
Abstract
Access to quality sexual assault (SA) care in rural communities is limited by challenges surrounding building and sustaining a skilled SA nurse examiner workforce. Telehealth can facilitate access to expert care while cultivating a local sexual assault response. The Sexual Assault Forensic Examination Telehealth (SAFE-T) Center aims to decrease disparities in SA care by providing expert, live, interactive mentoring, quality assurance, and evidence-based training via telehealth. This study examines multidisciplinary perceptions of pre-implementation barriers and SAFE-T program impact using qualitative methods. Implications for the implementation of telehealth programs to support access to quality SA care are considered.
Background
The trauma of sexual assault (SA) can have devastating effects on the physical and emotional health of survivors. Survivors may suffer from post-traumatic stress disorder (PTSD), stigmatization, depression, suicidal ideation, and are at increased risk for further victimization as well as chronic disease (Campbell, 2008; Campbell et al., 2006; Kennedy & Prock, 2018). The physical and emotional trauma experienced by SA survivors necessitates specialized, trauma-informed health care to achieve the best possible outcomes for survivors (Campbell et al., 2008; Fehler-Cabral et al., 2011). Sexual Assault Nurse Examiners (SANEs), registered nurses with specialty training in the delivery of SA care, are the ideal response to provide care for this population, demonstrating improvements in patient satisfaction, quality of evidence collection, and legal case trajectory (Campbell et al., 2014; Du Mont et al., 2014). Despite these benefits, SANEs are not uniformly available across all communities, especially in rural areas facing known challenges in the recruitment of specialists and delivery of specialty SA care (Thiede & Miyamoto, 2021).
The SANE is an integral member of a greater community response to sexual assault known as a multidisciplinary sexual assault response team (SART). These multidisciplinary, interagency teams promote collaboration with a goal of supporting victims of sexual assault and holding offenders accountable for their actions (National Sexual Violence Resource Center [NSVRC], 2018). SARTs are necessarily unique to their communities, but typically include law enforcement officials, prosecutors, advocates, SANES or medical-forensic examiners, and child and adult protection agencies (NSVRC, 2018).
The Sexual Assault Forensic Examination Telehealth (SAFE-T) program was created to solve disparities in SA access and care quality in rural and underserved communities by delivering a comprehensive hub of expertise that provides local program assessment and guidance, nurse training, 24/7 expert forensic SA nurse consultation via telehealth (teleSANE), and ongoing mentoring and continuing education. We aimed to create a model that is adaptable and effective in many different settings, therefore, continuous quality improvement is a central effort. Understanding how the model performs, whether it is acceptable to the multidisciplinary community response team (SART) members that engage with the program, and whether these stakeholders perceive the program as valuable is essential to determine both effectiveness and potential utility to other communities.
SANEs and SA Care
Central to SANE training is the integration of a trauma-informed approach to avoid secondary victimization, or the “second trauma” that can occur when individuals are shamed, blamed, or not believed by first responders (Campbell et al., 2005, 2009; Nugent-Borakove et al., 2006). SANE models are widely used to provide SA care to survivors given their specialized training, association with positive health and prosecutorial outcomes, and ability to leverage already available staff (registered nurses) on an as-needed basis (Campbell et al., 2014; Ciancone et al., 2000). The United States Department of Justice (DOJ) has endorsed the SANE model of delivering SA care (Littel, 2001).
Provision of care for survivors of SA is complex. Managing care that honors the needs and wishes of an individual who has just experienced a trauma requires navigation of emotionally difficult circumstances for survivors and their families. Importantly, survivors need to feel safe and supported, require guidance related to their rights, choice related to care and reporting, and assistance navigating personal safety and support needs. Comprehensive examinations can last more than five hours and typically include: obtaining a thorough patient history and history of the events, detailed physical examination, thorough written and photo-documentation, collection and preservation of evidence according to crime laboratory and/or state protocols, assessment and treatment of injury, assessment and treatment of mental health, provision of prophylactic medications for sexually transmitted infections (STIs) and pregnancy, and facilitating community referrals and interactions with SART members in the community (United States Department of Justice Office on Violence Against Women [OVW], 2018).
The diverse circumstances of those who have just experienced trauma mean that each case presentation may present unique challenges. Clinicians practicing in this specialty gain important experience and skills when they have participated in many cases (observing and being precepted by expert clinicians and participating in continued education and case review with peers) (Adams et al., 2012).
Rural Challenges in SA Care Delivery
Rural communities struggle to build and sustain SANE programs (United States Government Accountability Office [US GAO], 2016). Difficulty recruiting nurses to obtain specialty training, limited access to education, clinical training, and peer review, and limited resources for provision of comprehensive (24/7) coverage contribute to challenges in developing and sustaining SANE programs (Maier, 2011; US GAO, 2016). Additionally, low reimbursement rates create little financial incentive for rural hospitals to develop and sustain robust SANE programs (Logan et al., 2007; Maier, 2012).
Even when rural hospitals invest in sending nurses to SANE training, they often return to their community with core knowledge yet little to no opportunity for clinical precepting. As a result, a rural SANE may be the only provider in their community providing complex and emotionally taxing care (US GAO, 2016). These factors contribute to nurses abandoning the specialty (US GAO, 2016). Additionally, those practicing in rural communities have less opportunity to use and develop skills due to diminished patient volume in low population density settings. Together, these factors present substantial barriers to achievement of SA response expertise in rural communities even when SANEs are available.
The result of these challenges is that many communities have either an under-resourced SANE team (inexperienced or too few SANE examiners to cover a comprehensive response) or no SANE team at all. When SANEs are not available, many hospitals resort to untrained emergency department nurses/providers to deliver this care. When providers are not trained in trauma-informed forensic care, survivors are at risk of experiencing secondary victimization, which can deter survivors from seeking help or justice (Campbell et al., 2009). The community SART response, and the quality of healthcare provided to SA survivors following an assault is particularly critical for survivors’ physical and emotional well-being (Campbell et al., 2005). Ensuring that safe and timely access to care is available to all survivors in every community is also essential to individual well-being and healing from trauma. Moreover, the quality of forensic evidence collected during healthcare encounters is an important factor in whether SA cases progress through the criminal justice system (Campbell et al., 2014; Sommers & Baskin, 2011).
