
Abstract
Providing efficient psychosocial support for survivors of sexual assault is of critical societal importance. Around the globe, technology-based solutions (eHealth) are increasingly being used to accomplish this task, especially following COVID-19. Despite increased importance and reliance on eHealth for sexual assault, minimal efforts have been made to systematically synthesize research in this area. The present study therefore sought to synthesize what is known about eHealth targeting sexual assault survivors’ psychosocial needs using a systematic scoping review methodology. To this end, five databases (CINAHL, Embase, PsycINFO, MEDLINE, and Scopus) were systematically searched for studies published from 2010 onwards using terms such as “sexual assault”, “eHealth”, “digital health”, “telehealth”, and variations thereof. Of the 6,491 records screened for eligibility, 85 studies were included in the review. We included empirical studies from all countries pertaining to eHealth for sexual assault for survivors 13 years or older. Many innovative eHealth applications for sexual assault exist today, and the included studies suggested that survivors generally experience eHealth positively and seem to benefit from it. Nevertheless, much more clinical and empirical work is needed to ensure accessible and effective solutions for all.
Advances in technology has greatly impacted most domains of human interaction, including those related to sexual violence. Although the emergence of the internet has provided more opportunities for both virtual and face-to-face sexual harm (e.g., non-consensual sharing of sexual material (Patel & Roesch, 2020)), it has also created new opportunities for sexual assault prevention and intervention (Bakker et al., 2020). As an example, informal online communities (e.g., Facebook, Twitter) are increasingly being used to disclose sexual assault and conduct anti-rape activism (Gorissen et al., 2021). Digital solutions are also increasingly provided within formal interventions for sexual assault, especially in response to survivors’ psychosocial needs (Walby et al., 2015). On a basic level, this may involve posting information on various websites (e.g., lists of sexual assault resources), as well as utilizing more advanced technologies to treat the negative outcomes related to sexual assault (e.g., therapeutic apps, video therapy). The present review focuses on digital intervention services for survivors of sexual assault.
The provision of health-related services using the internet and other communication technologies has been termed “eHealth” (Oh et al., 2005; WHO, 2019). eHealth as a concept emerged in the early 2000s and has since become widely used in healthcare and health research (Boogerd et al., 2015). eHealth has received much scientific interest since its implementation, and numerous definitions of the term have been proposed. Indeed, 51 unique definitions had already been identified in 2005 in a review by Oh et al. Although eHealth still lacks a comprehensive definition (Boogerd et al., 2015; O’Connor & Heavin, 2019), two terms are used in virtually all definitions of eHealth: Health and technology (Oh et al., 2005).
Research from various fields has established both advantages and disadvantages of eHealth (Scheibner et al., 2021). General advantages of eHealth may include improved healthcare through increased service-access (e.g., elimination of physical barriers, availability of smart phones); better coordination between services; better service monitoring; increased patient-empowerment; confidentiality; and reduction of waiting times and treatment costs (e.g., by simplifying administrative tasks) (Scheibner et al., 2021). Disadvantages of eHealth may involve development and implementation difficulties; technical challenges; reduced access for some (e.g., lack of internet access); concerns about confidentiality (e.g., data protection); and lack of regulation and evaluation of interventions (Scheibner et al., 2021).
Although no study to date has examined eHealth for sexual assault survivors, several reviews have been conducted on eHealth for intimate partner violence (IPV) (Anderson, Krause et al., 2021; El Morr & Layal, 2020; Linde et al., 2020), and violence against women (VAW) (Eisenhut et al., 2020). Anderson, Krause et al. (2021) reviewed studies on mHealth (mobile health) for the prevention of IPV and found it to be a potentially effective means of educating the community about IPV; however, there was limited evidence around whether eHealth interventions were superior to conventional interventions. El Morrr and Layal (2020) reviewed ICT (information and communication technologies) for the prevention, screening, and disclosure of IPV and found it to be a potentially effective approach for creating awareness and screening for IPV. Linde et al. (2020) reviewed studies comparing various eHealth interventions to various standard care for IPV survivors and found no evidence that eHealth interventions reduced IPV survivors’ rates of IPV, depression, and posttraumatic stress disorder (PTSD) compared to no eHealth intervention. Finally, Eisenhut et al. (2020) reviewed the existence of actual apps (not studies) for VAW more generally and concluded that apps may be a promising tool addressing VAW when used effectively and integrated appropriately into existing strategies. While these reviews found high heterogeneity in the types of eHealth interventions and mixed results in terms of efficacy of eHealth for trauma survivors more generally, none of these studies focused on sexual assault eHealth interventions in particular. Given the highly stigmatized nature of sexual violence, eHealth services may play a particularly unique role for survivors of sexual violence perpetrated by a stranger, acquaintance, or intimate partner. The current study thus seeks to expand upon existing reviews of eHealth for IPV survivors by examining eHealth for sexual assault survivors as a distinct intervention modality.
eHealth sexual assault services may be particularly important for younger survivors. Young people (the demographic at highest risk for sexual assault) are frequently described as a “digital generation” (Buckingham, 2006). This generation is perceived to be highly familiar with digital technology, which also influences how people seek information and utilize supports (Schrag et al., 2021). For example, one study of 1,408 adolescent girls found that the internet is the most common source of information for sexual health and sexual assault (Black et al., 2018). Gaining a better understanding of how technology is used to aid survivors of sexual assault is of urgent importance. COVID-19 has further underlined the need for flexible and innovative approaches to service provision. While rates of domestic and sexual violence generally increased during the pandemic, COVID-19 simultaneously restricted the availability of traditional face-to-face services. As a result, global dependence and demand for technology-based violence-related services increased dramatically (Emezue, 2020; Viero et al., 2021).
To our knowledge, no previous review has systematically explored the utility of eHealth for sexual assault. It is thus unclear if the proposed advantages and disadvantages of eHealth also apply to sexual assault. It is also unclear what kinds of eHealth interventions are provided for sexual assault survivors and if eHealth interventions targeting survivors’ psychosocial needs are valued and effective.
