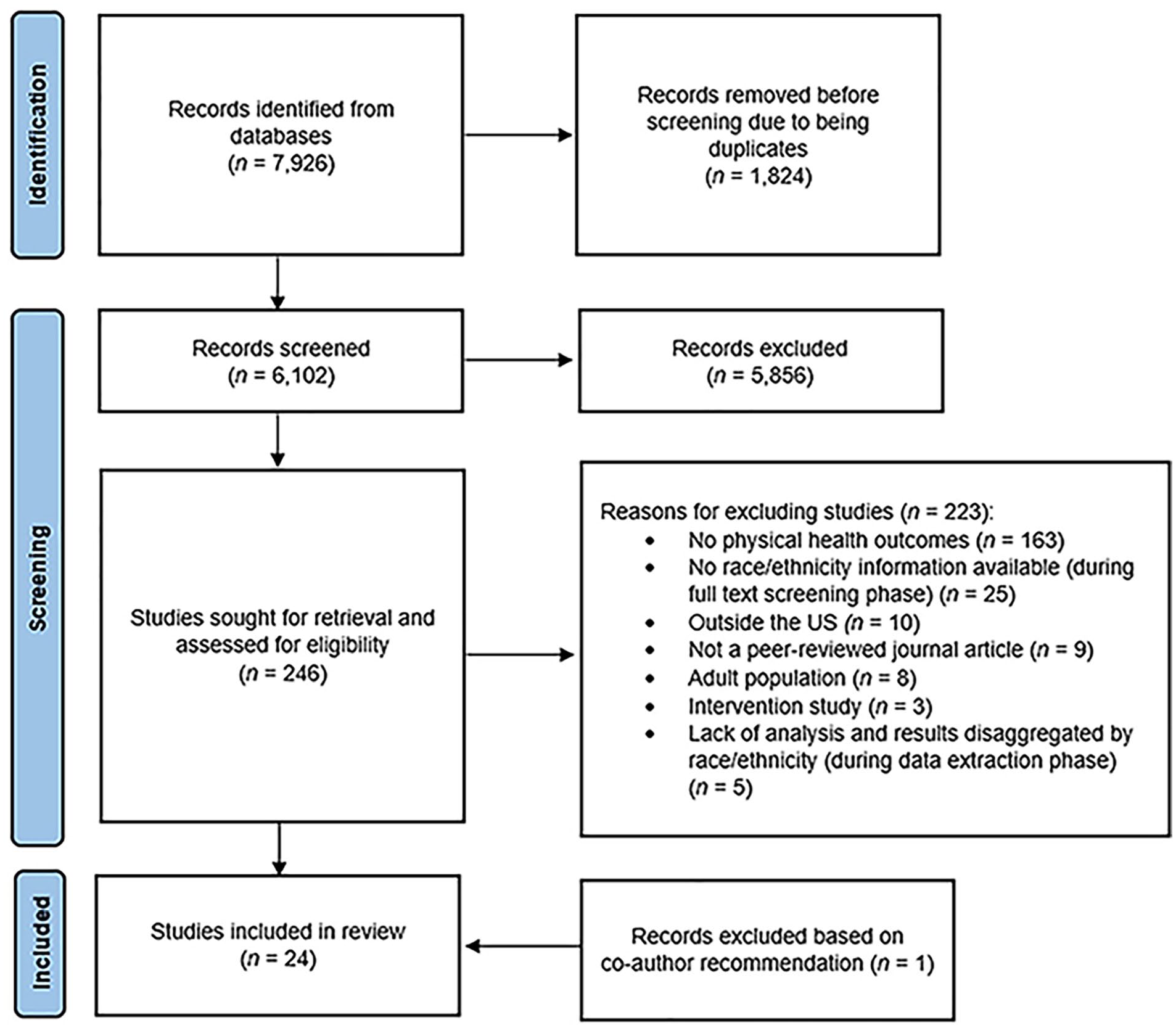
PRISMA flowchart.
All articles were charted using an Excel spreadsheet where the outcomes of each article were categorized as: physical health outcomes, mental health outcomes, health utilization outcomes, or a combination of the three. Of the 246 articles, a total of 223 articles were excluded for various reasons. Specifically, we excluded 163 that did not include physical health outcomes and thus were left with 90 relevant articles having a focus on the physical health outcomes of children in foster care. Next, the full-text review was completed on the 90 physical health outcome articles in Covidence, and articles were removed during this process for the following reasons: lack of race or ethnicity measure (n = 25); outside the United States (n = 10); not peer-reviewed (n = 9); adult population (n = 8); and intervention studies (n = 3). An additional five studies (i.e., Font, 2014; Huffhines & Jackson, 2019; Lindley & Slayter, 2018b; Schneiderman et al., 2013b; Turney & Wildeman, 2016) were excluded during the data extraction phase due to lack of analysis and presentation of results by race and ethnicity. Another reviewer (fourth author) with expertise in this topic reviewed the final article list and suggested 16 articles for inclusion. Of those, 14 (88%) had already been identified but did not meet the eligibility criteria for inclusion. Two articles were added to the full-text review process, and one met the inclusion criteria. A total of 24 studies were therefore included in the final review (see Figure 1).
Data Items
Physical health outcomes were defined in accordance with prior studies (Turney & Wildeman, 2016). As such, physical health outcomes of interest for the current systematic review focused on both general health and specific indicators of health conditions as diagnosed by healthcare providers, reported by either the children themselves or their caregivers (e.g., foster parents). There were a total of five indicators: (1) General health based on medical records or self-reports—included overall health, quality of health, and other conditions indicating the health status of children (e.g., cortisol production, vitamin D levels, sick symptoms, overweight, hospitalization); (2) physical or developmental delay or disability—included physical or developmental delays or disabilities (e.g., intellectual, motor, sensory disabilities); (3) health-compromising behaviors—included engagement in risky behaviors that can compromise health (e.g., HIV/sexually risky behaviors); (4) chronic or serious illness based on medical reports or self-reports—included chronic health conditions (e.g., asthma, diabetes, eczema, chronic heart condition); and (5) all-cause mortality or death—included all-cause mortality or death rates while in foster care. All main study results fit under one or more of the five physical health indicators although specific measures varied across studies (for details, see Table 1).
