
Abstract
Rates of both violent victimization and violence perpetration are known to be elevated among individuals with mental illness compared with those in the general population, though the relative risk of each outcome is less well established. In this systematic review, PubMed, Embase, Web of Science, PsycINFO, and Criminal Justice Abstracts were searched for articles published any time before October 2021 that reported the prevalence or incidence of both violent victimization and perpetration. We performed two searches to identify studies using samples or cohorts of (1) persons with mental illnesses and (2) persons in the general population. A total of 25 studies (9 examining persons with mental illnesses, 13 examining persons in the general population, and 3 examining both sample/cohort types) were identified and data was extracted to describe the type and size of cohort or sample, definitions and terminology (i.e., mental illness, violence victimization, violence perpetration), data source(s), observation period, prevalence/incidence of victimization, and prevalence/incidence of perpetration. The Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data was used to conduct a quality assessment of all included studies. Due to marked study heterogeneity, results were presented using a narrative synthesis approach. Across studies, findings were mixed, and the methodological approaches varied greatly. Broadly, the review provides evidence for (1) higher rates of victimization than perpetration for both individuals with mental illness and those in the general population and (2) higher rates of both victimization and perpetration for those with mental illness compared to those in the general population.
The public often views people with mental illness as being dangerous and prone to violent behavior (Jorm et al., 2012; Pescosolido et al., 2010, 2019; Thornicroft, 2006). Associations between mental disorders and violence perpetration have been found (Fazel et al., 2009; Whiting et al., 2021; Yu et al., 2012), although more recent research now also highlights the relationship between mental disorders and violence victimization (de Vries et al., 2018; Latalova et al., 2014; Maniglio, 2009; Passos et al., 2013). Generally, the existing evidence indicates that people with mental illness show elevated risks of both violence victimization and perpetration compared to their general population peers. Additionally, it is commonly stated that people with mental illness are more likely to be a victim of violence than to act violently (e.g., Choe et al., 2008; Thornicroft, 2020).
A major limitation of many of these previous studies is that either rates of victimization or perpetration, but not both, have typically been examined in cohorts or samples of people with mental illness diagnoses. For example, Choe et al. (2008) conducted a systematic review on this topic and found 10 studies of violence victimization and 31 studies of violence perpetration. Of these studies, only three assessed both victimization and perpetration among the same individuals. Comparing victimization and perpetration rates across different cohorts or samples limits considerably our ability to draw conclusions regarding the relative risk of the two outcomes. Indeed, Choe and colleagues specifically suggested that future studies should examine both victimization and perpetration in the same cohort or sample to overcome this limitation. However, no systematic review to date has specifically synthesized evidence reported from studies that have examined both outcomes in one sample or cohort.
The current study addressed these ongoing gaps in the literature by systematically gathering and synthesizing studies that reported rates of both violence victimization and perpetration in the same study. Comparing these two rates directly provided better insight into whether one was a greater risk than the other. Also, this review synthesized evidence reported from studies investigating two distinct populations: (1) people with a mental illness and (2) people in the general population. Thus, as a secondary research aim, we then also compared rates of violence victimization and perpetration between these groups.
Method
Literature Search
Two searches were performed using PubMed, Embase, Web of Science, PsycINFO, and Criminal Justice Abstracts. Search 1 focused on papers reporting on cohorts or samples of people with mental illness and Search 2 focused on papers reporting on general population studies. In Search 1, we looked for the following terms in the title or abstract: [mental illness* OR mental disorder* OR psychiatric* OR schizophrenia OR psychosis OR psychotic OR substance use disorder OR personality disorder] AND [victim* OR subject* to violence OR exposed to violence] AND [perpetrat* OR offen*] AND [violen*]. In Search 2, we looked for the following terms in the title or abstract: [risk OR rate OR prevalence OR incidence] AND [victim* OR subject* to violence OR exposed to violence] AND [perpetrat* OR offen*] AND [violen*] NOT [mental illness* OR mental disorder* OR psychiatric* OR schizophrenia OR psychosis OR psychotic OR substance use disorder OR personality disorder]. Full-text papers were assessed for inclusion by two independent researchers. A manual search was also conducted using reference lists of previously published reviews and retrieved papers. This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Page et al., 2021) and Synthesis Without Meta-Analysis (Campbell et al., 2020) guidelines (see Tables A and B in Supplemental Materials) and was preregistered on the Open Science Framework (https://tinyurl.com/OSF-link-blinded). Both searches were conducted on September 30, 2021.
Inclusion Criteria
Studies identified by Search 1 were included if they met the following criteria:
(a) Empirical findings reported in research articles, brief reports and correspondence and published in English in peer-reviewed journals (books, book chapters, commentaries, conference proceedings, editorials, reviews, and dissertations/theses excluded);
(b) People studied were aged at least 15 years;
(c) People studied were diagnosed with a mental illness such as schizophrenia, bipolar disorder, major depression, other psychotic disorders, substance use disorders, or personality disorders;
(d) Did not limit the investigation to a specific demographic or patient subgroup (e.g., those experiencing homelessness) and/or specific types of crime (e.g., sexual abuse, sexual assault, domestic violence, intimate partner violence), apart from homicide;
(e) Explicitly reported prevalence and/or incidence rates of both violence victimization and violence perpetration over a specified time period (e.g., 1-year period, lifetime, etc.) within the same study cohort or sample.
All criteria for Searches 1 and 2 were exactly the same, except for Criterion c, which referred to the cohort or sample type:
(c) Examined unselected general population cohort or sample (i.e., not restricted to those diagnosed mental illness such as schizophrenia, bipolar disorder, major depression, other psychotic disorders, substance use disorders, or personality disorders).
Data Extraction
We used a standardized form to extract details from the included studies, including authors, year of publication, country, cohort or sample size, type of cohort or sample, definitions and terminology (i.e., mental illness, violence victimization, violence perpetration), data source(s), observation period, prevalence/incidence of victimization, prevalence/incidence of perpetration, risk factor profiles (if reported; see Table C in Supplemental Material), and rates of being both a victim and a perpetrator (i.e., victim-offender overlap; if reported; see Table C in Supplemental Material). Where rates of victimization and/or perpetration were reported for subgroups, but not for the cohort or sample overall, the latter were calculated from the numbers provided (e.g., combining rates for males and females). As preregistered, data were extracted by a primary researcher and checked by a second independent researcher.
Study Quality
We also conducted a quality assessment of all included studies using the Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data. These criteria aimed to assess the extent to which representative sampling had been implemented, appropriate recruitment, adequate sample size, appropriate description and reporting of study subjects and setting, adequate data coverage of the identified sample, valid and reliable measurement, appropriate statistical analysis, and identification and accounting for confounding factors or subgroups (see Munn et al., 2014). For evaluating validity, we split this question into three parts to cover methods used for the identification of (1) mental illness (for Search 1 only), (2) violence victimization, and (3) violence perpetration. Reliable measurement of mental illness was also only applicable to Search 1 results. No studies were excluded based on quality rating, although study quality is discussed in our narrative synthesis.
Analysis Plan
In this preregistered systematic review, we aimed to present a narrative synthesis of results accompanying a tabular summary of the reviewed studies. This synthesis was structured around our main research questions to better understand (1) risks of violence victimization and perpetration in the same cohort or sample of adults with mental illness and how these risks compare to one another and (2) risks of violence victimization and perpetration in the same cohort or sample of unselected adults in the general population and how these risks compare to one another. Additionally, we narratively synthesized findings from these two groups of studies in two ways. First, we examined findings from studies with either adults with mental illness or those in the general population. Second, we reported and discussed a small set of studies that investigated both adults with mental illness and general population adults (i.e., investigations of victimization and perpetration in groups of adults with diagnosed mental illness compared with matched general population comparators).
Results
For Search 1, we identified 2,024 articles. 1 After removing duplicates, 975 titles and abstracts were screened, narrowing eligible articles to 42. Of these, 12 were deemed eligible: 9 articles solely reported on samples or cohorts with mental illness and 3 articles reported on samples or cohorts with mental illness along with matched comparison groups. For Search 2, we identified 7,704 articles. 2 After removing duplicates, 3,861 titles and abstracts were screened, narrowing eligible articles to 55. Of these, 13 were deemed eligible for inclusion (see Figure 1).