Purpose of the Present Study
The present scoping review aims to fill the above-mentioned literature gap by investigating how eHealth is currently used to support adolescent and adult survivors across the globe as they recover from sexual assault. In particular, the review will explore what is known about eHealth interventions targeting survivors’ post-assault psychosocial needs. As the present review is the first to provide an overview of eHealth utilization following sexual assault, we applied WHO’s broad definitions of both sexual assault and eHealth (WHO, 2017, 2019) (for details on the definitions see inclusion criteria). The present review will thus provide initial valuable insights into the potentially unique advantages and disadvantages to a broad range of eHealth modalities, including websites, video therapy, intervention videos, mobile apps, virtual reality, chat- and text-messaging services, podcasts, and other formats. This information can be used to guide organizations seeking to develop/implement eHealth, as well as identify areas for future research.
Methods
Identifying the Research Question and Relevant Studies
Due to the heterogeneity of the surveyed literature, a scoping review methodology was chosen for this review. An early step in the research involved developing a review protocol to guide the research and secure consensus among authors. The protocol was developed based on key literature on scoping reviews (Levac et al., 2010; Peters et al., 2020), and the PRISMA-P (Shamseer et al., 2015) was used to structure the protocol. A short version of the review protocol is available at Open Science Framework Registry at www.osf.io/3wreu (Bach et al., 2021). PRISMA-ScR (Tricco et al., 2018) was used to ensure adequate reporting in the present manuscript.
The present review seeks to answer the following research question: What is known about eHealth interventions targeting sexual assault survivors’ psychosocial needs? The following sub-questions were also posed: (a) What kinds of eHealth interventions are provided to sexual assault survivors today, and which psychosocial needs do they target? (b) How much are eHealth interventions used and what factors influence user-engagement? (c) How is eHealth experienced by survivors and what factors influence user experience? (d) Does eHealth improve psychosocial outcomes for survivors?
The systematic search was conducted in CINAHL, Embase, MEDLINE, PsycINFO, and Scopus in November 2021. The databases were selected because they provide good coverage of the topic of study and perform well in terms of precision, recall, and reproducibility (Bramer et al., 2017; Gusenbauer & Haddaway, 2020). Search terms (text words and index terms) were identified from thesauruses and publications on the topic (e.g., noting search terms in reviews about eHealth and noting titles and key words in potentially eligible studies). Since numerous terms are used for what we have termed “eHealth”, it was necessary to search for as many alternative terms as possible (e.g., “electronic health”, “telehealth”, “videoconferencing”). The final search string therefore contained approximately 50 terms relating to the term “eHealth”. Searches across databases were restricted to 2010 until current to ensure current relevancy. Since the search generated a large amount of hits it was necessary to restrict the search in Scopus (the largest of the databases searched). A third facet/block was therefore added to the Scopus search. Specifically, terms such as “eHealth”, “web,” or “online” had to appear close to terms such as “application”, “tool,” or “based.” No additional limits were used in the database searches. The complete search strategy is available in Supplementary Material A (using PsycINFO as an example). Several steps were taken to evaluate the quality of the search and selection strategy (e.g., consulting librarian specialists at the University of Southern Denmark and Cochrane Denmark; ensuring that all relevant publications known to us at this time appeared in the search; noting the number of disagreements in the first 100 records screened (n = 1)).
Eligibility Criteria
Inclusion criteria
We included studies about eHealth utilization following sexual assault. Sexual assault was broadly defined as “any sexual act, attempt to obtain a sexual act, or other act directed against a person’s sexuality using coercion, by any person regardless of their relationship to the victim, in any setting” (WHO, 2017, definition section). eHealth was broadly defined as the use of information and communication technology in support of health (WHO, 2019). Psychosocial impacts covered the mental health disorders commonly associated with sexual assault (e.g., depression, PTSD), as well as substance abuse and relational and sexual problems. Study participants in eligible studies were sexual assault survivors of all genders aged 13 or older, or sexual assault service providers/experts, if focused on survivors’ use of eHealth. Eligible studies did not have to include participants directly but could also describe the intervention itself (e.g., the contents and functions of a particular eHealth application). Non-survivor samples were only accepted if used as a separate comparison group. We included all types of empirical studies published in all languages in peer-reviewed journals and grey literature (e.g., reports, dissertations) from all countries.
Exclusion criteria
We excluded eHealth interventions for survivors under 13 years of age (if exceeding 10% of the sample) and interventions for IPV, unless focused on sexual IPV or equally focused on sexual assault and IPV (as seen at dual-focus services). Since the review is focused on survivors as consumers of eHealth, we also excluded service providers’ routine use of electronic systems (e.g., to access electronic patient data, screen patients, receive training). For this review, traditional telephone hotlines were not considered eHealth. Survivors’ use of informal online communities (e.g., Facebook and other social media) was also not considered eHealth, but organized support based on such platforms using either licensed professionals or volunteers was.
eHealth interventions not targeting survivors’ psychosocial needs were excluded. This included those limited to medical and criminal justice services (e.g., tele-assisted forensic medical examinations, systems to inform survivors about offenders such as VINE). Since primary prevention initiatives are not aimed at sexually assaulted individuals and their post-assault needs, they were also excluded. This included anti-rape technologies because they focus on how to avoid sexual assault (e.g., apps that automatically share users’ GPS location).
Study Selection
Figure 1 provides an overview of the selection of studies. In total, 10,979 records were retrieved from the database searches and exported to Endnote. 1 After duplicate removal, 6,491 records remained for screening. Title-Abstract screening was conducted in Covidence 2 by the first and fifth authors. Disagreements (n = 186) were discussed and resolved by the same authors, and 178 studies remained for full-text screening. Nine disagreements were resolved following full-text screening, and 81 studies were included in the review. Finally, four additional studies were retrieved by screening the reference lists of included studies.