Race and Ethnicity-Related Study Outcomes by Physical Health Domain (N = 24).
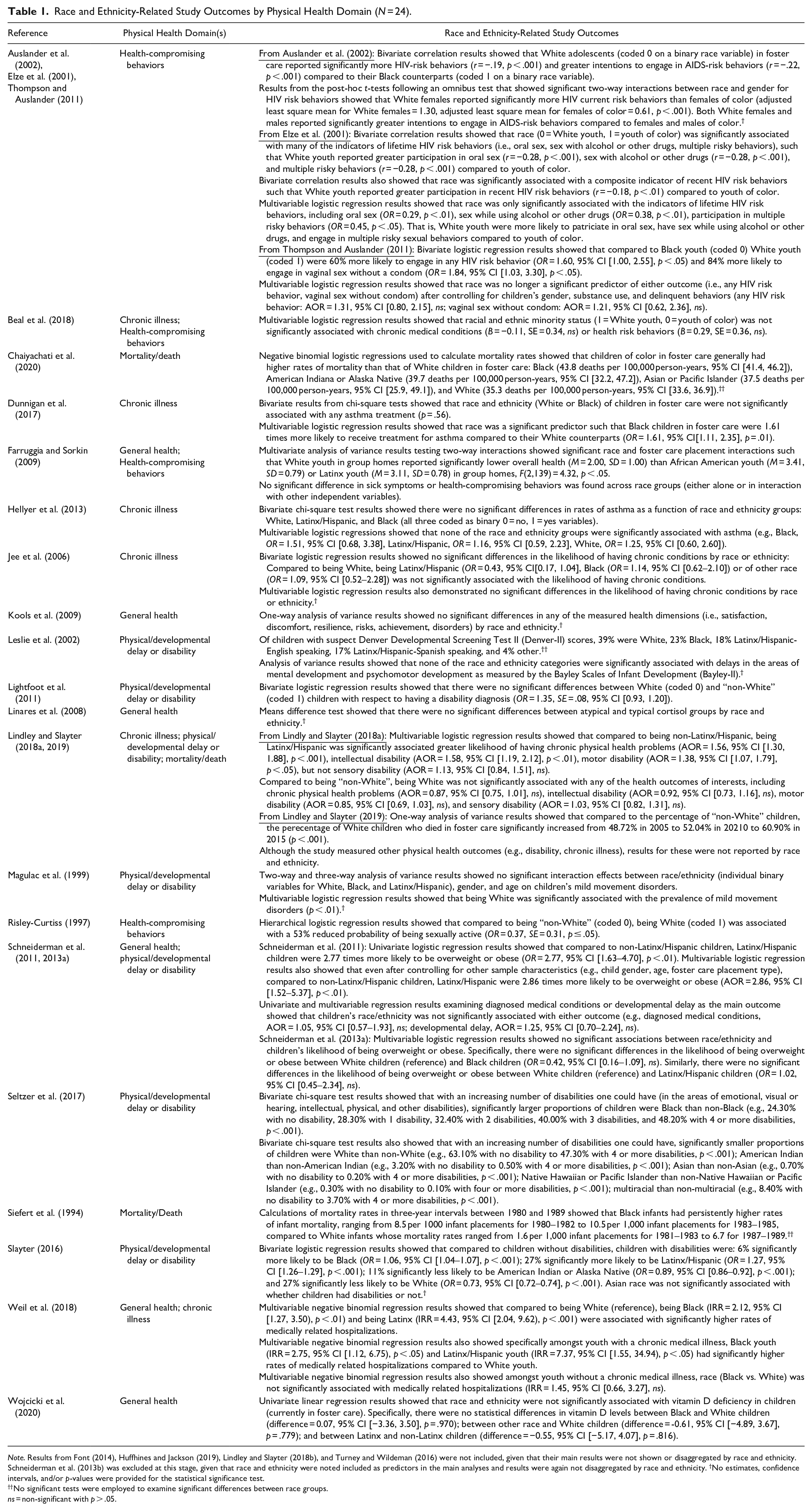
Note. Results from Font (2014), Huffhines and Jackson (2019), Lindley and Slayter (2018b), and Turney and Wildeman (2016) were not included, given that their main results were not shown or disaggregated by race and ethnicity. Schneiderman et al. (2013b) was excluded at this stage, given that race and ethnicity were noted included as predictors in the main analyses and results were again not disaggregated by race and ethnicity. †No estimates, confidence intervals, and/or p-values were provided for the statistical significance test.
No significant tests were employed to examine significant differences between race groups.
ns = non-significant with p > .05.
Author and publication year, age range of the analytic sample (in years), race and ethnicity (i.e., % of race and ethnicity categories), geographic location (i.e., specific location in the United States, national), data source (i.e., name of the dataset, if available), sample size (i.e., analytic sample in N), and study design (e.g., cross-sectional vs. longitudinal, type of analytic method used) were recorded for each article (Supplemental Material 1). Missing or unclear information was clarified by looking up related publications or contacting the authors for additional information. Phrases like “cannot determine” and superscript symbols were used to note the lack of available information.
For each outcome, differences in means, rates, or percentages; correlation coefficients; incident rate ratios; odds and adjusted odds ratios; regression betas, as well and accompanying statistical test results were extracted. For study results without information on statistical testing and relevant test statistics of the effect measures of interest, we noted that such information could not be found in the article (see Table 1).
Study Risk of Bias Assessment
The NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (NIH, 2016) was used to assess quality and bias. Ratings were gathered for each article by one team member (second author), who coded each of the 14 checklist items as “Y” (yes), “N” (no), “CD” (cannot determine), or “NA” (not applicable). A second review by another team member (fourth author) was completed to ensure accuracy. Reviewers discussed discrepancies to ensure agreement. Total percentages were calculated to indicate the quality of individual studies (Dworkin et al., 2021; Scoglio & Salhi, 2021). If an item received an “NA”, it was not included as part of the percentage calculation.