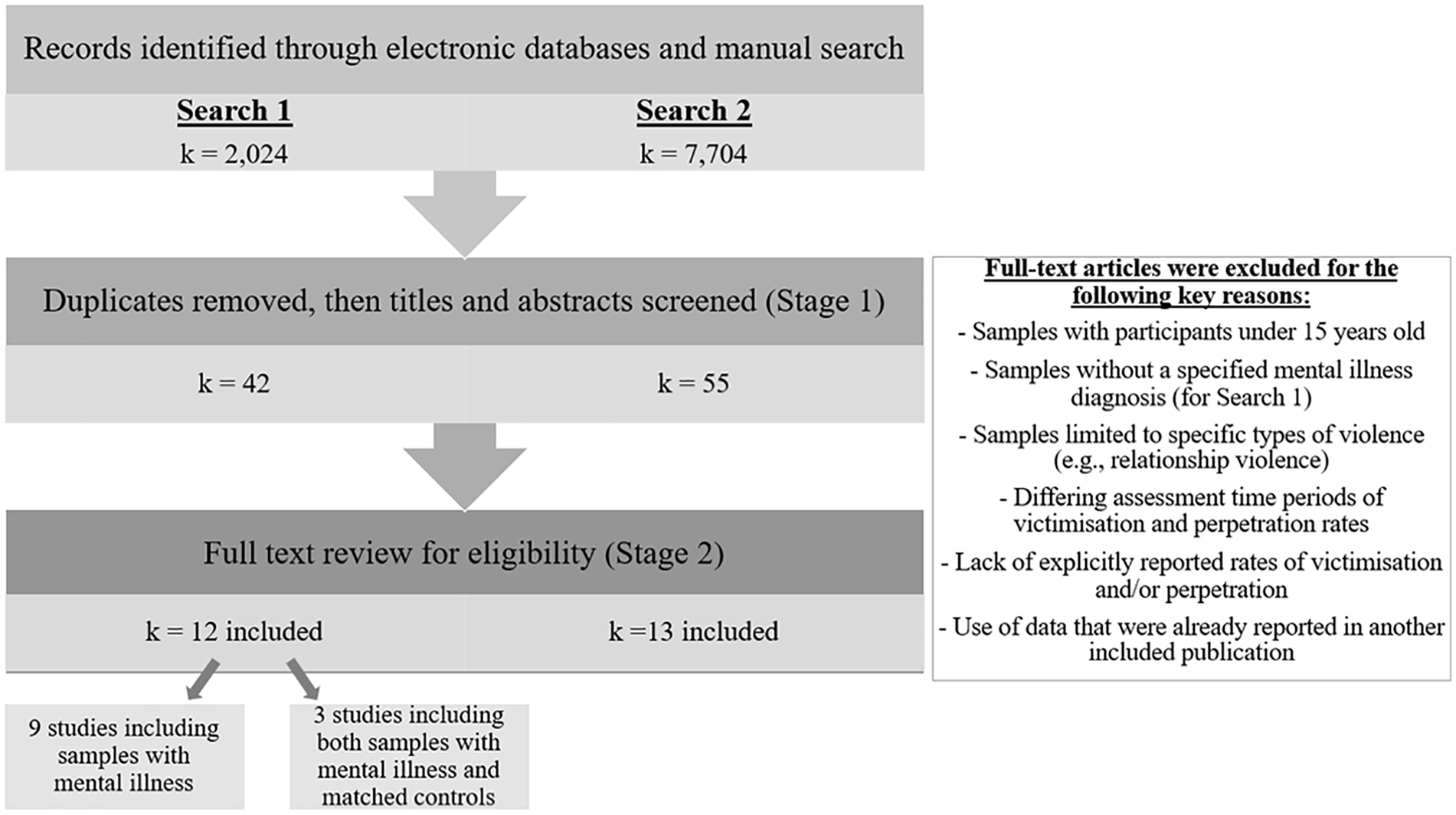
Flow chart of search outcomes.
Description of Included Studies
The characteristics of the included studies are reported in Tables 1 to 3.
Description of Included Studies With Samples of Individuals With Mental Illness.
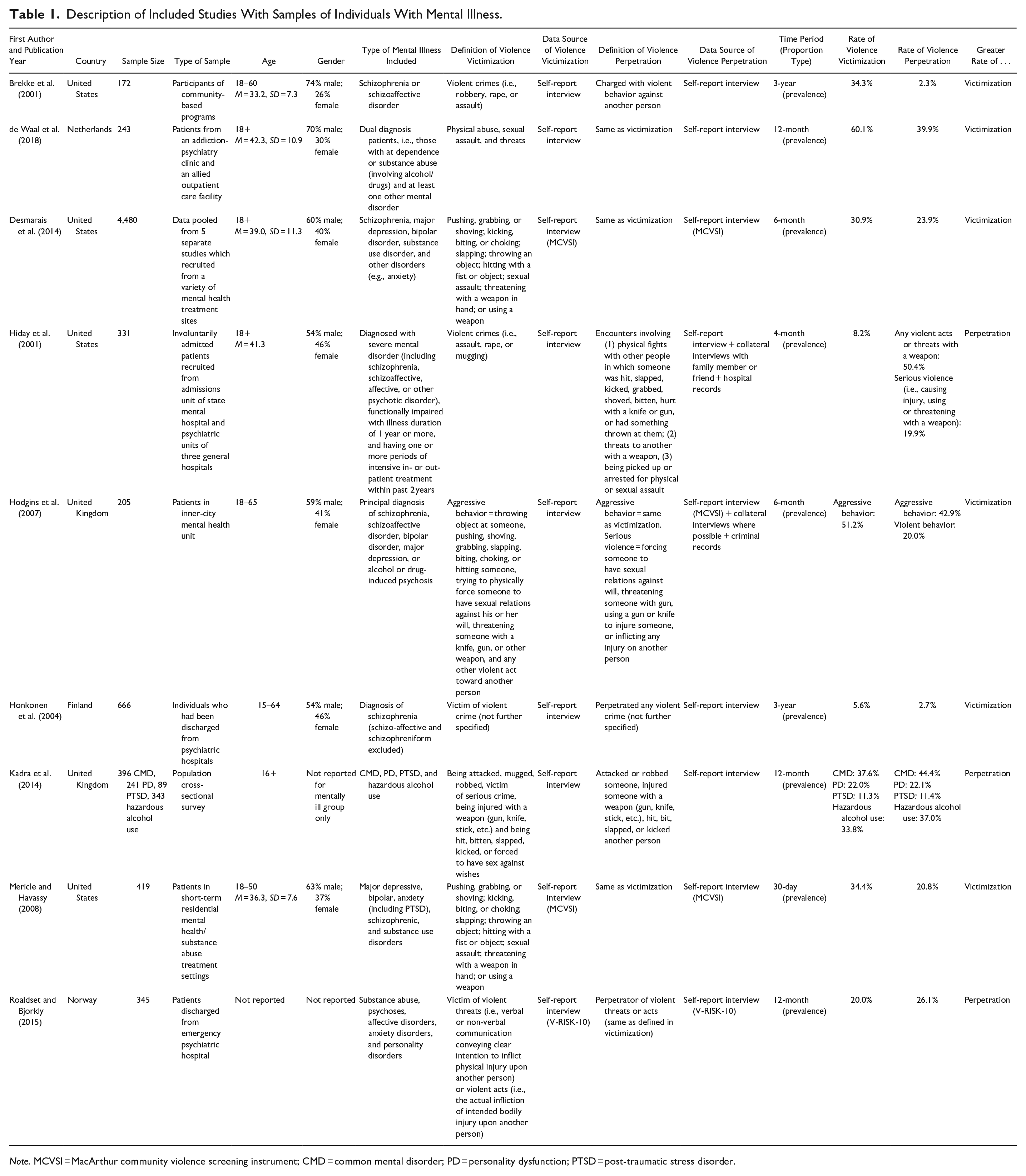
Note. MCVSI = MacArthur community violence screening instrument; CMD = common mental disorder; PD = personality dysfunction; PTSD = post-traumatic stress disorder.
Description of Included Studies With General Population Samples.