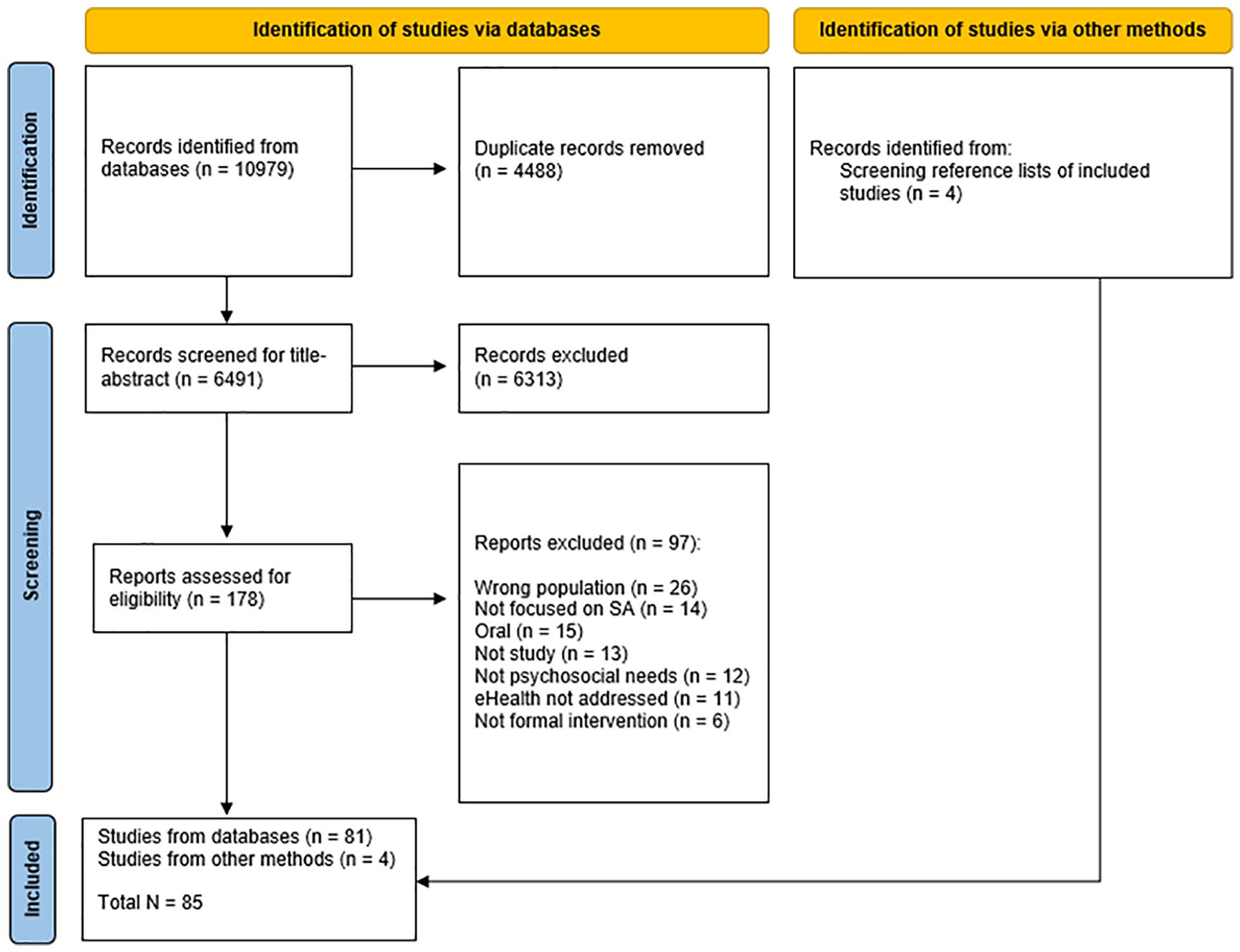
Preferred reporting items for systematic review and meta-analysis flow chart.
Extracting the Data and Reporting the Results
The extraction form was specially made for the present review. The following data was extracted by the first author and verified by the fifth author: Citation, Country, Population, Methods, and eHealth Intervention. Additional data about interventions, user-experience, user engagement, and effectiveness were extracted by the first author upon availability. An overview of included studies is available in Supplemental Material B. 3 A narrative synthesis of the included studies is presented in the Results section.
Results
Characteristics of Included Studies
Of the 85 studies included in the review, 78 were published in journals, five were dissertations, and two were book chapters. Most studies were conducted in North America (n = 73), followed by Europe (n = 7), and five were conducted elsewhere. All studies except two were published in English (i.e., German). Most studies were published in 2015 or thereafter (n = 70). The largest proportion of studies were quantitative (n = 46), 21 were mixed, and 18 were qualitative. Sample sizes ranged from zero to 4,703 (but N was not always provided). A total of 48 studies included survivors, 17 included service providers, and 26 studies examined aspects of an intervention without use of human samples (e.g., analyzed the content on university sexual assault pages, outlined the functions of a novel mobile app for survivors). 4 Of the studies containing survivors (n = 48), 10 included male or trans survivors (but participant gender was not always provided). Most samples consisted of survivors on the younger end of the age spectrum (e.g., 15–25), but some studies also contained older survivors (60+). Most studies did not disclose participants’ ethnicity/race.
Characteristics of eHealth
The present section will address the first research question: What kinds of eHealth interventions are provided to sexual assault survivors, and which psychosocial needs do they target? The included studies examined many forms of eHealth for sexual assault survivors including websites, video therapy, intervention videos, mobile apps, virtual reality, chat- and text-messaging services, podcasts, and virtual yoga and meditation. The largest proportion of studies focused on websites/platforms for survivors (n = 36), and the content and functions of these varied. To illustrate, one platform helped adult survivors of child sexual assault (CSA) prepare for pregnancy, birth, and parenthood (Montgomery et al., 2021), while another provided a space for survivors to share their sexual assault experience online and motivate others to seek help (Riggs, 2021). Some of the studied webpages were mainly informational (e.g., a list of sexual assault services), while others contained more interactive features (e.g., videos). Some of these studies (n = 4) also focused on organizations’ formal social media presence (e.g., Facebook), and service providers generally viewed social media as an important platform to facilitate outreach and provide formal support to survivors (Schrag et al., 2021; Storer et al., 2021; Webber, 2014). A total of 17 studies focused on video-based therapy for survivors. Video therapy generally consisted of individual therapy sessions based on various treatment orientations (e.g., Prolonged Exposure Therapy, Cognitive Behavioral Therapy) (e.g., Banducci, 2021). The transition/provision of video therapy often stemmed from COVID-19 restrictions (Azzopardi et al., 2021; Barbara et al., 2020; Sitz et al., 2021; Tener et al., 2021; Wood et al., 2020). The characteristics of eHealth Interventions are presented in Table 1.