Results
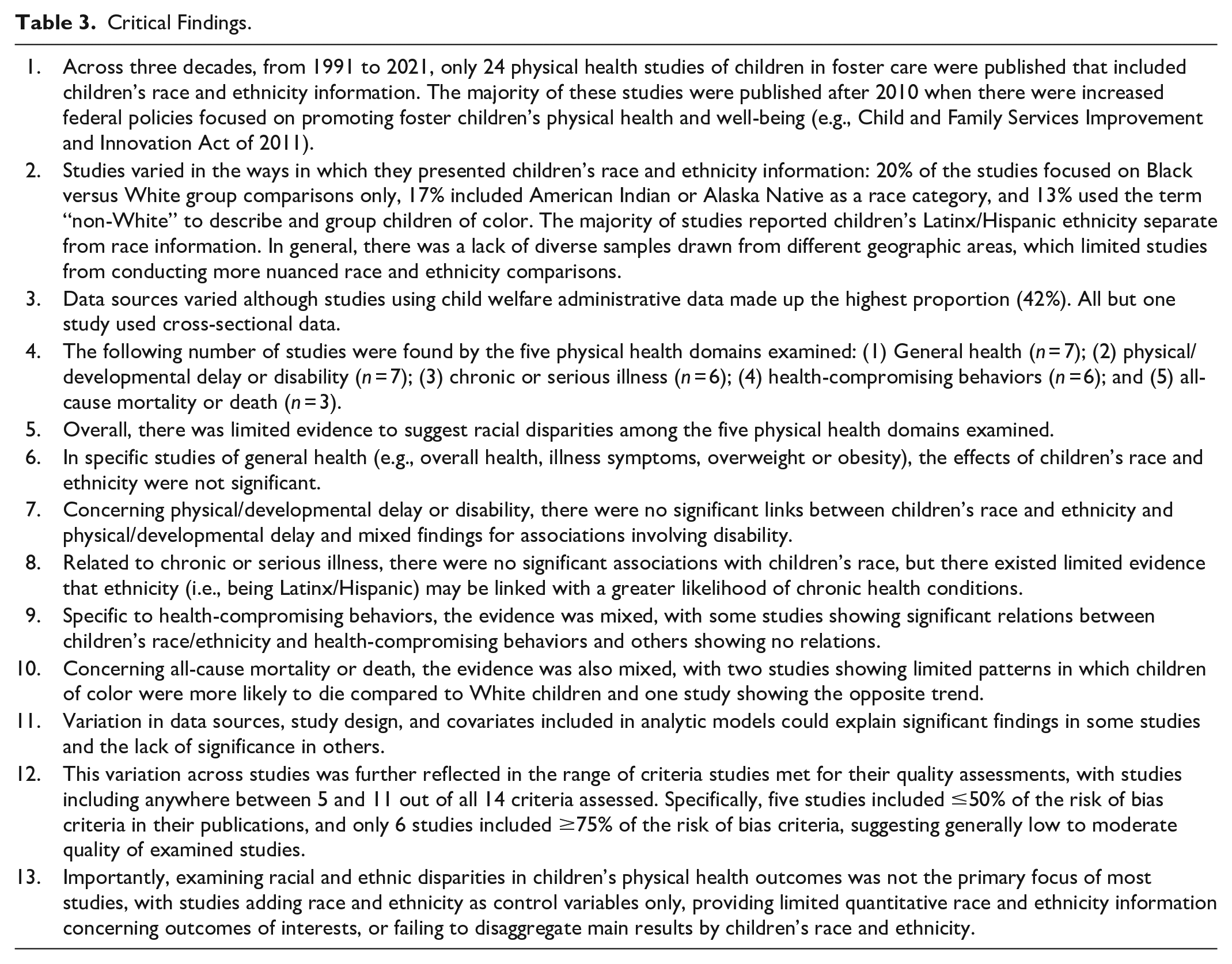
Critical findings of the current study are shown in Table 3.
Study Characteristics
Publication years for the final set of 24 studies ranged from 1994 to 2020, with approximately 60% (or n = 15) of the studies published after 2010 (Supplemental Material 1). The ages of children and youth in foster care ranged from 0 to 21 years. Participants were from various geographic locations across the country (i.e., West, Midwest, Northeast, South), with some studies focusing on samples from local regions (e.g., city or county) and others focusing on state or national populations of children in foster care. All 24 studies had race and ethnicity information per the study eligibility criteria, but not all provided specific percentage breakdowns of their analytic samples’ race and ethnicity categories. Two studies did not provide the number of percentages for the different race and ethnicity categories included in their analytic samples.
Furthermore, the way in which race and ethnicity information was presented varied across studies. For example, about a fifth of the studies (n = 5) focused on Black and White race groups only, and 13% (n = 3) used the term “non-White” to describe and group all children of color. On average, studies had approximately three race and ethnicity categories, with White, Black, and Latinx/Hispanic being the most common categories. Only 17% (n = 4) of the studies included American Indian or Alaska Native—another group that is overrepresented in foster care—as a race category. Approximately 63% (n = 15) of the studies reported ethnicity (i.e., Latinx/Hispanic vs. non-Latinx/Hispanic) and race information separately in their sample description. It is important to note that some of these variations may be due, in part, to regional differences in the population (e.g., low numbers of individuals who are Latinx/Hispanic or American Indian or Alaska Native in certain geographic locations of the country) or the quality of data collection, either by the researchers or in the administrative data source used.
In terms of study characteristics, the sample sizes of studies ranged widely from 21 to 8,348,656. Data sources also widely varied (e.g., medical records, child welfare administrative data, other state system information data, primary data collection, secondary data from individual projects or longitudinal surveys). Specifically, 42% (n = 10) of the studies used child welfare administrative data, 17% (n = 4) used data from medical records, 17% were primary data collection of individual projects, another 17% (n = 4) used secondary data from prior projects, and 8% used state system information data (e.g., vital birth records, Medicaid reimbursements, social services, special education records) other than child welfare administrative data. Most studies (n = 23) were cross-sectional. One study (Dunnigan et al., 2017) used data from a prior longitudinal study, but it was unclear whether key variables, including race or ethnicity and physical health outcome (i.e., asthma treatment), in their models were from different time points.