Telehealth Solves Access Issues and Improves Quality of Care
Creative solutions are needed to address issues that contribute to disparate care for rural and other vulnerable populations. Telehealth, defined by the Health Resources Services Administration (HRSA) as “the use of electronic information and telecommunications technologies to support long-distance clinical health care, patient and professional health-related education, public health and health administration” (HRSA, 2021) is an efficient and effective mode of remote provision of expert care and quality assurance (Ricci et al., 2003; Sterling et al., 2017). Telehealth has demonstrated utility in forensic SA care (Macleod et al., 2009; Miyamoto et al., 2014; Walsh et al., 2019). These telehealth forensic SA care models, which include live telehealth consultations and quality assurance as well as training and peer review, have shown promise in growing and supporting quality SANE care (Macleod et al., 2009; Miyamoto et al., 2014, Miyamoto, Thiede, et al. 2021; Walsh et al., 2019). However, none of the above studies explored stakeholder's perspectives on community SA response needs or perceptions of telehealth program value following implementation. Engaging SART members and other stakeholders (hospital administrators) in identifying their community needs and eliciting their perception of program value is vital knowledge to inform continuous quality improvement for the model, to provide evidence of program acceptability, and to demonstrate effectiveness to future community collaborators.
The Sexual Assault Forensic Examination Telehealth (SAFE-T) Program
SAFE-T is a comprehensive, community-engaged program that aims to improve access and quality of health care for SA survivors. SAFE-T works to improve the quality of health care received by survivors in rural/underserved areas by: (a) providing training and education to rural nurses providing SA care in emergency departments, (b) providing live expert SA nurse consultation via telehealth (teleSANEs), (c) providing program development guidance, and (d) engaging hospital, victim advocacy center, law enforcement, and prosecutor stakeholders to foster collaboration (Miyamoto, Thiede, et al., 2021).
Nurses in local partner communities (local nurses) receive foundational SAFE-T supported core SANE didactic training and 2-day skills training prior to conducting examinations. For SAFE-T sites, foundational training is followed by 24/7 access to live examination, expert telehealth consultation, and precepting delivered by teleSANEs (SANE-certified, highly experienced SA forensic examination experts), which is rarely available in rural and underserved communities (US GAO, 2016). TeleSANEs mentor, support, and empower local nurses during exams to provide trauma-informed, evidence-based SA care and evidence collection; this process cultivates local nurses’ skills to deliver quality SA care by providing distance hands-on training, peer review, and a supportive network of forensic nurses.
The SAFE-T program engages in the community beyond telehealth consultations to foster program success, longevity, encourage development of local infrastructure, and to nurture professional growth and investment among local SART members. This begins with broad identification of community stakeholders and invitation for those groups to participate in sessions to understand community needs and to learn about the SAFE-T model and how it may fit within existing community SA response efforts. Partner hospital administrators are members of the SAFE-T Advisory Board (SAB) where they participate in biannual meetings to identify and address needs and advance impact and long-term sustainability. SAFE-T facilitates meetings between local nurses, victim advocacy, law enforcement and prosecutors to encourage mutual understanding of multidisciplinary roles within the community and to discuss how they can work toward a coordinated community response to SA.
Implementing a comprehensive, community-based telehealth program is challenging and requires frequent evaluation, refinement, and adaptation (Chambers et al., 2013). The perspectives of key stakeholders can provide valuable insight into the need for services, implementation of programming, and subsequent effectiveness of programs. To elicit opportunities for improvement, we conducted in-depth stakeholder interviews to understand perceptions of local quality of SA response prior to SAFE-T implementation, and what impact the program had on accessibility of care and quality of care during the early implementation phase/launch and first year of the project.
SAFE-T's model requires customization to each community's needs with real-time adjustments. Therefore, “pre-” and “post-” examination of predetermined programmatic outcomes is not an appropriate design; rather, the evaluation must occur at various timepoints to allow for nonlinear optimization. The Dynamic Sustainability Framework (DSF) guides SAFE-T's evaluation process, allowing for continual refinement of the program's telehealth, mentorship, educational, and clinical components throughout planning and implementation (Chambers et al., 2013; Miyamoto, Thiede, et al., 2021). Consistent with the DSF framework, we aimed to understand how stakeholders perceived the early impact of the SAFE-T Program on three rural communities following implementation.
This study's purpose was to examine the perceived impact of the SAFE-T program on communities’ SA response, particularly as it relates to its impact on SA healthcare quality. This study examines nursing, hospital administration, victim advocate, and law enforcement stakeholder perspectives on the need for and impact of SAFE-T, focusing on the pre-implementation and first year of the program. Understanding these perceptions is essential to continuous quality improvement and increases the likelihood of program growth and sustainability within and across communities.
We aimed to answer the following research questions in this study: (a) What did stakeholders view as gaps in service or challenges to creating an ideal response to SA forensic health care prior to the SAFE-T program implementation?; (b) Following program implementation, what changes, if any, were observed by stakeholders related to local ability of staff to deliver SA care; quality of SA care; coordination with multidisciplinary partners; and (c) How could program implementation be improved and/or were there SA community response needs that were not addressed?
Partner Communities
The SAFE-T Program is housed within the Ross and Carol Nese College of Nursing at The Pennsylvania State University. All three initial pilot sites are in rural communities in Pennsylvania. One of the three hospitals is designated as a critical access hospital, having no more than 25 inpatient beds and no other hospitals within 35 miles (Pennsylvania Office of Rural Health, 2021). Site selection and engagement activities have been discussed in a previous publication (Miyamoto, Thiede, et al., 2021).
Methods
Design
This study used qualitative thematic analysis of in-depth, semi-structured, key informant interviews of stakeholders working in the initial three SAFE-T partnered communities. In-depth interviews provide more detailed information about an individual's experience or the perceived impact of a program than what may be elicited through other methods such as surveys (Boyce & Neale, 2006). An interview guide was developed by the first and second authors with input from the fifth author.