Characteristics of eHealth Interventions.
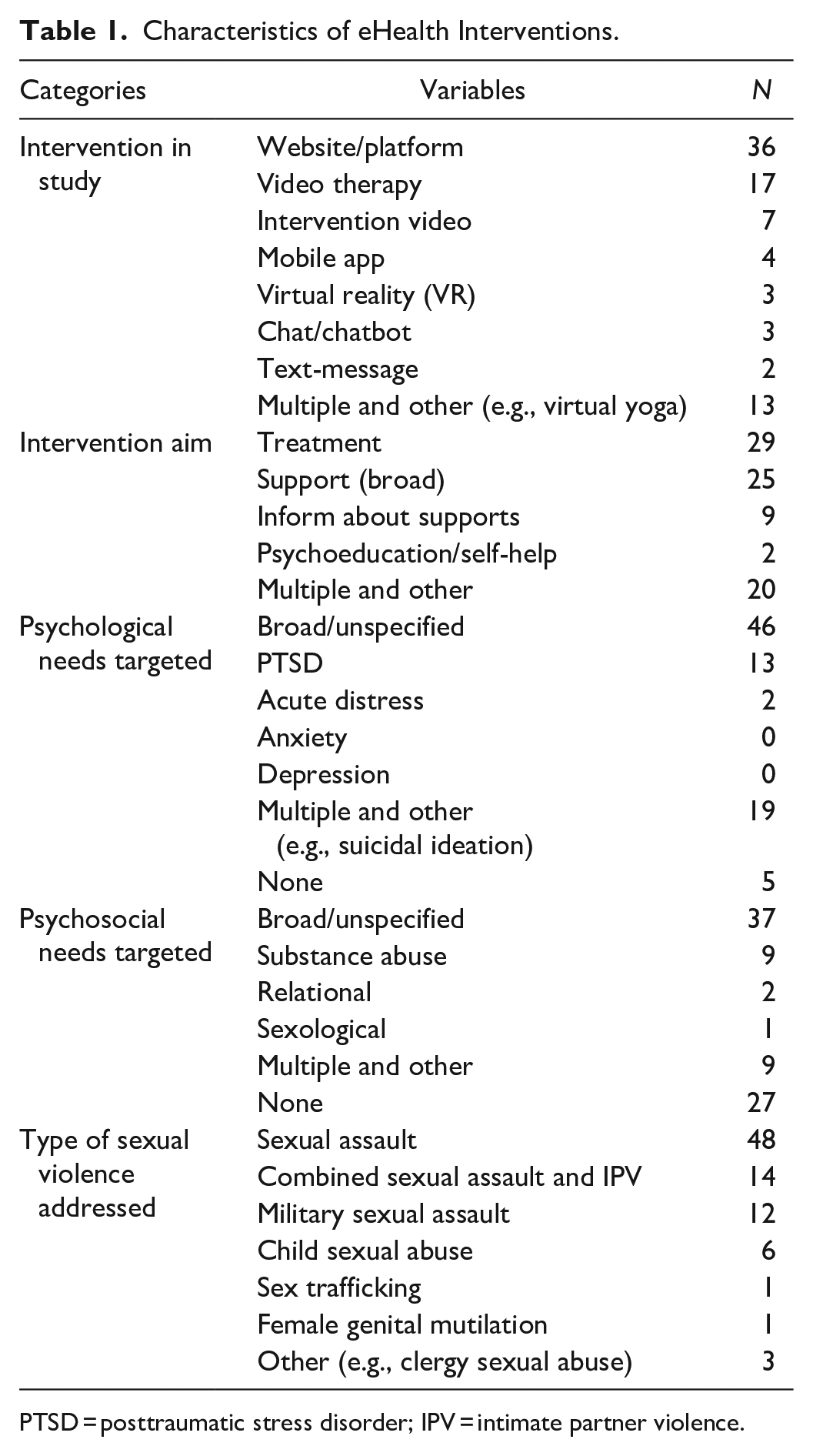
PTSD = posttraumatic stress disorder; IPV = intimate partner violence.
Examples of less studied interventions include brief intervention videos provided to survivors in acute settings, which typically focused on reducing/preventing substance use/abuse using breathing exercises or psychoeducation (e.g., Resnick et al., 2012). Bi-directional text-messaging interventions were also used in some acute settings to follow up on patients who received a forensic medical examination (Downing et al., 2021; Hicks et al., 2017). Virtual reality (VR) interventions were available in some locations and tended to focus on military sexual trauma (MST). VR interventions are generally based on the principles of exposure therapy and allow survivors to “face their fears” in a safe environment by taking participants through various hyper-realistic assault scenarios (e.g., a bar, a dark alley, or a sexual assault) (e.g., Loranger & Bouchard, 2017). Mobile apps were also identified in the review. In a Korean app named “Sister, I will tell you,” survivors are guided through various self-help modules by a female avatar (Lee & Cha, 2021).
Many of the identified eHealth solutions had a treatment component (n = 39), but the specific aim of the intervention was often unspecified or very broad (e.g., well-being). Among studies that did provide an explicit psychological aim, most focused on PTSD alone (n = 13) or in combination with other conditions (e.g., depression, anxiety) (n = 15). Among interventions with an explicit psychosocial aim, most focused on substance abuse (n = 9).
The included interventions addressed multiple forms of sexual violence, including sexual assault, combined sexual assault and IPV, CSA, MST, sex trafficking, and female genital mutilation (FGM). Most studies/interventions in the review focused on sexual assault (n = 48) alone or in combination with IPV (n = 14).