One study only calculated descriptive statistics, and three studies conducted only bivariate analyses. Of the 20 remaining studies that employed multivariable analyses, 70% (n = 14) used logistic regression, 15% (n = 3) linear regression, 10% (n = 2) negative binomial regression, and 5% (n = 1) both multivariate analysis of variance (MANOVA) and structural equation modeling. Of the 17 studies that conducted discernable statistical testing between race or ethnicity groups, approximately 40% (n = 7) used White as their reference group. Physical health outcomes, as described in the following section, focused on five domains (i.e., general health based on medical records or self-reports, health-compromising behaviors, physical or developmental delay or disability, chronic or serious illness based on medical records or self-reports, all-cause mortality or death). Measures for specific health outcomes pertaining to these domains included binary, categorical, and continuous variables (Supplemental Material 1).
Results on Physical Health Outcomes by Children’s Race and Ethnicity
Individual study results as they pertain to differences in physical health outcomes by children’s race and ethnicity yielded five distinct physical health domains: (1) general health based on medical records or self-reports (n = 7); (2) physical or developmental delay or disability (n = 7); (3) chronic or serious illness based on medical records or self-reports (n = 6); (4) health-compromising behaviors (n = 6); and (5) all-cause mortality or death (n = 3). Studies were not mutually exclusive in that a single study could focus on multiple physical health domains. In the following section and in Table 1, we describe individual study results pertaining to race and ethnicity and those from synthesizing findings across studies by each physical health domain.
General health based on medical records or self-reports
The seven studies on general health based on medical records or self-reports focused on overall health, illness symptoms, health quality, cortisol levels, vitamin D levels, medically related hospitalizations, diagnosed medical conditions, and overweight and obesity. The effects of race and ethnicity were generally not significant. One study examined the self-reported overall health of youth in foster care, and their MANOVA results showed that, specific to youth placed in group homes only, White youth reported significantly lower overall health than Black or Latinx youth (Farruggia & Sorkin, 2009). The same authors examined illness symptoms as an outcome and showed no significant association with race or ethnicity (Farruggia & Sorkin, 2009).
A separate study examined multiple dimensions of health quality (i.e., satisfaction, discomfort, risk, achievement, disorders) as reported by youth in foster care and found that race and ethnicity were not significantly linked with any of the health quality dimensions (Kools et al., 2009). A study focusing on salivary cortisol levels (a marker of vulnerability to stress and adverse events) in school-aged children in foster care also showed no significant mean differences in atypical or typical cortisol production groups by children’s race and ethnicity (Linares et al., 2008). Another study examining vitamin D levels using univariate linear regressions showed that children’s race and ethnicity were not significantly associated with vitamin D deficiency of children currently in foster care (Wojcicki et al., 2020). With regards to medically-related hospitalizations, one study demonstrated using multivariable negative binomial regressions that compared to being White, being Black and being Latinx were associated with significantly higher rates of medically-related hospitalizations in a combined sample of chronically ill and non-chronically ill youth (Weil et al., 2018). However, the negative binomial regression results also showed that among youth without a chronic medical illness, race was not significantly associated with hospitalizations (Weil et al., 2018).
Schneiderman et al. (2011) examined overweight or obesity as an outcome and found in their univariate logistic regression models that compared to non-Latinx children, Latinx children were 2.77 times significantly more likely to be overweight or obese. Multivariable logistic regression results also showed that compared to non-Latinx children, Latinx children were 2.86 times significantly more likely to be overweight or obese (Schneiderman et al., 2011). However, another overweight or obesity study by the same lead author, using a different sample (e.g., inclusive of older children, children in long-term foster care, different medical exam periods) from the same pediatric clinic, found in their multivariable logistic regression models no significant associations between race and ethnicity and children’s likelihood of being overweight or obese (Schneiderman et al., 2013a). Of note, in Schneiderman et al. (2011), with a sample of 449 children less than six years old in foster care, weight-related outcomes were assessed and recorded during children’s first exams between 2005 and 2006 at a pediatric clinic serving children in foster care, and covariates included placement and caregiver types, caregiver language, child sex, child age, child maltreatment type, and child length of time in the child welfare system. In contrast, in Schneiderman et al. (2013a), with a sample of 312 children between ages 2 and 19 years and in long-term foster care placements (i.e., children whose families were no longer eligible for reunification and without adoptive parents), weight-related outcomes were assessed and recorded during children’s first exams at the same pediatric clinic but between 2006 and 2010, and covariates included placement types, child sex, and child age only.
Physical or developmental delay or disability
Of the seven studies that focused on physical or developmental delay or disability, two examined children’s physical or developmental delay as their main outcome (Leslie et al., 2002; Schneiderman et al., 2011), and five examined disabilities as their main outcome (Lightfoot et al., 2011; Lindley & Slayter, 2018a; Magulac et al., 1999; Seltzer et al., 2017; Slayter, 2016). Overall, studies suggested no significant links between children’s race or ethnicity and physical or developmental delay, and mixed findings for associations involving disability. Both studies focusing on physical or developmental delay as their main outcomes showed in their univariate, bivariate, and multivariable models that children’s race and ethnicity were not significantly associated with developmental delays (e.g., mental, psychomotor, developmental delays; Leslie et al., 2002; Schneiderman et al., 2011).