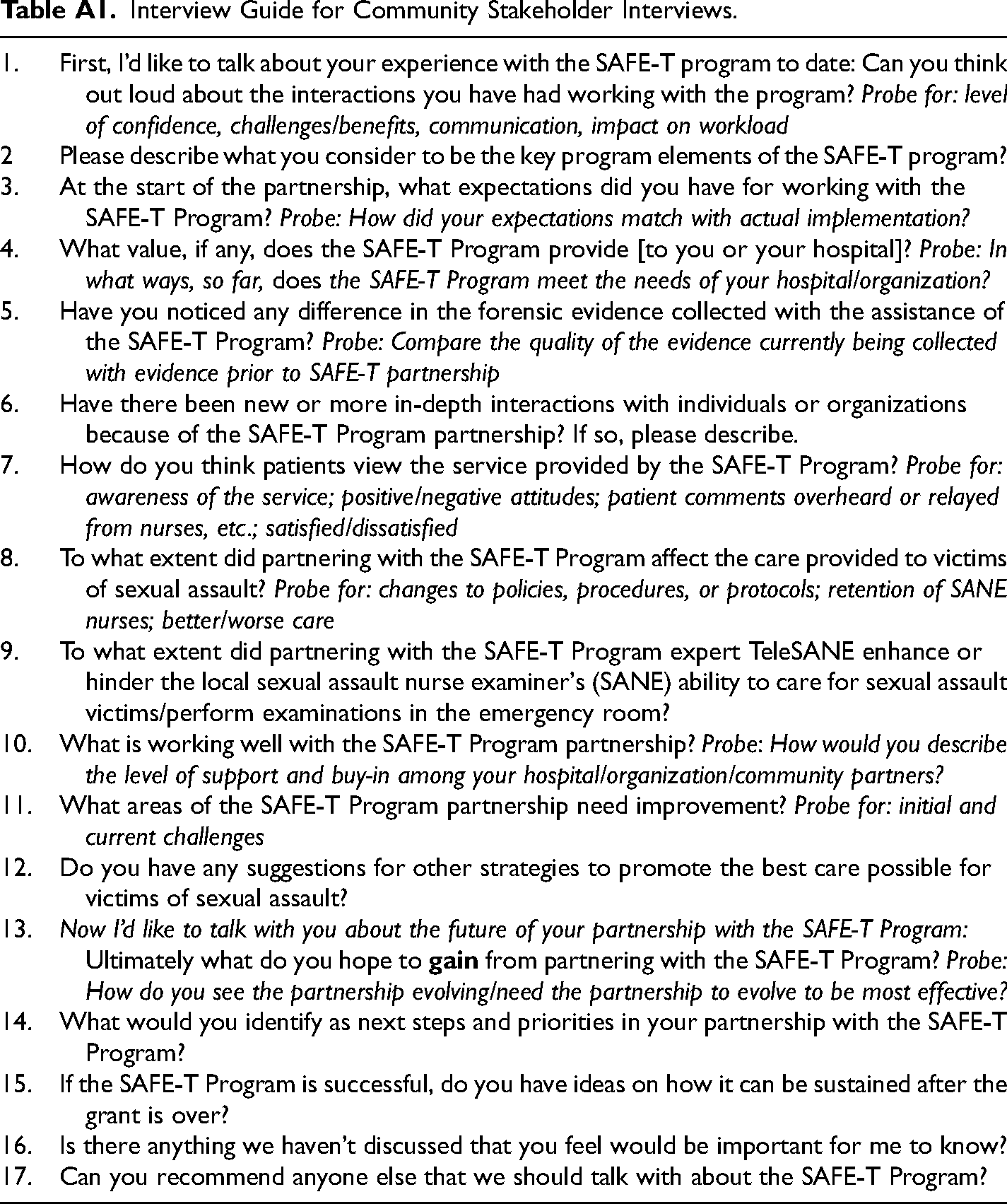
Interview questions focused on identifying and understanding site's pre-implementation needs and challenges, SAFE-T's effects on hospital systems (e.g., protocols, staffing procedures), perceived value and cost of participation, and identification of needs not met by SAFE-T. Questions related to quality focused on SAFE-T's impact on nursing, patients/survivors, and inter-agency collaboration. The interview guide was semi-structured, consisting of open-ended questions that guided the conversation through preassigned topics, but also allowed opportunities for participants to discuss topics the researchers may not have considered (Monroe, 2002). Sample questions from the interview guide are provided in Table A1. The university's Institutional Review Board determined the study to be exempt. Interviews were conducted between April and May 2019.
Following thematic analysis, results were organized broadly into two categories: Identified barriers to quality SA care (pre-implementation) and program impact (post-implementation).
Setting, Participants, and Recruitment
Participants
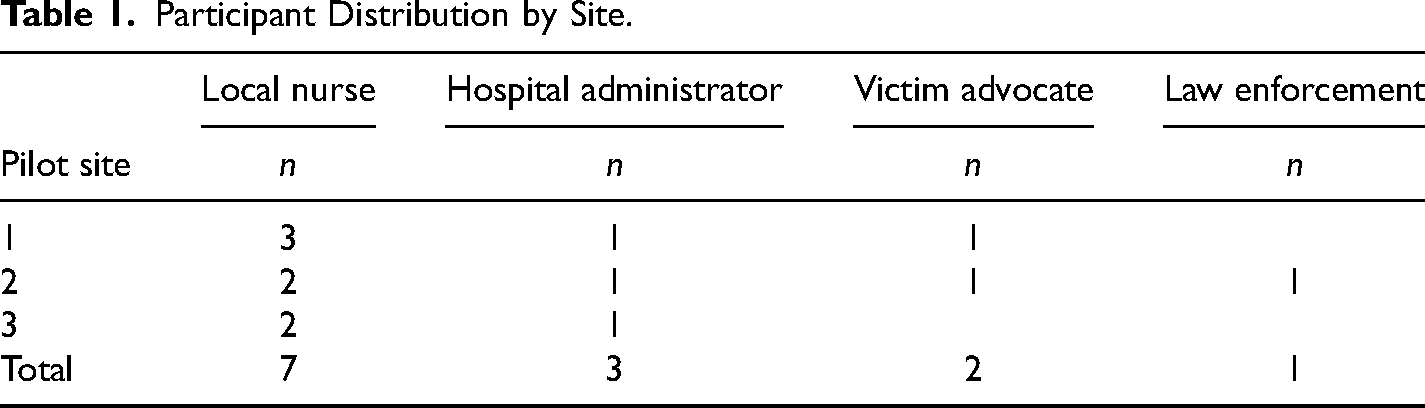
A total of 14 key stakeholders were invited to participate, with 13 interviews completed. Participant stakeholders included victim advocates (n = 2), nurses (n = 7), hospital administrators (n = 3), and law enforcement officers (n = 1) recruited from each of the first three SAFE-T Program rural site partner communities. Interviews took place approximately nine months after implementation using a purposive sampling approach. At that point, the SAFE-T Program had conducted 21 telehealth consultations among the 3 sites and each site had experienced a minimum of five consultations. We sought input at each site from the chief nursing officer (CNO), local SANE-trained nurses who conducted examinations using the telehealth program, community advocates who attended examinations to provide support to the victim, and law enforcement officers who interacted with the program. Participants must have interacted with the SAFE-T Program intervention in their community or had participated in SA exams where SAFE-T telehealth consultation occurred.