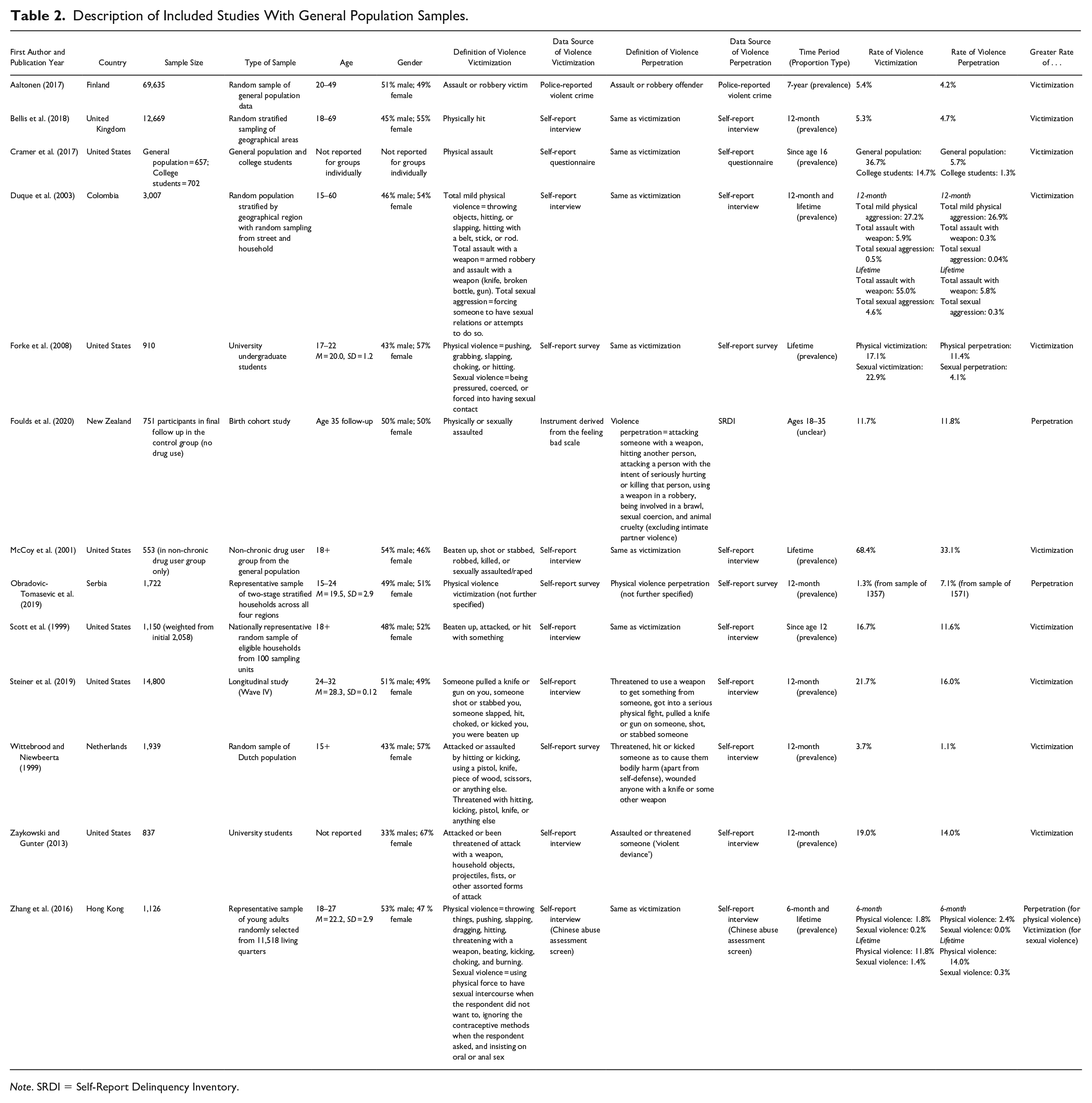
Note. SRDI = Self-Report Delinquency Inventory.
Description of Included Studies With Samples of Individuals With Mental Illness and Matched Control Samples.
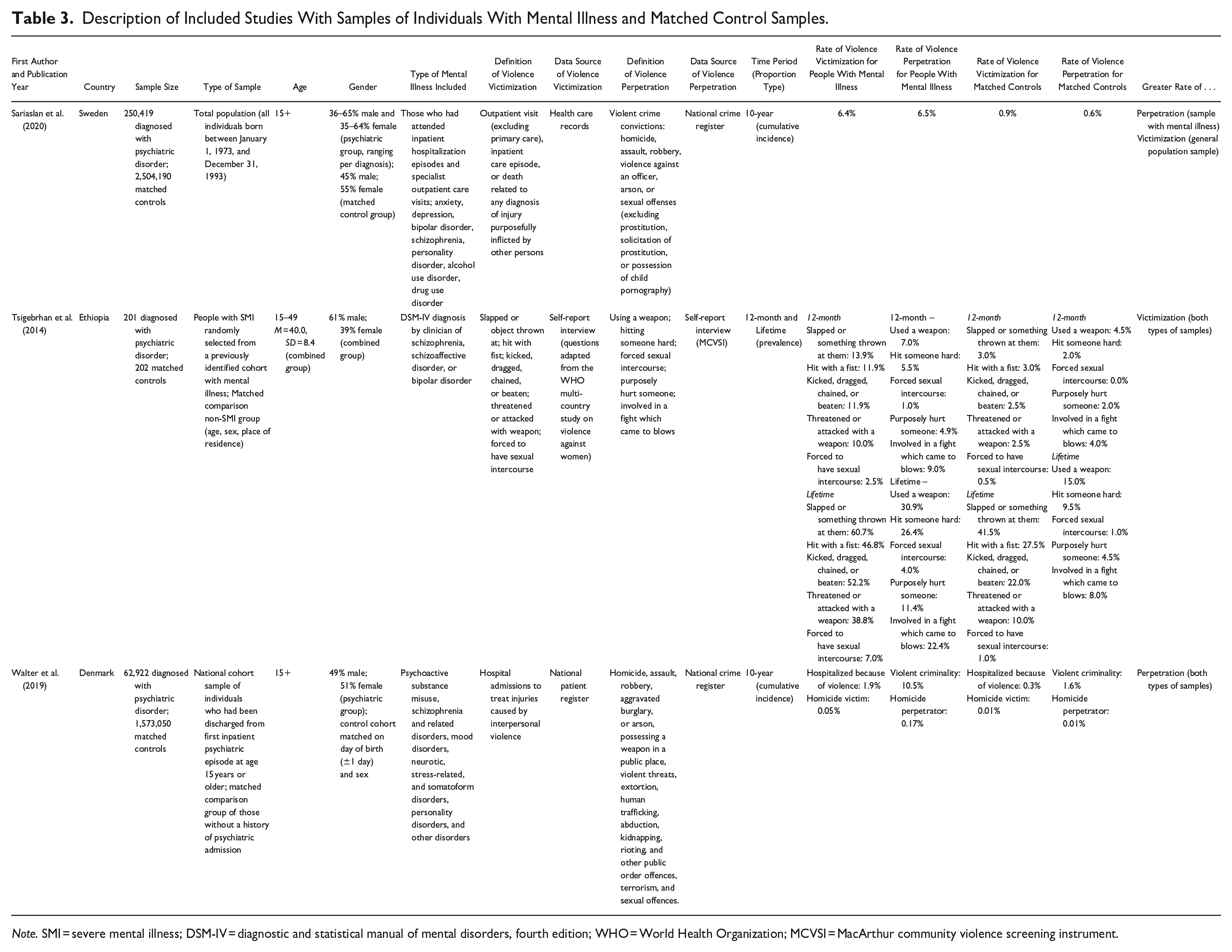
Note. SMI = severe mental illness; DSM-IV = diagnostic and statistical manual of mental disorders, fourth edition; WHO = World Health Organization; MCVSI = MacArthur community violence screening instrument.
Year of publication
Across the searches, studies were published across a similar time frame. The 9 studies identified by Search 1 that exclusively reported on cohorts or samples with mental illness were published between 2001 and 2018; the 13 studies identified by Search 2 were published between 1999 and 2020. The three studies that reported both cohort and sample types were published more recently, with respective publication dates of 2014, 2019, and 2020.