Survivors’ Utilization of eHealth
User-engagement
The present section will address the second research question: How much are eHealth interventions being used by sexual assault survivors and what factors influence user-engagement? In a study investigating sexual assault survivors’ needs, both survivors and providers (N = 33) requested increased access to eHealth (Munro-Kramer et al., 2017), and most survivors appear to accept eHealth, if offered (Downing et al., 2021; Hicks et al., 2017). For example, 64% of participating survivors (76 of 118) consented to a novel text-messaging intervention (iCare) (Hicks et al., 2017). Although few studies examined how frequently existing solutions are being used, there appears to be a sizeable demand for digital information (Moylan et al., 2021; Munro-Kramer et al., 2017; Zimmer, 2011). To illustrate, a website for sexual assault received 5,211 visits during the first 2 days of operation (Zimmer, 2011).
Retaining clients in online treatment appears more difficult. When reported, treatment completion rates were relatively low, even when clients were able to choose treatment modality (approximately 50% in several studies) (Acierno et al., 2021; Gilmore et al., 2020; Johnson, 2020; Lange & Ruwaard, 2010; Lee & Cha, 2021; Littleton et al., 2016; Loucks et al., 2019; Valentine et al., 2020). In a study of 171 participants, MST survivors who selected video therapy were significantly more likely to drop out of treatment than those receiving in-person treatment (50% vs 32%) (Valentine et al., 2020).
Factors that influence user-engagement
Situational factors may impact user-engagement. During the pandemic, many in-person services became unavailable, and services across the globe transitioned to eHealth. Service utilization rates following COVID-19 were investigated in five studies. Despite the transition to eHealth, caseloads significantly increased at service centers in Canada (Azzopardi et al., 2021) and the United States (Bennett et al., 2021; Wood et al., 2020). Interestingly, eHealth utilization during COVID-19 decreased at a service in Italy (Barbara et al., 2020) and at 46 services in Pennsylvania, United States (Wright et al., 2021). It was hypothesized in both studies that decreased eHealth utilization stemmed from a lack of privacy in the home and inadequate technology access.
Indeed, several studies emphasized that not all survivors have the technological equipment needed to receive eHealth (e.g., smart phones, internet connection) (Azzopardi et al., 2021; Banducci, 2021; Hicks et al., 2017; Kalmakis & Banning, 2012; Peuchaud, 2014; Wood et al., 2020). To illustrate, a large proportion of those who declined eHealth in one study (14 of 42), indicated that they did not have a cell phone (Hicks et al., 2017). Some survivors may therefore need to borrow equipment at services but this is not always an option (Azzopardi et al., 2021; Banducci, 2021; Wood et al., 2020). Furthermore, some applications charge a fee (Ellis & Fiondella, 2018).
Technical problems also impede service utilization (Banducci, 2021; Finn et al., 2011; Hicks et al., 2017). To illustrate, 29 of 76 participants in one study never received the intervention due to unforeseen technical problems (because intervention text-messages were blocked by phone providers) (Hicks et al., 2017). Similarly, technical problems delayed and complicated treatment in a case involving a male survivor in his mid-60s who converted to video therapy during COVID (Banducci, 2021). Technical problems appear widespread (Banducci, 2021; Finn et al., 2011; Hicks et al., 2017; Littleton et al., 2012). For example, technical problems such as freezing or being logged off occurred in 27% of all online sessions at one agency (N = 731) (Finn et al., 2011).
If interventions are difficult to navigate or comprehend, they are also less likely to be successfully utilized. A study of 193 U.S. agency websites found that most websites are built for “educated users”, making them inaccessible to survivors with limited literacy skills. In particular, 96.4% of websites were found to be “fairly difficult” to “very confusing” to read, and 81.4% of websites required 9 or more years of schooling to read. In addition, only 3% offered a changeable display for people with disabilities (e.g., changeable fonts or font size) (Sorenson et al., 2014). Results in other studies about the comprehensibility of interventions were mixed. Although seldomly reported, it also appears that most interventions were only provided in one language, thereby precluding language minorities from accessing them. According to a nationally representative study of U.S. agency websites, websites are generally built for English-speakers (Sorenson et al., 2014).
The inclusiveness of eHealth services for male and LGBTQ survivors were also questioned in several studies (Anderson, Pollitt et al., 2021; Du Mont et al., 2021; Simmons & Clay, 2019; Sorenson et al., 2014). To illustrate, of the 261 agency websites surveyed, 100% served women, 15% mentioned male survivors, and 8% mentioned gender and sexual minorities (Sorenson et al., 2014). One of the highest prioritized tasks for a newly established network to support trans survivors was therefore to develop an online resource list of trans-affirming organizations (Du Mont et al., 2021).
Finally, eHealth services are simply not always available. For example, not all sexual assault agencies have a webpage (Sorenson et al., 2014), and not all universities provide information about sexual assault on their website (Englander et al., 2016; Graham et al., 2017; Griffin et al., 2017; Krivoshey et al., 2013; Lund & Thomas, 2015; Schwartz et al., 2015; Simmons & Clay, 2019). Using the most recent of these studies as an example, 12.9% of universities (N = 465) did not provide any information pertaining to sexual assault on their website (Simmons & Clay, 2019). Checklists to assess gaps in sexual assault information on university websites have therefore been developed (Corcoran et al., 2020).
Intervention feasibility
While some eHealth interventions are relatively inexpensive and easy to implement (e.g., intervention videos in acute settings) (Miller et al., 2015; Walsh et al., 2021), developing, operating, and revising other kinds of interventions can be time-consuming and costly (Hicks et al., 2017; Villegas-Gold, 2018; Wood et al., 2021; Wright et al., 2021). Villegas-Gold (2018) estimated the costs of developing a fully-functioning, mobile-friendly website at a minimum of USD 10,000. In a similar vein, video and chat services may require increased staffing, in part because these services are typically not restricted to users from a specific geographical location (Hicks et al., 2017; Webber & Moors, 2015). Finally, a high degree of technico-legal expertise is generally required to safely implement eHealth, and providers in some studies thus worried about user-rights and confidentiality (Schrag et al., 2021; Sitz et al., 2021; Wood et al., 2021).