While law enforcement and district attorneys are important multidisciplinary community partners in the response to SA, rural communities often lack a dedicated SA unit or detectives who are more likely to have a nuanced awareness of the early impact of healthcare system response changes. District attorneys more frequently become involved as the investigation reaches the final stages and therefore more time is required before they will have feedback on the impact of the program on issues of importance for prosecution. As such, while attempts were made to recruit law enforcement informants at each site, only one respondent (a police officer) had clear program interaction. District attorneys did not have substantial interaction with cases conducted during this early stage of the program, and therefore were not interviewed at this time.
Recruitment
The principal investigator developed a comprehensive list of all stakeholders meeting the above criteria to be approached for participation in the study. All invited stakeholders agreed to participate; however, one indicated that they did not have enough interaction with SAFE-T to inform this study, and thus were not interviewed. Stakeholders were invited to participate by email. Subsequent interviews were conducted by one of two evaluation researchers.
Researcher description
Two interviewers, both with training and experience in qualitative interviewing methods, conducted the interviews. One interviewer, who also had training in qualitative analysis and worked on research-related aspects of SAFE-T, analyzed the data with the principal investigator. The researchers reviewed the interview guide and conducted three initial interviews together to standardize the approach. The interviewers were not known to those being interviewed and had not been engaged in SAFE-T implementation in the partner communities. The decision to have neutral interviewers was made to promote comfort for respondents to provide critical program feedback (negative as well as positive), decreasing possible response bias from stakeholders.
Data Collection and Analysis
Data collection and management
Interviews for this key informant analysis were conducted via Zoom (Zoom Video Communications, 2021). All interviews were audio recorded, transcribed, and checked for accuracy by the interviewers. The software program Dedoose (Version 8.2 14) was used to organize data and facilitate analysis of the interviews. Interview length ranged from 45 to 85 min.
Analysis
Thematic analysis was conducted through an iterative process of emergent coding within the two broad areas of interest for this study: (a) Identified barriers to quality SA care prior to SAFE-T implementation and (b) Program impact post-implementation. Following suggested methodologies, transcripts were read and coded by the second author and another researcher (Cavanagh, 1997). Coding discrepancies were resolved in meetings to develop a codebook. Coded data were used to identify patterns and similarities. The first and third authors read transcripts, reviewed codes, and identified emerging themes. Themes were coded and grouped into prominent themes and validated through team discussions. The authors conducted reliability and validity checks by continuously assessing for confirmatory and contradictory evidence of the themes (Morse et al., 2002). Participants’ verbal hesitations were deleted to improve readability. Data collection continued until all potential stakeholders had been interviewed. As we interviewed all available stakeholders, we were not aiming for data saturation.
Results
Sample/Participants
Fourteen stakeholders from each of the three SAFE-T Program partner sites were invited to participate in interviews. Thirteen interviews were completed. A preliminary discussion with the fourteenth stakeholder indicated they did not have enough interaction with SAFE-T to inform this study. Because of the small number of stakeholders that met criteria for participation, an equal number of each stakeholder type across each of the three sites was not possible (Table 1). All participants were white, and all but three were female.
Participant Distribution by Site.
Identified Barriers to Quality SA Care (Pre-Implementation)
Participants were asked to reflect on the barriers to the provision of quality SA care that existed prior to SAFE-T implementation. Participants frequently described challenges, or barriers, related to healthcare delivery, including rural settings, workforce, and training barriers. Participants felt that a comprehensive program such as SAFE-T was necessary for overcoming the many barriers they faced in mounting a comprehensive SA response.
Rural SA healthcare delivery and workforce barriers
Participants from each site described instances where survivors were turned away from their hospital due to staffing shortages. Though each partner hospital had taken measures to enhance their SA care programs prior to SAFE-T implementation, such as providing SA care training for a few nurses, they did not have a paid, “on-call” system to ensure survivors would have access to a trained nurse when they presented to their facility. This often led to long wait times and patients leaving.
Participants also cited the lack of a readily available, trained, and confident nursing workforce as a substantial barrier to delivery of consistent, high-quality SA care. A hospital administrator described how things worked prior to SAFE-T implementation: We had two or three SANE nurses, no consistent schedule, our coverage was just someone who was working. We were fortunate if [a SANE] was available over a weekend. People in the ER waited a very long for the nurse to come in at times. And, the nurses, they did not want to do the exams, just because of low volume. They did not feel comfortable doing it. (Hospital administrator, Site 3)
Participants pointed to low volume, or very few SA survivors presenting for care, as a major factor contributing to nurses’ lack of expertise and confidence. According to participants, nurses could receive training and continuing education, but without a sufficient volume of patients, they could not develop or maintain their clinical skills.