Country
For studies that exclusively reported on cohorts or samples with mental illness (n = 9), publications came from five countries: four from the United States (Brekke et al., 2001; Desmarais et al., 2014; Hiday et al., 2001; Mericle & Havassy, 2008), two from the United Kingdom (Hodgins et al., 2007; Kadra et al., 2014), and one each from Finland (Honkonen et al., 2004), the Netherlands (de Waal et al., 2018), and Norway (Roaldset & Bjorkly, 2015). For studies that exclusively reported on general population cohorts or samples (n = 13), publications came from eight countries: six from the United States (Cramer et al., 2017; Forke et al., 2008; McCoy et al., 2001; Scott et al., 1999; Steiner et al., 2019; Zaykowski & Gunter, 2013), and one each from Hong Kong (Zhang et al., 2016), Colombia (Duque et al., 2003), Finland (Aaltonen, 2017), the Netherlands (Wittebrood & Nieuwbeerta, 1999), New Zealand (Foulds et al., 2020), Serbia (Obradovic-Tomasevic et al., 2019), and the United Kingdom (Bellis et al., 2018). Three studies examined cohorts or samples that included both adults with mental illness and matched general population comparison groups; these studies were conducted in Denmark (Walter et al., 2019), Ethiopia (Tsigebrhan et al., 2014), and Sweden (Sariaslan et al., 2020).
Study setting
For Search 1 studies that reported only on cohorts or samples with mental illness (n = 9), all studies but one consisted of patients who were currently being treated in or had recently been discharged from mental health services, including community-based programs, psychiatric clinics/hospitals, and outpatient care facilities. The remaining study recruited a random sample from the general population and then reported on the subsample of participants who had been diagnosed with a mental disorder (Kadra et al., 2014).
For Search 2, most studies consisted of general population cohorts or samples (n = 8), with two studies that examined university students (Forke et al., 2008; Zaykowski & Gunter, 2013), one study that reported both on a general population group and a group of university students (Cramer et al., 2017), and two studies that reported on birth (Foulds et al., 2020) or other longitudinal cohorts (Steiner et al., 2019).
For articles that reported on both types of study (i.e., including individuals with mental illness and those from the general population), two were national cohorts (total population) with individuals with mental illness matched to comparators without mental illness by age and sex (Sariaslan et al., 2020; Walter et al., 2019). The remaining study sample consisted of people with severe mental illness who were randomly selected from a previously identified cohort of persons diagnosed with mental illnesses and matched to a comparison group by age, sex, and place of residence (Tsigebrhan et al., 2014).
Study cohort or sample
Inclusion criteria ensured that all cohorts or samples consisted of a mix of males and females who were aged at least 15 years. For Search 1, which identified studies that reported only cohorts or samples of people with mental illnesses (n = 9), three included participants aged 18 and older (Desmarais et al., 2014; de Waal et al., 2018; Hiday et al., 2001) and one included participants aged 16 and older (Kadra et al., 2014). The other four studies examined persons aged between 15 and 64 years (Honkonen et al., 2004), 18 and 50 years (Mericle & Havassy, 2008), 18 and 60 years (Brekke et al., 2001), and 18 and 65 years (Hodgins et al., 2007). Age was not explicitly reported in the remaining publication (Roaldset & Bjorkly, 2015). All samples reported inclusion of more males than females, with the percentage of females ranging from 26 to 46% (two papers did not report the cohort’s or sample’s gender breakdown: Kadra et al., 2014; Roaldset & Bjorkly, 2015).
For Search 2, two studies included persons aged 18 and older (McCoy et al., 2001; Scott et al., 1999) and one included persons aged 15 and older (Wittebrood & Nieuwbeerta, 1999). Four studies examined young adults (17–22, Forke et al., 2008; 15–24, Obradovic-Tomasevic et al., 2019; 24–32, Steiner et al., 2019; 18–27, Zhang et al., 2016) and three examined middle-aged adults (20–49, Aaltonen, 2017; 18–69, Bellis et al., 2018; 15–60, Duque et al., 2003). The birth cohort study reported data from the year when all members of the cohort were 35 years old (Foulds et al., 2020) and the remaining two studies did not report the age ranges of the people who were studied (Cramer et al., 2017; Zaykowski & Gunter, 2013). In the cohorts or samples of the studies that were identified by Search 2, there was less variability in the gender split versus those identified by Search 1, with the percentage of females ranging from 47 to 57% across all Search 2 studies (one study did not report this information: Cramer et al., 2017).
For the three studies that examined cohorts or samples of people diagnosed with mental illness as well as matched comparison groups, the two national cohort studies examined persons aged 15 years and older (Sariaslan et al., 2020; Walter et al., 2019) and the other study examined people aged 15 to 49 years (Tsigebrhan et al., 2014). The gender splits across the studies were as follows: Tsigebrhan et al. (2014), 39% females; Walter et al. (2019), 55% females; Sariaslan et al. (2020), between 35 and 64% females depending on mental illness diagnosis, with the comparison group consisting of 51% females. Across each of these studies, the general population comparison group was matched to the group with mental illness diagnoses using age and sex.
Psychiatric diagnoses
Search 2 included general population cohorts or samples in which psychiatric diagnoses were not explicitly measured or reported. For Search 1 studies that reported only on cohorts or samples of people diagnosed with mental illnesses (n = 9), two specifically examined schizophrenia-related disorders (Brekke et al., 2001; Honkonen et al., 2004), one examined dual diagnoses of substance use disorder along with another mental illness (de Waal et al., 2018), and one separately reported on common mental disorders, personality dysfunction, post-traumatic stress disorder (PTSD), and alcohol use (Kadra et al., 2014). The remaining four studies included a mix of diagnoses, including schizophrenia, major depression, bipolar disorder, substance use disorder, anxiety disorders, personality disorders, and other disorders (Desmarais et al., 2014; Hiday et al., 2001; Hodgins et al., 2007; Mericle & Havassy, 2008).
The studies that examined cohorts or samples of people diagnosed with mental illnesses and matched comparison groups (n = 3) consisted of people diagnosed with a range of conditions, as follows: anxiety disorders, depression, bipolar disorder, schizophrenia, personality disorder, alcohol use disorder, and drug use disorder (Sariaslan et al., 2020); schizophrenia, schizoaffective disorder, and bipolar disorder (Tsigebrhan et al., 2014); psychoactive substance misuse disorders, schizophrenia and related disorders, mood disorders, neurotic, stress-related, and somatoform disorders, personality disorders, and other disorders (Walter et al., 2019).
Observation periods for examining violence victimization and perpetration
The observation periods for occurrence of violence victimization or perpetration differed across studies. For studies that examined cohorts or samples with mental illness (n = 9), one used a 30-day period (Mericle & Havassy, 2008), one used a 4-month period (Hiday et al., 2001), two used a 6-month period (Desmarais et al., 2014; Hodgins et al., 2007), two used a 12-month period (de Waal et al., 2018; Kadra et al., 2014), and two used a 3-year period (Brekke et al., 2001; Honkonen et al., 2004). For studies that examined general population cohorts or samples (n = 13), one observed violent episodes since age 12 (Scott et al., 1999), one since age 16 (Cramer et al., 2017), one between the ages of 18 and 35 (Foulds et al., 2020), five used a 12-month observation period (Bellis et al., 2018; Obradovic-Tomasevic et al., 2019; Steiner et al., 2019; Wittebrood & Nieuwbeerta, 1999; Zaykowski & Gunter, 2013), one used a 7-year period (Aaltonen, 2017), and two used a lifetime period (Forke et al., 2008; McCoy et al., 2001). The remaining two studies reported multiple observation periods, with one reporting both 6-month and lifetime rates (Zhang et al., 2016) and the other reporting both 12-month and lifetime rates (Duque et al., 2003). For studies examining persons with mental illness and matched comparators (n = 3), two reported cumulative incidence over a 10-year period (Sariaslan et al., 2020; Walter et al., 2019) and the other reported both 12-month and lifetime rates (Tsigebrhan et al., 2014).
Data sources
Nearly all included studies relied on self-reported data regarding experiences of violence victimization and perpetration. Specifically, all studies that examined cohorts or samples of persons diagnosed with mental illnesses utilized self-reports from interviews or tools, with two additionally reporting other methods including collateral interviews and hospital records (Hiday et al., 2001) or criminal records (for violence perpetration; Hodgins et al., 2007). For studies that examined general population cohorts or samples, all but one utilized self-reports exclusively, with the other using victimization and perpetration information from a database of police-reported violent crimes (Aaltonen, 2017). Of the three studies that investigated persons with diagnosed mental illnesses and matched comparison groups, Tsigebrhan et al. (2014) used self-report methods and Sariaslan et al. (2020) and Walter et al. (2019) examined interlinked national registry data to identify injuries caused by interpersonal violence that required healthcare services (a proxy for victimization) and national crime registers to identify violent crime convictions (i.e., violence perpetration).