One of the earliest studies examining disability showed in their analysis of variance model that there was no significant main effect of race and ethnicity (White, Black, Latinx/Hispanic) on mild movement disorders defined as choreoathetotic and stereotypic movements and tics as detected, for example, in the face, in or around the mouth, upper or lower body limbs (Magulac et al., 1999). However, in their final multivariable logistic regression model, the researcher showed that being White was significantly associated with the prevalence of mild movement disorders. Another study showed that children with disabilities were 6% more likely to be Black, 27% more likely to be Latinx/Hispanic, 11% less likely to be American Indian or Alaska Native, and 27% less likely to be White (all significant differences; Slayter, 2016). In contrast, Lightfoot (2021) found that children’s race was not predictive of disability diagnosis. Finally, Lindley & Slayter (2018a) found that children’s ethnicity (i.e., being Latinx/Hispanic) was significantly linked with greater likelihoods of intellectual and motor disabilities, with no significant race differences (being White vs. being a child of color) identified.
Chronic or serious illness based on medical records or self-reports
Of the six studies examining chronic or serious illness based on medical records or self-reports, four studies focused on chronic health conditions broadly (Beal et al., 2018; Jee et al., 2006; Lindley & Slayter, 2018a; Weil et al., 2018) and two studies focused specifically on asthma (Dunnigan et al., 2017; Hellyer et al., 2013). Overall, there did not appear to be an association between children’s race and chronic health conditions (Beal et al., 2018; Jee et al., 2006; Lindley & Slayter, 2018a), with limited evidence that children’s ethnicity (i.e., Latinx/Hispanic) is significantly associated with a greater likelihood of having chronic health conditions (Lindley and Slayter, 2018a). As alluded to earlier, a study focused on medically-related hospitalizations among a subsample of youth with chronic medical illnesses found that Black and Latinx youth with chronic conditions had significantly higher rates of medically-related hospitalizations than White youth (Weil et al., 2018).
Specific to asthma, results seemed to indicate no differences in diagnosis, but differences in treatment. A study focused on asthma status as reported by children or their caregivers (e.g., foster parents) found that children’s race and ethnicity were not significantly associated with children’s asthma status (Hellyer et al., 2013). However, Black children were significantly more likely to have received treatment for asthma than White children (Dunnigan et al., 2017).
Health compromising behaviors
Of the six studies focused on HIV/AIDS (and other sexual risk behaviors) or general health risk behaviors, four studies examined HIV/AIDS (and other sexual risk behaviors such as vaginal sex without a condom, sex while using alcohol, or other drugs) as their main outcomes (Auslander et al., 2002; Elze et al., 2001; Risley-Curtiss, 1997; Thompson & Auslander, 2011), whereas two studies focused on general health risk behaviors in which sexual risk behaviors were included in their composite measures (Beal et al., 2018; Farruggia & Sorkin, 2009). Overall, the findings across studies seemed mixed, with some studies showing significant relations between race/ethnicity and health-compromising behaviors (Auslander et al., 2002; Elze et al., 2001; Risley-Curtiss, 1997) and others showing no significant relations (Beal et al., 2018; Farruggia & Sorkin, 2009; Thompson & Auslander, 2011).
Specifically, of the studies focusing on HIV/AIDS and other sexual risk behaviors as main outcomes, one of the earlier studies showed through their multivariable regression model that, compared to being a youth of color, being White was significantly linked with 53% reduced probability of being sexually active (Risley-Curtiss, 1997). Three HIV/AIDS and sexual risk behavior studies used the same data source (i.e., Missouri child welfare data; Auslander et al., 2002; Elze et al., 2001; Thompson & Auslander, 2011). Of these, two showed in their bivariate and multivariable models that White youth were significantly more likely to engage in sexual risk behaviors compared to Black youth and youth of color (Auslander et al., 2002; Elze et al., 2001), and one in their multivariable model showed no significant links between race/ethnicity and youths’ HIV risk behaviors and vaginal sex without a condom (Thompson & Auslander, 2011). In the two studies using a general health risk behavior measure (in which sexual risk behaviors were included along with other health risk behaviors such as smoked cigarettes, got drunk, etc.), both showed in their multivariable models that youths’ race and ethnicity were not significantly associated with health risk behaviors (Beal et al., 2018; Farruggia & Sorkin, 2009).
All-cause mortality or death
Only three studies focused on all-cause mortality or death of children in foster care and generally yielded mixed findings, with two studies showing limited patterns in which children of color were more likely to die compared to White children (Chaiyachati et al., 2020; Siefert et al., 1994) and one study showing the opposite trend (Lindley & Slayter, 2019). Specifically, using Michigan state-level infant mortality data, Siefert (1994) found that Black infants had persistently higher rates of infant mortality compared to White infants although no significance tests were conducted. Similarly, using national child welfare data from the Adoption and Foster Care Analysis and Reporting System (AFCARS), Chaiyachati et al. (2020) showed that children of color generally had higher mortality rates than White children although significance testing was not conducted between races given that the main focus of their study was to compare mortality rate differences between the foster care population and general child population. That is, within race differences were examined across the two populations but not between race differences within the foster care population. Finally, using also AFCARS, Lindley and Slayter (2019) in their bivariate models showed that the percentage of White children who died in foster care significantly increased from 2010 to 2015 compared to the percentages of children of color, while the percentage of Latinx/Hispanic children who died in foster care remained steady across the same period compared to non-Latinx/Hispanic children. Although not reported as part of their main findings, the authors noted in their discussion that the decedents who are children of color were disproportionately overrepresented in their data such that, for example, Black children made up 38% of the decedents in their study when they only make up 27% of decedents in the general population (Lindley & Slayter, 2019).
Risk of Bias in Studies
Risk of bias results are presented in Table 2. Study quality ranged from 42% to 92%, with an average quality rating of approximately 65%. All studies clearly stated their research questions or objectives of the study. Most studies clearly specified the study population (n = 21), had a participation rate of 50% or higher (n = 20), had clearly defined outcome measures (n = 22), and had subjects recruited from the same or similar populations (n = 19). Due to most studies being cross-sectional, no studies assessed for follow-up outcomes.
Risk of Bias in Final Set of Articles (N = 24).