Clinical training barriers
Workforce scarcity is complicated by the specialized training needed to provide quality SA care. Nurses do not receive SA training in their degree programs and when post-degree training is acquired, there are often inadequate support or expertise at rural hospitals for mentoring or quality assurance oversight (US GAO, 2016). Nurses described that training without clinical precepting and ongoing mentoring in low-volume centers was insufficient and led to discomfort in taking on the SANE role. You do not have those skills coming out of school…and with us not having that volume… if we were doing a ton of cases, you would learn it, but we do not have that ability here. The quality that we were providing to our patients would not be nearly as good as we can provide now [with SAFE-T]. I would not feel comfortable, even having years of experience as a nurse, because none of [my experience] was in forensic nursing or even OB/GYN trauma. Without having the support of the SAFE-T team, I would not feel comfortable doing this. (Local nurse, Site 3)
Nurses described feeling overwhelmed by assuming this role without access to experienced mentors or a network of colleagues who could provide guidance, education, and support through shared experiences. They acknowledged their skills and knowledge of best practices slipped over time without continuing education and access to expert review. A nurse described the challenges of maintaining skills in a low-volume rural setting: I think one of the biggest keys is the quality the program brings to our community. Because we have so few cases, our nurses do not see it [SA] very often. We are definitely not kept up to date with changes in practice. We had a couple of nurses go through the online course training, but there was no follow up from that course and with so few cases it is not something that we kept up on. So, the quality that it has brought to our exams has been huge. (Local nurse, Site 1)
Similarly, the lack of volume and experience often made it difficult for nurses to provide trauma-informed care. For example, a hospital administrator acknowledged the difficulty less experienced nurses have in balancing the detailed tasks of evidence collection with provision of patient-centered, trauma-informed care that meets victim needs. They were so focused on data collection and kit collection that they really neglected the [patient]. They truly were just always [evidence collection] kit-focused. They would open up the kit and there was a check sheet and they just went through the boxes…and kind of like an assembly line to make sure they’re doing it, because they’re just paranoid and worried… “I’m going to mess up something in the kit. I don’t want to do that.” (Hospital administrator, Site 3)
The concern that nurses shared related to low volume and quality were paralleled in reflections from multidisciplinary community partners. Participants discussed inconsistency in quality of care related to staffing, training, and evidence collection equipment. Prior to SAFE-T being implemented, rape exams were not done very frequently. …It really hindered the quality of evidence that was being gathered, the quality of the photos that were being taken with a small digital camera and people not being trained. Before the SANE nurses, it would be an emergency room doctor that would perform the rape exam, and they often were not familiar with the process. They had to keep stopping and reading the directions and it was a very long process. The victim would have to sit in the waiting room for hours waiting for a doctor to be available to do the exam, and it was just not an efficient process. (Advocate, Site 1)
SAFE-T Program Impact
Participants described that the SAFE-T Program impacted several areas that had previously been barriers to quality care provision. Participants noted changes in their hospital protocols and systems, increased access to care for victims with implementation of a trauma-informed approach, multiple impacts on local nurses, and support for multidisciplinary collaboration.
Hospital protocol and system changes
The SAFE-T implementation led to a transition from emergency physician-led SA examinations to SANE-trained nurse-led examinations at all sites. This change is in line with SA protocols developed and endorsed by the Department of Justice (OVW, 2018). The sites also initiated paid on-call schedules to ensure 24-h coverage by SANE-trained nurses. Additionally, all sites implemented a process to ensure that victim advocates were called to respond to the hospital for every examination. Prior to this change, patients were offered the option to call an advocate, and this was frequently declined as the role of the advocate was not clear to the patient. Once an advocate was present and could explain the support they could provide for the patient, their presence was always accepted. This was an important shift toward multidisciplinary collaboration and increased support for the patient. These examples reflect important system-level changes to care.
Participants emphasized the importance of external investment for the achievement of system-level changes. They explained that having SAFE-T investment stimulated local plans to accomplish change that was previously not possible (e.g., on-call pay for nurses). A hospital administrator explained how unprecedented change happened by leveraging the gains that SAFE-T would provide their hospital. So internally, some of the barriers… how we are going to pay for it? As we transitioned [to SAFE-T implementation], this little hospital actually changed the call time for the entire system, and we are not a large urban hospital. We have to do call time and it was a bit of a battle, but through lots of conversations and helping human resources, finance, and some other folks understand what our situation was… We got on-call pay, the way we wanted it. (Hospital administrator, Site 1)
Increased local SANE workforce and access to care
The availability of local SANE nurses impacts access to care. All sites endorsed that the promise of expert support led to increased interest from nurses in taking on the SANE role. This interest directly impacted the ability to attract and retain local nurses as SA responders. A local nurse had not previously been exposed to the role as it is not typically part of nursing education. It wasn’t until the SAFE-T Program came here for that first presentation that I learned about [forensic nursing]. After that presentation, I went to the ER manager and said, “I want to do this!” SAFE-T Center is the entire reason why I even started becoming a SANE nurse, why I have just really fallen in love with the process and the support that we give to our patients. (Local nurse, Site 1)
The SAFE-T Program also impacted local SANE-trained nurse retention. One local nurse said, “I couldn’t wait for the program to start—a second set of eyes, that expertise is so appealing and reassuring.”
Participants discussed the impact of program changes on local access to SA care, citing a difference in how patients and their families viewed the care received. A nurse participant described this change: Even family members have said how wonderful the program is and how lucky we are to have something like it. I had one experience where the patient had gone to a different hospital first and had a very, very poor experience and [left that hospital] then came to [our partner hospital for care]. She spoke so highly of how well the exam went and how she was happy with the process, so I think it is a big benefit for the hospital. Even her family members said how happy that they were and how they were treated, respected, listened to, and how having the extra set of eyes there [presence of SAFE-T teleSANE] was so beneficial. (Local nurse, Site 2)
The number of SA survivors cared for increased following program implementation (Table 2). Some participants perceived this increase was due to reduced wait time for care. Other participants attributed the increased number of cases seen to the possible impact of increased community awareness through the investment in quality SA care. One hospital administrator framed it this way: [Introduction of the SAFE-T program] added a general awareness to the community about the fact that this is a pretty prominent issue that needs to be addressed and we are trying to address it with high standards. And we are doing it as a partnership. (Hospital administrator, Site 2)
Increases in SA Examinations Conducted Pre- and Post-SAFE-T Program Implementation.