Study quality
As previously mentioned, we used the Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data to assess study quality. A summary of quality ratings is presented in Table F in Supplemental Materials. Between 9 (Search 2) and 11 (Search 1) criteria were assessed as to whether they were clearly met (“yes”), undetermined (“unclear”), or not met (“no”).
Of the studies examining persons diagnosed with mental illnesses, one met all criteria apart from valid methods of identification for violence victimization and perpetration (due to only using self-reports rather than an objective measure; Kadra et al., 2014). In contrast, two studies were of low quality, with fewer than four “yes” responses to the criteria (Desmarais et al., 2014; Roaldset & Bjorkly, 2015), with the remaining six studies rated a mix of “yes,” “unclear,” and “no” ratings.
Of the studies that investigated persons in general population, two met most criteria; one met all apart from reporting confidence intervals (Aaltonen, 2017), and the other met all apart from valid methods of ascertaining violence victimization and perpetration (due to only using self-reports rather than an objective measure; Steiner et al., 2019). Five showed low levels of study quality, meeting just one or two of the nine criteria (Cramer et al., 2017; Forke et al., 2008; McCoy et al., 2001; Wittebrood & Nieuwbeerta, 1999; Zaykowski & Gunter, 2013).
Studies that had examined persons diagnosed with mental illnesses as well as individuals in the general population were generally of high quality, meeting 8 of the 11 criteria (Tsigebrhan et al., 2014), 10 of the criteria (Sariaslan et al., 2020), or all 11 criteria (Walter et al., 2019).
Most of the included studies fell short on three of the criteria for the same reasons: first, as previously discussed, nearly all studies used self-report rather than objective measures for the identification of violence victimization. Second, only four of the included studies (n = 25) reported confidence intervals for reporting the victimization and perpetration rate estimates. Other common limitations in quality included a lack of (1) reporting or clarity on participant sampling (if applicable), (2) statistical power analyses, and/or (3) consideration of response rate (if applicable) (Tables 4 and 5) .
Summary of Critical Findings.

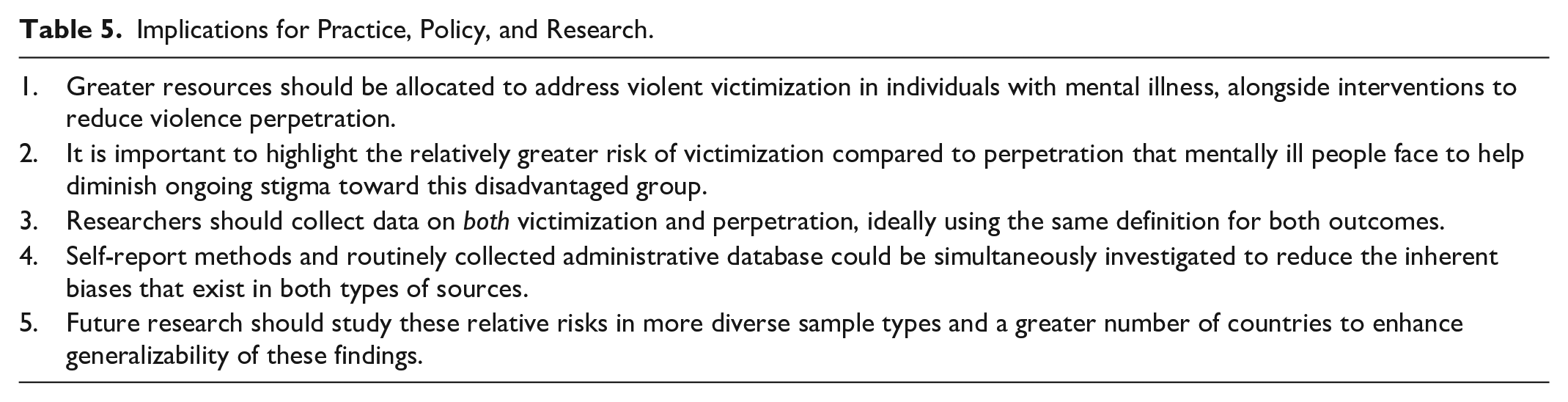
Implications for Practice, Policy, and Research.
Narrative Synthesis
As anticipated at preregistration, the set of included studies contained multiple variations in study design and methodology. Specifically, studies differed on several factors, including the time frame for estimating rates of victimization and perpetration, sampling approaches, terminology/definitions (of mental illness, violence), and data sources (see Table 1). To best synthesize these heterogeneous studies, we grouped studies first by observation period. The observation period was the most appropriate initial grouping to compare victimization and perpetration rates across studies with various time durations.
Prevalence or incidence rates of victimization and perpetration were reported directly from the included papers. Across the included papers, the terms prevalence and incidence tended to be used rather imprecisely and not always in line with the generally accepted usage (Porta, 2014). In general, prevalence was used in many papers to describe proportions (i.e., number of individuals experiencing the outcome divided by the total sample) over an indicated time period. The great majority of the studies provided information about rates of violence in this way, with only two studies reporting cumulative incidence (i.e., absolute risk modelled as a percentage value, with attrition, unequal follow-up time and competing risks accounted for; Sariaslan et al., 2020; Walter et al., 2019). Additionally, one study reported pooled victimization and perpetration rates across its entire observation period, but provided no specific indication regarding how these proportions were calculated, including whether the reported values were prevalence or incidence rates (Foulds et al., 2020). Some studies of prevalence reported gender-specific estimates but did not directly report prevalence for all persons in persons in the sample or cohort (e.g., Aaltonen, 2017; Bellis et al., 2018; Hodgins et al., 2007; Zhang et al., 2016). For these studies, we calculated and reported the prevalence rates for all persons in the sample or cohort if we were able to.
Our narrative synthesis reports findings across three categories of studies. First, we report on studies that examined cohorts or samples of people diagnosed with mental illness. Second, we report on studies that were conducted using general population cohorts or samples. Finally, we describe a small set of studies that examined people diagnosed with mental illnesses as well as an additional group of matched comparators who were sampled from the general population. These studies, though limited in number, provide the best insight into our research question as we can observe victimization and perpetration rates for both population types within the same applied study parameters.
Because of the heterogeneous nature of the reviewed studies, our narrative synthesis focuses mainly on a descriptive summary of the reported relative risks of violence victimization and perpetration across studies rather than on formally pooling absolute rates. Specifically, for each reviewed study, we report on whether the rate of victimization or perpetration was greater and then summarize these findings across each category of study. In the Discussion, we then further consider comparisons of rates within sample/cohort types as well as between sample/cohort types. As part of our analysis, we also reviewed methodological variations between studies that would contribute to differences in findings (e.g., data sources, definitions, study quality, etc.), in textual or tabular form. This between-study heterogeneity is then further explored in the Discussion section.
Studies of Persons Diagnosed With Mental Illness
30-Day Period
Mericle and Havassy (2008) investigated 419 patients in the United States in short-term residential mental health and/or substance abuse treatment settings diagnosed with a variety of mental illnesses. Via interviews, they found that a greater proportion of participants reported violence victimization (34.4%) than violence perpetration (20.8%) in the past month.
3- to 6-Month Period
Hiday et al. (2001) interviewed 331 involuntarily admitted patients diagnosed with a range of disorders in the United States and found higher rates of violence perpetration than victimization. Specifically, over a 4-month period, half (50.4%) of the sample engaged in violent acts or threats with a weapon and 19.9% perpetrated more serious violence (i.e., violence causing injury or using or threatening with a weapon), whereas only 8.2% of participants reported violence victimization, which included being a victim of an assault, rape, or mugging. Two other studies examined violence over a 6-month period and found greater levels of victimization than perpetration. Hodgins et al. (2007) examined 205 patients in an inner-city mental health unit in the United Kingdom. Over half of the sample (51.2%) reported being victimized by aggressive behavior in the past 6 months, while 42.9% reported acting aggressively toward other people. Desmarais et al. (2014) combined samples from five separate studies from the United States that included a total of 4,480 participants diagnosed with a range of mental illnesses. Using a definition that delineated more serious violence, including sexual assault, use of a weapon, and so on, they found that 30.9% of participants experienced violence victimization and 23.9% perpetrated violence.