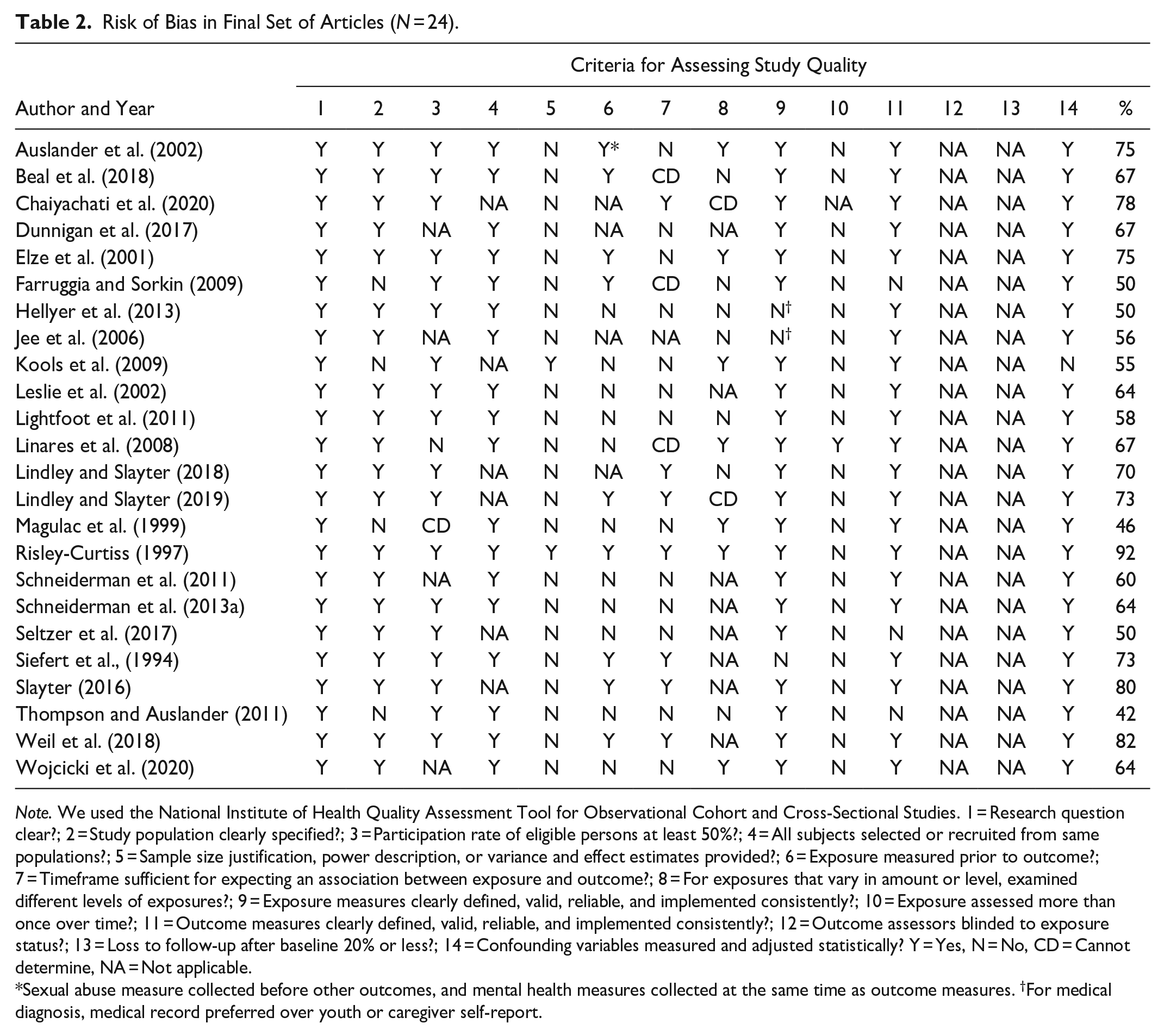
Note. We used the National Institute of Health Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 1 = Research question clear?; 2 = Study population clearly specified?; 3 = Participation rate of eligible persons at least 50%?; 4 = All subjects selected or recruited from same populations?; 5 = Sample size justification, power description, or variance and effect estimates provided?; 6 = Exposure measured prior to outcome?; 7 = Timeframe sufficient for expecting an association between exposure and outcome?; 8 = For exposures that vary in amount or level, examined different levels of exposures?; 9 = Exposure measures clearly defined, valid, reliable, and implemented consistently?; 10 = Exposure assessed more than once over time?; 11 = Outcome measures clearly defined, valid, reliable, and implemented consistently?; 12 = Outcome assessors blinded to exposure status?; 13 = Loss to follow-up after baseline 20% or less?; 14 = Confounding variables measured and adjusted statistically? Y = Yes, N = No, CD = Cannot determine, NA = Not applicable.
Sexual abuse measure collected before other outcomes, and mental health measures collected at the same time as outcome measures. †For medical diagnosis, medical record preferred over youth or caregiver self-report.
Critical Findings.
Discussion
The purpose of this review was to understand disparities in physical health outcomes of children in foster care across various racial and ethnic groups, as well as highlight the state of the literature related to this topic. Given established inequities across indicators of health and well-being for children of different racial and ethnic backgrounds (Flores et al., 2005; Flores & Tomany-Korman, 2008), and known disparities in health for children in foster care in the United States (Barth et al., 2020; Kennedy et al., 2022), it is critical to understand the extent to which inequities by race and ethnicity persist among children in foster care. Across 24 studies reviewed, mixed evidence of inequities by race and ethnicity was identified.
Our results suggested no significant race and ethnicity effects on general health outcomes. Simultaneously, it is important to note that specific outcomes (e.g., vitamin D levels, cortisol production, overweight, obesity) within the general health domain were disparate and were mostly based on single studies, making it challenging to pool results and draw conclusions. Although two studies focused on overweight and obesity (Schneiderman et al., 2011, 2013a), they yielded different results with one study showing that Latinx/Hispanic children were significantly more likely to be overweight or obese compared to non-Latinx/Hispanic children (Schneiderman et al., 2011) and another study showing no significant differences by race or ethnicity (Schneiderman et al., 2013a). Lack of replication may be due to differences in samples, the timing of weight-related outcome assessments, and covariates included in models. Relatedly, these results suggest that race and ethnicity may be only one of several, and not the most important, factors linked with weight-related outcomes of children and youth in foster care.