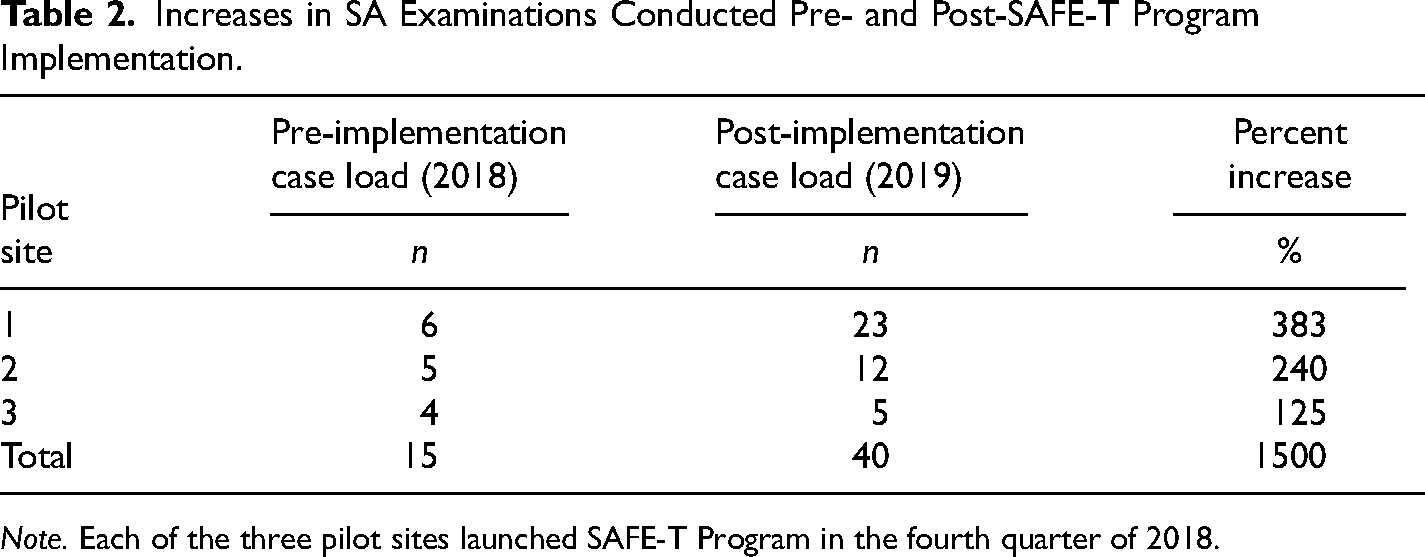
Note. Each of the three pilot sites launched SAFE-T Program in the fourth quarter of 2018.
Importantly, there was recognition from participants that previous inequalities in SA care quality were improved once SAFE-T was put in place. “It [SAFE-T Program] really benefits the community. It ensures that if something does happen to your sister, your mom, your brother, or whoever, that they are going to get the best care that they can in such a rural area” (Advocate, Site 1).
Impact on nursing
Nurses practicing in partner hospitals play a central role in the SAFE-T Program and the quality of the care received by SA survivors. Important themes emerged related to SAFE-T's impact on local nursing confidence, ability to conduct forensic examinations and provide compassionate care, and on nurse job satisfaction.
Enhanced nurse confidence. Stakeholders described that local nurses were more confident in the care they delivered. A hospital administrator explained: I think it is a big gain for the patients because we have a group of nurses that are more engaged and more confident about doing the exams. Instead of having nurses that are petrified, who are flipping a coin to see who is going to do the SA exam because they don’t feel comfortable and they’re worried. We have people who are up to bat and ready to do it. (Hospital administrator, Site 2)
Nurses discussed that being part of a larger peer network and receiving post-consultation support from the teleSANEs led to increased confidence in their role. Personally, the value [SAFE-T] has brought is that before, each case left me with the feeling of, “Oh my gosh, what did I just do in that room?” You know, no support emotionally when you left there. I would stay awake for hours, and think, “Did I serve this patient well? Should I have done that? Did I write this down right?” Because if this case does move forward to trial, am I going to do this person a justice, not only in that exam room, but also outside with the legal aspect too? There were always questions in my mind about how I did. Now we have that support. I know we are not perfect and there is still always room for improvement, but we feel more confident with each exam. (Local nurse, Site 3)
I was talking to them [SAFE-T teleSANEs] for days after this case …so you know they support you, not just during that [consultation] time, but afterwards. And we have weekly meetings. I think just the continual support is big. It is not just the two hours you spend in the room with the telehealth consultant. (Local nurse, Site 1)
Supportive mentoring and expert partnership. SAFE-T was designed to partner with local nurses to provide live mentoring and quality assurance to enhance SA care and build local expertise. Nurses talked about the value of having an experienced SANE present in real-time to support thorough, quality care during a complex examination. One nurse described the partnership: My team talked initially about how we are kind of anxious to have this person [teleSANE] with all this knowledge and experience [watching us] and we had real fears that we are going to look and feel like idiots. And that never occurred. It is such a team approach. It is constant feedback in such a positive nature. It feels like you have your best friend in the room with you. It is not like it is a robot monitor. It is like someone is right there with you to bounce ideas off or try something different. (Local nurse, Site 3)
Nurses discussed the complex care they were expected to deliver, concerns about lack of experience, and how the care they provided changed because of SAFE-T partnership. A nurse described her very first case and her experience with the SAFE-T consultation: It was a very complicated case. There were a lot of pieces that were not typical. The case was very tricky and nerve racking. I think if I had done it on my own it would have been very difficult. I do not even know if I would have known where to start. I think about some of the complexities of this case that I had not thought through and would not have been able to handle. It was not something that was covered in my training that I did online…so it was really helpful to have that one-on-one expertise and training right there. The professionalism that [the teleSANE] had that did not make the patient seem uncomfortable or make me feel like I didn’t know what I was doing. She was very supportive and respectful through all of it, so the patient felt like they were getting really good care as opposed to being stuck with a new nurse who had never done an exam before. (Local nurse, Site 1)
Local nurses discussed the importance of expert partnership in settings where their own exposure to SA cases is low, limiting their ability to develop internal expertise. I can start an IV with my eyes closed because I do so many of them in one shift. I have done three rape exams in one year. You can’t compare that to the TeleSANE nurse, who is on the monitor with me, who has done 300 that year and is able to tell me, “Try this position”, or “What are you seeing there? How would you describe that?” It's invaluable. This service is needed. (Local nurse, Site 3)
Impact on inter-Agency collaboration/Stimulating multidisciplinary collaboration
Participants discussed the development of multidisciplinary partnerships and resulting positive impacts for patients. Participants discussed partnerships that formed when they came together at their local SAFE-T launch. At one site, these new partnerships resulted in the collaborative creation of anonymous reporting policies so survivors can receive medical care and evidence collection without making a police report, allowing them time to decide if they want to pursue a criminal justice investigation. A law enforcement officer described the initial resistance to anonymous reporting and how the multidisciplinary partners came together to create protocols: Now that we have all sat down and talked, we can understand and appreciate each other's roles and where each agency is coming from. Then we worked toward our end result of a collaborative agreement between all entities that everyone is happy with and is able to work with. (Law enforcement officer, Site 3)
One of most recent [cases], the victim presented and did not want law enforcement involvement, did not like police. I still responded and gave a pamphlet of information to the SANE and they provided it to the victim. Within a day after talking to the [advocacy group], the victim reached out [to police]. It was only because I responded and provided information and broke that barrier. (Law enforcement officer, Site 3)
Implementing trauma-Informed care to promote a healing pathway
A clinical need identified by stakeholders was for nurses to not only be skilled at evidence collection, but to provide trauma-informed care that is supportive, without judgment or blame, and that empowers individuals to exercise control of all aspects of their care. A law enforcement participant described the impact of SAFE-T on patient care: “Victims feel as though they are regaining some type of control from an incident that took all control from them. I see that as an extreme positive from the past to where we are now” (Law enforcement officer, Site 3).