12-Month Period
Three studies examined violence over a 12-month period and reported mixed findings. In the Netherlands, de Waal et al. (2018) recruited 243 participants with comorbid diagnoses of a substance use disorder and another mental disorder and interviewed participants about their experiences of physical abuse, sexual assault, and threats. They found that more participants experienced violence victimization within the past year (60.1%) than had perpetrated violence (39.9%). Conversely, in a study rated as high quality, Kadra et al. (2014) randomly recruited participants from the UK general population and then assessed interview data from individuals with a common mental disorder (n = 396), personality dysfunction (n = 241), PTSD (n = 89), or hazardous alcohol use (n = 343). Though rates were similar for each diagnostic category, there was a slightly greater proportion of participants who reported violence perpetration compared with violence victimization, with victimization rates ranging from 11.3 to 37.6% and perpetration rates ranging from 11.4 to 44.4%. Similarly, Roaldset and Bjorkly (2015) interviewed 345 patients who were discharged from an emergency psychiatric hospital in Norway and found that 20.0% reported being a victim of violent threats or acts with a slightly greater proportion reporting perpetrating violent threats or acts (26.1%).
3-Year Period
Two studies examined violence over several years, and both found higher rates of victimization than perpetration. Brekke et al. (2001) interviewed 172 participants with schizophrenia-related disorders from community-based programs in the United States. Over a third (34.3%) of participants reported being victims of robbery, rape, or assault in the past 3 years, whereas only 2.3% reported having been charged with violent behavior against another person. Similarly, Honkonen et al. (2004) followed 666 individuals diagnosed with schizophrenia who had been discharged from psychiatric hospitals in Finland. Lower levels of victimization were reported than in Brekke et al.’s sample, with 5.6% of participants reporting violent crime victimization. Still, this rate more than doubled the perpetration rate, with only 2.7% of participants reporting perpetrating any violent crime.
Summary
Rates of violence victimization ranged from 5.6 to 60.1% depending on the specific study characteristics including country, sample or cohort type, length of observation period, data source, and outcome definitions. Rates of violence perpetration were also varied greatly from 2.3 to 50.4%. Across these nine studies that investigated persons diagnosed with mental illnesses, six reported higher rates of violence victimization than perpetration, whereas three reported higher rates of perpetration than victimization.
Studies Conducted Using General Population Samples or Cohorts
6-Month Period
Zhang et al. (2016) interviewed 1,126 young adults in Hong Kong regarding recent experiences with physical and sexual violence. Low rates of victimization were found: 1.8% reported physical violence victimization and 0.2% reported sexual violence victimization. A slightly higher proportion reported physical violence perpetration (2.4%), though no participants reported sexual violence perpetration.
12-Month Period
Six studies reported on violence victimization and perpetration within the past year. Obradovic-Tomasevic et al. (2019) reported that 1.3% of their Serbian general population sample of 1,357 people reported physical violence victimization, while 7.1% of their sample of 1,571 people reported physical violence perpetration. All other studies showed higher rates of victimization than perpetration. Bellis et al. (2018) asked 12,669 UK general population participants about being physically hit: 5.3% reported past-year victimization and 4.7% reported past-year perpetration. In Colombia, Duque et al. (2003) similarly reported on mild violence in a sample of 3,007: 27.2% of participants reported victimization and 26.9% reported perpetration. These authors also described more severe forms of violence, showing 5.9 and 0.5% victimization rates and 0.3 and 0.04% perpetration rates for total assault with a weapon and total sexual aggression, respectively. Similarly, fairly low rates were found by Wittebrood et al. (1999) in a sample of 1,939, with 3.7% of participants reporting violence victimization and 1.1% reporting violence perpetration in the Netherlands. Steiner et al. (2019) showed higher rates in their high-quality study, with 21.7% of their U.S. general population sample of 14,800 participants reporting violence victimization and 16.0% reporting violence perpetration. Zaykowski and Gunter (2013) posed similar questions in a sample of 837 university students in the United States and found that 19.0% reported being a victim of assault while 14.0% reported assaulting or threatening anyone within the past year.
7-Year Period
Aaltonen (2017) examined a Finnish general population sample of 69,635 people using police-reported crime data in a study rated as high quality. They found that 5.4% of the sample were victims of an assault or robbery and 4.2% of the sample acted as perpetrators in assaults or robberies in the 7-year period.
17-Year Period
Foulds et al. (2020) followed a New Zealand birth cohort through their 35th year and found similar rates of self-reported violence victimization and perpetration during their adult lives from ages 18 through 35 (n = 751). Specifically, 11.7% of the pooled cohort reported being physically or sexually assaulted during the time period, whereas 11.8% of the pooled cohort reported perpetrating violence.
Since Ages 12/16
Scott et al. (1999) asked a 1,150-person U.S. general population sample about their experiences with physical assault since age 12. They found that 16.7% of the sample reported being violently victimized whereas 11.6% reported perpetrating violence. Cramer et al. (2017) similarly examined rates of physical assault, asking both a general population sample of 657 people and a college sample of 702 students in the United States about their experiences since age 16. Of the general population sample, 36.7% said they had been victims of physical assault and 5.7% reported acting as a perpetrator of physical assault. College students reported lower rates, with rates of 14.7% victimization and 1.3% of perpetration since age 16.
Lifetime
The young adult sample from Zhang et al. (2016) also reported lifetime rates of physical and sexual violence (n = 1,126). As with the 6-month period, there was a higher rate of physical violence perpetration (14.0%) than victimization (11.1%), but a lower rate of sexual violence perpetration (0.27%) than victimization (1.42%). Duque et al.’s (2003) general population sample of 3,007 also reported lifetime rates of total assault with a weapon and total sexual aggression. In this study, victimization rates (55.0 and 5.8%, respectively) were higher than perpetration rates (4.6 and 0.3%, respectively). Similarly, McCoy et al.’s (2001) examination of a U.S. general population (n = 553) found higher rates of victimization than perpetration, with 68.4% of the sample reporting having been beaten up, shot, stabbed, robbed, or sexually assaulted/raped, and only a third of the same sample (33.1%) reporting being a perpetrator of those actions. Forke et al. (2008) reported physical and sexual violence in a sample of 910 U.S. university students and also found greater victimization rates (17.1 and 22.9%, respectively) than perpetration rates (11.4 and 4.1%, respectively).
Summary
Rates of violence victimization in general population cohorts or samples ranged from 1.3 to 68.4% depending on the specific study characteristics including country, sample features, length of observation period, and definition and data source of violent incidents. Rates of violence perpetration ranged from 1.1 to 33.1% (excluding rates of sexual violence that were reported separately). Across these 13 studies examining rates of violence victimization and perpetration in the general population, 10 showed higher rates of victimization than perpetration. Two showed higher rates of perpetration compared to victimization, though in one of these studies, the rates were nearly the same (11.8 vs. 11.7%). The final study was mixed depending on the type of violence: physical violence perpetration occurred more frequently than physical violence victimization both over a 6-month and lifetime period, but sexual violence victimization was more common than sexual violence perpetration over both time periods.
Studies Investigating People Diagnosed With Mental Illnesses With Matched General Population Comparison Groups
12-Month Period
Tsigebrhan et al. (2014) recruited a sample of 201 people in Ethiopia with schizophrenia, schizoaffective disorder, or bipolar disorder and a matched comparison group (n = 202) using age, sex, and place of residence for their high-quality study. They interviewed participants concerning a range of interpersonal violence experiences. Participants diagnosed with mental illnesses reported higher levels of victimization (ranging from 2.5 to 13.9% depending on the type of violent episode) than perpetration (ranging from 1.0 to 9.0%). Furthermore, these rates were higher than those reported from the sample of persons without mental illnesses, who reported both lower rates of victimization (ranging from 0.5 to 3.0% depending on the type of violent experience) and perpetration (ranging from 0.0 to 4.5%) than the group with mental illness.