Findings in studies examining developmental delay were also consistent with no evidence of inequities by race and ethnicity. However, findings regarding racial and ethnic differences in disability were mixed, with some evidence that White children in foster care were more likely to have movement disorders (Magulac et al., 1999); some evidence that, compared to children without disabilities, children with disabilities were more likely to be Black (Slayter, 2016); and other studies finding no differences by race and ethnicity (Lightfoot et al., 2011). This pattern of mixed findings mirrors that of the general U.S. population (Bellows et al., 2013; Dinehart & Manfra, 2013; McKenzie et al., 2002) and may be reflecting a combination of differences in measures and indicators used to screen for developmental delay (e.g., self-report vs. objective task-based assessments) and how race and ethnicity, along with other confounding factors, are captured and included in analyses (e.g., reliability of caregiver report; Greiner et al., 2021).
With respect to chronic illness, health-compromising behaviors, and all-cause mortality, the inconsistency across study findings possibly speaks to the complexity and intersectionality of race and ethnicity with other factors, including gender, age, and exposure to other adversity (e.g., child maltreatment, poverty) that could modify health for children and youth of color. Furthermore, variation in study design, reliance on a combination of self-report and administrative data sources, and covariates included in analytic models could explain significant findings in some studies and the lack of significance in others. This variation across studies was further reflected in the range of criteria studies met for their quality assessments, with studies including anywhere between 5 and 11 of all 14 criteria assessed. A universally agreed-upon strategy for assessing and reporting race and ethnicity, along with a standardized set of covariates to be included across all studies, may help to reduce this variation and move the field toward a better understanding of race and health inequity for children in foster care.
Limitations of the Evidence Base Concerning Diversity Issues
The search strategy deployed for this study resulted in a broad number of articles identified, and validated criteria were used to evaluate the quality of studies that met inclusion criteria, which are both strengths of the current study. In spite of those strengths, there were still relatively few studies identified within each health domain that evaluated racial and ethnic differences. Regarding quality assessments of the studies, five studies included ≤50% of the risk of bias criteria in their publications, and only six studies included ≥75% of the risk of bias criteria, suggesting the generally low quality of studies. Additionally, a lack of diverse samples drawn from different geographic areas limited many studies beyond two group comparisons (e.g., Latinx/Hispanic vs. non-Latinx/Hispanic White; Black vs. White). For example, although American Indian children are some of the most overrepresented groups in child welfare (Lawler et al., 2012; Yi et al., 2020), many studies in our systematic review did not include American Indian or Alaska Native as a race category (in part due to geographic limitations). This finding is consistent with results from Kennedy et al. (2022).
Although not explicitly mentioned as part of our results, we also observed that examining racial and ethnic disparities in children’s physical health outcomes was not the primary focus of most studies. This was evident in studies typically adding race and ethnicity as control variables only, selecting White race as the reference category in their analytic models (and thus possibly normalizing the experiences of White children over the experiences of children of color), providing limited quantitative race and ethnicity information concerning outcomes of interests (e.g., article texts would mention significant differences by race and ethnicity but no relevant parameter estimates, confidence intervals, p-values were provided), or failing to disaggregate main results by children’s race and ethnicity (i.e., five such studies otherwise eligible were excluded during the full-text review phase). Relatedly, a number of studies—both older and more contemporary—used “non-White” to describe children of color, centering Whiteness and White children still even when the findings pertained to children of color.
Our result pointing to the generally low to moderate quality of studies suggest that additional work is needed in this research area, with more robust methods (e.g., nuanced race and ethnicity categories, validated measures with children of color, longitudinal study designs) to better understand racial and ethnic disparities in physical health outcomes and inform intervention and policy efforts to promote health and race equity in the U.S. child welfare system. Additionally, studies that are designed to be nationally representative while also capturing regional variation in child welfare and healthcare practices and policies are needed to address the remaining questions about the extent to which inequities in health by race and ethnicity persist for children in foster care.
Study Limitations and Future Research Directions
There are several limitations to the current systematic review. First, it is important to note that this study did not include any gray literature (i.e., studies that were unpublished or were not peer-reviewed). Future research may consider adding such gray literature to their systematic reviews in addition to the peer-reviewed article we examined here. Second, there were insufficient numbers of studies identified in each physical health domain to support a meta-analysis, which would have allowed for estimating effect sizes of race and ethnicity in relation to physical health outcomes of interest. This points to the clear need for additional research in this area and provides justification for a systematic and programmatic research effort to gather detailed information from multiple communities to address questions about race and health inequity for children in foster care. Finally, because our research interests were primarily in examining racial and ethnic disparities in the physical health outcomes of children in foster care (as well as the robustness of the related evidence base), we did not investigate which factors or mechanisms contribute to identified racial and ethnic disparities (e.g., chronic illness, physical/developmental delay, mortality domains). The quality assessments we used did not allow for inferring mechanisms contributing to health inequity by race and ethnicity, if inequities exist. Future research examining sociodemographic and contextual risk and protective factors and pathways associated with racial and ethnic disparities in children’s health outcomes in foster care is needed.
Implications for Race Equity Policy in Child Welfare and Conclusion
Implications for practice, policy, and research are shown in Table 4. Overall, across three decades, only two dozen studies reported on physical health outcomes by children’s race and ethnicity, pointing to the very small evidence base available so far and the need for additional research in this area with an eye for racial justice and health equity in child welfare. It is no coincidence that the preponderance of articles that met study selection criteria was published after 2010, a period that coincides with increased federal legislative focus and funding on foster children’s physical health and well-being. Given that significant federal law and state policy only credibly began to frame provisions for health care coordination as a central service for children starting in 2011 (via the Child and Family Services Improvement and Innovation Act, 2011), the study of health outcomes in the child welfare literature base is indeed in its early stages, not to mention the more focused attention on health conditions by race and ethnicity. Still, this topic is imperative because, again, children of color have higher out-of-home placements and thus are more likely to be impacted by foster care systems and processes. Based on disparities in prevention services, access to care, provision of health education, and the like, we would expect racial and ethnic outcomes to differ by certain health categories (e.g., general health conditions) and not as much by others (e.g., disabilities). Although our findings are inconclusive, the potential racial disparity in disability status is worthy of considerable future research.