A nurse described how her understanding of trauma-informed care grew through the SAFE-T partnership. I have learned a lot more about the victim role, how they must feel or how to respond to them better or in a different way. There was always compassion, and I still have that, but as a nurse, now I’m able to take that to a different level…to ask them different questions than I normally wouldn’t have asked before. “Do you have a place to go after you leave here?” I would not have done those things [before]. I did not think of it—it was more like a process: you have a patient, you get the consent, you take their history, you do an exam. (Local nurse, Site 3)
Patient advocates discussed changes in nurses’ understanding and supportive response to the trauma victims experienced. They also reflected on the impact of improved relationships and multidisciplinary team approach to care because of process changes encouraged by SAFE-T (e.g., advocates are called to respond to every SA). This multidisciplinary change that occurred under the SAFE-T model may also impact patient engagement with supportive community services. As one advocate explains, “The exam that I attended where the SAFE-T program took place, that client is still very active, still receiving follow-up counseling services. I think it builds a stronger rapport in the initial visit and encourages them to receive follow-up care” (Advocate, Site 1).
Discussion
This paper highlights participant's perceptions of barriers to the delivery of quality SA care within their rural communities and the impact of the implementation of a comprehensive telehealth forensic SA model that provided training, support, and access to expert SANE consultation and quality assurance. Novel SA telehealth programs, like SAFE-T, aim to address trained workforce shortages and SA access and quality issues in underserved communities. In our study of multidisciplinary perspectives of stakeholders on the implementation and impact of SAFE-T on local SA care, findings confirm previous research showing the barriers rural health systems face in building and sustaining quality SA care (Littel, 2001; Logan et al., 2007; Taylor, 2002; Ullman, 1996) and adds data that illuminates the perceived value of this program to stakeholders engaged in SA care and response.
Evaluation research following implementation of programs is essential to support growth of this novel solution. To date, evaluation of SA telehealth programs has focused on quality-of-care outcomes and provider perspectives of consultations (Macleod et al., 2009; Miyamoto et al., 2014, Walsh et al., 2019). As stakeholders reflected on the impact of SAFE-T, they frequently cited program elements outside of clinical consultation. Guidance and advocacy from SAFE-T for system-level changes (i.e., on-call pay for SA nurses) to support local nurses and multidisciplinary collaborations were cited as important in fulfilling community and workforce needs. Without financial incentives or regulatory mandates to guide hospital investment in SA programs, many lack the understanding of how to establish quality models of SA care and it may not be a priority area for hospital administrators when the number of patients requiring SA services is low. As participants spoke about needs and gaps prior to SAFE-T implementation, there was a sense of not knowing where to begin to make change. Thus, comprehensive hubs of expertise, such as SAFE-T, may be needed to guide hospitals to implement change strategies.
Similarly, nurses talked about their relationship with the SAFE-T teleSANE team and the wraparound support they received in addition to live examination support including pre-consultation training, court testimony preparation, and emotional support post-consultation. They described being connected to a broader community of SA nurses and how that increased their confidence and made them feel less alone in the work. These findings suggest that while telehealth can readily place an expert in a remote clinical location, enthusiastic acceptance, adoption, and program sustainability may lie in comprehensive supports, such as coaching, and relationships that extend beyond the case-by-case clinical consultation (Chilenski et al., 2016, 2018). Our findings suggest that external expertise and clinical program guidance constructed within an adaptive, community collaborative approach positively impacts local system change and the quality and consistency of rural SA care. These findings add information regarding the implementation of telehealth programs that are acceptable, meet community needs, and are valued by stakeholders. Importantly, since this study was conducted, the SAFE-T program has been implemented in additional sites including suburban and urban, level 1 trauma centers. The SAFE-T program has continued to be accepted and valued by stakeholders in helping to solve access issues in all types of hospital settings.
This study has notable strengths. Many programs are implemented with attention to only clinical outcomes; multidisciplinary stakeholder perspectives have not been previously reported in SA telehealth program research. Programs are more likely to be sustained when value is recognized broadly across community stakeholder groups (Israel et al., 1998). Our research also allowed us to learn from our first three implementation sites about the perceived value of the SAFE-T program implementation and impact. We sought to learn about the actual implementation process with a research question focused intentionally on participant's perception of need for implementation improvement or aspects of the program that were not working or well-accepted. The only feedback of this kind came from one participant who mentioned that there were some technology issues during initial consultations. Many other statements seemed to reflect stakeholders’ perception that they were active partners in a continuous quality improvement process and were accepting of start-up issues as we learned together. A participant emphasized that the program was tailored to the needs of each site and designed to build on local strengths. I mean, [SAFE-T] is flexible enough to see what each individual institution needs and then make changes to the bigger program. It is not just a face on a screen telling a nurse what to do. It is an expert to guide us through everything from the technical aspects to the psychosocial needs [of the patient]. (Hospital administrator, Site 1)
Lack of suggestions for improvement may be reflective of our adaptable, strengths-based approach to implementation in each community. We conducted interviews with multidisciplinary stakeholders (hospital leadership and nurses, advocacy, law enforcement, and district attorneys) prior to implementation to understand what worked well and what they would like help with. We then tailored program activities to specifically target unmet needs. We gave all partners access to SAFE-T program staff and encouraged their input throughout the implementation. This approach allowed us to address community requests rapidly and may have contributed to little reflective feedback for ways we could improve the implementation process.
We applied a dynamic systems-approach when implementing SAFE-T, as technology issues were anticipated and technology support was on-call and readily available (blinded for review, 2021; Chambers et al., 2013). As cases progressed, we analyzed technology issues and found that user error rather than equipment failure was responsible for identified malfunction. We took this information and enhanced technology training by adding hands-on mock consultations and streamlined technology instructions in later site implementations, preventing similar issues. This real-time optimization approach, as emphasized in the guiding DSF framework, made it likely that many such issues were resolved prior to conducting these interviews within the first year of implementation and resulted in the lack of findings related to areas for improvement.