Survivors’ Experience of eHealth
Survivor-preferences
The present section will address the third research question: How is eHealth experienced by sexual assault survivors and what factors influence user experience? Studies examining survivors’ preferences indicate that most survivors are positive about eHealth and that some survivors favor eHealth to traditional face-to-face services (Carretta, 2011; Carretta et al., 2016; Munro-Kramer et al., 2017). Advantages to eHealth included an increased sense of privacy and anonymity (Moylan et al., 2021; O’Brien & Li, 2020; Steinmetz & Gray, 2017). To illustrate, most online services can be accessed without providing a face and a name. Text-based services furthermore enable survivors to reach out without being overheard by others. This can be vital for survivors living with others, especially for those residing with the abuser/trafficker, since these survivors are often under surveillance (Moylan et al., 2021; O’Brien & Li, 2020; Wright et al., 2021).
Online services also increase the availability and flexibility of services, since many services can be accessed at any time and place (Gilmore et al., 2016; Tener et al., 2021). Online services can therefore help overcome linguistic, cultural, and geographical barriers to service utilization (Bennett et al., 2021; Chien, 2013; Gray et al., 2015; Hassija & Gray, 2011; Peuchaud, 2014; Steinmetz & Gray, 2017; Weiss et al., 2018; Zheng & Gray, 2014). To illustrate, survivors in the Weiss et al. (2018) study (N = 10) each saved an average of 255 km travel per session by converting to video therapy. Similarly, video therapy enabled two Mandarin-speaking survivors living in rural United States to connect with Mandarin-speaking therapists who appreciated their Chinese heritage (Zheng & Gray, 2014). In addition, not all survivors feel comfortable in formal support settings. As emphasized by Gilmore et al. (2016), female veterans with MST may favor video therapy to face-to-face services, since veteran services are often male oriented/dominated. Correspondingly, participants in one study indicated that they preferred texting formal providers to talking (Downing et al., 2021).
Individual preferences were noted, however. Not all survivors are comfortable using technology for help-seeking (Hicks et al., 2017; Kalmakis & Banning, 2012; Kavemann, 2021; Sitz et al., 2021; Steinmetz & Gray, 2017; Tener et al., 2021; Wood et al., 2020). In a study of 37 survivors, 19% (n = 7) were uncomfortable using the internet for sexual assault information, almost half (n = 17) were unsure, and only 35% (n = 13) were comfortable (Kalmakis & Banning, 2012). Those uncomfortable using the internet often cited issues of confidentiality (Kalmakis & Banning, 2012). Furthermore, cultural values also influence individual preferences. A study of 23 Israeli-based service providers emphasized that ultra-Orthodox families in Israel generally do not use the internet (Tener et al., 2021).
Intervention satisfaction
The vast majority of studies investigating user-satisfaction suggest that most survivors are satisfied with the services received (Anderson, Pollitt et al., 2021; Bennett et al., 2021; Bomyea et al., 2015; Creech, Pulverman, Kahler, et al., 2021; Creech, Pulverman, Shin, et al., 2021; Downing et al., 2021; Finn et al., 2011; Gilmore, Davidson, et al., 2019; Gray et al., 2015; Gulati et al., 2021; Hassija & Gray, 2011; Johnson, 2020; Lange & Ruwaard, 2010; Lee & Cha, 2021; Littleton et al., 2012, 2016; Loucks et al., 2019; Montgomery et al., 2021; Norman et al., 2020; Stappenbeck et al., 2021; Steinmetz & Gray, 2017; Villegas-Gold, 2018; Weiss et al., 2018; Zheng & Gray, 2014).Participants perceived interventions to be beneficial because they helped them “heal,” made them feel supported, used minimal and survivor-centered language, and applied modern and intuitive designs. User-satisfaction was evaluated using qualitative interviews, specially designed surveys, and questionnaires (e.g., The Wyoming Telehealth Trauma Clinic Client Satisfaction Scale).
Although feedback from survivors was mostly positive, recommendations for services and areas for improvement were identified in some studies. Participants in these studies emphasized a need to avoid ambiguous content, impersonal language, blaming language, gender-specific pronouns, and delayed and incomplete responses. Participants also underscored the importance of using clear, inclusive, and caring language (Anderson, Pollitt et al., 2021; Gulati et al., 2021; Littleton et al., 2012; Montgomery et al., 2021; Schrag et al., 2021). Results relating to intervention design were mixed. While some users appreciated the use of interactive elements (e.g., videos) and colorful designs, others preferred a more neutral, simple design (Gilmore, Davidson, et al., 2019; Gulati et al., 2021).
Adverse effects
Since no adverse effects were explicitly reported in any of the included studies, eHealth interventions generally appear safe. Nevertheless, participants in one study stated that online therapy evoked traumatic memories of having their assault videotaped (Kavemann, 2021). If survivors reside with the abuser, receipt of eHealth may be unsafe, and providers must identify the safest method to contact the client (Wright et al., 2021).
Indirect influences on experience
Factors “external” to survivors may also influence survivors’ eHealth experience. During COVID-19 lockdowns, eHealth was often the only available support option. Survivors who preferred face-to-face treatment therefore rated video therapy as “better than nothing” (Kavemann, 2021). Factors relating to service delivery also appear relevant. For example, challenges in terms of establishing rapport, interpreting clients’ emotional state, and showing empathy over video/audio/chat were noted by some service providers (Moylan et al., 2021; Sitz et al., 2021). Many service providers also experienced increased stress and fatigue following online work due to insufficient technical support; inadequate equipment; lack of privacy when videoing from home; literately bringing the traumatic content of sessions into the home; having to acquire new skills (Azzopardi et al., 2021; Tener et al., 2021; Wood et al., 2020, 2021).