10-Year Period
The two high-quality studies examining violence victimization and perpetration over a 10-year period found a similar pattern of results. Both studies examined violent crime convictions to determine the cumulative incidence of perpetration and hospitalization admissions caused by interpersonal violence to determine the cumulative incidence victimization rates. In Sweden, Sariaslan et al. (2020) found a slightly higher cumulative incidence for perpetration (6.5%) than victimization (6.4%) in the group with diagnosed mental illnesses (n = 250,419). The matched comparison sample showed lower rates of both victimization and perpetration, with a higher cumulative incidence of victimization (0.9%) than perpetration (0.6%; n = 2,504,190). In Denmark, Walter et al. (2019) found higher rates of perpetration in both groups. The group with mental illness showed a cumulative incidence of 10.5% for violent criminality and a cumulative incidence of 1.9% for being hospitalized because of violence (n = 62,922). These rates were considerably lower for the matched comparison group, with a cumulative incidence of 1.60% for violent criminality and 0.30% for hospitalization due to violence (n = 1,573,050).
Lifetime
Tsigebrhan et al. (2014) also investigated lifetime rates of victimization and perpetration in the same study that assessed these outcomes over a 12-month period. A similar pattern emerged as in the 12-month rates. Specifically, there was a higher frequency of perpetration in the group with mental illness (4.0–30.9%) compared to the general population sample (1.0–15.0%). However, there was also a greater rate of victimization in the group with mental illness (7.0–60.7%) than in the general population group (1.0–41.5%). Lifetime rates of victimization in both groups were greater than lifetime perpetration rates.
Summary
Three studies investigated people diagnosed with mental illness and matched general population comparison groups. One study found that experiences of victimization were more common than acts of perpetration among both groups (Tsigebrhan et al., 2014). One study found the opposite, with higher cumulative incidence of perpetration than victimization among both groups (Walter et al., 2019). The final study found higher cumulative incidence of perpetration than victimization for the group with mental illness, but higher cumulative incidence of victimization than perpetration for the matched control cohort (Sariaslan et al., 2020). All three studies showed higher rates of both victimization and perpetration among individuals with mental illness than in the matched general population comparison groups.
Discussion
Individuals diagnosed with a mental illness are known to be at increased risk of both violence victimization and perpetration when compared to the general population. But of these two risks, which is the greater? In this systematic review, we found 9 studies examining both outcomes in samples or cohorts of persons with mental illnesses, 13 general population-based studies that examined both outcomes, and 3 studies that examined both victimization and perpetration in both population types. Overall, the findings were mixed and the methodological approaches heterogeneous. Broadly, we found (1) higher rates of victimization than perpetration for both individuals with mental illness and those in the general population and (2) higher rates of both victimization and perpetration for those with mental illness compared to those in the general population (Table 4).
Comparison of Rates of Victimization and Perpetration Within Sample/Cohort Types
Most studies that have investigated the two outcomes in samples or cohorts of people with mental illness have reported higher rates of violence victimization than perpetration and, of the three studies that showed otherwise, two reported rates of victimization and perpetration that were similar (Kadra et al., 2014; Roaldset & Bjorkly, 2015). Just one study reported a much higher frequency of perpetration than victimization (Hiday et al., 2001). Of note, this study used a broader definition of perpetration than of victimization: victimization was defined as experiencing a violent crime (i.e., an assault, rape, or robbery) while the definition of perpetration included lesser forms of violence, such as physical fights and threats with a weapon. As noted by Choe et al. (2008), the high rate of violence perpetration in this study could also be due to the sample comprising involuntarily admitted patients interviewed soon after commitment, given the possibility that their commitment was, at least in part, due to their violent behavior. Additionally, information about participants’ perpetration came from collateral interviews and hospital records in addition to self-reports, whereas information about victimization was based primarily on self-reports. In most of the other studies in this category, victimization and perpetration were assessed using the same definition and data source. In fact, the one other included study with differing definitions also showed a large discrepancy between rates of victimization and perpetration: Brekke et al. (2001) defined victimization as experiencing a violent crime (including robbery, rape, or assault), whereas perpetration was defined as being charged with violent behavior against another person. Given the additional layer of formalities that receiving an official legal charge would entail, it is perhaps unsurprising over a third of participants reported being victimized while only 2.3% of participants reported perpetration in this study.
The majority of studies investigating general population samples or cohorts also found higher rates of victimization than perpetration and again, two further studies with higher perpetration rates actually found similar victimization rates (Foulds et al., 2020; Zhang et al., 2016). In the remaining study with higher rates of perpetration (Obradovic-Tomasevic et al., 2019), the study’s quality was hard to judge because the applied definitions of violence victimization or perpetration were not specified.
The findings of studies that investigated both persons diagnosed with mental illness and general population comparators were mixed. The two studies that examined total population cohorts using routinely collected data to calculate cumulative incidence showed greater levels of perpetration than victimization for individuals diagnosed with mental illnesses, though victimization and perpetration rates were similar in one of these studies (6.4 vs. 6.5%; Sariaslan et al., 2020). For the general population cohorts in these two studies, one showed greater perpetration than victimization for both reported outcomes (i.e., hospitalizations vs. violent criminality and homicide victims vs. perpetrators; Walter et al., 2019), whereas the other showed the opposite (Sariaslan et al., 2020). The third study, which relied on self-report, showed greater levels of victimization than perpetration across both sample types over a 12-month and lifetime observation period (Tsigebrhan et al., 2014). Marked differences in the characteristics of the respective data sources are likely to have played a key contributory role in the generating the discrepant findings.
Comparison of Rates of Victimization and Perpetration Between Sample/Cohort Types
Comparing victimization and perpetration rates across studies of persons with diagnosed mental illnesses and studies of individuals in the general population samples is challenging due to the marked degree of heterogeneity in study methodologies and definitions. Broadly, however, of the studies examining comparable timeframes (i.e., 3-to-6-month and 12-month periods), higher rates of victimization and perpetration were reported from the studies that investigated persons with diagnosed mental illnesses compared to those that included individuals in the general population (Bellis et al., 2018; de Waal et al., 2018; Kadra et al., 2014; Obradovic-Tomasevic et al., 2019; Steiner et al., 2019; Wittebrood & Nieuwbeerta, 1999; Zaykowski & Gunter, 2013). This is consistent with the literature supporting an association between mental illness and risk of both violence victimization and perpetration (e.g., de Vries et al., 2018; Fazel et al., 2009; Latalova et al., 2014; Maniglio, 2009; Whiting et al., 2021). One exception was a study involving a general population sample (Duque et al., 2003) that reported higher rates of victimization and perpetration than one of the studies of participants with mental illness (Roaldset & Bjorkly, 2015). However, the higher rates were in relation to broader definitions of violence (defined by the authors as “mild physical aggression,” which included throwing objects, hitting or slapping, hitting with a belt, stick or rod); when just considering armed robbery or assault with a weapon, the victimization and perpetration rates were far lower in the general population than the mental illness samples or cohorts.
A more informative comparison for this research question comes from the three studies that investigated persons with mental illness and those from the general population sampled and assessed in the same way (Sariaslan et al., 2020; Tsigebrhan et al., 2014; Walter et al., 2019). Notably, each of these studies also demonstrated high study quality assessment scores. Across these studies, victimization and perpetration rates were greater in the samples of individuals with mental illness than in the matched comparison groups. Both comparisons thus suggest that rates of both victimization and perpetration are consistently elevated in samples of individuals with mental illness compared to the general population. However, these results should be viewed as preliminary and interpreted with caution given that only three studies allowed for relative comparisons across both sample/cohort types.
Comparison With Previous Reviews
Integrating results from across the included studies, most evidence points toward (1) higher rates of victimization than perpetration, both among people diagnosed with mental illnesses as well as among individuals without such illnesses, and some preliminary evidence points toward (2) higher rates of both victimization and perpetration among individuals with mental illness compared to general population samples. This conclusion aligns with findings from previous reviews that have separately investigated victimization and perpetration rates. That is, past reviews have generally suggested that victimization and perpetration rates are higher among individuals with mental illness than among the general population (e.g., Latalova et al., 2014; Maniglio, 2009; Passos et al., 2013; but see Verdolini et al., 2018).