Implications for Practice, Policy, and Research.
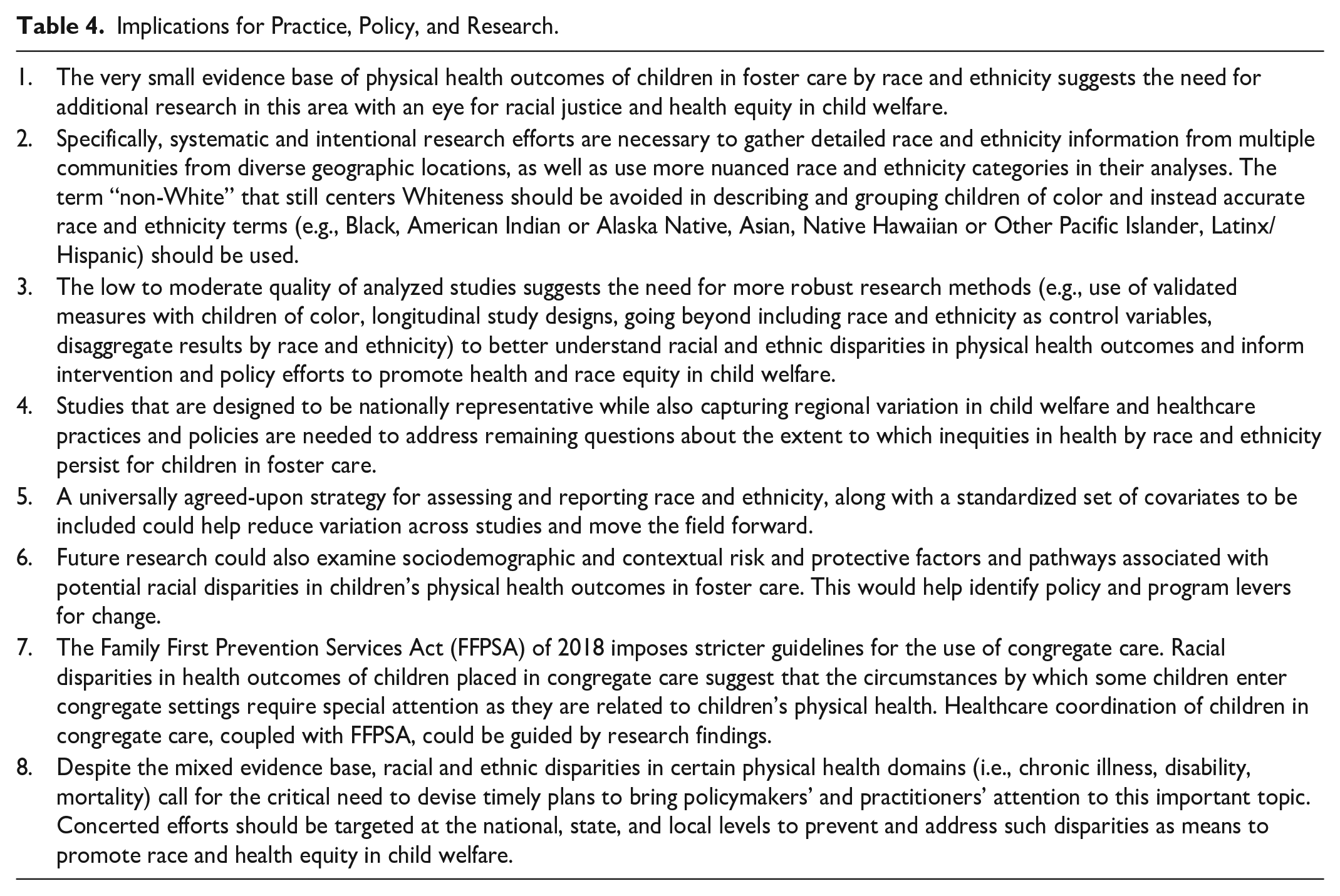
Another finding worthy of note, in part, because of the direction of current federal policy, including the Family First Prevention Services Act of 2018 (FFPSA) (Bipartisan Budget Action of 2018), is the one related to children placed in congregate care settings. We found in one study worse health outcomes for White children experiencing group care. The circumstances by which some children enter congregate settings (e.g., previously failed placements, higher levels of behavioral needs, use of Other/Another Planned Permanent Living Arrangement [O/APPLA]) require special attention as they are related to children’s health outcomes. FFPSA legislation now imposes stricter guidelines for the use of congregate care. The fact that children in these settings experience poorer outcomes and are disproportionately children of color, coupled with the new law, provides an opportunity for healthcare coordination that is guided by research findings.
In conclusion, the current evidence suggests there are many unknowns regarding racial and ethnic disparities with regard to the physical health outcomes of children in foster care. There is some mixed evidence that racial disparities exist in certain domains (i.e., chronic illness, disability, mortality). Recognition of potential racial disparities is needed to devise timely solutions so bringing policymakers’ and practitioners’ attention to this important topic. Concerted efforts should be targeted at the national, state, and local levels to address such disparities and thus promote race and health equity in child welfare.
Supplemental Material
sj-docx-1-tva-10.1177_15248380221145911 – Supplemental material for Racial and Ethnic Disparities in the Physical Health Outcomes of Children in Foster Care: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380221145911 for Racial and Ethnic Disparities in the Physical Health Outcomes of Children in Foster Care: A Systematic Review by Joyce Y. Lee, Jaclyn Kirsch, Sarah Presley, Sarah J. Beal, Yanfeng Xu, Angelise Radney and Ramona Denby in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We would like to thank Dr. Anao Zhang for recommending relevant search terms and reviewing the study protocol, including the PROSPERO pre-registration, used for the current systematic review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.