Effectiveness of eHealth
The present section will address the fourth and final research question: Do eHealth interventions improve psychosocial outcomes for sexual assault survivors? Although the studies cited in this section involved different populations, interventions (e.g., virtual therapy, video therapy), and psychosocial outcomes (e.g., PTSD, depression, substance abuse), most focused on eHealth interventions for PTSD for survivors of sexual assault or MST. The research methods used to evaluate effectiveness ranged from case studies to randomized controlled trials, but most studies involved pre- and post-intervention symptom measures.
Of the 29 studies that investigated if eHealth interventions reduce the negative impacts of sexual assault (and in particular PTSD), at least some positive impacts of eHealth were noted in all studies (Acierno et al., 2021; Banducci, 2021; Bomyea et al., 2015; Creech, Pulverman, Kahler, et al., 2021; Creech, Pulverman, Shin, et al., 2021; Gilmore et al., 2021; Gilmore, Walsh, et al., 2019; Gray et al., 2015; Hassija & Gray, 2011; Jaffe et al., 2021; Johnson, 2020; Lange & Ruwaard, 2010; Lee & Cha, 2021; Littleton & Grills, 2019; Littleton et al., 2012, 2016; Lopez et al., 2021; Loucks et al., 2019; Miller et al., 2015; Norman et al., 2020; Resnick et al., 2012; Sitz et al., 2021; Stappenbeck et al., 2021; Steinmetz & Gray, 2017; Walsh et al., 2017, 2020, 2021; Weiss et al., 2018; Zheng & Gray, 2014). To provide an example, 6–12 virtual reality exposure sessions led to significant reductions in PTSD and depression symptoms in 15 MST survivors (Loucks et al., 2019).
eHealth was, however, not always more effective than conventional treatment (Acierno et al., 2021; Creech, Pulverman, Kahler, et al., 2021; Gilmore et al., 2021; Lopez et al., 2021). To illustrate, in-person therapy and video therapy were equally effective for PTSD and depression in a randomized controlled trial of MST survivors (N = 136) (Acierno et al., 2021). Furthermore, many interventions were not effective on all measured outcomes (e.g., improvements were measured for PTSD but not substance abuse) (Creech, Pulverman, Kahler, et al., 2021; Johnson, 2020; Littleton et al., 2012; Miller et al., 2015; Norman et al., 2020; Resnick et al., 2012), and some interventions were only effective for specific subgroups of participants (Gilmore, Walsh, et al., 2019; Jaffe et al., 2021; Walsh et al., 2017, 2021). In a study of 154 recent survivors, for example, an intervention video to reduce prescription opioid abuse was only effective for survivors who had experienced more than one sexual assault (Gilmore, Walsh, et al., 2019).
Discussion
The present scoping review sought to identify what is known about eHealth interventions for sexual assault focusing on four research questions reflecting the following sub-topics: characteristics of eHealth; user-engagement; user-experience; and effectiveness. Through a systematic literature search of five databases, 85 eligible studies were identified and included in the review.
Characteristics of eHealth
Several conclusions can be drawn from this scoping review. First, since the vast majority of studies included in the review were published in 2015 or thereafter (especially in 2021), interest and implementation of eHealth for sexual assault appears to be on the rise. This increase is not surprising given continuous growths in technology use (International Telecommunication Union, 2021), as well as recent efforts to maintain services during COVID-19. It is also evident that a variety of innovative solutions exist today (e.g., video therapy, chat services, apps). Most interventions did not have a clear treatment aim, but when provided, PTSD was the most targeted psychological need, and substance abuse the most targeted psychosocial need. Although included technologies addressed multiple forms of sexual violence (e.g., sexual assault, MST), certain forms of sexual violence were barely addressed. FGM was, for example, only addressed in one intervention (Perez & Turetsky, 2015). As such, there is a need for more diverse eHealth interventions, including interventions for survivors of FGM.
Survivors’ Utilization of eHealth
It appears as if eHealth interventions for sexual assault are widely implemented and utilized today, but interpretating the evidence pertaining to user-engagement was sometimes difficult (e.g., how was the intervention advertised? How many visits should a sexual assault website receive per day?). However, keeping survivors engaged in treatment over time appears difficult given high dropout. The review also suggests that some survivors may be precluded from using eHealth (e.g., survivors with low literacy skills, disabilities, language minorities, and those affected by poverty). Although technology adaptation is on the rise, an American study shows that people with lower incomes are far less likely to own a smartphone or computer than people with higher incomes (Vogels, 2021). Financially vulnerable survivors may therefore need to borrow devices, but, according to included studies, doing so is not always possible (Azzopardi et al., 2021; Banducci, 2021; Wood et al., 2020). Constructing fully-equipped private “pods” in public buildings could potentially help to overcome this barrier.
Interventions should also be accessible to people with disabilities, but disability perspectives were rarely mentioned in included studies, and few interventions included disability features (e.g., changeable fonts or font size) (e.g., Sorenson et al., 2014). Similarly, the reading level required to read most agency websites in the United States is comparable to the reading level required to read Time or Newsweek (Sorenson et al., 2014). This is counter to guidelines proposed by the Bureau of Internet Accessibility (n.d.) who recommend that digital information must be communicated in simple and accessible language (e.g., use short sentences and provide illustrations). This is not only important for people with intellectual disabilities or low literacy skills (and the law), but also of general importance for sexual assault survivors who may be in a state of acute crisis.
Due to the traumatic nature of sexual violence, it is also important to use trauma-informed language (e.g., avoid blaming and “triggering” language). Interventions should also be provided in multiple languages, but most of the included interventions were monolingual (English). Finally, interventions must also reflect the diversity of those using them, which requires the use of inclusive language, as indicated by participants in the included studies (e.g., avoid gender-specific pronouns). Survivors least likely to receive eHealth largely overlap with those generally underserved by formal supports (e.g., financially vulnerable survivors, sexual and gender minority survivors, survivors with disabilities) (Bach et al., 2021), highlighting the need to develop further supports for underserved survivors. Guidelines for enhancing cultural competency and inclusiveness in eHealth interventions have been developed to enhance the effectiveness of eHealth interventions for racially, economically, and gender diverse populations (Nimmon et al., 2012; Yellowlees et al., 2008; Young, 2022). While some have argued that tailored services may not always be feasible as it would require both the development, implementation, and maintenance of potentially different tailored user interfaces (Hicks et al., 2017; Villegas-Gold, 2018; Wood et al., 2021; Wright et al., 2021), doing so should nonetheless remain a priority. Research on the effectiveness of eHealth services should also strive to include more diverse samples as much of the existing research on telehealth has been lacking in diversity (Weaver et al., 2021) and the differential impact of eHealth on diverse survivors is currently unknown.