To our knowledge, only one previous review has assessed both violence victimization and perpetration. Choe et al. (2008) investigated distinct studies of violence victimization (n = 10) and perpetration (n = 31) and similarly concluded that victimization and perpetration rates were elevated among those with severe mental illness. In line with our findings, they also note that victimization rates were generally higher than perpetration rates. However, only three of the included studies in the systematic review by Choe et al. (2008) assessed victimization and perpetration among the same individuals. Additionally, 15 of the 25 studies included in the current systematic review were published after 2008. The current review thus adds additional and expanded evidence to these earlier findings.
Between-Study Heterogeneity
As anticipated, the included studies in the current systematic review varied in relation to several factors considered. In addition to varying observation periods and sample/cohort types, the data sources and definitions of victimization and perpetration rates differed substantially across studies. As previously mentioned, self-reported rates of violence victimization or perpetrated violence are likely to differ from rates of hospital-reported injuries or police-reported crimes or convictions. Studies using self-report methods generally found higher rates of victimization and perpetration than did studies using routinely collected administrative databases. However, both methods have strengths and limitations. Official data are a more valid and reliable data source but are likely to underestimate the occurrence of violence since only more serious of violence will be captured, including episodes resulting in hospitalization and/or in filed police reports. Self-reported data may include less severe violence and crimes that have not been reported, but this approach also introduces biases due to recall and the impact of social desirability on reporting. In particular, perpetration rates may be underreported, especially acts perceived as potentially criminally reportable. Thus, both methods have major limitations as well as strengths, and therefore observed differences between rates generated from self-reported information versus official databases should be carefully considered in any study comparison.
Definitions of violence victimization and perpetration also varied widely across the included studies. For example, some studies included more minor acts of violence (e.g., pushing), others included only more serious forms of violence (e.g., use of a weapon, violent crime such as rape, robbery, or assault), and others did not specify or define the type or severity of violence under investigation. Unsurprisingly, the different definitions of violence appeared to affect the reported rates. For example, Hiday et al. (2001) reported perpetration rates for both more minor and serious violence separately. The self-reported minor violence perpetration rate was 50.4%, whereas the more serious definition (requiring injury or weapon) considerably reduced this rate to 19.9%. Therefore, considering the type and severity of violent acts is vital when assessing victimization and perpetration rates more generally across these studies.
Strengths and Limitations of this Systematic Review
The current review fills a gap in the existing literature by reviewing studies that have assessed rates of both violence victimization and perpetration within the same study cohort or sample, and additionally reviewed studies that specifically determined these rates for those diagnosed with mental illness and those reporting rates for the two outcomes in the general population. Our narrative synthesis included an assessment of two primary research questions to evaluate (1) comparisons of rates of victimization and perpetration within each study type and (2) comparisons of such rates between study types. We also identified and appraised a small set of studies that reported victimization and perpetration rates among individuals with mental illnesses as well as a matched general population group, providing further insight into the comparison of rates between these groups. Future studies on victimization and perpetration risks should aim to investigate persons with and without mental illness to enable this more informative comparison to be made.
The main limitation of this systematic review was that we were unable to conduct a statistical meta-analysis due to the marked heterogeneity in study populations and settings, definitions and classifications, data sources, samples and cohorts, study designs and analytical approaches. This heterogeneity limits absolute comparisons of outcome rates, which are highly varied given the discussed differences in methodology, and our review thus focuses mainly on relative comparisons. Although our examination of the three studies examining both persons with mental illness and the general population is best suited to address both research questions, these findings should be viewed as preliminary given the limited number of studies. Additional future work examining both outcomes in the same study sample or cohort is needed to enable more robust conclusions to be drawn. Additionally, though we collated reports of victim-offender overlap and risk profiles for the outcomes, few of the included studies reported on these variables (see Table C in Supplemental Materials) and thus a review of these elements could not be included. A better understanding of the separate or shared risk and protective factors for victimization and perpetration, as well as the overlap between the two outcomes, is important for both theoretical and applied advances in this topic area (e.g., see Jennings et al., 2012; Sampson & Lauritsen, 1994; Silver et al., 2011). Finally, important cultural differences may have influenced study findings in relation to rates of victimization and perpetration. Additionally, although we found and included studies from all continents, the majority of included studies were from North America and Europe. Future studies should aim to increase diversity in this topic area—for example by conducting studies in non-Western countries—to increase the generalizability of these findings. Datasets from a wider variety of countries would also allow for better comparison between nations. However, future comparative work will need to closely consider the effects of national and cultural influences on rates of violence victimization and perpetration and the sources of such data (e.g., Harrendorf, 2018; van Dijk et al., 2021), as well as international differences in the identification, diagnosis, and treatment of mental illness (e.g., Gopalkrishnan, 2018; Krendl & Pescosolido, 2020).
Implications
This work has important implications for research, practice, and policy (Table 5). The finding that victimization is likely of even greater concern than perpetration for people with mental illness is often overlooked when research focuses solely on associations between mental illness and violence perpetration. This conclusion is important to highlight given the ongoing societal stigma that exists around the perceived relationship between severe mental illness and violence (e.g., Pescosolido et al., 2019). Furthermore, recent work suggests that stigma is associated with increased risk of victimization among people with mental illness (Harris et al., 2022). As such, efforts to reduce stigma are essential to help end this cycle of victimization.
In addition to reducing stigma, more resources should be allocated to prevent both violence victimization and perpetration among people who experience mental illness. Thus far, very little research has focused on how best to reduce the risk of victimization among those with severe mental illness, although studies examining interventions that aim to reduce victimization and its associated negative effects have begun to emerge (e.g., Albers et al., 2021). Importantly, future evaluations of interventions for those with mental illness should include victimization as an outcome variable, just as perpetration risk is commonly considered (Fazel & Sariaslan, 2021). As for violence perpetration prevention, other recent research suggests that some treatments are effective at reducing risk of criminal offending (e.g., clozapine and other mental health treatment for patients with psychotic disorders; Bhavsar et al., 2020; Weatherburn et al., 2021). In addition to benefiting society as a whole, preventing violence perpetrated by individuals with mental illness would significantly reduce overall government costs. One recent analysis suggested that the annual economic impact of violence perpetrated by people with severe mental illness in England and Wales was £2.5 billion, which included costs to victims (i.e., physical and emotional harm, lost productivity, etc.), police and criminal justice systems, health services, and forensic mental services (Senior et al., 2020). As such, a greater level of proactive investment in the treatment of mental illness and alcohol/drug misuse could assist with reducing offending and related spending. Findings from this systematic review highlight the importance of allocating further resources to prevent future or repeated violence victimization and perpetration for individuals with mental illness.
There are additional implications for future research. Specifically, these findings highlight the importance of assessing both victimization and perpetration when investigating violence, especially in cohorts and samples of people diagnosed with mental illnesses. Furthermore, choice of data source is critically important, as official records and self-report data alone may not yield accurate information on frequencies of violence victimization and perpetration. Therefore, research based only on one source of information about episodes of violence could thereby misinform policy decisions.
Conclusion
Previous reviews suggest that the risk of violence victimization and perpetration are both elevated in individuals with mental illness (e.g., Latalova et al., 2014; Maniglio, 2009; Passos et al., 2013; Whiting et al., 2021). However, consolidated knowledge regarding the relative risk of victimization and perpetration is lacking. This systematic review provided further evidence of the elevated risk of victimization and perpetration by comparing studies that assess both victimization and perpetration rates within the same sample or cohort. We found that people diagnosed with mental illnesses and individuals in the general population are generally found to have higher rates of victimization than perpetration. We also found some preliminary evidence that, compared with persons in the general population, individuals diagnosed with mental illnesses experienced higher rates of both victimization and perpetration. Greater resource allocation is needed to address both violence victimization and perpetration outcomes for people with mental illness.
Supplemental Material
sj-docx-1-tva-10.1177_15248380221145732 – Supplemental material for A Systematic Review of Interpersonal Violence Perpetration and Victimization Risk Examined Within Single Study Cohorts, Including in Relation to Mental Illness
Supplemental material, sj-docx-1-tva-10.1177_15248380221145732 for A Systematic Review of Interpersonal Violence Perpetration and Victimization Risk Examined Within Single Study Cohorts, Including in Relation to Mental Illness by Carey Marr, Roger T. Webb, Natalia Yee and Kimberlie Dean in Trauma, Violence, & Abuse
Footnotes
CRediT Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project is funded by an NHMRC Emerging Leadership Investigator Grant (GNT1175408) awarded to Professor Kimberlie Dean.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.