This study has several limitations. First, SAFE-T was implemented in hospitals eager to improve SA care. Overall acceptance and impact may differ if the program were randomly assigned. Second, during interviews we tried to elicit areas for improvement in the implementation process; however, participants largely reflected on program success and positive impacts. Interviews were conducted approximately nine months after program implementation, so participants had to reflect on early aspects of collaboration and may have decreased memory of events. Third, there was a lack of diversity among the sample in terms of race or ethnicity as all participants in this study were white. Although we do not know the demographics of each site location or its hospital (employees, patients), it is important to note that all the stakeholders in our rural partner settings are white, therefore it was not possible to include more diverse perspectives. The lack of perspective from individuals from historically marginalized groups (e.g., racial and/or gender minorities) may make the findings difficult to generalize across diverse communities, as these individuals may have different perspectives on the effectiveness of the health care and legal system due to experiences of racism, bias, or violence within those systems. Additionally, the lack of diverse racial representation among SA response leaders (medical staff and administrators, law enforcement, and victim advocates) likely contributes to additional barriers to care-seeking among minority groups. Efforts to grow a racially diverse workforce within local SA community response sectors should be encouraged and may lead to enhanced disclosure and access to services if a racially concordant response between victims and first responders is available (Cohen et al., 2002). Finally, the acceptability of telehealth services by those who have sought care for sexual assault, is an important perspective of any SA care evaluation. The patient perspective was not addressed in this study, as this paper was focused on program need prior to implementation of the SAFE-T program and the changes or impact within the first year of implementation by those engaged with the program. The perspective of the individual SA victim on the quality and acceptability of SAFE-T services has been described previously (Miyamoto, Thiede, et al., 2021) and additional manuscripts detailing survivor perspectives are in press.
Conclusion
According to stakeholders, SAFE-T provided valuable solutions to address community, workforce, clinical and patient needs for SA care. Understanding stakeholder needs, perspectives on meeting those needs, and overall program impact is essential to improve implementation of future sites, and to provide effective knowledge for preparing and launching SA telehealth partnerships. Our data also suggest there is value in the comprehensive program elements that extend beyond clinical consultation including training, advocacy and guidance for system-level change to support nurses and connect them to a supportive network of colleagues. Based on our study, local nurses, hospital administrators, victim advocates, and law enforcement see improved clinical care and compassionate, trauma-informed support of patients due to SAFE-T.
Future research should follow these stakeholders across time with questions relevant to the status of SAFE-T at each site and the patients seen. Knowing what the changing involvement is across time for some community stakeholders not represented here (i.e., DA's) also would be beneficial. Further, as new sites are added it would be important to see if findings are similar to what is reported here. Gathering data about community differences (e.g., population, demographics, etc.) of those sites may contribute to understanding similarities or differences and in turn, modifications in the program.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, U.S. Department of Justice, National Center for Advancing Translational Sciences (grant number P50HD089922, 2016-NE-BX-K001, UL1 TR002014).
Author Biographies
![]() ). Daniel is interested in hybrid evaluations of preventions and interventions, implementation science, and community-based delivery models. He has been designing and evaluating strengths-based family and youth development programs in Cooperative Extension and leading complex projects for 25 plus years. Since 2001, he has co-led the implementation of an evidence-based University-community partnership model for delivery, dissemination and sustainability of evidence-based preventive interventions.
). Daniel is interested in hybrid evaluations of preventions and interventions, implementation science, and community-based delivery models. He has been designing and evaluating strengths-based family and youth development programs in Cooperative Extension and leading complex projects for 25 plus years. Since 2001, he has co-led the implementation of an evidence-based University-community partnership model for delivery, dissemination and sustainability of evidence-based preventive interventions.
Appendix
Interview Guide for Community Stakeholder Interviews.
| 1. | First, I’d like to talk about your experience with the SAFE-T program to date: Can you think out loud about the interactions you have had working with the program? Probe for: level of confidence, challenges/benefits, communication, impact on workload |
| 2 | Please describe what you consider to be the key program elements of the SAFE-T program? |
| 3. | At the start of the partnership, what expectations did you have for working with the SAFE-T Program? Probe: How did your expectations match with actual implementation? |
| 4. | What value, if any, does the SAFE-T Program provide [to you or your hospital]? Probe: In what ways, so far, does the SAFE-T Program meet the needs of your hospital/organization? |
| 5. | Have you noticed any difference in the forensic evidence collected with the assistance of the SAFE-T Program? Probe: Compare the quality of the evidence currently being collected with evidence prior to SAFE-T partnership |
| 6. | Have there been new or more in-depth interactions with individuals or organizations because of the SAFE-T Program partnership? If so, please describe. |
| 7. | How do you think patients view the service provided by the SAFE-T Program? Probe for: awareness of the service; positive/negative attitudes; patient comments overheard or relayed from nurses, etc.; satisfied/dissatisfied |
| 8. | To what extent did partnering with the SAFE-T Program affect the care provided to victims of sexual assault? Probe for: changes to policies, procedures, or protocols; retention of SANE nurses; better/worse care |
| 9. | To what extent did partnering with the SAFE-T Program expert TeleSANE enhance or hinder the local sexual assault nurse examiner's (SANE) ability to care for sexual assault victims/perform examinations in the emergency room? |
| 10. | What is working well with the SAFE-T Program partnership? Probe: How would you describe the level of support and buy-in among your hospital/organization/community partners? |
| 11. | What areas of the SAFE-T Program partnership need improvement? Probe for: initial and current challenges |
| 12. | Do you have any suggestions for other strategies to promote the best care possible for victims of sexual assault? |
| 13. | Now I’d like to talk with you about the future of your partnership with the SAFE-T Program: Ultimately what do you hope to |
| 14. | What would you identify as next steps and priorities in your partnership with the SAFE-T Program? |
| 15. | If the SAFE-T Program is successful, do you have ideas on how it can be sustained after the grant is over? |
| 16. | Is there anything we haven’t discussed that you feel would be important for me to know? |
| 17. | Can you recommend anyone else that we should talk with about the SAFE-T Program? |