Survivors’ Experience of eHealth
Most survivors described their eHealth experience in positive terms, and some survivors even preferred eHealth to conventional services. Advantages to eHealth included increased sense of privacy and anonymity; increased flexibility and availability of services (e.g., reduced linguistic, cultural, and geographical barriers to service utilization), and increased sense of safety and comfort (e.g., not necessary to leave the home to receive help). eHealth should therefore be considered an essential component of comprehensive and contemporary sexual assault service provision. Still, individual preferences and disadvantages to eHealth were also identified in the review including costs; safety issues (e.g., if the client resides with the abuser); confidentiality issues; technical issues; communication difficulties (e.g., more difficult to register emotional cues); and discomfort utilizing technology (applied to survivors and providers alike). Ideally, services should therefore be tailored to individual preferences and needs, and both clinical and ethical considerations are warranted (e.g., are clients in a safe space to receive eHealth?). eHealth is therefore best viewed as a tool to expand and individualize service provision and not as a replacement for in-person services.
Effectiveness of eHealth
There is reason to be optimistic about the efficacy of eHealth interventions for reducing the negative impacts of sexual assault (especially PTSD). Caution is still warranted, however. The evaluated interventions were often not effective on all outcomes and virtual treatment was not necessarily more effective than face-to-face treatment. These results are somewhat similar to the reviews of eHealth interventions for IPV and VAW. Although there was virtually no overlap in the studies included in the current review and previous reviews on eHealth for IPV and VAW (i.e. overlap of two studies in Anderson, Krause et al., 2021, one study in El Morr & Layal, 2020, zero studies in Eisenhut et al., 2020, and Linde et al., 2020), some general advantages and disadvantages did emerge across studies. Future research is thus needed to tease apart potential differences in eHealth interventions targeting sexual assault, IPV, and other forms of gender-based violence. Given the wide range of intervention aims, modes of delivery, study designs, and participant characteristics, conclusions about effectiveness only occurred at a general level. Furthermore, we did not systematically assess the quality of studies and risk of bias (since doing so is uncommon for scoping reviews (Levac et al., 2010; Tricco et al., 2018)). Taken together, the present review can only provide initial evidence concerning the effectiveness of eHealth for sexual assault. Nevertheless, we believe the review provided a much-needed overview of the eHealth scene. Having established a general overview for the field, future systematic reviews could employ narrower research questions to explore specific aspects of effectiveness (e.g., if 5 to 10 sessions of telehealth-delivered cognitive behavioral therapy is effective for adult survivors of sexual assault with depression).
Limitations
The present review is not without limitations. Broad definitions of both the term “eHealth” and “sexual assault” were applied in the present review to get a first inclusive overview of the field; however, this also meant that analysis occurred at a more general level, making it difficult to draw more detailed conclusions. Furthermore, the vast majority of included studies were conducted in North America (and in particular the United States), the findings of the review may not be generalizable to survivors in other regions. Furthermore, there were no studies from Africa and South America, which may also reflect regional disparities in technology use and access (International Telecommunication Union, 2021). It is therefore also likely that eHealth is more accessible to survivors in some parts of the world compared to others. Although most of the included studies were quantitative in nature, sample sizes were generally small (under 50), which also limits the generalizability of the review. Furthermore, most samples only involved women, few studies included men, and almost no studies included or even mentioned gender and sexual minority survivors. The findings of the review may therefore only apply to survivors identifying as female. Future interventions and research should thus focus more on diversity.
Conclusions
To conclude, many innovate eHealth applications for sexual assault exist today, survivors generally describe their eHealth experience positively, and there is reason to be optimistic about the efficacy of eHealth for negative outcomes related to sexual assault. eHealth should therefore be considered an integral part of contemporary sexual assault service provision, and eHealth proved particularly essential during the pandemic. Still, survivors have individual needs and preferences, and there are also serious disadvantages to eHealth, including limited access for some, as well as unanswered questions regarding its effectiveness. eHealth should therefore not replace face-to-face treatment, and interventions should be continuously monitored and evaluated. Much more clinical and empirical work is therefore still needed to ensure accessible and effective eHealth for all.
Critical Findings
This is the first systematic scoping review pertaining to eHealth targeting the psychosocial needs of sexual assault survivors.
The present review finds that numerous innovative eHealth interventions exist today, and many survivors seem to value and benefit from them.
Disadvantages to eHealth for sexual assault include limited access for some, as well as unanswered questions regarding effectiveness. More work is therefore still needed to ensure inclusive and effective solutions for all.
Implications for Practice, Policy, and Research
Supplemental Material
sj-docx-1-tva-10.1177_15248380221143355 – Supplemental material for EHealth for Sexual Assault: A Systematic Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380221143355 for EHealth for Sexual Assault: A Systematic Scoping Review by Maria Hardeberg Bach, Courtney Ahrens, Miranda Olff, Cherie Armour, Sascha Strauss Krogh and Maj Hansen in Trauma, Violence, & Abuse
Supplemental Material
sj-xlsx-2-tva-10.1177_15248380221143355 – Supplemental material for EHealth for Sexual Assault: A Systematic Scoping Review
Supplemental material, sj-xlsx-2-tva-10.1177_15248380221143355 for EHealth for Sexual Assault: A Systematic Scoping Review by Maria Hardeberg Bach, Courtney Ahrens, Miranda Olff, Cherie Armour, Sascha Strauss Krogh and Maj Hansen in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The first and last author would like to thank TrygFonden for their financial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant to Maj Hansen from TrygFonden (ID: 152374).
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
![]() ).
).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.